Embed Size (px)
DESCRIPTION
arrhythmia management
Citation preview

Management of Arrhythmias
Abhishek reddy
KMC Manipal

Agents classified according to•Mode of action•Site
Anti arrhythmic drugs




• Acts principally by suppressing excitability and slowing down conduction in atrial or ventricular muscle.
• Blocks Na+ channels• Contraindicated in patients w/ heart failure as
they depress myocardial function.
Class 1 drugs

Class 1a drugs:
• Prolongs cardiac action potential • ↑ tissue refractory period• Uses: atrial and ventricular arrhythmias
• E.g. Disopyramide:• Causes anticholinergic side effects- urinary
retention, ppts glaucoma.• Depresses myocardial function n hence avoided
in cardiac failure• E.g. Quinidine:• Rarely used as it increases mortality n causes GI
upset.

Class 1b drugs:
They shorten the AP and tissue refractory period
Acts on ventricles so used in Ventricular tachycardia and ventricular fibrillation.
E.g. Lidocaine, Mexiletine

Class 1c
Affects slope of AP w/o altering duration or refractory period.
Uses: prophylaxis of AF, SVA, VA. Contraindicated in patients w/ previous MI-
leads to pro- arrhythmias E.g. Flecainide Effective- AF Given w/ AV node blocking drugs- β
blockers to prevent pro-arrhythmias E.g. Propafenone

Class 2 drugs Group comprises of β blockers These drugs diminish Phase 4
depolarization, thus depresheart rate and contractility. sing automaticity, prolonging AV conduction, and decreasing
These reduce the rate of SA node depolarization and causes a relative block in AV node.
Uses: Rate control in Atrial Flutter, AF, SVA, VT
Reduces myocardial excitability and risk of arrhythmic death in patients w/ CHD & heart failure.

Cardio selective β blockers: Acts on myocardial β1 receptors E.g. Atenolol, Bisoprolol, Metoprolol
Non selective β blockers: Acts on β1 & β2 receptors Β2 blockade- bronchospasm and peripheral
vasoconstriction E.g. Propranolol, Nadolol, Carvedilol
Sotalol: Causes torsade de pointes

Class 3 drugs
o Acts by prolonging plateau phase of AP.o Hence lengthens refractory periodo Effective- atrial & ventricular tachyarrhythmiao Causes QT prolongation and predisposes to
torsade de pointes and VTo E.g. Amiodaroneo Principal drug o Also has class 1, 2, 4 activityo Most effective drug- paroxysmal AFo Uses: to prevent recurrent episodes of VTo Side effects: photosensitivity, skin discoloration,
thyroid dysfunction, nausea, vomiting etc

Class 4 drugs
Blocks the slow calcium channels( important for impulse generation and conduction in atrial and nodal tissues
Acts at the AV node E.g. Verapamil, Diltiazem

Other anti- arrhythmic drugs
Atropine Sulphate (0.6 mg i.v., repeated if necessary- maximum of 3 mgs)
↑ sinus rate and SA, AV conduction Best choice- severe bradycardia or
hypotension due to vagal over activity. Side effects: dry mouth, thirst, blurred
vision, atrial and ventricular extra systoles.

Adenosine:
Given i.v. bolus, initially 3mg over 2 sec. If no response after 1-2 mins, 6mg should be given; and if needed after 1-2 mins, max dose 12mg may be given.
Uses: terminate SVT when AV node is part of re-entry circuit or in Atrial Flutter with 2:1 AV block or broad complex tachycardia.
Side effects: flushing, dyspnea, chest pain Contraindications: Asthma

Digoxin
Slows conduction and prolongs refractory period in AV node.
Controls ventricular rate in AF & SVT of AV node.
Shortens refractory period and enhances conduction and excitability in other parts of the heart.
Side effects: GI disturbances, xanthopsia, arrhythmias




Therapeutic Procedures
• External defibrillation and cardio version
• Catheter ablation • Temporary pacemakers• Permanent pacemakers• Implantable cardiac
defibrillators(ICDs)• CRT (cardiac resynchronization
therapy

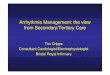
External defibrillation

cardio version

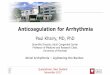
Catheter ablation

Flouroscopic image showing catheter

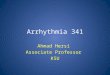
pacemakerImplantable cardiac defibrillators(ICDs)

pacemaker ICDs


CRT (cardiac resynchronization therapy)