Embed Size (px)
Citation preview

'4I
PITUITARY, PINEAL AND THIRD VENTRICLETUMOURS
By JOE PENNYIIACKER, M.D., F.R.C.S.The Nuffield Department of Surgery, Radcliffe Infirmary, Oxford
The pituitary gland is concerned with suchdiverse functions as growth, sexual activity, carbo-hydrate and water metabolism, physical energyand the character and distribution of hair. For itssize it is a very eloquent structure and although notsolely responsible for any of these activities, it hasbeen described as the leader of the endocrineorchestra. Many of its disturbances of functionare more in the province of the physician than thesurgeon. This section is concerned only withthe effects produced by tumours. For practicalpurposes only two types need description, thechromophobe and chromophil adenomas. Thesetumours acquire their descriptive titles from pre-ponderance of either the chromophobe or chromo-
phil cells found in the normal gland, although puregrowths of either are rare, and in most cases itwould be more correct to speak of a mixed-celladenoma. The basophil element occasionallyundergoes hyperplasia and in some cases isassociated with what is widely known as Cushing'ssyndrome, but in about half the recorded cases ofthis condition the essential lesion seems to be inthe suprarenal gland-another example of theinter-relation of the pituitary with other endo-crine glands. The basophil adenoma is generallynot a surgical problem, and although some goodresults have followed the implantation of radonseeds in the pituitary gland, treatment usually con-sists of deep X-rays directed to the region ofthe sella.
FIG. I.-Enlarged sella in chrorniophobe adenoma.
Protected by copyright.
on Novem
ber 2, 2020 by guest.http://pm
j.bmj.com
/P
ostgrad Med J: first published as 10.1136/pgm
j.26.293.141 on 1 March 1950. D
ownloaded from

i142 POSTGRADUATE MEDICAL JOURNAL March 1950
Although endocrine disturbances are commonin pituitary adenomas, the effect on vision isequally important. Indeed, it is generally thiswhich leads the patient-to seek advice, and surgicaltreatment is directed largely to preserving eyesight.The normal gland lies snugly in the pituitary fossawith the optic chiasm suspended above it in acapacious part of the subarachnoid space known asthe chiasmatic cistern. As the tumour grows it iseasier for it to push the diaphragma sella upwardsthan to displace the bony walls of the sella,although this does happen eventually and in almostall cases there is radiological evidence of enlarge-ment of the sella turcica by the time the patientcomes for treatment (Fig. i). As the tumour ex-pands in an upward direction it first obliterates thechiasmatic cistern, then begins to compress theoptic chiasm. The effect of this is to interrupt con-duction in the visual fibres coming from the nasalhalf of each retina which subserve the temporalfield of vision.
Bitemporal hemianopia is thus common. Itmay be complete and easily detectable by simpleconfrontation tests with the examiner's hands.The patient may be aware of it, and it may be hisfirst symptom. In the early stages of its develop-ment, however, the hemianopia may be so slight
that it can only be detected by careful perimetry;it usually begins with a defect in the upper quad-rant of the temporal field, and it is commonlyasymmetrical, one eye being more affected thanthe other (Fig. 2). Rarely the- defect may belimited to one eye; in such cases the tumour pre-sumably exerts specific pressure on one part of thechiasm or on the medial border of one optic nerve,although it is often impossible to be certain ofthese relations at operation.The acuity of vision is not disturbed until the
macular fibres are involved and the field defectencroaches on the fixation point. Thus it ispossible for a person to have a complete bitem-poral hemianopia, except for a degree or so ofsparing at the fixation point, and to have normalacuity. As soon as central vision begins to go, thevisuai acuity drops quickly, and the field defectprogresses until there is only a bean-shaped islandpreserved in the nasal field. Eventually this goesand the eye is rendered completely blind.Although the initial effect is usually on the optic
chiasm, both optic nerves are eventually involvedand at operation these nerves are usually found tobe splayed apart and flattened on the upper surfaceof the tumour. This direct pressure inducesprimary optic atrophy and some degree of pallor of
.......... .. ..........;
. .- e biema hem a in a ce o b aena of th pitry.
..:
FJG .... ......et bie prlhmaopai..aeo hrm poeaeo a fteptiay
Protected by copyright.
on Novem
ber 2, 2020 by guest.http://pm
j.bmj.com
/P
ostgrad Med J: first published as 10.1136/pgm
j.26.293.141 on 1 March 1950. D
ownloaded from

March i 950 PENNYBACKER: Pituitary, Pineal and Third Ventricle Tumours 143
................... .e
FIG. 3.-Chromophobe adenoma with massive extra-sellar extension into third ventricle, compressingbrain stem.
the optic discs is usual; in early cases the pallormay be difficult to detect with certainty, andgenerally compression of the optic nerves andchiasm can be detected earlier and with morecerti.inty by perimetry than by ophthalmoscopicexamination.
It is rare for a pituitary adenoma to causepapilloedema. In one of our cases the adenomahad grown laterally to invade the cavernous sinus,and had then burst through this to obstruct theposterior part of the third ventricle and the upperpart of the aqueduct of Sylvius. This blockage ofthe circulation of the cerebrospinal fluid'causedobstructive hydrocephalus, much as any othertumour involving the third ventricle or aqueduct,and gave rise to the common ophthalmoscopicappearance of increased intracranial pressurewithout any evidence of direct pressure on theoptic nerves or chiasm. Although this event israre, it is common for the tumour to continue togrow upwards and in the late stages to assume asausage shape, one end resting in the expandedpituitary fossa and the other compressing theanterior end of the third ventricle (Fig. 3). Thismay also cause a certain amount of obstructivehydrocephalus but by the time it has happenedthere is usually a well-established primary opticatrophy and papilloedema does not develop.As mentioned above, the tumour may occasion-
ally expand laterally to involve the cavernous sinus.If so, ocular palsies may result from compressionof 'the third, fourth and sixth cranial nerves asthey traverse the sinus. The tumour may burstthrough the sinus and compress one optic tract,thus producing a homonymous field defect ratherthan the common bitemporal one. Or it may con-tinue to extend laterally, stripping up the durafrom the middle cranial fossa as it does so, andcome to expand in the temporal lobe. Similarly,supras'ellar extensions may grow to one or other
side and form a mass in one frontal lobe rather thanin the third ventricle as is usually the case.Some degree of downward extension is common
by expansion and thinning of the bony floor of thesella, but occasionally the floor is eroded com-pletely and the growth then expands to fill thesphenoidal air sinus.These are the mechanical effects of a pituitary
tumour, and as already noted surgical treatmentis largely concerned with them. The endocrinedisturbances to which they give rise will be dis-cussed in the clinical description of the chromo-phobe and chromophil adenomas.
Chromophobe Adenomas. These are about twiceas common as chromophil tumours. In ourmaterial there were 96 verified chromophobeadenomas and 49 chromophil adenomas. Theyare rare before the age of 20, but thereafter mayoccur at any age. Males and females sre aboutequally affected (52 males and 44 females in ourseries). It is usually some disturbance of visionwhich brings them under observation, but by thistime there are often some endocrine symptoms aswell, and it is not uncommon for a symptom suchas amenorrhoea or impotence to lead the patientto seek advice.
..
;0.0. jES, : MW8,,.,0,NNWFIG. 4.-Characteristic 'habitus of a patient with a
chromophobe adenoma.
Protected by copyright.
on Novem
ber 2, 2020 by guest.http://pm
j.bmj.com
/P
ostgrad Med J: first published as 10.1136/pgm
j.26.293.141 on 1 March 1950. D
ownloaded from

144 POSTGRADUATE MEDICAL JOURNAL March 1950
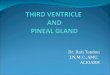
FIG. 5.-Arteriogram in a case of a moderately large chromophobe adenoma. Note displacement of terminal portionsof internal carotid arteries.
Intelligent and observant patients may first beaware of a defect in one or both temporal fields ofvision before there is any impairment of visualacuity. A defect in the right temporal field forinstance may cause difficulty in reading the end ofa line of type %without ' following it.' A defect inthe left temporal field may make it difficult topick up the beginning of the next line in reading.But more often it is reduction of visual acuity inone or both eyes which takes the patient to hisdoctor, and it is remarkable how often this is dis-covered accidentally; the patient may be rubbingor washing his good eye and suddenly realize thatthe sight in the other is defective. By this timethere is usually a well-marked temporal hemi-anopia as described above, and ophthalmoscopicexamination reveals primary optic atrophy. Alldegrees of field defects and loss of visual acuitymay be encountered up to complete bilateral blind-ness, depending on the stage at which the patientcomes under observation.Apart from the visual signs the neurological
examination is usually normal, unless there areextrasellar extensions of the tumour to causeocular palsies, mental symptoms, hemiparesis,etc. Some degree of headache is common, but itis rarely severe or persistent unless the tumour hasgrown into the third ventricle to such an extentas to cause hydrocephalus. In such late casesthere may be severe and protracted headache,
stupor and finally death as from any tumour in-volving the third ventricle.The findings described above are related to the
anatomical situation of the tumour. But there areother features, related to endocrine dysfunction,which may be little less striking. The patient isoften plump, and in the male the fat is commonlymost marked around the lower abdomen and pelvisto produce a somewhat feminine contour. Theface is rather round, ascribed by Cushing toprominence of the maxillae (as opposed to themandible in chromophil tumours) with relativesmallness and recession of the chin (Fig. 4). Theskin is soft and hairless on the extremities, andthe complexion is often somewhat sallow. Thehair of the head is soft and silky and that in theaxillae and around the pelvis is scanty or may bealmost absent. Adult males often need to shaveonly once or twice a week and to have their haircut at infrequent intervals, and the pubic hair hasthe feminine distribution.
Tht se patients often complain of lack of physicalenergy and of abnormal fatigue in normal occupa-tions. The objective counterparts of these symp-toms is sometimes found in low blood pressurereadings, lowering of the basal metabolic rate andincreased sugar tolerance.The endocrine symptoms so far described
usually manifest themselves in varying degrees;they are often slight and rarely profound. Sexual
Protected by copyright.
on Novem
ber 2, 2020 by guest.http://pm
j.bmj.com
/P
ostgrad Med J: first published as 10.1136/pgm
j.26.293.141 on 1 March 1950. D
ownloaded from

March 1950 PENNYBACKER: Pituitary, Pineal and Third Ventricle Tumours
7K
FIG. 6.-Arteriogram of basal aneurysm producing bitemporal F-emianopia.
activity is usually entirely lost; in females there isamenorrhoea and sterility, and in males impotenceand lack of sexual desire. As the secondary sexcharacters have usually developed before thetumour starts to grow they are not affected, but inadvanced cases there may be some atrophy of thebreasts and external genitalia. The control ofsexual functions exercised by the pituitary glandis so finely balanced that amenorrhoea or im-potence is often the first symptom of a pituit'rytumour and may long precede any other symptomsincluding impairment of vision. It is thus a usefulindex as to the length of the history. A patientmay report a sudden and recent awareness of abitemporal field defect, but on enquiry prove tohave had amenorrhoea for three years. It can betaken that the tumour has been present for at leastthis length of time.
It should be noted that endocrine symptomsand signs may be largely if not entirely absent, orthey may be very specific. Thus occasionallythere is a patient with only a bitemporal hemi-anopia and no other symptoms or signs, especiallyif the tumour begins to develop late in life whensexual activity has already ceased naturally. Orthere may be amenorrhoea or impotence; theseindeed are the most constant defects, but occasion-ally this function too is preserved. We have seenone case of chromophobe adenoma in which therewas persistent lactation for two years after child-
birth, and this symptom led to the detection of abitemporal hemianopia. Conversely it is veryrare to be able to diagnose a chromophobe'adenomafrom the endocrine manifestations alone, i.e;without a field defect; the same symptoms maybe due to various functional disorders of thepituitary without any enlargement of the sella asdetermined by skiagrams. By the time the sella issignificantly enlarged there is usually a defect inthe visual fields, and this means that enlargementof the sella is necessary for the diagnosis of achromophobe adenoma in almost every case'However there are a few cases of chromophobeadenoma which grow above the diaphragma sellaewithout enlarging the sella, presumably becausethey arise from chromophobe cells in the stalk ofthe hypophysis.The accessory methods of diagnosis are not
often of much help. The cerebrospinal fluid isnormal as to pressure and content unless there is aconsiderable extrasellar extension, in which casethe pressure and the protein content may be in-creased, e.g. to 90-IOO mgm. Ventriculographyshows no significant abnormality unless thegrowth has extended to involve the third ventricleand produce ventricular dilatation, or to invadethe temporal or frontal lobe and thus causecharacteristic deformities. Arteriography likewisereveals little abnormal in early cases, but if thereis a massive tumour with extrasellar extension;
Protected by copyright.
on Novem
ber 2, 2020 by guest.http://pm
j.bmj.com
/P
ostgrad Med J: first published as 10.1136/pgm
j.26.293.141 on 1 March 1950. D
ownloaded from

146 POSTGRADUATE MEDICAL JOURNAL March I950
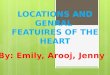
FIG. 7.-Arteriogram of supraseller meningioma. Note abnormal vascular pattern above tuberculum sellae.
there may be characteristic displacements of theterminal portions of the internal carotid and thebeginning of the anterior cerebral arteries (Fig. 5).These accessory diagnostic procedures have a
very important role in differential diagnosis.Thius. an intracranial aneurysm, e.g. on the anteriorcommunicating or anterior cerebral artery, cancause bitemporal hemianopia (Fig. 6). This lesionusually is associated with a good deal of frontalpain or headache, more than is common withadenomas, endocrine disturbances are slight, andthe sella is usually not enlarged. But the diagnosiscan only be made with certainty before operationby demonstrating the aneurysm by arteriography.A more common cause of bitemporal hemianopiais a suprasellar meningioma. This tumour arisesfrom the tuberculum sellae, in front of the chiasmand between the two optic nerves. It growsslowly and may produce a bitemporal or altitudinalhemianopia and even serious reduction of visionbefore there are any other symptoms and signs,such as those of increased intracranial pressure.There are usually no significant endocrine defects.X-rays show the sella to be of normal size, andindeed the whole skull appears to be normalunless, as is sometimes the case, a hyperostosis canbe seen at the site of the tumour attachment tothe tumberculum sella. The cerebrospinal fluidpressure is normal, but the fluid commonly con-tains an excess of protein as the tumour is closelyrelated to the large subarachnoid space in thewicinity of the optic chiasm. The ventriculogram
may show little abnormality unless the tumour hasattained a sufficient size to displace the frontalhorns of the ventricle. An arteriogram, however,may reveal the characteristic vascular pattern ofthe tumour before it is large enough to produoeany major displacement of the anterior cerebral oarother arteries at the base of the brain (Fig. 7).!A much more rare cause of chiasmal com-
pression is the suprasellar cholesteatoma or pearlytumour. There is only one example of this tumourin our series, and judging from it the diagnosis maydepend almost entirely on exclusion. In this casethere was a bitemporal field defect without head-ache or any endocrine disturbance, normal X-rays,normal cerebrospinal fluid and normal ventriculo-gram.More common than any of these diagnostic
problems is that of distinguishing a pitiuitaryadenoma from a craniopharyngioma or tumour bfRathke's pouch. The clinical features of thistumour will be described later; suffice it to saynow that it is often impossible to make thedifferentiation, even at operation, until the tumourhas been examined histologically.
Chromophil Adenomas. These tumours declarethemselves by producing acromegaly, which riybe their only manifestation. Accordingly many ofthem, the majority indeed, are never verified atoperation; but the invariable association of acro-megaly with a chromophil adenoma has been toowell documented by autopsy records to admit ofany doubt. As noted they are less common than
Protected by copyright.
on Novem
ber 2, 2020 by guest.http://pm
j.bmj.com
/P
ostgrad Med J: first published as 10.1136/pgm
j.26.293.141 on 1 March 1950. D
ownloaded from

M,qrch 1950 PENNYBACKER: Pituitary, Pineal and ThirdVentricle Tumours '4
chromophobe adenomas in hospital practice,possibly because they do not so constantly affectvision. It is also remarkable how stealthily acro-megaly may manifest itself; within the familycircle or in a small community the change in thepatients appearance is so gradual that it mayalmost be unnoticed.The physical features are well known, and it is
usually the facies rather than the appearance ofthe extremities which is so striking (Fig. 8). En-largement and prominence of the frontal sinusescauses an overhanging brow, the nose is enlargedand the lower jaw juts forward so that the lowerteeth rest in front of the upper ones in biting.Enlargement of the mandible gives rise to widespacing of the teeth which, against the large back-ground of the jaw and tongue, appear to be smallerthan normal. The tongue is broad and thick anddeeply furrowed. The scalp likewise is thick andfurrowed and the hair is coarse and wiry. Theaffection derives its name from the enlargement ofthe extremities, and there is usually enlargement ofthe hands and feet so that a woman finds that herrings are having to be expanded and larger sizes ingloves and shoes worn. The soft tissues alter sothat the hand feels like a cushion, and it has beensaid that this feeling is characteristic enough toenable a physician to recognize an acromegalic byshaking hands with him in the dark. The trunkand limbs are generally somewhat massive withcoarse, hairy skin. There is often a considerablethoracic kyphosis which gives rise to a deepthoracic cage and may account for some loss ofbodily height. The voice becomes deep andsomewhat thick because of enlargement of the airsinuses, tongue and vocal cords.
This descriptiQn of course applies to well-narked cases. There are many others in whichonly a few features will be obvious, and some inwhich the changes are slight enough to give rise tothe term ' fugitive acromegaly.' In the definitecases there is almost always enlargement of thesella turcica as seen in skiagrams, indicating ex-pansion by a tumour (Fig. 9). It is a remarkablefact, however, that the tumour does not often ex-pand sufficiently to compress the optic chiasm andendanger eyesight; only three of 49 cases requiredoperation for preservation of vision whereas xvithchromophobe adenomas necessity for operation isthe rule. It is also a fact that acromegaly can pro-gress up to a point slowly over many years and thenseemingly become arrested.
If the tumour begins in adolescence before theepiphyses of the long bones have united, the bonescontinue to lengthen and gigantism results. Theacromegalic giant is familiar in medical literature,but on the whole marked degrees of gigantism arerare. An incongruous feature is that the giants
are often physical weaklings, and this applies tosome extent to acromegalics in general; theirmassive build and features give an appearance ofgreat physical strength which is not borne out bytrial. Indeed the patient often comes to his doctorcomplaining of weakness and fatigue. In somethere may be diabetes mellitus, . not infrequentaccompaniment of acromegaly. It has been saidthat diabetes is the commonest cause of death inacromegaly but this has not been the case in ourexperience; we have had more with severe degreesof arterial hypertension than with diabetes, and itmay be the headache due to high blood pressurewhich brings the patient to his doctor.
Another type of headache, not associated withhypertension, is a common and sometimes a verydistressing symptom. It is often described as atight or bursting feeling between the temples, andmay be continuous for weeks or months with littlevariation and may be associated with somelachrymation. It is clearly not due to increasedintracranial pressure as there is no papilloedema
6r
FIG. --5rmegI-
Protected by copyright.
on Novem
ber 2, 2020 by guest.http://pm
j.bmj.com
/P
ostgrad Med J: first published as 10.1136/pgm
j.26.293.141 on 1 March 1950. D
ownloaded from

148 POSTGRADUATE MEDICAL JOURNAL March 1950
... ............. ...S...
Aj:J
...~~~.. 0-....... . .........
FIG. 9.-The skull in acromegaly. Note large frontal sinuses, enlarged sella,malocclusion of teeth, and prominent lower jaw.
and no increase in the cerebrospinal fluid pressure,nor is it at all relieved by decompressing opera-tions. It has been ascribed to increased pressurewithin the sella itself, but it is a matter in which it isvery difficult to determine causes. It is a fact,however, that this headache may eventually clearup spontaneously, and that it usually respondssatisfactorily to X-ray therapy.Acromegaly is usually accompanied by de-
pression or abolition of sexual function althoughthis feature is not as constant as in the chromo-phobe adenomas. In females galactorrhoea iscommon, and the disease may manifest itself aftera pregnancy. Enlargement of the thyroid some-times occurs and a large goitre may cause con-siderable respiratory embarrassment.Thus the symptoms of a chromophil adenoma
are similar to those of the chromophobe tumour,the differences being that in acromegaly the skeletaland somatic changes are more marked, headacheis, more common and serious visual disturbancesare less common. There are, of course, manycases in which some features of both types of
tumour are manifest, i.e. the patient with most ofthe features of a chromophobe adenoma who hasacromegalic hands and feet, and histologically itmay be difficult to classify such ' mixed tumours'as either chromophobe or chromophil.As to the clinical course of these tumours the
chromophobe adenoma usually progresses steadily,unless it is treated, to cause blindness and laterdeath by developing a large extrasellar extension,e.g. in the third ventricle. This may take severalyears, or a much shorter time depending on howrapidly the tumour grows. The untreated chromo-phil adenoma on the other hand carries a longerexpectation of life, and many patients with acro-megaly beginning in early adult life live to the fifthand sixth decades. As noted above, the acro-megalic may die from hypertension or diabetes,and those cases in which asthenia is a niarkedfeature succumb to relatively mild infections.
Treatment. For the chromophobe adenomataoperation is usually called for to preserve vision.It should be stressed that removal of a pituitarytumour can hold out little hope of improving the
Protected by copyright.
on Novem
ber 2, 2020 by guest.http://pm
j.bmj.com
/P
ostgrad Med J: first published as 10.1136/pgm
j.26.293.141 on 1 March 1950. D
ownloaded from

March 1950 PENNYBACKER: Pituitary, Pineal and Third Ventricle Tumours 149
FIG. IO. Rathke Pouch Tumour. Note calcification in lower part and cyst filling third ventricle.
endocrine symptoms, e.g. sterility, asthenia and thelike. Although the patient often expresses someimprovement in general well-being, it is difficultto say how much of this is referable to improve-ment or restoration of vision. As to the time tooperate, the indication generally is evidence of aprogressive field defect, even before central visionis affected. Within limits, operation offers thebest chances in early cases with incomplete fielddefects and no loss of central vision; in such thefields may return to normal after operation.Further, the more acute and recent the loss, eitherof fields or acuity of vision, the better chance thereis of restoration by operation. Thus in one caseunder observation with a slight bitemporal defectthere was a rapid loss of vision in both eyes withina few days to almost complete blindness. Opera-tion undertaken as an emergency disclosed a cyst inthe tumour, evacuation of which restored centralvision at once and within two weeks the fields werevirtually full again. On the other hand, long-standing cases of bitemporal hemianopia, withperhaps considerable loss of acuity in one eye,often do not improve much after operation, butthe operation should prevent further deteriorationwhich would otherwise be inevitable.The operation commonly practised nowadays
entails an osteoplastic craniotomy in the frontal
region. The frontal lobe is elevated from theanterior fossa to expose the optic nerve and chiasm,and the tumour usually presents as a smoothpurple or pinkish dome between the two opticnerves and in front of the chiasm. These tumoursare often cystic and a needle is inserted for a trialaspiration. The capsule is then incised and theinterior of the tumour is removed by suction,special biting forceps and curettage. The tumourtissue is usually soft and is easily dealt with bythese means. The collapsed capsule is then gentlydislodged from the optic nerves and chiasm and asmuch as possible is excised. Bleeding from theraw interior of the tumour is often troublesome butit can usually be checked by firm pressure withcotton wool pledgets, or by the application of fibrinfoam or similar haemostatic agents. As soon as thecavity is dry, the bone flap is replaced and suturedin position and the scalp incision is closed with adouble layer of interrupted stitches.
It will be seen from this brief description thatthe tumour is not completely removed. To do sowould often entail total removal of all the activepituitary gland, and would produce a state of pro-found pituitary cachexia as in a hypophysectom-ized animal. In humans this state may be fatal,so it is just as important not to remove too much asto remove sufficient to provide freedom for the
Protected by copyright.
on Novem
ber 2, 2020 by guest.http://pm
j.bmj.com
/P
ostgrad Med J: first published as 10.1136/pgm
j.26.293.141 on 1 March 1950. D
ownloaded from

150 POSTGRADUATE MEDICAL JOURNAL March I950
::.::::..
FIG. i 2. Colloid Cyst of Third Ventricle. The roofof the third ventricle has been removed to show thecyst impacted in the foramen of Monro.
optic nerves and chiasm, which is the primary pur-pose of the operation. As some neoplastic tissue isleft, recurrence of visual symptoms may be ex-pected, but a satisfactory operation may providereliet for iO or I2 years or even longer. There is aconsiderable body of evidence that recurrence maybe delayed by X-ray treatment directed to thesella after operation, and this is now the rule inmany surgical clinics. We think it unwise toiirradiate these tumours before operation, becauseoccasionally the radiation causes the tumour toswell during the course of treatment and fuitherdamage may be done to the visual pathway. Thuswe have seen a case of acromegaly without anyfield defect develop a complete bitemporal hemi-anopia while undergoing radiation treatment forthe type of headache mentioned above.
'The same type of operation is employed inacromegaly when there is evidence of progressivechiasmal compression endangering eyesight, butas already mentioned, this is rare. The operationis more tedious because of the altered architectureof the skull, and some surgeons prefer the trans-sphenoidal approach. For this an incision is madein the mucous membrane of the upper gum be-neath the nose and a submucous resection of theseptum carried back to the sphenoidal sinus. Insome cases of large tumours of both types, thefloor of the sella is eroded so that the tumourpresents in the sinus and can be excavated muchas from above by the transfrontal approach. 'Inothers the thin bony'floor of the sella has to be re-
moved to expose the tumour. This operation issaid to be safer in cases of very large tumours inwhich little vision remains, because of the vul-nerability of the greatly stretched and flattenedoptic nerves to even gentle manipulations when thetumour is approached from above.The endocrine deficiencies are generally not
benefited by operation. Indeed, as mentionedabove, they may be more marked after an extensiveoperation. For them some form of substitutiontreatment is worth trying but the results are rarelydramatic. Anterior pituitary hormones sometimeshelp, and testosterone given by mouth or im-plantation sometimes restores sexual activity inmales and increases general well-being andphysical strength.
Rathke Pouch TumoursThese tumours, also spoken of as cranio-
pharyngiomas, adamantinoma and cranio-buccalcysts develop from a remnant of the foetal cranio-buccal pouch. This is an outgrowth from theprimitive stomodaeum which fuses with a down-ward evagination from the forebrain. From thelatter the infundibulum and the pars posterior ofthe pituitary gland develop, while the buccal out-growth becomes sealed off from the enteric canaland is responsible for the pars anterior and parsintermedia of the pituitary. A part of the buccalpouch may be isolated during development andlater begin to develop a cyst, or to show neoplasticproperties. These lesions are usually cyatic,develop anterior to the pituitary gland and arecommonly above the diaphragma sella;: thus theyare often called suprasellar cysts. The anatomicaland physiological effects of such a tumour are thusvery similar to those produced by pituitaryadenomata, but there are important differences.
Being the result of developmental abnormalities,it is not surprising that the majority of them causesymptoms in early childhood or adolescence,although they may manifest themselves, at anyage and we have had patients over 6o years of agewith recent symptoms of such tumours. The localor anatomical effects are generally one of twotypes:- (i) The tumour may grow in such a waythat it compresses the chiasm and later one or bothoptic nerves to cause bitemporal hemianopia, uni-lateral or bilateral blindness, with primary opticatrophy. In this group the ophthalmic picture isin no way different from that produced by pituitaryadenomas. (2) Or the tumour may grow straightupward to fill the third ventricle from below,without directly affecting the visual pathway (Fig.io). In this group the clinical picture is one ofincreased intracranial pressure which results fromobstruction of the foramen of Monro and theaqueduct of Sylvius. There is severe headache,
Protected by copyright.
on Novem
ber 2, 2020 by guest.http://pm
j.bmj.com
/P
ostgrad Med J: first published as 10.1136/pgm
j.26.293.141 on 1 March 1950. D
ownloaded from

March 1950 PENNYBACKER: Pituitary, Pineal and Third Ventricle Tumours I51I
iSoi
FIG. 13.Ventriculogram of colloid cyst of third ventricle. Note spherical filling defect below and behind foramenof Monro.
vomiting, papilloedema and later secondary opticatrophy, and these tumours cause death from in-creased intracranial pressure much as with anyother tumour of the third ventricle.The endocrine effects seem to bear no relation
to the anatomical disposition of the tumour; inboth types there is usually marked hypopituitar-ism. In childhood there is often some degree ofgraceful dwarfism, and the Lorain type is charac-teristic. Sexual development is delayed and im-perfect. In later adult life there is often a smooth,hairless skin on the trunk and limbs, silky hair onthe head and amenorrhoea and impotence as seenin pituitary adenomas.The X-ray appearances may be characteristic.
The sella is often not significantly enlarged, but inthe majority of cases some calcification is apparentin the vicinity of the sella. This appearance isalmost pathognomonic (Fig. ii). If the cyst hasgrown up into the third ventricle there may alsobe appearances due to increased intracranialpressure, namely convolutional thinning of thevault of the skull and, in children, separation of thesutures.
It will be seen that the diagnosis may be easy ifa hypopituitary child or adult; presents with abitemporal field defect and radiological evidence ofcalcification in the sellar region. But there aresome cases of adults with a chiasmaI syndrome andno clear radiological abnormalities; in such theabsence of enlargement of the sella is unlike apituitary adenoma, and the hypopituitarism is un-
like a suprasellar meningioma, but in some of thesethe pathological diagnosis can only be made atoperation.Treatment. It must be admitted that these
tumours are generally not very favourable forsurgical treatment. Those that involve the chiasmare often so adherent to neighbouring structuresthat they cannot be removed completely, and thisis even more true of those growing up into thethird ventricle. As mentioned, they are oftencystic and the operation usually amounts toemptying the cyst and removing as much of itswall as possible, though in a few cases it is possibleto remove the whole tumour successfully. For thecases presenting with chiasmal symptoms, thisentails much the same sort of operation as forpituitary adenomas, i.e. by elevation of the frontallobe, and if an extensive removal can be carriedout there may be a period of relief for several yearsbut recurrence is the rule. Simple aspiration ofthecyst is rarely effective for longer than a few weeks.
For the tumours causing obstruction in thethird ventricle there are two types of operation. Inthe first, the tumour is exposed by excising awindow of the frontal lobe to open into the anteriorhorn of the ventricle (Fig. 14). The tumour canthen be seen impacted in the foramen of Monro.More room can then be obtained if the thirdventricle is opened by cutting the anterior pillarof the fornix, as well as by aspirating the cyst. Itis then often possible to remove a large part of thecyst wall, but attempts to remove the solid part of
Protected by copyright.
on Novem
ber 2, 2020 by guest.http://pm
j.bmj.com
/P
ostgrad Med J: first published as 10.1136/pgm
j.26.293.141 on 1 March 1950. D
ownloaded from

152 POSTGRADUATE MEDICAL JOURNAL Mar
....... ...
.... ...
..i::i j
Z
....
..... ....
iAi !i .i 03
u :uRi 14-
'Vek-Shor6i
FIG. 14.-Transventricular removal of colloid cyst in third ventricle.
the tumour in the floor of the third ventricle areusually unsuccessful and carry a high mortalityfrom a profound hypothalamic disturbance in theimmediate postoperative period.More recently attempts have been made to deal
with this type of tumour by ventriculocisternos-tomy, an ingenious procedure devised by Torkild-sen. In this operation a rubber or polythene tubeis passed from the lateral ventricle to the cisternamagna so that the cerebrospinal fluid does not haveto traverse the third ventricle, aqueduct and fourthventricle. This procedure will deal with theproblem of increased intracranial pressure, but itmay not relieve the local effects of pressureexerted on the third ventricle by the cyst. Inother words headache and vomiting may cease andpapilloedema subside, and yet the patient remainsdrowsy, apathetic and in a state of lowered vitality.In some cases, however, the effect is strikinglybeneficial and on the whole this procedure seems
to hold out more promise than attempts at radicaltransvntricular removal.
Because of the unsatisfactory results of opera-tion in Rathke pouch tumours, there have beenmany attempts to deal with them by X-ray therapy,but in our series we have no good evidence thatthey are radio-sensitive.
Third Ventricle TumoursThe commonest type of third ventricle tumour
is a glioma growing from one of its walls, e.g. theoptic thalamus. Much rarer are the benigntumours arising from the blood vessels, meningesand ependyma. Thus angioma, meningioma andependymoma have all been encountered, butcommoner than any of them is what is known as acolloid cyst. This is a spherical cyst containingmucoid viscous fluid which develops from and isadherent to the inferior surface of the roof of thethird ventricle just behind the foramen of Monro.
Protected by copyright.
on Novem
ber 2, 2020 by guest.http://pm
j.bmj.com
/P
ostgrad Med J: first published as 10.1136/pgm
j.26.293.141 on 1 March 1950. D
ownloaded from

March 1950 PENNYBACKER: Pituitary, Pineal and Third Ventricle Tumours 153
T-L-
FIG.5-Vetiuormo piea tmu.Note rone filn deeti.otr-upro atohr vetil.-
It may attain a size of 2 to 3 cm. in diameter and itplugs up both foramina and causes hydrocephalusmuch as does a Rathke pouch cyst (Fig. I2).Third ventricle tumours cause symptoms of in-
creased intracranial pressure and there may belittle or nothing in the way of focal neurologicalabnormalities. Because of their situation theymay occasionally act like a ball-valve and produceparoxysmal headache, vomiting and stupor, butthis is by no means characteristic. There areoccasionally symptoms of hypothalamic disorders,e.g. somnolence, obesity, abnormalities of watermetabolism, but these too may occur as indirecteffects of a lesion elsewhere, e.g. in the fourthventricle and are rarely diagnostic.The diagnosis of a third ventricle tumour rests
in ventriculography, and the appearances aregenerally unmistakable (Fig. 13). The gliomascannot be removed and treatment usually consistsof a ventriculocisternostomy (v.s.) followed byX-ray therapy. The intrinsic tumours call for anexploration and this is usually done by the trans-ventricular route described above (Fig. 14). Many
of them can be completely removed with full re-covery. Those which cannot be removed shouldhave a ventriculocisternostomy and radiation sub-sequently if necessary, e.g. in extensive angiomas.
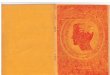
Pineal TumoursTumours of the pineal gland (Fig. i6) are rare,
but they produce effects which may be indis-tinguishable from other tumours in the immediatevicinity, i.e. in the postero-superior part of thethird ventricle and the upper part of the brainstem. The mechanical effect of such tumours is toproduce hydrocephalus from obstruction to thecirculation of the cerebrospinal fluid in the pos-terior part of the third ventricle and aqueduct ofSylvius. Thus, there is usually headache, vomit-ing, stupor and papilloedema. The neurologicalabnormalities are often limited to the oculo-motor mechanism and are characterized by de-fective upward movement of the eyeballs andimmobility of the pupils to stimulation by light,with preservation of the reaction on accommoda-tion and convergence. There is often a degree of
Protected by copyright.
on Novem
ber 2, 2020 by guest.http://pm
j.bmj.com
/P
ostgrad Med J: first published as 10.1136/pgm
j.26.293.141 on 1 March 1950. D
ownloaded from

154 POSTGRADUATE MEDICAL JOURNAL March 1950
....
.. ......................~~~... .....:... ...... :.:::::!:..... :.:::ii,,°'
... .... .. ...
,..........i.
F :4
:. ..
FIG. I6. Pineal tumour.
bilateral ptosis and there may be a disorder ofconjugate lateral movement of the eyeballs akin toskew deviation in which the abducting eye looks out-ward and downward while the adducting eye looksinward and upward with corresponding diplopia.
In some cases of pineal tumour in boys, there ismarked sexual precocity. The more commonendocrine effect in males and females is mildhypopituitarism which results from the pressureof a dilated third ventricle on the pituitary gland,a common effect in hydrocephalus due to what-ever cause.The diagnosis of a pineal tumour can sometimes
be inferred from the clinical evidence but con-firmation depends on ventriculography (Fig. I5).E'ven so it may be impossible to say whether thecharacteristic filling defect in the postero-superiorpart of the third ventricle is due to a pineal tumouror to a tumour arising from neighbouring struc-tures. Attempts at removal carry a high mortality
or produce a permanent homonymous hemianopia,and the tendency nowadays is to deal with thehydrocephalus by a short-circuiting proceduresuch as a ventriculo-cisternostomv or the anteriorventriculostomy described by Stookey and Scarff(in which the anterior wall of the third ventricle,the lamina terminalis, is incised, thus allowing thecerebrospinal fluid to escape from the anterior endof the third ventricle into the subarachnoid spacewithout having to traverse the posterior end,aqueduct and fourth ventricle), and to administerradiation treatment afterwards. These measuresare often highly successful and we have such caseswhich have remained free from symptoms forperiods up to 14 years. Although not verifiedhistologically, the clinical and ventriculographicevidence left little doubt that there was a tumourin the pineal region, and the response suggests thattheseI may be among the most radio-sensitivetumours in the bodv.
Protected by copyright.
on Novem
ber 2, 2020 by guest.http://pm
j.bmj.com
/P
ostgrad Med J: first published as 10.1136/pgm
j.26.293.141 on 1 March 1950. D
ownloaded from