Physiology of Thyroid Gland. The thyroid gland, located below the larynx on each side of and...
62
Physiology of Thyroid Gland
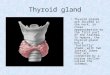
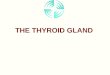
Physiology of Thyroid Gland. The thyroid gland, located below the larynx on each side of and anterior to the trachea, is one of the largest of the endocrine
The thyroid gland, located below the larynx on each side of and
anterior to the trachea, is one of the largest of the endocrine
glands.
Slide 3
The thyroid gland contains numerous follicles, composed of
epithelial follicle cells and colloid. The major constituent of
colloid is the large glycoprotein thyroglobulin, which contains the
thyroid hormones within its molecule. Also, between follicles are
clear parafollicular cells, which produce calcitonin Histology of
the Thyroid Gland
Slide 4
O OH I I I I O NH 2 Thyroxine (T 4 ) O OH I I I O NH 2
3,5,3-Triiodothyronine (T 3 ) THYROID HORMONES Tyrosine There are
two biologically active thyroid hormones: - tetraiodothyronine (T4;
usually called thyroxine) - triiodothyronine (T3) Derived from
modification of an amino acid (tyrosine)
Slide 5
The thyroid secretes about 80 micrograms of T4, but only 5
micrograms of T3 per day. However, T3 has a much greater biological
activity (about 10X) than T4. An additional 25 micrograms/day of T3
is produced by peripheral monodeiodination of T4. T4 thyroid I-I-
T3 Differences between T4 and T3
Slide 6
Thyroid hormones are unique biological molecules in that they
incorporate iodine in their structure. Thus, adequate iodine intake
(diet, water) is required for normal thyroid hormone production.
Major sources of iodine: - iodized salt - iodated bread - dairy
products Minimum requirement: 75 micrograms/day Why is Iodine
Important in Thyroid Hormone Production?
Slide 7
Dietary iodine is absorbed in the GI tract, then taken up by
the thyroid gland (or removed from the body by the kidneys). The
basal membrane of the thyroid cell has the specific ability to pump
the iodide actively to the interior of the cell. This is called
iodide trapping. The transport of iodide into follicular cells is
dependent upon a sodium/iodine cotransport system. Iodide taken up
by the thyroid gland is oxidized by peroxide in the lumen of the
follicle (via pendrin receptor): Thyroid peroxidase I - I +
Oxidized iodine ( I + ) can then be used in production of thyroid
hormones. Iodine Metabolism
Slide 8
The follicle cells of the thyroid produce thyroglobulin.
Thyroglobulin is a very large glycoprotein. Thyroglobulin is
released into the colloid space (via pendrin receptor), where its
tyrosine residues are iodinated by I +. (organification) This
results in monoiodotyrosine (MIT) or diiodotyrosine (DIT).
Production of thyroglobulin
Slide 9
Ion transport by the thyroid follicular cell I-I- I-I-
organification Propylthiouracil (PTU) blocks iodination of
thyroglobulin COLLOID BLOOD NaI symporter (NIS) Thyroid peroxidase
(TPO) PTU, a thioamide drug used to treat hyperthyroidism
Slide 10
follicle cell extracellular space colloid space I-I- I-I-
thyroglobulin with monoiodotyrosines and diiodotyrosines iodination
thyroglobulin gene I+I+ oxidation I-I- Na+ K+ Initial Steps in
Thyroid Hormone Synthesis Pendrin
Slide 11
The iodinated tyrosine residues on thyroglobulin are modified
and joined to form T3 and T4, still attached to the thyroglobulin
molecule. Second step: Production of Thyroid Hormones from
Iodinated Thyroglobulin
Slide 12
In order to secrete T3/T4, the thyroglobulin in the colloid
space is internalized by endocytosis via megalin receptor back into
the follicle cell. (receptor mediated endocytosis) This
internalized vesicle joins with a lysosome, whose enzymes cause
cleavage of T3 and T4 from thyroglobulin. Utilization of
Thyroglobulin to Secrete Thyroid Hormones
Slide 13
follicle cell colloid space Endocytosis (via megalin)
thyroglobulin T3 T4 colloid droplet lysosome T3/T4 (deiodinated,
recycled) extracellular space (T4 T3) T3 and T4 are then released
into the extracellular space by diffusion. Only minute amounts of
thyroglobulin are released into the circulation.
Slide 14
Thyroid hormones are not very soluble in water (but are lipid
soluble). Thus, they are found in the circulation associated with
binding proteins: - Thyroid Hormone-Binding Globulin (~70% of
hormone) - Pre-albumin (transthyretin), (~15%) - Albumin (~15%)
Less than 1% of thyroid hormone is found free in the circulation.
Only free and albumin-bound thyroid hormone is biologically
available to tissues. Transport of Thyroid Hormones
Slide 15
T3 has much greater biological activity than T4. A large amount
of T4 (25%) is converted to T3 in peripheral tissues. This
conversion takes place mainly in the liver and kidneys. The T3
formed is then released to the blood stream. In addition to T3, an
equal amount of reverse T3 may also be formed. This has no
biological activity. Conversion of T4 to T3
Slide 16
In addition to T3, an equal amount of reverse T3 may also be
formed. This has no biological activity.
Slide 17
Three deiodinases (D1, D2 & D3) catalyze the generation
and/disposal of bioactive thyroid hormone. D1 & D2 bioactivate
thyroid hormone by removing a single outer-ring iodine atom. D3
inactivates thyroid hormone by removing a single inner-ringiodine
atom. All family members contain the novel amino acid
selenocysteine (Se-Cys) in their catalytic center. Thyroid hormone
deiodinases: THYROID HORMONE METABOLISM
Slide 18
Slide 19
The thyroid gland is capable of storing many weeks worth of
thyroid hormone (coupled to thyroglobulin). If no iodine is
available for this period, thyroid hormone secretion will be
maintained. One Major Advantage of this System
Slide 20
Thyroid hormone synthesis and secretion is regulated by two
main mechanisms: - an autoregulation mechanism, which reflects the
available levels of iodine - regulation by the hypothalamus and
anterior pituitary Regulation of Thyroid Hormone Levels
Slide 21
The rate of iodine uptake and incorporation into thyroglobulin
is influenced by the amount of iodide available: - low iodide
levels increase iodine transport into follicular cells - high
iodide levels decrease iodine transport into follicular cells Thus,
there is negative feedback regulation of iodide transport by
iodide. Autoregulation of Thyroid Hormone Production
Slide 22
T3 & T4 Control Pathways Feedback regulation the
hypothalamic-pituitary-thyroid axis Key players for the thyroid
include: TRH TSH T3, T4
Slide 23
TSH acts on follicular cells of the thyroid. TSH binds to
specific cell surface receptors that stimulate adenylate cyclase to
produce cAMP. - increases iodide transport into follicular cells -
increases production and iodination of thyroglobulin - increases
endocytosis of colloid from lumen into follicular cells Na+ I-I-
thyroglobulinfollicle cell gene I-I- endocytosis thyroglobulin T3
T4 colloid droplet I-I- I+I+ iodination thyroglobulin Na+ K+ ATP
Action of TSH on the Thyroid 1 2 3
Slide 24
Mechanism of Action of T3 T3/T4 acts through the thyroid
hormone receptor - intracellular, in steroid receptor superfamily -
acts as a transcription factor - receptor binds to TRE on 5
flanking region of genes as homodimers and/or heterodimers. -
multiple forms (alphas and betas) exist - one form (alpha-2) is an
antagonist at the TRE hypervariable
Slide 25
Expression and Regulation of Thyroid Hormone Receptors Thyroid
hormone receptors are found in many tissues of the body, but not in
adult brain, spleen, testes, uterus, and thyroid gland itself.
Thyroid hormone inhibits thyroid hormone receptor expression (TRE
on THR genes).
Slide 26
One Major Target Gene of T3: The Na + /K + ATPase Pump Pumps
sodium and potassium across cell membranes to maintain resting
membrane potential Activity of the Na + /K + pump uses up energy,
in the form of ATP About 1/3rd of all ATP in the body is used by
the Na + /K + ATPase T3 increases the synthesis of Na + /K + pumps,
markedly increasing ATP consumption. T3 also acts on mitochondria
to increase ATP synthesis The resulting increased metabolic rate
increases thermogenesis (heat production).
Slide 27
Thyroid hormones: Key Points Held in storage Bound to
mitochondria, thereby increasing ATP production Bound to receptors
activating genes that control energy utilization Exert a
calorigenic effect
Slide 28
Required for GH and prolactin production & secretion
Required for GH action Increases intestinal glucose reabsorption
(glucose transporter) Increases mitochondrial oxidative
phosphorylation (ATP production) Increases activity of adrenal
medulla (sympathetic; glucose production) Induces enzyme synthesis
Result: stimulation of growth of tissues and increased metabolic
rate. Actions of Thyroid Hormones
Slide 29
Thyroid hormones are essential for normal growth of tissues,
including the nervous system. Lack of thyroid hormone during
development results in short stature and mental deficits
(cretinism). Thyroid hormone stimulates basal metabolic rate. What
are the specific actions of thyroid hormone on body systems?
Actions of Thyroid Hormones
Slide 30
Thyroid Hormone Actions which Increase Oxygen Consumption
Increase mitochondrial size, number and key enzymes Increase plasma
membrane Na-K ATPase activity Increase futile thermogenic energy
cycles Decrease superoxide dismutase activity
Slide 31
Stimulation of Carbohydrate Metabolism by Thyroid hormone
Stimulates all of carbohydrate metabolism: including rapid uptake
of glucose by the cells, increased glycolysis, increased
gluconeogenesis, increased rate of absorption from the
gastrointestinal tract, increased insulin secretion with its
resultant secondary effects on carbohydrate metabolism. All these
effects probably result from the overall increase in cellular
metabolic enzymes caused by thyroid hormone.
Slide 32
Stimulation of Fat Metabolism Lipids are mobilized rapidly from
the fat tissue, which decreases the fat stores and increases the
free fatty acid levels in the plasma. Increased thyroid hormone
decreases the levels of cholesterol, phospholipids, and
triglycerides in the plasma, and increases the free fatty acids.
But, decreased thyroid secretion greatly increases the plasma
levels of cholesterol, phospholipids, and triglycerides. TH
decreases the plasma cholesterol concentration through increase the
rate of cholesterol secretion in the bile and consequent loss in
the feces.
Slide 33
Increased Basal Metabolic Rate Because thyroid hormone
increases metabolism in almost all cells of the body, excessive
quantities of the hormone can increase the basal metabolic rate
Conversely, when no thyroid hormone is produced, the basal
metabolic rate falls.
Slide 34
Effects of Thyroid Hormones on the Cardiovascular System
Increased metabolism in the tissues causes more rapid utilization
of oxygen than normal and release of greater than normal quantities
of metabolic end products from the tissues. So, the increased blood
flow leads to increased cardiac output and, Increase heart rate
Increase force of cardiac contractions Increase stroke volume
Up-regulate catecholamine receptors
Slide 35
Slide 36
Effects of Thyroid Hormones on the Respiratory System Increase
resting respiratory rate Increase minute ventilation Increase
ventilatory response to hypercapnia and hypoxia
Slide 37
Effects of Thyroid Hormones on the Renal System Increase blood
flow Increase glomerular filtration rate
Slide 38
Thyroid hormones affect renal function by both pre-renal and
direct renal effects. 1. Pre-renal effects are mediated by the
influence of thyroid hormones on the cardiovascular system and the
renal blood flow (RBF). 2. The direct renal effects are mediated by
the effect of thyroid hormones on glomerular filtration rate (GFR),
tubular secretory and re-absorptive processes, as well as the
hormonal influences on renal tubular physiology. Thyroid hormones
influence Na reabsorption at the PCT primarily by increasing the
activity of the Na/K ATPase and tubular potassium permeability
Slide 39
Slide 40
Effects of Thyroid Hormones on Oxygen-Carrying Capacity
Increase RBC mass Increase oxygen dissociation from hemoglobin
Slide 41
Effects of Thyroid Hormones on Intermediary Metabolism Increase
glucose absorption from the GI tract Increase carbohydrate, lipid
and protein turnover Down-regulate insulin receptors Increase
substrate availability
Slide 42
Effects Thyroid Hormones in Growth and Tissue Development
Increase growth and maturation of bone Increase tooth development
and eruption Increase growth and maturation of epidermis,nhair
follicles and nails Increase rate and force of skeletal muscle
contraction Inhibits synthesis and increases degradation of
mucopolysaccharides in subcutaneous tissue
Slide 43
Effects of Thyroid Hormones on the Nervous System Enhances
wakefulness and alertness Enhances memory and learning capacity
Required for normal emotional tone Increase speed and amplitude of
peripheral nerve reflexes
Slide 44
TH in Intrauterin and infantil periods: Critical for normal CNS
neuronal development: Development of cerebral and cerebellar cortex
Proliferation of axons Branching of dendrite Synaptogenesis
Myelinization Migration of cells
Slide 45
Deficiency of TH in infant or intrauterin periods (Cretenism)
Mostly affected development of cerebral cortex, basal ganglia and
cochlea, so: Loss of hearing CNS exitation, motor activity,
learning capacity, memory, response to stimulus
Slide 46
Effects of Thyroid Hormones on the Reproductive System Required
for normal follicular development and ovulation in the female
Required for the normal maintenance of pregnancy Required for
normal spermatogenesis in the male
Slide 47
Slide 48
Diet: a high carbohydrate diet increases T3 levels, resulting
in increased metabolic rate (diet-induced thermogenesis). Low
carbohydrate diets decrease T3 levels, resulting in decreased
metabolic rate. Cold Stress: increases T3 levels in other animals,
but not in humans. Other Factors Regulating Thyroid Hormone
Levels
Slide 49
Early onset: delayed/incomplete physical and mental development
Later onset (youth): Impaired physical growth Adult onset
(myxedema) : gradual changes occur. Tiredness, lethargy, decreased
metabolic rate, slowing of mental function and motor activity, cold
intolerance, weight gain, goiter, hair loss, dry skin. Eventually
may result in coma. Many causes (insufficient iodine, lack of
thyroid gland, lack of hormone receptors, lack of TBG.) Thyroid
Hormone Deficiency: Hypothyroidism
Slide 50
During iodine deficiency, thyroid hormone production decreases.
This results in increased TSH release (less negative feedback). TSH
acts on thyroid, increasing blood flow, and stimulating follicular
cells and increasing colloid production. How is Hypothyroidism
Related to Goiter?
Slide 51
Emotional symptoms (nervousness, irritability), fatigue, heat
intolerance, elevated metabolic rate, weight loss, tachycardia,
goiter, muscle wasting, apparent bulging of eyes, may develop
congestive heart failure. Also due to many causes (excessive TSH
release, autoimmune disorders,) Thyroid Hormone Excess:
Hyperthyroidism
Slide 52
Graves' disease:A condition usually caused by excessive
production of thyroid hormone and characterized by an enlarged
thyroid gland, protrusion of the eyeballs, a rapid heartbeat, and
nervous excitability. Also called exophthalmic goiter.
Slide 53
Calcitonin Calcitonin is a 32-amino acid polypeptide hormone
that is produced in humans primarily by the parafollicular (also
known as C-cells) of the thyroid. It acts to reduce blood calcium
(Ca 2+ ), opposing the effects of parathyroid hormone(PTH).
Slide 54
Biosynthesis Calcitonin is formed by the proteolytic cleavage
of a larger prepropeptide, which is the product of the CALC1 gene
(CALCA). The CALC1 gene belongs to a superfamily of related protein
hormone precursors including islet amyloid precursor protein,
calcitonin gene-related peptide, and the precursor of
adrenomedullin. The calcitonin receptor, found primarily on
osteoclasts, is a G protein-coupled receptor, which is coupled by G
s to adenyl cyclase and thereby to the generation of cAMP in target
cells.
Slide 55
Physiology The hormone participates in calcium(Ca 2+ ) and
phosphorus metabolism. In many ways, calcitonin has the counter
effects of parathyroid hormone(PTH). To be specific, reduces blood
Ca 2+ levels in three ways: 1) Decreasing Ca 2+ absorption by the
intestines. 2) Decreasing osteoclast activity in bones. 3)
Decreasing Ca 2+ and phosphate reabsorption by the kidney
tubules.
Slide 56
Slide 57
These stimulate secretion of calcitonin: Increased plasma Ca
levels Feeding ( Gis hormones, especially gastrin) -adrenergic
agonist drugs Dopamine Estrogens
Slide 58
High levels of blood Ca (>11mg) When blood Ca levels are
high, Calcitonin is released. Causes bone deposit to occur Ca from
the blood is stored into bone. (Osteoblasts and Osteocytes are
working.) 99% of all Ca is found in bone.
Slide 59
Osteoclasts cause bone resorption Controlled by PTH Osteoblasts
cause bone deposit Controlled by calcitonin
Slide 60
Action 1) Bone mineral metabolism: - Prevent postprandial
hypercalcemia resulting from absorption of Ca 2+ from foods during
a meal - Promote mineralization of skeletal bone. - Protect against
Ca 2+ loss from skeleton during periods of Ca 2+ stress such as
pregnancy and lactation. - It have hypophostatemic effects:
*inhibits of bone resorption * stimulates of phosphate deposition
in bone * increases excretion of phosphate in tubules
Slide 61
2) Vitamin D regulation 3) A satiety hormone: - Inhibit food
intake in rats and monkeys - May have CNS action involving the
regulation of feeding and appetite.
Slide 62
In human, CT increases gastric acid and pepsin secretion and
decreases pancreatic amylase and pancreatic polypeptide. The kidney
is the principal site of CT degradation by neutral endopeptidase
(NEP). The effect of CT on the kidney is to stimulate diuresis and
increase the fractional excretion rate of sodium and chloride. In
addition, in urine a calcium and phosphate excretion
increases.