Embed Size (px)
Citation preview

PHYSICAL EXAMINATION OF THE KNEE

THE KNEE
• - is the largest joint in the body. • - it is a ginglymus joint, and as such provides a
fairly wide range of motion.• - the knee’s greatst range of motion is in
flexion.

INSPECTION• Starts when the patient walks into the
examination room, his gait should flow in a smooth, rhythmic motion.
• Ask the patient to remove his clothing from the waist down, watch carefully for any movement used to compensate for pain or stiffness in the knee.
• To inspect the anterior aspect of the knee have the patient stand strainght, with knee fully extended.


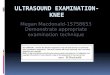
PALPATION• Have the patient sit on the edge of the examining
table. A bed patient should be in supine position with his knees flexed in 90 degree.
• Place your hand upon the knee joint so that your fingers curve around the posterior popliteal area.
• Place your thumbs on the anterior portion of the knee and press into the soft tissue depression on either side of the infrapatellar tendon. This depression will serve as the central point of orientation for palpating the lateral and the medial aspect of the knee.


BONY PALPATION • MEDIAL ASPECT• LATERAL ASPECT

BONY PALPATION OF THE MEDIAL ASPECT

MEDIAL ASPECT: Medial tibial plateau
• Push your thumb inferiorly into the soft tissue depression until you can feel the sharp upper edge of the medial tibial plateau.

MEDIAL ASPECT: Tibial tubercle
• Follow the infrapatellar tendon distally to where it inserts into the tibial tubercle

MEDIAL ASPECT: Medial femoral condyle
• As you move your thumb upward you will, palpate the medial femoral condyle

MEDIAL ASPECT: Adductor tubercle

BONY PALPATION OF THE LATERAL ASPECT

LATERAL ASPECT: Lateral Tibial Plateau
• Push down with your thump finger into the soft tissue depression until you feel the upper edge of the lateral tibial plateau

LATERAL ASPECT: Lateral Tubercle
• Is the large prominence of bone immediately below the lateral tibial plateau

LATERAL ASPECT: Lateral Femoral Condyle
• From the soft tissue depression, move upward and laterally onto the sharp edge of the lateral femoral condyle

• Lies lateral to lateral femoral condyle
LATERAL ASPECT:Lateral Femoral Epicondyle

LATERAL ASPECT: Head of the Fibula
• From the lateral femoral epicondyle, move your thumb inferiorly and posteriorly across the joint
• The head is the same level as the tibial tubercle

PALPATION:Trochlear Groove and Patella
• Place the thumb in the medial and lateral joint lines, move upward along the two femoral condyle to the hishest point of patella, then palpate towards the midline until you reach the depression.

The patella is fixed in the
groove during flexion and mobile in
extension. It is easier to push medially than
laterally.


SOFT TISSUE PALPATION
• Zone 1 – anterior aspect• - Quadriceps, Infrapatellar Tendon, Pes Anserine Bursa, Prepatellar Bursa,
Superficial Infrapatellar Bursa
• Zone II- medial aspect• - Medial Meniscus,Medial Collateral Ligament,Sartorius, Gracilis, semitendinosus
• Zone III- lateral aspect• - Lateral meniscus, Anterior Superior Tibiofibular Ligament, Common Peroneal
Nerve, Biceps Femoris Tendon, Iliotibial Tract, Lateral Collateral Ligament
• Zone IV- posterior aspect• - Popliteal Fossa- where we can also locate the Posterior Tibial Nerve, Popliteal
Vein, Popliteal Artery.

SOFT TISSUE PALPATION: Zone I Anterior aspect

Quadriceps

Infrapatellar Tendon
• often tender in patient with Osgood schlatter’s Syndrome.

Bursa • Superficial Infrapatellar Bursa- becomes inflamed as a result of excessive kneeling.
• Prepatellar Bursa- inflamed in combination of excessive kneeling and leaning forward (housemaids knee)
• Pes Anserine Bursa- when palpable indicates pathology

SOFT TISSUE PALPATION: Zone II medial aspect

Medial Meniscus
• tears are more common in this area


Medial Collateral Ligament
• frequenly in valgus stress injuries such as clipping injuries

Sartorius, Gracilis, semitendinosus muscle

SOFT TISSUE PALPATION: Zone III- lateral aspect

Lateral meniscus

Lateral Collateral Ligament

Biceps Femoris Tendon

Common Peroneal Nerve
• should be palpated carefully, injury can cause foot drop

SOFT TISSUE PALPATION: Zone IV- posterior aspect

Popliteal Fossa

TEST FOR JOINT STABILITYCollateral Ligaments

TEST FOR JOINT STABILITY Cruciate ligaments

RANGE OF MOTION
Four basic movement in the knee:• Flexion – performed by quadriceps• Extension- performed by hamstring muscle and
gravity• Internal rotation and External rotation –
performed by the reciprocal action of the semimembranosus, semitendinosus, gracilis, and Sartorius on the medial side, and biceps in the lateral side.

RANGE OF MOTION

Reflex testing: patellar reflex
• Have the patient sit on the edge of the examining table with his legs dangling freely. Then locate the tendon by palpating the soft tissue depression on either side of the infrapatellar tendon. Using a hammer tap the tendon at the level of the knee joint.

SPECIAL TESTS: McMurray test
• test for the integrity of posterior meniscal tears
• Positive if it causes a palpable or audible “click” within the joint

SPECIAL TESTS: Apley’s compression and distraction test:
• Positive if causes pain

SPECIAL TESTS: Bounce Home test
• designed to evaluate a lock of full knee extension

SPECIAL TESTS: Patella femoral grinding test
• designed to determine the quality of the articulating surfaces of the patella and the trochlear groove of the femur.
• Positive if the patient complain of pain and discomfort

SPECIAL TESTS: Apprehension test for patellar dislocation and subluxation
• designed to determine whether or not the patella is prone to lateral dislocation.
• The expression of the patient’s face will become one of the apprehension and distress if the patella begins to dislocate.

SPECIAL TESTS: Tinel Signs:
• refer to the elicitation of pain from tapping for neuromata on the end of a cut nerve, or to the provocation of pain on the leading edge of a regenerating nerve.

SPECIAL TESTS: Knee joint effusion test:
• designed to determine suspected effusion in the knee.

• The knee should be fully extended at heel strike and flexed during all stages of stance phase.

The knee is bent during the swing phase