Embed Size (px)
Citation preview

Phase II TrialsPhase II Trials
Lillian L. SiuLillian L. Siu
Division of Medical Oncology & Division of Medical Oncology & HematologyHematology
Princess Margaret Hospital, Princess Margaret Hospital, University of TorontoUniversity of Toronto

An Approach to Classifying Clinical Studies An Approach to Classifying Clinical Studies According to ObjectiveAccording to Objective
• Phase I:Phase I: Human Pharmacology Human Pharmacology
• Phase II:Phase II: Therapeutic Exploratory* Therapeutic Exploratory*
• Phase III:Phase III: Therapeutic Confirmatory Therapeutic Confirmatory
• Phase IV:Phase IV: Therapeutic Use Therapeutic Use
Federal Register 62, No. 242 1997

Estimated Number of Agents in Development Estimated Number of Agents in Development in 2002/2003in 2002/2003
Preclinical: ~800Preclinical: ~800
Phase I : ~200Phase I : ~200
Phase II: ~250Phase II: ~250
Phase III: ~80Phase III: ~80
Total: ~1300Total: ~1300
How safe is drug / How safe is drug / intervention A?intervention A?
How good is drug / How good is drug / interventionintervention A against against
Cancer X?Cancer X?
How good does drug / How good does drug / intervention A intervention A
compare to standard compare to standard of care in Cancer X?of care in Cancer X?

Essential Elements of Phase II TrialEssential Elements of Phase II Trial
• Why?Why?
• Who?Who?
• What?What?
• How?How?

Essential Elements of Phase II TrialEssential Elements of Phase II Trial
Why?Why? Objective and Objective and hypothesishypothesis
• State clearly one primary hypothesis-State clearly one primary hypothesis-testing objectivetesting objective
• May include a limited number of May include a limited number of secondary objectives secondary objectives

Primary Objective of a Phase II TrialPrimary Objective of a Phase II Trial
• Provide an estimate of the clinical “activity” Provide an estimate of the clinical “activity” of a new treatment approach:of a new treatment approach:
• Examples:Examples:– To determine the objective response rate To determine the objective response rate
(CR + PR) of drug A in patients with (CR + PR) of drug A in patients with advanced X cancer advanced X cancer
– To determine the 6 month progression-free To determine the 6 month progression-free
survival (PFS) rate of the combination AB in survival (PFS) rate of the combination AB in
patients with recurrent or metastatic Y cancerpatients with recurrent or metastatic Y cancer

Secondary Objective(s) of a Phase II TrialSecondary Objective(s) of a Phase II Trial
• Examples:Examples:– Hypothesis-generatingHypothesis-generating– Subset analysisSubset analysis– Alternative endpoint analysis (e.g. survival)Alternative endpoint analysis (e.g. survival)– Correlative scienceCorrelative science– Better define toxicity in a more homogeneous Better define toxicity in a more homogeneous
populationpopulation

Essential Elements of Phase II TrialEssential Elements of Phase II Trial
Who?Who? Patient selectionPatient selection
• Inclusion and exclusion criteria Inclusion and exclusion criteria

Choice of Patient Population - 1Choice of Patient Population - 1
• Disease:Disease:
– Be explicit Be explicit
– e.g. malignant neuroendocrine tumors: e.g. malignant neuroendocrine tumors: Do you include all subtypes? Do you include all subtypes? well-differentiated carcinoid well-differentiated carcinoid tumors have different biology compared to tumors have different biology compared to small cell variantssmall cell variants
• Target expression:Target expression:
– Is there a biological basis to enrich the Is there a biological basis to enrich the patient population?patient population?
– Is the turn-around time for the screening Is the turn-around time for the screening procedure fast enough to be feasible?procedure fast enough to be feasible?

Choice of Patient Population - 2Choice of Patient Population - 2
• Performance statusPerformance status
• Organ functionOrgan function
• Prior therapy allowed:Prior therapy allowed:
– What prior systemic therapy is allowed?What prior systemic therapy is allowed?
– For targeted therapies, should exclude other For targeted therapies, should exclude other targeted therapies of the same class if cross-targeted therapies of the same class if cross-resistance is a concern resistance is a concern
– Should exclude prior extensive radiotherapy Should exclude prior extensive radiotherapy if myelosuppression is a concern if myelosuppression is a concern
• Concomitant therapy disallowed:Concomitant therapy disallowed:
– Concern for drug interactions e.g. cyt P450Concern for drug interactions e.g. cyt P450

Essential Elements of Phase II TrialEssential Elements of Phase II Trial
WhatWhat
• Drug / intervention, dose, scheduleDrug / intervention, dose, schedule• Specify supportive therapy allowedSpecify supportive therapy allowed• Dose modificationDose modification• Dosing details: Dosing details:
- IV: premedications, infusion IV: premedications, infusion detailsdetails
- PO: fasting or fed, what to do if PO: fasting or fed, what to do if vomitted, missed dosevomitted, missed dose
Treatment planTreatment plan

Essential Elements of Phase II TrialEssential Elements of Phase II Trial
HowHow Endpoints and Endpoints and designdesign
Endpoints:Endpoints:• Measurable tumor mass reductionMeasurable tumor mass reduction• Progression-based endpoints: TTP, Progression-based endpoints: TTP,
PFSPFS• Serologic response: PSA, CA125Serologic response: PSA, CA125• SurvivalSurvival• Disease “stabilization”Disease “stabilization”• Correlative studiesCorrelative studies

Measurable Tumor Mass ReductionMeasurable Tumor Mass Reduction
ProPro
• ““Standard”Standard”
• ““Proves” antitumor Proves” antitumor activityactivity
• Standard criteriaStandard criteria
• Early readoutEarly readout
ConCon• Not applicable in all Not applicable in all
cancers e.g. prostatecancers e.g. prostate• Difficult to assess in Difficult to assess in
some cancers e.g. some cancers e.g. mesotheliomamesothelioma
• ““RR” relationship to RR” relationship to survival (is RR a survival (is RR a surrogate for an surrogate for an important effect?)important effect?)
• May not be appropriate May not be appropriate for some classes of for some classes of compoundscompounds

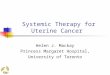
Copyright © American Society of Clinical Oncology
Zia, M. I. et al. J Clin Oncol; 23:6982-6991 2005
Reported response rates in phase III and phase II studies

Progression-Based EndpointsProgression-Based Endpoints
ProPro
• Reflects “biologic Reflects “biologic activity”activity”
• More clinically More clinically meaningful than RR meaningful than RR for some agents for some agents
ConCon• Variable definition Variable definition
(serologic, (serologic, symptomatic, symptomatic, measurable disease)measurable disease)
• Influenced by Influenced by frequency of frequency of observationobservation
• Influenced by tumor Influenced by tumor doubling-time more doubling-time more than therapythan therapy

Progression-Based EndpointsProgression-Based EndpointsSurvival TTP PFS
Patient Outcome Censor Time Censor Time Censor Time
001 Progressed day 15; alive @ LFU day 70
C 70 E 15 E 15
002 Alive @ LFU day 65; no progression; still on-treatment
C 65 C 65 C 65
003 Clinically progressed day 35; died day 55
E 55 E 35 E 35
004 Patient withdrew on day 20; no progression known
C 20 C 20 C 20
005 Died day 25 due to adverse event; no progression
E 25 C 25 E 25
006 Removed from study due to AE day 30; died day 80
E 80 C 30 C 30
007 Removed from treatment due to investigator discretion day 45; died day 90
E 90 C 45 C 45
008 Died day 85 due to progressive disease
E 85 E 85 E 85
009 Died day 60 due to MI; no prior PD
E 60 C 60 E 60

TTP, PFS, OSTTP, PFS, OS
50-day: TTP = 71%, PFS = 61%, OS = 88%
0 20 40 60 80
0.0
0.2
0.4
0.6
0.8
1.0
Overall SurvivalTime to ProgressionProgression-Free Survival

Progressive Disease
Day 1 of Study
Ch
an
ge in
Mark
er
of
Resp
on
se“Progression depends on when you look”
Death
@ 2 months: 50% progressed

Progressive Disease
Day 1 of Study
Ch
an
ge in
Mark
er
of
Resp
on
se“Progression depends on when you look”
Death
@ 3 months: 100% progressed

Serologic ResponseSerologic Response
ProPro
• Easy to measure!Easy to measure!
• Easy to quantitate!Easy to quantitate!
• ““Generally” reflects Generally” reflects tumor biologytumor biology
ConCon
• ““Generally” reflects Generally” reflects tumor biology but tumor biology but relationship to survival, relationship to survival, cell kill? i.e. not cell kill? i.e. not validated surrogatevalidated surrogate
• Secretion / synthesis Secretion / synthesis may be influenced may be influenced without cell kill or without cell kill or reduced tumor growthreduced tumor growth

SurvivalSurvival
ProPro
• Easy to measure!Easy to measure!
• Easy to quantitate!Easy to quantitate!
ConCon
• Delayed endpointDelayed endpoint
• Influenced by Influenced by “subsequent” “subsequent” therapiestherapies

StabilizationStabilization
ProPro
• Nothing!Nothing!ConCon
• Depends on intrinsic Depends on intrinsic growth rate of the growth rate of the tumor …which is tumor …which is almost almost NEVERNEVER measured in a clinical measured in a clinical trialtrial
Unless you employ special design (randomized
discontinuation) or you measure doubling-time prior
to therapy

Progressive Disease
Day 1 of Study
Day 180 of Study
Ch
an
ge in
Mark
er
of
Resp
on
se“Stabilization” also depends on
the biology of the disease

Correlative StudiesCorrelative Studies
• Important, hypothesis-generating, Important, hypothesis-generating, exploratory studiesexploratory studies– However, don’t do them because everyone However, don’t do them because everyone
else is…..else is…..
• BUT during course of study:BUT during course of study:– Validation of targets and assays may occur Validation of targets and assays may occur – New markers and pathways may be New markers and pathways may be
identified identified – Consider collecting specimens to evaluate Consider collecting specimens to evaluate
only if activity signals are seen in stage I only if activity signals are seen in stage I (for 2-stage designs)(for 2-stage designs)

Correlative StudiesCorrelative Studies
Prognostic MarkersPrognostic Markers• Correlate with disease Correlate with disease
outcomeoutcome• e.g. Clinical: stage, PSe.g. Clinical: stage, PS
• e.g. Lab: LDH in non-e.g. Lab: LDH in non-Hodgkin’s lymphomaHodgkin’s lymphoma
Predictive MarkersPredictive Markers• Predict outcome with Predict outcome with
specific therapy - specific therapy - match drugs with match drugs with appropriate pts appropriate pts
• e.g. HER2 in breast e.g. HER2 in breast cancercancer
Pharmacodynamic Markers
• Confirm biological Confirm biological activityactivity
• e.g. e.g. pERK with a pERK with a targeted agenttargeted agent


Design OptionsDesign Options
• Single arm, 2 stageSingle arm, 2 stage
• Randomized, phase IIRandomized, phase II
• Randomized discontinuationRandomized discontinuation
• BayesianBayesian

Single-Arm, 2-Stage DesignSingle-Arm, 2-Stage Design(Simon, Mini-max,..)(Simon, Mini-max,..)
• Treat Treat ~12-18~12-18 patients at 1 patients at 1stst stage stage
• Determine the “response rate”Determine the “response rate”• Less than that projected to indicate Less than that projected to indicate
activity (p0): STOP!activity (p0): STOP!• Sufficiently great to indicate activity: Sufficiently great to indicate activity:
CONTINUECONTINUE
• At the end of 2At the end of 2ndnd stage, declare drug / stage, declare drug / intervention worthy of further evaluation intervention worthy of further evaluation if > x number of “responses” are if > x number of “responses” are observed (p1)observed (p1)

Example of Single-Arm, 2-Stage Design Example of Single-Arm, 2-Stage Design
• 2-stage (Simon) of gefitinib in NSCLC as 2-stage (Simon) of gefitinib in NSCLC as first-line therapyfirst-line therapy
• p0 = 0.1, p1 = 0.25p0 = 0.1, p1 = 0.25
• Stage I: proceed if Stage I: proceed if >> 2 RR in 22 pts 2 RR in 22 pts
• Stage II: interest if Stage II: interest if >> 7 RR in 40 pts 7 RR in 40 pts
• Results:Results:– 12 PR / 40 pts (RR = 30%, 95% C.I. 17% - 12 PR / 40 pts (RR = 30%, 95% C.I. 17% -
47%)47%)
Niho et al, J Clin Oncol, 2006Niho et al, J Clin Oncol, 2006

““Setting the bar in phase II trials”Setting the bar in phase II trials”
• A review of 134 phase II trialsA review of 134 phase II trials• 70/134 (52%) defined as requiring 70/134 (52%) defined as requiring
historical data for design:historical data for design:– Nearly half did not cite source of historical Nearly half did not cite source of historical
datadata
• No study incorporated statistical No study incorporated statistical methods to account for sampling error, methods to account for sampling error, or possible differences in case mix or possible differences in case mix between the phase II sample and between the phase II sample and historical cohorthistorical cohort
Vickers et al, Clin Cancer Res, 2007Vickers et al, Clin Cancer Res, 2007

Randomized Phase II Design Randomized Phase II Design
1)1) Randomized phase II selection design:Randomized phase II selection design:• ““Pick-the-winner“, prioritizationPick-the-winner“, prioritization• Randomized 2 or more experimental Randomized 2 or more experimental
agents or regimensagents or regimens• ““Winning” agent or regimen will then Winning” agent or regimen will then
be subjected to a definitive phase III be subjected to a definitive phase III trial against standardtrial against standard
• e.g. RP2T of carboplatin vs paclitaxel + e.g. RP2T of carboplatin vs paclitaxel + carboplatin in platinum-sensitive carboplatin in platinum-sensitive recurrent advanced ovarian cancer recurrent advanced ovarian cancer (Gonzalez-Martin et al, Ann Oncol, 2005)(Gonzalez-Martin et al, Ann Oncol, 2005)

Randomized Phase II Design Randomized Phase II Design
2)2) Randomized phase II design including a Randomized phase II design including a reference standard treatment control reference standard treatment control arm:arm:
• Non-comparativeNon-comparative• Standard control arm acts as a checkStandard control arm acts as a check• Not to be compared directly with the Not to be compared directly with the
experimental arm(s)experimental arm(s)• e.g. RP2T of docetaxel + prednisone e.g. RP2T of docetaxel + prednisone
vs docetaxel + prednisone + new vs docetaxel + prednisone + new drug in hormone refractory prostate drug in hormone refractory prostate cancer cancer

Randomized Phase II Design Randomized Phase II Design
3)3) Phase II/III trial design:Phase II/III trial design:• Randomized phase II trial embedded Randomized phase II trial embedded
within phase III trialwithin phase III trial• This design is efficient only if the This design is efficient only if the
experimental regimen has a experimental regimen has a reasonably high likelihood of reasonably high likelihood of “success”, otherwise intensive efforts “success”, otherwise intensive efforts are expended in developing a phase III are expended in developing a phase III protocolprotocol
• e.g. Phase II/III trial of docetaxel + e.g. Phase II/III trial of docetaxel + cisplatin + 5FU (DCF) vs CF in cisplatin + 5FU (DCF) vs CF in advanced gastric cancer advanced gastric cancer (Van Cutsem et al, J Clin Oncol, 2006)(Van Cutsem et al, J Clin Oncol, 2006)

Randomized Phase II Design Randomized Phase II Design
ProPro
• Reduces selection biasReduces selection bias
• Improve patient Improve patient comparabilitycomparability
• Non-survival endpoints Non-survival endpoints can be ascertained can be ascertained fairly quicklyfairly quickly
ConCon
• Generally requires Generally requires more pts than a single-more pts than a single-arm phase II trialarm phase II trial
• A “positive” result in A “positive” result in the screening design the screening design often compromise the often compromise the ability to conduct ability to conduct definitive phase III trialsdefinitive phase III trials

Randomized Discontinuation Trials (RDT)Randomized Discontinuation Trials (RDT)
• Enrichment design, in which all pts Enrichment design, in which all pts receive study drug for an initial run-in receive study drug for an initial run-in period, followed by random assignment period, followed by random assignment of patients with disease stabilization to of patients with disease stabilization to either the study drug or placeboeither the study drug or placebo

*Placebo patients who progressed could cross over to sorafenib
†Including 36 patients without bidimensional tumor measurements, but with radiological evidence of progression
Patient FlowPatient Flow
Sorafenib 12-week run-in
(n=202)
Tumor shrinkage ≥25%(n=73)
Tumor growth/ shrinkage <25%
(n=69)
Tumor growth ≥25%
(n=51†)
Off study(n=58)
Sorafenib 12 weeks
(n=32)
Placebo* 12 weeks
(n=33)
Continue open-label sorafenib
(n=79)
50% Progression free 24 weeks
Disease status at 12 weeks unknown
(n=9)
18% Progression free 24 weeks
Ratain et al, J Clin Oncol, 2006Ratain et al, J Clin Oncol, 2006

12 Week Changes from Baseline in Bidimensional Radiographic Measurements*12 Week Changes from Baseline in Bidimensional Radiographic Measurements*
Data shown for 166 patients (12-week bidimensional measurements were not available for 36 patients, who had radiographic evidence of progression). Mean change at 12 weeks = -18 33%
*Investigator-assessed
-100
-75
-50
-25
0
25
50
75
100
125
% c
ha
ng
e f
rom
ba
se
lin
e i
n b
idim
en
sio
na
l tu
mo
r m
ea
su
rem
en
t
≥25% growth
<25% change
≥25% shrinkage
PRPR

Randomized Discontinuation DesignRandomized Discontinuation Design
ProPro heterogeneity of heterogeneity of
randomized ptsrandomized pts statistical powerstatistical power
• Evaluates true Evaluates true disease disease “stabilization”“stabilization”
• Minimizes use of Minimizes use of placeboplacebo
ConCon
• Large sample sizeLarge sample size
• Longer accrual timeLonger accrual time
• Many patients never Many patients never reach stable diseasereach stable disease
• Unknown how long to Unknown how long to give a new agentgive a new agent

Bayesian DesignBayesian Design
• Uses prior information and assumptions in the Uses prior information and assumptions in the decision making processdecision making process
• Updates prior information with trial dataUpdates prior information with trial data• Trial data will “overwhelm” the prior Trial data will “overwhelm” the prior
information in a well designed trialinformation in a well designed trial• Outcome is a probability with “credible” Outcome is a probability with “credible”
intervals (e.g. the probability of RR >20% is intervals (e.g. the probability of RR >20% is 0.95)0.95)

Bayesian DesignBayesian Design
• Both prior Both prior information and real information and real trial data are trial data are incorporated in a incorporated in a thorough evaluationthorough evaluation
• Can make frequent Can make frequent stop or go stop or go evaluationsevaluations
• Collaboration with Collaboration with biostatisticiansbiostatisticians
• Prior information is Prior information is subjectivesubjective
ProPro ConCon

ConclusionsConclusions
• Phase II trials are exploratory studies Phase II trials are exploratory studies and rarely are definitiveand rarely are definitive
• Efficient to exclude inactive therapiesEfficient to exclude inactive therapies
• Results must be interpreted cautiously, Results must be interpreted cautiously, in the context of the availability of other in the context of the availability of other therapies therapies
• Estimate clinical activity and provide Estimate clinical activity and provide further safety information – important in further safety information – important in the “go/no go” decisionthe “go/no go” decision
• Require confirmation in phase III trialsRequire confirmation in phase III trials