Embed Size (px)
Citation preview

Patterson, Kalcich and ScherlagMid-Myocardium Reentry
Phase 1B Ventricular Arrhythmia in the Dog:Localized Reentry Within the Mid-Myocardium
Eugene Patterson, Michael Kalcich, andBenjamin J. ScherlagDepartments of Pharmacology and Medicine, the University ofOklahoma Health Sciences Center, and Department of VeteransAffairs Medical Center, Oklahoma City, Oklahoma, USA
Abstract. Intramural and epicardial composite electro-
grams, signal-averaged orthogonal bipolar electrograms
across the ischemic zone, and closely-spaced bipolar elec-
trograms from subendocardium, mid-myocardium, and
subepicardium were utilized to determine if phase 1B reen-
try resulted from localized reentry within ischemic mid-
myocardium. During the ~rst 10 minutes following coronary
ligation, activation delays were largest in ischemic subepi-
cardium, with continuous electrical activity in ischemic epi-
cardium linking a ventricular extrasystole to the preceding
beat. During the 15–30 minute period, activation delay ob-
served in ischemic mid-myocardium exceeded activation
delay on the epicardial surface. Ventricular extrasystoles
were associated with mid-myocardial delays . 130 msec.
With short-coupled extrasystoles (,300 msec), electrical
activity in ischemic mid-myocardium linked an extrasystole
with the preceding beat. Although single extrasystoles with
coupling intervals .300 msec were also associated with
mid-myocardial delays .130 msec, most extrasystoles
(68%) demonstrated an isoelectric gap .20 msec. The data
demonstrate an association between delayed activation
within ischemic mid-myocardium and phase 1B arrhythmia
resulting from (1) localized reentry in ischemic mid-myo-
cardium and (2) a delay-dependent “non-reentrant” mecha-
nism.
Key Words. ventricular tachycardia, ventricular ~brillation,
acute myocardial ischemia, sudden coronary death, myocar-
dial reentry
Introduction
Ventricular arrhythmias arising during the initial 30minutes following coronary artery ligation are ob-served in two distinct temporal phases [1–4]. The ~rstphase, phase 1A, is observed during the initial 10–12minutes following coronary artery ligation. Phase 1Aarrhythmia is preceded by the rapid evolution of de-layed activation within ischemic subepicardium. Whenthe duration of delayed activation within ischemicsubepicardium exceeds 120–140 msec, localized reen-try and ventricular arrhythmia are observed [5–7].Evidence for localized reentry includes localized con-tinuous diastolic electrical activity spanning the dia-stolic interval preceding a ventricular extrasystole in
composite electrogram recordings [5–7] and multielec-trode maps [8,9]. Ventricular extrasystoles, ventriculartachycardia, and spontaneous ventricular ~brillationmay be observed during phase 1A [2–7]. The partialrecovery towards baseline of delayed activation in is-chemic subepicardium during the 10–15 minute periodfollowing coronary artery ligation is associated withthe dissipation of phase 1A arrhythmia [1–7].
A second, temporally-distinct phase of ventriculararrhythmia observed during the 15–30 minute periodfollowing left anterior descending coronary artery(LAD) ligation (phase 1B) has been described byKaplinsky and co-workers [2] and by Menken and co-workers [3]. Ventricular extrasystoles, ventriculartachycardia, and ventricular ~brillation are observedwith a similar incidence during phase 1A [2,3]. Unlikephase 1A, evidence for localized reentry within is-chemic subepicardium during phase 1B arrhythmia isconspicuously absent [1,7,10,11]. Enhanced ventricularautomatically and an accelerated idioventricular heartrate are also not observed to accompany phase 1B ar-rhythmia [2].
The following experiments were performed to de-termine if delayed activation and localized reentrywithin ischemic mid-myocardium could provide a basisfor ventricular arrhythmias observed during the 15- to30-minute period following LAD ligation in the anes-thetized dog. Composite electrograms, signal-aver-aged bipolar electrograms from the borders of the is-chemic zone, and multiple, closely-spaced bipolarelectrograms from subendocardium, mid-myocardium,and subepicardium were recorded from acutely is-
Journal of Interventional Cardiac Electrophysiology 1998;2:145–161
© Kluwer Academic Publishers. Boston. Printed in U.S.A.
145
Supported by a grant-in-aid from the American Heart Associa-tion, National Af~liate, Dallas, TX, and research funds from theDepartment of Veterans Affairs
Address for correspondence: Eugene Patterson, Ph.D., ResearchService 151-F, Department of Veterans Affairs Medical Center,921 NE 13th Street, Oklahoma City, OK 73104 USA. E-mail:[email protected]
Received 7 November, 1997; accepted 23 January, 1998
PIPS#164052

chemic myocardium. Using atrial pacing and vagusnerve stimulation, the role of heart rate in modifyingdelayed activation and phase 1B ventricular arrhyth-mia was also examined.
Materials and Methods
1. Surgical preparation
Mongrel dogs were anesthetized with intravenous so-dium pentobarbital, 30 mg/kg. A cuffed endotrachealtube was inserted and the animals were ventilatedwith room air using a Harvard respirator. Cannulaewere inserted into the right femoral artery and rightfemoral vein for the measurement of arterial bloodpressure and for drug administration, respectively. Anelectrode catheter was inserted into the left commoncarotid artery and was advanced to the proximal aorticroot to record His-bundle activation. Insulated silverwires (0.25 mm diameter) were inserted into the leftcervicovagal trunk. Vagus nerve stimulation (0.05 msecduration stimuli, 20 Hz, 1–15 V) was used to slow thesinus heart rate and/or produce AV nodal blockade.
II. Experimental series #1–Intramural
composite electrode recordings
In 28 dogs, composite bipolar electrodes were alsoplaced on the epicardial surface of the left ventricle [7].One electrode was placed on the epicardial surface ofmyocardium served by the left circum_ex coronaryartery and the second electrode was placed on the an-terior epicardial surface of the left ventricle. Compos-ite electrode recordings from the epicardial surfacewere ampli~ed and ~ltered (30–500 Hz) using an Elec-tronics for Medicine VR-16 recorder and were re-corded at paper speeds of 100 or 250 mm/second on aGould electrostatic recorder. Five pairs of insulatedsilver wires (0.25 mm diameter, 4–5 cm long exposedrecording surface) were inserted mid-wall into the mid-LAD distribution and into the mid-left circum_ex coro-nary artery distribution using 6.3 cm long 20 gaugeneedles (Fig. 1, panel A). The distance between oppos-ing recording poles was estimated to vary between 2–4mm. The individual bipolar electrode recordings weresummed to form a composite electrode recording, andwere recorded after ~ltering at 30–500 or 100–500 Hz.Plunge bipolar electrodes (0.13 mm diameter Te_on-coated stainless steel) passed through 21-gauge hypo-dermic needles were used to record from subendo-cardium in the left circum_ex and LAD distributions.
The natural course of arrhythmia development wasmonitored in 17 anesthetized dogs subjected to abruptLAD ligation (silk ligature). Ventricular ~brillation de-veloped in four animals at 4.0, 5.5, 16 and 23 minutesfollowing LAD ligation. In an additional 11 animals,atrial pacing and vagus nerve stimulation were used toalter the atrial rate. The rate-dependence of epi-cardial/mid-myocardial conduction disturbances and
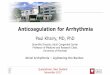
Fig. 1. Experimental models. Electrical recordings were ob-tained from the intact heart in anesthetized dogs. Activation ofthe His-bundle was recorded using an electrode catheter in-serted into the root of the aorta. A bipolar electrode was at-tached to the left atrial appendage. The LAD was isolated proxi-mal to the ~rst major diagonal branch. Experimental series #1:Mid-myocardial composite electrode recordings were obtainedfrom the LAD and circum_ex coronary artery distributions.Five pairs of plunge wires (4–5 cm long) were inserted intomid-myocardium served by each of the respective arteries. Theindividual wires of each electrode pair were separated by a dis-tance of 2–4 mm. Bipolar composite electrograms were also re-corded from the epicardial surface. In some experiments,closely-spaced bipolar electrode recordings were obtained fromthe endocardial surface of the heart using plunge wires (0.005in diameter Te_on-coated stainless steel) inserted through a 6.3cm long hypodermic needles. Experimental series #2: Orthogo-nal bipolar electrograms (X, Y, and Z leads with a 3–4 cm in-terelectrode separation in the X and Y leads, 1.2-2.0 cm in thetransmural Z lead) were recorded from the borders of the LADdistribution. Bipolar composite electrograms were recordedfrom epicardium in the LAD and LCX coronary artery distri-butions. Experimental series #3: Needle electrodes containing 3bipolar recording sites (centered 1.5, 4.5, and 7.5 mm deep, 1.2mm interelectrode distances) were placed in a 3 3 4 patternwith a 5 mm interelectrode separation.
146 Patterson, Kalcich and Scherlag

arrhythmia formation were studied over the 15- to 30-minute period following LAD ligation.
III. Experimental series #2—
Signal averaging from the borders
of the ischemic zone.
In 35 dogs, composite electrograms were recordedfrom the epicardium served by the LAD and cir-cum_ex coronary arteries (as previously described),and orthogonal leads (X, Y, and Z planes) were re-corded from the borders of anterior myocardium. Therecording electrodes were 1.5 mm diameter silver ballson 0.25 mm diameter Te_on-coated silver wire insertedby a 21-gauge hypodermic needle (Fig. 1, panel B). X,Y, and Z electrograms were ampli~ed, digitized at 1KHz, and stored on magnetic media for 32 minutes,beginning 2 minutes before coronary artery occlusion.Signal-averaging of X, Y, and Z electrograms (25–40consecutive beats) was performed using a 80386-basedpersonal computer and Predictor version 6.1 software(Corazonix). Signal averaging of the interval betweena single premature beat and the preceding sinus heartbeat was performed for repetitive, constant coupledventricular beats having X, Y, and Z electrogram mor-phologies with a correlation co-ef~cient of 0.97 or bet-ter with a selected template value.
IV. Experimental series #3—
Multiple, closely-spaced bipolar
electrograms recorded from ischemic
subendocardium, mid-myocardium,
and subepicardium
Plunge electrodes containing 3 bipolar electrodes (1.2mm interelectrode distance, 3.0 mm between bipolarelectrode pairs) were placed in a 3 3 4 pattern (5 mmapart in the X and Y planes) into the anterior myocar-dium. The recording electrodes were centered approxi-mately 1.5, 4.5, and 7.5 mm below the epicardial surfaceof the heart (Z plane) (Fig. 1, panel C). Continuousrecordings of surface ECGs (lead I, II, and V-2) andbipolar electrograms were digitized and stored onmagnetic media (Bard Electrophysiology System).
V. Statistics
Differences within a group were determined using ananalysis of variance for repeated measures followed byDunnett’s test. Differences between groups were de-termined using a one-way analysis of variance followedby Bonferoni’s test. A value of p # 0.05 was used ascriterion for signi~cance.
Results
In each of the three experimental series, two tempo-rally distinct phases of ventricular arrhythmia [1,2]were observed during the ~rst 30 minutes followingLAD ligation (Fig. 2). The ~rst phase of ventriculararrhythmia peaked at 4–8 minutes following LAD oc-
clusion and the second phase peaked at 18–26 minutes.We have chosen to use the designations, phase 1A(0–15 minutes) and phase 1B (15–30 minutes) as pre-viously described by Menken and co-workers [3], forthe designation of the two temporal phases of ventricu-lar arrhythmia.
I.A. Experimental series #1—
Before coronary artery occlusion
Before LAD ligation, activation within subepicardiumand mid-myocardium during sinus rhythm was rapid.A lead II and an anterior (V-2) surface ECG, a His-bun-dle electrogram, and mid-myocardial and epicardialcomposite electrograms are shown before LAD liga-tion (Pre-occlusion)(Fig. 3).
I.B. Phase 1A arrhythmia
With LAD ligation, delayed activation developed rap-idly within both mid-myocardial and epicardial com-posite electrograms recorded from the LAD distribu-tion (Fig. 2). The low-amplitude electrical activity wasobserved to extend into the J-T segment of the surfaceECG. Within the ~rst 8 minutes following coronaryartery ligation, premature ventricular beats and ven-tricular tachycardia were observed in 13 of 17 animals.Ventricular arrhythmia occurred only when the dura-tion of electrical activity within ischemic subepi-cardium exceeded 130 msec (Table 1). Ventricular ar-rhythmia was observed in association with continuoussubepicardial electrical activity linking a ventricularextrasystole with the preceding ventricular beat. Dur-ing the initial 15 minutes following LAD ligation, acti-vation delays were always larger in the ischemic epi-cardial composite electrogram than in the ischemicmid-myocardial composite electrogram.
During the ~rst 15 minutes following LAD ligation(Fig. 2), activation in subepicardium was observed topersist after the cessation of electrical activity in mid-myocardium An example of delayed epicardial activa-tion and localized reentry within ischemic subepi-cardium is shown in Figure 3 (3 minutes). Ventriculararrhythmia was accompanied by continuous electricalactivity recorded from the epicardial surface, duringthe diastolic interval preceding a premature ventricu-lar beat. A partial regression of delayed activation inischemic subepicardium was observed during the 8–15minute period following coronary artery ligation. Witha decrease in delayed activation to ,130 msec withinischemic subepicardium, phase 1A ventricular arrhyth-mia ceased (Fig. 2).
I.C. Phase 1B arrhythmia
A mean delay of 94 6 9 msec was present in ischemicsubepicardium, 15 minutes following LAD ligation. Al-though the subepicardial delay was larger than ob-served pre-ligation, no signi~cant change in delayedelectrical activation recorded from the epicardial sur-face was observed during the next 15 minutes (Fig. 2).
Mid-Myocardium Reentry 147
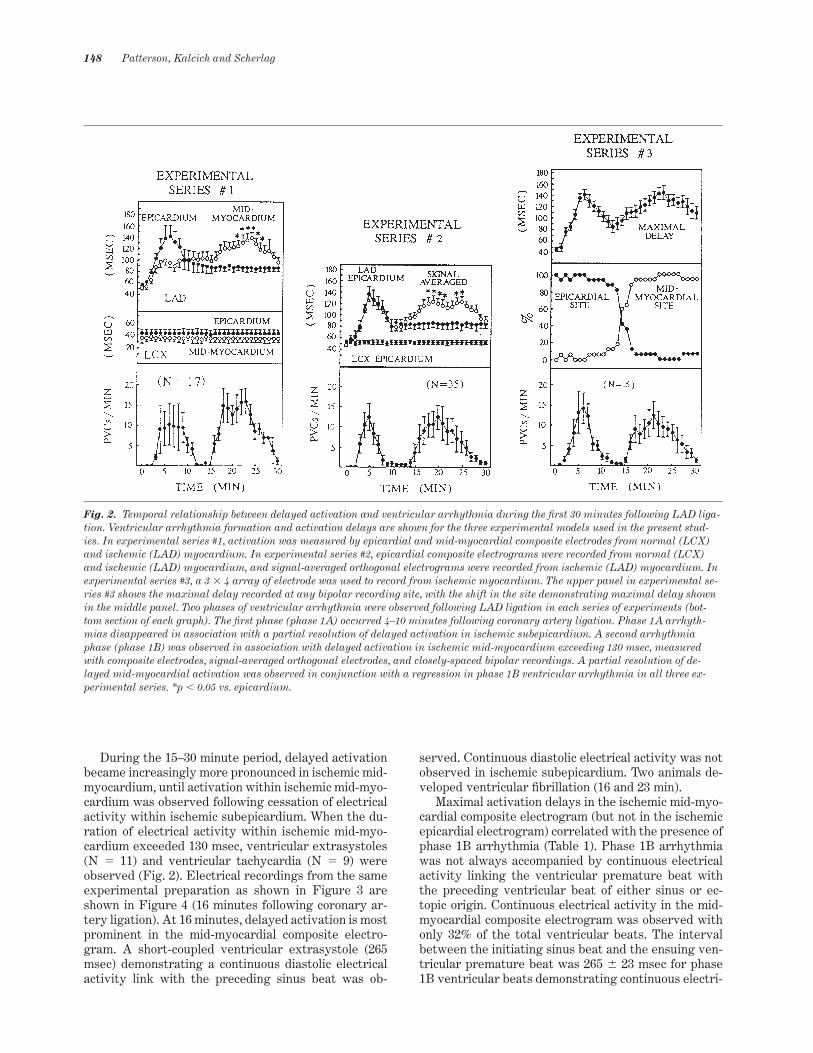
During the 15–30 minute period, delayed activationbecame increasingly more pronounced in ischemic mid-myocardium, until activation within ischemic mid-myo-cardium was observed following cessation of electricalactivity within ischemic subepicardium. When the du-ration of electrical activity within ischemic mid-myo-cardium exceeded 130 msec, ventricular extrasystoles(N 5 11) and ventricular tachycardia (N 5 9) wereobserved (Fig. 2). Electrical recordings from the sameexperimental preparation as shown in Figure 3 areshown in Figure 4 (16 minutes following coronary ar-tery ligation). At 16 minutes, delayed activation is mostprominent in the mid-myocardial composite electro-gram. A short-coupled ventricular extrasystole (265msec) demonstrating a continuous diastolic electricalactivity link with the preceding sinus beat was ob-
served. Continuous diastolic electrical activity was notobserved in ischemic subepicardium. Two animals de-veloped ventricular ~brillation (16 and 23 min).
Maximal activation delays in the ischemic mid-myo-cardial composite electrogram (but not in the ischemicepicardial electrogram) correlated with the presence ofphase 1B arrhythmia (Table 1). Phase 1B arrhythmiawas not always accompanied by continuous electricalactivity linking the ventricular premature beat withthe preceding ventricular beat of either sinus or ec-topic origin. Continuous electrical activity in the mid-myocardial composite electrogram was observed withonly 32% of the total ventricular beats. The intervalbetween the initiating sinus beat and the ensuing ven-tricular premature beat was 265 6 23 msec for phase1B ventricular beats demonstrating continuous electri-
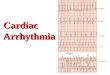
Fig. 2. Temporal relationship between delayed activation and ventricular arrhythmia during the ~rst 30 minutes following LAD liga-tion. Ventricular arrhythmia formation and activation delays are shown for the three experimental models used in the present stud-ies. In experimental series #1, activation was measured by epicardial and mid-myocardial composite electrodes from normal (LCX)and ischemic (LAD) myocardium. In experimental series #2, epicardial composite electrograms were recorded from normal (LCX)and ischemic (LAD) myocardium, and signal-averaged orthogonal electrograms were recorded from ischemic (LAD) myocardium. Inexperimental series #3, a 3 3 4 array of electrode was used to record from ischemic myocardium. The upper panel in experimental se-ries #3 shows the maximal delay recorded at any bipolar recording site, with the shift in the site demonstrating maximal delay shownin the middle panel. Two phases of ventricular arrhythmia were observed following LAD ligation in each series of experiments (bot-tom section of each graph). The ~rst phase (phase 1A) occurred 4–10 minutes following coronary artery ligation. Phase 1A arrhyth-mias disappeared in association with a partial resolution of delayed activation in ischemic subepicardium. A second arrhythmiaphase (phase 1B) was observed in association with delayed activation in ischemic mid-myocardium exceeding 130 msec, measuredwith composite electrodes, signal-averaged orthogonal electrodes, and closely-spaced bipolar recordings. A partial resolution of de-layed mid-myocardial activation was observed in conjunction with a regression in phase 1B ventricular arrhythmia in all three ex-perimental series. *p , 0.05 vs. epicardium.
148 Patterson, Kalcich and Scherlag

Fig. 3. Composite electrogram recordings—pre-ligation. A lead II (L-II) electrocardiogram, an anterior surface lead (V-2), a His-bundle electrogram (HB(Eg)), composite electrograms from both mid-myocardium (MID) and subepicardium (EPI), and endo-cardial plunge recordings (ENDO) are shown for left anterior descending (LAD) and left circum_ex coronary artery (LCX) distribu-tions. Two different ~lter settings are shown for the composite electrogram recorded from ischemic mid-myocardium (upper traceMID-LAD, 100–500 Hz; lower trace, 30–500 Hz). The electrical recordings shown in Figures 4 and 6 are from this same experiment.Experimental recordings are shown before LAD coronary artery ligation (Pre-occlusion) and at 3 minutes after LAD ligation (3 min-utes). The inset panel at the bottom is an enlarged view from the 3-minute panel.
Table 1. Delayed activation following left anterior descending coronary artery ligation in the dog
No phase 1A arrhythmia Phase 1A arrhythmia(N 5 4) (N 5 13)
Maximal epicardial delay (msec) 127 6 16 146 6 13*Maximal mid-myocardial delay (msec) 130 6 16 126 6 12
No phase 1B arrhythmia Phase 1B arrhythmia(N 5 4) (N 5 9)
Maximal epicardial delay (msec) 132 6 16 140 6 13Maximal mid-myocardial delay (msec) 110 6 16 149 6 12†
(X 6 SEM) *p , 0.01 vs. No phase 1A arrhythmia †p , 0.01 vs. No phase 1B arrhythmia
Mid-Myocardium Reentry 149

cal activity in the ischemic mid-myocardial compositeelectrogram (short-coupled extrasystoles) and was 3396 24 msec (p , 0.05) for phase 1B ventricular beatsdemonstrating an isoelectric gap greater than 20 msec(37 6 13 msec) (long-coupled extrasystoles). Althoughthe weighted means for short-coupled extrasystoles(19.8 6 2.3 minutes) and long-coupled extrasystoles(26.2 6 3.6 minutes) were different (p , 0.05), the twodifferent forms of extrasystole did not occur in tempo-rally-distinct phases, with the simultaneous presenceof both arrhythmia forms observed in 8 experimentalpreparations. Histograms are shown for a constant-coupled ventricular beat with a coupling interval of 260msec and a constant-coupled ventricular beat with acoupling interval of 440 msec (Fig. 5).
Examples of the two different forms of ventricularextrasystole are shown in Figure 6. The experimentalpreparation is the same as shown in Figures 3 and 4. Inthe left-hand panel of Figure 6, a ventricular couplet isobserved. The coupling interval between the sinus beatand the ~rst beat of the ventricular couplet is 325 msec.Although there is markedly delayed electrical activitypresent in the mid-myocardial composite electrogram(205 msec), there is a prolonged 102 msec isoelectricperiod between the cessation of activation in the mid-myocardial electrogram and the ventricular extra-systole. In the right-hand panel of Figure 6 (a recordingtaken 30 seconds after the recording in the left-handpanel) is a short-coupled extrasystole (265 msec). Con-tinuous electrical activity in the mid-myocardial com-
Fig. 4. Composite electrogram recordings—16 minutes. Electrical recordings from the same experiment as shown in Figure 3 areshown at 16 minutes following LAD ligation. The inset bottom panel is an enlarged view of the mid-myocardial recordings during pre-mature ventricular beat formation from the upper tracing.
150 Patterson, Kalcich and Scherlag
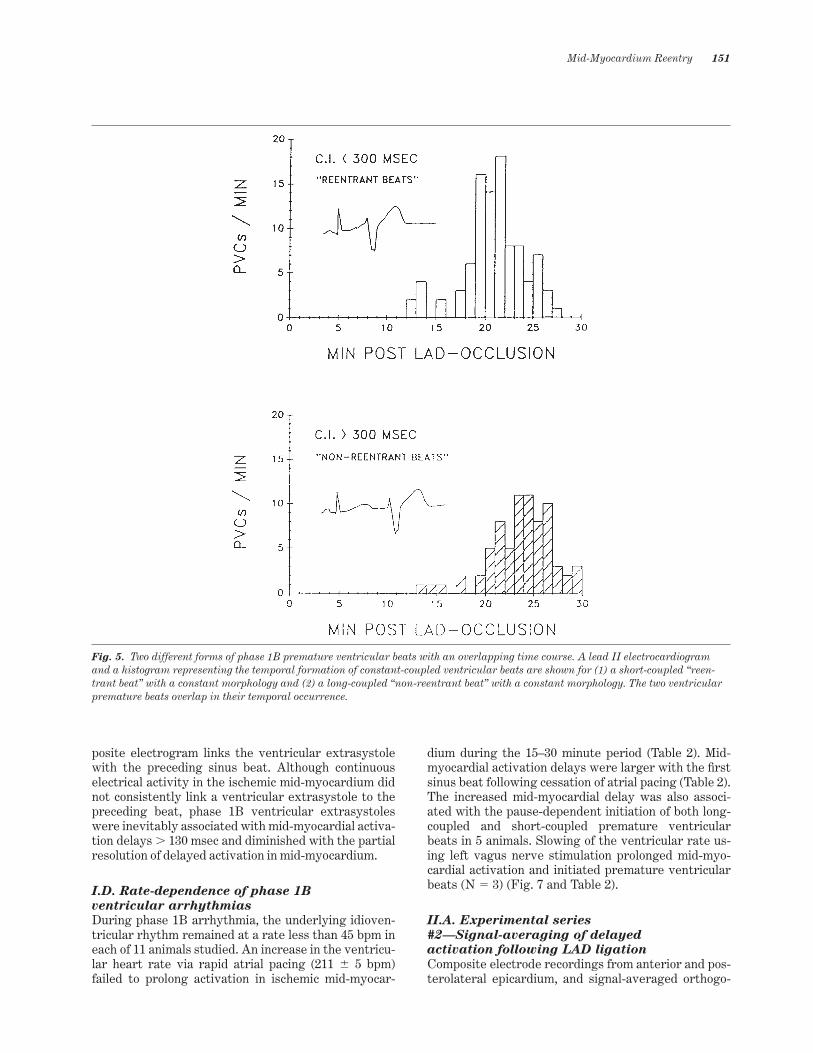
posite electrogram links the ventricular extrasystolewith the preceding sinus beat. Although continuouselectrical activity in the ischemic mid-myocardium didnot consistently link a ventricular extrasystole to thepreceding beat, phase 1B ventricular extrasystoleswere inevitably associated with mid-myocardial activa-tion delays . 130 msec and diminished with the partialresolution of delayed activation in mid-myocardium.
I.D. Rate-dependence of phase 1B
ventricular arrhythmias
During phase 1B arrhythmia, the underlying idioven-tricular rhythm remained at a rate less than 45 bpm ineach of 11 animals studied. An increase in the ventricu-lar heart rate via rapid atrial pacing (211 6 5 bpm)failed to prolong activation in ischemic mid-myocar-
dium during the 15–30 minute period (Table 2). Mid-myocardial activation delays were larger with the ~rstsinus beat following cessation of atrial pacing (Table 2).The increased mid-myocardial delay was also associ-ated with the pause-dependent initiation of both long-coupled and short-coupled premature ventricularbeats in 5 animals. Slowing of the ventricular rate us-ing left vagus nerve stimulation prolonged mid-myo-cardial activation and initiated premature ventricularbeats (N 5 3) (Fig. 7 and Table 2).
II.A. Experimental series
#2—Signal-averaging of delayed
activation following LAD ligation
Composite electrode recordings from anterior and pos-terolateral epicardium, and signal-averaged orthogo-
Fig. 5. Two different forms of phase 1B premature ventricular beats with an overlapping time course. A lead II electrocardiogramand a histogram representing the temporal formation of constant-coupled ventricular beats are shown for (1) a short-coupled “reen-trant beat” with a constant morphology and (2) a long-coupled “non-reentrant beat” with a constant morphology. The two ventricularpremature beats overlap in their temporal occurrence.
Mid-Myocardium Reentry 151

nal electrograms were recorded before and after LADocclusion. Within the ~rst 5–7 minutes, a similar extentof delayed activation was observed in the compositeelectrogram recorded from anterior epicardium and inthe signal-averaged orthogonal electrograms (Fig. 2).Ventricular arrhythmia (phase 1A) was accompaniedby continuous electrical activity linking prematureventricular beats with the preceding sinus heart beat
in the composite electrogram recorded from anteriorepicardium. By 15 minutes, however, both delayed ac-tivation in anterior subepicardium and delayed activa-tion in the signal-averaged orthogonal electrogramshad resolved (Table 3).
During the 15–30 minute period, activation in thesignal-averaged orthogonal electrograms was observedto occur after a resolution of electrical activity within
Fig. 6. Composite electrogram recordings—18–19 minutes. Electrical recordings from the same experiment as shown in Figures 3and 4 are shown 18–19 minutes following LAD ligation. The inset recordings shown at the bottom of the ~gure are enlargements ofLAD mid-myocardial electrical recordings shown above.
Table 2. Bradycardia-dependent activation delays
Cycle length Epicardial Mid-myocardial(msec) delay (msec) delays (msec)
Sinus rhythm 403 6 69 90 6 23 118 6 12Pacing-induced pause 563 6 78 86 6 18 137 6 13*Vagus nerve stimulation 1089 6 237 97 6 21 149 6 19*
(X 6 SEM) *p , 0.01 vs. Sinus rhythm
152 Patterson, Kalcich and Scherlag

the composite electrogram recorded from anteriorsubepicardium, suggesting a secondary source for de-layed activation within anterior myocardium. When ac-tivation delays within the signal-averaged orthogonalelectrograms were .130 msec, phase 1B arrhythmiawas observed (Fig. 2). The decrease in delayed activa-tion within the signal-averaged electrograms occurredin conjunction with the resolution of ventricular ar-rhythmia.
Phase 1B ventricular arrhythmia was dependentupon delayed activation in the signal-averaged orthogo-nal electrograms developed during the 15–30 minuteperiod. An absence of delayed activation in the signal-averaged orthogonal electrograms was associated withan absence of phase 1B arrhythmia, regardless of thepresence of phase 1A arrhythmia and delay during theinitial 10 minutes following coronary artery ligation. Asobserved in experimental series #1, phase 1B arrhyth-
mia occurred without a signi~cant change in activationrecorded from anterior subepicardium (Fig. 2).
Signal-averaging was used to examine electrical ac-tivity within the interval connecting constant-coupled,repetitive ventricular premature beats with a uniformmorphology, to the preceding ventricular beat of sinusorigin (Fig. 8). Short-coupled ventricular ectopic beats(coupling intervals ,300 msec) occurred in conjunctionwith continuous electrical activity (.50 uV) spanningthe diastolic interval between the sinus beat and thesubsequent premature ventricular beat. Constant-cou-pled ventricular ectopic beats with a uniform morphol-ogy and constant coupling intervals .300 msec wereassociated temporally with delayed activation in signal-averaged electrograms exceeding 130 msec, but demon-strated a mid-diastolic isoelectric period of 20–100 msecin signal-averaged recordings of the interectopic inter-val (Fig. 8).
Fig. 7. Mid-myocardial activation—effects of rapid atrial pacing and bradycardia. Mid-myocardial composite electrograms areshown at two different ~lter settings (upper trace, 100–500 Hz; Iower trace, 30–500 Hz). During sinus rhythm (175 beats/min) (left-hand panel), an activation delay is recorded in mid-myocardium. With atrial pacing at 240 bpm, there is only a slight prolongation ofthe activation delay to 65 msec (middle panel). With vagal stimulation induced slowing of the heart rate (45 bpm), the mid-myocar-dial composite electrogram lengthens to a duration of 120 msec.
Table 3. Conduction delays measured in anterior myocardium following left anterior descending coronary artery ligation
No phase 1A arrhythmia Phase 1A arrhythmia(N 5 21) (N 5 14)
Maximal signal-averaged delay (0–15 min) (msec) 102 6 14 168 6 11*Maximal signal-averaged delay (15–30 min) (msec) 112 6 13 24 6 11
No phase 1B a rrhythmia Phase 1B arrhythmia(N 5 12) (N 5 23)
Maximal signal-averaged delay (0–15 min) (msec) 106 6 11 120 6 11Maximal signal averaged delay (15–30 min) (msec) 90 6 12 150 6 11†
(X 6 SEM) *p , 0.01 vs. No phase 1A arrhythmia †p , 0.01 vs. No phase 1B arrhythmia
Mid-Myocardium Reentry 153

III.A. Bipolar electrode recordings from
the central ischemic zone.
Electrical recordings were obtained from a 3 x 4 x 3(deep) electrode array in the central LAD distribution(N 5 16). During the initial 15 minutes following LADligation, delayed activation was observed in all threemyocardial zones (subendocardium, mid-myocardium,and subepicardium), with the largest activation delaysobserved in subepicardium (Fig. 2). Phase 1A arrhyth-mia was observed when maximal subepicardial delaysexceeded 130 msec. Continuous electrical activity inthe subepicardial electrograms was observed to linkpremature ventricular beats with the preceding ven-tricular beat of sinus origin.
In the 15–30 minute period, the site of maximal delayshifted to mid-myocardium (Fig. 2), in association withphase 1B arrhythmia. The inability to identify discreteactivation times for delayed, fractionated mid-myocar-dial electrograms prevented the construction of activa-tion maps. Continuous localized electrical activity inmid-myocardial electrograms spanned the interval pre-ceding ventricular premature beats having coupling in-tervals , 300 msec. Continuous or near continuous elec-trical activity was commonly observed at multiple sites
(2 or 3 neighboring mid-myocardial sites). Continuouselectrical activity was always observed at contiguousrecording sites (direct neighbors).
Bipolar electrode recordings from a representativeexperiment are shown in Figures 9–13. Subendocardial,mid-myocardial, and subepicardial recording sites areshown for 7 of the 12 electrodes. In Figure 9 (Pre-occlu-sion), activation in the anterior wall occurs only duringthe QRS interval of the surface ECGs. At 16 minutes(Fig. 10), delayed activation was largest at mid-myocar-dial sites, and conducted in a 2:1 block pattern at 3 mid-myocardial sites. At 16.3 minutes, constant-coupledventricular extrasystoles (285 msec) were connected tothe preceding sinus beat by continuous mid-myocardialelectrical activity (Fig. 11). Constant-coupled ventricu-lar extrasystoles and ventricular tachycardia were ob-served from 16.3 to 19.13 minutes, when ventriculartachycardia progressed to ventricular ~brillation (Fig.12). The initial beat of the ventricular tachycardia wasaccompanied by continuous diastolic electrical activitywithin mid-myocardium. At 23 minutes (Fig. 13), con-stant-coupled ventricular extrasystoles with couplingintervals .300 msec were observed, each having a 28msec duration isoelectric interval.
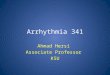
Fig. 8. Signal-averaged orthogonal electrogram recordings. Signal-averaged orthogonal electrograms (X, Y, and Z as described inFigure 1) are shown before LAD ligation (Pre-occlusion), for a short-coupled extrasystole at 25 min (25 MIN), and for a long-coupledextrasystole (30 min). The number of intervals averaged for the 25-min recording was 28 and for the 30-min recording was 23.
154 Patterson, Kalcich and Scherlag

Discussion
I. Phase 1A ventricular arrhythmia
Ventricular extrasystole and tachycardia observedduring the ~rst 15 minutes following LAD ligation (1)were prefaced by prolonged activation delays (.130msec) in ischemic subepicardium, (2) were accompa-nied by continuous electrical activation in subepi-cardium spanning the preceding diastolic interval, and(3) were not observed subsequent to a partial resolu-tion of delayed activation on the epicardial surface ofthe heart (activation delays ,130 msec). Electrical ac-tivity within the ischemic mid-myocardial compositeelectrogram terminated more than 30 msec before elec-trical activation ceased in ischemic subepicardium. Al-though mid-myocardium may participate in the slow-
ing of the transmural spread of activation followingLAD ligation in the dog, ventricular arrhythmia duringthe ~rst 15 minutes following coronary artery occlusionwas accompanied by continuous electrical activitywithin ischemic subepicardium. The observationsmade in the present study during the ~rst 15 minutesfollowing LAD ligation do not differ from previous ob-servations [1,2,5–7,9] and are consistent with localizedreentry on the anterior epicardial surface of the heart.
II. Phase 1B ventricular arrhythmia
During the 15–30 minute period, phase 1B arrhythmiawas associated with activation delays in ischemic mid-myocardium .130 msec (Fig. 2). Delayed activation inischemic mid-myocardium was observed as late as
Fig. 9. Transmural ventricular activation—experimental studies #3 (Pre-occlusion). Lead I, II, and AVF electrocardiograms (I, II,and AVF), His-bundle activation (HB(eg)), and subendocardial (ENDO), mid-myocardial (MID), and subepicardial (EPI) bipolarelectrograms were recorded as described in Figure 1. Before LAD occlusion, activation is discrete, and contained within the QRS inter-val of the surface EKG). Activation is shown for only 7 of the 12 transmural recording sites. Activation at the remaining 5 transmu-ral sites demonstrated only moderate delay (,100 msec) during subsequent coronary artery occlusion and have been omitted for im-proved clarity.
Mid-Myocardium Reentry 155

60–70 msec after electrical activity ceased on the epi-cardial surface. Either the failure to achieve activationdelays of 130 msec in ischemic mid-myocardium, or thepartial resolution of delayed activation to values ,130msec was associated with an absence of ventriculararrhythmia, regardless of the method utilized to recordmid-myocardial activation. Slowing of the normaltransmural spread of excitation from endocardium toepicardium cannot provide for greater delay in mid-myocardium vs. subepicardium. Delayed activation inmid-myocardium would be consistent with localizedconduction block during transmural activation, andslow conduction around or through sites of conductionblock [7,9].
Previous investigators have hypothesized a possiblerole for mid-myocardium as a substrate for reentrantarrhythmias during the ~rst 30 minutes following coro-nary artery ligation [3,5,7,9]. Reentrant pathways inmid-myocardium have been demonstrated, however
only during the initial 10 minutes following coronaryartery ligation [2,3,5]. Evidence for mid-myocardialreentry during phase 1B arrhythmia has been absent,even when closely-spaced bipolar electrograms wererecorded at multiple sites from endocardium to epi-cardium surface of the canine heart [12]. The authorsstated that phase 1B arrhythmias appeared to be inde-pendent of delayed and fragmented electrical activityin both subepicardial and intramyocardial zones. Theabove observations were limited to 8 experiments,with transmural recordings from only 6 sites in eachexperiment [12]. The absence of prolonged intramyo-cardial delay during the 15–30 minute period contrastswith recordings performed in the present experiments,in a recent report by Mori and co-workers [5], and in asingle example published by Kabell et al. [9].
Activation delays within ischemic mid-myocardiumaccompany a slow rise in extracellular potassium ionactivity over the 12–20 minute time period [5]. Both
Fig. 10. Transmural ventricular activation, 16 minutes. The present recordings were obtained 16 minutes following LAD ligation.The recordings are labeled as described in Figure 9. A repetitive 2:1 pattern of conduction block (delayed-truncated activation delay)can be observed in recordings ENDO-2, MID-2, MID-4, and MID-5. The latest site of ventricular activation is MID-2. Ventricular ar-rhythmia was not present.
156 Patterson, Kalcich and Scherlag

intramyocardial delay [5, present study] and potassiumion activity in mid-myocardium [5] are larger in dogsdeveloping phase 1B arrhythmia versus dogs failing todevelop phase 1B arrhythmia. There may be a partial“resolution” of delayed activity due to inexcitability inpreviously excitable mid-myocardium [5]. Along withthe partial resolution of conduction delay, phase 1Barrhythmia ceases (present studies).
Continuous electrical activity spanning the intervalbetween a ventricular extrasystole and the precedingventricular beat was demonstrated only with short-coupled extrasystoles (265 6 23 msec), constitutingonly 32% of all ventricular extrasystoles in the 15–30minute period. Although all phase 1B ventricular ex-trasystoles were associated with activation delays.130 msec in mid-myocardium, continuous electricalactivity was absent with the more commonly observedextrasystoles having longer-coupling intervals (339 624 msec). Although we do not assume a non-reentrantmechanism as a basis for long-coupled, constant-cou-pled ventricular extrasystoles with a mid-diastolic
isoelectric interval, we have chosen to use the term“non-reentrant” ventricular extrasystoles, consistentwith the description previously used by Pogwizd andCorr [10].
III. The electrophysiologic bases for
short-coupled versus long-coupled
ventricular extrasystoles
Localized intramural reentry demonstrating continu-ous electrical activity linking a premature ventricularbeat to a sinus beat has been previously described inthe ~rst ~ve minutes following coronary artery ligationin porcine [8] and feline [10,11] hearts, and in acutelyischemic canine mid-myocardium following coronaryartery ligation in the presence of previous myocardialinfarction [13]. In three studies [8,10,11], however, an-other mechanism for ventricular arrhythmia was ob-served. Ventricular extrasystoles demonstrating bothdelayed activation and a prolonged isoelectric windowduring mid-diastole were observed and termed “non-
Fig. 11. Transmural ventricular activation, 16.3 minutes. The present recordings were obtained 16.3 minutes following LAD ligation.The recordings are labeled as described in Figure 9. Two short-coupled (,300 msec coupling interval) premature ventricular beatswere present, associated with a fragmented potential in the delayed-truncated activation pattern observed in Figure 10.
Mid-Myocardium Reentry 157

reentrant” beats [10,11]. Although the inability to con-sistently record from the entire reentrant pathway forlong-coupled beats does not eliminate reentry as amechanism, observations made using multielectrodemapping suggest another mechanism for long-coupledventricular extrasystoles [8,10,11].
Ventricular extrasystoles having a prolongedisoelectric interval and a “long-coupling interval” havebeen described in the feline heart during the ~rst 10minutes following coronary artery ligation [10,11]. The“long-coupled” ventricular extrasystoles were associ-ated with prolonged conduction delays in ischemic mid-myocardium (149 6 7 msec), and despite the use of 200closely spaced bipolar recording sites in the feline leftventricle, demonstrate prolonged isoelectric periods of20–220 msec during mid-diastole preceding a ventricu-lar extrasystole. The earliest site of activation follow-ing the isoelectric interval could be observed at sitesacross an inexcitable gap, at a site distant from the last
active electrogram preceding the isoelectric interval.Although the experiments of Pogwizd and Corr [10,11]were performed in a different species, and at a differ-ent interval following coronary artery ligation, thecharacteristics of the “non-reentrant” arrhythmia arestrikingly similar to the present studies. In the presentstudies, following a similar isoelectric interval, the ear-liest recorded electrical activity for “non-reentrant”ventricular extrasystoles was almost equally distrib-uted between non-ischemic and ischemic subepi-cardium, mid-myocardium, and endocardium. The gapwas apparent regardless of the mechanism (signal-av-eraging of multiple beats with an identical (X, Y, and Z)morphology and coupling interval, composite elec-trode, or local bipolar electrodes) used for electricalrecording. As observed by Pogwizd and Corr [10,11],and in the present study, both reentrant and non-reen-trant mechanisms could occur over the same time pe-riod, in the same heart. Moreover, “non-reentrant”
Fig. 12. Transmural ventricular activation, 19.13 minutes. The recordings were obtained 19.13 minutes following LAD ligation. Therecordings are labeled as described in Figure 9. Ventricular ~brillation was observed 19.13 minutes following LAD ligation. The ~rstsinus beat occurs after a prolonged (485 msec) pause following ventricular bigeminy. Mid-diastolic electrical activation leading the~rst ventricular beat was observed in mid-myocardium (MID-2, MID-4, and MID-7). Activation of subsequent ventricular beats be-came more disorganized and degenerated into ventricular ~brillation.
158 Patterson, Kalcich and Scherlag

beats were not uncommon, comprising a majority ofthe observed extrasystoles.
“Non-reentrant” ventricular beats are associatedwith a critical conduction delay, i.e., ventricular ar-rhythmia is associated with delayed mid-myocardialactivation .130 msec and are not observed with mid-myocardial delays ,130 msec. One possible mechanismfor reentry in the absence of continuous diastolic elec-trical activity would be electrotonic excitation acrossinexcitable tissue, alone or in combination with in-creased excitability in marginally-ischemic tissue dis-tal to the site of block [14,15]. Such a mechanism wouldbe consistent with (1) the late development of delayand conduction block in ischemic mid-myocardium, (2)the simultaneous observation of localized reentry and“non-reentrant” beats in mid-myocardium resultingfrom either active or electrotonic exit, respectively,from a site of delayed activation, (3) multiple sites of
exit across inexcitable tissue, and (4) the presence of aprolonged isoelectric interval for “non-reentrant”beats [8,15].
IV. Bradycardia-dependent conduction
delays during the 15- to 30-minute period
Epicardial activation delays during the ~rst minutesfollowing coronary artery ligation are progressivelyincreased with an increase in heart rate and are corre-spondingly reduced with a decrease in the heart rate[16]. In contrast, during the 15–30 minute period,larger activation delays in mid-myocardium were ob-served with slower heart rates. Both reentrant andnon-reentrant ventricular extrasystoles were fre-quently observed to follow a pacing-induced sinuspause. There is a prolongation of the ischemic zonemid-myocardial composite electrogram with the ~rstsinus beat following a pacing-induced sinus pause and
Fig. 13. Transmural ventricular activation, 23-minute recordings. The present recordings were obtained 23 minutes following LADligation. The recordings are labeled as described in Figure 9. At 23 minutes, ventricular bigeminy is present. The coupling interval ofthe ventricular extrasystoles exceeds 300 msec. Although delayed activation was present in mid-myocardium, an isoelectric gap of 30msec was present in MID-5 for each diastolic period preceding the initial premature ventricular beat.
Mid-Myocardium Reentry 159

a rapid, progressive shortening of the ischemic zonemid-myocardial electrogram with the ~rst 2–3 sinusbeats following a prolonged pause (Table 2). Brady-cardia-dependent prolongations of ventricular activa-tion and resultant reentrant ventricular arrhythmiahave been previously observed in both ischemic mid-myocardium and epicardium during a 2–3 hr periodfollowing coronary artery ligation in the dog [17,18].Whether the larger mid-myocardial activation delayswith bradycardia result from an additional delay ofconduction at a slower heart rate or from a partialrecovery from previously provoked tachycardia-de-pendent block is not known. The observation howeveragrees with the failure of b-adrenergic receptor block-ade and the resultant reduction in the sinus heart rateto signi~cantly attenuate phase 1B arrhythmia in thedog [3].
V. Bases for slow conduction in
mid-myocardium
Electrophysiologic changes occurring during the 15–30minute period following coronary artery occlusion in-clude (1) an increase in extracellular potassium [5], and(2) a secondary increase in activation times simultane-ous with localized conduction block [19]. At 30 minutesor later most mid-myocardial sites within the ischemiczone become completely inactive. Cell-to-cell uncou-pling and 2:1 block in mid-myocardium are consistentwith the present results. The second PVC variant (longcoupling interval with a signi~cant mid-diastolic iso-electric interval) may represent slow electrotonic acti-vation across an inexcitable gap caused by an incre-mental increase in tissue resistivity.
During the 15–30 minute period following LAD liga-tion, the loss of mid-myocardial excitability may also betime-dependent and may recover with bradycardia ora sinus pause. The resolution of phase 1B arrhythmiamay result from a progressive loss of excitabilitywithin ischemic mid-myocardium and a failure to de-velop activation delays suf~cient for active or electro-tonic conduction to neighboring myocardium.
VI. Limitations of the present study
Continuous electrical activity during the diastole inter-val preceding an ectopic beat is not unequivocal prooffor reentry. Neither is the absence of continuous elec-trical activity proof of a non-reentrant mechanism. Thepresent studies, however, demonstrate a consistencybetween three methods of electrical recording, eachdemonstrating delayed electrical activity within mid-myocardium during the 15–30 min time period closelyassociated with phase 1B arrhythmia and each demon-strating reproducible, continuous, diastolic electricalactivity linking a ventricular beat with the precedingventricular beat for beats with coupling intervals ,300msec. Although the use of signal-averaged electricalrecordings and composite electrical recordings lacksadequate precision and speci~city to de~ne anatomic
reentrant pathways, the same criticism can not be as-cribed to closely-spaced bipolar electrode recordingsdemonstrating the same electrical activation patterns.Concentrating 36 bipolar recording sites in the centralischemic zone detected previously unreported activa-tion delays. The inability to delineate a macroreentrantreentrant circuit may not be a limitation of the bipolarrecording density or electrode con~guration. The elec-trode separation and the number of electrode record-ing sites within the central ischemic zone are similar tothat used in numerous 3-D mapping studies [10,11].Although it is troubling in that such local fragmentedelectrical activity has been absent with other bipolar orunipolar mapping studies [10,11] in another species,the delayed and fragmented mid-myocardial activationin mid-myocardium is a measurable and reproduciblephenomenon temporally-associated with phase 1B ar-rhythmia and may represent very small, circumscribedreentrant circuits or abortive reentrant circuits lo-cated near the bipolar recording site. The delayed mid-myocardial activity recorded in the present studies us-ing multiple recording methods can not be disprovedby the inability of previous investigators to record suchactivity at individual recording sites in the same ex-perimental model [4,5,12], or a failure of multielectrodemapping to de~ne macroreentrant circuits in the pre-sent studies.
Acknowledgments
The authors would like thank Bobby Fitts for his technical assis-tance in the performance of the present studies.
References
1. Haase M, Schiller U. Zur zeitlin parallelitat zwishen deractivitat ectopischer schrittmacher und dem eintritt vonkammer_immern nach ligatur eines hauptkoronarastesbeim hued. Acta Biol Med Germ 1969;23:413–422.
2. Kaplinsky E, Ogawa S, Balke CW, Dreifus LS. Two periodsof early ventricular arrhythmia in the canine acute myocar-dial infarction model. Circulation 1979;60:397–403.
3. Menken U, Wiegand V, Bucher P, Meesmann W. Prophylaxisof ventricular ~brillation after experimental coronary arteryocclusion by chronic beta-adrenoceptor blockade withatenolol. Cardiovasc Res 1979;13:588–594
4. Russell DC, Lawrie JS, Riemersma RA, Oliver MF. Mecha-nisms of phase la and lb early ventricular arrhythmias dur-ing myocardial ischemia in the dog. Am J Cardiol 1984;53:307–312.
5. Mori H, Sakurai K, Miyazaki T, Ogawa S, Nakamura Y.Local myocardial electrogram and potassium concentrationchanges in super~cial and deep intramyocardium and theirrelations with early ischemic ventricular arrhythmias. Car-diovasc Res 1987;21:447–454.
6. Waldo A, Kaiser GA. A study of ventricular arrhythmiasassociated with acute myocardial infarction in the canineheart. Circulation 1973;47:1222–1228.
7. Williams DO, Scherlag BJ, Hope RR, El-Sherif N, LazzaraR. The pathophysiology of malignant ventricular arrhyth-
160 Patterson, Kalcich and Scherlag

mias during acute myocardial ischemia. Circulation 1974;50:1163–1172.
8. Janse MJ, van Capelle FJL, Morsink H, Kleber AG, Wilms-Schopman F, Cardinal R, d’Alnoncourt CN, Durrer D. Flowof “injury” current and patterns of excitation during earlyventricular arrhythmias in acute regional myocardial is-chemia in isolated porcine and canine hearts. Circ Res 1980;47:151–165.
9. Kabell G, Scherlag BJ, Hope RR, Lazzara R. Regional myo-cardial blood _ow and ventricular arrhythmias followingone-stage and two-stage coronary artery occlusion in anes-thetized dogs. Am Heart J 1982;104:537–544.
10. Pogwizd SM, Corr PB. Reentrant and nonreentrant mecha-nisms contribute to arrhythmogenesis during early myocar-dial ischemia: results using three-dimensional mapping. CircRes 1987;61:352–371.
11. Pogwizd SM, Corr PB. Mechanisms underlying the develop-ment of ventricular ~brillation during early myocardial is-chemia. Circ Res 1990;66:672–695.
12. Kaplinsky E, Ogawa S, Kmetzo J, Balke CW, Dreifus L.Intramyocardial activation in early ventricular arrhythmiasfollowing coronary artery ligation. J Electrocardiol 1980;13:1–6.
13. Patterson E, Lucchesi BR. Electrophysiologic and antiar-rhythmic actions of d,l-nadolol—acute ischemia in the pres-ence of previous myocardial infarction. Am Heart J 1988;116: 1223–1232
14. Coronel R, Wilms-Schopman FJG, Opthof T, van CapelleFJL, Janse MJ. Injury current and gradients of diastolicthreshold, TQ potential, and extracellular potassium concen-tration during acute regional ischemia in the isolated per-fused pig heart. Circ Res 1991;68:1241–1249.
15. Janse MJ, van Capelle FJL. Electrotonic interactions acrossan inexcitable region as a cause of ectopic activity in acuteregional myocardial ischemia: A study in intact porcine andcanine hearts and computer models. Circ Res 1982;50:527–537.
16. Hope RR, Williams DO, El Sherif N, Lazzara R, ScherlagBJ. The ef~cacy of antiarrhythmic agents during acute myo-cardial ischemia and the role of heart rate. Circulation1974;50:507–514.
17. Hope RR, Scherlag BJ, Lazzara R. The induction of ven-tricular arrhythmias in acute myocardial ischemia by atrialpacing with long-short cycle sequences. Chest 1977;71:651–658.
18. Scherlag BJ, Kabell G, Harrison L, Lazzara R. Mechanismof bradycardia-induced ventricular arrhythmias in myocar-dial ischemia and infarction. Circulation 1982;89:1429–1434.
19. Smith WT, Fleet WF, Johnson TA, Engle CL, Cascio WE.The lb phase of ventricular arrhythmias in the ischemic insitu porcine heart is related to changes in cell-to-cell electri-cal coupling. Circulation 1995;92:3051–3060.
Mid-Myocardium Reentry 161