Embed Size (px)
Citation preview

Pharmacists as Agents of Innovation in COPD Diagnosis and Management
Tatiana Makhinova, BScPharm, PhD Assistant Professor Faculty of Pharmacy and Pharmaceutical Sciences University of Alberta

Outline
• COPD: why do we care?
• COPD: gaps in care
• The role of the pharmacist in prevention and screening
• The role of the pharmacist in management
• Future steps and opportunities for innovative care
2

Facts about COPD
• COPD is currently the fourth leading cause of death in the world
• COPD is projected to be the 3rd leading cause of death by 2030
• More than 3 million people died of COPD in 2012 accounting for 6% of
all deaths globally
• Globally, the COPD burden is projected to increase in coming decades
because of continued exposure to COPD risk factors and aging of the
population
Lozano, 2012; Mathers, 2006
3

Facts about COPD: Alberta context
Economic surveillance for chronic obstructive pulmonary disease (COPD) in Alberta, IHE 2016 4

Facts about COPD: Alberta context
Economic surveillance for chronic obstructive pulmonary disease (COPD) in Alberta, IHE 2016 5

6 © Canadian Pharmacists Association, December 2016

Pharmacy Services Framework
7
Patient assessment services
• Injections
• Prescribing
• Follow-ups (CACP, SMMA)
Comprehensive chronic care assessment
• Comprehensive annual care plan (CACP)
• Structured medication management assessment (SMMA)

CACP/SMMA eligibility
8
Chronic disease
Hypertension
Diabetes Mellitus
Heart Failure
Ischaemic Heart Disease
Angina Pectoris
Asthma
Chronic Obstructive Pulmonary Disease (COPD)
Mental Health Disorders
Risk factor
Tobacco
Obesity
Addictions
CACP • ≥2 Chronic diseases
OR
• Chronic disease + ≥1 Risk factor
SMMA • Chronic disease + 3 medications
OR
• Diabetes + Insulin/medication
OR
• Daily tobacco use

Prevention
9

https://www.sancda.org.za/who-world-no-tobacco-day-2018-awards-call-for-nominations/
10

Primary prevention
• 85% of all COPD cases are attributed to
smoking
• The level of awareness of COPD is
inadequate
• Common belief: dyspnoea and
limitations in performing daily
activities/exercise are a part of the
ageing process
11 Jarab, 2012; van der Molen, 2016

Gaps in prevention
• Extent of services and programs, their use and effectiveness is
somewhat limited
• Services are underutilized
• About 10% of patients diagnosed with COPD had claims for
prescription smoking cessation drugs
12 Economic surveillance for chronic obstructive pulmonary disease (COPD) in Alberta, IHE 2016

What is the role of the community pharmacist?
Smoking cessation
Screening
Screening
13

Primary prevention
Pharma-cological treatment
Behaviour support
Effective strategy
Meta-analysis: RR=2.21
(95% CI 1.49-3.29)
14 GOLD, 2016; Mdege, 2014; Saba, 2014

Community pharmacists in Alberta
• An SMMA Tobacco Cessation Initial Assessment may be claimed for a resident
using a tobacco product daily and willing to receive Tobacco Cessation
Services.
• Up to four SMMA Tobacco Cessation Follow-up Assessments may be claimed
during the 365 day period after the SMMA Tobacco Cessation Initial
Assessment.
• Tobacco Cessation Services are defined as the provision by a clinical
pharmacist of evidence-based tobacco cessation support and counselling
including pharmacotherapy support. Use ICD-9 diagnosis code 305.1 for
Tobacco Use. 15

Community pharmacists in Alberta
16

Components for success
17 Greenhalgh et al. BMC Medicine (2016) 14:209

Early diagnosis
18

Importance of early disease management
• Patient health outcomes
• Reduced treatment benefit
• Increased risk hospitalization
• Costs to healthcare system
• Costs for treatment rise 10x when treating severe stage vs. mild
• Increased expenditures for inpatient/outpatient resources
19 Lyngso, 2010; APhA White paper on expanding role of pharmacists in COPD, 2011

Where are the gaps in care?
• Underdiagnosis
• Nearly half of COPD sufferers lack a clinical diagnosis
• Patients with spirometrically confirmed but not yet physician diagnosed
COPD utilize the health care system as frequently than those with
physician diagnosed disease
• Delayed case identification and intervention
• Often patients have progressed to mod-severe stages, at which time
treatment benefit is greatly reduced
20 Evans, 2014; Labonte, 2014

What is the role of the community pharmacist?
Smoking cessation
Screening
Screening
21

Early detection and case finding
• Timely diagnosis: earlier intervention improved QoL & reduced
healthcare burden
• Pharmacists are often the first point of contact between the patient
and the healthcare system
• Patient's needs (symptoms/meds): opportunity for screening
• Completion of a validated disease risk assessment questionnaire • Spirometry testing • Referral to a physician for confirmatory diagnosis and treatment
22

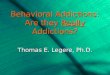
Example of Screening Questionnaire (COPD-PS)
23 Martinez, 2008

Early detection and case finding
• Trained community pharmacists are
able to perform accurate and
reproducible spirometry screenings
• Targeted screening could identify one
patient with moderate COPD for every
two individuals screened
• Portable device: Simplifies spirometry
technique (FEV6)
24 Wright, 2015; Castillo, 2015

Remaining knowledge gaps
• Lack of follow up data • Accuracy of pharmacist-led case finding interventions?
• Were the cases ultimately diagnosed with COPD?
• Were the patients initiated on treatment?
• Did the case findings have an impact on patient important outcomes?
• Which screening methods are most effective?
• How generalizable are findings?
• What training should be provided for pharmacists?
• How can we overcome barriers eg. lack of reimbursement models?
Further research is required to demonstrate the effect of pharmacist-led screening
interventions on patient important outcomes
25

Management
26

Appropriate management
• Diagnosis of at-risk individuals using spirometry so
that timely intervention can be provided
• Appropriate therapy management
• Strategies to prevent and manage acute
exacerbations
• Promotion of smoking cessation
• Use of routine follow-ups for a regular evaluation
of inhaler technique and adherence
• Influenza and pneumococcal vaccination
• Pulmonary rehabilitation
It is estimated
that only 30-55%
of patients are
provided with this
recommended
care
Mularski, 2006; Seys, 2017
27

Gaps in management: pharmacotherapy
• 30% of COPD patients in Alberta were found not to have any pharmacological therapy; of those, almost 22% were considered high severity
• PCP: 34% provided treatment with accordance to guidelines
• 28% of patients were dispensed an ICS inhaler as the first medication,
where only 52.4% of those patients met the CTS criteria for ICS use and only 0.8% had been on LABA or LAMA prior to initiation of ICS
28 Jones, 2014; Bourbeau, 2008

What is the role of the community pharmacist?
Medication management
Inhalation technique
Adherence
Vaccinations
Patient education
29

Inhalation technique: evidence
• Common errors
• Failure to hold breath after inhalation
• Inappropriate inspiration flow
• Failure to shake the canister before use
• Measured through use of checklists
• Increase in percentage of correct steps
performed from 67.6% to 93.4%
• Decrease in major errors from 15.6% to 1.2%
• Average number of errors made per patient
dropped from 2.5 to 0.5
• Written info vs. physical demonstration 30
Tommelein, 2014

Medication management: self-management
• COPD Action Plan
• COPD rescue pack
• Advising on how to recognize an
acute exacerbation
• Monitoring use of both maintenance
and rescue medication
• Improved quality of life, increased
medication adherence, and
reductions in doctor visits and
hospitalization rates 31 Clark, 2009; Bourbeau, 2006

Health resource utilization: evidence
Implementation of structured education programs and its effect on the following
parameters:
• ED visits: • 50% reduction
• Hospitalization: • Hospitalization decreased by 60%
• GP visits: • Per participant level of resource use decreased from 1.40 to 0.90
• Cost to healthcare system • Total National Health Service (NHS) costs reduced by £87.66 per participant
• Cost of intervention was £63.62 per participant
32 Tommelein, 2014

Conclusions
• Pharmacists are well-placed in the community to address
gaps in care
• Pharmacists are capable of preventing, screening,
improving inhalation technique, medication adherence,
and healthcare resource utilization
• Spacialized training: CRE, CTE
• The role of the pharmacist: significant impact
33

Thank You! Questions?
34

References 1. Statistics Canada. Chronic obstructive pulmonary disease in Canadians, 2009 to 2011. http://www.statcan.gc.ca/pub/82-625-x/2012001/article/11709-eng.htm Updated February
11, 2013. 2. Alberta Health Services. COPD. http://www.albertahealthservices.ca/info/Page7731.aspx 3. Benady S. The Human and Economic Burden of COPD: A Leading Cause of Hospital Admission in Canada. Canada: Canadian Thoracic Society; 2010. 4. Mittmann N, Kuramoto L, Seung SJ, Haddon JM, Bradley-Kennedy C, Fitzgerald JM. The cost of moderate and severe COPD exacerbations to the Canadian healthcare system.
Respir Med. 2008;102(3):413-421. 5. Statistics Canada. Chronic obstructive pulmonary disease (COPD). http://www.phac-aspc.gc.ca/cd-mc/crd-mrc/copd-mpoc-eng.php Updated February 8, 2013. 6. Beauchesne MF, Bercier D, Julien-Baker F, Lalonde L, Boileau R, Blais L. Community pharmacy-based medication assessment program for asthma and chronic obstructive
pulmonary disease. Can Pharm J. 2012;145:70–71. 7. Mehuys E, Boussery K, Adriaens E, et al. COPD Management in Primary Care: An Observational, Community Pharmacy-based Study. Ann Pharmacother. 2010;44(2):257-266. 8. Basheti IA, Armour CL, Bosnic-Anticevich SZ, Reddel HK. Evaluation of a novel educational strategy, including inhaler-based reminder labels, to improve asthma inhaler technique.
Patient Educ Couns. 2008;72(1):26-33. 9. Crompton GK, Barnes PJ, Broeders M, et al. The need to improve inhalation technique in Europe: a report from the aerosol drug management improvement team. Respir Med.
2006;100(9):1479-1494. 10. Restrepo RD, Alvarez MT, Wittnebel LD, et al. Medication adherence issues in patients treated for COPD. Int J Chron Obstruct Pulmon Dis. 2008:3(3):371-384. 11. Sabaté E. Adherence to Long Term Therapies: Evidence for Action. Switzerland: WHO, World Health Organisation; 2003. 12. Mäkelä MJ, Backer V, Hedegaard M, Larsson K. Adherence to inhaled therapies, health outcomes and costs in patients with asthma and COPD. Respir Med. 2013;107(10):1481-
1490. 13. Tommelein E, Mehuys E, Van Hees T, et al. Effectiveness of pharmaceutical care for patients with chronic obstructive pulmonary disease (PHARMACOP): a randomized controlled
trial. Br J Clin Pharmacol. 2014;77(5):756-766. 14. Takemura M, Mitsui K, Ido M, et al. Effect of a network system for providing proper inhalation technique by community pharmacists on clinical outcomes in COPD patients. Int J
Chron Obstruct Pulmon Dis. 2013;8:239-244. 15. Morisky DE, Green LW, Levine DM. Concurrent and predictive validity of a self-reported measure of medication adherence. Med Care. 1986;24(1):67-74. 16. Margolis A, Young H, Lis J, Schuna A, Sorkness CA. A telepharmacy intervention to improve inhaler adherence in veterans with chronic obstructive pulmonary disease. Am J Health
Syst Pharm. 2013;70:1875-1876. 17. Ottenbros S, Teichert M, de Groot R, et al. Pharmacist-led intervention study to improve drug therapy in asthma and COPD patients. Int J Clin Pharm. 2014;36(2):336-344. 18. Hämmerlein A, Müller U, Schulz M. Pharmacist-led intervention study to improve inhalation technique in asthma and COPD patients. J Eval Clin Pract. 2011;17(1):61-70. 19. Bosnic-Anticevich SZ, Sinha H, So S, Reddel HK. Metered-dose inhaler technique: the effect of two educational interventions delivered in community pharmacy over time. J Asthma.
2010;47(3):251-256. 20. Van der Palen J, Klein JJ, Kerkhoff AH, Van Herwaarden CL. Evaluation of the effectiveness of four different inhalers in patients with chronic obstructive pulmonary disease. Thorax.
1995;50(11): 1183-1187. 21. Khdour MR, Kidney JC, Smyth BM, McElnay JC. Clinical pharmacy-led disease and medicine management programme for patients with COPD. Br J Clin Pharmacol. 2009;68(4):588-
598. 22. Jarab AS, Alqudah SG, Khdour M, Shamssain M, Mukattash TL. Impact of pharmaceutical care on health outcomes in patients with COPD. Int J Clin Pharm. 2012;34(1):53-62. 23. Wright D, Twigg M, Barton G, Thornley T, Kerr C. An evaluation of a multi-site community pharmacy-based chronic obstructive pulmonary disease support service. Int J Pharm Pract.
2015;23(1):36-43.
35