Embed Size (px)
Citation preview

Thorax 1991;46:843-850
New perspectives in lung cancer Series editor: S G Spiro
1-Neuroendocrine differentiation in lung tumours
Mary N Sheppard
Great advances in knowledge of neuroendo-crine lung tumours have resulted in the past20 years from the application of newtechniques, including electron microscopy,cell culture, immunocytochemistry, radio-immunoassay, and more recently molecularbiology. These techniques have added greatlyto our understanding of these complicated andoften fatal tumours but they also raise manyfurther questions, to which we do not yet haveanswers. For pathologists this is reflected inthe multiple and at times complicated clas-sifications applied to these tumours, depend-ing on the techniques used and the tissuesstudied. For clinicians this explosion inknowledge has provided many new avenuesfor investigation and the possibility ofdeveloping new therapeutic tools. The subjectof neuroendocrine differentiation in lungtumours is only now being unravelled. Thesenew findings may soon help to unlock some ofthe secrets of lung carcinogenesis and helppatients by providing diagnostic, prognostic,and possibly therapeutic information.
Department ofLung Pathology,National Heart andLung Institute,Royal BromptonNational Heart andLung Hospital,London SW3 6NPMN SheppardReprint requests to:Dr Sheppard
Neuroendocrine cells in the lungIt was Feyrter' in 1938 who first describedclear cells in the respiratory epithelium of thehuman airway and included them in a "diffuseendocrine system" with other clear cells in thegastrointestinal tract and pancreas. Frohlich2found that these cells were argyrophilic (tak-ing up silver salts) and with foresight (but no
evidence) he considered them to be chemo-receptors capable of monitoring gas tensionsin the airways and releasing hormones.Hamperl3 saw the similarity of these cells tothe Kulschitsky or K cell of the gastrointes-tinal tract and suggested this name for them.Electron microscopy showed that the cellscontained cytoplasmic dense core granulessimilar to granules found in endocrine cellselsewhere and in neurones.' The cells were
therefore called neuroendocrine cells to
emphasise the association between the endo-crine and the nervous system. Immunocyto-chemical and sensitive radioimmunoassaytechniques confirmed the presence of severalamines and peptides within these neuroendo-crine cells, including serotonin, gastrin releas-ing peptide (GRP), the C flanking peptide ofpreproGRP, calcitonin, leu-enkephalin, cal-citonin gene related peptide (CGRP), andendothelin.56 Many of these peptides are alsofound in neurones and nerves of the centraland peripheral nervous system, again showingthe close link between the endocrine andnervous systems.
This widespread collection of peptide con-taining cells and nerves is known as the diffuseneuroendocrine system.67 All these peptideshave potent actions on airway smooth muscle,vasomotor tone, and airway secretion andhave been proposed as important modulatorsof physiological changes in the lung.8 Thepeptides may carry out their effects in a clas-sical endocrine manner via the bloodstream,via nerve transmission (neuroendocrine), or ina local ("paracrine") fashion. Not surpris-ingly, given the extensive nature of thispeptide containing system in the human res-piratory tract, lung tumours can producemany of these neuroendocrine features.
Neuroendocrine lung tumourclassificationThe secretion of what were originallyconsidered to be "ectopic" hormones bylung tumours has been known for sometime.9 Adrenocortical overactivity leading toCushing's syndrome was described in a patientwith lung carcinoma in 1928. Sensitive assayand cell culture techniques have permitted thedetection of peptide hormone secretion bytumours, particularly lung tumours,'°01 in theabsence of clinically overt syndromes. Overtendocrinological disturbance and biologicallyactive peptide hormone production is commonin small cell carcinomas and carcinoid tumours;but almost all lung cancers, irrespective ofhistological type, are capable of producingsmall amounts of peptide.'2Both carcinoid tumours and small cell car-
cinomas can be recognised by light microscopy.Dense core neurosecretory granules in smallcell carcinomas and carcinoid tumours addedan ultrastructural feature to establish neuro-endocrine differentiation4 13 and showed theclose association between these tumours andnormal pulmonary endocrine cells, which alsocontain dense core granules. Thus both carcin-oid tumours and small cell carcinomas areconsidered neuroendocrine tumours of thelung and included in the World Health Organ-isation histological classification of lungtumours.'4 Carcinoid tumours are consideredto form the benign end of the spectrum andsmall cell carcinomas the highly malignant end.A distinct subgroup of carcinoid tumours,labelled atypical carcinoids, with histologicaland clinical evidence of malignancy and with ahigh rate of metastases,'5 were described in1972. These lung neuroendocrine tumoursform a link between carcinoid tumours andsmall cell carcinomas. To reflect the overlapbetween these tumours it was suggested that
843
on July 4, 2020 by guest. Protected by copyright.
http://thorax.bmj.com
/T
horax: first published as 10.1136/thx.46.11.843 on 1 Novem
ber 1991. Dow
nloaded from

Sheppard
Classifications of neuroendocrine carcinomas of the lung
WHOclassification'4 Paladugu" Gould"6 Travis61Carcinoid KCC* 1 Carcinoid CarcinoidAtypical
carcinoid KCC 2 Well differentiated Atypical carcinoidneuroendocrine carcinomaNeuroendocrine carcinoma Neuroendocrine
carcinomaintermediate cell carcinoma large cell carcinoma
Small cellcarcinoma KCC 3 Neuroendocrine carcinoma Small cell carcinoma
Small cell carcinoma
*Kulschitsky cell carcinoma.
they should be reclassified as Kulschitsky cellcarcinomas to indicate their spectrum ofaggressiveness and emphasise their origin fromthe pulmonary endocrine or Kulschitsky cell"6(table).Immunocytochemical techniques using
antibodies to general neuroendocrine markers,including neurone specific enolase,'7 PGP 9-5,synaptophysin, and chromogranin,1819 were
applied to neuroendocrine lung tumours byourselves and others. Sensitive radioimmu-noassay techniques were also used to detectthese markers in serum and monitor tumourprogression and recurrence.202'
These new techniques clarified the neuro-endocrine nature of the tumours, suspectedfrom light microscopy, and produced some
unexpected findings, which at first were difficultto explain. The presence of dense core gran-ules, peptide or amine hormone production,and neuroendocrine immunocytochemicalmarkers in undifferentiated large cell carcin-omas, squamous cell carcinomas and adenocar-cinomas gave rise to the concept of atypicalendocrine tumours,2223 non-small cell carcin-omas with neuroendocrine features,24 and largecell neuroendocrine tumours of the lung.25These categories have caused much confusionamong pathologists and clinicians concerningtheir behaviour, prognosis, and response totreatment.The important question is whether these
tumours with neuroendocrine features behaveaggressively like small cell carcinomas andwhether they therefore respond to chemo-therapy. Alternatively, is neuroendocrine dif-ferentiation ofno significance, merely reflectingthe general heterogeneity of lung tumours?Another possibility is that neuroendocrine dif-ferentiation may indicate a more benignbehaviour as typical carcinoid tumours, whichdisplay many neuroendocrine features, are
usually indolent.In an attempt to answer these questions
Gould26 suggested a spectrum comprisingseveral related but distinct types of neuro-
endocrine neoplasms in the lung (table). Heretained the typical carcinoid tumour groupbut labelled atypical carcinoids as well differen-tiated neuroendocrine carcinomas to empha-sise their malignant behaviour. Small cellcarcinomas are categorised as neuroendocrinecarcinoma of small cell type. In addition, heintroduced a new category, which he called
neuroendocrine carcinoma of intermediate celltype, and included many large cell undifferen-tiated carcinomas and tumours with squamousand glandular differentiation in this group(table). His clinical follow up of patients withthese tumours shows a spectrum of behaviour,the intermediate cell type behaving in a fashionsimilar to that of the small cell type and beingmore aggressive than other large cell carcin-omas.27 He considers that neuroendocrine dif-ferentiation in non-small cell carcinomasindicates aggressive behaviour and suggeststhat chemotherapy should be assessed for suchtumours.This classification is useful in delineating a
spectrum of endocrine lung tumours withpredictable behaviour but falls short on severalpoints. Firstly, the description of the neuro-endocrine carcinoma of intermediate cell typeis too vague and non-specific to allow this to beseparated from other undifferentiated tumoursby light microscopy in my experience. Sec-ondly, it is unfortunate that this category wasnamed intermediate cell type as it is oftenconfused with the "intermediate" small cellcarcinoma subgroup of the WHO classifica-tion. 4 Thirdly, the classification presupposes ahistogenetic relationship that has not yet beenestablished. There is now sufficient evidence toregard carcinoid tumours as separate fromsmall cell carcinomas and other lung tumours.Carcinoid tumours occur in a younger popula-tion and are not related to smoking habits orother risk factors for the more common formsof lung cancer. Furthermore, small cell carcin-omas are rarely seen in association with carcin-oid tumours. The initial response of a small cellcarcinoma to combination chemotherapy andthe poor long term prognosis contrast with thechemoresistance and good prognosis of mostcarcinoid tumours. These observations callinto question the value of attempts to devise aterminology for a spectrum of neuroendocrinetumours and the classification of these tumoursremains in a state of flux.
Difficulties in the diagnosis ofneuroendocrine lung tumoursThe more recent classifications of neuroendo-crine lung tumours are difficult for pathologiststo apply, particularly for the non-small celltypes. Classification requires basic light micro-scopy plus electron microscopy and the use ofimmunocytochemical markers, which are ex-pensive and time consuming. A patient with anunusual lung tumour suspected of being aneuroendocrine tumour should probably bereferred to a specialist centre for appropriateinvestigations; formal follow up is essential toestablish their behaviour and prognosis.A second problem is that lung tumours show
heterogeneity with both light microscopy andelectron microscopy, which can lead toproblems in interpreting neuroendocrinefeatures. Up to 7% of lung tumours have amixed morphology according to light micro-scopic appearances. Multiple sampling of atumour by electron microscopy may revealglandular, squamous, and neuroendocrine
-844
on July 4, 2020 by guest. Protected by copyright.
http://thorax.bmj.com
/T
horax: first published as 10.1136/thx.46.11.843 on 1 Novem
ber 1991. Dow
nloaded from

Neuroendocrine differentiation in lung tumours
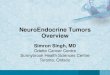
Figure 1 Typicalcarcinoid tumour of lungwith islands and ribbons(trabeculae) of cellsshowing uniformity ofnuclei and cytoplasm.There is hyperchromatismof the nuclei at theperiphery of the islands.
Figure 2 Dense granulesin the cytoplasm of acarcinoid tumour cell.(Electron micrography byA Dewar, National Heartand Lung Institute.)
areas even within the same cell; the significanceof large or small areas of neuroendocrine dif-ferentiation in a mixed tumour remains to beassessed. For definitive diagnosis large quan-tities of tissue may be required for specialinvestigations. This may be a problem withbronchial biopsy, the only diagnostic techniqueused for many lung tumours as the patients areinoperable. Most neuroendocrine classifica-tions rely heavily on the architecture ofthe cellswithin the tumour and this may not be seeneasily in small biopsy specimens. Crush arte-fact, cellular distortion, and degeneration maymake it difficult at times to separate carcinoidtumours from small cell carcinomas, a fact ofgreat importance for treatment and prognosis.
At electron microscopy the definition of adense core neurosecretory granule, the hall-mark of neuroendocrine differentiation, is notclear and several studies show a wide diver-gence in the size, shape, and distribution ofthese granules. Differentiating them from smalllysosomes may be difficult.
Finally, the specificity of the general neuro-endocrine markers has been questioned asthese markers have been found in non-neuro-endocrine tumours, such as breast or kidneytumours. The use of only one marker forimmunocytochemical diagnosis of neuro-endocrine differentiation is open to criticismand a panel of markers is now recommended(see below).
845
on July 4, 2020 by guest. Protected by copyright.
http://thorax.bmj.com
/T
horax: first published as 10.1136/thx.46.11.843 on 1 Novem
ber 1991. Dow
nloaded from

Sheppard
Carcinoid tumours of the lungAbout 12% of all carcinoids arise in the lungbut less than 1% of lung tumours are carcin-oid.' Hamperl29 was the first to separate carcin-oids from other bronchial adenomas and pointout their similarity to gastrointestinal carcin-oids. The highest incidence occurs in the 31-40year age group, with a female preponderance(62%). The tumour usually arises in a mainbronchus (85%) but may be peripheral(15%).3 Multicentric growths scatteredthroughout the lung have been described3" andcarcinoids can be associated with endocrinetumours elsewhere as part of a pluriglandularsyndrome.32
Carcinoid tumours contain uniform cellswith small round to oval nuclei, few nucleoli,and granular eosinophilic cytoplasm. The cellsare most commonly in islands interweavingwith one another in a mosaic pattern (fig 1), asinterconnecting ribbons of cells in a trabecularpattern, or in an adenopapillary pattern; mixedforms are also seen.33 In a typical carcinoidnuclear pleomorphism and mitoses are rare.At the ultrastructural level the main feature
of all carcinoids is the large numbers of densecore neurosecretory granules in the cytoplasmof virtually all tumour cells4 (fig 2). Mostcarcinoid tumours are strongly immunoreac-
Figure 3 Positive immunostaining for chromogranin A in the cell cytoplasm of a
carcinoid tumour.
tive for general neuroendocrine markers"7 1834(fig 3), and immunocytochemical methods andradioimmunoassay show that bronchial carcin-oids produce a wide range of amines andpeptide hormones.1226 Gould found that 5-hydroxytryptamine was the most frequentlyoccurring immunoreactive substance in pul-monary carcinoids, followed in descendingorder offrequency by gastrin releasing peptide,vasoactive intestinal polypeptide, leu-enke-phalin, somatostatin, calcitonin, and adreno-corticotrophic hormone. A single tumour mayproduce several peptides as well as 5-hydroxy-typtamine. The latter has been put forward asan immunocytochemical marker of carcinoidsbut is found in only half of foregut carcinoids,which limits its diagnostic usefulness.35 S-100positive sustentacular cells have been reportedin pulmonary carcinoids36 and labelled as"paragangloid" carcinoids. The feature thatdistinguishes these from the rare primary pul-monary paraganglioma is that paragangliomasrarely express keratin and are strongly im-munoreactive for neurofilaments.37
Carcinoid tumours are generally easy todiagnose by light microscopy and do not re-quire further investigations. They have anexcellent prognosis generally. Five per cent oftypical cases with no features of malignancymetastasise" so the behaviour of individualtumours cannot be predicted. Deeply invasivetumours,38 tumours greater than 3 0 cm indiameter, and lymph node metastases predis-pose to recurrence.39
Atypical carcinoid tumoursArrigoni'5 first identified a group of tumourswith a carcinoid architecture but with evidenceof malignancy, characterised by nuclear pleo-morphism, mitoses, and necrosis. The tumourswere larger and more likely to be peripheral,and their behaviour was more aggressive thanthat of typical carcinoids, with regional ordistant metastases in 70% of patients and amortality of 30%.
In two studies that examined stage 1 resect-able tumours diagnosed initially as small cell orlarge cell undifferentiated carcinomas 25%4and 80%41 turned out to be atypical carcinoidsor well differentiated neuroendocrine carcin-omas. These tumours were associated with avery much better survival rate at two years (60-75%) than small cell carcinomas even whenthese were resectable (9%).' The improvedsurvival described for stage 1 resectable smallcell carcinoma" 13 and the subsequent resur-gence of interest in resecting small cell carcin-omas must be looked at closely in view of thesefindings. Strict criteria must be used in labellingany peripheral lung lesion as a small cellcarcinoma.Dense core neurosecretory granules are far
less numerous than in true carcinoids and theytend to be smaller (80-140 nm). Intertwinedcytoplasmic processes are prominent and thegranules are usually concentrated there. In atypical carcinoid more than half of the cellscontain granules with at least five per cellwhereas atypical carcinoids possessed granules
846
-.
'Al
kti.rr Ap
on July 4, 2020 by guest. Protected by copyright.
http://thorax.bmj.com
/T
horax: first published as 10.1136/thx.46.11.843 on 1 Novem
ber 1991. Dow
nloaded from

Neuroendocrine differentiation in lung tumours
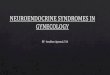
Figure 4 Small cell carcinoma of the lung showing the small hyperchromatic nuclei,nuclear moulding, little cytoplasm, and high cell death rate.
Figure 5 Small cellcarcinoma of the lunggiving a focal intensesignalfor chromogranin Amessenger RNA. (FromHamid et al'8; reproducedby courtesy of the Journalof Pathology.)
7)
in half of the cells or less with less than five per
cell."These tumours are immunoreactive for
many of the neuroendocrine, peptide hormone
and epithelial antigens already described for
carcinoids." "'4 No immunocytochemical
marker, however, distinguishing this tumour
from typical carcinoid or small cell carcinoma
has so far been discovered.
Small cell carcinoma
The WHO classification'4 divides small cell
carcinomas into three main types: (1) small or
oat cell carcinoma, consisting of small round to
elongated nuclei with finely granular chroma-
tin, no nucleoli, and little cytoplasm (fig 4);
(2) intermediate or polygonal cell carcinoma,composed of slightly larger cells with more
abundant cytoplasm and with nuclear charac-
teristics similar to those of oat cell carcinoma;(3) small cell combined with squamous cellcarcinoma or adenocarcinoma (only about %
of tumours fall into this category).These tumours often produce hormonal syn-
dromes and contain dense core neurosecretorygranules at the ultrastructral level" confirming
their neuroendocrine nature. The granules areusually scanty and small (80-140 nm) andmultiple sampling of a tumour is necessary todetect them. The use of electron microscopyhas introduced new problems in the diagnosisof small cell carcinoma. Several authors reportthe absence of dense core granules in whatappears at light microscopy to be classic smallcell carcinoma. The presence of tonofilamentsand desmosomes led Churg et al44 to label themsmall cell squamous tumours whereas Nomoriet al45 labelled them undifferentiated carcin-oma, small cell type. Patients with thesetumours have been reported to survive longerthan those with tumours with classical gran-ules, but numbers of cases are small.'There has also been controversy about the
prognostic significance of the subdivisions ofsmall cell carcinomas. Some studies have led toclaims that the small cell type has a betterprognosis and is more responsive to chemo-therapy,4748 whereas others suggest that theintermediate cell type does best.49 Two furtherstudies suggest no difference.5' This contro-versy, as well as the difficulty of separating thesmall cell from the intermediate cell typehistologically, has led many pathologists andclinicians to abandon this subclassification.The mixed small cell/large cell carcinoma
was first proposed as a separate entity in 1982.These mixed tumours, originally thought to berare, are being recognised more frequentlyespecially in biopsy and necropsy specimensfrom patients treated intensively with radiationor chemotherapy. They represent 5-12% of'allsmall cell carcinomas and have shown a poorresponse to chemotherapy with a shortersurvival.52"5The International Association for the Study
of Lung Cancer (IASLC) has recommendedthat small cell carcinoma should be divided intothree groups: (1) small cell carcinoma, combin-ing the classic small cell and intermediate celltypes (90% of untreated small cell carcinomasare of this type); (2) small cell/large cell carcin-oma, in which at least 24% of the cells havelarge granular or more open nuclei withprominent eosinophilic nucleoli (4-6% ofuntreated small cell carcinomas fall into thiscategory); (3) carcinoma of mixed type similarto WHO group 3.This classification is supported by experi-
mental studies on small cell carcinoma. Manycontinuous cell lines and xenographs have beenestablished.5 Most contain dense core gran-ules, express neuroendocrine and other mark-ers associated with small cell carcinoma, andare radiosensitive. The cytological features ofthese "classic" cell lines are of the small cellsubtype of small cell lung carcinoma. Somesmall cell lines have a "variant" morphologicalappearance and resemble small/large cell car-cinomas or large cell carcinomas. They lackdense core granules and other neuroendocrinefeatures. They are somtimes associated withamplification of the c-myc oncogene and theygrow more rapidly, are cloned more efficiently,and are radioresistant. These variant cell linesmay develop from classic small cell carcinomas,especially if these have been treated with
847
on July 4, 2020 by guest. Protected by copyright.
http://thorax.bmj.com
/T
horax: first published as 10.1136/thx.46.11.843 on 1 Novem
ber 1991. Dow
nloaded from

Sheppard
chemotherapy, or from mixed small cell/largecell carcinomas. The development of large cellfeatures in a small cell carcinoma after chemo-therapy may be due to the treatment or to thesurvival of large cells already present in thetumour before treatment. There is wide sup-
port for the above classification, though some
studies suggest no difference in prognosis.5'Small cell carcinomas are immunoreactive
for general neuronal markers.' 1 34 Serum con-
centration of neuroendocrine markers, such as
neurone specific enolase, have been used as
tumour markers for small cell carcinoma andmay be used to monitor treatment and predictrelapse.202' Unfortunately from the diagnosticand prognostic point of view, in general themore malignant the neuroendocrine tumour isthe less likely it appears to be to give positiveimmunocytochemical results for neuroendo-crine antigens or peptide hormones.26A surprising immunocytochemical finding is
that gastrin releasing peptide, an establishedgrowth factor, is rarely expressed in small cellcarcinomas. This may be due to the productionofabnormal forms ofthe precursor preporGRPmolecle, and the C terminal peptide in par-
ticular. Antibodies to C terminal peptide showstrong immunostaining in 12% of typical car-
cinoids, in 56% of atypical carcinoids, and in70% of small cell carcinomas,'8 and theseappear to be associated with a shorter survivalthan those without the immunoreactive pep-
tide. The more malignant a tumour is the morelikely it is to produce an abnormal peptideprecursor. The mechanism underlying any ofthe paraneoplastic syndromes, such as neuro-
pathies, encephalomyelitis, and myopathies, isunknown, though production of antigens bythe tumour similar to neuronal antigens and thesubsequent induction ofantibodies by the bodyin response to the antigens are thought toexplain many ofthe syndromes.55 This suggeststhat many more tumour products remain to bediscovered.Immunocytochemistry and radioimmuno-
assay provide useful data on stored andsecreted peptide; information on gene expres-
sion and regulation requires molecular biologytechniques, including Northern and Southernblotting, in situ hybridisation, and the poly-merase chain reaction. When these techniquesare applied the gene for gastrin releasing pep-
tide has been found in all carcinoids and smallcell carcinomas56 and in most large cell carcin-omas.57 We have localised the neuroendocrineantigen chromogranin A gene in small cellcarcinomas58 (fig 5).These techniques have also helped to detect
oncogenes and anti-oncogenes and abnormali-ties in their expression in neuroendocrinetumours. The major oncogenes implicated inneuroendocrine tumours are the myc and ras
families. Myc amplification appears to be asso-
ciated with tumour progression rather thanpathogenesis. C-jun is also amplified in smallcell lung cancer.59
Restriction fragment length polymorphism(RFLP) analysis indicates that deletions ofchromosome arms 3p, 13q, and 17p are fre-quent in small cell lung cancer. Chromosome
13q is the site of the retinoblastoma gene and17p of the p53 gene, and 3p is the site of an asyet unidentified anti-oncogene.60
Non-small cell neuroendocrinecarcinomasThe first description of non-small cell neuro-endocrine carcinomas, which by light micro-scopy had been diagnosed as large cell orsquamous cell carcinomas or adenocarcinomas,came in 1981, when McDowell et al22 describedseven cases in the periphery of the lung.Electron microscopy subsequently showeddense core neurosecretory granules, thusestablishing them as neuroendocrine tumours(in 4% of 150 lung tumours). The tumourswere argyrophilic and contained 5-hydroxy-tryptamine, confirming endocrine differentia-tion at the level of light microscopy. McDowelllabelled them atypical endocrine tumours ofthe lung. Another report23 suggested that asmany as 9% ofnon-small cell carcinomas in thelung contained neurosecretory granules, andthat median survival and rates of response totreatment were in the ranges seen with non-small cell carcinoma. Others,2425 however,claimed that they behaved more aggressively,like small cell carcinoma, and labelled themlarge cell neuroendocrine tumours or non-small cell carcinomas with neuroendocrinefeatures. Gould26 included them as inter-mediate cell type in his spectrum of neuro-endocrine carcinomas and suggested that cellnesting with peripheral palisading of nucleiwould help to identify this tumour by lightmicroscopy, a point emphasised by Mooi etal.24 Travis et al"6 emphasised that the cells arelarge with prominent nucleoli in the nuclei, ahigh mitotic rate, and a low nuclear:cytoplas-mic ratio and have an organoid, trabecular, andpalisading pattern. In a later study and followup by Gould's group the tumours behaved in afashion similar to that of small cell carcinoma.27The clinical relevance of a separate group ofnon-small cell neuroendocrine carcinomasremains to be determined; most studies aresmall and lack follow up.61
Specificity of neuroendocrine markersSeveral workers applying neuroendocrinemarkers to lung tumours have found that aproportion of all tumour types give positiveresults.3462 This may reflect the heterogeneity oflung tumours; others consider that the markerslack specificity for neuroendocrine tumours.6'We found that, although neurone specificenolase and PGP9.5 are positive in mostneuroendocrine tumours,34 they are alsopresent in 10-60% of non-neuroendocrinelung tumours and are not now considered asreliable markers of neuroendocrine differen-tion. Chromogranin, Leu-7, and synapto-physin appear to be more useful markers butthey stain fewer neuroendocrine tumours thanneurone specific enolase and PGP9.5.4 6' Use ofa panel ofmarkers rather than a single marker isadvised, with a combination ofneurone specificenolase, PGP9.5, chromogranin, and synapto-
848
on July 4, 2020 by guest. Protected by copyright.
http://thorax.bmj.com
/T
horax: first published as 10.1136/thx.46.11.843 on 1 Novem
ber 1991. Dow
nloaded from

Neuroendocrine differentiation in lung tumours
physin. A positive result with two of the fourmarkers is recommended before a tumour canbe labelled as neuroendocrine.
ConclusionNeuroendocrine lung tumours are proving afruitful area of research for understanding thebasic mechanisms of carcinogenesis. Rapidadvances in the molecular and cell biology ofthese tumours should help to determine theirspectrum of behaviour. New studies are essen-tial, using light microscopy, electron micro-scopy, immunocytochemistry, and molecularbiology techniques, for clarifying different sub-types and designing future treatments, par-ticularly now that many growth factors areknown to be produced by these tumours. Aclassification based on morphological and func-tional criteria may prove to be of therapeuticimportance in the future.
1 Feyrter F. Ueberdiffuse endokrineepitheliale Organe. Leipzig:Bath, 1938.
2 Frohlich F. Die "Helle Zelle" der Bronchialschleim hautaud ihre Beziehungen zum problem der Chemorecep-toren. Frankfurt Z Pathol 1949;60:517-59.
3 Hamperl H. Uber argyrophile Zellen. Arch Pathol AnatPhysiol 1952;321:482-507.
4 Bensch KG, Gordon GB, Miller LR. Electron microscopicand biochemical studies on the bronchial carcinoidtumour. Cancer 1965;18:592-602.
5 Giaid A, Hamid QA, Springall DR, Yanagisawa-M, Shinmi0, Sawamura T, et al. Detection of endothelin immuno-reactivity and mRNA in pulmonary tumours. J Pathol1990;162:15-22.
6 Springall DR, Polak JM. Localization of peptides in thelung. In: Piper PJ, ed. Advances in the understanding andtreatment of asthma. New York: Academy of Sciences,1991:1-20.
7 Polak JM, Bloom SR. Occurrence and distribution ofregulatory peptides in the respiratory tract. In: HavemannK, Sorenson G, Gropp C, eds. Recent results in cancerresearch. Berlin: Springer, 1985:1-16.
8 Becker KL. Lung Cancer. Peptide hormones and theirpossible functions in the normal and abnormal lung. In:Havemann K, Sorenson G, Gropp C, eds. Recent results incancer research. Berlin: Springer, 1985:17-28.
9 Brown WH. A case of pluriglandular syndrom. Lancet1928;ii:1022-3.
10 Ratcliffe JG, Podmore J. Ectopic hormones. In: Boelsma E,Rumke Ph, eds. Tumour markers: impact and prospects.Amsterdam: Elsevier/North Holland Biomedical Press,1979:3-23.
11 Baylin SB, Mendelsohn G. Ectopic (inappropriate) hormoneproduction by tumours: mechanisms involved and thebiological and clinical implications. Endocr Rev 1980;1(No 1):45-77.
12 Kameya T, Kodama T, Shimosato Y. Morphology of lungcancer in relation to its function. In: Shimosato Y,Melamed MR, Nettesheim P, eds. Morphogenesis of lungcancer. Vol 2. Florida: CRC Press, 1982:107-29.
13 Bensch KG, Corrin B, Pariente R, Spencer H. Oat cellcarcinoma of the lung: its origin and relationship tobronchial carcinoid. Cancer 1968;22:1163-72.
14 World Health Organisation. Histological typing of lungtumours. 2nd ed. Geneva: WHO, 1981.
15 Arrigoni MG, Wooner LB, Bematz PE. Atypical carcinoidtumours of the lung. Journal of Thoracic and CardiovascSurg 1972;64:413-21.
16 Paladugu RR, Benfield JR, Pak HY, Ross RK, Teplitz RL.Bronchopulmonary Kulchitzky cell carcinomas. A newclassification scheme for typical and atypical carcinoids.Cancer 1985;55:1303-1 1.
17 Sheppard MN, Corrin B, Bennett MH, Marangos PJ,Bloom SR, Polak JM. Immunocytochemical localisationof neuron-specific enolase in small cell carcinoma andcarcinoid tumours of the lung. Histopathology 1984;8:171-81.
18 Addis BJ, Hamid Q, Ibrahim NBN, Fahey M, Bloom SR,Polak JM. Immunohistochemical markers of small cellcarcinoma and related neuroendocrine tumours of thelung. JPathol 1987;153:137-50.
19 Wiedenmann B, Huttner WB. Synaptophysin and chromo-granins/secretogranins-widepsread constituents of dis-tinct types of neuroendocrine vesicles and new tools intumor diagnosis. Virchows Arch B Cell Pathol 1989;58:95-121.
20 Carney DN, Idhe DC, Cohen MH, Marangos PJ, Bunn PA,Minna JD. Serum neuron-specific enolase a marker fordisease extent and response to therapy of small-cell lungcancer. Lancet 1982;ii:583-5.
21 Burghuber OC, Worofka B, Schernthaner G, et al. Serumneuron-specific enolase is a useful tumour marker for smallcell lung cancer. Cancer 1990;65:1386-90.
22 McDowell EM, Wilson TS, Trump BS. Atypical endocrinetumours ofthe lung. Arch Pathol LabMed 1981;105:20-8.
23 Neal MH, Kosinski R, Cohen P, Ohrenstein JM. Atypicalendocrine tumours of the lung. A clinicopathologic studyof 19 cases. Hum Pathol 1986;17:1264-77.
24 Mooi WJ, Dewar A, Springall DR, Polak JM, Addis BJ.Non-small cell lung carcinomas with neuroendocrinefeatures. A light microscopic, immunohistochemical andultrastructural study of 11 cases. Histopathology 1988;13:329-37.
25 Hammond ME, Sause WT. Large cell neuroendocrinetumors of the lung. Cancer 1985;56:1624-9.
26 Gould VE, Linnoila I, Memoli VA, Warren WH. Neuro-endocrine cells and neuroendocrine neoplasms ofthe lung.In: Sommers SC, Rosen PP, eds. Pathology annual.Appleton, Connecticut: Century-Crofts, 1983:287-330.
27 Warren WH, Penfield Faber L, Gould VE. Neuroendocrineneoplasms of the lung. A clinicopathologic update. JThorac Cardiovasc Surg 1989;98:321-32.
28 Godwin JD. Carcinoid tumours. Cancer 1975;36:560-9.29 Hamperl H. Uber Gutartige. Bronchial Tumoren (cylin-
drome und carcinoide). Virchows Arch A Pathol AnatHistol 1937;300:46-8.
30 Oike N, Bernatz PE, Woolner LB. Carcinoid tumors of thelung. Ann Thorac Surg 1976;22:270-7.
31 Skinner C, Ewen SWB. Carcinoid lung: diffuse pulmonaryinfiltration by a multifocal bronchial carcinoid. Thorax1976;31:212-9.
32 Williams ED, Celestin LR. The assocation of bronchialcarcinoid and pluriglandular adenomatosis. Thorax 1962;17:120-7.
33 Jones RA, Dawson IMP. Morphology and staining patternsof endocrine tumours in the gut, pancreas and bronchusand their possible significance. Histopathology 1977;1:137-50.
34 Sheppard MN, Morittu L, Moss F, et al. A study ofepithelial, neuroendocrine and natural killer cell anti-bodies in adult lung and lung tumours. Lung Cancer1988;4:70-2.
35 Shaw PAV. Comparison of immunologic detection of5-hydroxytryptamine by monoclonal antibodies withstandard silver stains as an aid to diagnosing carcinoidtumours. J Clin Pathol 1988;41:265-72.
36 Barbareschi M, Frigo B, Mosca L, Carboni N, Arrigoni GP,Leonardi E, et al. Bronchial carcinoids with S-100 positivesustentacular cells. A comparative study with gastro-intestinal carcinoids, pheochromocytomas and paragan-gliomas. Pathol Respir Pract 1990;186:212-22.
37 Hoefier H, Denk H, Lackinger E, Helleis G, PolakJM, HeitzPU. Immunocytochemical demonstration of intermediatefilament cytoskeletal proteins in human endocrine tissuesand (neuro-) endocrine tumours. Virchows Arch A PatholAnat 1986;409:609-26.
38 Hajdu SI, Winawer SJ, Myers WPL. Carcinoid tumours: astudy of 204 cases. Am J Clin Pathol 1974;61:521-8.
39 McCaughan BC, Martini N, Bains MS. Bronchial carci-noids. Review of 124 cases. J Thorac Cardiovasc Surg1985;89:8-17.
40 Warren WH, Memoli VA, Jordan AG, Gould VE. Re-evaluation of pulmonary neoplasms resected as small cellcarcinomas. Significance of distinguishing between well-differentiated and small cell neuroendocrine carcinomas.Cancer 1990;65:1003-10.
41 Kron IL, Harman PK, Mills SE, et al. A reappraisal oflimited stage undifferentiated carcinoma of the lung. JThorac Cardiovasc Surg 1982;84:734-7.
42 Karrer K, Shields TW, Denck H, Hrabar B, Vogt-MoykopfI, Salzer GM. The importance of surgical and mul-timodality treatment for small cell bronchial carcinoma. JThorac Cardiovasc Surg 1989;97:168-76.
43 Prasad US, Naylor AR, Walker WS, Lamb D, CameronEWJ, Walbaum PR. Long term survival after pulomonaryresection for small cell carcinoma of the lung. Thorax1989;44:784-7.
44 Churg A, Johnston WH, Stulbarg M. Small cell squamousand mixed small cell squamous-small cell anaplasticcarcinomas of the lung. Am J Surg Pathol 1980;4:255-63.
45 Nomori H, Shimosato Y, Kodama T, Morinaga S, NakajimaT, Watanabe S. Subtypes of small cell carcinomas of thelung: morphometric ultrastructural and immunohisto-chemical analysis. Hum Pathol 1986;17:604-13.
46 Wei-Li MD, Hammar SP, Jolly PC, Hill LD, Anderson RP.Unpredictable course of small cell undifferentiated lungcarcinoma. J Thorac Cardiovasc Surg 1981;81:34-43.
47 Nixon DW, Murphy GF, Sewell CW, Kutner M, Lynn MJ.Relationship between survival and histologic type in smallcell anaplastic carcinoma of the lung. Cancer 1979;44:1045-9.
48 Davis S, Stanley KE, Yesner R, Kuang DT, Morris JF.Small-cell carcinoma of the lung-survival according tohistologic sub-type. Cancer 1981;47:1863-6.
849
on July 4, 2020 by guest. Protected by copyright.
http://thorax.bmj.com
/T
horax: first published as 10.1136/thx.46.11.843 on 1 Novem
ber 1991. Dow
nloaded from

Sheppard
49 Katlic M, Carter D. Prognostic implications of histology,size and location of primary tumours. In: Muggia F,Rozencweig M, eds. Lung cancer: progress in therapeuticresearch. New York: Raven Press, 1979:143-50.
50 Carney DN, Gazdar AF, Bepler G, et al. Establishment andidentification of small cell lung cancer cell lines havingclassic and variant features. Cancer Res 1985;45:2913-23.
51 Bepler G, Neumann K, Holle R, Havemann K, KalbfleischH. Clinical relevance of histologic subtyping in small celllung cancer. Cancer 1989;64:74-9.
52 RadicPA, Matthews MJ, IhdeDC, GazdarAF, CarneyDN,Bunn PA, et al. The clinical behavior of "mixed" small
cell/large cell bronchogenic carcinoma compared to"pure" small cell subtypes. Cancer 1982;50:2894-902.
53 Hirsch FR, Osterlind K, Hansen HH. The prognosticsignificance of histopathologic subtyping of small cellcarcinoma of the lung according to the World HealthOrganization classification. Cancer 1983;52:2144-60.
54 Hirsch FR, Matthews MJ, Aisner S, et al. Histopathologicclassification of small cell lung cancer: changing conceptsand terminology. Cancer 1988;62:973-7.
55 Graus F, Elkon KB, Cordon-Cardo C, Posner JB. Sensoryneuropathy and small cell lung cancer. Am J Med1983;80:45-52.
56 Hamid QA, Bishop AE, Springall DR, et al. Detection ofhuman pro-bombesin mRNA in small cell carcinoma ofthe lung: in situ hybridisation with a cRNA probe. Cancer
1989;63:266-71.57 Hamid QA, Corrin B, Dewar A, Hoefier H, Sheppard MN.
Expression of gastrin-releasing peptide (human bom-besin) gene in large cell undifferentiated carcinoma of thelung. JPathol 1990;161:145-51.
58 Hamid Q, Corrin B, Sheppard MN, Polak JM. Localisationof chromogranin mRNA in small cell carcinoma of thelung. JPathol 1991;163:293-7.
59 Minna JD. Autocrine growth factor production, chro-mosomal deletions and oncogene activation in the patho-genesis of lung cancer. Lung Cancer 1988;4:6-10.
60 Gazdar AF. 1990 Oncogenes, antioncogenes and growthfactors in the pathogenesis of small cell lung cancer(SCLC). In: Fiorentini G, Marangolo M, Rosti G, eds.Proceedings ofthe Second International Conference on SmallCell Lung Cancer Ravenna: Augustea, 1990:23-5.
61 Travis WD. Linnoila RL, Tsokos ME, et al. Neuroendo-crine tumours ofthe lung with proposed criteria for large-cell neuroendocrine carcinoma: Am J Surg Pathol 1991;15:529-53.
62 Reeve JG, Stewart J, Watson JV, Wulfrank D, TwentymanPR, Bleehen NM. Neuron specific enolase expression incarcinoma of the lung. Br J Cancer 1986;53:519-28.
63 Leader M, Collins M, Patel J, Henry K. Antineuron specificeiiolase staining reactions in sarcomas and carcinomas: itslack of neuroendocrine specificity. J Clin Pathol 1986;39:1186-92.
850
on July 4, 2020 by guest. Protected by copyright.
http://thorax.bmj.com
/T
horax: first published as 10.1136/thx.46.11.843 on 1 Novem
ber 1991. Dow
nloaded from