Embed Size (px)
DESCRIPTION
Citation preview

Janice M. Bell, RN, PhD
Author, Speaker, Educator, & Researcher of
Family-Focused Practice
Editor, Journal of Family Nursing
Member, Board of Directors, International Family Nursing Association
http://janicembell.com
Janice M. Bell, RN, PhD
www.janicembell.com

transform
health care with
individuals and families
Janice M. Bell, RN, PhD
www.janicembell.com
metamorphosis
verb: |ch ānj|

Family Systems Care
Family Centered Care
Family-focused Care
Relational practice
Patient Centered Care
Janice M. Bell, RN, PhD
www.janicembell.com
Patient and Family

The Institute for Family-Centered Care: An
Approach to Care
“Family centered care is an innovative
approach to the planning, delivery, and
evaluation of health care that is grounded
in mutually beneficial partnerships
among health care providers, patients,
and families.”
Institute of Family Centered Care
http://www.familycenteredcare.org Janice M. Bell, RN, PhD
www.janicembell.com

Elements of Patient and
Family-Centered Care
(Kuo et al., 2012} Janice M. Bell,, RN, PhD
www.janicembell.com
Information Sharing
Respect and Honoring Differences
Partnership and Collaboration
Negotiation
Care in the Context of Family and Community

Many Ideas about how to
Implement Patient and Family
Centered Care
• Shift from “allowing” to welcoming
family presence and involvement.
• Partnering with individuals and families to involve
them in care giving and decision making, and
inviting participation in the development of
organizational policy.
Janice M. Bell, RN, PhD
www.janicembell.com

Example: Family Medication Awareness Project
“I would like you to know that I believe in FCC, which means I believe in
working with you as a partner in caring for your child. Please ask me
questions about your child’s medication(s) any time you wish. I care about
your child’s safety and encourage your participation and questions.”
Janice M. Bell, RN, PhD
www.janicembell.com

“Despite widespread endorsement,
Patient and Family Centered Care
continues to be
insufficiently implemented into clinical practice.”
(Kuo et al., 2012; Shields, 2010)
Janice M. Bell, RN, PhD
www.janicembell.com

A Paradigm Shift: If partners in care… then what does this
mean for the patient-family-health care
provider relationship?
Janice M. Bell,, RN, PhD
www.janicembell.com

at the heart of the matter…
health
professionals
Janice M. Bell, RN, PhD
www.janicembell.com relationships
illness
families larger systems
individuals
health
beliefs

THE ILLNESS BELIEFS MODEL ™
Wright, L.M., & Bell, J.M. (2009). Beliefs and Illness: A Model for
Healing. Calgary, Alberta, Canada: 4th Floor Press.
http: //www.illnessbeliefsmodel.com
Janice M. Bell, RN, PhD
www.janicembell.com

Intersection of Beliefs
Beliefs of Society/Culture
Beliefs of Family
Members
Beliefs of the
Patient
Beliefs of Health
Care Providers
(Wright & Bell, 2009) Janice M. Bell, RN, PhD
www.janicembell.com

at the heart of the matter…
Our beliefs often
constrain our
relationships with
patients and families
Janice M. Bell, RN, PhD
www.janicembell.com

Sample Constraining Belief
Janice M. Bell, RN, PhD
www.janicembell.com
“If I talk to patients and family
members, I will not have time to
complete my other responsibilities.”
“I have more knowledge and
expertise and I am usually right.”

at the heart of the matter…
Do you hear me?
Do you see me?
Does what I say mean anything
to you?
Dr. Janice M. Bell
www.janicembell.com
(quote from Oprah, 2011)
Patients and Families want to know:

E
Janice M. Bell, RN, PhD
www.janicembell.com
Empathy exercise from Daniel Pink, 2013

Tips for Perspective-taking
• Increase your power by reducing it.
• Use your head as much as your heart.
• Mimic strategically.
Janice M. Bell, RN, PhD
www.janicembell.com
(Daniel Pink, 2013)

Sample Facilitating Beliefs
Health and illness is a family affair.
I am willing to “open space” to ideas
and preferences that are different
than my own.
Janice M. Bell, RN, PhD
www.janicembell.com
(Wright & Bell, 2009)

Sample Constraining Beliefs:
Janice M. Bell, RN, PhD
www.janicembell.com
•“If I talk to patients and families I may
open up a can of worms, and I will
have no time or skills to deal with it.”
•“I cannot possibly be helpful families
in the brief time that I will be caring for
them.”

Relationships are made visible within a
therapeutic conversation
Janice M. Bell, RN, PhD
www.janicembell.com (Wright & Bell, 2009)

Janice M. Bell, RN, PhD
www.janicembell.com
therapeutic conversations
The importance of the
first 3 seconds
(Wright & Bell, 2009)

• Take the temperature of the relationship frequently
Janice M. Bell, RN, PhD
www.janicembell.com
therapeutic conversations
“Goodness of fit conversations”
(Wright & Bell, 2009)

• In what ways was our discussion useful to each of you, or not useful?
• On a scale of 1-10 how well do you think I understood your situation?
• Is there anything I can to do improve my care of your family?
• Is there anything you were hoping for in this meeting that did not happen?
Janice M. Bell , RN, PhD
www.janicembell.com
therapeutic conversations
(Wright & Bell, 2009)

The skills of therapeutic conversation
with patients and families can be
LEARNED, MODELED, and COACHED
Janice M. Bell, RN, PhD
www.janicembell.com

Sample Facilitating Beliefs
Talking can be healing. (Wright & Bell, 2009)
The quality of the relationship
between patient-family-health-care-
provider influences quality care and
safety
Janice M. Bell, RN, PhD
www.janicembell.com

EVIDENCE: Landspitali University Hospital
Implementation Project, Reykjavik, Iceland
Janice M. Bell, RN, PhD
www.janicembell.com
Erla
Svavarsdottir,
RN, PhD

EVIDENCE: Providence Health Care
Janice M. Bell, RN, PhD
www.janicembell.com
Peggy Simpson RN, PhD
Clinical Nurse Specialist
Psychiatric Consultation
Liaison Mental Health
HIV/AIDS Programs and
Addiction Services
Providence Health Care -
St. Paul's Hospital
Vancouver, B.C.
CANADA

Helpful…
Very h…
Feedback on the …
Physician Coaching Program at the University of
Rochester: A Pilot Study Susan H. McDaniel, PhD
University of Rochester School of Medicine & Dentistry, Rochester, NY
To develop and determine feasibility of a physician
coaching program with the following objectives:
• establishment of sustainable learning community
of physicians to improve patient- and family-
centered care (PFCC)
• improved quality, safety, team communication,
patient/family experience of care, and physician
satisfaction and retention.
Methods
• In 2009, the Vice President of Health Affairs at
URMC articulated a commitment to PFCC in
response to his experiences as a patient in the
wake of a traumatic bicycle accident.
• Newly-announced Centers for Medicare &
Medicaid Services (CMS) enhanced
reimbursements partially based on consumer
satisfaction with interpersonal care (Hospital
Consumer Assessment of Healthcare Providers
and Systems, or HCAHPS)
• PFCC Leader Council meets monthly, advises medical
center leadership, receives training, shares wisdom and
experience.
• Leaders articulated key PFCC behaviors that I distilled
into :
I (Introduce yourself and your role),
C (ask for patient/family Concerns),
U (check for Understanding).
These behaviors top the observational checklist in the
coaching program.
URMC Physician Coaching Program
• I directly observed a broad sampling of 12 physicians
with 78 patients, coding each encounter.
• Physicians received post-session verbal feedback,
written reports on ICU and other PFCC behaviors,
highlighting strengths and specific suggestions for
improvement.
Background
Outcomes
2012 ELAM Leaders
Forum
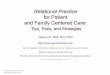
Outcomes Table. Physician characteristics by ICU.
Introduce Concern Understand Characteristic Sex Male 70.8% (17) 70.4% (38) 13.0% (7) Female 100.0% (12) 76.2% (16) 47.6% (10) Physician Status Surgeon 70.8% (17) 64.4% (29) 24.4% (11) Non-surgeon 100.0% (12) 83.3% (25) 20.0% (6) HCAHPS Score Low 76.5% (13) 55.8% (24) 14.0% (6) High 84.2% (16) 93.7% (30) 34.4% (11)
Next Steps
• Scale up the Physician Coaching Program
• Prioritize next groups: MD’s close to reimbursement
threshold, new faculty, disruptive/low scoring MDs,
everyone at reappointment
• Conduct larger descriptive study
• Study coaching intervention and patient
satisfaction, quality, safety, and physician
satisfaction.
•Non-surgeons and females introduced themselves 100%
of the time to new patients.
•Physicians with higher HCAHPS scores 10.6x more likely
to ask about patient concerns than those with lower scores.
•Female physicians 6x more likely to check for
understanding.
•Physicians with higher HCAHPS scores and males took
more time with patients.
Thank you to collaborators Jacqueline Beckerman MSW, Jean Joseph MD,
Tziporah Rosenberg PhD, and Paul Winters MS, and mentors Ronald Epstein
MD, Elizabeth McAnarney MD, and Yeates Conwell MD, for their support of this
project.
“What it did was alleviate my concerns
regarding my patient interactions. She
showed me all the things I was doing
correctly and pinpointed some areas that
could be tweaked in the future. I think
every provider in our department should
meet with her if we are truly going to
make PFCC a global buy-in behavioral
initiative.“
“…I believe this type of experience is
valuable since habits (good or bad)
creep into communication…Very
professional and insightful. I would like
to do this again…”
“She made me realize that I did a lot of
teaching, but did not always elicit
patients’ concerns.”
Purpose

at the heart of the matter…
Changing our beliefs about and
skills to create healing
relationships with patients and
families affects the quality of
care and satisfaction
Janice M. Bell, RN, PhD
www.janicembell.com

a particular
PATIENT AND FAMILY
CENTERED CARE
Janice M. Bell, RN, PhD
www.janicembell.com
kind of practice
(Bell & Wright, 2011; Wright & Bell, 2009)

a particular kind of practice
offered by a
PATIENT AND FAMILY
CENTERED CARE
Janice M. Bell, RN, PhD
www.janicembell.com
particular kind of
health care provider (Bell & Wright, 2011; Wright & Bell,
2009)

at the heart of the matter…
health
professionals
Janice M. Bell, RN, PhD
www.janicembell.com relationships
illness
families larger systems
individuals
health
beliefs

Janice M. Bell, RN, PhD
www.janicembell.com
Wright, L.M., & Bell, J.M. (2009). Beliefs and Illness: A
Model for Healing. Calgary, Alberta, Canada: 4th Floor
Press.
Wright, L.M. (2005). Spirituality, Suffering, and Illness:
Ideas for Healing. Philadelphia, PA: F.A. Davis.
Wright, L.M., & Leahey, M. (2013). Nurses and Families:
A Guide to Family Assessment and Intervention (6th ed.).
Philadelphia, PA: F.A. Davis.
Useful Resources

THE ILLNESS BELIEFS MODEL ™
Wright, L.M., & Bell, J.M. (2009). Beliefs and Illness: A Model for
Healing. Calgary, Alberta, Canada: 4th Floor Press.
http: //www.illnessbeliefsmodel.com
Janice M. Bell, RN, PhD
www.janicembell.com

Journal of Family Nursing
http://jfn.sagepub.com
5 year average Impact Factor: 1.25
Janice M. Bell, RN, PhD, Founding Editor
Janice M. Bell, RN, PhD
www.janicembell.com