-
7/24/2019 Perthes Disease - By Abdul Karim
1/68
Perthes disease
ByDr. Abdul Karim
Postgraduate Resident Orthopedic Surgery
PGMI!G". !A"OR#$ PAKIS%A&.
-
7/24/2019 Perthes Disease - By Abdul Karim
2/68
'IRS% D#S(RIB#DB) LEGG* A&D
WALDENSTORMI& +,-,* A&D B)PERTHESA&DCALVEI&
+,+-
-
7/24/2019 Perthes Disease - By Abdul Karim
3/68
D#'I&I%IO&
!egg(al/0Perthes
disease 1!(PD2 is thename gi/en toidiopathicosteonecrosis o3
the
capital 3emoralepiphysis in a child.
-
7/24/2019 Perthes Disease - By Abdul Karim
4/68
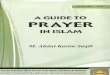
Increased Joint
space
Smaller head
Denser headNormal
joint
-
7/24/2019 Perthes Disease - By Abdul Karim
5/68
#pidemiology
Prevalence4
-
7/24/2019 Perthes Disease - By Abdul Karim
6/68
#pidemiology
Race: Caucasiansare a33ectedmore 3re5uently than persons o3other
races.
Sex: Malesare a33ected !" #imesmoreo3ten than 3emales.
A$e: !(PD most commonly is seen inpersons aged %!&' (ears*
6ith amedian age o3 7 years.
-
7/24/2019 Perthes Disease - By Abdul Karim
7/68
B!OOD S8PP!)
-
7/24/2019 Perthes Disease - By Abdul Karim
8/68
(auses
#9act causeun:no6n.
Pro)ose*
#+eories. Inherited protein (
andor S de3iciency. ;enous thrombosis Arterial occlusion Raised
intra
osseous pressure
-
7/24/2019 Perthes Disease - By Abdul Karim
9/68
(auses
Pro)ose* #+eories. #9cessi/e 3emoral anti/ersion. Syno/itis.
Generali
-
7/24/2019 Perthes Disease - By Abdul Karim
10/68
Causes
-
7/24/2019 Perthes Disease - By Abdul Karim
11/68
Pa#+o)+(siolo$( %he capital 3emoral epiphysisal6ays is in/ol/ed.
In +=
>-?o3 patients 6ith !(PD* in/ol/ement is bilateral.
%he blood supplyto the capital 3emoral epiphysis is
interrupted.
Bone in3arctionoccurs* especially in the subchondralcortical
bone* 6hile articular cartilage continues togro6. 1Articular
cartilage gro6s because its nutrients
come 3rom the syno/ial 3luid.2
Re/asculari
-
7/24/2019 Perthes Disease - By Abdul Karim
12/68
Pa#+o)+(siolo$(
At this point* a percentage o3 patients de/elop!(PD* 6hile other
patients ha/e normal bonegro6th and de/elopment.
!(PD is present 6hen a subchondral 3ractureoccurs. %his is
usually the result o3 normalphysical acti/ity* not direct trauma to
the area
(hanges to the epiphyseal gro6th plate occursecondary to the
subchondral 3racture.
-
7/24/2019 Perthes Disease - By Abdul Karim
13/68
Pa#+o$enesis
A/ascular necrosis %emporary cessation o3 gro6th
Re/asculari
-
7/24/2019 Perthes Disease - By Abdul Karim
14/68
Clinical
His#or(: Symptoms usually ha/e beenpresent 3or 6ee:s.
"ip or groin pain* 6hich may be
re3erred to the thigh Mild or intermittent pain in anterior
thigh or :nee
!imp 8sually no history o3 trauma
-
7/24/2019 Perthes Disease - By Abdul Karim
15/68
Clinical
P+(sical: Pain3ul gait
Decreased range o3 motion1ROM2*particularly 6ith internal
rotation andabduction
Atrophy o3 thigh musclessecondary to
disuse Muscle spasm !eg length ine5ualitydue to collapse
-
7/24/2019 Perthes Disease - By Abdul Karim
16/68
Clinical
Short stature4 (hildren 6ith !(PDo3ten ha/e delayed bone
age.
Roll test @ith patient lying in the supine position*the e9aminer
rolls the hip o3 the a33ectede9tremity into e9ternal and
internal
rotation. %his test should in/o:e guarding or
spasm* especially 6ith internal rotation.
-
7/24/2019 Perthes Disease - By Abdul Karim
17/68
Di,,eren#ials
-nila#eral Septic hip %o9ic syno/itis
Slipped 3emoralcapital epiphysis
Spondyloepiphysealdysplasia
Metaphysealdysplasia !ymphoma
.ila#eral "ypothyroidism Multiple epiphyseal
dysplasia Spondyloepiphyseal
dysplasia Sic:le cell disease
-
7/24/2019 Perthes Disease - By Abdul Karim
18/68
Wor/u)
La0 S#u*ies:
(B(
#rythrocyte sedimentation rate Maybe ele/ated i3 in3ection
present
-
7/24/2019 Perthes Disease - By Abdul Karim
19/68
Wor/u)
1ma$in$ S#u*ies: Plain 9rays o3 the hipare e9tremely use3ul
in
establishing the diagnosis. 'rog leg /ie6s o3 the a33ected hip
are /ery help3ul.
Plain radiographs ha/e a sensiti/ityo3 ,7?and aspeci3icityo3
7?in the detection o3 !(PD
Multiple radiographic classi3ication systemse9ist*based on the
e9tent o3 abnormality o3 the capital3emoral epiphysis.
@aldenstrom* (atterall* Salter and %hompson* and"erringare the
most common classi3icationsystems.
&o agreement has been reached as to the bestclassi3ication
system.
-
7/24/2019 Perthes Disease - By Abdul Karim
20/68
Radiographic stages
'i/e radiographic stagescan be seenby plain 9ray. In se5uence*
they areas 3ollo6s4
-
7/24/2019 Perthes Disease - By Abdul Karim
21/68
Radiographic stages
1.Cessation of growth at
the capital femoral
epiphysis; smallerfemoral head epiphysis
and widening of
articular space on
affected side.
-
7/24/2019 Perthes Disease - By Abdul Karim
22/68
Radiographic stages
>. Subchondral3racture$ linear
radiolucency 6ithinthe 3emoral headepiphysis
-
7/24/2019 Perthes Disease - By Abdul Karim
23/68
Radiographic stages
C. Resorption o3 bone
-
7/24/2019 Perthes Disease - By Abdul Karim
24/68
Radiographic stages
. Reossi3ication o3 ne6 bone
-
7/24/2019 Perthes Disease - By Abdul Karim
25/68
Radiographic stages
=. "ealed stage
-
7/24/2019 Perthes Disease - By Abdul Karim
26/68
-
7/24/2019 Perthes Disease - By Abdul Karim
27/68
(atterall classi3ication
Ca##erall Grou) 14 In/ol/ement only o3 the an#eriorepiphysis
1there3ore seen only on the 3rog lateral 3ilm2
Ca##erall Grou) 114 Cen#ral segment 3ragmentation
and collapse. "o6e/er the lateral rim is intact and thusprotects
the central in/ol/ed area. Ca##erall Grou) 1114 %he la#eralhead is
also in/ol/ed
or 3ragmented and only the medial portion is spared.%he loss o3
lateral support 6orsens the prognosis.
Ca##erall Grou) 1V4 %he en#ire +ea*is in/ol/ed. (atteralls
classi3ication has a signi3icant inter and intra
obser/er error.
-
7/24/2019 Perthes Disease - By Abdul Karim
28/68
-
7/24/2019 Perthes Disease - By Abdul Karim
29/68
(atterall classi3ication
Grou)s 1 an* 11had a goodprognosis1in ,-?2 and re5uired
nointer/ention.
Grou)s 111 an* 1Vhad a poorprognosis1in ,- ?2 and
re5uiredtreatment.
%he classi3ication is applied to the 3roglateral and AP 3ilm
during the3ragmentation phase
-
7/24/2019 Perthes Disease - By Abdul Karim
30/68
Salter and %hompson (lassi3ication
Salter and %hompson recognihead in/ol/ed.
Sal#er 2 T+om)son Grou) .4 More than+>head in/ol/ed.
Again the main di33erence bet6een theset6o groups is the
integrity o3 the lateralpillar.
-
7/24/2019 Perthes Disease - By Abdul Karim
31/68
-
7/24/2019 Perthes Disease - By Abdul Karim
32/68
1"erring2 !ateral Pillar(lassi3ication
La#eral Pillar Grou) A:%here is no lossin heighto3the lateral +C
o3 the head and minimal densitychange. 'ragmentation occurs in the
central segmento3 the head.
La#eral Pillar Grou) .:%here is lucency and loss o3height in the
lateral pillar but not more that =-?o3the original 1contralateral2
pillar height. there may besome lateral e9trusion o3 the head.
La#eral Pillar Grou) C:%here is greater than =-?
lossin the height o3 the lateral pillar. %he lateral pillaris
lo6er than the central segment early on.
-
7/24/2019 Perthes Disease - By Abdul Karim
33/68
-
7/24/2019 Perthes Disease - By Abdul Karim
34/68
1n#rao0server an* in#ero0server relia0ili#( o,Ca##erall3
Herrin$3 Sal#er!T+om)son an* S#ul0er$classi,ica#ion s(s#ems in
Per#+es4
Conclusions4 %he results o3 our studysuggest the use o3
(atterall and Salter%hompson systems prior to treatment and the
Stulberg system at the end o3 the treatmentat s:eletal
maturity."o6e/er* e/aluation o3the patients during the treatment
period isstill a dilemma and necessitates a ne6 morereliable
classi3ication system. Eournal o3 Pediatric Orthopaedics B.
+C1C24+FF+F,* May >--.
Agus, Haluk a; Kalenderer, Onder a; Eryanlmaz, Gurkan
b[latin
dotless i]; Ozcalabi, Isa Turkay a
-
7/24/2019 Perthes Disease - By Abdul Karim
35/68
Unilateral erthes with entire head in!ol!ement and
fragmentation. "he
reossification phase has not yet #egun.
-
7/24/2019 Perthes Disease - By Abdul Karim
36/68
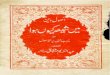
Unilateral erthes disease with widening of the medial joint
space$ #lurring of
the physis$ increased density of the head and lucency #etween
the medial and
central 1%&'s of the head corresponding to early
fragmentation phase.
-
7/24/2019 Perthes Disease - By Abdul Karim
37/68
Unilateral erthes in the
reossification phase with
a !isi#le su#chondral line
similar to (aldenstrom's
sign. )owe!er
(aldenstrom's
su#chondral fracture is
seen !ery early in the
disease process$ #efore
fragmentation. In this
case the lateral pillar hasmaintained some
integrity.
-
7/24/2019 Perthes Disease - By Abdul Karim
38/68
Hea* a# ris/ si$nsH
+. Ga$e5s si$n. a ; shaped lucency in thelateral epiphysis.
>. la#eral calci,ica#ion1lateral to the
epiphysis2 1implies loss o3 lateral support2C. la#eral
su0luxa#ion o, #+e +ea*.
1implies loss o3 lateral support2
. A +ori6on#al $ro7#+ )la#e.1implies agro6th arrest phenomenon
andde3ormity2
-
7/24/2019 Perthes Disease - By Abdul Karim
39/68
Wor/u)
%echnetium ,, bonescan "elp3ul indelineating the e9tento3
a/ascular changesbe3ore they are e/ident
on plain radiographs. %he sensiti/ity o3
radionuclide scanningin the diagnosis o3 !PDis ,?* and
thespeci3icity is ,=?.
Dynamic arthrographyAssesses sphericity o3the head o3 the
3emur.
-
7/24/2019 Perthes Disease - By Abdul Karim
40/68
8ltrasonographyin transientsyno/itis and early Perthes
disease
8ltrasonography may pro/ide signi3icant
diagnostic clues to di33erentiate earlyPerthes 3rom transient
syno/itis.
% 'utami* ) Kasahara* S Su
-
7/24/2019 Perthes Disease - By Abdul Karim
41/68
(% Scan Staging determined
by using plainradiographic3indings is
upgraded in C-? o3patients.
&ot as sensiti/e asnuclear medicine or
MRI. (% may be used 3or
3ollo6up imagingin patients 6ith!PD.
-
7/24/2019 Perthes Disease - By Abdul Karim
42/68
MRI
It allo6s more preciselocali
-
7/24/2019 Perthes Disease - By Abdul Karim
43/68
Ou#come varia0les
Age #9tent o3 in/ol/ement
Duration Remodeling potential Premature physeal closure
%ype o3 treatment Stage o3 disease at treatment.
-
7/24/2019 Perthes Disease - By Abdul Karim
44/68
Trea#men#
Goals o, #rea#men# Achie/e and maintain ROM Relie/e 6eight
bearing (ontainment o3 the 3emoral epiphysis
6ithin the con3ines o3 the acetabulum %raction
-
7/24/2019 Perthes Disease - By Abdul Karim
45/68
Ra#ional 0e+in* 8con#ainmen#8
Salter has demonstrated the biologicplasticity"o3 the 3emoral
head in pigs3ollo6ing a /ascular insult.
(ontainment o3 the head 6ithin theacetabulum is reported to
encouragespherical remodelling during thereossi3ication and
subse5uent phases.
"o6e/er i3 there is total head in/ol/ement
and the lateral pillar collapses then the e33ecto3 containment
is probably less. %here3ore it seems that the e9tent o3
in/ol/ement o3 the head is the critical 3actorand containment
simply optimi
-
7/24/2019 Perthes Disease - By Abdul Karim
46/68
Me*ica#ions Medical treatment does not stop or re/erse
the bony changes. Appropriate analgesic medication should be
gi/en. onsteroidal anti!in"lammatory drugs
Ibupro3en Adult dose4 >---- mg PO 5Fh$ not to e9ceed C.>
gd. Pediatric dose4 F months to +> years4 >-- mg:gd PO
di/ided
tid or 5id$ start at lo6er end o3 dosing range andtitrate
up6ard$ not to e9ceed >. gdJ+> years4 Administer as in
adults.
-
7/24/2019 Perthes Disease - By Abdul Karim
47/68
Non sur$ical con#ainmen#
-
7/24/2019 Perthes Disease - By Abdul Karim
48/68
Scotish Rite abduction brace
-
7/24/2019 Perthes Disease - By Abdul Karim
49/68
Japenes modification ofpetrie abduction cast
-
7/24/2019 Perthes Disease - By Abdul Karim
50/68
-
7/24/2019 Perthes Disease - By Abdul Karim
51/68
Surgical containment
-
7/24/2019 Perthes Disease - By Abdul Karim
52/68
-
7/24/2019 Perthes Disease - By Abdul Karim
53/68
-
7/24/2019 Perthes Disease - By Abdul Karim
54/68
-
7/24/2019 Perthes Disease - By Abdul Karim
55/68
-
7/24/2019 Perthes Disease - By Abdul Karim
56/68
Grea#er #roc+an#ericover$ro7#+
%he trochanteric o/ergro6th can be dramatic onradiographs but
se/eral studies ha/e sho6n thata %rendelenberg gait does not al6ays
occur.
I3 it does occur* and is signi3icant* thentrochanteric
ad/ancementmay impro/e thegait.
An alternati/e is to per3orm a trochantericarrestat an earlier
date but this assumes thatthe 3irst statement 6ill not apply to
theparticular child.
-
7/24/2019 Perthes Disease - By Abdul Karim
57/68
R#(O&S%R8(%I;# S8RG#R)
1ND1CAT1ONS4 Hin$e a0*uc#ion4 /algus subtrochanteric
osteotomy. Mal,orme* ,emoral +ea*
in late group III or residualgroup I;. Garceaus cheilectomy.
Coxa ma$na4 shel3 augmentation A lar$e mal,orme*
,emoral +ea* 7i#+ la#eralsu0laxa#ion4 (hiaris
pel/icosteotomy.
Ca)i#al ,emoral )+(sealarres#4 trochanteric
ad/ancement or
arrest.
-
7/24/2019 Perthes Disease - By Abdul Karim
58/68
A S%8D) A% (I&(I&&A%II&S%I%8%#
Hin$e a0*uc#ion an* 9oin# s#i,,ness in)er#+es *isease: E,,ec# o,
me*ial so,# #issue release an* )e#rie
cas#in$ )rior #o ,emoral +ea* con#ainmen#4
"ypothesis4 (orrect hinge abduction Impro/e motion
&ormali
-
7/24/2019 Perthes Disease - By Abdul Karim
59/68
-
7/24/2019 Perthes Disease - By Abdul Karim
60/68
-
7/24/2019 Perthes Disease - By Abdul Karim
61/68
(O&(!8SIO&
Medial capsulotomy and dynamicpositiong e33ecti/ely corrects
hingedabduction.
ROM 6as impro/ed in all parameters. "igh degree o3 patient and
parent
satis3action.
-
7/24/2019 Perthes Disease - By Abdul Karim
62/68
S-MMAR
'or patients less that F yearsold theprognosisis good3or the
maLority.
I3 they are sti33 or pain3ul they respondto bed rest* traction
and pain relie/ingantiin3lammatory medication.
%here is no e/idence that abduction
splints or surgical inter/ention is6arranted in the maLority o3
theseyounger patients.
-
7/24/2019 Perthes Disease - By Abdul Karim
63/68
S-MMAR
'or patients bet6een F and yearsbut 6ith abone age less than F
and an intact lateral pillar1"erring A and B2 the prognosisis
similar tothat 3or the 3irst group and obser/ation is as
goodas surgical inter/ention 3or the maLority. I3 they ha/e bone
ages greater than F years
and "erring lateral pillar classi3ication B thencontainment o3
the head 6ithin theacetabulum seems to be 6arranted.
%his may be done by abduction bracing*3emoral /arus osteotomy or
a pel/ic osteotomy.
-
7/24/2019 Perthes Disease - By Abdul Karim
64/68
S-MMAR
I3 they are bet6een F and and are inlateral pillar group (then
the result o3inter/ention are e5ui/ocal.
(hildren presenting 6ith Perthes disease atage , or oldero3ten
ha/e lateral pillar B or(and a poor prognosis.
%he trend is to6ards early containmento3
these hips although sti33ness can be aproblem 3ollo6ing early
pel/ic 1Salters2osteotomy.
-
7/24/2019 Perthes Disease - By Abdul Karim
65/68
;ollo7!u)
Initially* close 3ollo6upis re5uired todetermine the e9tent o3
necrosis.
Once the healing phasehas beenentered* 3ollo6up can be e/ery
Fmonths.
!ongterm 3ollo6upis necessary to
determine the 3inal outcome.
-
7/24/2019 Perthes Disease - By Abdul Karim
66/68
Com)lica#ions
;emoral Shortening
sti33ness Malrotation !imp Positi/e
trendelenburg
Pelvic !enghtening Sti33ness (hondrolysis 'ailure o3
containment
-
7/24/2019 Perthes Disease - By Abdul Karim
67/68
Pro$nosis
%he youngerthe age o3 onset o3 !(PD*the betterthe prognosis.
(hildren older than +- yearsha/e a
/ery high ris: o3 de/elopingosteoarthritis.
Most patients ha/e a 3a/orable outcome.
Prognosis is proportional to the degreeo3 radiologic
in/ol/ement.
-
7/24/2019 Perthes Disease - By Abdul Karim
68/68