Embed Size (px)
Citation preview

17th Photonet National Meeting
On Thursday 23rd May 2019, the network hosted another successful annual meeting at Perth Royal In-firmary. The meeting was very well attended by around 80 people and the feedback we have received was extremely positive. It looks like the electronic feedback passed its test as we have received the ma-jority of the responses back! A short report is now available on Photonet website: (National Meeting Report)
August 2019 Newsletter
Photonet National Managed Clinical Network
Issue 1
Photonet Standards document has been up-dated and is now available on the Photonet website: www.photonet.scot.nhs.uk/professionals area/standards-protocols New guidance on photosensitising drugs and phototherapy has been launched at the National Meeting on 23 May and is now availa-ble on the Photonet website: www.photonet.scot.nhs.uk/professionals area/standards-protocols
Save the Date
The Photonet Annual Conference has been
scheduled to take place on
Thursday 21 May 2020 provisionally in
Perth Royal Infirmary
It’s never too early to mark your diaries!
Updated & New Guidance
‘Standardised’ Nurse Dermatology Education for Scotland and Ireland Hilary Nicholson and Dianne Ross featured in a recent ‘Nursing Times’ article as leads for three year transfor-mation pro-gramme. Follow-ing an initial scop-ing exercise a range of educa-tional tools are being developed for the 400 nurs-ing staff working in dermatology across Scotland and Ireland. Ms Ross and Ms Nicolson have also secured Scot-land’s first ever masters-level dermatology training programme that will be delivered from the Univer-sity of Stirling from September this year.

We have introduced Frequently
Asked Questions section -
please hover over Profession-
als tab to reveal this new part of
the website. If you or your col-
leagues have a questions that
requires professional input please do not hesi-
tate to get in touch ([email protected]) —
we will do our best to present the question to
the experts and publish it.
Photonet website update
Farewell to Kevin
Kevin Campbell, our Photonet Technician, has announced he will retire from his role in September 2019. Kevin has been valuable member of Photonet team since 2006 per-forming dosimetry measurements in photo-therapy units across Scotland. Following a tea & strawberry tarts farewell we wish Kevin a long and happy retirement.
Magali Redding the Eczema Outreach Support
CEO presented at the National Meeting for Pho-
tonet on the 23 May. We have received a lot of
positive feedback with staff confidently recom-
mending this organisation to patients and their
families struggling with eczema. The organisa-
tion offers wide range of materials/advice and
help to schools, breakfast clubs, healthcare staff / families. For more information
please go to www.eos.org.uk / Twitter @EczemaOutreach
Treating Children
Following number of requests
from the delegates of National
Meeting we have asked speak-
ers and workshop facilitators to
publish their presentations. You
can now find them on Events
tab of the website: www.photonet.scot.nhs.uk/
events
Ref: Eczema Outreach Support
Dr Eadie accepting an invitation to speak at Eczema Outreach Support’s family day on 16 March where he took the opportunity to raise awareness about UV phototherapy as an avail-able treatment option for severe eczema and answer questions from delegates. REMINDER: Guidelines on treating children are available on the website: Guidance for Derma-tology Ultraviolet Phototherapy and Pho-tochemotherapy for Children
Photonet National Meeting-Powerpoint Presentations NEW!

Get involved
Further details can be found on the
Photonet website:
Or contact us at: Mhairi Gallacher-Photonet Programme Manager Aneta Gorczynski-Programme Support Officer
www.photonet.scot.nhs.uk
Photonet Dashboard has been live for some time now and has recently received a new look.
All Photosys users should have received an email from the NHS NSS IT with instructions how to access the system. If you are not sure—please search your email for ‘Directory Information Service’ If you can’t remember your password—please get in touch with NHS NSS IT department directly on 0131 275 7777 or [email protected] When phoning—please ask for ‘LDAP password for Tableau’ - if you ask for a password to Photonet Dashboard—they might not know how to direct your call as there are number of Dashboards out there! Here is direct link to the system:
https://login.nhsnss.scot.nhs.uk/ If you would like to gain the access to the Photonet
dashboard please get in touch with Photonet Network Office providing: name & designation, unit & health board: [email protected] You can find Dashboard user guide on Photonet
website: www.photonet.scot.nhs.uk/ pho-tonet-dashboard
Photonet Dashboard—New pages added
In the near future we are hoping to include visuali-sation of Patient Experience Questionnaire re-turns within the dashboard. A project is also underway to produce short treat-ment centre outcome reports with the plan to provide 2019/20 reports in the new format.
Logging in & passwords
User guide
New access
Future plans
2018/19 Self Audit Outcomes now available for review
The audit returns for 2018/19 have been published in newly developed pages on the dashboard. PLEASE NOTE THAT 2018/19 AUDIT REPORTS WILL NOT THEREFORE BE CIRCULATED HOW-EVER OUTCOMES AGAINST STANDARDS ARE AVAILABLE TO VIEW WITHIN THE DASH-BOARD.

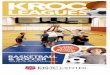
Since whole body phototherapy machines have bulbs on 4 sides, does that prevent any shadows that would usually be caused by one sided light? (Dr Ewan Eadie, Photonet Lead Clinician, Head of Scientific Services for Photobiology) Whole body phototherapy cabinets, as typically found in phototherapy centres, have long fluores-cent tubes which fully surround the person inside the cabinet. The purpose is to illuminate all body surfaces of the cabinet occupant at once, although there will still be shadows where the light cannot reach (see image below from Diffey BL, Harrington TR,Challoner AV. A comparison of the anatomi-cal uniformity of irradiation in two different photochemotherapy units. Br J Dermatol 1978; 99:361–3 and Moseley, H. et al. (2015), Guidelines on the measurement of ultraviolet radiation levels in ul-traviolet phototherapy: report issued by the British Association of Dermatologists and British Photo-dermatology Group 2015. Br J Dermatol, 173: 333-350. doi:10.1111/bjd.13937). A single flat bank of tubes can only treat one side of the body surface at a time, in other words when the front is being treated the back (and to a cer-tain extent the sides of the body) are in shadow. Howev-er this is overcome in one-sided light sources by repeat-ing the treatment with the pa-tient rotated. Therefore if you assume the body has four surfaces (front, back, left side and right side) the treatment would be repeated four times with a different side facing the tubes each time. This means that a single side of tubes would take four times as long to deliver the treatment as a full body cabinet. Sometimes a single side of tubes is appropriate and such systems are used in the Western Isles, for self-administration in Arbroath and in the home phototherapy ser-vice delivered by NHS Tay-side. These systems are more compact, can be easily moved and stored and are much cheaper than a full phototherapy cabinet. Therefore both types of system have their pros and cons, it depends upon the needs of the phototherapy provider.
At the Photonet National Meeting on 23 May 2019 we unfortu-nately ran out of time to consider the questions submitted for the ‘Ask the expert’ session at the end of the day. As promised we have collated answers to all the questions sub-mitted prior to the event via Mentimeter and also via postcards during the day. Please find the feedback below:

Why are ceiling tiles above some cabinets white and some are black? (Dr Ewan Eadie, Photonet Lead Clinician, Head of Scientific Services for Photobiology) Whole-body phototherapy cabinets are completely enclosed - except at the top where they are open to the surrounding room. This means that some ultraviolet radiation (UVR) from the photo-therapy cabinet exits from the top, reflects off the ceiling and back down towards the floor. The po-tential concern is that the UVR that has reflected from the ceiling is then exposing staff and / or members of the public. The amount of UVR that is reflected from the ceiling will depend upon a number of factors including the height of the ceiling above the cabinet and the material that the ceil-ing is made from. Local Medical Physics departments carry out regular measurements and risk assessment to deter-mine if the reflected UVR is a hazard. They compare their measurements to values which are set down in law. If their measurements indicate that there is a potential hazard then they will take steps to further reduce the reflected light or the staff exposure. One such step might be to paint the ceil-ing tiles black on the assumption or knowledge that a particular black paint reflects less UVR than the white tile. However different black paints reflect different amounts of UVR so it is important to choose the paint carefully. There are a number of other steps that can be taken to reduce UVR exposure of staff - for exam-ple, creating a curtained zone around the cabinet. The curtain, as well as being useful for priva-cy, acts as a barrier to the UVR. If Risk Assessed appropriately, the area within the curtain will have higher levels of UVR exposure and staff should minimise their time in this area. Outwith the curtain area there would be no restrictions. Details of the control measures that have been put in place for your local therapy unit will be availa-ble in the Risk Assessment and Local Rules, copies of which can be obtained from your local Medi-cal Physics.
UVB for PLE. How many courses are recommended? Should it be continuous annually or a break? (Dr Alastair Kerr, Consultant Dermatologist, NHS GGC) Some units may have a feeling that they have accumulated a cohort of patients that have been re-ceiving PLE desensitisation for some number of years “automatically.” This can have an effect on the equity of service provision, whereby continuing such a pattern means phototherapy resources may be reduced for other patients who would also merit phototherapy for their skin condition. Broaching this issue with such patients may require sensitive discussion in parallel with clinical judgement on their current PLE severity. It can be explained that desensitisation should not routinely be offered to patients with mild PLE to allow them to subsequently “sunbathe” on holiday. Instead, it should be reserved for more severe cases, to allow incident sunlight exposure via everyday activities on subsequent holidays. For many patients, PLE naturally improves with time. Therefore, it could be recommended that a “gap year” be trialled after every 4 years of treatment, where no desensitisation course is given. In around half of cases, patients may find the condition has improved and desensitisation is not required in subsequent years.

What advice should we be giving patients regarding the use of sunscreen on day of phototherapy treatment / prior to treatment?
(Dr Alastair Kerr, Consultant Dermatologist, NHS GGC) For most patients, using sunscreens on large areas of the body on the day of phototherapy, prior to UV exposure would not be standard practice and should be avoided. One main issue is that it would effectively reduce the effectiveness of the UV exposure and consequently the clinical improvement. However, another potentially greater risk could occur whereby the same area was not covered in a similar amount of the same sunscreen prior to a subsequent exposure and then developed erythema as it had not been subject to an incremental exposure. The setting where sunscreen is sometimes used prior to UV exposure is that of herpes labialis (“Cold sores”) being triggered by UV exposure. In some patients who are prone to this (they may have had it previously on earlier phototherapy courses) nursing staff may apply a high factor sunscreen to the ar-ea around the mouth/nose prior to exposure at each visit. If this is continued for a number of expo-sures, the nurse and patient have to be careful to ensure the same sunscreen is applied to the same area of the face each time. In some cases, if the rest of the face may benefit from UV exposure, a face mask is not used until fur-ther in to the course, or possibly not at all during the course. However, if the face has no significant skin condition areas that require treatment, a decision may be made at the start or early on in the course to use a face mask at that point and not use any sunscreen around the mouth/lips. (Antonia Dailly, Phototherapy Nurse, NHS Lothian) General advice to ALL patients- whether they are having PUVA, UVB, to whole body or to just hands and feet is to cover up before treatment- and in the case of PUVA patients, for 24 hours after taking psoralen. In practice we would therefore suggest long sleeves, hats and sunglasses, and long trousers or skirts. We do advise that post UVB treatment, sun cream can be applied to any exposed areas- but recommend at least 4* or 5* and using a higher SPF than the individual would normally use- and for PUVA patients, to cover up for 24 hours. In regards to the use of sun cream to reduce risk of herpes labialis, we usually ask the patient to apply their own sun cream to the (potentially) affected area (unless they are unable to manage this- a VERY rare situation). By asking the patient to apply their own cream allows a greater consistency in application as there are 11 nurses working various shifts in this department, so getting treated by the same nurse for an entire course is extremely unlikely.
When a patient uses a visor, why do we need to input on the database how many treatments they have used it for? e.g. 11/30 (Lynn Fullerton, Senior Clinical Technologist, NHS Tayside) We only have to input a ‘Yes’ or ‘No’ value into Photosys in regards to if the patient has used a face visor or not. If they have used it for more than half of the treatment course, we would respond ‘Yes’. If they have used it for less than half the treatments in a course, then respond ‘No’. It is helpful to add in the free text section how many treatments the mask has been used for however not essential. This is something perhaps some centres have been asked to collate however in Tayside we only use the Y/ N option.

When do we expect to go over to National Services Scotland for registering all patient discharges? (Mhairi Gallacher, Photonet Programme Manager) There have been various delays in taking this project forward, including issues experienced as a result of User Acceptance Testing and the late decision to include CHI linkage within Phase 1 of the project. NSS IT and the Photonet Programme Manager are prioritising the project and the delays have been raised as a risk with the NSD Senior Management Team. Although Phase 1 of the project is well underway there remains the require-ment for Phase 2 (which includes a number of long awaited important changes) to be fully costed to allow these developments to be made. It is planned that system will be relocated to National Services Scotland by the end of November 2019. When inputting into the database, the dropdown menu for moisturisers does not include many of the newer creams / ointments - how can we get the list updated? (Mhairi Gallacher, Photonet Programme Manager) Currently if the treatment used is not in the drop down list there is not an option to enter the topical treatment as free text. This is a change which we have requested to the system. In the meantime the list will be updated to include some newer creams and ointments. If a patient has skin type V and is receiving hand and foot PUVA, would you limit the dose? And what about UVB? (Dr Robert Dawe, Consultant Dermatologist, NHS Tayside) Not necessarily. The top dose (for both UVB and for PUVA) is set as what is practicable, considering reasona-ble times for patients and also to ensure adequate throughput of patients (if one patient has very high doses, corresponding to long treatment times, fewer other patients can be treated so, depending on the unit, possibly lengthening waiting times to start treatment). Most centres consider about 15 minutes (some take 10 minutes) as the maximum reasonable time for a treatment with either UVA, to activate the psoralen in PUVA, or for UVB. There is flexibility – if for an individual increasing the dose further seems a good idea (perhaps that patient has benefitted from higher doses before) then if the patient is comfortable with longer times and the unit can offer this a higher top dose is reasonable. No studies have compared different policies regarding top doses. What is the etymology of 'psor' in psoriasis and psoralen? (Dr Robert Dawe, Consultant Dermatologist, NHS Tayside) In psoriasis it comes from an initially ancient Greek word for itch (transliterated as “psor”) that was then bor-rowed by Latin and is now used in ‘psoriasis’ in many languages including English. So, the term emphasises the importance of itch for many with psoriasis: many doctors have been taught that itch is perhaps not such a prob-lem in psoriasis (as in undergraduate medical training often atopic eczema and psoriasis, as two common der-matoses, are compared and contrasted and atopic eczema is, on average, even more itchy). It is important that itch is often severe in psoriasis. The etymology is likely different for the ‘psor’ of psoralen with the scientific name of a common leguminous plant source of psoralens being Psoralea corylifolium and this probably being from Greek ‘psoraleos’ meaning rough-ly scabby referring to some of the appearance of this plant which also has leaves (‘folia’) a bit like those of the Hazelnut tree (genus Corylus). Another ‘psor’ that can cause confusion is that in “Psoracomb” – these are small devices, usually fitted with UVB lamps, often used to treat localised psoriasis (although there are many other indications such as vitiligo and peristomal dermatitis). Here the ‘psor’ refers to psoriasis not to psoralen. What cleaning protocols do other phototherapy units in Scotland follow after treating patients in their cabinets? I.e. Do you hoover between every patient? If you wish to find out more about the cleaning of phototherapy equipment please get in touch with the network office as there is too much information to include within the newsletter.
When to stop pro topic before UV exposure? (Dr Robert Dawe, Consultant Dermatologist, NHS Tayside) Generally, at least 24 hours (and ideally a few days) before starting a course of ultraviolet (UV) treatment. The main issue is that tacrolimus (“Protopic” is tacrolimus ointment) immunosuppression might when combined with ultraviolet DNA damage increase skin cancer risks. It is not directly photosensitising. Most on oral tacrolimus (after transplants) start to get skin cancers on exposed sites about 5 years after transplantation. The amount of tacrolimus in the skin can be just as great or higher with ointment as with tablet tacrolimus so when tacrolimus ointment first became more readily available (before “Protopic” was introduced it had to be made up specially) there was a major concern about skin cancer risks with it, especially if combined with ultravi-olet. However, 1) people who have had transplants usually take other immunosuppressives in combination and 2) they are on it all the time without any breaks (whereas most using Tacrolimus ointment don’t use it all the time without any breaks). Now, some years on since “Protopic” became available, it is reassuring that there has not been an epidemic of tacrolimus ointment skin cancers. Several now deliberately combine tacrolimus ointment and UVB for vitiligo. Most are still wary of this combination because of the theoretical risks and because there usually is no major extra benefit. As a precaution it is still usual to avoid deliberately combining tacrolimus ointment and ultraviolet. How long a gap there should be is arguable, but the elimination half-life of oral tacrolimus (duration of effect in the skin when applied as an ointment has not been well studied) is 12 hours. It seems likely that it will not be exerting a strong immunosuppressive effect after 24 hours of application to the skin. How do we communicate risk to patients so as not to underplay the increased risk of skin cancer from photochemotherapy but also not to induce anxiety by overplaying the relatively low risk? (Prof Chris Bundy, Professor Behaviour Medicine, University of Cardiff) We know that the way information is presented can influence adherence especially if it contains something ac-tive that the person is capable of, knows why they need to do it and is willing to do to benefit themselves. My advice is to use a 4 step approach:
1. First ask what if anything they know about the links (risks) and then…..
2. Be honest and open about what is known, ask permission by saying “can I share with you what we do know and what we are not so sure about / the studies have not shown yet?” 3. Then ‘frame’ the information: gain frame v loss frame and positive v negative (usually behaviour that you or the patient can use),
A couple of examples “We know the likelihood of you having benefit from phototherapy is very high if you attend for all of the appointments, think of it as a medicine, when taken as prescribed it works (this is gain framed and posi-tive)” v “If you don’t come for all of your phototherapy appointments you won’t get the full benefit of treatment” (loss and negative) “Unfortunately there is a risk of skin cancer from light treatment (negative and loss (ie passive, nothing can be done) but we will keep an eye on you to ensure the risk is reduced” v “Light therapy is an effec-tive treatment for (skin condition) (gain frame), any increased risk of skin cancer comes from long-term use of light treatment. Your risk is reduced as we have calculated the dose carefully and by coming to every session (active behaviour) we can monitor you regularly” Use numbers if you need to, but people in general are not good with percentages so 5 out of 10 as op-posed to 50%. Last but not least, give absolute risk not relative risk – “There is an XX % increase in heart disease from drinking 1.5 L of coffee per day” v “…..for someone like you who drinks one cup a day this means an increased risk of 1 in XXXXXX thousand”
4. Finish by asking “what do you make of what I just told you?” i.e. check what they have understood. If you suspect a person doesn’t quite understand ask them to tell you what they would say to a friend, family member or the bloke in the pub who asks the question.