-
7/31/2019 Phys Ther 2011 Armijo Olivo 1184 97
1/16
doi: 10.2522/ptj.20100233
Originally published online June 9, 20112011; 91:1184-1197.PHYS
THER.
W. Major, Norman M.R. Thie and David J. MageePaulBruno R. da
Costa, Inae C. Gadotti, Sharon Warren,
Susan Armijo-Olivo, Rony Silvestre, Jorge Fuentes,Flexion Test:
A Cross-Sectional StudyDisorders While Performing the
CraniocervicalMuscles in Patients With
TemporomandibularElectromyographic Activity of the Cervical
Flexor
http://ptjournal.apta.org/content/91/8/1184found online at:The
online version of this article, along with updated information and
services, can be
Collections
Tests and MeasurementsInjuries and Conditions: Head and
JawAnatomy and Physiology: Musculoskeletal System
in the following collection(s):This article, along with others
on similar topics, appears
e-Letters
"Responses" in the online version of this article."Submit a
response" in the right-hand menu under
or click onhereTo submit an e-Letter on this article, click
E-mail alerts to receive free e-mail alertshereSign up
by guest on June 1, 2012http://ptjournal.apta.org/Downloaded
from
http://ptjournal.apta.org/cgi/collection/tests_and_measurementshttp://ptjournal.apta.org/cgi/collection/tests_and_measurementshttp://ptjournal.apta.org/cgi/collection/injuries_and_conditions_head_and_jawhttp://ptjournal.apta.org/cgi/collection/injuries_and_conditions_head_and_jawhttp://ptjournal.apta.org/cgi/collection/anatomy_and_physiology_musculoskeletal_systemhttp://ptjournal.apta.org/cgi/collection/anatomy_and_physiology_musculoskeletal_systemhttp://ptjournal.apta.org/letters/submit/ptjournal;91/8/1184http://ptjournal.apta.org/letters/submit/ptjournal;91/8/1184http://ptjournal.apta.org/subscriptions/etoc.xhtmlhttp://ptjournal.apta.org/http://ptjournal.apta.org/http://ptjournal.apta.org/http://ptjournal.apta.org/subscriptions/etoc.xhtmlhttp://ptjournal.apta.org/letters/submit/ptjournal;91/8/1184http://ptjournal.apta.org/cgi/collection/tests_and_measurementshttp://ptjournal.apta.org/cgi/collection/injuries_and_conditions_head_and_jawhttp://ptjournal.apta.org/cgi/collection/anatomy_and_physiology_musculoskeletal_system
-
7/31/2019 Phys Ther 2011 Armijo Olivo 1184 97
2/16
Electromyographic Activity of theCervical Flexor Muscles in
Patients
With Temporomandibular DisordersWhile Performing the
CraniocervicalFlexion Test: A Cross-Sectional StudySusan
Armijo-Olivo, Rony Silvestre, Jorge Fuentes, Bruno R. da Costa,Inae
C. Gadotti, Sharon Warren, Paul W. Major, Norman M.R. Thie,David J.
Magee
Background. Most patients with temporomandibular disorders (TMD)
have beenshown to have cervical spine dysfunction. However, this
cervical dysfunction has
been evaluated only qualitatively through a general clinical
examination of thecervical spine.
Purpose. The purpose of this study was to determine whether
patients with TMDhad increased activity of the superficial cervical
muscles when performing thecraniocervical flexion test (CCFT)
compared with a control group of individuals who
were healthy.
Design. A cross-sectional study was conducted.
Methods. One hundred fifty individuals participated in this
study: 47 werehealthy, 54 had myogenous TMD, and 49 had mixed TMD.
All participants performedthe CCFT. Data for electromyographic
activity of the sternocleidomastoid (SCM) and
anterior scalene (AS) muscles were collected during the CCFT for
all participants. A3-way mixed-design analysis of variance for
repeated measures was used to evaluatethe differences in EMG
activity for selected muscles while performing the CCFTunder 5
incremental levels. Effect size values were calculated to evaluate
the clinicalrelevance of the results.
Results. Although there were no statistically significant
differences in electromyo-graphic activity in the SCM or AS muscles
during the CCFT in patients with mixed andmyogenous TMD compared
with the control group, those with TMD tended to haveincreased
activity of the superficial cervical muscles.
Limitations. The results obtained in this research are
applicable for the group of
individuals who participated in this study under the protocols
used. They couldpotentially be applied to people with TMD having
characteristics similar to those ofthe participants of this
study.
Conclusion. This information may give clinicians insight into
the importance ofevaluation and possible treatment of the deep neck
flexors in patients with TMD.However, future research should test
the effectiveness of this type of programthrough a randomized
controlled trial in people with TMD in order to determine thereal
value of treating this type of impairment in this population.
S. Armijo-Olivo, BScPT, MSc, PhD,Department of Physical
Therapy,Faculty of Rehabilitation Medicine,and Alberta Research
Centre for
Health Evidence, Faculty of Medi-cine and Dentistry, University
ofAlberta, Edmonton, Alberta, Can-ada. Mailing address:
Departmentof Physical Therapy, RehabilitationResearch Centre,
Faculty of Rehabil-itation Medicine, University ofAlberta, 350
Corbett Hall, Edmon-ton, Alberta, Canada T6G 2G4.Address all
correspondence to DrArmijo-Olivo at: [email protected]
[email protected].
R. Silvestre, BScPT, MSc, ResearchCenter of Human Movement,Mayor
University, Santiago, Chile.
J. Fuentes, BSc, MScRS, Rehabilita-tion Research Centre, Faculty
ofRehabilitation Medicine, Univer-sity of Alberta, and Department
ofPhysical Therapy, Catholic Univer-sity of Maule, Talca,
Chile.
B.R. da Costa, BScPT, MSc, Instituteof Social & Preventive
Medicine,University of Bern, Bern, Switzerland.
I.C. Gadotti, BScPT, MScPT, PhD,Department of Physical
Therapy,College of Nursing and Health Sci-ences, Florida
International Uni-versity, Miami, Florida.
S. Warren, PhD, Faculty of Reha-bilitation Medicine, University
ofAlberta.
Author information continues onnext page.
Research Report
Post a Rapid Response tothis article at:ptjournal.apta.org
1184 f Physical Therapy Volume 91 Number 8 August 2011
by guest on June 1, 2012http://ptjournal.apta.org/Downloaded
from
mailto:[email protected]:[email protected]://ptjournal.apta.org/http://ptjournal.apta.org/http://ptjournal.apta.org/http://ptjournal.apta.org/mailto:[email protected]:[email protected]
-
7/31/2019 Phys Ther 2011 Armijo Olivo 1184 97
3/16
Temporomandibular disorders(TMD) are the most prevalentcategory
of nondental chronic
pain conditions in the orofacialregion. These disorders are
charac-
terized by pain affecting the masti-catory muscles, the
temporo-mandibular joint (TMJ), and relatedstructures.1
Temporomandibular dis-orders interfere with daily activitiesand can
significantly affect quality oflife, diminishing patients
capacityfor work and ability to interact withtheir social
environment.2 It hasbeen calculated that approximately$2 billion
has been spent in theUnited States due to TMD directcare.3 Patients
with TMD have
shown high levels of unemploymentand decreased work
effectiveness.4
In a large, population-based, cross-sectional study, it was
shown thatTMD chronic pain had an individualimpact and burden
similar to that ofback pain, severe headache, andchest and
abdominal pain.5
In a recent study,6 women com-prised more than 70% of the
patientshaving TMD, and the ratio between
women and men was 2.4:1 forarthralgia, 2.5:1 for
osteoarthritis,3.4:1 for myofascial pain, and 5.1:1for TMJ disk
displacement.6 The lit-erature supports the fact that
women are more sensitive to painconditions, reporting more
severepain, more frequent pain, and painof longer duration than
men.714 Inaddition, women are more promptin seeking help than men.
Therefore,it seems that women more com-
monly have TMD and may seek carefor TMD pain more often than
men.3
Temporomandibular disorders havecommonly been associated
withsymptoms affecting the head andneck region, such as
headache,cervical spine dysfunction,15,16 andaltered head and
cervical pos-ture.1721 It has been reported thatpain in the
cervical musculoskeletaltissues may be referred to cranial
structures, including the jaw mus-cles22,23; thus, a connection
betweencervical muscle dysfunction and jawsymptoms could
exist.2427Addition-ally, animal studies have revealed
considerable convergence of cranio-facial and cervical afferents
in thetrigeminocervical nucleus and uppercervical nociceptive
neurons.2831
All of this evidence has been the the-oretical foundation of
pain localiza-tion and referral and of neuromuscu-lar adaptations
in the cervical andorofacial regions.3234 However, todate, no
research has demonstrated acause-and-effect relationship.
As stated above, TMD are catego-
rized as musculoskeletal disordersthat commonly involve the
cervicalregion. Other musculoskeletal disor-ders associated with
the cervicalregion, such as neck pain, cervico-genic headache, and
whiplash-associated disorders, are character-ized by abnormal
function of thecervical muscles.3537 However, it isunknown whether
people with TMDhave these muscular alterations.Given the close
connection between
the cervical spine and the orofacialregion, knowledge about
impairmentsin the cervical spine in people withTMD could help
clinicians focus theirefforts on properly evaluating andtreating
these impairments.
Previous work has shown that grosschanges in strength
(force-generatingcapacity) and endurance have beenobserved in
cervical-related disor-ders. However, according to Jull et
al36
and Falla and Farina,38
finerchanges in cervical muscular activityof the cervical spine
are present.Reduced activation of deep cervicalmuscles, augmented
superficial activ-ity of the sternocleidomastoid (SCM)and anterior
scalene (AS) muscles,changes in feedforward activation,reduced
capacity to relax the cervi-cal muscles, and prolonged
muscleactivity following voluntary contrac-tion could lead to a
compromise in
P.W. Major, DDS, MSc, FRCD(c), School ofDentistry, University of
Alberta.
N.M.R. Thie, BSc, MSc, DDS, TMD/OrofacialPain Graduate Program,
School of Dentistry,University of Alberta.
D.J. Magee, PhD, Department of PhysicalTherapy, Faculty of
Rehabilitation Medicine,University of Alberta.
[Armijo-Olivo S, Silvestre R, Fuentes J, et al.Electromyographic
activity of the cervicalflexor muscles in patients with
temporoman-dibular disorders while performing thecraniocervical
flexion test: a cross-sectionalstudy. Phys Ther.
2011;91:11841197.]
2011 American Physical Therapy Association
Published Ahead of Print: June 9, 2011Accepted: April 8,
2011Submitted: July 14, 2010
Cervical Flexor Activity and Temporomandibular Disorders
August 2011 Volume 91 Number 8 Physical Therapy f 1185
by guest on June 1, 2012http://ptjournal.apta.org/Downloaded
from
http://ptjournal.apta.org/http://ptjournal.apta.org/http://ptjournal.apta.org/http://ptjournal.apta.org/
-
7/31/2019 Phys Ther 2011 Armijo Olivo 1184 97
4/16
the control of the cervical spine andconsequently lead to pain
and dys-function.36 Study of these muscularalterations has gained
attention inthe last few years, as exercises
addressing these motor control alter-ations have had good
results inpatients with cervical involve-ment.3941 Therefore, the
assess-ment and treatment of muscularimpairments is considered a
key ele-ment in the management of cervical-associated disorders.
Because TMDhave been considered part of thecervical-associated
disorders, it maybe plausible that similar featurescould be seen in
this patient group.Knowledge about these features
would be useful for clinicians treat-ing patients with TMD.
However,studies of muscular impairments inpatients with TMD are
lacking.
Cervical dysfunction in patients withTMDs has been evaluated
only qual-itatively through a general clinical
examination of the cervical spine.Most of the studies have
looked atcervical spine signs and symptoms inpeople with TMD, but
they have notinvestigated any motor alterations
in a quantitative way. For example,de Wijer and
colleagues27,42
concluded that symptoms of thestomatognathic system overlap
inpatients with TMD and cervicalspine disorders and that symptomsof
the cervical spine overlap in thesame group of patients. Visscher
etal25 found that patients with chronicTMD more often had cervical
spinepain than those without this disor-der. Stiesch-Scholz et al43
found thatasymptomatic functional disorders
of the cervical spine occurred morefrequently in patients with
internalderangement of the TMJ than in acontrol group. The presence
of ten-der points in the cervical spine andshoulder girdle in
patients with thesame diagnosis was more common,especially in upper
segments of the
cervical spine, compared with a con-trol group of individuals
who werehealthy. Furthermore, a recent sys-tematic review44 showed
that exer-cises for the neck that also were used
to improve neck and head posturedecreased symptoms in
patientswith TMD. However, the systematicreview found that details
of the exer-cises and exercise programs (ie, typeof exercise,
dosage, and frequency)
were lacking, as well as a clearunderlying mechanism of why
theseexercises, directed toward to theneck, improved TMD
symptoms.
Based on the above information, itwas evident that a more
quantitative
evaluation of the motor activity ofthe cervical muscles through
electro-myographic (EMG) assessment, look-ing at performance
patterns ofthe cervical musculature activity inpatients with TMD,
could assist inclarifying the role of the cervicalmuscles
involvement in the symp-toms of these patients. Additionally,this
evaluation could open an areaof study aimed at treating these
alter-ations through improvement of
motor control of the cervical mus-cles in patients with TMD.
The main objective of this study wasto determine, through EMG
evalua-tion, whether patients with myoge-nous TMD and mixed TMD
hadaltered muscle activity (ie, higherEMG activity) of the
superficial cer-
vical muscles (SCM and AS) whenperforming the CCFT compared
with a control group of individuals
who were healthy. The secondaryobjectives of this study were:
(1) todetermine whether there was anassociation between the
perfor-mance of the cervical flexor musclesduring the 5 stages of
the CCFT andneck disability and jaw disability and(2) to determine
whether there wasan association between level ofchronic disability
in patients withTMD based on the Research Diagnos-tic Criteria for
Temporomandibular
The Bottom Line
What do we already know about this topic?
Cervical spine dysfunction has been reported to be associated
with tem-
poromandibular disorders (TMD). Temporomandibular disorders also
are
commonly associated with other symptoms affecting the head and
neck
region such as headache, ear-related symptoms, and altered head
and
cervical posture. However, no study has investigated the
presence of
cervical muscle impairments using electromyography.
What new information does this study offer?
The results of this study may give clinicians insight into the
importance of
the evaluation and possible treatment of the deep neck flexors
in patientswith TMD. However, randomized clinical trials are
necessary to determine
the effectiveness of an exercise program targeting the deep neck
flexors
in these patients.
If youre a patient, what might these findings meanfor you?
If you have a TMD, these findings may help your physical
therapist
evaluate your condition. This evaluation would include an
examination of
the cervical musculature as well as the TMD.
Cervical Flexor Activity and Temporomandibular Disorders
1186 f Physical Therapy Volume 91 Number 8 August 2011
by guest on June 1, 2012http://ptjournal.apta.org/Downloaded
from
http://ptjournal.apta.org/http://ptjournal.apta.org/http://ptjournal.apta.org/http://ptjournal.apta.org/
-
7/31/2019 Phys Ther 2011 Armijo Olivo 1184 97
5/16
Disorders45 (RDC/TMD) (ChronicPain Grade Disability
Questionnairefor TMD), pain intensity, duration ofcomplaint, and
performance of thecervical flexor muscles during the 5
stages of the CCFT.
MethodDesign
A cross-sectional study wasconducted.
ParticipantsA convenience sample of patientswho attended the
TMD/OrofacialPain Clinic at the School of Dentistry,Faculty of
Medicine and Dentistry,University of Alberta, and students
and staff at the University of Albertawho were healthy was
recruited forthis study. The sample size for thisstudy was
calculated based on arepeated-measures analysis of vari-ance
(ANOVA) following the guide-lines established by Stevens (with.05,
0.20, power80%, andeffect size0.57).46 A minimum of 40participants
per group was needed.
The inclusion and exclusion criteria
for the individuals who were healthyand the patients with TMD
havebeen described elsewhere.47,48 Inbrief, people who were healthy
wereincluded if they were womenbetween the ages of 18 and 50
years16 and they did not have a his-tory of musculoskeletal
pain, TMDsymptoms, neurological disease, sys-temic disease, or
mental illness thatcould interfere with the outcomes.Patients with
TMD were included if
they were women between 18 and50 years of age, had pain in the
mas-ticatory muscles or TMJ of at least 3months duration, and had a
moder-ate or severe baseline pain score(30 mm) on a 100-mm visual
ana-log scale (VAS).49 Patients were clas-sified as having
myogenous TMDbased on the classification Ia and Ibof Dworkin and
LeResche.45 In addi-tion, they had to have pain uponpalpation in at
least 3 of the 12 mus-
cular points proposed by Fricton andSchiffman.5052 Patients were
diag-nosed as having mixed TMD if theycomplained of muscular
symptomsin addition to TMJ symptoms suchas painful clicking,
crepitation, orpain in the TMJ at rest or duringfunction53 and
during a compressiontest.54
A total 168 individuals were assessedfor inclusion in this
study. A total of18 individuals were excluded. Themain reasons for
exclusion were: nottotally healthy (n9), older than 50
years of age (n2), having a neuro-logical disease (n1), having
cancer(n1), and having a pain score lowerthan 30 mm on the VAS
(n5). Onehundred fifty participants provideddata for this study: 47
were healthy,
54 had myogenous TMD, and 49 hadmixed TMD.
The general demographics for eachgroup and the clinical
characteristicsof the participants are displayed inTable 1. There
were no significantdifferences in age and height in thesample
(P.05). However, weight
was significantly different betweenparticipants with mixed TMD
andthose with myogenous TMD (meandifference8.0 kg, 95%
confidenceinterval [CI]1.9 to 14.2; P.006)and between participants
withmixed TMD and those who werehealthy (mean difference7.8 kg,95%
CI1.4 to 14.2; P.01).
Participants with mixed TMD weresimilar to those with
myogenous
Table 1.Descriptive Statistics of Height, Weight, and Age and
Clinical Characteristics ofParticipants by Groupa
Variable Group X SD
Height (cm) Myogenous TMD (n54) 165.1 5.1
Healthy (n47) 165.0 6.8
Mixed TMD (n49) 166.3 5.9
Weight (kg) Myogenous TMD 64.1b 9.9
Healthy 64.3b 12.7
Mixed TMD 72.1c 15.9
Age (y) Myogenous TMD 31.4 9.0
Healthy 28.3 7.5
Mixed TMD 31.3 8.3
Duration of complaint (y) Myogenous TMD 6.5c 6.4
Healthy 0.0 0.0
Mixed TMD 8.3c 6.4
Pain intensity (0100 mm) Myogenous TMD 45.3c 17.3
Healthy 0.0 0.0
Mixed TMD 49.0c 16.1
Neck Disability Index
(050 points)
Myogenous TMD 10.5c 5.5
Healthy 1.6 1.6
Mixed TMD 12.6c 6.8
Jaw Function Scale
(1050 points)
Myogenous TMD 18.6b,c 6.6
Healthy 10.1 0.4
Mixed TMD 22.7c 7.1
a TMDtemporomandibular disorders.b Significantly different
compared with participants with mixed TMD at .05.c Significantly
different compared with participants who were healthy at .05.
Cervical Flexor Activity and Temporomandibular Disorders
August 2011 Volume 91 Number 8 Physical Therapy f 1187
by guest on June 1, 2012http://ptjournal.apta.org/Downloaded
from
http://ptjournal.apta.org/http://ptjournal.apta.org/http://ptjournal.apta.org/http://ptjournal.apta.org/
-
7/31/2019 Phys Ther 2011 Armijo Olivo 1184 97
6/16
TMD in most of the general charac-teristics such as duration of
com-plaint and pain intensity (P.05).Both groups had a moderate
inten-sity of pain in the jaw and a long
history of pain. Both groups also hada mild level of disability
in the neckand a moderate level of disability inthe jaw (Tab. 1).
The Limitations ofDaily Functions in TMD Question-naire/Jaw
Function Scale (JFS) dis-ability score was significantly higherfor
participants with mixed TMDcompared with those with myoge-nous TMD
(mean difference4.1points, 95% CI1.4 to 6.9; P.001).
The prevalence of neck pain in the
sample of participants with TMD washigh. Approximately 88%
(87.5%) ofthe participants with myogenousTMD and 87.8% of those
with mixedTMD had self-reported neck pain.
Clinical ExaminationThe participants underwent a clini-cal
examination by a physical thera-pist with experience in
musculo-skeletal rehabilitation to determineeligibility for this
study and to deter-
mine their diagnosis. The clinicalexamination followed the
guidelinesof the RDC/TMD.45 All participantsread an informational
letter andsigned an informed consent state-ment in accordance with
the Univer-sity of Albertas policies on researchusing human
subjects.
ProcedureDemographic data were collectedon all participants who
satisfied the
inclusion criteria. In addition, allincluded participants were
askedto report specific characteristicsregarding their jaw problem
(eg,onset, duration of symptoms, treat-ments received) and their
intensityof pain in the jaw (VAS score)49,5558
and to complete the Neck DisabilityIndex (NDI),59,60 the JFS,61
and aquestionnaire for history of jaw painused by the RDC/TMD.45 In
addition,participants were asked to complete
the Chronic Pain Grade DisabilityQuestionnaire for TMD used by
theRDC/TMD to evaluate the level ofchronic disability due to
TMDs.45
The reliability and validity of these
tools have been reported else-where.45,59 61 After the
participantswere evaluated clinically and hadcompleted the
questionnaires, theyperformed the CCFT. This testing
was performed in one session.
Electromyographic Evaluation ofthe Cervical Flexor
MusclesElectrode placement. Surface elec-trodes were located on the
sternalhead of the SCM muscle and on the
AS muscle as described in the proto-
col used by Falla and colleagues.62,63
A reference electrode was placed onthe wrist.
Normalization procedure for EMGdata. For normalization
purposes,EMG data were collected for 5 sec-onds during a maximal
voluntarycontraction (MVC). The EMG activityof the SCM and AS
muscles wasrecorded during this maximal con-traction and saved in
the computer.
This procedure was repeated a sec-ond time. Submaximal
contractionsobtained during the CCFT were nor-malized using these 2
MVC values.Submaximal contractions wereexpressed as a percentage of
the3-second root mean square (RMS)
value obtained during the MVC. Theaverage between the normalized
con-tractions using the 2 MVC measure-ments was used for
statistical analysis.
EMG data processing. Data onEMG activity of the SCM and
ASmuscles were obtained using theBagnoli-8 EMG system* in a
bipolarconfiguration with DE-2.1 elec-trodes.* This system is
designed tomake the acquisition of EMG signalseasy and reliable
(common-moderejection ratio92 dB, system
noise1.2 V [RMS]). The EMGactivity was recorded (analog
rawsignal) with a data acquisition pro-gram, written in Labview
7.1,whichcollected data at 1,024 Hz using a
PCMCIA card
filtered between 20and 450/Hz 10% and amplifiedusing a gain of
1,000 according tothe established standards for EMGacquisition and
reporting.64,65 Toobtain a measure of EMG amplitude,maximum root
mean square (RMS)
was calculated for 4 seconds duringthe 10-second submaximal
contrac-tions for each muscle while per-forming the CCFT using
IGORPro5.1 and was expressed a per-centage of the 3-second EMG
activity
obtained during the MVC normaliza-tion procedure.
Instrumentation for Registeringthe Pressure Exerted
WhilePerforming the CCFT
An air-filled pressure sensor (pres-sure biofeedback unit) was
placedin the suboccipital region of eachpatients neck and inflated
to a pres-sure of 20 mm Hg. The cuff wasconnected to a pressure
transducer
(miniature pressure cell) designedto register increases in
pressure withthe movement of nodding action forthe CCFT. Electrical
signals from thepressure transducer were amplifiedto a visual
feedback device and pro-
jected onto a computer screen sothat the participants were able
to seethe targeted pressure level. Graphs
with the performance of each partic-ipant during the CCFT were
storedusing Igor Pro5.1. These data wereanalyzed offline by a
blinded assessor.
Craniocervical Flexion Test:Description and ProceduresBefore
testing began, participants
were asked to perform a warm-up,which consisted of 2 movements
ofthe neck and head in all directions
* Delsys Inc, PO Box 15734, Boston, MA02215.
National Instruments Corporation, 11500 NMopac Expwy, Austin, TX
78759-3504.WaveMetrics Inc, PO Box 2088, LakeOswego, OR 97035.
Cervical Flexor Activity and Temporomandibular Disorders
1188 f Physical Therapy Volume 91 Number 8 August 2011
by guest on June 1, 2012http://ptjournal.apta.org/Downloaded
from
http://ptjournal.apta.org/http://ptjournal.apta.org/http://ptjournal.apta.org/http://ptjournal.apta.org/
-
7/31/2019 Phys Ther 2011 Armijo Olivo 1184 97
7/16
(flexion [forward neck movement],extension, side flexion
[lateral move-ment of the neck], and rotation). Theparticipants
were placed in a relaxedsupine position with the knees
flexed and the head and neck main-tained in a mid-position (ie,
neutralposition, no flexion or extension)following a protocol
established pre-
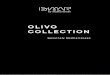
viously.66 The head and chin wereparallel to the plinth (Fig.
1).
The CCFT is a low-load test that isthe most common method used
toevaluate the performance of thedeep cervical muscles (ie,
longuscolli and rectus capitis). The CCFTconsists of a
craniocervical flexion
(nodding) movement, which com-bines the action of flexion at
thecraniocervical junction, performedby the longus capitis muscles,
along
with the flattening of the cervicallordosis, an action of the
longus collimuscles. Electromyographic activityof the superficial
cervical flexor mus-cles such as the SCM and AS may beregistered
during the CCFT. ElevatedEMG activity may be a compensationfor
reduced or impaired activity of
the deep cervical flexor muscles inindividuals with
cervical-associatedpain compared with those who arehealthy.67
The CCFT required each participantto perform the craniocervical
flexionmovement in 5 progressive stages ofincreasing pressure (22,
24, 26, 28,and 30 mm Hg) with the aid of a
visual feedback device. Participantswere instructed to perform
this gen-
tle nodding movement (craniocervi-cal flexion) and at practiced
progres-sive targeted pressure levels. Theorder of the targeted
pressure level
was randomized by an independentassessor. Participants had to
main-tain a steady pressure at each tar-geted level for a duration
of 10 sec-onds (Fig. 1). They repeated eachtargeted level 2 times,
with a restperiod of 1 minute between repeti-tions to avoid the
effects of fatigue.68
Data Analysis
The normalized data of the EMGactivity of all muscles were
analyzeddescriptively (ie, mean, standarddeviation). Variables were
tested fornormality, homogeneity of variance,and linearity. All EMG
variables werereasonably normally distributed. His-tograms and box
plots show thatmost of the variables were slightlyskewed to the
right. However,
ANOVA analysis is robust to thesemild deviations from normality
and
can provide accurate estimates ofthe analyzed variables.69
A 3-way mixed-design ANOVA forrepeated measures (3
independent
variables: muscles [SCM and AS], test[5 levels], and groups
[myogenousTMD, mixed TMD, and control]) wasused to evaluate the
differences inEMG activity for selected muscles(dependent variable)
while perform-ing the CCFT at 5 levels of pressure.
Pair-wise comparisons using the
Bonferroni procedure were adminis-tered to evaluate the
differencesbetween variables and groups (ie,control and TMD groups)
in all ofthe different conditions (objective1). The Spearman rho
test was usedto evaluate the relationship amongNDI, JFS, and
clinical variables withEMG variables (correlational
matrix)(objectives 2 and 3). The correlation
was considered important when thecorrelation coefficient value
was
higher than .70. The reference val-ues to make this decision
were basedon values reported by Munro.70
To clearly show the impact of theresults for clinical practice,
clinicalrelevance of the results was assessedusing a
distribution-based method.71
The effect size (Cohen d) valueswere calculated to determine
clinicalrelevance of the differences in theEMG measurements across
different
Figure 1.Craniocervical flexion test.
Cervical Flexor Activity and Temporomandibular Disorders
August 2011 Volume 91 Number 8 Physical Therapy f 1189
by guest on June 1, 2012http://ptjournal.apta.org/Downloaded
from
http://ptjournal.apta.org/http://ptjournal.apta.org/http://ptjournal.apta.org/http://ptjournal.apta.org/
-
7/31/2019 Phys Ther 2011 Armijo Olivo 1184 97
8/16
levels of pressure and groups.72
Effect sizes of 0.4 or higher wereconsidered clinically
relevant.73 Asubgroup analysis also was con-ducted to determine
differencesbetween participants with pureTMD (ie, without neck
pain) and
those who were healthy.
The level of significance was set at.05. The SPSS version 17
andSTATA version 10 statistical pro-grams were used to perform the
sta-tistical analysis. The analysis was per-formed blinded to group
condition.
ResultsEMG Activity of the CervicalFlexors Muscles
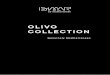
WhilePerforming the CCFTLarge variability of the normalizedEMG
activity across conditions andgroups was observed (Fig. 2).
Using
a 3-way mixed-design ANOVA forrepeated measures, we foundthat
the main effects of muscles(F18.5, P.0001) and pressure lev-els
(F27.3, P.0001) were statisti-cally significant. This finding
meansthat there was a statistically signifi-cant difference in EMG
activityamong muscles and among pressurelevels. The interaction
between mus-cles and pressure also was statisti-cally significant
(F2.9, P.001).
However, there was no significantdifference in EMG activity of
the ana-lyzed muscles among groups (ie,mixed TMD, myogenous TMD,
andcontrol) across conditions (F2.6,P.07). Weight was not
significantlyassociated with EMG activity (P.49),
so it was not included in the model.
Subgroup Analysis: EMG Activityin Patients With Pure TMD(Without
Neck Pain) ComparedWith Participants Who WereHealthy
When analyzing a subgroup of par-ticipants with TMD but
withoutneck pain (n13) compared withthe control group (n47),
statisti-cally significant differences in EMG
SPSS Inc, 233 S Wacker Dr, Chicago, IL60606. StataCorp LP, 4905
Lakeway Dr, College Sta-tion, TX 77845.
Mixed TMDHealthyMyogenous TMD
NormalizedEMGActivity
(%MVC)
60
50
40
30
20
10
0 AvASL_30mmH
g
AvASL_28mmH
g
AvASL_26mmH
g
AvASL_24mmH
g
AvASL_22mmH
g
AvASL_30mmH
g
AvASL_28mmH
g
AvASL_26mmH
g
AvASL_24mmH
g
AvASL_22mmH
g
AvASL_30mmH
g
AvASL_28mmH
g
AvASL_26mmH
g
AvASL_24mmH
g
AvASL_22mmH
g
AvASR_28mmH
g
AvASR_26mmH
g
AvASR_24mmH
g
AvASR_22mmH
g
AvASR_30mmH
g
AvASR_28mmH
g
AvASR_26mmH
g
AvASR_24mmH
g
AvASR_22mmH
g
AvASR_30mmH
g
AvASR_28mmH
g
AvASR_26mmH
g
AvASR_24mmH
g
AvASR_22mmH
g
AvASR_30mmH
g
AvSCML_30mm
Hg
AvSCML_28mm
Hg
AvSCML_26mm
Hg
AvSCML_24mm
Hg
AvSCML_22mm
Hg
AvSCML_30mm
Hg
AvSCML_28mm
Hg
AvSCML_26mm
Hg
AvSCML_24mm
Hg
AvSCML_22mm
Hg
AvSCML_30mm
Hg
AvSCML_28mm
Hg
AvSCML_26mm
Hg
AvSCML_24mm
Hg
AvSCML_22mm
Hg
AvSCMR_24mm
Hg
AvSCMR_22mm
Hg
AvSCMR_30mm
Hg
AvSCMR_28mm
Hg
AvSCMR_26mm
Hg
AvSCMR_24mm
Hg
AvSCMR_22mm
Hg
AvSCMR_30mm
Hg
AvSCMR_28mm
Hg
AvSCMR_26mm
Hg
AvSCMR_24mm
Hg
AvSCMR_22mm
Hg
AvSCMR_30mm
Hg
AvSCMR_28mm
Hg
AvSCMR_26mm
Hg
Figure 2.Normalized electromyographic (EMG) activity of
sternocleidomastoid (SCM) and anterior scalene (AS) muscles in
participants withmyogenous temporomandibular disorders (TMD), those
with mixed TMD, and those who were healthy while performing
thecraniocervical flexion test. Error bars95% confidence interval.
%MVCpercentage of maximum voluntary contraction,
AvSCMR_22mmHgaverage right SCM muscle EMG activity at 22 mm Hg,
AvSCML_22mmHgaverage left SCM muscle EMGactivity at 22 mm Hg,
AvASR_22mmHGaverage right AS muscle EMG activity at 22 mm Hg,
AvASL_22mmHgaverage left
AS muscle EMG activity at 22 mm Hg, AvSCMR_24mmHgaverage right
SCM muscle EMG activity at 24 mm Hg,AvSCML_24mmHgaverage left SCM
muscle EMG activity at 24 mm Hg, AvASR_24mmHgaverage right AS
muscle EMG activityat 24 mm Hg, AvASL_24mmHgaverage left AS muscle
EMG activity at 24 mm Hg, AvSCMR_26mmHgaverage right SCM muscleEMG
activity at 26 mm Hg, AvSCML_26mmHgaverage left SCM muscle EMG
activity at 26 mm Hg, AvASR_26mmHgaverageright AS muscle EMG
activity at 26 mm Hg, AvASL_26mmHgaverage left AS muscle EMG
activity at 26 mm Hg,
AvSCMR_28mmHgaverage right SCM muscle EMG activity at 28 mm Hg,
AvSCML_28mmHgaverage left SCM muscle EMGactivity at 28 mm Hg,
AvASR_28mmHgaverage right AS muscle EMG activity at 28 mm Hg,
AvASL_28mmHgaverage left AS
muscle EMG activity at 28 mm Hg, AvSCMR_30mmHgaverage right SCM
muscle EMG activity at 30 mm Hg,AvSCML_30mmHgaverage left SCM
muscle EMG activity at 30 mm Hg, AvASR_30mmHgaverage right AS
muscle EMG activityat 30 mm Hg, AvASL_30mmHgaverage left AS muscle
EMG activity at 30 mm Hg.
Cervical Flexor Activity and Temporomandibular Disorders
1190 f Physical Therapy Volume 91 Number 8 August 2011
by guest on June 1, 2012http://ptjournal.apta.org/Downloaded
from
http://ptjournal.apta.org/http://ptjournal.apta.org/http://ptjournal.apta.org/http://ptjournal.apta.org/
-
7/31/2019 Phys Ther 2011 Armijo Olivo 1184 97
9/16
activity were found between groups(F4.831, P.01). Post hoc
analysisusing a Bonferroni test indicatedthere were many
statistically signifi-
cant differences between groups inthe analyzed muscles and
conditions(Tab. 2).
Association Between EMGVariables and Clinical VariablesWhile
Performing the CCFT
Very weak (although statistically sig-
nificant) correlations were found,mainly between the EMG
activity ofthe SCM muscles during the 5 stages
of the CCFT and clinical variablessuch as pain intensity,
duration ofcomplaint, neck disability, jaw dis-ability, and level
of chronic disability
of TMD based on the RDC/TMD(Chronic Pain Grade Disability
Ques-tionnaire for TMDs) (Tab. 3).
Table 3.Correlations Between Electromyographic Activity and Neck
Disability (as Measured by Neck Disability Index), Chronic Pain
GradeClassification, Jaw Disability (as Measured by Jaw Function
Scale), Pain Intensity, and Duration of Complainta
Electromyographic
Activity
Neck
Disability
Chronic Pain
Grade Classification
Jaw
Disability
Pain
Intensity
Duration of
Complaint (y)
Average SCM at 22 mm Hg .23b .26b .26b .32b .15
Average AS at 22 mm Hg .13 .15 .15 .21b .05
Average SCM at 24 mm Hg .23b
.26b
.30b
.32b
.19c
Average AS at 24 mm Hg .14 .16 .17c .21c .08
Average SCM at 26 mm Hg .18c .19c .24b .29b .09
Average AS at 26 mm Hg .13 .12 .15 .21b .04
Average SCM at 28 mm Hg .18c .17 .23b .27b .13
Average AS at 28 mm Hg .13 .10 .17c .22b .03
Average SCM at 30 mm Hg .24b .21c .28b .33b .16c
Average AS at 30 mm Hg .20c .18c .22b .28b .11
a SCMsternocleidomastoid muscle, ASanterior scalene muscle.b
Correlation is significant at the .05 level.c Correlation is
significant at the .01 level.
Table 2.Subgroup Analysis Between Participants With Pure
Temporomandibular Disorders and Participants Who Were
Healthy:Electromyographic Activity of the Analyzed Muscles While
Performing the Craniocervical Flexion Test a
Muscle
Pressure
(mm Hg) Group Group
Mean
DifferenceBetween Groups
(%MVC)
Standard
Error Pb
95% Confidence
Interval for
Difference
Lower
Bound
Upper
Bound
SCMR 22 Myogenous TMD Healthy 9.51c 3.315 .017 1.35 17.68
24 Myogenous TMD Healthy 11.06c 3.719 .013 1.90 20.22
28 Myogenous TMD Healthy 11.92c 4.580 .035 0.637 23.20
30 Myogenous TMD Healthy 12.17c 5.149 .050 0.051 24.86
SCML 22 Healthy Myogenous TMD 6.80c 2.715 .045 13.48 0.11
Mixed TMD 9.54c 3.380 .019 17.87 1.22
24 Healthy Myogenous TMD 7.32c 2.922 .045 14.52 0.124
Mixed TMD 12.64c 3.637 .003 21.59 3.68
26 Healthy Mixed TMD 10.68 4.393 .050 21.50 0.014
ASR 22 Myogenous TMD Healthy 9.74 3.981 .050 0.062 19.55
ASL 24 Healthy Mixed TMD 17.43c 6.631 .033 33.759 1.093
aValues based on estimated marginal means. TMDtemporomandibular
disorders, SCMRright sternocleidomastoid, SCMLleft
sternocleidomastoid,ASRright anterior scalene, and ASLleft anterior
scalene.b Bonferroni adjustment for multiple comparisons.c The mean
difference is significant at the .05 level.
Cervical Flexor Activity and Temporomandibular Disorders
August 2011 Volume 91 Number 8 Physical Therapy f 1191
by guest on June 1, 2012http://ptjournal.apta.org/Downloaded
from
http://ptjournal.apta.org/http://ptjournal.apta.org/http://ptjournal.apta.org/http://ptjournal.apta.org/
-
7/31/2019 Phys Ther 2011 Armijo Olivo 1184 97
10/16
Clinical RelevanceEffect sizes of comparisons betweenmixed TMD
and myogenous TMDgroups compared with the controlgroup while
performing the CCFT
are displayed in Table 4 and Figures3 and 4.
DiscussionThe main finding of this study wasthat, although
statistically significantdifferences in EMG activity of theSCM and
AS muscles in patients withTMD compared with participants
who were healthy while performingthe CCFT were not attained
(P.07),there was a trend for patients with
TMD to have consistently higherEMG activity in all of the
analyzedmuscles. This increased activity ofthe superficial muscles
of the cervi-cal spine might be associated with
the neck disturbances seen inpatients with TMD. This
informationmay give clinicians insight into theimportance of
evaluation and possi-ble treatment of the deep neck flex-ors in
patients with TMD. However,at this point, more research on
theseissues is necessary to provide defi-nite conclusions.
The results of this study cannot bedirectly compared with those
of
other studies of cervical flexor mus-cle performance in patients
withTMD because no studies investigat-ing this issue in this
population werefound. However, the CCFT has
widely been used by physical thera-pists to determine
alterations in themotor control of the craniocervicalflexor muscles
in people with cervi-cal disorders such as neck pain,
whiplash-associated disorders, andcervicogenic headache
becauseimpairment of the deep flexor mus-cles appears to be generic
to neckdisorders.37 All of the studies analyz-ing craniocervical
performance usingthe CCFT36,63,74,75 converge in that
Table 4.Moderate Effect Sizes for Comparisons Among Groups at
Different Levels of Pressure While Performing the Craniocervical
FlexionTesta
Outcome Measure:
Electromyographic Activity
Raw Differences Standardized Effect Size
Mean
Difference
(%MVC)
Confidence Interval
for Difference
Effect
Size
Confidence Interval
for Effect Size
Effect Size
Based onHealthy Group
Standard
Deviation
Lower
Bound
Upper
Bound
Lower
Bound
Upper
Bound
Average SCMR at 22 mm Hg,
mixed TMD vs healthy
5.36 1.65 9.07 0.59 0.17 0.99 0.73
Average SCMR at 24 mm Hg,
mixed TMD vs healthy
5.88 1.83 9.93 0.59 0.18 0.99 0.72
Average SCMR at 28 mm Hg,
mixed TMD vs healthy
5.94 0.77 11.11 0.47 0.06 0.87 0.54
Average SCMR at 30 mm Hg,
mixed TMD vs healthy
6.31 0.67 11.95 0.45 0.04 0.85 0.48
Average SCML at 22 mm Hg,
myogenous TMD vs healthy
5.10 0.66 9.54 0.45 0.06 0.85 0.72
Average SCML at 22 mm Hg,
mixed TMD vs healthy
5.79 2.06 9.52 0.63 0.21 1.03 0.82
Average SCML at 24 mm Hg,
myogenous TMD vs healthy
4.87 0.79 8.95 0.47 0.07 0.87 0.66
Average SCML at 24 mm Hg,
mixed TMD vs healthy
6.53 2.49 10.57 0.66 0.24 1.06 0.89
Average SCML at 26 mm Hg,
mixed TMD vs healthy
4.63 0.25 9.01 0.43 0.02 0.83 0.50
Average SCML at 30 mm Hg,
mixed TMD vs healthy
5.19 0.06 10.32 0.41 0.00 0.81 0.42
Average ASR at 22 mm Hg,
myogenous TMD vs healthy
6.39 0.49 12.29 0.43 0.03 0.82 0.60
Average ASR at 30 mm Hg,
myogenous TMD vs healthy
12.07 1.02 23.12 0.43 0.03 0.82 0.72
Average ASR at 30 mm Hg,
mixed TMD vs healthy
8.24 0.17 16.31 0.41 0.01 0.81 0.49
a TMDtemporomandibular disorders, SCMRright sternocleidomastoid
muscle, SCMLleft sternocleidomastoid muscle, ASRright anterior
scalene muscle,%MVCpercentage of maximum voluntary contraction.
Cervical Flexor Activity and Temporomandibular Disorders
1192 f Physical Therapy Volume 91 Number 8 August 2011
by guest on June 1, 2012http://ptjournal.apta.org/Downloaded
from
http://ptjournal.apta.org/http://ptjournal.apta.org/http://ptjournal.apta.org/http://ptjournal.apta.org/
-
7/31/2019 Phys Ther 2011 Armijo Olivo 1184 97
11/16
patients with cervical involvementhave an impaired performance
of thedeep and superficial flexor cervicalmuscles. The increased
activity inthe superficial muscles could be seenas a strategy to
compensate for thedysfunction of the deep flexor mus-cles. Sterling
et al76 suggested thatthe presence of pain could lead toinhibition
or delayed activation of
specific muscles or group of musclesin the spine. This
inhibition gener-ally occurs in deep muscles such asthe longus
colli and longus capitis,
which control joint stability.76
The results of this study are not intotal agreement with those
ofthe majority of the above-mentionedstudies. In our study, we
found no
statistically significant differences insuperficial cervical
flexor muscularactivity among groups while per-forming the CCFT, as
evaluatedthough EMG analysis. One possibleexplanation for these
results couldbe the level of dysfunction presentedby the
participants with TMD. Wefound that the level of dysfunction,not
only at the level of the neck but
Study or
Subgroup
Mixed TMD Healthy
Weight
Mean Difference Mean Difference
X SD Total X SD Total IV, Fixed, 95% CI IV, Fixed, 95% CI
ASR at 30 mm Hg 38.09 22.55 49 29.85 16.7 47 3.2% 8.24 (0.32,
16.16)
SCML at 22 mm Hg 22.83 10.83 49 17.04 7.09 47 14.8% 5.79 (2.14,
9.44)
SCML at 24 mm Hg 24.85 11.93 49 18.32 7.36 47 12.7% 6.53 (2.58,
10.48)SCML at 26 mm Hg 26.61 12.07 49 21.98 9.29 47 10.7% 4.63
(0.33, 8.93)
SCML at 28 mm Hg 28.82 12.5 49 24.2 10.4 47 9.4% 4.62 (0.03,
9.21)
SCML at 30 mm Hg 30.49 12.93 49 25.3 12.35 47 7.7% 5.19 (0.13,
10.25)
SCMR at 22 mm Hg 21.01 10.59 49 15.65 7.34 47 15.0% 5.36 (1.73,
8.99)
SCMR at 24 mm Hg 23.19 11.48 49 17.31 8.15 47 12.5% 5.88 (1.91,
9.85)
SCMR at 28 mm Hg 28.57 14.25 49 22.63 10.98 47 7.7% 5.94 (0.86,
11.02)
SCMR at 30 mm Hg 30.58 14.5 49 24.2 13.27 47 6.4% 6.38 (0.82,
11.94)
Total (95% CI) 490 470 100.0% 5.68 (4.27, 7.08)
Heterogeneity: 21.16, df9 (P1.00), I20%
Test for overall effect: Z7.92 (P.00001)
Figure 3.Moderate effect sizes found for comparisons between
participants with mixed temporomandibular disorders (TMD) and those
whowere healthy at different levels of pressure while performing
the craniocervical flexion test. IVinverse variance, 95%
CI95%confidence interval, ASRright anterior scalene muscle,
SCMLleft sternocleidomastoid muscle, SCMRright
sternocleidomastoidmuscle.
Study or
Subgroup
Myogenous TMD Healthy
Weight
Mean Difference Mean Differen ce
X SD Total X SD Total IV, Fixed, 95% CI IV, Fixed, 95% CI
ASR at 22 mm Hg 26.05 17.83 54 19.66 10.59 47 19.3% 6.39 (0.75,
12.03)
ASR at 30 mm Hg 41.92 34.82 54 29.85 16.73 47 5.6% 12.07 (1.62,
22.52)
SCML at 22 mm Hg 22.14 13.83 54 17.04 7.09 47 34.7% 5.10 (0.89,
9.31)
SCML at 24 mm Hg 23.19 12.3 54 18.32 7.36 47 40.4% 4.87 (0.97,
8.77)
Total (95% CI) 216 188 100.0% 5.65 (3.17, 8.13)
Heterogeneity: 21.74, df3 (P.63), I20%
Test for overall effect: Z4.47 (P.00001)
Figure 4.Moderate effect sizes found for comparisons between
participants with myogenous temporomandibular disorders (TMD) and
thosewho were healthy at different levels of pressure while
performing the craniocervical flexion test. IVinverse variance, 95%
CI95%confidence interval, ASRright anterior scalene muscle,
SCMLleft sternocleidomastoid muscle.
Cervical Flexor Activity and Temporomandibular Disorders
August 2011 Volume 91 Number 8 Physical Therapy f 1193
by guest on June 1, 2012http://ptjournal.apta.org/Downloaded
from
http://ptjournal.apta.org/http://ptjournal.apta.org/http://ptjournal.apta.org/http://ptjournal.apta.org/
-
7/31/2019 Phys Ther 2011 Armijo Olivo 1184 97
12/16
also at the level of the jaw, wasconsidered mild for our
participants
with TMD. We might speculate thatbecause the disability was
mild, it didnot have an impact on function or
physical impairment, which gener-ally is found in people with
moredisabling pain. Our results are inagreement with the results
obtainedby Falla et al63 in individuals with alevel of disability
similar to that ofthe participants in this present study(mean NDI
score12.4 points,SD9.563). Falla et al63 found thateven though the
normalized EMGamplitude of the deep cervical flexormuscles was
significantly lower inpatients with neck pain compared
with individuals who were healthy(P.05), the increase in EMG
activityof the superficial muscles did notreach statistical
significance,although there was a trend ofincreased EMG activity
for the super-ficial muscles in patients with neckpain. The main
explanation of thisfinding was the large variability inthe EMG
activity found acrossgroups and conditions. These resultsagree with
our findings, which also
showed a large amount of variabilityin EMG activity among
muscles andconditions (as evidenced by the
wide CIs). When interpreting CIs,lower and upper boundaries need
tobe taken into account to make con-clusions.77 Based on this
interpreta-tion, we can say that 95% of the timethe estimated
difference betweengroups could fall between theselower and upper
boundaries. If welook at the upper boundaries of the
CIs for the raw mean differences(Tab. 4), we can see that the
differ-ence between groups can be as highas 8.95% to 23.12% of MVC.
How-ever, if we look at the lower bound-aries, the difference
between groupscan be as low as 0.06% to 2.49% ofMVC. Therefore,
based on this large
variability, we could have a situationwhere a clinically
significant differ-ence between groups as well as a
nonclinically significant differencebetween groups could
occur.
Although there was great variabilityin EMG activity, the mean
EMG activ-
ity of the superficial muscles wasalways higher for participants
withTMD pain compared with the con-trol group across all conditions
andmuscles (Fig. 2). However, the large
variability of the normalized EMGactivity across participants
andgroups did not lead to a finding ofstatistical significance.
The large variability seen in theEMG activity of the cervical
flexormuscles also has been observed in
other regions such as the low back.78
Hodges et al78 found that peopleresponded differently to
experimen-tal pain in the low back muscles.They reported that no 2
individualsshowed identical patterns ofincreased activity of the
low backmuscles when they underwentexperimental pain. If this
phenome-non were extrapolated to the cervi-cal spine, it could be
speculated thateach individual has a different mus-
cle activation strategy to adapt topain. The motor response in
the cer-
vical spine, especially in people withpain, would be an increase
of theactivity of the SCM and AS muscles;however other strategies,
using dif-ferent muscles not investigated inthis research, also
could be present.Further research investigating possi-ble cervical
motor strategies in peo-ple with TMD under different condi-tions
would help further clarify the
role of the cervical muscles in TMD.
Our study did not measure directlythe activity of the deep
cervicalflexor muscles because the tech-nique for measuring the
activity ofthe deep cervical muscles is invasiveand adherence to
the testing proto-col would have been impaired. Wemeasured the
superficial cervicalmuscles such as the SCM and AS onlyas an
indirect measure of impairment
of the activity of the deep cervicalflexor muscles. Thus, it is
still uncer-tain whether deep cervical muscleactivity was impaired
in thesepatients. In addition, because the
cervical spine is a very complex sys-tem characterized by a high
degreeof redundancy in the muscular sys-tem,36,79 it is not
surprising thatother motor strategies and musclesnot analyzed in
this study (other thanSCM and AS muscles) could be usedby people
with pain to stabilize thecervical spine.
The CCFT has become a gold stan-dard for isolating the
activation ofthe deep flexor muscles and identi-
fying possible co-contraction pat-terns of superficial muscles
in thecervical spine.63,75,80 Its construct
validity66,81 as well as its reliability67
have been established; however,other psychometric properties
suchas concurrent validity with clinical
variables such as neck disability andpain intensity of this test
need to beascertained. Thus, this study investi-gated the
associations between themuscular activity of the analyzed
muscles through the 5 stages of theCCFT and clinical variables
such asthe level of chronic pain grade clas-sification of TMD based
on theRDC/TMD, pain intensity, time ofcomplaint, jaw disability,
and neckdisability. Most of the associations
were positive but weak, indicatingthat the performance of the
CCFT isnot strongly related to other clinical
variables such as pain intensity, neckdisability, or jaw
disability. These
results are in agreement with thoseof Falla et al,82 who
reported thatreduction in pain in patients withneck pain after a
training program
was not accompanied by animprovement in performance of
thecervical flexor muscles. It appearsthat pain and physical
performanceof the craniocervical muscles repre-sent different
aspects of disability inpeople with cervical involvement.83
Thus, a more focused evaluation
Cervical Flexor Activity and Temporomandibular Disorders
1194 f Physical Therapy Volume 91 Number 8 August 2011
by guest on June 1, 2012http://ptjournal.apta.org/Downloaded
from
http://ptjournal.apta.org/http://ptjournal.apta.org/http://ptjournal.apta.org/http://ptjournal.apta.org/
-
7/31/2019 Phys Ther 2011 Armijo Olivo 1184 97
13/16
regarding disability and its relatedfactors in future research
is neededto understand the intricacies amongphysical impairments,
pain, anddisability.
Because of the variability of EMGactivity among groups and
condi-tions found in this study, an analysisof the clinical
relevance of theresults through the calculation ofeffect sizes was
conducted to evalu-ate the relevance of these findings.To our
knowledge, this is the firsttime that a study has evaluated
theclinical relevance of EMG activity.
According to Musselman,71 effectsize calculation is one of the
most
common ways to evaluate clinicalrelevance after the fact.71,84
Thelarger this effect size index, thelarger the difference
betweengroups and the larger the clinical rel-evance of the
results.71 It is recog-nized that effect sizes of 0.2, 0.5, and0.8
correspond to small, moderate,and large effects.73 Although there
isno known research that establishes acutoff of EMG activity
(percentage ofMVC) to be considered clinically rel-
evant when comparing the EMGactivity of different groups, it
hasbeen shown that EMG activity as lowas 2% to 5% of MVC can be
related topain in neck-shoulder areas.8587 Inaddition, a minimally
important dif-ference for EMG activity has beenfound to be 2.9% of
MVC.88
Although a large variability in theestimates of effect sizes was
presentin this data set (which had wide CIs),
based on the calculated mean effectsizes (ie, standardized mean
differ-ences ranging between 0.41 and0.66) and the raw mean
differencesobtained from the comparisons(ranging from 4.63% to
12.07% ofMVC), differences in EMG activity
were found in some of the compari-sons between patients with
TMDand the control group (Tab. 3). Thus,standardized effect sizes
and mini-mally important difference could
serve as an index to guide cliniciansin the relevance of the
findings. Itcould be said that in the absence ofknowledge and
guidelines to deter-mine the clinical relevance of certain
outcomes, calculation of the clinicalrelevance, based on the
distributionmethods, could be an option. Theseresults could be of
importance forclinicians who work in this fieldbecause this
analysis might indicatethat patients with TMD tended tohave
increased activity of the super-ficial cervical muscles
compared
with the control group. In addition,the results of the subgroup
analysisconsidering only patients with pureTMD provide more support
for these
findings. Furthermore, preliminaryevidence has shown that
exercisesaddressing these types of impair-ments (ie, training of
neck flexormuscles) as part of cervical spinetreatment in people
with TMDreduced pain and improved function(ie, increased pain-free
mouth open-ing) in patients with TMD, whichpotentially supports the
fact thatpatients with TMD could benefitfrom treatment of impaired
cervical
flexor muscles.89 Therefore, theseresults might be considered
whenevaluating and treating patients withTMD.
Nevertheless, it is necessary toimplement a randomized
controlledtrial that addresses these cervicalimpairments through
cervical flexorexercises in patients with TMDand test whether these
exercisesdecrease pain and improve function
and quality of life in patients withTMD. In this way, research
couldadvance clinical practice in this area.
LimitationsThe results obtained in this researchare applicable
for the group of indi-
viduals who participated in thisstudy under the protocols
used.They potentially could be applied topeople with TMD having
character-istics similar to those of the partici-
pants in this study. This limitationshould be taking into
consideration
when attempting to extrapolatethese results. In addition, it
must beacknowledged that because this
project was cross-sectional, a cause-and-effect relationship
between cervi-cal muscular impairment and TMDcannot be
established.
ConclusionsThere were no statistically signifi-cant differences
(P.07) in EMGactivity in the SCM or the AS musclesin patients with
mixed and myoge-nous TMD compared with individu-als who were
healthy when perform-ing the CCFT. However, the patients
with TMD tended to have increasedactivity of the superficial
cervicalmuscles compared with the controlgroup. This increased
activity of thesuperficial muscles of the cervicalspine might be
associated with theneck disturbances seen in patients
with TMD. This information maygive clinicians insight into the
impor-tance of evaluation and possibletreatment of the deep neck
flexorsin patients with TMD. However,
future research should test the effec-tiveness of this type of
programthrough a randomized controlledtrial in individuals with TMD
todetermine the real value of treatingthis type of impairment in
thispopulation.
Dr Armijo-Olivo, Dr Warren, Dr Major, andDr Magee provided
concept/idea/researchdesign. Dr Armijo-Olivo, Mr da Costa,
DrGadotti, Dr Major, Dr Thie, and Dr Mageeprovided writing. Dr
Armijo-Olivo, Mr Fuen-
tes, Mr da Costa, and Dr Gadotti provideddata collection. Dr
Armijo-Olivo and Dr War-ren provided data analysis. Dr
Armijo-Olivoand Dr Magee provided project manage-ment. Dr
Armijo-Olivo provided fund pro-curement. Dr Magee provided
facilities/equipment and institutional liaisons. DrArmijo-Olivo, Mr
Fuentes, Mr da Costa, DrGadotti, Dr Warren, Dr Major, Dr Thie,
andDr Magee provided consultation (includingreview of manuscript
before submission).
The authors thank all of the participants inthis study and
Darrel Goertzen, Luis Cam-
Cervical Flexor Activity and Temporomandibular Disorders
August 2011 Volume 91 Number 8 Physical Therapy f 1195
by guest on June 1, 2012http://ptjournal.apta.org/Downloaded
from
http://ptjournal.apta.org/http://ptjournal.apta.org/http://ptjournal.apta.org/http://ptjournal.apta.org/
-
7/31/2019 Phys Ther 2011 Armijo Olivo 1184 97
14/16
pos, and Rodrigo Guzman for their technicalassistance.
The study was approved by the Ethics Com-mittee of the
University of Alberta, Edmon-ton, Alberta, Canada.
This research was presented at the XVIIIInternational Conference
of the InternationalSociety of Electrophysiology and Kinesiol-ogy,
June 16 19, 2010, Aalborg, Denmark;the 5th International Conference
on Orofa-cial Pain and Temporomandibular Disorders,August 26 30,
2009, Praia do Forte, Bahia,Brazil; and the 13th World Conference
onPain, August 29September 2, 2010, Mon-treal, Quebec, Canada.
Dr Armijo-Olivo was supported by the Cana-dian Institutes of
Health Research (CIHR), theAlberta Provincial CIHR Training Program
inBone and Joint Health, an Izaak Walton Kil-lam Scholarship from
the University ofAlberta, and the Physiotherapy Foundationof Canada
through an Ann Collins WhitmoreMemorial Award.Mr Fuentes is
supportedbythe government of Chile (BECAS Chile Schol-arship
Program) and Catholic University ofMaule, Chile.
DOI: 10.2522/ptj.20100233
References1 De Leeuw R, ed. Orofacial Pain: Guide-
lines for Assessment, Diagnosis, andManagement. 4th ed. Chicago,
IL: Quin-tessence Publishing Co Inc; 2008:124.
2 McNeill C. Temporomandibular Disorders:Guidelines for
Classification, Assessment,and Management. Chicago, IL:
Quintes-sence Publishing Co Inc; 1993:1230.
3 Drangsholt M, LeResche L. Temporo-mandibular disorder pain.
In: Crombie I,Croft P, Linton S, et al, eds. Epidemiologyof Pain.
Seattle, WA: IASP Press; 1999:203233.
4 Von Korff M, Ormel J, Keefe FJ, DworkinSF. Grading the
severity of chronic pain.Pain. 1992;50:133149.
5 Von Korff M, Dworkin SF, Le Resche L,Kruger A. An
epidemiologic comparisonof pain complaints. Pain.
1988;32:173183.
6 Kino K, Sugisaki M, Haketa T, et al. Thecomparison between
pains, difficultiesin function, and associating factors ofpatients
in subtypes of temporomandibu-lar disorders. J Oral Rehabil.
2005;32:315325.
7 Robinson ME, Dannecker EA, George SZ,et al. Sex differences in
the associa-tions among psychological factors andpain report: a
novel psychophysical studyof patients with chronic low back pain.J
Pain. 2005;6:463470.
8 Dannecker EA, Hausenblas HA, KaminskiTW, Robinson ME. Sex
differences indelayed onset muscle pain. Clin J
Pain.2005;21:120126.
9 Robinson ME, George SZ, Dannecker EA,et al. Sex differences in
pain anchors re-
visited: further investigation of mostintense and common pain
events. Eur JPain. 2004;8:299305.
10 Robinson ME, Wise EA. Prior pain experi-ence: influence on
the observation of
experimental pain in men and women.J Pain. 2004;5:264269.
11 Robinson ME, Wise EA, Gagnon C, et al.Influences of gender
role and anxiety onsex differences in temporal summation ofpain. J
Pain. 2004;5:7782.
12 Robinson ME, Wise EA. Gender bias in theobservation of
experimental pain. Pain.2003;104:259264.
13 Myers CD, Riley JL III, Robinson ME. Psy-chosocial
contributions to sex-correlateddifferences in pain. Clin J Pain.
2003;19:225232.
14 Robinson ME, Gagnon CM, Riley JL III,Price DD. Altering
gender role expecta-tions: effects on pain tolerance,
painthreshold, and pain ratings. J Pain. 2003;
4:284288.15 de Wijer A, de Leeuw JR, Steenks MH,
Bosman F. Temporomandibular and cervi-cal spine disorders:
self-reported signs andsymptoms. Spine (Phila Pa 1976).
1996;21:16381646.
16 Gremillion HA. The prevalence and etiol-ogy of
temporomandibular disorders andorofacial pain. Texas Dent J.
2000;117:3039.
17 Nicolakis P, Nicolakis M, Piehslinger E,et al. Relationship
between craniomandib-ular disorders and poor posture.
Cranio.2000;18:106112.
18 Solow B, Sandham A. Cranio-cervical pos-ture: a factor in the
development and func-tion of the dentofacial structures. EurJ
Orthod. 2002;24:447456.
19 Armijo-Olivo S, Frugone R, Wahl F, GaeteJ. Clinic and
teleradiographic alterationsin patients with anterior disc
displace-ment with reduction. Kinesiologia. 2001;64:8287.
20 Braun BL. Postural differences betweenasymptomatic men and
women andcraniofacial pain patients. Arch Phys MedRehabil.
1991;72:653656.
21 Sonnesen L, Bakke M, Solow B. Temporo-mandibular disorders in
relation to cranio-facial dimensions, head posture and biteforce in
children selected for orthodontictreatment. Eur J Orthod.
2001;23:179192.
22 Fricton JR, Kroening R, Haley D, Siegert R.
Myofascial pain syndrome of the headand neck: a review of
clinical characteris-tics of 164 patients. Oral Surg Oral Med,Oral
Pathol. 1985;60:615623.
23 Simons D, Travell JC, Simons LS. Travell &Simons
Myofascial Pain and Dysfunc-tion: The Trigger Point Manual. Vol
1.2nd ed. Baltimore, MD: Williams &
Wilkins; 1999.
24 de Wijer A, de Leeuw JR, Steenks MH,Bosman F.
Temporomandibular and cervi-cal spine disorders: self-reported
signs andsymptoms. Spine (Phila Pa 1976). 1996;21:16381646.
25 Visscher CM, Lobbezoo F, de Boer W,et al. Prevalence of
cervical spinal painin craniomandibular pain patients. EurJ Oral
Sci. 2001;109:7680.
26 Fink M, Tschernitschek H, Stiesch-ScholzM. Asymptomatic
cervical spine dysfunc-tion (CSD) in patients with
internalderangement of the temporomandibular
joint. Cranio. 2002;20:192197.
27 de Wijer A, Steenks MH, de Leeuw JR,et al. Symptoms of the
cervical spine intemporomandibular and cervical spine dis-orders. J
Oral Rehabil. 1996;23:742750.
28 Hu JW, Sessle BJ, Amano N, Zhong G. Con-vergent afferent
input patterns in the med-ullary dorsal horn (trigeminal
subnucleuscaudalis): a basis for referred orofacialpain? Pain.
1984;18(suppl 2):S281.
29 Hu JW, Sessle BJ, Raboisson P, et al. Stim-ulation of
craniofacial muscle afferentsinduces prolonged facilitatory effects
intrigeminal nociceptive brain-stem neu-rones. Pain.
1992;48:5360.
30 Kerr FW. Central relationships of trigemi-
nal and cervical primary afferents in thespinal cord and
medulla. Brain Res. 1972;43:561572.
31 Sessle BJ, Hu JW, Amano N, Zhong G. Con-vergence of
cutaneous, tooth pulp, vis-ceral, neck and muscle afferents onto
noci-ceptive and non-nociceptive neurones intrigeminal subnucleus
caudalis (medul-lary dorsal horn) and its implications forreferred
pain. Pain. 1986;27:219235.
32 Sessle BJ. The neural basis of temporoman-dibular joint and
masticatory muscle pain.J Orofac Pain. 1999;13:238245.
33 Sessle BJ. Acute and chronic craniofacialpain: brainstem
mechanisms of nocicep-tive transmission and neuroplasticity,
andtheir clinical correlates. Crit Rev Oral BiolMed.
2000;11:5791.
34 Browne PA, Clark GT, Kuboki T, AdachiNY. Concurrent cervical
and craniofacialpain: a review of empiric and basic sci-ence
evidence. Oral Surg Oral Med OralPathol Oral Radiol Endod.
1998;86:633640.
35 Jull G, Falla D, Treleaven M, et al. A ther-apeutic exercise
approach for cervicaldisorders. In: Boyling J, Jull G, eds.Grieves
Modern Manual Therapy. Lon-don, United Kingdom: Churchill
Living-stone; 2004:451470.
36 Jull GA, Sterling M, Falla D, et al. Whip-lash, Headache, and
Neck Pain:Research-Based Directions for PhysicalTherapies.
Philadelphia, PA: Elsevier; 2008:4158.
37 Jull GA, OLeary SP, Falla DL. Clinicalassessment of the deep
cervical flexormuscles: the craniocervical flexion test.J
Manipulative Physiol Ther. 2008;31:525533.
38 Falla D, Farina D. Neuromuscular adap-tation in experimental
and clinical neckpain. J Electromyogr Kinesiol. 2008;18:255261.
39 Falla D, Jull G, Hodges P, Vicenzino B.An endurance-strength
training regime iseffective in reducing myoelectric manifes-tations
of cervical flexor muscle fatigue infemales with chronic neck pain.
Clin Neu-rophysiol. 2006;117:828837.
Cervical Flexor Activity and Temporomandibular Disorders
1196 f Physical Therapy Volume 91 Number 8 August 2011
by guest on June 1, 2012http://ptjournal.apta.org/Downloaded
from
http://ptjournal.apta.org/http://ptjournal.apta.org/http://ptjournal.apta.org/http://ptjournal.apta.org/
-
7/31/2019 Phys Ther 2011 Armijo Olivo 1184 97
15/16
40 Falla D, Jull G, Russell T, et al. Effect ofneck exercise on
sitting posture inpatients with chronic neck pain. PhysTher.
2007;87:408417.
41 Jull G, Trott P, Potter H, et al. A random-ized controlled
trial of exercise and manip-ulative therapy for cervicogenic
headache.Spine (Phila Pa 1976). 2002;27:18351843.
42 de Wijer A, Steenks MH, Bosman F, et al.Symptoms of the
stomatognathic systemin temporomandibular and cervical
spinedisorders.J Oral Rehabil. 1996;23:733741.
43 Stiesch-Scholz M, Fink M, TschernitschekH. Comorbidity of
internal derangementof the temporomandibular joint and
silentdysfunction of the cervical spine. J OralRehabil.
2003;30:386391.
44 McNeely ML, Armijo Olivo S, Magee DJ. Asystematic review of
physical therapyinterventions for temporomandibular dis-orders.
Phys Ther. 2006;86:710725.
45 Dworkin SF, LeResche L. Research diag-nostic criteria for
temporomandibular dis-orders: review, criteria, examinations
and
specifications, critique. J CraniomandibDisord.
1992;6:301355.
46 Stevens J, ed. Applied Multivariate Statis-tics for the
Social Sciences. 4th ed. Mah-
wah, NJ: Lawrence Erlbaum Associates;2002:492552.
47 Armijo Olivo S, Fuentes J, Major P, et al.The association
between neck disabilityand jaw disability. J Oral Rehabil. In
press.
48 Armijo Olivo S. Relationship between Cer-vical
Musculoskeletal Impairments andTemporomandibular Disorders:
Clinicaland Electromyographic Variables [thesis].Edmonton, Alberta,
Canada: Faculty of Reha-bilitation Medicine, University of
Alberta;2010.
49 Collins SL, Moore RA, McQuay HJ. The
visual analogue pain intensity scale: whatis moderate pain in
millimetres? Pain.1997;72:9597.
50 Fricton JR. TMJ and Craniofacial Pain:Diagnosis and
Management. St Louis,MO: Ishiyaku EuroAmerica; 1988:4647.
51 Fricton JR, Schiffman EL. Reliability of acraniomandibular
index. J Dent Res. 1986;65:13591364.
52 Fricton JR, Schiffman EL. The cranioman-dibular index:
validity. J Prosthet Dent.1987;58:222228.
53 Lobbezoo-Scholte AM, De Leeuw JR,Steenks MH, et al.
Diagnostic subgroupsof craniomandibular disorders, part I:
self-report data and clinical findings. J OrofacPain.
1995;9:2436.
54 de Wijer A, Lobbezoo-Scholte AM, SteenksMH, Bosman F.
Reliability of clinicalfindings in temporomandibular disorders.J
Orofac Pain. 1995;9:181191.
55 Conti PC, De Azevedo LR, De Souza NV,Ferreira FV. Pain
measurement in TMDpatients: evaluation of precision and
sen-sitivity of different scales. J Oral
Rehabil.2001;28:534539.
56 Koho P, Aho S, Watson P, Hurri H. Assess-ment of chronic pain
behaviour: reliabilityof the method and its relationship
withperceived disability, physical impairmentand function. J
Rehabil Med. 2001;33:128132.
57 Lundeberg T, Lund I, Dahlin L, et al. Reli-ability and
responsiveness of three differ-ent pain assessments. J Rehabil
Med.2001;33:279283.
58 McCarthy M Jr, Chang CH, Pickard AS,et al. Visual analog
scales for assessingsurgical pain. J Am Coll Surg. 2005;201:
245252.59 Vernon H. The Neck Disability Index:
state-of-the-art, 19912008. J Manipula-tive Physiol Ther.
2008;31:491502.
60 Vernon H, Mior S. The Neck DisabilityIndex: a study of
reliability and validity[erratum in: J Manipulative Physiol
Ther.1992;15(1)]. J Manipulative Physiol Ther.1991;14:409415.
61 Sugisaki M, Kino K, Yoshida N, et al.Development of a new
questionnaire toassess pain-related limitations of dailyfunctions
in Japanese patients with tem-poromandibular disorders.
CommunityDent Oral Epidemiol. 2005;33:384395.
62 Falla D, DallAlba P, Rainoldi A, et al. Loca-tion of
innervation zones of sternocleido-
mastoid and scalene muscles: a basis forclinical and research
electromyographyapplications. Clin Neurophysiol. 2002;113:5763.
63 Falla DL, Jull GA, Hodges PW. Patientswith neck pain
demonstrate reduced elec-tromyographic activity of the deep
cervi-cal flexor muscles during performance ofthe craniocervical
flexion test. Spine(Phila, Pa 1976). 2004;29:21082114.
64 Standards for reporting EMG data. J Elec-tromyogr Kinesiol.
1996;6:IIIIV.
65 Standards for reporting EMG data. J Elec-tromyogr Kinesiol.
1997;7:III.
66 Falla DL, Campbell CD, Fagan AE, et al.Relationship between
cranio-cervical flex-ion range of motion and pressure changeduring
the cranio-cervical flexion test.Man Ther. 2003;8:9296.
67 Falla D, Jull G, DallAlba P, et al. An elec-tromyographic
analysis of the deep cer-
vical flexor muscles in performance ofcraniocervical flexion.
Phys Ther. 2003;83:899906.
68 Jensen C, Westgaard RH. Functional sub-division of the upper
trapezius muscle dur-ing maximal isometric contractions. J
Elec-tromyogr Kinesiol. 1995;5:227237.
69 Plichta SB, Garzon LS. Statistics for Nurs-ing and Allied
Health. Philadelphia, PA:Lippincott Williams & Wilkins;
2009.
70 Munro BH. Statistical Methods for HealthCare Research.
Philadelphia, PA: Lippin-
cott Williams & Wilkins; 2005.71 Musselman KE. Clinical
significance test-
ing in rehabilitation research: what, why,and how? Phys Ther
Rev. 2007;12:287296.
72 Perera S, Mody SH, Woodman RC, Studen-ski SA. Meaningful
change and responsive-ness in common physical performancemeasures
in older adults. J Am GeriatrSoc. 2006;54:743749.
73 Cohen J. Statistical Power Analysis forthe Behavioral
Sciences. 2nd ed. Hillsdale,NJ: Academic Press Inc; 1988:117.
74 Jull G. Deep cervical flexor muscle dys-function in whiplash.
J MusculoskeletPain. 2000;8:143154.
75 Jull G, Kristjansson E, DallAlba P. Impair-ment in the
cervical flexors: a comparisonof whiplash and insidious onset neck
painpatients. Man Ther. 2004;9:8994.
76 Sterling M, Jull G, Wright A. The effect ofmusculoskeletal
pain on motor activityand control. J Pain. 2001;2:135145.
77 McNeely M, Warren S. Value of confidenceintervals in
determining clinical signifi-cance. Physiother Can.
2006;58:205211.
78 Hodges PW, Cholewicki J, CoppietersMW, MacDonald D. Trunk
muscle activityis increased during experimental backpain, but the
pattern varies between indi-
viduals. Presented at: Proceedings of theXVI Congress of the
International Societyof Electrophysiology and Kinesiology;
June 29 July1, 2006; Turino, Italy.
79 Winters J. Biomechanical modeling of thehuman head and neck.
In: Peterson B,Richmond FJ, eds. Control of Head Move-ment. New
York, NY: Oxford UniversityPress; 1988:2236.
80 Jull GA. Deep cervical flexor muscle dys-
function in whiplash. J MusculoskeletPain. 2000;8:143154.
81 Falla D, Jull G, OLeary S, DallAlba P. Fur-ther evaluation of
an EMG techniquefor assessment of the deep cervical flexormuscles.
J Electromyogr Kinesiol. 2006;16:621628.
82 Falla D, Jull G, Hodges P. Training the cer-vical muscles
with prescribed motor tasksdoes not change muscle activation
duringa functional activity. Man Ther. 2008;13:507512.
83 Denison E, Asenlof P, Lindberg P. Self-efficacy, fear
avoidance, and pain intensityas predictors of disability in
subacuteand chronic musculoskeletal pain patientsin primary health
care. Pain. 2004;111:
245252.84 Kirk RE. Practical significance: a concept
whose time has come. Educational Psycho-logical Measurement.
1996;56:746759.
85 Veiersted KB, Westergaard RH, AndersenP. Pattern of muscle
activity during stereo-typed work and its relation to muscle
pain.Int Arch Occup Environ Health. 1990;62:3141.
86 Jonsson B. The static load component inmuscle work. Eur J
Appl Physiol OccupPhysiol. 1988;57:305310.
87 Jensen BR, Schibye B, Sogaard K, et al.Shoulder muscle load
and muscle fatigueamong industrial sewing-machine opera-tors. Eur J
Appl Physiol Occup Physiol.1993;67:467475.
88 Armijo-Olivo S, Warren S, Fuentes J, MageeD. Clinical
relevance vs. statistical signifi-cance: using neck outcomes in
patients
with TMD as an example. Man Ther. Inpress.
89 La Touche R, Fernandez-de-las-Penas C,Fernandez-Carnero J, et
al. The effects ofmanual therapy and exercise directed atthe
cervical spine on pain and pressurepain sensitivity in patients
with myofas-cial temporomandibular disorders. J OralRehabil.
2009;36:644652.
Cervical Flexor Activity and Temporomandibular Disorders
August 2011 Volume 91 Number 8 Physical Therapy f 1197
by guest on June 1, 2012http://ptjournal.apta.org/Downloaded
from
http://ptjournal.apta.org/http://ptjournal.apta.org/http://ptjournal.apta.org/http://ptjournal.apta.org/
-
7/31/2019 Phys Ther 2011 Armijo Olivo 1184 97
16/16
doi: 10.2522/ptj.20100233
Originally published online June 9, 20112011; 91:1184-1197.PHYS
THER.
W. Major, Norman M.R. Thie and David J. MageePaulBruno R. da
Costa, Inae C. Gadotti, Sharon Warren,
Susan Armijo-Olivo, Rony Silvestre, Jorge Fuentes,Flexion Test:
A Cross-Sectional StudyDisorders While Performing the
CraniocervicalMuscles in Patients With
TemporomandibularElectromyographic Activity of the Cervical
Flexor
References
http://ptjournal.apta.org/content/91/8/1184#BIBLfor free at:This
article cites 73 articles, 7 of which you can access
InformationSubscription
http://ptjournal.apta.org/subscriptions/
Permissions and Reprints
http://ptjournal.apta.org/site/misc/terms.xhtml
Information for Authors
http://ptjournal.apta.org/site/misc/ifora.xhtml
http://ptjournal.apta.org/content/91/8/1184#BIBLhttp://ptjournal.apta.org/content/91/8/1184#BIBLhttp://ptjournal.apta.org/content/91/8/1184#BIBLhttp://ptjournal.apta.org/content/91/8/1184#BIBL