Embed Size (px)
Citation preview
10/7/2016
1
Perspectives on EMS ValueViews from our Partners in Care
Your Panel…
John MezoGeneral ManagerVITAS Healthcare of Fort Worth
Trudi Stafford, PhD, RN, NEA‐BCPresident & CEOStafford & Associates, LLC
Stacy Elmer, Senior ConsultantCommunity Paramedicine Program LeadKaiser Permanente
Kate Jones, MSN, RN, CCMSVP, Public Policy and ResearchAmedisys Inc.
What We’re Gonna Do…
• Answer key questions…
– How has your perception of value in general changed in the past 2‐3 years?
– What have you looked for from EMS in the past?
– What will you be looking for from EMS in the future?
– What are the ways EMS agencies can demonstrate value to you?
10/7/2016
2
Txt to 817‐991‐4487
Quick Glance at Skilled Home Health Care (Medicare benefit)
Approximately 12,000 home health agencies
provide care to about 3.4 million Medicare beneficiaries
24% of Medicare home health users are 85years of age or older, 37% live alone, and 85%
have 3 or more chronic conditions
Kate Jones
CMS / Home Health Quality
• Home health star ratings
• Publicly reported on “Home Health Compare”
•medicare.gov/homehealthcompare
• Home health value based purchasing (HHVBP)
• innovation.cms.gov/initiatives/home‐health‐value‐based‐purchasing‐model
10/7/2016
3
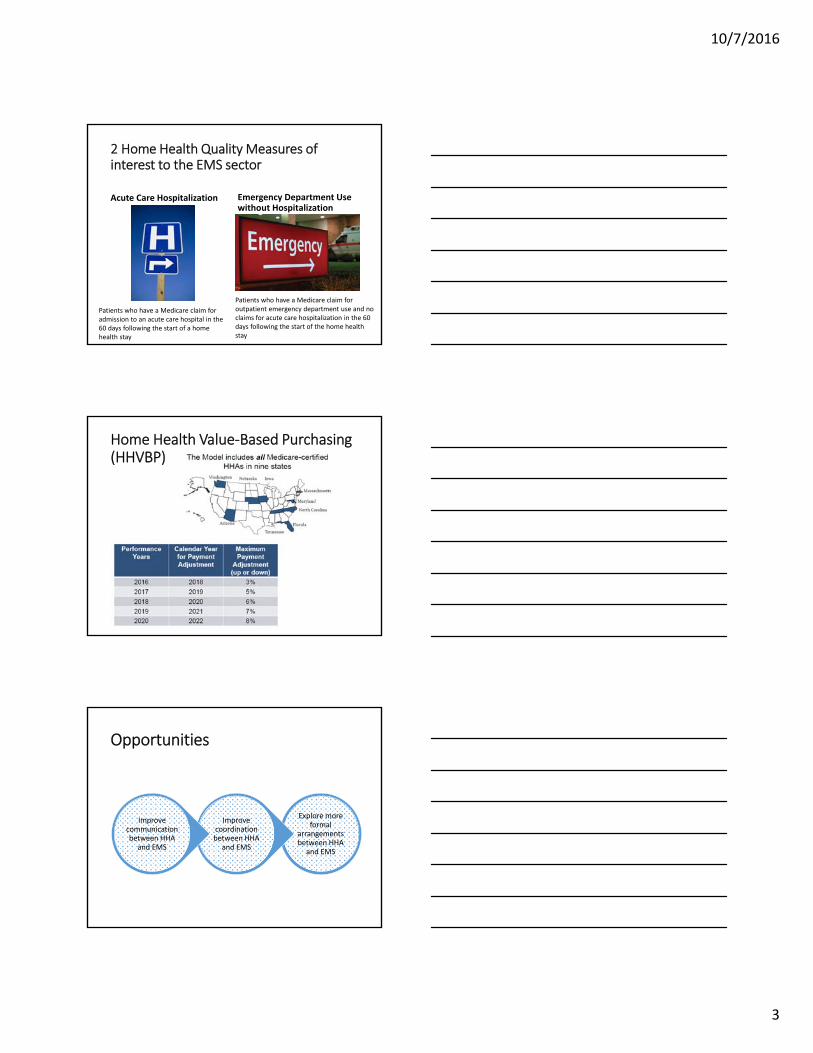
2 Home Health Quality Measures of interest to the EMS sector
Acute Care Hospitalization Emergency Department Use without Hospitalization
Patients who have a Medicare claim for admission to an acute care hospital in the 60 days following the start of a home health stay
Patients who have a Medicare claim for outpatient emergency department use and no claims for acute care hospitalization in the 60 days following the start of the home health stay
Home Health Value‐Based Purchasing (HHVBP)
Opportunities
Explore more formal
arrangements between HHA
and EMS
Improve coordination between HHA
and EMS
Improve communication between HHA
and EMS
10/7/2016
4
Txt to 817‐991‐4487
Framing the Hospice Issue:
• Patients & families want the patient to pass comfortably at home
• Hospice wants the patient to pass peacefully at home
• Death is scary
• When death is near….
• 9‐1‐1 usually = Hospice Revocation
– Voluntary or involuntary
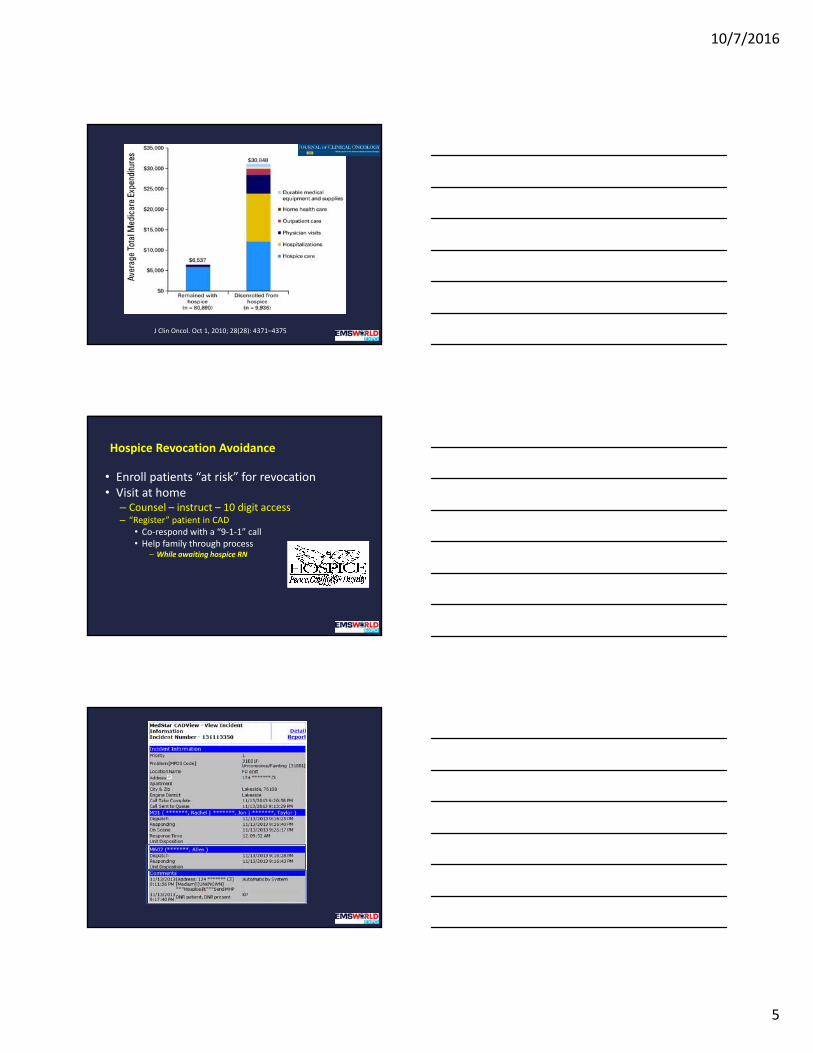
Economic Model
• Hospice benefit– Per diem from payer to agency– Agency pays hospice related care– LOS issues– Varies based on Dx
• MedPAC recommends increasing hospice benefit
• IHI recommends increase hospice enrollment
10/7/2016
5
J Clin Oncol. Oct 1, 2010; 28(28): 4371–4375
Hospice Revocation Avoidance
• Enroll patients “at risk” for revocation• Visit at home
– Counsel – instruct – 10 digit access– “Register” patient in CAD
• Co‐respond with a “9‐1‐1” call• Help family through process
– While awaiting hospice RN
10/7/2016
6
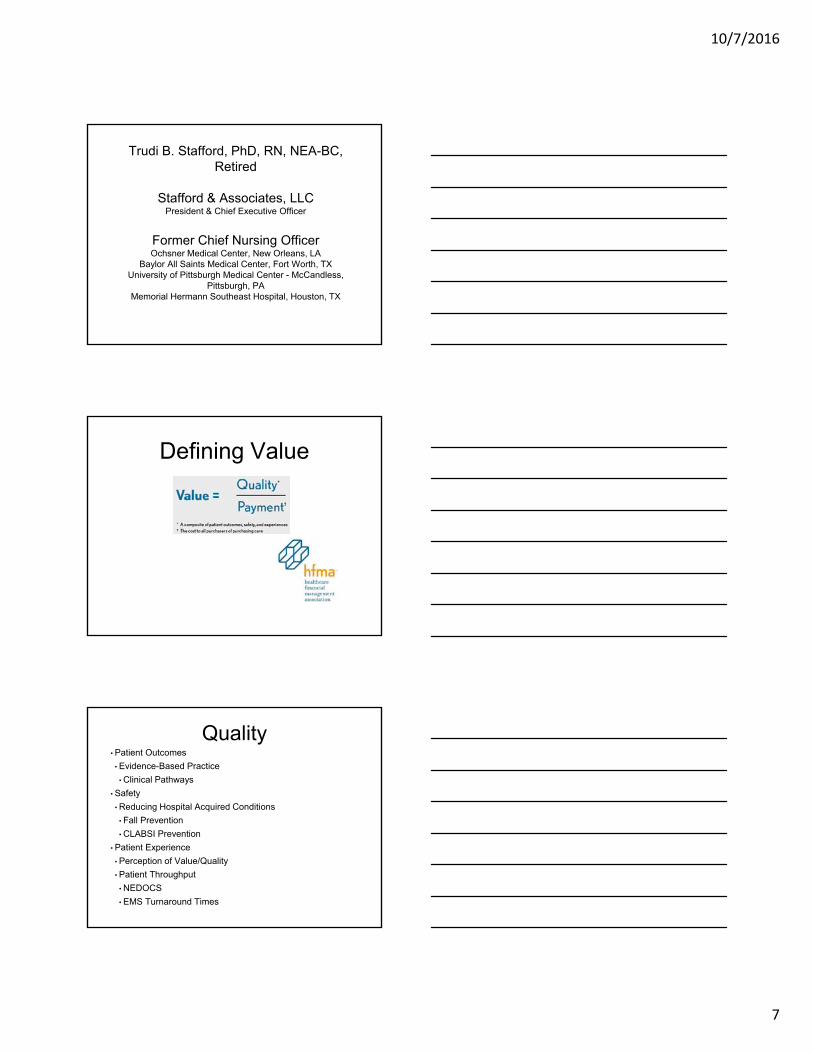
Notes:(1) Patients referred who are identified as at high risk for voluntary disenrollment, or
involuntary revocation.(2) Difference results from referrals outside the MedStar service area, or patients
who declined program enrollment.(3) Patients who either voluntary disenrolled, or had their hospice status revoked.
Hospice Program SummarySept. 2013 ‐ July 2016
# %Referrals (1) 321Enrolled (2) 225
Deceased 161 71.6%Active 27 12.0%
Improved 2 0.9%
Revoked (3) 37 16.4%
Activity:EMS Calls 93
Transports 53 57.0%Hospice Related 29 31.2%
Direct Admits 7 13.2%ED visits 46 86.8%
From: John Mezo [mailto:[email protected]] Sent: Tuesday, February 9, 2016 10:38 AMTo: Matt Zavadsky; Desiree PartainCc: Monica CushionSubject: Great call!
Hi Matt & Desi,Excellent call last night by MedStar! It's so good when everything works as planned.
Also, JCAHO recommended we submit the Hospice Revocation Avoidance program to them as a Joint Commission Leading Practice for Healthcare Providers.
Very cool,JM
10/7/2016
7
Trudi B. Stafford, PhD, RN, NEA-BC, Retired
Stafford & Associates, LLCPresident & Chief Executive Officer
Former Chief Nursing OfficerOchsner Medical Center, New Orleans, LA
Baylor All Saints Medical Center, Fort Worth, TXUniversity of Pittsburgh Medical Center - McCandless,
Pittsburgh, PAMemorial Hermann Southeast Hospital, Houston, TX
Defining Value
THE
Quality• Patient Outcomes
• Evidence-Based Practice
• Clinical Pathways
• Safety
• Reducing Hospital Acquired Conditions
• Fall Prevention
• CLABSI Prevention
• Patient Experience
• Perception of Value/Quality
• Patient Throughput
• NEDOCS
• EMS Turnaround Times
10/7/2016
8
Payment
• Value-Based Purchasing
• Hospital Acquired Conditions
• Readmission Reductions Program
Future of Healthcare• Healthcare Value Equation Refinement
• Technology
• Wearable
• Electronic Medical Records
• Point of Care Testing
• Evidence-based Practice
• Right role, right place, right time, right treatment
• Patient Experience
• Wellness
• Communication
• Transparency
"It's gotta go. Repeal and replace with something terrific."Donald Trump, candidate for the Republican presidential nomination, on the Affordable Care Act, in an interview with CNN
"Repeal of the ACA would let insurers write their own rules again, and wipe out coverage for 16 million Americans."Hillary Rodham Clinton, candidate for the Democratic presidential nomination, on Twitter
10/7/2016
9
25
The Value of Mobile Integrated Healthcare for Kaiser PermanenteStacy Elmer, MA, MPA, EMTEMS World ConferenceOctober 2016
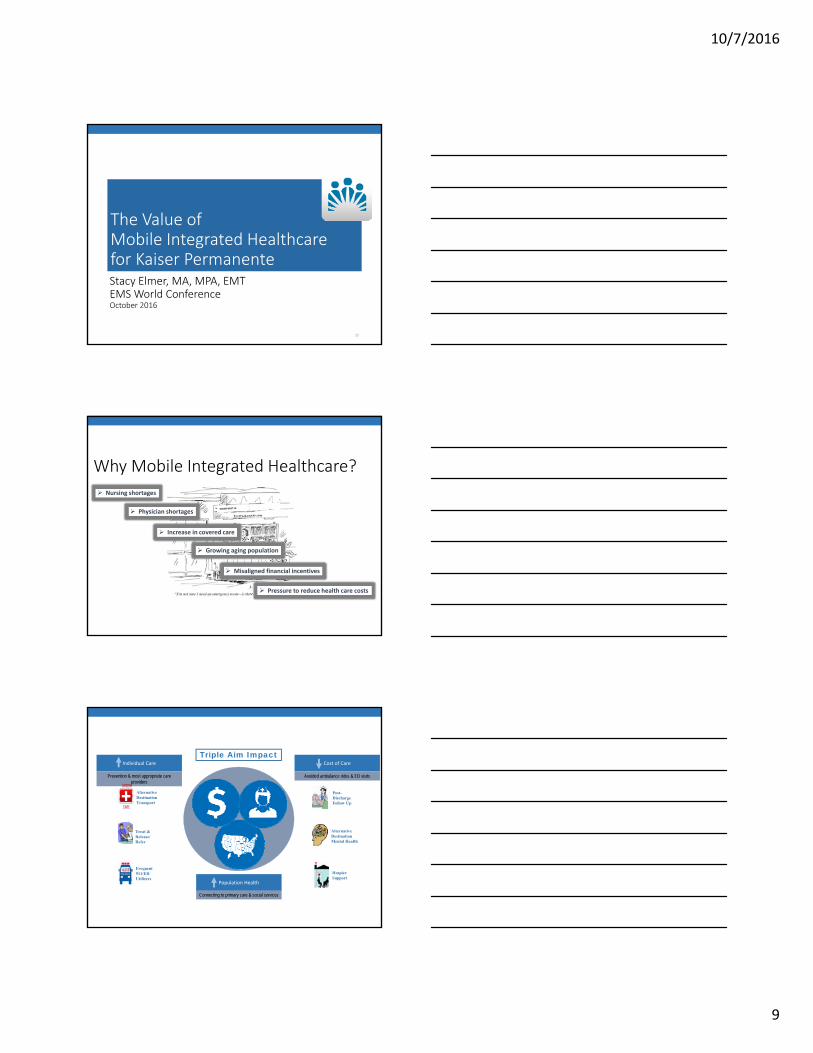
Why Mobile Integrated Healthcare?
Growing aging population
Pressure to reduce health care costs
Increase in covered care
Nursing shortages
Physician shortages
Misaligned financial incentives
Cost of Care
Avoided ambulance rides & ED visits
Individual Care
Prevention & most appropriate care providers
Population Health
Connecting to primary care & social services
URGENT
CARE
Alternative Destination Transport
Frequent 911/ED Utilizers
Treat & Release/ Refer
Post-Discharge Follow Up
Alternative Destination Mental Health
Hospice Support
Triple Aim Impact
10/7/2016
10
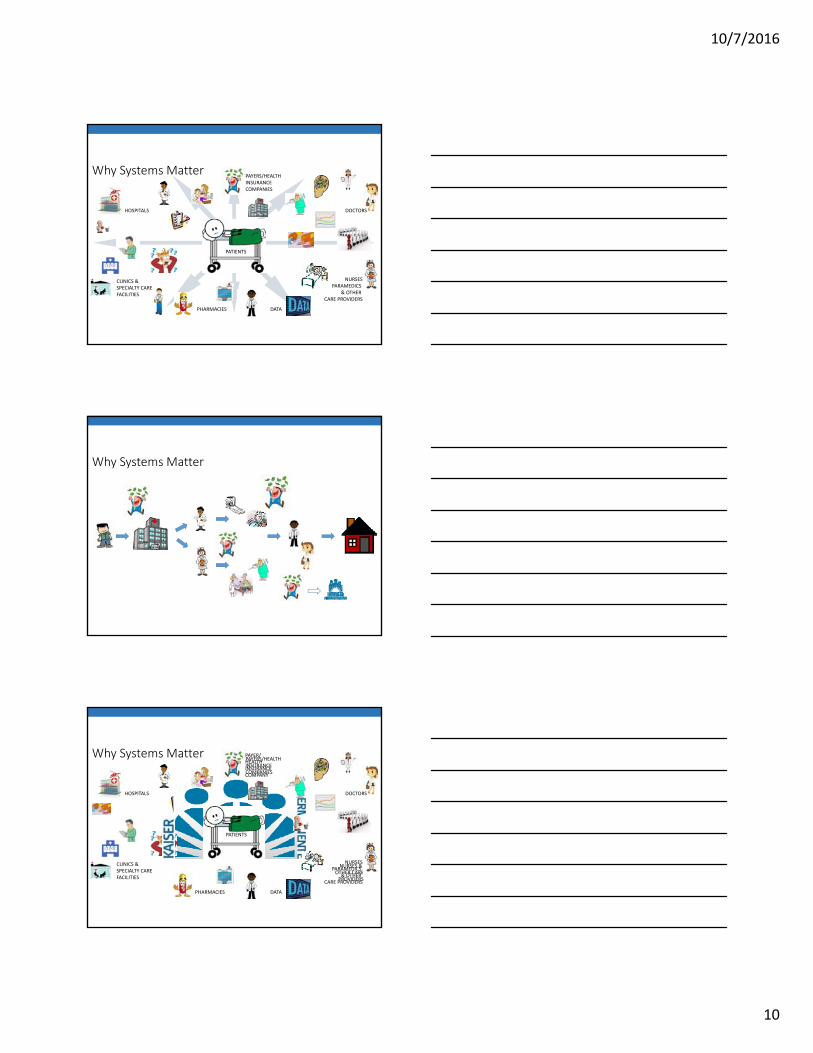
Why Systems Matter
HOSPITALS
CLINICS & SPECIALTY CAREFACILITIES
DOCTORS
NURSESPARAMEDICS
& OTHER CARE PROVIDERS
PHARMACIES
PAYERS/HEALTH INSURANCECOMPANIES
DATA
PATIENTS
Why Systems Matter
Why Systems Matter
HOSPITALS
CLINICS & SPECIALTY CAREFACILITIES
DOCTORS
NURSESPARAMEDICS
& OTHER CARE PROVIDERS
PHARMACIES
PAYERS/HEALTH INSURANCECOMPANIES
DATA
PATIENTS
PAYER/HEALTH INSURANCE COMPANY
NURSES & OTHER CAREPROVIDERS
10/7/2016
11
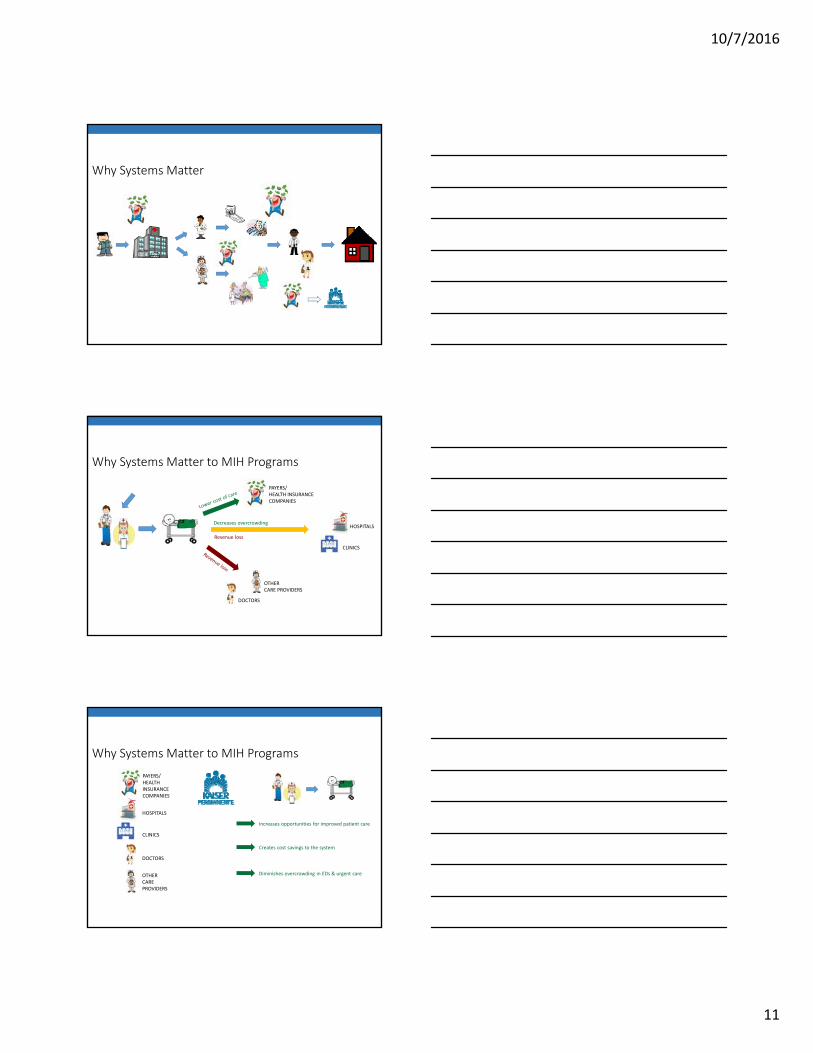
Why Systems Matter
Why Systems Matter to MIH Programs
HOSPITALS
CLINICS
DOCTORS
OTHER CARE PROVIDERS
PAYERS/HEALTH INSURANCE COMPANIES
Decreases overcrowding
Revenue loss
Why Systems Matter to MIH Programs
Creates cost savings to the system
Diminishes overcrowding in EDs & urgent care
Increases opportunities for improved patient care
HOSPITALS
CLINICS
DOCTORS
OTHER CARE PROVIDERS
PAYERS/HEALTH INSURANCE COMPANIES
10/7/2016
12
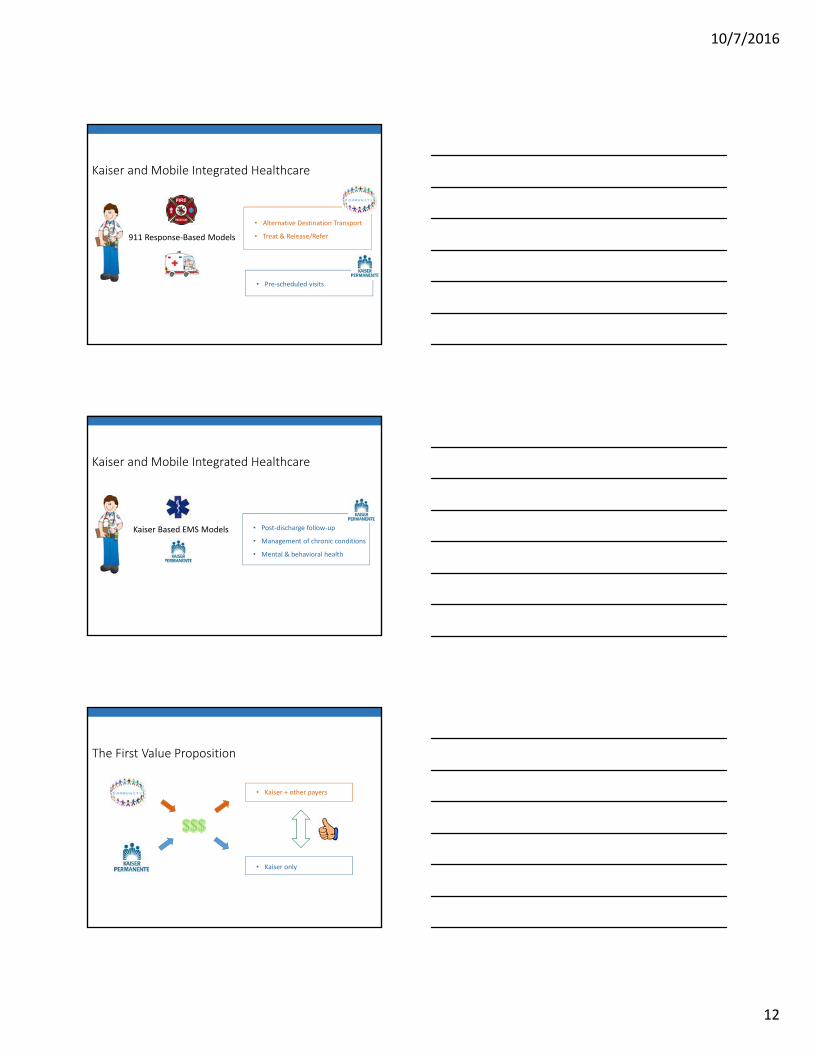
Kaiser and Mobile Integrated Healthcare
911 Response‐Based Models
• Alternative Destination Transport
• Treat & Release/Refer
• Pre‐scheduled visits
Kaiser and Mobile Integrated Healthcare
Kaiser Based EMS Models • Post‐discharge follow‐up
• Management of chronic conditions
• Mental & behavioral health
The First Value Proposition
• Kaiser + other payers
• Kaiser only
$$$
10/7/2016
13
High utilizers of 911
ED high utilizers
ED high cost utilizers
Outside medical expenses
The Second Value Proposition
Held MCAT meeting
MCAT formed ED High Utilizers Workgroup
Pulled Pan CityED data
Visualized the data
Chart review super high utilizers
KP MIH Pilot Process
2. ED High Utilizers Workgroup – Meeting 2
Reviewed data analysis
Narrowed down subgroups to target
3. Chart Review Party!!!!
1. ED High Utilizers Workgroup – Meeting 1
Identified the problem
Socialized the data analysis process – introduced Tableau
KP MIH Pilot Process
10/7/2016
14
5. Utilize video ethnography capability to talk with members in the identified subgroups about their ED utilization
KP Now
Health Leads
Phone Call Back
KP On Call
4. ED High Utilizers Workgroup – Meeting 3
Review chart review outcomes
Finalize subgroups to target
Map current KP assets and interventions available to address subgroups problems – identify gaps in the continuum for these members
6. ED High Utilizers Workgroup – Meeting 4
Review video ethnography
Empathy map members in targeted subgroups
Identify quality improvement needs in existing assets
Develop options for solutions to address gaps
KP MIH Pilot Process
7. Validate proposed solutions with members
8. Convene ED High Utilizers Workgroup – Meeting 5
Review member input
Design plan for operationalizing solutions
9. Present proposal to MCAT
10. Present proposal to SCAL leadership
11. Implement pilot program
KP MIH Pilot Process
Data as We Typically Know It
10/7/2016
15
Data as We Can Know It
ED Disposition (group) ED Disposition
HOME HOME
ADMIT TO INPATIENT, ADMIT TO OBS, ADMIT TOOR and 2 more
ADMIT TO INPATIENT
ADMIT TO OBS
ADMIT TO OR
TRANSFER TO L&D
TRANSFER FOR CARDIAC CATH (DC/Transfer toanother type of Health Care Institution not
DC TO KFH, DC TO LAW ENFORCEMENT, DC TONON KFH and 7 more
DC TO NON KFH
DC TO KFH
DC/TRANS TO BEHAVIORAL HEALTH
DC/TRANSFER TO SNF
DC TO LAW ENFORCEMENT
DC/TRANSFER TO ICF
DC/TRANSFER TO HOME W/HOSPICE CARE
DC/TRANSFER TO IP REHAB FACILITY
DC/TRANSFER TO HOME UNDER CARE OF HOMEHEALTH
DC/TRANSFER TO SHELTER
LEFT AGAINST MEDICAL ADVICE (AMA) & LEFTWITHOUT BEING SEEN (LWBS)
LEFT AGAINST MEDICAL ADVICE (AMA)
LEFT WITHOUT BEING SEEN (LWBS)
ELOPED POST MSE, MD ELOPED, RN ELOPED RN ELOPED
MD ELOPED
ELOPED POST MSE
EXPIRED EXPIRED
Pt Zip
0.00
0.01
0.02
0.03
0.04
0.05
0.06
0.07
0.08
0.09
0.10
0.11
0.12
Valley Village, N Hollywood, North Hollywood, Sherman Village, Studio City
Sun Valley, La Tuna Canyon, Shadow Hills, Rancho La Tuna Canyon
Canyon Country, Santa Clarita, Fair Oaks Ranch, Canyon Cntry
Sylmar, Kagel Canyon, Lake View Terrace, Lake View Ter
Pacoima, Arleta, Hansen Hills, Lakeview Terrace
North Hollywood, N Hollywood, Valley Glen
Studio City, N Hollywood, North Hollywood
Van Nuys, Sherman Oaks, Valley Glen
Newhall, Friendly Valley, Santa Clarita
North Hills, Northridge, Sepulveda
North Hollywood, N Hollywood
Granada Hills, San Fernando
Sherman Oaks, Van Nuys
Panorama City, Van Nuys
Van Nuys, Lake Balboa
Valencia, Santa Clarita
Van Nuys, Valley Glen
San Fernando
Frazier Park
Tujunga
AverageAverageAverage
Understanding ED High Utilizers
We started with all ED encounters that occurred at the Panorama City Medical Center from July 2014 – June 2015 (one calendar year).62,152 encounters
Kept only the ED encounters attributable to patients who live in the Panorama City Service Area.
Before 62,152 encounters After 51,348 encounters
Understanding ED High Utilizers
10/7/2016
16
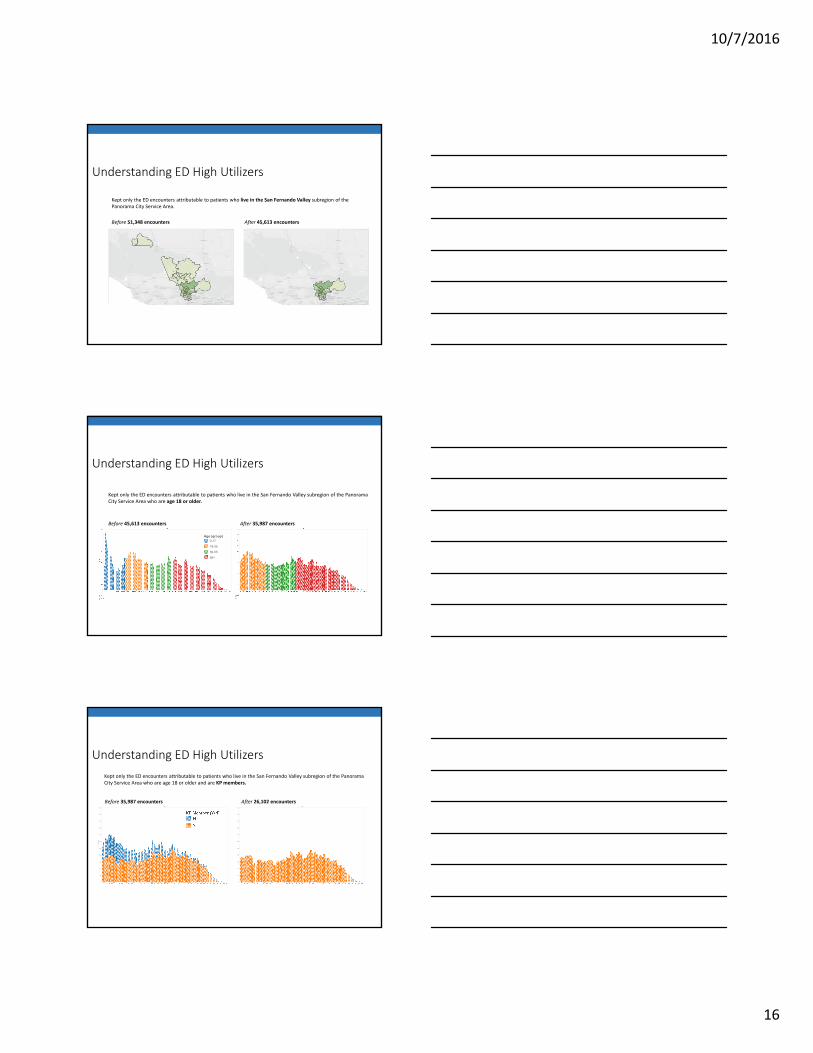
Kept only the ED encounters attributable to patients who live in the San Fernando Valley subregion of the Panorama City Service Area.
Before 51,348 encounters After 45,613 encounters
Understanding ED High Utilizers
Age (group)0-17
18-35
36-55
56+
Kept only the ED encounters attributable to patients who live in the San Fernando Valley subregion of the Panorama City Service Area who are age 18 or older.
Before 45,613 encounters After 35,987 encounters
Understanding ED High Utilizers
Age
0
100
200
300
400
500
600
700
800
900
1000
1100
Age
0
100
200
300
400
500
600
700
800
900
1000
1100
Kept only the ED encounters attributable to patients who live in the San Fernando Valley subregion of the Panorama City Service Area who are age 18 or older and are KP members.
Before 35,987 encounters After 26,102 encounters
Understanding ED High Utilizers
10/7/2016
17
Age
0
100
200
300
400
500
600
700
800
900
1000
1100
Age
0
100
200
300
400
500
600
700
800
900
1000
1100
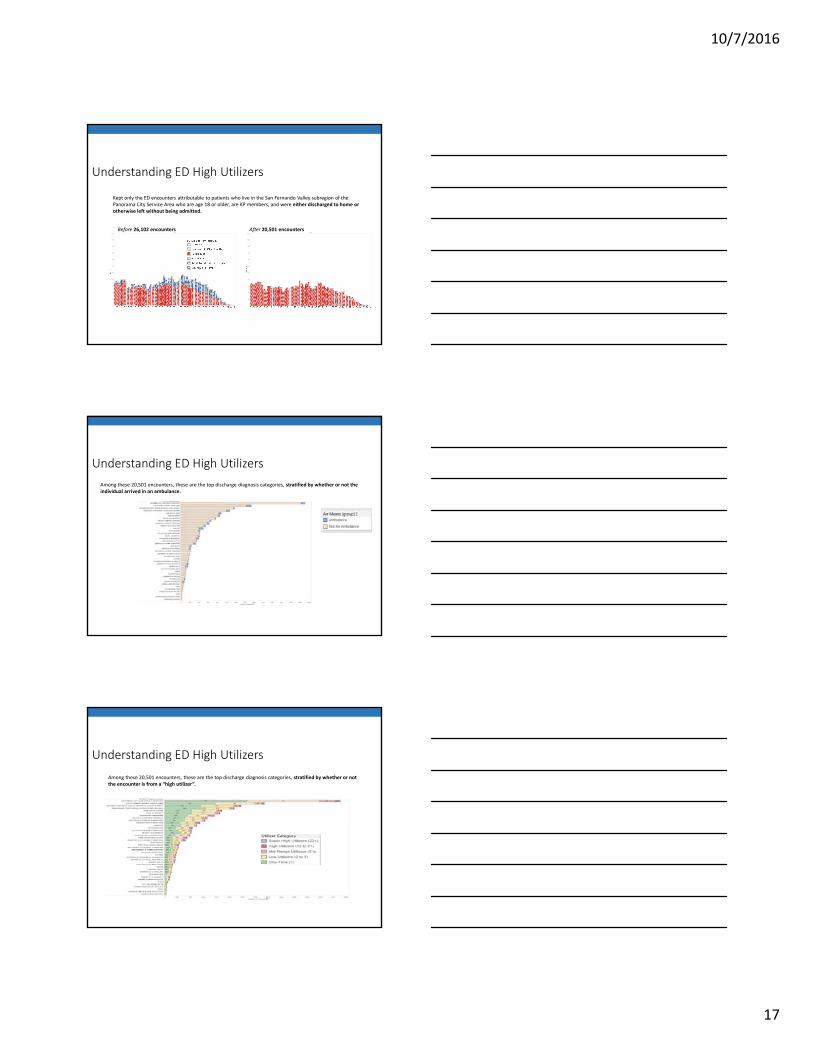
Kept only the ED encounters attributable to patients who live in the San Fernando Valley subregion of the Panorama City Service Area who are age 18 or older, are KP members, and were either discharged to home or otherwise left without being admitted.
Before 26,102 encounters After 20,501 encounters
Understanding ED High Utilizers
Among these 20,501 encounters, these are the top discharge diagnosis categories, stratified by whether or not the individual arrived in an ambulance.
Understanding ED High Utilizers
Among these 20,501 encounters, these are the top discharge diagnosis categories, stratified by whether or not the encounter is from a “high utilizer”.
Understanding ED High Utilizers
10/7/2016
18
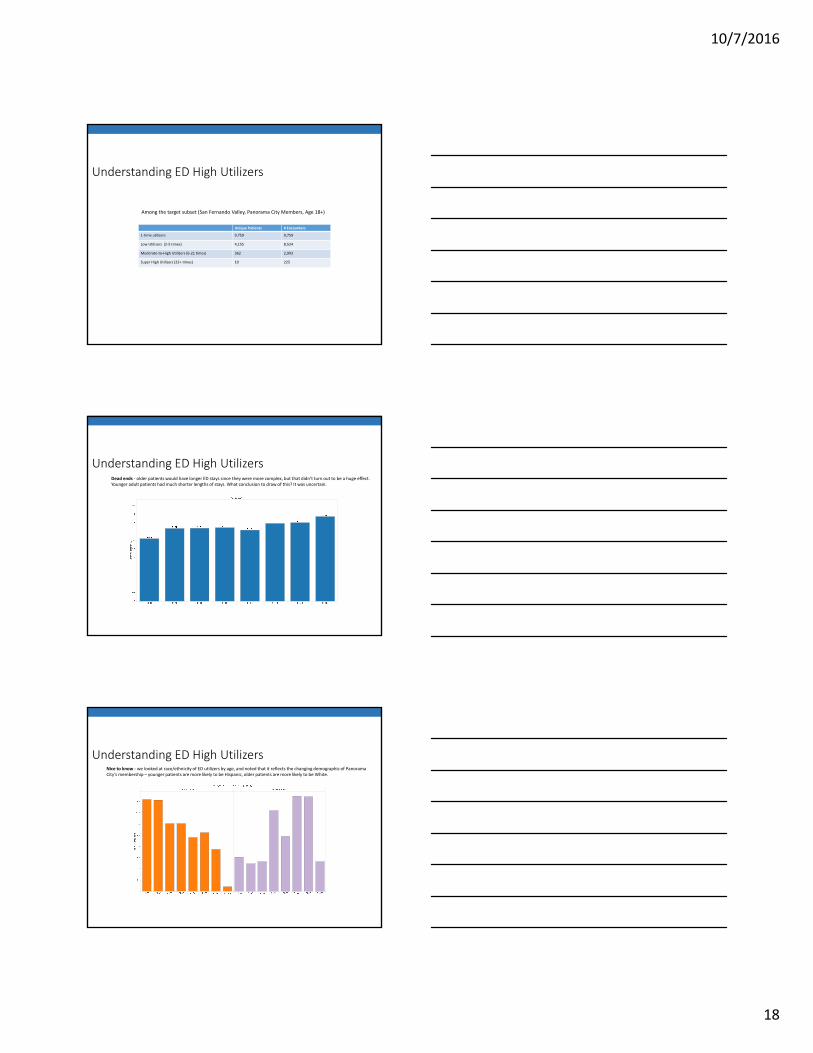
Unique Patients # Encounters
1‐time utilizers 9,759 9,759
Low Utilizers (2‐5 times) 4,155 8,524
Moderate‐to‐High Utilizers (6‐21 times) 362 2,993
Super High Utilizers (22+ times) 10 225
Among the target subset (San Fernando Valley, Panorama City Members, Age 18+)
Understanding ED High Utilizers
Dead ends ‐ older patients would have longer ED stays since they were more complex, but that didn’t turn out to be a huge effect. Younger adult patients had much shorter lengths of stays. What conclusion to draw of this? It was uncertain.
Understanding ED High Utilizers
Nice to know ‐ we looked at race/ethnicity of ED utilizers by age, and noted that it reflects the changing demographic of Panorama City’s membership – younger patients are more likely to be Hispanic, older patients are more likely to be White.
Understanding ED High Utilizers
10/7/2016
19
Cost Analysis – Predicted High Utilizers
8.9% of ED encounters were due to Predicted High Utilizers.
1 out of every 20 of this subgroup is predicted to be a member who might spend close to $60,000 per year (compared to the average member yearly cost of $5,300).
Understanding ED High Utilizers
The Second Value Proposition
Know the
problem you are trying to
solve
DATA SHARING
DATA INTEGRATION
DATA IS THE KEY
Closing Thought