-
`
1
PHARMACOKINETICS OF IBUPROFEN UNDER
HEAD-DOWN-BED-REST TECHNIQUE (HDBR)
IN HEALTHY HUMANS
By
Mahmoud Musa Eid Abu Dhair
A thesis Submitted inPartial Fulfillment of the
Master of ScienceIn Pharmaceutical Science
At
Petra UniversityFaculty of Pharmacy
Amman-JordanMay 2011
-
`
2
-
`
3
Abstract
PHARMACOKINETICS OF IBUPROFEN UNDER HEAD-DOWN-BED-REST
TECHNIQUE (HDBR) IN HEALTHY HUMANS
By
Mahmoud Musa Eid Abu Dhair
Petra University 2011
Under the supervision of Prof. Nasir Idkaidek and Prof. Tawfiq
Arafat
Space medicine is a new field that is growing fast as the
international
space station becomes a reality. Medications had been taken
since the first flight
to space and, since then, had been used for several indications.
A large number of
studies had been performed in the past 30 years in the attempt
to understand how
the human body responds to the lack of gravity.
Microgravity can be simulated on earth by using
head-down-bed-rest
technique (HDBR). This involves sleeping while the body is down
by 6° from
head side. The aim of this study is to compare the
pharmacokinetic parameters of
ibuprofen under head-down-bed-rest technique & normal
position in plasma and
saliva in six healthy human volunteers.
The study has been conducted according to open, completely
randomized,
single dose, two periods, one treatment sequential design, under
fasting conditions
in healthy volunteers. A total number of 6 healthy subjects had
completed the
trial. A wash-out period of 7 days separated the two
periods.
-
`
4
-
`
5
Dedicated to ... My parents
-
`
6
ACKNOWLEDGMENTS
First and foremost, I would like to express my deep and sincere
gratitude
to my supervisory Professor Nasir Idkaidek, Faculty of Pharmacy,
Petra
University, for his guidance, continuous support, encouragement,
and for giving
me the opportunity to work on such an exciting project. His wide
knowledge and
his logical way of thinking have been of great value for me.
I am deeply grateful to my co-supervisor Professor Tawfiq
Arafat, Dean of
Faculty of Pharmacy, Petra University, for his high support and
guidance, which
came always in the right moment. Prof. Arafat opened the doors
for this research
at “Jordan Center for Pharmaceutical Research” where I carried
out my research.
I also want to thank my examination committee members (Prof.
Mohammed Shubair and Dr. Mutasim Al-Gazawi) for their support
and guidance,
which came always in the right moment.
I warmly thank Mr. Hamza Alhorob, Mr. Mahmoud Jamal, Mr.
Ahmad
Abu Awad and Eng. Monther Melhim from Jordan Center for
Pharmaceutical
Research for their valuable advice and friendly help.
The overall support of Petra University is gratefully
acknowledged.
-
`
7
Table of Contents
Contents Page
Title Page 1
Examination Committee 2
Abstract 3
Dedication 5
Acknowledgment 6
Table of Contents 7
List of Figures 11
List of Tables 12
List of Abbreviations 13
Chapter One: Introduction
No. Contents Page
1. Introduction 16
1.1 Physiological Changes in Space 16
1.2 Pharmacological Changes During Space Flight 18
1.3 Current Practice for Use of Medications in Space 19
1.4 Pharmacokinetics in Space 20
1.4.1 Absorption and Bioavailability 20
1.4.2 Distribution 22
1.4.3 Elimination and Clearance 22
-
`
8
1.4.4 Metabolism 23
1.5 Pharmacodynamics in Space 23
1.6 Head-Down-Bed-Rest (HDBR) 24
1.7 Ibuprofen 26
1.8 Objective 27
Chapter Two: Experimental
2. Experimental 29
2.1 Design 29
2.2 Volunteers 30
2.2.1 Selection of Subjects 30
2.2.1.1 Inclusion Criteria 31
2.2.1.2 Exclusion Criteria 31
2.3 Medication 33
2.3.1 Reference Drug 33
2.3.2 Blinding 33
2.4 Dosage and Duration of Treatment 33
2.4.1 Randomization List 34
2.5 Benefit – Risk Evaluation 34
2.6 Study Procedure 35
2.6.1 General Procedure 35
2.6.2 Special Procedures 36
2.6.3 Daily Activities in Each Period of the Trial 36
-
`
9
2.6.3.1 Entry Examination 36
2.6.3.2 Period I of the Trial 37
2.6.3.3 Wash Out 38
2.6.3.4 Period II of the Trial 38
2.6.3.5 Final Examination 39
2.6.4 Restrictions 39
2.6.5 Drug Administration 40
2.7 Assay Method of Ibuprofen 40
2.7.1 Instrumentation 40
2.7.2 Reagents 41
2.7.3 Standards and Stock Solutions 41
2.7.3.1 Preparation of Glibenclamide, (Internal Standard) 41
2.7.3.2 Preparation of Ibuprofen in Plasma 41
2.7.3.3 Preparation of Quality Control Samples in Plasma 42
2.7.4 Description of Method 43
2.7.4.1 Sample Preparation 43
2.7.4.2 Chromatographic Conditions 43
2.7.5 Method Validation 44
2.8 Data Analysis 44
Chapter Three: Results and Discussion
3. Results and Discussion 47
3.1 Plasma Concentrations for All the Volunteers in Normal
and Head-Down-Bed-Rest positions
47
-
`
10
3.2 Data for Maximum Concentrations (Cmax) 57
3.3 Data for K elimination 58
3.4 Data for Area Under the Curve ( AUC) 59
3.5 Data for Volume of Distribution ( V/F ) and
Clearance (CL)
60
3.6 Data and Statistical Comparisons for (AUMClast ) and
(AUMCinf_obs)
62
3.7 Data for ( MRT ) 63
3.8 Pharmacokinetic Parameter Means (CV%) of
Ibuprofen Under Normal and Head-Down-Bed-Rest
Positions
64
Chapter Four: Conclusions
4. Conclusions 68
References 69
Appendices
1 Institutional Review Board (IRB) Approval 72
2 Jordan Food and Drug Administration (JFDA)
Approval
74
3 Informed Constant Form 76
4 Winnonlin Output 89
-
`
11
List of Figures
No. Contents Page
Fig. 1 Fluid Shift from the Lower to the Upper Part of the
BodyInduced by Real and Simulated Weightlessness.
25
Fig 2 Ibuprofen Plasma Concentrations of Volunteer 1 inNormal
and Head-Down-Bed-Rest Positions.
47
Fig 3 Ibuprofen Plasma Concentrations of Volunteer 2 inNormal
and Head-Down-Bed-Rest Positions.
48
Fig 4 Ibuprofen Plasma Concentrations of Volunteer 3 inNormal
and Head-Down-Bed-Rest Positions.
49
Fig 5 Ibuprofen Plasma Concentrations of Volunteer 4 inNormal
and Head-Down-Bed-Rest Positions.
50
Fig 6 Ibuprofen Plasma Concentrations of Volunteer 5 inNormal
and Head-Down-Bed-Rest Positions.
51
Fig 7 Ibuprofen Plasma Concentrations of Volunteer 6 inNormal
and Head-Down-Bed-Rest Positions.
52
Fig 8 Ibuprofen Plasma Concentrations of 6 Volunteers Averagein
Normal and Head-Down-Bed-Rest Positions.
54
-
`
12
List of Tables
No. Contents Page
Table 1 Randomization List. 34
Table 2 Ibuprofen Plasma Concentrations (µg/ml) after 600 mgOral
Dose in 6 Volunteers in Normal Position.
55
Table 3 Ibuprofen Plasma Concentrations (µg/ml) after 600 mgOral
Dose in 6 Volunteers in Head-Down-Bed-RestPosition.
56
Table 4: Cmax and Tmax in Both Phases for All the
Volunteers.
57
Table 5: Kel in Both Phases for All the Volunteers. 58
Table 6.a AUClast, AUC0-4, AUCinf_obs and AUC_%Extrap
inHead-Down-Bed-Rest Phase for All the Volunteers.
59
Table 6.b AUClast, AUC0-4, AUCinf_obs and AUC_%Extrap inNormal
Phase for All the Volunteers.
60
Table 7 V/F and Cl/F in Both Phases for All the Volunteers.
61
Table 8 AUMClast and AUMCinf_obs in Both Phases for All
theVolunteers.
62
Table 9 MRT in Both Phases for All the Volunteers. 63
Table 10 Pharmacokinetic Parameter Means (CV%) of IbuprofenUnder
Normal and Head-Down-Bed-Rest Positions.
64
-
`
13
List of Abbreviations
µG MicrogravityABR Anti-orthostatic Bed RestADME Absorption,
Distribution, Metabolism, ExcretionADR Adverse Drug ReactionAE
Adverse EventALC EthanolART Adverse Reaction TerminologyAUC Area
Under Plasma Concentration-Time CurveAUMC Area Under Moment CurveBA
BioavailabilityBE BioequivalenceBILI BilirubinBMI Body Mass IndexBP
Blood PressureCa CalciumCLR Renal ClearanceCmax Maximal Plasma Drug
ConcentrationCNS Central Nervous SystemCp Concentration PointCREA
CreatinineCRF Case Report FormGCP Good Clinical PracticeGIT
Gastrointestinal TractGMP Good Manufacturing Practicehr HourHR
Heart RateHB HemoglobinHBS-AG Hepatitis B AntigenHcvg Hepatitis C
AntigenHDBR Head-Down-Bed-Rest
-
`
14
HIV Human Immunodeficiency VirusHPLC High Performance Liquid
ChromatographyIEC Independent Ethics CommitteeIRB Institutional
Review Boardi.v IntravenousJCPR Jordan Center for Pharmaceutical
ResearchJFDA Jordan Food and Drug AdministrationK PotassiumKel
Terminal Rate ConstantLLOQ Lower Limit Of Quantificationmin.
MinuteMRT Mean Residence TimeNa SodiumNASA National Aeronautics and
Space AdministrationPBC PlateletspH Hydrogen Ion ConcentrationPK
Pharmacokinetic ParameterRBC Red Blood CountSAE Serious Adverse
EventSMS Space Motion SicknessSOP Standard Operating ProcedureT
Timet0.5 Terminal Elimination Half –LifeTmax Time of Maximum Plasma
Drug ConcentrationVd Volume of DistributionWBC White Blood CountWHO
World Health Organization
-
`
15
Chapter 1:
Introduction
-
`
16
1. Introduction:
Space medicine is a new field that is growing fast as the
international
space station becomes a reality. Medications had been taken
since the first flight
to space and, since then, had been used for several indications
such as space
motion sickness, sleeplessness, headache, nausea, vomiting, back
pain, and
congestion. As the duration of space missions get longer, it is
even more likely
that astronauts will encounter some of the acute illnesses that
are frequently seen
on Earth. Microgravity environment induces several physiological
changes in the
human body.
National Aeronautics and Space Administration (NASA) has
ongoing
studies on how the astronauts' health is affected by space
travel, & how the
gravity affects the pharmacokinetics of the medications
The gravity may define as the force that attracts a body toward
the center
of the earth, while microgravity is a condition, especially in
space orbit, where
the force of gravity is so weak that weightlessness results.
1.1 Physiological Changes in Space:
Exposure to the microgravity (µG) environment of space flight
causes
several physiological changes to the body. These changes are
believed to occur in
two phases : The initial response phase takes place during the
first 3 to 6 weeks of
flight, when gradual readjustments in all body systems take
place. This phase is
characterized by changes in neurovestibular receptors,
sympathetic and
parasympathetic function, fluid volume, metabolism,
hemodynamics, and
-
`
17
endocrine regulation. One of the most noticeable changes early
in flight is the
fluid shifts. Fluids are redistributed from the extremities to
the upper body and
neck region, causing two common syndromes called “bird legs” and
“puffy face”
(Nicogossian et al 1994).
This fluid shift causes heart to enlarge in order to handle the
increased
blood flow. This "flooding" in the upper part of the body causes
the body -
through negative feedback - to correct this situation by getting
rid of some of the
excess fluids. The human becomes less thirsty than normal, and
the kidneys
increase the output of the urine. Both these actions decrease
the over all quantity
of fluids and electrolytes. Once the fluid level decreases, the
heart shrinks back to
its normal shape and size.
This decrease in fluid volume leads to electrolyte imbalance and
decrease
the plasma volume (Blood volume may decrease by 10 %) (Edgar et
al 2004).
The adaptation phase begins after several months in space. It is
during this
period that changes such as regional bone and muscle mass loss,
changes in
neurotransmitter and receptor functions, and perhaps decreased
immune responses
and central nervous system (CNS) function take place(Edgar et al
2004).
A large number of studies had been performed in the past 30
years in
attempt to understand how the human body responds to the lack of
gravity. As of
today, most of the physiological changes experienced in space
have been fairly
well characterized and understood. Countermeasures to the most
significant ones,
such as cardiovascular deconditioning, loss of plasma volume,
and muscle and
-
`
18
bone degeneration are being developed and tested. It is not the
scope of this work
to review the details of all the physiological changes observed
in space.
Several general and specific reviews (Graebe et al 2004, Zhang
LF 2001,
Wang et al 2001, Watenpaugh DE 2001, Harm et al 2001 and Fitts
et al 2000) had
been published recently. These publications should be consulted
for a more
detailed explanation of all the physiological alterations that
occur as a
consequence of adaptation to space µG.
1.2 Pharmacological Changes During Space Flight:
Pharmacological effects can be viewed as the result of
pharmacokinetic
(PK) and pharmacodynamic (PD) contributions. Pharmacokinetics
deals with
what the body does to the drug. It describes the time course of
drug and
metabolite concentrations in the body. Pharmacodynamics
describes the
relationships between pharmacological effects and
drug/metabolite
concentrations. The combination of the two, PK-PD modeling,
leads to the
identification of the optimum dose and dosage regimen to achieve
the desired
therapeutic effect. For many drugs, the relationship between PK
and PD has been
studied in normal gravity. However, the established normal
gravity dosing
recommendations may not be applicable in space because of
possible changes in
PK or PD or both.
As previously indicated, space travel induces several
physiological
changes in the human body. The first signs of exposure to a
zero-gravity
atmosphere include symptoms such as headache, nausea, vomiting,
congestion,
back-pain, and sleeplessness. Space motion sickness (SMS), as is
commonly
-
`
19
known, is experienced by 50% or more of astronauts during the
first few days of
exposure to the µG environment of space. It is no surprise that
since the first
mercury flight in 1967, medications have been a common and
necessary part of
space missions.
1.3 Current Practice for Use of Medications in Space:
All pharmacological agents that are used on the shuttle are
carefully
reviewed for potential benefits as well as potential negative
effects on the
individual or the mission. Astronauts test all frequently used
medications before
mission assignment, to identify potential side-effects,
performance-related
problems, and individual therapeutic effect.
This procedure helps to evaluate the effect of these medications
in space,
although precise predictions are still not possible. Critical
issues such as “What
are the pharmacodynamics and pharmacokinetics of drug therapy
in
weightlessness?” and “What drug forms, administration routes,
and treatment
regimen must be used to optimize therapeutic intervention in
weightlessness?” are
still largely unknown.
For example, the crewmembers’ responses to their preferred
sleeping
medication are evaluated preflight to determine any side effects
or idiosyncratic
reactions. Different doses are tested in each individual to
adjust for the decreased
bioavailability of drugs as a result of alterations in
gastrointestinal function in µG
(Santy et al 1988).
Most of the medications taken during space flight were taken for
space
motion sickness (SMS), sleep disturbances, headache, backache,
and sinus
-
`
20
congestion. Commonly used sleep medications were temazepam,
zolpidem,
triazolam, and flurazepam. The medications taken for pain were
acetaminophen,
aspirin and ibuprofen. Promethazine was the predominant
medication used for
SMS, either by itself, or in combination with dextroamphetamine
(Putcha et al
1999).
1.4 Pharmacokinetics in Space:
1.4.1 Absorption and Bioavailability:
Drug absorption from gastrointestinal tract (GIT) depends on
many factors
such as gastric emptying rate, intestinal motility, blood
perfusion and mean
residence time. Gastric emptying rate depends on volume of the
meal,
temperature of food, body position and also earth gravity.
Similarly, intestinal
motility, blood perfusion and mean residence time will also
change at
microgravity.
The oral route is generally preferred for administering drugs.
However,
experience with the administration of medications in the µG
environment has
stimulated a reevaluation of the relative advantages and
disadvantages of the
various dosage forms formulations. Few data exist on
bioavailability in space, but
(Pool SL and Nicogossian A 1983) showed that a few orally
administered
medications taken during flight were less effective than
expected.
Preflight and in-flight salivary levels of acetaminophen where
shown to
differ, probably due to changes in gastrointestinal transit
time. In-flight salivary
concentration-time curves of scopolamine /dextroamphetamine,
given as
conventional oral tablets, also were shown to be erratic and
exhibited higher intra-
-
`
21
and inter-individual variability compared to those of preflight
data (Cintron et al
1987).
Of all factors that can influence the absorption of orally
administered
drugs, the rate of absorption may be the most variable parameter
noted in space
(Benet LZ. 1988). Gastric emptying is highly influenced by
several factors:
volume, calories, exercise, size and density of particles,
temperature, viscosity,
and osmolality, and factors associated with physiologic
responses (such as
splanchnic blood flow, body position, and electrolyte balance).
Gastric emptying
in µG can also be altered by changes in particle size
discrimination by the
stomach, which is strongly dependent on the force of
gravity.
Also, particles are no longer restricted to the lower pyloric
region of the stomach
by gravity, but move throughout all regions of the stomach. This
array of factors
can lead to variability in drug plasma levels. Another important
consideration
concerning gastric emptying is the effect of motion sickness
(Amidon et al 1991).
Stewart (Stewart et al 1994) showed that motion sickness can be
considered the
major source of gastric stasis in space. By using nuclear
medicine techniques,
Stewart et al observed that the additive effect of scopolamine
and promethazine
on gastric emptying in Malaise-III (M-III) subjects was little,
confirming the
strong inhibitory effect of motion sickness on gastric
motility.
Intestinal transit rate in a gravity environment is highly
dependent on the
motility state of the GI tract either fasted or fed partly
because of the higher
viscosity of chyme in the fed state. In space, the absence of
gravity may tend to
increase the transit rate along the small intestine by
decreasing the dimensionless
-
`
22
ratio of gravitational forces to viscous forces. In zero
gravity, therefore, these
alterations in GI emptying and intestinal transit rate could
lead to inefficient
absorption and erratic plasma levels.
1.4.2 Distribution:
Physiological changes like the decrease in total body water and
plasma
volume, tissue perfusion, and muscle mass loss may alter the
volume of
distribution of drugs. This may have an impact on the plasma and
tissue
concentrations achieved after administering a drug in space, and
depending on the
magnitude of the change, may require a completely new dosing
scheme to be
designed to avoid subtherapeutic or toxic concentrations.
Drug binding in blood occurs to different structures as plasma
proteins,
lipids and erythrocytes. As only the unbound fraction of drug is
active, changes in
total plasma proteins will affect pharmacokinetics. During space
flight no
significant changes in plasma protein concentrations had been
observed
(Nicogossian et al 1994), but a reduction in red blood cell mass
(hemoglobin and
number of erythrocytes) is reported. Altered tissue binding is
observed as a result
of protein loss, muscle atrophy and decrease in lean body mass
(Edgar et al 2004).
1.4.3 Elimination and Clearance:
Clearance is defined as the volume of blood cleared per time
unit, and
hence, can be expressed as the product of blood flow across an
eliminating organ
and the respective extraction ratio. Because plasma volume is
decreased during
space flight there might be a possibility of changes in organ
perfusion. Studies in
anti-orthostatic bed rest did not show a significant change in
hepatic blood flow or
-
`
23
effective renal plasma flow. However, this may be because of
differences in the
underlying mechanisms that cause the fluid shifts in
ground-based models and in
space flight. Therefore, these studies need to be confirmed in
space before any
conclusions can be made (Edgar et al 2004).
1.4.4 Metabolism:
Amounts of cytochrome P-450 isoforms and other enzymes were
shown to
decrease during space flight and simulated µG, suggesting that
metabolism may
also be altered by space flight (Merrill et al 1990).
Although generalized predictions of the effect of µG on drug
metabolism
cannot be made based on these observations, these alterations
could result in
higher plasma levels of some drugs, especially low- extraction
drugs, and
increased incidence of adverse effects.
1.5 Pharmacodynamics in Space:
Little is known about the effect of µG on pharmacodynamics.
Pharmacodynamic changes due to microgravity are hard to evaluate
since the
dose-response relation is a hybrid: it depends on
pharmacokinetic characteristics,
pharmacodynamic characteristics or both.
The pharmacological changes that may be observed during space
flights are more
likely to be resulting from the physiological perturbations that
arise from
exposure to µG. Intra and inter-individual variability in
pharmacological response
to medications can also be caused by factors such as stress and
lack of sleep.
-
`
24
1.6 Head-Down-Bed-Rest (HDBR):
Microgravity can be simulated on earth by using
head-down-bed-rest technique.
This involves sleeping while the body is down by 6° from head
side. Head-Down-
Bed-Rest (HDBR) has proved its usefulness as a reliable
simulation model for the
most physiological effects of spaceflight. As well as continuing
to search for
better understanding of the physiological changes induced,
upward fluid shift,
unloading the body’s upright weight, absence of work against
gravity, reduced
energy requirements and reduction in overall sensory
stimulation.
The upward fluid shift by acting on central volume receptors
induces a
10–15% reduction in plasma volume, Calcium excretion is
increased from the
beginning of bed rest leading to a sustained negative calcium
balance. Calcium
absorption is reduced. Body weight, muscle mass, muscle strength
is reduced.
Bone density, stiffness of bones of the lower limbs and spinal
cord and bone
architecture are altered (Pavy-Le et al 2007).
Bed rest, ranging from several hours to several weeks or months,
has been
the model most frequently used to simulate the physiological
effects of
weightlessness, in particular on the cardiovascular system and
body fluid
regulation. Most experiments since 1986 were performed using the
–6 degree
HDBR model, in male volunteers. Bed rest induces a fluid shift
from the lower to
the upper part of the body (Fig. 1a, b). This fluid shift
results in a transient
increase of plasma volume, as more fluid moves into the vascular
compartment
from the lower body than that is filtered out of capillaries
into the upper body
(Pavy-Le et al 2007).
-
`
25
Fig. 1 This shows the fluid shift from the lower to the upper
part of the bodyinduced by real (a) and simulated weightlessness
(b) (Pavy-Le et al 2007).
-
`
26
1.7 Ibuprofen:
Ibuprofen is a non-steroidal anti-inflammatory agent used in
painful and
inflammatory conditions. It is usually given 3 to 4 times daily
in a dose of 200 -
800 mg. It is an inhibitor of cyclo-oxygenase enzyme. The usual
dose by mouth is
1.2 to 1.8 gm daily in divided doses; if necessary the dose may
be increased to 2.4
gm daily.
The main adverse effects are gastro-intestinal disturbances;
reactions
range from abdominal discomfort, nausea and vomiting, and
abdominal pain to
serious gastro-intestinal bleeding or activation of peptic
ulcer. Central Nervous
System (CNS) related side effects include headache, dizziness,
nervousness,
depression, drowsiness and insomnia. Hypersensitivity reactions
may occur and
include fever and rashes. Ibuprofen or other non-steroidal
anti-inflammatory
drugs should not be given to patients with active peptic
ulcer.
Pharmacokinetics: Ibuprofen is rapidly absorbed after oral
administration,
with peak serum or plasma levels generally appearing within 1.5
to 2 hours. Oral
absorption is estimated to be 80% of the dose. Both the rate of
absorption and
peak plasma concentrations are reduced when the drug is taken
with food, but,
bioavailability as measured by total area under the
concentration-time curve is
minimally altered.
Ibuprofen has an elimination half-life of approximately 2 hours.
It is
rapidly metabolized through oxidation and glucuronic acid
conjugation with
urinary excretion of the inactive metabolites usually complete
within 24 hours.
-
`
27
Less than 10% is excreted unchanged in the urine. Clinical
studies indicate
duration of clinical effect for up to 8 hours for fever and 6
hours for pain.
The therapeutic concentration of Ibuprofen is 20 to 30 mg/L
(Kleinbloesem et al 1995).
1.8 Objective:
The aim of this study is to compare the pharmacokinetic
parameters of
ibuprofen under Head-Down-Bed-Rest technique & normal
position in plasma
and saliva in six healthy human volunteers.
Ibuprofen will be used as model drug since no previous ground
studies were
performed on it. Hence, our results can help understand more the
effects of
microgravity conditions on pharmacokinetics and if needed to
correct the dose
regimens for ibuprofen to be used in flight by crew members.
-
`
28
Chapter2:
Experimental
-
`
29
2. Experimental:
2.1 Design:
The study has been conducted according to open, completely
randomized,
single dose, two periods, one treatment sequential design, under
fasting conditions
in healthy volunteers.
A total number of 6 healthy subjects had completed the trial. A
wash-out period
of 7 days was left between the two periods.
Under HDBR the volunteers were rested in a 6° head-down tilt
position in
which subject has been able to eat and urinate. The selected
subjects had been
randomized to receive a single 600 mg oral dose of Ibuprofen
after a 10 hour
overnight fasting, in two different occasions: during a normal
position and during
HDBR position.
The normal phase lasted 8 hours of sample and data collection
and the
HDBR phase lasted 18 hours; 10 hours prior to drug
administration and 8 hours of
data collection thereafter.
After volunteers received the dose by 4 hours, they had their
first meal and
the second meal was after finishing blood sample collection.
Subjects were
allowed to consume water all over the study.
Subjects were allowed to rest on an elbow for about 20 minutes
during
meals, Physiological (BP, heart and respiratory rate) were
monitored every 4
hours during wake hours, Labs (cell counts, differential,
electrolytes, liver
enzymes, etc.) were measured once at admission and once
immediately at the end
of the HDBR phase.
-
`
30
Saliva samples (0.5-3 ml) & blood samples (5 ml) were
collected at the
following times: pre-dose, and 0.25, 0.5, 0.75, 1, 1.33, 1.66,
2, 2.5, 3, 4, 5, 6 and 8
hours post dosing. Plasma was immediately separated by
centrifugation and all
samples stored at -20º C until analysis.
2.2 Volunteers:
Six healthy volunteers participated in a randomized sequential
design
clinical study to evaluate and compare the pharmacokinetics of
ibuprofen after a
single oral dose under head-down-bed-rest position and normal
position.
The experiment details and a written informed consent were
provided to
volunteers for their approval. However, the study was started
after IRB and JFDA
approvals. (Appendices 1, 2&3)
Each candidate was subjected to a screening examination
including
medical history and physical examination, complete blood count
& clinical blood
chemistry.
Subjects were non-smokers, non-obese, with no history of
migraine,
recurrent headaches, clotting disorders, no history of gastric
or duodenal ulcers or
drug allergies, and in good general health as accessed by the
physical examination
and laboratory results. Also, subjects were tolerant to HDBR
position.
2.2.1 Selection of Subjects:
Six subjects, who fulfilled the inclusion criteria (Section
2.2.1.1), do not
present any of the exclusion criteria (Section 2.2.1.2), had
been entered into the
study.
-
`
31
Drug assays and statistical analysis of the data had been
performed on all
plasma samples of the subjects who completed the study according
to the
protocol. Subjects had been recruited from the volunteer pool of
Jordan Center
for Pharmaceutical Research.
The criteria were set to ensure a homogeneous subject population
without
accompanying diseases interfering with the conduct and
scientific evaluation of
the study. Additionally, the criteria had been selected to
minimize risk to the
subjects’ well-being.
2.2.1.1 Inclusion Criteria:
Only subjects presenting all of the following criteria had been
enrolled in
the trial:
• Subject agrees to eat during HDBR position.
• Age between 18 and 50 years.
• Physically and mentally healthy as judged by means of a
medical and standard
laboratory examination.
• Weight not less than 60 kg.
• No allergic history to ibuprofen.
• Body weight within ±10% of the ideal body weight in relation
to height
according to the Body Mass Index: (BMI = Weight (kg) / Height
(m) 2, (17.1
to 28.6)).
2.2.1.2 Exclusion Criteria:
Subjects presenting any of the following had not been included
in the
trial:
-
`
32
• Subjects with a baseline pressure less than 110/60 mm Hg
before dosing while
in HDBR position.
• Any clinically significant allergic disease.
• Any history or presence of Ibuprofen or other NSAIDS induced
peptic ulcer.
• History of allergic response to Ibuprofen or other NSAIDS.
• Presence or a history of clinically significant
cardiovascular, renal, hepatic,
pulmonary, metabolic, endocrine, hematological,
gastrointestinal, neurological,
psychiatric or other major disease.
• Clinically significant illness within 4 weeks before the start
of the study.
• Intake or administration of any prescribed systemic or topical
medication
within 2 weeks prior to the start of the study.
• Concomitant intake or administration of any systemic or
topical drugs.
• Treatment with any investigational drug (i.e. drug not yet
approved) in the last
3 months before beginning of the trial.
• Participation in another clinical trial within the last 2
months.
• Treatment with drugs known to alter the major metabolic
systems such as
barbiturates, phenothiazines, cimetidine, omeprazole etc. within
the last 30
days.
• Major surgery of the gastrointestinal tract except for
appendectomy.
• Donation of blood or plasma within the last two months.
• Supine blood pressure, after resting for 5 min, higher than
140 /90 or lower
than 90/60 mmHg.
• Supine pulse, after resting of 5 min, outside the range of
60-90 beats /min.
-
`
33
• Smoking.
• Consumption of more than 4 cups of Coffee or equivalent per
day.
• Vegetarian.
• Knowledge to have a hepatitis B infection or carrier of the
respective antigens
(HBs Ag, positive).
• Evidence of an uncooperative attitude.
• Alcohol Abuse.
2.3 Medication:
The study medication was manufactured by The Boots Company
PLC
Nottingham, England, according to GMP-requirements.
2.3.1 Reference drug:
• Name: Brufen® oral tablet 600 mg.
Each tablet containing 600 mg of Ibuprofen as active
ingredient.
• Mode of administration: oral administration of one tablet in
the morning
with 240 ml tap water.
• Batch-No: 21V
• Expiry date: 06/2011
2.3.2 Blinding:
No blinding was planned.
2.4 Dosage and Duration of Treatment:
After an overnight fast of 10 hours, all subjects received a
single oral dose
of 600 mg Ibuprofen in the morning of each period of the trial,
given as one tablet
of the reference preparation, under HDBR body position during
first period of the
-
`
34
study and under normal body position during second period of the
study. The first
period of the trial has been followed after a wash-out of seven
days before the
second period of the trial.
Before administration of study medication on clinic days, the
Principal or
the Clinical Investigator checked each unit and label against
the randomization
schedule and also ensured that the subject number on the label
corresponds to the
number allocated to each recipient.
2.4.1 Randomization List:
Table 1: Randomization List
Subject No. Period I Period II
01 HDBR N
02 HDBR N
03 HDBR N
04 HDBR N
05 HDBR N
06 HDBR N
HDBR: Head down bed rest body position N: Normal body
position
2.4 Benefit – Risk Evaluation:
The efficacy and safety of Ibuprofen as an active ingredient
has
been proved in clinical trials. The Brufen® oral tablet 600 mg
Ibuprofen is
produced by Knoll.
A healthy subject had taken two doses each containing 600 mg
Ibuprofen
of one products with 7 days interval was very small. Mild and
minimal adverse
-
`
35
events when occurred, from the study medications or study
procedures were
expected in this study.
The planned procedures within the present trial also represent
no special
risk to the volunteers. All volunteers had been subjected to
safety examinations.
The entry examination had been carried out 14 days before the
beginning of the
trial and the final examination on the day of last sampling
thereafter. Blood
samples (total number of 28 blood samples for 2 periods, 5 ml
each) for drug
analysis had been taken at the following times: pre-dose, 0.25,
0.5, 0.75, 1, 1.33,
1.66, 2, 2.5, 3, 4, 5, 6 and 8 hours post dosing. A total blood
loss of approximately
150 ml (including laboratory examinations) per volunteer was to
be expected.
In general, blood loss could provoke faintness, dizziness,
thirst, sweating,
weak and rapid pulse, rapid respiration, orthostatic hypotension
and eventual
decrease in some laboratory parameters such as red blood cells
and hemoglobin.
Having in mind that the blood loss in the present trial had
taken place over a
period of two weeks, the risk for the volunteers to experience
one of the upper
side effects was relatively low.
2.6 Study Procedure:
2.6.1 General Procedure:
The entry examination was carried out before the beginning of
the trial by
14 days and the final examination on the day of last sampling.
All laboratory tests
were carried out at Al Mowasah Hospital laboratories.
The subjects attended the clinic at 7:00 pm at night on the day
before dosing
(day 0 in each study period), and remained there for 8 hours
after dosing.
-
`
36
In the morning of day one the volunteers received the trial
medication under
fasting conditions. The volunteers had to fast from food for 10
hours before and
until 4 hours after administration of study medication on day
1.
At the end of period II, standard clinical examination performed
for each and
every subject.
2.6.2 Special Procedures:
All subjects had been at HDBR body position for the whole
duration of
period I (around 18 hours), while they had been in normal body
position during
period II.
2.6.3 Daily Activities in Each Period of the Trial:
2.6.3.1 Entry Examination:
The entry examination carried out before the beginning of the
trial by 14
days. Following parameters were documented and /or
investigated:
• Thorough explanation of the study medication from the
Investigators.
• Date of inclusion (date of signing the informed consent).
• Date of examination.
• Inclusion criteria (according to protocol).
• Exclusion criteria (according to protocol).
• Informed consent.
• Demographic data: date of birth, ethnic group, sex, height,
weight, BMI.
• Additional information concerning: illness within the last 4
weeks prior
start of the trial, last participation in any clinical trial,
last donation of
blood or plasma, last administration of any medication
(including OTC or
-
`
37
topical medication), last administration of drugs known to alter
the major
organs or systems as well as specification of the drug name,
dosage, start
and end of treatment.
• Vital signs: registration of body temperature, measurements of
supine
heart rate (HR) and blood pressure (BP) after 5 minutes supine
rest.
• Physical examination.
• Laboratory examination of blood which includes Blood
hematology,
Blood chemistry and check for presence of Hepatitis B, C, and
HIV.
• Urinalysis which includes, pH, protein and glucose (semi
quantitatively)
and evaluation of sediment.
A blood sample of 10 ml was taken for laboratory screening
before the
study. Both drug abuse test and alcohol test had been done
before the two periods
of the study. ECG had been done before the study.
2.6.3.2 Period I of the Trial:
Day 0: This day is the day before administration of study
medication, for this
purpose the subjects had to attend to the clinic at 7:00 pm.
The following procedures were performed and documented in case
report form
(CRF) on this day:
• Urine drug screen
• Alcohol test in saliva
• Check of exclusion criteria, adverse events and concomitant
medication,
• Evening snack not later than 7.30 p.m.,
• Overnight stay in the clinic.
-
`
38
• They started the HDBR body position directly after the snack
in day 0.
Day 1: The following procedures carried out for HDBR body
position on this
day:
• A venous cannula was inserted and 5 ml blood sample was drawn
before the
morning dose.
• Measurement of blood pressure
• Administration in the morning of day 1 of an oral single dose
of one tablet
of the reference drug Brufen® with 240 ml tap water while
seating on bed in
the upright position then return to HDBR body position after 5
minutes of
the dose.
• Saliva and blood sampling was continued at the following
times: pre-dose,
and 0.25, 0.5, 0.75, 1, 1.33, 1.66, 2, 2.5, 3, 4, 5, 6 and 8
hours.
• Breakfast 4 hours post dose (volunteers had to eat up the
meals while
seating on beds in the upright position during period one of the
study,
volunteers had to eat their meals in 15 minutes then returned to
HDBR body
position directly).
• Standard lunch 8 hours post dose (after last blood sample) was
given.
• Discharged from hospital 8 hours post dose.
2.6.3.3 Wash Out:
7 days from Day 1
2.6.3.4 Period II of the Trial:
It was exactly the same as period I while at normal body
position.
-
`
39
2.6.3.5 Final Examination:
The final examination carried after the end of period II. The
following
parameters were documented and /or investigated:
• Date of examination.
• Check of exclusion criteria.
• Physical examination.
• Registration of vital signs.
• Registration of adverse events
2.6.4 Restrictions
Volunteers were requested not to undertake vigorous exercise
beginning 2
days before the entry screening laboratory test until after the
final examination.
The chewing of chewing gum was not allowed on the days of
dosing. Smoking
was restricted. Foods and beverages containing xanthines or
grapefruit were
prohibited 7 days before dosing until the final sampling time.
Alcohol
consumption was prohibited 48 hours before dosing until the
final sampling time.
The volunteers had not take any prescribed medicine or over the
counter
medications at least 2 weeks before the beginning of the study.
The subjects were
fast from food and beverages other than water, for at least ten
hours, from 8:00
pm on the evening before dosing (Day 0) until breakfast on the
following day
(Day 1). Volunteers were requested to restrict their movements
as much as
possible while at HDBR body position during first period of the
study. Volunteers
were allowed to lie, sit or walk after administrating the dose
except the first 4
-
`
40
hours after the dose where the volunteer should stay seated on
chair in the upright
position while at normal body position during second period of
the study.
2.6.5 Drug Administration
The precise instructions for drug administration were given to
subjects by the
investigators.
All subjects received in each period of the trial a single dose
of 600 mg Ibuprofen of
the reference drug Brufen®. The drug administrations were
separated by a washout
period of 7 days. Volunteers swallowed the tablet of the
reference preparation with
240 ml of water while seating on bed in the upright position
then return to HDBR
body position after 5 minutes of the dose during period one of
the study.
2.7 Assay Method of Ibuprofen:
All samples analyzed by HPLC method, Mean of Ibuprofen
concentration
versus time curves generated in Microsoft Excel for plasma, in
both normal phase
and HDBR phase.
The procedure and analysis was done at Jordan Center for
Pharmaceutical
Research.
2.7.1 Instrumentation:
A Dionex HPLC auto-sampler system was used and composed of
the
following:
• A constant solvent delivery system (P580).
• A 100 µL fixed volume injector (Rheodyne 7125).
• UV Detector (UVD340S).
• Autosampler (ASI-100).
-
`
41
• Computer System, Windows2000, Chromeleon Chromatography
Management System.
• Thermo Electron Corporation, BDS Hypersil C18 Column (150 x
4.6 mm),
5 µ.
2.7.2 Reagents:
• Methanol and Acetonitrile of HPLC grade (ACR S)
• Glacial acetic acid.
• Deionized Water (Nanopure)
• Human Plasma (harvested from donors)
2.7.3 Standards and Stock Solutions:
• Ibuprofen, a concentrated stock solution was prepared in
Methanol (2000
g/ml).
• Glibenclamide, a concentrated stock solution was prepared in
Methanol.
(1000 g/ml).
2.7.3.1 Preparation of Glibenclamide, (Internal Standard):
10 mg of Glibenclamide was dissolved in 10 ml of Methanol;
solution (A),
this contains 1000 g/ml. 0.3 ml of solution (A) was taken and
diluted to 100 ml of
Methanol; solution (B), which contains 3.0 µg/ml. Solution (B)
is considered to be
working solution contains 3.0 µg/ml of Glibenclamide.
2.7.3.2 Preparation of Ibuprofen in Plasma:
Spiked plasma samples were prepared by taking 20 mg of Ibuprofen
in 10 ml of
Methanol, (solution A), which contains 2000 g/ml of Ibuprofen.
1.0 ml from solution
-
`
42
(A), which contains 2000 g/ml was taken and diluted to 20 ml of
Plasma, solution (B),
which contains 100 g/ml of Ibuprofen (solution B).
From solution B, which contains 100.0 g/ml the following
dilutions were
prepared:
0.05 ml to 10 ml plasma ‡ 0.5 g/ml ….. STD 1
0.10 ml to 10 ml plasma ‡ 1.0 g/ml ….. STD 2
0.20 ml to 10 ml plasma ‡ 2.0 g/ml ….. STD 3
0.50 ml to 10 ml plasma ‡ 5.0 g/ml ….. STD 4
1.00 ml to 10 ml plasma ‡ 10.0 g/ml ….. STD 5
2.00 ml to 10 ml plasma ‡ 20.0 g/ml ….. STD 6
3.00 ml to 10 ml plasma ‡ 30.0 g/ml ….. STD 7
Samples of the standard curve in plasma were prepared using
seven
concentrations, not including zero these concentrations are:
0.5, 1.0, 2.0, 5.0, 10.0, 20.0 AND 30.0 g /ml.
Each concentration of the plasma sample was divided to 0.20 ml
in an eppendorf
tube and kept at – 20 0C, standard samples were given daily to
gather with the
quality control samples.
2.7.3.3 Preparation of Quality Control Samples (Q.C) in
Plasma:
Spiked plasma samples were prepared by taking 20 mg of Ibuprofen
in 10 ml of
Methanol, (solution A), which contains 2000 g/ml of Ibuprofen.
1.0 ml from solution
(A), which contains 2000 g/ml was taken and diluted to 20 ml of
Plasma, solution (B),
which contains 100 g/ml of Ibuprofen (solution B).
-
`
43
From solution B, which contains 100.0 g/ml the following
dilutions were
prepared:
0.30 ml to 20 ml plasma‡ 1.5 g/ml ….. (QC Low)
3.00 ml to 20 ml plasma‡ 15.0 g/ml ….. (QC Mid)
5.00 ml to 20 ml Plasma‡ 25.0 g/ml ….. (QC High)
Quality Control Samples were kept at - 20 0C until required for
subsequent
analysis.
2.7.4 Description of Method:
2.7.4.1 Sample Preparation:
A 0.20 ml of plasma was add to 0.35 ml of 3.0 g/ml Glibenclamide
prepared in
Methaol in an Eppendorf, the mixture was vortex-mixed for 30
seconds, then
centrifuged for 15 minutes at 14000 rpm. 200 l was transferred
to flat bottom insert, 30
l was injected on BDS, C-18 Column. Ibuprofen and the internal
standard were
separated from endogenous substances.
2.7.4.2 Chromatographic Conditions:
• Column: Thermo Electron Corporation, BDS Hypersil, C18, (150 X
4.6 mm
i.d).
• Solvent system: 65 % Acetonitrile, 35 % Water, 150 l of
Glacial acetic acid
per one liter of mobile phase, pH = 4.35
• Detection: UV Detector = 230 nm.
• Injection volume: 30 microliters.
• Flow Rate: 1.0 ml/min.
• Retention time for Ibuprofen: 4.0 – 4.5 minutes.
-
`
44
• Retention time for Glibenclamide: 3.0 – 3.5 minutes (Internal
Standard)
(Retention times dependent upon HPLC conditions).
2.7.5 Method Validation:
To guarantee reliability and reproducibility of the assay for
quantitation of
Ibuprofen in human plasma, the method was validated in
concordance with the FDA
guideline requirements in Jordan Center for Pharmaceutical
Research (JCPR). The
method was evaluated for linearity, sensitivity, selectivity,
accuracy, precision, and
stability.
The method was sensitive for Ibuprofen. The variability in
concentrations at
LLOQ of 0.5 µg/ml was within the acceptable limits of precision
(4.72%) and
accuracy (100.94%), and LLOQ intensities were 5 times of the
blank in all
samples. (US FDA, Guidance for Industry: Bioanalytical Method
Validation, 2011).
2.8 Data Analysis:
Pharmacokinetic parameters were determined by standard non-
compartmental estimation method using Winnonlin software V 5.2 .
They include
the following parameters:
• AUC: Area under the curve.
• Cmax: Maximum concentration of drug in plasma.
• Tmax: Time to achieve Cmax.
• Kel: Elimination rate constant.
• t0.5: Half life.
• V: Volume of distribution.
• CL: Clearance.
-
`
45
• MRT: Mean residence time.
• AUMC: Area under moment curve.
Statistical comparisons for the above parameters were performed
by t-test
using Excel program. Friedman design was applied for Tmax
comparison using
Kinetica. 0.05 level of significance was used for all
comparisons. For P values
less than 0.05, significant difference was concluded.
-
`
46
Chapter 3:
Results and Discussion
-
`
47
3. Results and Discussion:
3.1 Plasma Concentrations for All the Volunteers in Normal (N)
and HDBR
Positions:
In the first volunteer the Tmax at HDBR was faster than it at
normal position,
(Tmax at HDBR was 0.75 hr, while Tmax at normal position was
1.66 hr) and Cmax
was higher at HDBR than it at normal position, (Cmax at HDBR was
48.316 µg/ml,
while the Cmax for normal position was 39.242 µg/ml. (Fig 2,
Table 2, Table 3)
05
10152025303540455055
0 2 4 6 8 10Time (hr)
Con
c (u
g/m
l)
1 N1 HDBR
Fig 2: Ibuprofen plasma concentrations of volunteer 1 in normal
(N) and HDBRpositions
-
`
48
In the second volunteer the Tmax at HDBR was faster than it at
normal
position, (Tmax at HDBR was 0.50 hr, while Tmax at normal
position was 2.50 hr)
and Cmax was slightly higher at HDBR than it at normal position,
(Cmax at HDBR
was 38.149 µg/ml, while the Cmax for normal position was 39.096
µg/ml). (Fig 3,
Table 2, Table 3)
05
10152025303540455055
0 2 4 6 8 10Time (hr)
Con
c (u
g/m
l)
2 N2 HDBR
Fig 3: Ibuprofen plasma concentrations of volunteer 2 in normal
(N) and HDBRpositions
-
`
49
In the third volunteer the Tmax at HDBR was also faster than it
at normal
position, (Tmax at HDBR was 0.75 hr, while Tmax at normal
position was 1.33 hr)
and Cmax was slightly higher at HDBR than it at normal position,
(Cmax at HDBR
was 35.631 µg/ml, while the Cmax for normal position was 36.553
µg/ml). (Fig 4,
Table 2, Table 3)
05
10152025303540455055
0 2 4 6 8 10Time (hr)
Conc
(ug
/ml)
3 N3 HDBR
Fig 4: Ibuprofen plasma concentrations of volunteer 3 in normal
(N) and HDBRpositions
-
`
50
In the fourth volunteer the Tmax for both HDBR and normal
position were the
same, (Tmax for HDBR and for normal position were 1.00 hr) while
Cmax was lower
at HDBR than it at normal position, (Cmax at HDBR was 43.145
µg/ml, while the
Cmax for normal position was 48.654 µg/ml). (Fig 5, Table 2,
Table 3)
05
10152025303540455055
0 2 4 6 8 10Time (hr)
Con
c (u
g/m
l)
4 N4 HDBR
Fig 5: Ibuprofen plasma concentrations of volunteer 4 in normal
(N) and HDBRpositions
-
`
51
In the fifth volunteer the Tmax at HDBR was more than normal
position,
(Tmax for HDBR was 1.33 hr, and for normal position was 1.00 hr)
while Cmax was
lower at HDBR than it at normal position, (Cmax at HDBR was
42.704 µg/ml, while
the Cmax for normal position was 49.097 µg/ml). (Fig 6, Table 2,
Table 3)
05
10152025303540455055
0 2 4 6 8 10Time (hr)
Con
c (u
g/m
l)
5 N5 HDBR
Fig 6: Ibuprofen plasma concentrations of volunteer 5 in normal
(N) and HDBRpositions
-
`
52
In the sixth volunteer the Tmax at HDBR was more than normal
position,
(Tmax for HDBR was 2.50 hr, and for normal position was 0.75 hr)
while Cmax was
lower at HDBR than it at normal position, (Cmax at HDBR was
24.768 µg/ml, while
the Cmax for normal position was 28.088 µg/ml). (Fig 7, Table 2,
Table 3)
05
10152025303540455055
0 2 4 6 8 10Time (hr)
Conc
(ug
/ml)
6 N6 HDBR
Fig 7: Ibuprofen plasma concentrations of volunteer 6 in normal
(N) and HDBRpositions
-
`
53
Volunteers average and also median Tmax at HDBR was faster than
normal
position, (average and median Tmax values for HDBR were 1.138 hr
and 0.875 hr,
and for normal position were 1.373 hr and 1.165 hr). However,
average Cmax at
HDBR was slightly lower than it at normal position, (average
Cmax at HDBR was
38.785 µg/ml, while the average Cmax for normal position was
40.121 µg/ml).
(Fig 8)
This changes in the Tmax and Cmax are due to changes in the body
fluid
concentration in HDBR position, as it is known during the HDBR
position the fluids
shift from the lower part of the body to the upper part of the
body causing increasing
of the blood concentration in the upper part of the body and in
gastro intestinal tract.
Hence the disintegration and dissolution of Ibuprofen in GIT was
faster, leading to
an increase in absorption.
As it is shown in figure number 8, the therapeutic
concentrations of
Ibuprofen, 20 to 30 µg/ml, were achieved.
-
`
54
0
5
10
15
20
25
30
35
40
45
50
55
0 2 4 6 8 10Time (hr)
Con
c (u
g/m
l)
N HDBR
Fig 8: Ibuprofen plasma concentrations of 6 volunteers average
in normal (N) andHDBR positions
-
`
55
Normal Phase:Table 2: Ibuprofen plasma concentrations (µg/ml)
after 600 mg oral dose in 6volunteers in normal position, the Cmax
for each volunteer is bolded.
Timing
(hr)
Vol. # 1
Conc.
(µg/ml)
Vol. # 2
Conc.
(µg/ml)
Vol. # 3
Conc.
(µg/ml)
Vol. # 4
Conc.
(µg/ml)
Vol. # 5
Conc.
(µg/ml)
Vol. # 6
Conc.
(µg/ml)
0.00 0.000 0.000 0.000 0.000 0.000 0.000
0.25 0.426 0.000 0.906 1.574 2.139 11.622
0.50 4.220 0.835 10.917 10.437 12.617 26.126
0.75 8.163 3.387 21.149 41.728 38.950 28.088
1.00 13.732 23.636 33.900 48.654 49.097 26.957
1.33 36.058 29.289 36.553 45.008 45.138 26.127
1.66 39.242 32.176 29.605 42.801 38.307 27.853
2.00 35.070 36.452 24.710 34.747 33.406 27.843
2.50 27.774 39.096 18.251 26.801 29.247 24.608
3.00 26.119 29.731 14.280 20.695 21.857 18.595
4.00 14.974 19.377 8.874 15.005 15.100 11.489
5.00 9.502 13.412 5.220 10.457 9.300 6.811
6.00 5.203 8.435 3.198 6.726 6.605 4.362
8.00 2.583 4.522 1.403 3.303 3.715 1.893
-
`
56
HDBR Phase:Table 3: Ibuprofen plasma concentrations (µg/ml)
after 600 mg oral dose in 6volunteers in HDBR position, the Cmax
for each volunteer is bolded.
Timing
(hr)
Vol. # 1
Conc.
(µg/ml)
Vol. # 2
Conc.
(µg/ml)
Vol. # 3
Conc.
(µg/ml)
Vol. # 4
Conc.
(µg/ml)
Vol. # 5
Conc.
(µg/ml)
Vol. # 6
Conc.
(µg/ml)
0.00 0.000 0.000 0.000 0.000 0.000 0.000
0.25 16.097 30.769 0.000 1.740 10.669 8.824
0.50 45.831 38.149 25.256 23.338 24.220 19.978
0.75 48.316 34.146 35.631 39.436 34.177 18.287
1.00 43.520 32.659 32.933 43.145 42.431 17.776
1.33 31.480 28.477 29.912 42.324 42.704 15.036
1.66 25.138 26.675 24.842 38.062 32.339 13.550
2.00 21.404 25.218 18.732 31.392 29.669 11.383
2.50 15.945 22.477 14.713 25.798 21.461 24.768
3.00 13.108 18.477 12.943 20.679 16.447 23.965
4.00 8.548 13.316 7.282 14.849 11.458 18.583
5.00 5.667 9.355 4.536 9.542 7.508 10.895
6.00 3.618 6.127 2.612 6.898 4.776 6.936
8.00 1.713 3.576 1.059 3.566 2.911 3.675
-
`
57
3.2 Data for Maximum Concentration of Drug in Plasma (Cmax):
Cmax is maximal plasma drug concentration that was reached in
plasma.
Tmax is time of maximum plasma drug concentration.
The results are shown in table number 4.
Table 4: Cmax and Tmax in both phases for all volunteers.
Position Subject Tmax (hr) Cmax (µg/ml)
HDBR 1 0.75 48.316
HDBR 2 0.50 38.149
HDBR 3 0.75 35.631
HDBR 4 1.00 43.145
HDBR 5 1.33 42.704
HDBR 6 2.50 24.768
Position Subject Tmax (hr)
Cmax
(µg/ml)
N 1 1.66 39.242
N 2 2.50 39.096
N 3 1.33 36.553
N 4 1.00 48.654
N 5 1.00 49.097
N 6 0.75 28.088
-
`
58
3.3 Data for K elimination:
Elimination rate constant is the rate constant for removal of
drugs from
the body. Kel = First order elimination rate constant associated
with the
terminal (log-linear) portion of the curve. Estimated by linear
regression of
log concentration versus time.
The results are shown in table number 5.
Table 5: Kel in both phases for all volunteers
Position Subject Kel (hr-1) Half life (hr)
HDBR 1 0.4027 1.7209
HDBR 2 0.3300 2.1000
HDBR 3 0.4845 1.4303
HDBR 4 0.3508 1.9755
HDBR 5 0.3411 2.0317
HDBR 6 0.3559 1.9472
Position Subject Kel (hr-1) Half life (hr)
N 1 0.4431 1.5640
N 2 0.3664 1.8914
N 3 0.4580 1.5131
N 4 0.3812 1.8179
N 5 0.3033 2.2849
N 6 0.4465 1.5521
-
`
59
3.4 Data for Area Under the Curve ( AUC):
The area under curve, AUC, corresponds to the integral of the
plasma
concentration versus an interval of definite time. In practice,
the approximation is
used by application of linear trapezoidal method. One of AUC
uses is to allow the
measurement of the bioavailability of a drug.
AUCinf_obs = AUC from dosing time extrapolated to infinity,
based on the
last observed concentration (obs).
AUC_%Extrap_obs = Percentage of AUCinf_obs due to extrapolation
from Tlast
to infinity.
The results are shown in tables number 6.a and 6.b.
Table 6.a : AUClast, AUC0-4, AUCinf_obs and AUC%Extrap in HDBR
phase for allvolunteers
position Subject
AUClast
(µg/ml) hr
AUC0-4
(µg/ml)hr
AUCinf_obs
(µg/ml) hr
AUC_%Extrap
(%)
HDBR 1 107.1396 90.0586 111.3936 3.8189
HDBR 2 124.6960 95.9165 135.5327 7.9957
HDBR 3 84.6915 71.5375 86.8772 2.5159
HDBR 4 135.2551 104.3756 145.4201 6.9901
HDBR 5 119.0651 95.7531 127.5992 6.6882
HDBR 6 105.1240 70.8585 115.4508 8.9448
-
`
60
Table 6.b : AUClast, AUC0-4, AUCinf_obs and AUC_%Extrap in
normal phase forall volunteers.
position Subject
AUClast
(µg/ml) hr
AUC0-4
(µg/ml)hr
AUCinf_obs
(µg/ml) hr
AUC_%Extrap
(%)
N 1 115.2989 87.9224 121.1281 4.8124
N 2 135.4739 95.1989 147.8155 8.3493
N 3 90.5619 74.7049 93.6253 3.2720
N 4 139.1049 107.7534 147.7702 5.8641
N 5 138.4623 107.9898 150.7115 8.1276
N 6 106.9095 85.918 111.1488 3.8140
3.5 Data for Volume of Distribution ( V/F ) and Clearance
(CL/F):
The volume of distribution (Vd) is the fictitious volume,
expressed in liter
or in liter per kilogram, in which the drug would have been
distributed by
supposing that its concentration is homogeneous, for a given
drug, the knowledge
of its desirable concentration in blood and of its volume of
distribution allows
evaluation of the dose to administer.
Clearance is the fraction of a theoretical volume completely
purified (i.e.
no longer containing any of the drug concerned) per unit of
time. Plasma
clearance is the apparent volume of plasma purified per unit of
time. Total
clearance (Clt) is the fraction of the volume of distribution,
Vd, which is
-
`
61
completely purified per unit of time. The total clearance
depends on the constant
of elimination and thus on T ½ and on Vd. Clearance is a
constant in linear
kinetics.
The results are shown in table number 7.
Table 7: V/F and Cl/F in both phases for all volunteers.
Position Subject V/F (L) Cl/F (L/hr)
HDBR 1 13.3762 5.3863
HDBR 2 13.4156 4.4270
HDBR 3 14.2541 6.9063
HDBR 4 11.7612 4.1260
HDBR 5 13.7853 4.7022
HDBR 6 14.6037 5.1970
Position Subject V/F (L) Cl/F (L/hr)
N 1 11.1787 4.9534
N 2 11.0783 4.0591
N 3 13.9930 6.4085
N 4 10.6523 4.0604
N 5 13.1266 3.9811
N 6 12.0888 5.3982
-
`
62
3.6 Data for (AUMClast ) and (AUMCinf_obs):
AUMClast is the area under the moment curve from the time of
dosing
(Dosing time) to the last measurable concentration.
AUMCinf_obs Area under the first moment curve (AUMC)
extrapolated to
infinity, based on the last observed concentration.
The results are shown in table number 8.
Table 8: AUMClast and AUMCinf_obs in both phases for all
volunteers.
Position Subject AUMClast (µg/ml) hr2 AUMCinf_obs (µg/ml)
hr2
HDBR 1 232.4074 277.0039
HDBR 2 324.5403 444.0741
HDBR 3 193.3673 215.3640
HDBR 4 365.5351 475.8308
HDBR 5 297.5320 390.8232
HDBR 6 340.8410 452.4741
Position Subject AUMClast (µg/ml) hr2 AUMCinf_obs (µg/ml)
hr2
N 1 341.5563 401.3454
N 2 441.3853 573.8016
N 3 225.0263 256.2229
N 4 375.4078 467.4642
N 5 374.2287 512.6107
N 6 274.4322 317.8397
-
`
63
3.7 Data for Mean Residence Time (MRT):
Mean residence time (MRT) is the average total time molecules of
a given
dose spend in the body. Thus, this includes all ADME
processes.
MRT = AUMC/AUC.
The results are shown in table number 9.
Table 9: MRT in both phases for all volunteers.
Position Subject MRT (hr)
HDBR 1 2.4867
HDBR 2 3.2765
HDBR 3 2.4789
HDBR 4 3.2721
HDBR 5 3.0629
HDBR 6 3.9192
Position Subject MRT (hr)
N 1 3.3134
N 2 3.8819
N 3 2.7367
N 4 3.1635
N 5 3.4013
N 6 2.8596
-
`
64
3.8 Pharmacokinetic Parameter Means (CV %) of Ibuprofen Under
Normal
(N) and Head-Down-Bed-Rest (HDBR) positions:
Table 10: Pharmacokinetic parameter means (CV %) of ibuprofen
under normal (N)and Head-Down-Bed-Rest (HDBR) positions
Pk parameter N HDBR P values *
CV%
N
CV%
HDBR
Kel (hr-1) 0.399 0.377 0.317 15.099 15.375
Half life (hr) 1.770 1.867 0.348 16.717 13.367
Tmax (hr) 1.373 1.138 0.167 * * 46.290 63.580
Cmax (µg/ml) 40.121 38.785 0.510 19.711 21.010
AUC0-8 (µg/ml) hr 120.968 112.661 0.015 16.532 15.708
AUC0-4 (µg/ml) hr 93.247 88.083 0.137 14.043 15.730
AUC4-8 (µg/ml) hr 27.720 24.578 0.388 30.801 33.526
AUCinf_obs (µg/ml)hr 128.699 120.378 0.071 18.417 17.170
AUC_% Extrap_obs 5.707 6.159
V_/F_obs (L) 10.951 13.341 0.056 13.781 20.377
Cl_/F_obs (L/hr) 4.810 5.124 0.071 20.230 19.339
AUMC0-8 (µg/ml) hr2 338.672 292.370 0.158 22.953 22.770
AUMCinf_obs
(µg/ml) hr2 421.547 375.928 0.329 28.481 28.220
MRT (hr) 3.226 3.082 0.568 12.751 17.728
* P values of t test after logarithmic transformation of
parameters** Friedman DESIGN for Tmax was done using Kinetica.
-
`
65
The logarithmic transformation of parameters was used to be sure
that the
distribution was normal.
The P values of t test results were not significant for all the
parameters
except for AUClast, it was less than 0.05 (0.015), but the P
value results of t test for
AUC0-4 was 0.137 which is not significant and for AUC4-8 was
0.388 which is
also not significant and for AUCinf_obs was 0.071 which is also
not significant. As it
was mentioned above, the P values of t test for AUC after
dividing it to three zones
became not significant, that is suggested to be due to the
increase in difference
between both positions for AUClast, as compared to the
differences in AUC0-4 and
AUC4-8. . The average AUC % extrapolated for normal phase was
(5.707 %) and for
HDBR position was (6.159 %), in both cases the result is less
than 10% which
indicates of enough sampling times (Guidance for Industry,
Bioavailability and
Bioequivalence Studies for Orally Administered Drug, USFDA,
2003).
The average Tmax in HDBR (1.138 hr) was faster, yet not
significantly
different than it in Normal phase (1.373 hr), these changes are
due to changes in the
body fluid concentration in HDBR position, as it is known during
the HDBR
position the fluids shift from the lower part of the body to the
upper part of the body
causing increasing of the blood volume in the upper part of the
body and in gastro
intestinal tract. In addition, ibuprofen is low soluble drug and
hence the
disintegration rate in GIT was faster in HDBR position leading
to increase of
absorption of Ibuprofen in the body (Newa M, Bhandari KH, Oh DH,
et al, 2008).
Mean residence time (MRT) which indicates the average total
time
molecules of a given dose spend for all ADME processes in the
body, in both
-
`
66
phases was almost same, P value of t test result was (0.568)
which is not
significant.
Half life (t0.5) which indicates the period of time required for
the
concentration or amount of drug in the body to be reduced to
one-half of a given
concentration or amount, in HDBR phases the average half life
was 1.87 hr and in
normal phase the average half life was 1.77 hr. and the P value
of t test result was
(0.348) which is not significant.
The average volume of distribution of ibuprofen at HDBR position
was
13.341L and normal position was 10.951L. Yet P-value of t test
result for volume
of distribution was (0.056) which is not significant. This
increase in volume of
distribution at HDBR was as a result of decrease in the AUCinf
and Kel at HDBR,
according to the following formula:
V/F= Dose/ (Kel * AUCinf)
The average clearance at HDBR position was 5.124 L/hr which is
faster
than it at normal position which was 4.810 L/hr. The P-value of
t test result for
clearance was (0.071) which is not significant. This slight
increase of clearance at
HDBR is due to increase of volume of distribution at HDBR
position according to
the following formula :
Cl/F=V*Kel=D/AUCinf.
-
`
67
Chapter 4:
Conclusions
-
`
68
4. Conclusions:
AUCs were similar in both positions. However, slight differences
in Cmax
and Tmax were observed between HDBR position and normal
positions due to faster
drug dissolution in HDBR position, yet such differences were not
significant.
This indicates that relative bioavailability is similar and
hence no need for
dose adjustment of ibuprofen for crew members of space
flight.
However, this can not be generalized to other drugs, especially
highly
soluble medications.
Ibuprofen was not detected in all saliva samples, suggesting
that Ibuprofen
is not excreted in saliva.
-
`
69
References
Amidon GL, DeBrincat GA, Najib N; 1991. Effects of gravity on
gastric emptying,intestinal transit, and drug absorption. J Clin
Pharmacol 31(10):968-973.
A. Pavy-Le Traon . M. Heer . M. V. Narici . J. Rittweger . J.
Vernikos, Eur J ApplPhysiol ; 2007. From space to earth: advances
in human physiology from 20 years ofbed rest studies (1986–2006).
101:143–194, DOI 10.1007/s00421-007-0474-z.
Benet LZ; 1988. Pharmacokinetic considerations of space flight.
ed., Houston, TX:Lunar and Planetary Institute - NASA. p 15-16.
C. H. Kleinbloesem et al.,Arzneimittelforschung; 1995, 45,
1117–1121
Cintron NM, Putcha L, Chen YM, Vanderploeg JM; 1987. Inflight
salivarypharmacokinetics of scopolamine and dextroamphetamine.
Results of the lifesciences DSOs conducted aboard the space
schuttle 1981-1986, Houston, TX:NASA. p 25-29.
Edgar L. Schuck, PhD, Maria Grant, MD and Hartmut Derendorf,
PhD, FCP, fromthe department of pharmaceutics; 2004. Effect of
simulated microgravity on thedisposition and tissue penetration of
Ciprofloxacin in healthy volunteers. Universityof florida,
Gainesville.
Fitts RH, Riley DR, Widrick JJ; 2000. Physiology of a
microgravity environmentinvited review: microgravity and skeletal
muscle. J Appl Physiol 89(2):823-839.
Graebe A, Schuck EL, Lensing P, Putcha L, Derendorf H; 2004.
Physiological,pharmacokinetic, and pharmacodynamic changes in
space. J Clin Pharmacol44(8):837-853.
Guidance for Industry, Bioavailability and Bioequivalence
Studies for OrallyAdministered Drug, Products — General
Considerations, U.S. Department ofHealth and Human Services, Food
and Drug Administration, Center for DrugEvaluation and Research
(CDER); March 2003.
Harm DL, Jennings RT, Meck JV, Powell MR, Putcha L, Sams CP,
Schneider SM,Shackelford LC, Smith SM, Whitson PA; 2001. Invited
review: gender issuesrelated to spaceflight: a NASA perspective. J
Appl Physiol 91(5):2374-2383.
Merrill AH, Jr., Hoel M, Wang E, Mullins RE, Hargrove JL, Jones
DP, Popova IA;1990. Altered carbohydrate, lipid, and xenobiotic
metabolism by liver from ratsflown on cosmos 1887 [published
erratum appears in FASEB J 1990May;4(8):2539]. Faseb J
4(1):95-100.
-
`
70
Newa M, Bhandari KH, Oh DH, et al; 2008. Enhancement of
solubility, dissolutionand bioavailability of ibuprofen in solid
dispersion systems. Chem PharmBull.56(4):569-574.
Nicogossian AE, Sawin CF, Huntoon CL; 1994. Overall physiologic
response tospace flight. In Nicogossian AE, Huntoon CL, Pool SL,
editors. Space physiologyand medicine, Phildelphia: Lea &
Febiger. p 213-227.
Pool SL, Nicogossian A; 1983. Biomedical results of the space
shuttle orbital flighttest program. Aviat space environ Med 54(12
Pt 2):S41-49.
Putcha L, Berens KL, Marshburn TH, Ortega HJ, Billica RD; 1999.
Pharmaceuticaluse by U.S. astronauts on space shuttle missions.
Aviat space environ Med70(7):705-708.
Santy PA, Kapanka H, Davis JR, Stewart DF; 1988. Analysis of
sleep on shuttlemissions. Aviat space environ Med 59(11 Pt
1):1094-1097.
Stewart JJ, Wood MJ, Wood CD, Mims ME; 1994. Effects of motion
sickness andantimotion sickness drugs on gastric function. J Clin
Pharmacol 34(6):635-643.
US Food and Drug Administration (US FDA) Centre for Drug
Evaluation andResearch; 2001. Guidance for Industry: Bioanalytical
Method Validation, Rockville,MD, Retrieved from
http://www.fda.gov/cder/guidance/4252fnl.pdf
Wang DS, Ren W, Xiang QL, Sun L, Liu ZX, Su SN; 2001. [Changes
of arterialblood pressure during various stages in spaceflight
activities]. Space Med Eng(Beijing) 14(1):66-69.
Watenpaugh DE; 2001. Fluid volume control during short-term
space flight andimplications for human performance. J Exp Biol
204(Pt 18):3209-3215.
Zhang LF; 2001. Vascular adaptation to microgravity: what have
we learned? J ApplPhysiol. 91(6):2415-2430.
http://www.fda.gov/cder/guidance/4252fnl.pdf
-
`
71
Appendix # 1
Institutional Review Board (IRB)
Approval
-
`
72
-
`
73
Appendix # 2
Jordan Food and Drug Administration
(JFDA) Approval
-
`
74
-
`
75
Appendix # 3
Informed Constant Form
-
`
76
-
`
77
-
`
78
-
`
79
-
`
80
-
`
81
-
`
82
-
`
83
-
`
84
-
`
85
-
`
86
-
`
87
-
`
88
Appendix # 4
Winnonlin Output
-
`
89
Input File: Workbook - [C:\PROGRAM
FILES\PHARSI...\ABRN.PWO]position=ABRSubject=1
Date: 10/04/2010 Time: 13:57:23
WINNONLIN NONCOMPARTMENTAL ANALYSIS PROGRAM Version 5.2 Build
200701231637 Core Version 18Sept2006
Settings--------Model: Plasma Data, Extravascular
AdministrationNumber of nonmissing observations: 14Dose time:
0.00Dose amount: 600.00Calculation method: Linear Trapezoidal with
Linear InterpolationWeighting for lambda_z calculations: Uniform
weightingLambda_z method: User-specified lambda_z range, Log
regressionUser's lambda_z bounds: 4.00, 8.00
Summary Table------------- Time Conc. Pred. Residual AUC AUMC
Weight hr ug/ml ug/ml ug/ml hr*ug/ml
hr*hr*ug/ml-------------------------------------------------------------------------------
0.0000 0.0000 0.0000 0.0000 0.2500 16.10 2.012 0.5030 0.5000 45.83
9.753 3.871 0.7500 48.32 21.52 11.26 1.000 43.52 33.00 21.23 1.330
31.48 45.38 35.32 1.660 25.14 54.72 49.12 2.000 21.40 62.63 63.49
2.500 15.95 71.97 84.16 3.000 13.11 79.23 104.0 4.000 * 8.548 8.422
0.1263 90.06 140.7 1.000 5.000 * 5.667 5.630 0.03683 97.17 172.0
1.000 6.000 * 3.618 3.764 -0.1459 101.8 197.0 1.000 8.000 * 1.713
1.682 0.03079 107.1 232.4 1.000
*) Starred values were included in the estimation of
Lambda_z.
Final Parameters---------------Rsq 0.9985Rsq_adjusted
0.9977Corr_XY -0.9992No_points_lambda_z 4Lambda_z 1/hr
0.4027Lambda_z_lower hr 4.0000Lambda_z_upper hr 8.0000HL_Lambda_z
hr 1.7213Tlag hr 0.0000Tmax hr 0.7500Cmax ug/ml 48.3160Cmax_D
ug/ml/mg 0.0805Tlast hr 8.0000Clast ug/ml 1.7130AUClast hr*ug/ml
107.1396AUCall hr*ug/ml 107.1396AUCINF_obs hr*ug/ml
111.3936AUCINF_D_obs hr*ug/ml/mg 0.1857AUC_%Extrap_obs %
3.8189Vz_F_obs ml 13376.2132Cl_F_obs ml/hr 5386.3043AUCINF_pred
hr*ug/ml 111.3172AUCINF_D_pred hr*ug/ml/mg 0.1855AUC_%Extrap_pred %
3.7528
-
`
90
Vz_F_pred ml 13385.4024Cl_F_pred ml/hr 5390.0046AUMClast
hr*hr*ug/ml 232.4074AUMCINF_obs hr*hr*ug/ml
277.0039AUMC_%Extrap_obs % 16.0996AUMCINF_pred hr*hr*ug/ml
276.2022AUMC_%Extrap_pred % 15.8561MRTlast hr 2.1692MRTINF_obs hr
2.4867MRTINF_pred hr 2.4812AUC0_4 hr*ug/ml 90.0586AUC4_8 hr*ug/ml
17.0810
-
`
91
Input File: Workbook - [C:\PROGRAM
FILES\PHARSI...\ABRN.PWO]position=ABRSubject=2
Date: 10/04/2010 Time: 13:57:24
WINNONLIN NONCOMPARTMENTAL ANALYSIS PROGRAM Version 5.2 Build
200701231637 Core Version 18Sept2006
Settings--------Model: Plasma Data, Extravascular
AdministrationNumber of nonmissing observations: 14Dose time:
0.00Dose amount: 600.00Calculation method: Linear Trapezoidal with
Linear InterpolationWeighting for lambda_z calculations: Uniform
weightingLambda_z method: User-specified lambda_z range, Log
regressionUser's lambda_z bounds: 4.00, 8.00
Summary Table------------- Time Conc. Pred. Residual AUC AUMC
Weight hr ug/ml ug/ml ug/ml hr*ug/ml
hr*hr*ug/ml-------------------------------------------------------------------------------
0.0000 0.0000 0.0000 0.0000 0.2500 30.77 3.846 0.9615 0.5000 38.15
12.46 4.307 0.7500 34.15 21.50 9.893 1.000 32.66 29.85 17.18 1.330
28.48 39.94 28.81 1.660 26.68 49.04 42.37 2.000 25.22 57.86 58.47
2.500 22.48 69.78 85.13 3.000 18.48 80.02 113.0 4.000 * 13.32 12.88
0.4391 95.92 167.4 1.000 5.000 * 9.355 9.258 0.09737 107.3 217.4
1.000 6.000 * 6.127 6.656 -0.5286 115.0 259.2 1.000 8.000 * 3.576
3.440 0.1360 124.7 324.5 1.000
*) Starred values were included in the estimation of
Lambda_z.
Final Parameters---------------Rsq 0.9900Rsq_adjusted
0.9851Corr_XY -0.9950No_points_lambda_z 4Lambda_z 1/hr
0.3300Lambda_z_lower hr 4.0000Lambda_z_upper hr 8.0000HL_Lambda_z
hr 2.1005Tlag hr 0.0000Tmax hr 0.5000Cmax ug/ml 38.1490Cmax_D
ug/ml/mg 0.0636Tlast hr 8.0000Clast ug/ml 3.5760AUClast hr*ug/ml
124.6960AUCall hr*ug/ml 124.6960AUCINF_obs hr*ug/ml
135.5327AUCINF_D_obs hr*ug/ml/mg 0.2259AUC_%Extrap_obs %
7.9957Vz_F_obs ml 13415.5564Cl_F_obs ml/hr 4426.9758AUCINF_pred
hr*ug/ml 135.1207AUCINF_D_pred hr*ug/ml/mg 0.2252AUC_%Extrap_pred %
7.7151Vz_F_pred ml 13456.4634
-
`
92
Cl_F_pred ml/hr 4440.4746AUMClast hr*hr*ug/ml
324.5403AUMCINF_obs hr*hr*ug/ml 444.0741AUMC_%Extrap_obs %
26.9175AUMCINF_pred hr*hr*ug/ml 439.5295AUMC_%Extrap_pred %
26.1619MRTlast hr 2.6027MRTINF_obs hr 3.2765MRTINF_pred hr
3.2529AUC0_4 hr*ug/ml 95.9165AUC4_8 hr*ug/ml 28.7795
-
`
93
Input File: Workbook - [C:\PROGRAM
FILES\PHARSI...\ABRN.PWO]position=ABRSubject=3
Date: 10/04/2010 Time: 13:57:24
WINNONLIN NONCOMPARTMENTAL ANALYSIS PROGRAM Version 5.2 Build
200701231637 Core Version 18Sept2006
Settings--------Model: Plasma Data, Extravascular
AdministrationNumber of nonmissing observations: 14Dose time:
0.00Dose amount: 600.00Calculation method: Linear Trapezoidal with
Linear InterpolationWeighting for lambda_z calculations: Uniform
weightingLambda_z method: User-specified lambda_z range, Log
regressionUser's lambda_z bounds: 4.00, 8.00
Summary Table------------- Time Conc. Pred. Residual AUC AUMC
Weight hr ug/ml ug/ml ug/ml hr*ug/ml
hr*hr*ug/ml-------------------------------------------------------------------------------
0.0000 0.0000 0.0000 0.0000 0.2500 0.0000 0.0000 0.0000 0.5000
25.26 3.157 1.579 0.7500 35.63 10.77 6.497 1.000 32.93 19.34 13.95
1.330 29.91 29.71 25.95 1.660 24.84 38.74 39.32 2.000 18.73 46.15
52.70 2.500 14.71 54.51 71.26 3.000 12.94 61.43 90.16 4.000 * 7.282
7.218 0.06370 71.54 124.1 1.000 5.000 * 4.536 4.446 0.08954 77.45
150.0 1.000 6.000 * 2.612 2.739 -0.1270 81.02 169.2 1.000 8.000 *
1.059 1.039 0.01968 84.69 193.4 1.000
*) Starred values were included in the estimation of
Lambda_z.
Final Parameters---------------Rsq 0.9985Rsq_adjusted
0.9978Corr_XY -0.9993No_points_lambda_z 4Lambda_z 1/hr
0.4845Lambda_z_lower hr 4.0000Lambda_z_upper hr 8.0000HL_Lambda_z
hr 1.4306Tlag hr 0.2500Tmax hr 0.7500Cmax ug/ml 35.6310Cmax_D
ug/ml/mg 0.0594Tlast hr 8.0000Clast ug/ml 1.0590AUClast hr*ug/ml
84.6915AUCall hr*ug/ml 84.6915AUCINF_obs hr*ug/ml
86.8772AUCINF_D_obs hr*ug/ml/mg 0.1448AUC_%Extrap_obs %
2.5159Vz_F_obs ml 14254.1174Cl_F_obs ml/hr 6906.2965AUCINF_pred
hr*ug/ml 86.8366AUCINF_D_pred hr*ug/ml/mg 0.1447AUC_%Extrap_pred %
2.4703Vz_F_pred ml 14260.7836
-
`
94
Cl_F_pred ml/hr 6909.5264AUMClast hr*hr*ug/ml
193.3673AUMCINF_obs hr*hr*ug/ml 215.3640AUMC_%Extrap_obs %
10.2138AUMCINF_pred hr*hr*ug/ml 214.9553AUMC_%Extrap_pred %
10.0430MRTlast hr 2.2832MRTINF_obs hr 2.4789MRTINF_pred






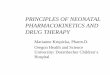







![Resolution of Ibuprofen Enantiomers by Rhizomucor miehei … · ibuprofen [9] Enzymatic kinetic resolution of racemic ibuprofen: past, present and future [10] Lipases for biotechnology](https://img.pdfslide.us/doc/110x75/60fb9a046f3ed71e8020a41e/resolution-of-ibuprofen-enantiomers-by-rhizomucor-miehei-ibuprofen-9-enzymatic.jpg)














