Embed Size (px)
Citation preview

Original article
Progressive neuropsychiatric manifestations ofphenylketonuria in adulthood
Phenylcetonurie progressant a l’age adulte : manifestationsneurologiques et modalites evolutives
L. Daelman a,b, F. Sedel c,d, A. Tourbah a,*,b,e
aDepartment of Neurology, CHU de Reims, 45, rue Cognacq-Jay, 51100 Reims, FrancebURCA, UFR Medecine, 45, rue Cognacq-Jay, 51100 Reims, FrancecDepartment of Neurology, Neurometabolic Unit and Reference Center for Lysosomal Diseases, Salpetriere Hospital,
47-83, boulevard de l’Hopital, 75651 Paris cedex 13, FrancedGroupe de recherche en neurometabolisme (GRC13), Universite Pierre-et-Marie-Curie, 4, place Jussieu, 75005 Paris,
FranceeEA 2027 LPN, UFR psychologie, Universite Paris VIII, 2, rue de la Liberte, 93526 Saint-Denis cedex, France
r e v u e n e u r o l o g i q u e 1 7 0 ( 2 0 1 4 ) 2 8 0 – 2 8 7
i n f o a r t i c l e
Article history:
Received 14 May 2013
Received in revised form
14 August 2013
Accepted 13 September 2013
Available online 13 April 2014
Keywords:
Phenynylketonuria
MRI
Leukoencephalopathy
Paraparesis
Mots cles :
Phenylcetonurie
IRM
Leucoencephalopathie
Paraparesie spastique
a b s t r a c t
Introduction. – Neuropsychiatric signs and MRI abnormalities can occur in patients with
phenylketonuria in adulthood. We describe clinical and radiological features of phenylke-
tonuric patients and we discuss the advantage of continuing diet in adulthood.
Method. – We report late onset neuropsychiatric symptoms of four phenylketonuric
patients (33–45 years) diagnosed in infancy and report the case of a patient (33 years)
diagnosed with phenylketonuria because of late onset neurological signs. We describe
clinical and radiological features of these 5 patients, and their evolution under diet and
propose a review of the literature.
Results. – The main neurological abnormalities in phenylketonuric patients diagnosed in
infancy are: brisk reflexes, spastic paraparesis, psychiatric signs that appear 10.5 years after
the diet arrest. A leukoencephalopathy was present in 93% of cases and 91.7% improve
clinically after poor phenylalanine diet reintroduction. In 4 patients, neurological abnor-
malities (spastic paraparesis, dementia, Parkinsonism) led to the late diagnosis. Two of
them had a leukoencephalopathy on brain MRI. Patients had high levels of phenylalanine
(above 1500 mmol/L) when neuropsychiatric signs occurred. Improvement after diet sug-
gests that hyperphenylalaninemia has a direct toxic effect on the brain.
Discussion/Conclusion. – The long-term follow-up of phenylketonuric patients is mandatory
to depict and treat neurological complications in time. Diet reintroduction is efficacious in
most cases.
# 2014 Published by Elsevier Masson SAS.
* Corresponding author.E-mail addresses: [email protected], [email protected] (A. Tourbah).
Available online at
ScienceDirectwww.sciencedirect.com
http://dx.doi.org/10.1016/j.neurol.2013.09.0120035-3787/# 2014 Published by Elsevier Masson SAS.

1. Introduction� articles published in French or English;
� patients with clear neurological or psychiatric syndromes,
excluding patients with minor cognitive abnormalities only;
r e s u m e
Introduction. – La phenylcetonurie peut entraıner a l’age adulte des troubles neuropsychia-
triques et des anomalies a l’IRM cerebrale. Nous decrivons l’evolution des manifestations
cliniques et IRM de patients phenylcetonuriques.
Methode. – Etude de cas et revue de la litterature. Nous rapportons les manifestations
neuropsychiatriques tardives de 5 patients phenylcetonuriques et nous presentons une
revue de la litterature.
Resultats. – Les sympto mes neurologiques chez les phenylcetonuriques connus apparais-
sent en moyenne 10,5 ans apres la suspension du regime. Une leucoencephalopathie est
presente dans 93 % des cas. Lors de l’apparition des troubles, les patients ont une hyper-
phenylalaninemie elevee. Apres reprise du regime, une amelioration clinique est constatee
dans 91,7 % des cas suggerant un effet toxique direct de la phenylalanine.
Discussion/Conclusion. – La surveillance de la phenylalaninemie a l’age adulte permettrait
d’eviter les complications neuropsychiatriques grace a la reprise du regime.
# 2014 Publie par Elsevier Masson SAS.
r e v u e n e u r o l o g i q u e 1 7 0 ( 2 0 1 4 ) 2 8 0 – 2 8 7 281
Phenylketonuria (PKU) is an autosomal recessive genetic
disorder characterized by a deficiency in the hepatic enzyme
phenylalanine hydroxylase (PAH). Incidence is about 1:10,000
in Europe [1]. The level of phenylalaninemia correlates with
the prognosis, as patients with moderate hyperphenylanani-
nemia (180–600 mmol/L) usually remain asymptomatic whe-
reas untreated patients with classical PKU (Phe > 1200 mg/dL),
will suffer from neurological or psychiatric disorders (mental
retardation, behavioural problems, epilepsy, movement dis-
orders, or spasticity) [2]. Postnatal screening diagnosis
followed by early treatment with a Phe free diet results in a
nearly normal cognitive development [2]. Treatment guide-
lines vary among countries. In France, it is recommended to
maintain Phe between 120 and 300 mmol/L until 10–11 years of
age then below 900 mmol/L until the end of school age and then
below 1200 mmol/L in adulthood [3]. Many patients show white
matter abnormalities on brain MRI. These abnormalities are
not correlated to intellectual or neurological signs and can be
reversible after reintroduction of the diet [4]. A very small
proportion of adolescent and adult patients will develop frank
neurological symptoms that may improve under dietary
treatment [5]. In addition, very few publications reported
the cases of adult patients that escaped neonatal screening
and remained poorly symptomatic until neurological symp-
toms progressed in adulthood. Here, we took advantage of 5
personal cases and of a literature review to delineate the
neuropsychiatric signs observed in adults with PKU.
2. Methods
Five patients were referred to the Adult Neurometabolic Unit,
Ho pital de la Salpetriere for adult-onset neurological or
psychiatric symptoms in the context of PKU. A literature
review was performed, using the Pubmed database and the
authors own bibliography to gather previous published cases.
Inclusion criteria were:
� age at onset of neuropsychiatric signs after 15 years old;
� neuropsychiatric signs not explained by other causes.
3. Description of our cases
3.1. Patient 1
A man, aged 32 years, was evaluated for a 2 years history of
slowly progressive spastic paraparesis. He was diagnosed with
PKU by neonatal screening and low Phe diet was introduced at
1 month (see Table 1 for a summary). Observance of the diet
was reported to be non-optimal with poor metabolic control
during infancy and childhood. He walked at 16 months and
spoke at 2 years. He went in a specialised school, but he never
learned to read or to write. He totally stopped the diet at
30 years. Clinical examination at 32 revealed a marked low
limbs pyramidal syndrome with spastic gait. Brain MRI
disclosed a leukoencephalopathy involving the posterior
and periventricular white matter. A poor Phe diet was then
introduced leading to disappearance of the spasticity and
normalisation of the gait while brain MRI remained unchan-
ged. Follow-up during the next years revealed that high Phe
values above 900 mmol/L were associated with reappearance
of the spastic gait and that strict Phe control below this range
was associated with gait normalization.
3.2. Patient 2
This woman was aged 38 when she was evaluated for
psychiatric symptoms. She was diagnosed with PKU at 10 days
of age through neonatal screening. The patient was abando-
ned by her parents and lived in an institution until she was
adopted at the age of 6 years. A low Phe diet was introduced
from 1.5 months to 4.5 years old and interrupted thereafter.
The metabolic control in infancy and childhood is difficult to
evaluate but was probably bad, as Phe was measured once at
2650 mmol/L when she was 5 years old. Walking and speaking

Table 1 – Literature data: PKU patients diagnosed during infancy and our patients 1 to 4.
Patients Sex Phe levels ondiet duringinfancy (mmol/L)
Age at dietonset (m)
Age at dietarrest (y)
Age at onsetof neurologicalworsening (y)
Phe at neurologicaldeterioration(mmol/L)
Improvement withreintroduction ofthe diet
Phe withre-institutionof the diet(mmol/L)
Genetics
Villasana et al. M NA 36 12 28 1660 + 217 NA
M NA Neonat 6 18 1640 + NA NA
McCombe et al. M 893–1200 0.5 18 19 1900 + 1760–2410 Haplotype 2
Wood et al. M 120–480 10 14 15 1600 + 340 NA
Thompson et al. M NA 1.75 16 20 1334 + NA NA
M 60–1100 1.5 18 16 NA No diet No diet NA
M 180–1600 0.25 19 19 NA No diet No diet NA
M NA 36 7 25 1386 – 180 NA
F 330–1400 15 7 20 1533 + NA NA
F 180–1000 18 7 15 NA + NA NA
Evans et al. F 180–360 24 13 33 590 NA NA NA
Patient 1 M 790–1520 1 30 30 1200 + 670–1360 NA
Patient 2 F NA 1.5 4.5 16 2000 + 750–1540 NA
Patient 3 F NA 42 7 40 NA + NA NA
Patient 4 F NA 1 5 26 1380 + 60–480 NA
Patients Leukoen-cephalopathy
Brisk reflexes Spastic paraparesis Tremor Psychiatric signs Epilepsy Dystonia Ataxia Parkinsonism IQ
Villasana et al. + + + + – + – – – Mental retardation
+ – – + + – – – – 81
McCombe et al. + + + – + – – – – 88
Wood et al. NA + + + + + – – – 59
Thompson et al. 5/6 + + – + – – – – Mental retardation
+ – + + + – – – 64
+ + – – – – + – 61
+ + + – – + – – 95
+ + – – – – – – 45
+ + + – – + – – 45
Evans et al. + + – + – – – – + NA
Patient 1 + + + – – – – – – Mental retardation
Patient 2 + + – – + – – – – 53
Patient 3 + – – – + – – – – Mental retardation
Patient 4 + – – + + – – – – NA
r e
v u
e n
e u
r o
l o
g i
q u
e 1
7 0
(
2 0
1 4
) 2
8 0
– 2
8 7
28
2

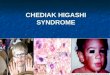
Fig. 1 – FLAIR sequences, axial plane. a: patient 2: leukoencephalopathy appearing as a mild hyperintensity, involving
posterior areas, both centrum semi-oval and outlining the splenium of corpus callosum; b and c: patient 3:
leukoencephalopathy involving frontal, parieto-occipital areas and both centrum semi-oval before diet (b); decrease of
hypersignal intensity, 6 months after diet reintroduction, with persistence in optic radiations (c).
r e v u e n e u r o l o g i q u e 1 7 0 ( 2 0 1 4 ) 2 8 0 – 2 8 7 283
were delayed (IQ around 50 at 7 years). In late teens, she
started to develop psychotic symptoms including auditory
hallucinations, interpretative thoughts, and hypochondriac
complaints. These psychiatric symptoms remained during the
following years, leading to social and familial withdrawal.
Neurological examination showed brisk reflexes and a left
Babinski’s sign. Brain MRI disclosed a mild posterior leukoen-
cephalopathy (Fig. 1a). Introduction of a low Phe diet was
followed by a marked improvement of psychiatric symptoms
with disappearance of hallucinations within few months.
3.3. Patient 3
This woman started to suffer from attention deficits and
psychiatric problems including marked irritability and anxiety
when she was 40 years old. She had been diagnosed with PKU
at 3.5 years of age when investigated for severe walking and
speech delay. A low phenylalanine diet was introduced from
3.5 to 7 years and interrupted thereafter. She started walking
at 5 years, and learned to write and read in a specialised
school. At 41 years old, neurological examination was normal,

Table 2 – Literature data: patients with diagnosis in adulthood and our patient 5.
Sex Age at onsetof neurologicalworsening
Age atdiagnosis(y)
Phe atdiagnosis(mmol/L)
Briskreflexes
Spasticparaparesis
Leukoence-phalopathy
Dementia Tremor
Kasim et al. F 53 57 2153 + + – + –
Weglage et al. F 45 45 882 + + + + +
Jousserand et al. M 54 55 1140 + + + – –
Patient 5 F 33 47 2358 – – – – +
Parkinsonism Epilepsy Ataxia IQ Diet Phe on diet(mmol/L)
Improvementwith diet
Genetic
Kasim et al. – – – 108 Protein
restricted
diet
NA + R158Q/IVS12+g>a
Weglage et al. – – + 95 + 240 + R408W/R68S
Jousserand et al. – – – Mental
retardation
Protein
restricted
diet
NA NA I65T/R252W
Patient 5 + + – Mental
retardation
No diet – – IVS4+5G>T/p.P281L
r e v u e n e u r o l o g i q u e 1 7 0 ( 2 0 1 4 ) 2 8 0 – 2 8 7284
but intelligence was low. Brain MRI showed a periventricular
and posterior leukoencephalopathy. A poor Phe diet was re-
introduced resulting in marked improvement of anxiety and
attention difficulties.
3.4. Patient 4
This woman noted at the age of 26, walking difficulties,
anxiety and depression leading her to stop working. She was
diagnosed with PKU after neonatal screening and started a
poor Phe diet at 1 month with good metabolic control then
stopped the diet at 5 years. She attended normal school with
some difficulties in reading and arithmetic. In her late teens,
she developed lupus erythematosous and cutaneous sclero-
dermia. Although neurological examination was considered
normal, a brain MRI showed a severe periventricular leu-
koencephalopathy (Fig. 1b). A poor Phe diet was re-introduced
with complete disappearance of the leukoencephalopathy
(Fig. 1c) and psychiatric symptoms. A mild ataxia remained.
3.5. Patient 5
This 47-year-old woman of Iranian origin presented with a 14-
year history of Parkinsonism. She exhibited speech delay
(7 years) and went in a specialized school. She experienced
two epileptic seizures at 10 years. When she was 33 years, she
noticed a rest upper limbs tremor. Examination revealed
rigidity and akinesia. Parkinson’s disease was suspected with
a dramatic response to levodopa. After 14 years of evolution,
the UPDRS III score was 47 during the ‘‘off’’ state but levodopa
responsiveness was still excellent without obvious dyskinesia.
A metabolic workup was performed because of the association
of mental retardation with early onset Parkinsonism. Ami-
noacids chromatography showed high serum Phe levels
(39.3 mg/dL, 2370 mmol/L). DaTSCAN imaging showed a loss
in dopaminergic terminals predominating on the right side.
Levels of neurotransmitter metabolites in CSF were low
(5HIAA at 27 nM, N = 66–141; HVA at 85 nM, N = 115–488)
whereas neopterins and biopterins were normal. Molecular
genetic studies revealed mutations in the PAH gene. Since
Parkinsonism was well equilibrated with levodopa, no specific
diet was introduced.
4. Literature review and compilation of data
Only 14 cases of PKU patients with late onset neuropsychiatric
manifestations were found during our literature survey [5–12].
These cases are summarized in Tables 1 and 2.
In 11 cases, PKU was diagnosed and treated in infancy or
childhood but neuropsychiatric manifestations appeared in
adulthood [5–8,11]. Characteristics of these 11 patients and of
our 4 patients diagnosed in childhood are pooled in Table 1.
Overall, there were 9 men and 6 women. Most patients were
diagnosed with newborn screening. The genotype was not
available for most of them. Seven patients were diagnosed
because of psychomotor delay (Patient 3, Wood, Villasana-
patient 1, Evans, Thompson-patients 4, 5, 6). Mean age at diet
introduction was 13.5 months (1 week to 3.5 years). Mean age
at diet withdrawal was 12.2 years (4.5 to 30 years). Mean age at
onset of neuropsychiatric symptoms was 22.7 years (15 to
40 years), with a delay of 10.5 years after stopping diet (0 to
33 years). One patient had neurological complications while
still on diet, but the observance was probably low in this
patient. Mean Phe level at onset of neuropsychiatric signs was
1475 mmol/L (590 to 2000 mmol/L). Among 14 patients with
available brain MRI, 13 patients (93%) displayed white matter
changes reminiscent of a diffuse leukoencephalopathy.
Clinical signs encompassed brisk reflexes (80%), spastic
paraparesis (60%), tremor (53%), psychiatric manifestations
(53%), epilepsy (20%), dystonia (13%), ataxia (7%) and Parkin-
sonism (7%). Moreover, all the patients had mild mental
retardation with low IQ. In 91.7% of the patients, improvement
of the clinical signs was noticed after reintroduction of the
diet.
In 3 patients reported in the literature and in our patient 5,
PKU was diagnosed in adulthood because of late onset
neurological abnormalities [9,10,12]. Clinical, biological and
radiological data of these 4 patients as well as genotypes are
summarized in Table 2. There were 1 man and 3 women. The

r e v u e n e u r o l o g i q u e 1 7 0 ( 2 0 1 4 ) 2 8 0 – 2 8 7 285
mean age at onset of neurological abnormalities was
46.25 years (33 to 54 years) with a mean age at diagnosis of
51 years (45 to 57 years). Mean Phe level at diagnosis was
1633 mmol/L (882 to 2358 mmol/L). Clinical signs included brisk
reflexes (3/4), spastic paraparesis (3/4), dementia (2/4), tremor
(2/4), Parkinsonism (1/4), epilepsy (1/4), bilateral visual loss (1/
4) and ataxia (1/4). Only 2/4 patients exhibited leukoencepha-
lopathy on brain MRI. It is noticeable that none of these
patients presented with psychiatric symptoms. Most of them
(3/4) had mental retardation. Improvement of clinical signs
with diet was noticed in two patients and not available for the
two others.
5. Discussion
Here we describe late neuropsychiatric signs occurring in
classic PKU patients. Two categories of patients are indivi-
dualized: those diagnosed with neonatal screening who
stopped diet in childhood or adulthood and those who never
received diet and developed neurological signs only in
adulthood. In both groups the same MRI and clinical
abnormalities (spastic paraparesis, epilepsy and Parkinso-
nism) were noticed.
Most of the cases reported in this article do not describe
true adult-onset neuropsychiatric manifestations of PKU but
rather patients who already had symptoms since childhood
and who showed deterioration of their clinical status in
adulthood. For instance, although most of our patients
exhibited late onset neuropsychiatric manifestations in
adulthood, including spastic paraparesis, psychiatric signs
or Parkinsonism, 4 out of 5 patients already presented some
intellectual delay in childhood or seizures (patient 5). As a
consequence although some progressive neuropsychiatric
signs may occur in adulthood, they can be viewed as clinical
worsening in adulthood rather than true adult-onset neuro-
psychiatric signs.
In PKU, several cerebral tissue damages have been
described in untreated patients, such as reduction of white
matter volume, diffuse cortical atrophy, and myelin changes
including spongiosis and gliosis [13,14]. To our knowledge,
there are no available histological data concerning early
treated patients. As a consequence, MRI appears as the most
adapted examination for brain abnormalities. Periventricular
parietal and occipital regions are the most concerned.
Abnormalities may be extensive observed in one of the
patients described in this series. However, hypersignal can
extend to frontal and temporal lobes and corpus callosum
[15,16]. They may be detected in PKU patients free of
neurological symptoms [16–18], and are not always related
to early diagnosis and treatment. Some studies have shown
correlations between Phe level at the time of MRI and the
extension of white matter abnormalities [16–18]. These
radiologic alterations are subsequently reversible and can
decrease with reintroduction of a phenylalanine restricted
diet [4,5,17], within a delay that seems to be correlated to
myelin turnover [4]. These white matter abnormalities may be
explained by cytotoxic oedema [19], dysmyelination due to
increased myelin content in water [20,21], increase in free
water trapped in myelin sheaths [17,22]. The absence of
neuronal damage [17] is confirmed with MR Spectroscopy that
shows normal Choline and NAA peaks together with a high
Phe peak [15].
In children with PKU, many studies have shown increased
attention deficit hyperactivity disorder (ADHD) [23–25] and
increased behaviour disturbances that correlate with the age
at poor Phe diet withdrawal [26]. In adults PKU, depressive
mood and anxiety are more common than in controls [27].
Women are particularly subjected to depression [28].
In early treated children, IQ is lower than in healthy
patients but remains in the average range [29,30]. Dietary
treatment that is strictly controlled and early introduced is the
best condition for normal intellectual development [31]. The
main parameters that are correlated with final IQ and
behavioural problems are the age at interruption of a strict
Phe level control and the initial IQ at dietary treatment onset
[32]. No correlation has been established between white
matter abnormalities on brain MRI and neuropsychological
alterations or psychiatric disturbances [28].
Gait disturbance as spastic paraparesis was reported in 11
patients [5–10,12]. The bladder function was normal for all
patients. In one case, vitamin B12 deficiency was detected and
supplemented [8]. In another case, spastic paraparesis
appeared after nitrous oxide anaesthesia in a PKU patient
with low B12 serum level [33]. Strict diet permits improvement
of walking and spasticity in most cases. Spastic paraparesis
started in the second decade of life in all cases, even in
patients without Phe low diet [34]. In the same review, spastic
paraparesis was reported in 5% of untreated PKU patients. The
fact that diet reintroduction in most cases led to improvement
of the paraparesis (as shown in our patient No. 1) indicates
that this complication is directly related to high Phe levels and
not a consequence of low B12 caused by the diet.
Electroencephalogram abnormalities are reported in 80% of
untreated PKU patients but epilepsy occurs in only 25% [34].
Correlation has been established in mice between serum Phe
level and epilepsy [35]. In this review, epilepsy was present in 4
patients [5–7]. Three had generalised epilepsy and one
complex partial seizure. Before systematic birth screening,
few child were diagnosed because of acquisitions delay and
infantile spasms. When diet was re- introduced, cessation of
seizures and improvement of electroencephalogram occurred
even in patients with hypsarrythmia [13]. Finally, epilepsy in
adults with PKU seems less common than epilepsy in
childhood and is highly responsive to the diet.
Parkinsonism was present in 2 cases [11]. Biochemical
modifications due to PKU include increased Phe level, reduced
tyrosine in blood, and decreased dopamine synthesis in brain.
DaTSCAN in the 2 cases are in favour of a typical Parkinson’s
disease (bilateral and asymmetrical loss in dopaminergic
terminals). Moreover, tremor and akinesia responded well to
L-dopa. In addition to true Parkinsonism, hand tremor has
been noticed in around 33% of untreated PKU patients [34].
It remains unclear why some adults will develop neuropsy-
chiatric signs and others not. All patients had high levels of Phe
(above 12 mg/dL, 720 mmol/L) at onset of neurological signs
suggesting a direct effect of Phe. The fact that clear improve-
ment was noticed in most patients after diet introduction
reinforces this hypothesis. In general, most adults who
interrupt their diet do not develop neuropsychiatric signs

r e v u e n e u r o l o g i q u e 1 7 0 ( 2 0 1 4 ) 2 8 0 – 2 8 7286
despite very high levels of Phe. Therefore, high Phe levels
should not be the sole explanation for the development of
neuropsychiatric symptoms and other explanations must be
hypothesized. The first is poor metabolic control in infancy
and childhood. Indeed, the fact that almost all patients who
develop late onset neuropsychiatric problems have a low IQ
suggests early brain toxicity of high Phe levels. Unfortunately,
it is difficult to conclude from our study since precise follow-
up of Phe values in childhood were not available for most
patients, and especially for those who did not follow their diet
rigorously. Another explanation is that some mutations in
Phe gene may predispose to late neuropsychiatric problems.
To date, more than 400 mutations have been described and
each mutation has an influence on the enzyme residual
activity. However, until now, no correlations have been found
between genotype and phenotype in PKU. Although genetic
data are lacking in early treated patients described in this
study (including literature review), they were available in
patients with late diagnosis and mutations were all different.
Therefore, it seems that the occurrence of late neuropsy-
chiatric symptoms is not correlated with a specific mutation.
A third explanation may concerns modifiers gene that
represent risk factors. Overall, most patients who stopped
their diet after the age of 7 years will never develop any
neuropsychiatric signs. However, this study suggests that all
patients with PKU need to be followed in adulthood to depict
very late onset complications or clinical worsening that are
potentially reversible upon diet reintroduction.
Disclosure of interest
The authors declare that they have no conflicts of interest
concerning this article.
r e f e r e n c e s
[1] Hardelid P, Cortina-Borja M, Munro A, Jones H, Cleary M,Champion MP, et al. The birth prevalence of PKU inpopulations of European, South Asian and sub-SaharanAfrican ancestry living in South East England. Ann HumGenet 2008;72(Pt 1):65–71.
[2] Walter JH, Lee PJ, Burgard P. In inborn metabolic diseases:hyperphenylalaninaemia. In: Saudubray JM, Van denBerghe G, Walter J, editors. Inborn errors of metabolism.Berlin: Springer Verlag; 2012. p. 222–32.
[3] Abadie V, Berthelot J, Feillet F, Maurin N, Mercier A, Ogierde Baulny H, et al. Management of phenylketonuria andhyperphenylalaninemia: the French guidelines. Associationfrancaise pour le depistage et la prevention des handicapsde l’enfant (AFDPHE). Arch Pediatr 2005;12(5):594–601.
[4] Cleary MA, Walter JH, Wraith JE, White F, Tyler K, JenkinsJP. Magnetic resonance imaging in phenylketonuria:reversal of cerebral white matter change. J Pediatr1995;127(2):251–5.
[5] Thompson AJ, Smith I, Brenton D, Youl BD, Rylance G,Davidson DC, et al. Neurological deterioration in youngadults with phenylketonuria. Lancet 1990;336:602–5.
[6] Wood B. Neurological disturbance in a phenylketonic childafter discontinuation of dietary treatment. Dev Med ChildNeurol 1976;18:657–66.
[7] Villasana D, Butler IJ, Williams JC, Roongta SM. Neurologicaldeterioration in adult phenylketonuria. J Inherit Metab Dis1989;12:451–7.
[8] McCombe PA, McLaughlin DB, Chalk JB, Brown NN, McGillJJ, Pender MP. Spasticity and white matter abnormalities inadult phenylketonuria. J Neurol Neurosurg Psychiatry1992;55:359–61.
[9] Weglage J, Oberwittler C, Marquardt T, Schellscheidt J,Teeffelen-Heithoff A, Koch G, et al. Neurologicaldeterioration in adult phenylketonuria. J Inherit Metab Dis2000;23:83–4.
[10] Kasim S, Moo LR, Zschocke J, Jinnah HA. Phenylketonuriapresenting in adulthood as progressive spatic paraparesiswith dementia. J Neurol Neurosurg Psychiatry 2001;71:791–5.
[11] Evans AH, Costa DC, Gacinovic S, Katzenschlager R,O’sullivan JD, Heales S, et al. L-DOPA responsiveParkinson’s syndrome in association withphenylketonuria: in vivo dopamine transporter and D2receptor findings. Mov Disord 2004;19:1232–6.
[12] Jousserand G, Antoine JC, Camdessanche JP. Musty odour,mental retardation, and spastic paraplegia revealingphenylketonuria in adulthood. J Neurol 2010;257:302–4.
[13] Pietz J. Neurological aspects of adult phenylketonuria. CurrOpin Neurol 1998;11(6):679–88.
[14] Anderson PJ, Leuzzi V. White matter pathology inphenylketonuria. Mol Genet Metab 2010;99(Suppl. 1):S3–9.
[15] Leuzzi V, Tosetti M, Montanaro D, Carducci C, Artiola C,Carducci C, et al. The pathogenesis of the white matterabnormalities in phenylketonuria. A multimodal 3.0tesla MRI and magnetic resonance spectroscopy (1H MRS)study. J Inherit Metab Dis 2007;30(2):209–16 [Epub 2007Jan 23].
[16] Cleary MA, Walter JH, Wraith JE, Jenkins JP, Alani SM, TylerK, et al. Magnetic resonance imaging of the brain inphenylketonuria. Lancet 1994;344(8915):87–90.
[17] Bick U, Ullrich K, Stober U, Moller H, Schuierer G, LudolphAC, et al. White matter abnormalities in patients withtreated hyperphenylalaninaemia: magnetic resonancerelaxometry and proton spectroscopy findings. Eur J Pediatr1993;152(12):1012–20 [Review].
[18] Thompson AJ, Tillotson S, Smith I, Kendall B, Moore SG,Brenton DP. Brain MRI changes in phenylketonuria.Associations with dietary status. Brain 1993;116(Pt 4):811–21.
[19] Kono K, Okano Y, Nakayama K, Hase Y, Minamikawa S,Ozawa N, et al. Diffusion-weighted MR imaging in patientswith phenylketonuria: relationship between serumphenylalanine levels and ADC values in cerebral whitematter. Radiology 2005;236(2):630–6.
[20] Dezortova M, Hajek M, Tintera J, Hejcmanova L, Sykova E.MR in Phenylketonuria-related brain lesions. Acta Radiol2001;42(5):459–66.
[21] Phillips MD, McGraw P, Lowe MJ, Mathews VP, Hainline BE.Diffusion-weighted imaging of white matter abnormalitiesin patients with phenylketonuria. AJNR Am J Neuroradiol2001;22(8):1583–6.
[22] Vermathen P, Robert-Tissot L, Pietz J, Lutz T, Boesch C,Kreis R. Characterization of white matter alteration inphenylketonuria by magnetic resonance relaxometry anddiffusion tensor imaging. Magn Reson Med 2007;58(6):1145–56.
[23] Antshel KM, Waisbren SE. Developmental timing ofexposure to elevated levels of phenylalanine is associatedwith ADHD symptom expression. J Abnorm Child Psychol2003;31(6):565–74.
[24] Antshel KM, Waisbren SE. Timing is everything: executivefunctions in children exposed to elevated levels ofphenylalanine. Neuropsychology 2003;17(3):458–68.

r e v u e n e u r o l o g i q u e 1 7 0 ( 2 0 1 4 ) 2 8 0 – 2 8 7 287
[25] Antshel KM. ADHD, learning, and academic performance inphenylketonuria. Mol Genet Metab 2010;99(Suppl. 1):S52–8.
[26] Holtzman NA, Kronmal RA, van Doorninck W, Azen C,Koch R. Effect of age at loss of dietary control onintellectual performance and behaviour of children withphenylketonuria. N Engl J Med 1986;314(10):593–8.
[27] Brumm VL, Bilder D, Waisbren SE. Psychiatric symptomsand disorders in phenylketonuria. Mol Genet Metab2010;99(Suppl. 1):S59–63.
[28] Pietz J, Fatkenheuer B, Burgard P, Armbruster M, Esser G,Schmidt H. Psychiatric disorders in adult patients withearly-treated phenylketonuria. Pediatrics 1997;99(3):345–50.
[29] De Groot MJ, Hoeksma M, Blau N, Reijngoud DJ, vanSpronsen FJ. Pathogenesis of cognitive dysfunction inphenylketonuria: review of hypotheses. Mol Genet Metab2010;99(Suppl. 1):S86–9.
[30] Berry HK, O’Grady DJ, Perlmutter LJ, Bofinger MK.Intellectual development and academic achievement of
children treated early for phenylketonuria. Dev Med ChildNeurol 1979;21(3):311–20.
[31] Burgard P. Development of intelligence in early treatedphenylketonuria. Eur J Pediatr 2000;159(Suppl. 2):S74–9.
[32] Holtzman C, Slazyck WE, Cordero JF, Hannon WH.Descriptive epidemiology of missed cases ofphenylketonuria and congenital hypothyroidism.Pediatrics 1986;78(4):553–8.
[33] Lee P, Smith I, Piesowicz A, Brenton D. Spastic paraparesisafter anaesthesia. Lancet 1999;353(9152):554.
[34] Brenton DP, Pietz J. Adult care in phenylketonuria andhyperphenylalaninaemia: the relevance of neurologicalabnormalities. Eur J Pediatr 2000;159(Suppl. 2):S114–20.
[35] Martynyuk AE, Ucar DA, Yang DD, Norman WM, Carney PR,Dennis DM, et al. Epilepsy in phenylketonuria: a complexdependence on serum phenylalanine levels. Epilepsia2007;48(6):1143–50 [Epub 2007 May 1].