Embed Size (px)
Citation preview

Role of HLA in Unrelated
Donor Transplantation
Effie Petersdorf
13th ESH-EBMT Training Course
Blood and Marrow Transplantation
25 May 2009 Latimer, UK

Theme
Human genetic variation is a reflection of the
ethnic/racial background of the population.
• MHC and non-MHC
The biologic implications of genetic diversity
are best examined in ethnically and
racially diverse populations.
• Autoimmunity, infectious diseases, cancer,
transplantation.

The Human Major
Histocompatibility Complex
• The most gene-dense region in the entire
human genome: over 300 loci of which 30%
have immune-related function.
• Functional genes in infection, inflammation,
autoimmunity, cancer and transplantation:
recent genome-wide association studies confirm
MHC region genes involved in T1D, RA, CD,
HIV/AIDs progression.
• High degree of sequence variation and strong
positive long-range linkage disequilibrium.

Challenges in Unrelated
Hematopoietic Cell
Transplantation
1. Diversity of the HLA System
Many patients do not have allele-matched donors.
Can the bar be lowered without compromising safety?
2. Linkage Disequilibrium
Even with precise donor matching, GVHD remains a significant complication.
How can LD be used advantageously to identify new transplantation determinants?

Hallmark of the MHC:
Polymorphism
No.
Alleles*
A B C DRB1 DQB1
697 1109 381 1603 95
9.0 x 1024 Unique Genotypes!
*2008 WHO Nomenclature

Hallmark of the MHC:
Linkage DisequilibriumNon-random association of alleles at nearby loci
Ethnicity/Race A1-B8-
DR0301
A33-
B58-
DR0301
A30-B42-
DR0302
A29-B44-
DR0701
Caucasian 0.062 0.0002 0.00009 0.016
Asian 0.003 0.019 0.00005 0.0007
African 0.012 0.0004 0.0143 0.004
Hispanic 0.017 0.0002 0.002 0.018
www.nmdpresearch.org/HLA/em_haplotype_freq.html

State-of-the-Art: May 2009
Clinical outcome is shaped by:
I. Recipient-donor race/ethnicity
II. Donor HLA match status
III. HLA haplotypes and MHC resident
variation
IV. Non-HLA variation

International Histocompatibility Working
Group in Hematopoietic Cell
TransplantationEst 1996
Theme
The safety and efficacy of HCT may be
increased through a more complete
understanding of the nature of genetic
and non-genetic factors that affect
transplant outcome.

International Histocompatibility Working
Group in Hematopoietic Cell Transplantation
Established 1996
• International collaboration: 37 laboratories,
240 transplant centers and 21 transplant
and donor registries.
• Database: 17,341 (16,198 accepted)
unrelated transplants as of September,
2008.

IHWG Study Population
N=17,341 September 2008
Donor Registry Transplant Registry

HLA Match Status

Characteristics of the 15th WS
IHWG HCT Study PopulationSeptember 200810/10 HLA matched 9 of 10 HLA matched 8 of 10 or less HLA matchedN=7579 N=4136 N=4483
Median recipient age, y (range) 35.8 (0.38-74.5) 33.9 (0.35-75) 30.0 (0.47-72.0)
Year of transplantation - no. (%)1983-1991 202 (2.7) 113 (2.7) 224 (5.0)
1992-1997 1580 (20.8) 920 (22.2) 1285 (28.7)
1998-2002 3115 (41.1) 1722 (41.6) 1817 (40.5)
2003-2007 2626 (34.6) 1329 (32.1) 1116 (24.9)
Unknown 56 (0.7) 52 (1.3) 41 (0.9)
Recipient/donor gender, no. (%)Male/male 3089 (40.8) 1516 (36.7) 1651 (36.8)Male/female 1315 (17.4) 812 (19.6) 1011 (22.6)
Female/male 1645 (21.7) 925 (22.4) 906 (20.2)Female/female 1386 (18.3) 812 (19.6) 865 (19.3)
Unknown 144 (1.9) 71 (1.7) 50 (1.1)
Diagnosis/disease severity*, no. (%)/ no.Acute leukemia/ high-risk, intermediate-risk,missing 3917 (51.7)/ 1088,2773,56 2198 (53.1)/641,1514,43 2342 (52.2)/732,1569,41
Myeloproliferative disorders/ high-risk, intermediate-risk,
low-risk, missing 1843 (24.3)/ 87,454,1246,56 994 (24.0)/ 42,253,654,45 1153 (25.7)/ 98,351,666,38
MDS/ high-risk, intermediate-risk 1009 (13.3)/ 292,435,282 507 (12.2)/151,216,140 476 (10.6)/ 97,142,237Other /high-risk, intermediate-risk, missing 810 (10.7)/ 208,406,196 437 (10.6)/ 108,237,92 512 (11.4)/ 99,303,110
Recipient/donor CMV serology, no. (%)Positive/positive 901 (11.9) 550 (13.3) 475 (10.6)Positive/negative 1323 (17.5 754 (18.2) 617 (13.8)
Negative/positive 657 (8.7) 409 (9.9) 666 (14.9)
Negative/negative 1672 (22.1) 925 (22.4) 366 (8.2)
Unknown 3026 (39.9) 1498 (36.2) 2359 (52.6)

Characteristics of the 15th WS
IHWG HCT Study PopulationSeptember 2008
10/10 HLA matched 9 of 10 HLA matched 8 of 10 or less HLA matchedN=7579 N=4136 N=4483
Transplant type/ Conditioning regimen, no. (%)Ablative/ No TBI 1044 (13.8) 514 (12.4) 336 (7.5)Ablative/ TBI 3134 (41.4) 1763 (42.6) 2094 (46.7)Nonablative 901 (11.9) 535 (12.9) 546 (12.2)Unknown 2500 (33.0) 1324 (32.0) 1507 (33.6)
Source of cells - no. (%)Bone marrow 5857 (77.3) 3208 (77.6) 4058 (90.5)Peripheral blood stem cells 1646 (21.7) 865 (20.9) 363 (8.1)Unknown 76 (1.0) 63 (1.5) 62 (1.4)
GVHD ProphylaxisAny single agent by itself 221 (2.9) 128 (3.1) 104 (2.3)T-cell depletion ± other 829 (10.9) 709 (17.1) 690 (15.4)Two or more agents mixed together 5849 (77.2) 2905 (702) 3484 (77.7)Other or unknown 680 (9.0) 394 (9.5) 205 (4.6)

State-of-the-Art: May 2009
Clinical outcome is shaped by:
I. Recipient-donor race/ethnicity
II. Donor HLA match status
III. HLA haplotypes and MHC resident
variation
IV. Non-HLA variation

Impact of Donor-Recipient Ethnicity on Risk
of Acute GVHD and Survival
in HLA-A, B, C, DRB1, DQB1 Matched
Unrelated Transplantation
Yasuo Morishima, Takakazu Kawase, Satoko
Morishima
on behalf of the IHWG
Aichi Cancer Center, Nagoya, Japan
Japan Marrow Donor Program

Background• The association of ethnicity with GVHD and other
outcomes after HLA identical BMT is well documented.
Comparison of GVHD and survival after HLA-identical sibling BMT in
ethnic population. (Oh H, et al. Blood 105:1408-1416, 2005 )
2-4 A-GVHD

Purpose
● Comparison of the incidence of acute GVHD between ethnic groups based on the same background
1. Large scale IHWG HCT database: 5555 pairs2. HLA allele matched transplant. 10/10 match3. GVHD prophylaxis: T cell replete stem cell
source 4. Leukemia and MDS patients
● Results obtained from this analysis will become basic data for further international analysis of HLA mismatched unrelated HSCT and for donor exchange of unrelated donor.

Ethnicity
Patient – Donor No. of pairs
Asian/Pacific – Asian/Pacific (AA) 2062
(Japanese – Japanese) (2039)
Caucasian – Caucasian (CC) 2419
Black – Black (BB) 39
Hispanic – Hispanic (HH) 21
Native American – Native American (NN) 2
Mismatch race pair (in non-JMDP) (MM) 268
Unknown donor ethnicity 744

Acute GVHD and EthnicityMultivariate models adjusted for clinical factors

Overall SurvivalMultivariate models adjusted for clinical factors

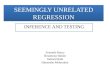
SurvivalLow and intermediate-risk leukemia
HLA - A – DPB1 (12/12) matched
A A (n=505)
C C (n=332)
H H (n=11)
Mismatch ethinicity (n=30)
A:Asian/Pacific C:Caucasian H:Hispanic
Days after transplantation
0 1000 2000 3000 3650
Surv
ival(%
)
0
20
40
60
80
100

State-of-the-Art: May 2009
Clinical outcome is shaped by:
I. Recipient-donor race/ethnicity
II. Donor HLA match status
III. HLA haplotypes and MHC resident
variation
IV. Non-HLA variation

HLA Genetic Variation
• Complex: not SNPs
• Substitutions distributed across 3 class I
exons, one class II exon
• Nucleotide substitutions are concentrated
at positions that are functionally important
for T cell and NK cell allorecognition.
• “Patchwork” overlap in amino acid motifs.

“Patchwork” Nature of HLA
Variation: HLA-DPB1A B C D E F
Courtesy of Bronwen Shaw, MD

Background
Risks after unrelated donor HCT are
influenced by:
• the number of HLA mismatches
• the locus that is mismatched
• the allele and antigen mismatch defined
by their sequence (residues)

Effect of Number of HLA
Mismatches on Mortality
*tally=4, 335/488=69%; tally=5, 125/182=69%; tally=6, 34/51=67%; tally=7, 13/13=100%; tally=8, 2/4=50%; tally=9, 1/2=50%
Tally HR 95% CI p-value
0 (3894/7549=52%)
1 (2403/4116=58%)
2 (1567/2502=63%)
3 (821/1232=67%)
≥ 4* (510/740=69%)
1
1.21
1.45
1.68
1.84
---
1.15-1.27
1.37-1.54
1.56-1.82
1.68-2.02
---
<.0001
<.0001
<.0001
<.0001
Risk of mortality increases as the number of HLA mismatches increases:
Assumption: all mismatches contribute equally to outcome.

Impact of Single Mismatches Relative
to Single HLA-DQB1 Mismatch
Single Mismatch HR 95% CI P-Value
HLA-DQB1 1 --- ---
HLA-A 1.2 1.05 - 1.37 .007
HLA-B 1.29 1.10 - 1.53 .002
HLA-C 1.18 1.05 - 1.33 .004
HLA-DRB1 1.08 0.89 - 1.32 .45
Compared to single DQB1 mismatches, single A, B, C, and DRB1
mismatches are associated with increased risk. Model adjusts for disease risk.

The Impact of HLA-DPB1 Epitope
Matching on the Outcome of URD
HCT
Bronwen Shaw, Katharina Fleischhauer, Elisabetta
Zino, Mari Malkki, Ted Gooley, Effie Petersdorf

HypothesisMismatching for T cell epitopes (TCE) in the HLA-DP molecule may be as
(more) important as allele-matching for predicting outcome of URD HSCT
Zino et al., 2004
DPB1*1001
DPB1*1401
DPB1*1701
DPB1*0301
DPB1*4501
DPB1*0401
and others
DPB1*0901
group 1
group 2
group 3
+ -
-
T cell clones
+ +
TCE
Group-specific rather than allele-specific DPB1 matching:
• TCE-Disparate = “Non-Permissive”
• TCE-Matched = All Others

Methods and Results• 5838 pairs matched for HLA-A,-B,-C,-DRB1,-DQB1 at high
resolution (4 digit) “10/10 matched”
– DPB1 allele-mismatched (n=4490) or 12/12 (n=1348)
– TCE disparate (TCED) in GvH or HvG, or TCE matched (TCEM)
– Results adjusted for classical variables
– Reference: TCEM, DPB1 allele mismatched
HR 95% CI P
TRM 10/10 TCED
12/12
1.26
0.837
1.134-1.399
0.735-0.954
0.00002
0.007
aGvHD 3-4 10/10 TCED
12/12
1.289
0.77
1.104-1.505
0.636-0.933
0.0013
0.007
Overall
mortality
10/10 TCED
12/12
1.156
0.966
1.065-1.255
0.879-1.062
0.00054
0.481
Relapse 10/10 TCED
12/12
0.92
1.316
0.802-1.055
1.151-1.505
0.23613
0.00006

Conclusion and Future Plans
• Ongoing work
– Define impact of the TCE in the 9/10 context
– Analysis of particular diseases (B cell malignanices)
– Role of hypervariable region (HvR) disparity in defining non-
permissive mismatches
10/10 (80%)12/12 (20%)
aGvHD
TRM
Relapse
OS =
14th IHWS
TCED (35%)
OS
TRM
aGvHD
Relapse =
TCEM (55%)
OS
TRM
aGvHD
Relapse =
15th IHWS

Summary
Clinical outcome after unrelated HCT is influenced by:
• The number of HLA mismatches: as the number of mismatches increases, mortality increases. Choose donors with the fewest number of HLA mismatches.
• The locus that is mismatched: compared to single HLA-DQB1 mismatches, other single locus mismatches are associated with increased risk of mortality. There is no “good” mismatch, but relative degrees of “bad” mismatches. When matched donors are not available, avoid HLA-A,B,C and probably DRB1 mismatches.
• The disease risk at the time of HCT: influence of a single HLA mismatch is most evident among low-risk patients. Potential “gain” in a prolonged URD search in the hopes of finding a better matched donor at the expense of disease progression should be weighed very carefully.
• HLA-DPB1 mismatching: an epitope-based matching algorithm may provide choices in optimizing donor selection for up to 55% of patients. Beneficial GVLE associated with mismatching.

State-of-the-Art: May 2009
Clinical outcome is shaped by:
I. Recipient-donor race/ethnicity
II. Donor HLA match status
III. HLA haplotypes and MHC resident
variation
IV. Non-HLA variation


Traherne in International Journal of Immunogenetics 35:179, 2008

Haplotypes
• A combination of markers (alleles) at two or more sites physically linked on the same chromosomal strand.
• The markers are inherited together.
• Markers that are always observed together on the same haplotype can serve as “tags” for one another.
• Tags can be used to identify unknown variation that are linked on the same haplotype.
• How does knowledge of haplotype-linked tag markers facilitate disease mapping?

Tag SNPs
Manolio et al J Clinical Invest 118:1590, 2008

HLA-DR Haplotypes
DR1, 10, 103
DR Haplotype
DRB1 ψ ψ DRA
DRAψ ψDR15, 16
DRB1
DR8
DRAψDRB1
DRB5
DR3, 11, 12, 13, 14
DRAψ ψDRB1 DRB3
DR4, 7, 9
DRAψ ψψDRB1 DRB4
DR Genes

Global Survey of
Haplotype Variation
Conrad et al Nature
Genetics 38:1251, 2006
How similar are ethnically
diverse populations at the
haplotype level?
Surveyed 927 individuals
from 52 populations for
3,024 SNPs in 36 genomic
regions .
Conclusions:
Nearby populations (same
continent) share haplotype
structure.
Number of distinct
haplotypes per region
declines from Africa.

Hypotheses
• MHC haplotypes are a tool for mapping novel transplantation determinants.
• HLA alleles on haplotypes are markers for functional linked MHC resident variation.
• We can query the MHC with the use of Msat and SNP markers.
• We can measure risks associated with donor genotype, recipient genotype, and donor-recipient mismatching.

Father Mother
A1
B8
DR3
DQ2
A2
B44
DR7
DQ2
A3
B7
DR2
DQ1
A11
B60
DR4
DQ4
DonorPatient
A1
B8
DR3
DQ2
A3
B7
DR2
DQ1
A1
B8
DR3
DQ2
A3
B7
DR2
DQ1
a b c d
aa cc a d
Family Segregation of HLA
← Identical by Descent →

PotentialPotential
Unrelated Unrelated
DonorsDonors
PatientPatient
A1
B8
DR3
DQ2
A3
B7
DR2
DQ1
Unrelated Donor Search
? ?
Identical by State

HLA-A,B,DR Matched
Unrelated Pairs

The HLA Complex
6p21.3

HLA-B-Specific Capture and
Haplotype Separation Guo et al PNAS 103:6964,2006

MHC Haplotypes in TransplantationPetersdorf et al PLoS Medicine 4:e8, 2007
• 248 HLA-A,B,C,DRB1,DQB1 allele-identical unrelated donor transplants
• Myeloablative conditioning: TBI-Cy or Bu-Cy
• GVHD prophylaxis: Csp and Mtx
• T-replete Marrow (88%) or PBSC (12%)
• Heterozygous at HLA-B plus at least one other locus (HLA-A and/or DRB1)

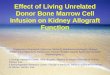
Haplotype Matching Defines
Transplant Outcome
A: Grades 3-4 acuteGVHD; B: Relapse; C: TRM; D: Overall survival
Petersdorf et al PLoS Med, 4(1):e8, 2007

IHWG: Degree of Mismatching for Class I, III, II Microsatellites in
HLA-A, C, B, DRB1, DQB1 Allele-Matched URD Transplants
(n= 819)
Association of Msat mismatching with GVHD or overall mortality.
Malkki et al BBMT 2006

State-of-the-Art: May 2009
Clinical outcome is shaped by:
I. Recipient-donor race/ethnicity
II. Donor HLA match status
III. HLA haplotypes and MHC resident
variation
IV. Non-HLA variation

Immune Response Gene (IRG) and
Cytokine Gene (CG) Polymorphisms in
Unrelated HCT
Hypotheses
CGs/IRGs lower or enhance risks of GVHD and mortality after unrelated HCT.
May account for GVHD after HLA matched HCT.

Pathophysiology of GVHD
Ferrara JML, Best Pract Res Clin Haematol. 20: 91-97, 2007

Study Study Population and
Methods• 1215 10/10 matched BM (95%) and PBSC (5%)
URD transplants (1041 NMDP, 23 FRABET, 151
FHCRC)
• Diagnoses: AML 24%, ALL 16%, CML 60%
• Transplant regimens: TBI 84%; non-TBI 16%
• aGVHD prophylaxis: T-replete 86%; TCD 14%
• 43 SNPs representing 27 IRGs/CGs selected from
literature, dbSNP, Seattle SNPs, SNP 500 CA db
• MAF > 5%
• TaqMan chemistry

Comparison with Current Literature
Bottom line: Comparison of results challenging; larger transplant populations
with diverse ethnicity required through collaborative research
Gene No. aGVHD Relapse Mortality
� � - � � - � � -
CD31 14 7 7 1 2 2 3
IL10 15 4 1 10 1 1 2 9
IL1B 7 1 6 1 1 1 5
MTHFR 7 2 2 2 1 1 1 3
TGFB1 4 2 2 1 3
TLR4 3 3 2 1 1
IL6 9 2 7 1 7
IL4 2 2 1 2
HLA-E 3 1 1 1 2 1 2
NOD2 6 2 1 3 1 1 2 2 2

Theme
• Human genetic variation (MHC and non-
MHC) is a reflection of the ethnic/racial
background of the population.
• The biologic implications of genetic
diversity are best examined in ethnically
and racially diverse populations.

Novembre et al Nature 456:98, 2008
3000 Europeans genotyped for > 500,000
SNPs. Close correlation between genetic
and geographic distances: 2D picture of
genetic variation and geographic map.
Disease associations must account for
genetic structure of population to avoid
spurious associations.

Haplotype Studies
FHCRC/ Petersdorf Lab
Zhen Guo, PhD
Mari Malkki, PhD
Paul Martin, MD
Ted Gooley, PhD
Mark Gatterman
Michelle Baillie
Charlie Du
Sharie Cheng
Institute for Systems
Biology
Leroy Hood, MD,
PhD

HCT Working GroupHCT Working Group
Australia Jeremy Chapman, Jim McCluskey, Frank Christiansen, Peter Bardy,
Campbell Witt, Heather Dunckley, Zlatibor Velickovic, John-Paul Hogbin,
Greg Bennett, Ian Humphries, Patrick Hogan, Rhonda Holdsworth, Ian
Nicholson, Simon Knowles, Mike Varney, Carmel Kanaan, Mary Diviney,
Brian Tait, Linda Smith
Austria Wolfgang Mayr, Gottfried Fischer
Belgium Marie-Paule Emonds, Marc A. Boogaerts, Tribaut Gervais, Augustin
Ferrant, Dominique Latinne
Brazil Noemi Pereira, Ricardo Pasquini
Canada Marlis Schroeder, Luvinia Kwan, Shaunna Kawaleski
Czech Republic Jindra Pavel, Vladimir Koza, Petra Venigova
Denmark Mette Voldby Larsen, Soren Buus, Ilka Hoof, Ole Lund
France Colette Raffoux, Jean Dausset, Jean-Denis Bignon, Eliane Gluckman ,
Katia Gagne, Valerie Dubois, Lucette Gebuhner, Agnes Moine, Lena
Absi, Dominique Charron, Pascale Loiseau, Monique Bois, Marie-Lorraine
Appert, Marc Busson, Anne Dormoy, Dominique Masson, Muriel
DeMatteis, Christophe Picard, Agnes Basire, Coralie Frassati, Anne
Cambon-Thomsen, Pierre Antoine Gourrard
Germany Gerhard Ehninger, Carlheinz Muller, Shraga Goldman, Ekkehard Albert
Dietger Niederwieser, Ute Hegenbart, Martin Bornhauser, Monika
Fuessel
Italy Domenico Adorno, Sonia Nesci, Miryam Martinetti, Angelica Canossi,
Paolo Di Bartolomeo, Annamaria Pasi, Emilio Paolo Alessandrino,
Giuseppe Visani, Katarina Fleischhauer, Elisabeta Zino, Andrea Velardi

Japan Takehiko Sasazuki, Takakazu Kawase,Takeo Juji, Yoshika Kodera, Yasuo
Morishima
Netherlands Jan van Rood, Machteld Oudshoorn, Jan Cornelissen, Marcel Tilanus, John
Lee, Martin Heemskerk, Anja van Biezen
Norway Torstein Egeland, Erik Thorsby, Lorentz Brinch
South Africa Ernette DuToit, Peter Jacobs, Sister Lucille Wood
Sweden Mats Bengsson, Olle Olerup, Olle Ringden, Marie Schaffer
Switzerland Jean-Marie Tiercy, Alois Gratwohl, U. Schanz, R. Seger, Jacob Passweg
Taiwan Tsung Dao Lee
United Kingdom John Goldman, Alejandro Madrigal, Steven Marsh, Bronwen Shaw,
Ann-Margaret Little, Anne Dickinson, Kim Pearce, Arlene Frater,
Brendan Clarke, Gordon Cook, Cristina Navarrete, Carmen Ruiz de Elvira,
Marco Miretti
USA Mary Horowitz, Steve Spellman, Michelle Setterholm, Michael Haagenson,
Martin Maiers, Loren Gragert, John Klein, Waleska Perez, Seth Ketelsen,
Doug Rizzo, Mary Carrington, Katharine Hsu, Bo Dupont, Michelle Chiu,
David Senitzer, John Hansen, Eric Mickelson, Gary Olsem, Gary Schoch,
Lue Ping Zhao, Sue Li
Registries ABMDR, ANRC, CIBMTR/NMDP, EBMT, Europdonor, JMDP, SFGM, Typhon
NIH NCBI, NLM; Francesca Macchiarini, Mike FeoloSeattle Lab Mari Malkki, Mark Gatterman, Dawn MoranBiostatistics Ted Gooley, John Klein, Tao Wang