Embed Size (px)
Citation preview

A
K
1
wieimqarptemabfbmA
l
1d
Perspective on everyday technologies for Alzheimer’s care: Researchfindings, directions, and challenges
Eric Dishmana, Maria C. Carrillob,*aIntel Corporation, Beaverton, OR, USA
bAlzheimer’s Association, Chicago, IL, USA
bstract The Everyday Technologies for Alzheimer’s Care (ETAC) initiative was launched by the Alzhei-mer’s Association and Intel Corporation in 2003 to identify and fund promising research in the useof technology—especially information and communication technologies (ICTs)—for monitoring,diagnosing, and treating Alzheimer’s disease (AD). Agilent Technologies joined the initiative in2005. In October 2006, representatives of the three partners, together with ETAC award grantees,met to review the most recent research, and discuss how current and developing technologies canaddress growing needs in Alzheimer’s care.© 2007 The Alzheimer’s Association. All rights reserved.
Alzheimer’s & Dementia 3 (2007) 227–234
eywords: Alzheimer’s; Dementia; Technology; Information; Communication; Caregiving; Diagnosis; Treatment
idcaacaamwtcaaond
cpcvgC
. Introduction
By this century’s midpoint, global demographic changesill double or even triple the number of people over age 65
n many countries, putting healthcare systems and entireconomies at risk as chronic conditions and age-relatedllness and injuries become even more pervasive. A funda-ental question challenges all of us: how will we deliver
uality care and quality of life to today’s and tomorrow’sging population while reducing healthcare costs that al-eady threaten to swamp national economies? Cross-disci-line research centers that bring together computer scien-ists, engineers, gerontologists, social scientists, medicalxperts, and clinicians are emerging to explore how infor-ation and communication technologies (ICTs) might help
nswer this pressing social question. Small-scale, evidence-ased pilots of ICTs that will promote a shift from hospital-ocused or “mainframe healthcare” paradigms to home-ased or “personal health” paradigms [1] are cropping up inany parts of the world, with many of them focused onlzheimer’s disease (AD).It is not surprising that the majority of these independent
iving technology centers focus on AD. Alzheimer’s disease
*Corresponding author. Tel.: 312-335-5722; Fax: 866-741-3716
vE-mail: [email protected]552-5260/07/$ – see front matter © 2007 The Alzheimer’s Association. All righoi:10.1016/j.jalz.2007.04.387
s a debilitating and slowly progressing neurodegenerativeisease that presents unique challenges to caregivers. Be-ause many people suffering from AD remain physicallyble-bodied while gradually losing memory and cognitivebility, monitoring their behavior and activity becomes cru-ially important. Caregivers face overwhelming obstacles inssisting their loved ones with activities of daily living, inn effort to sustain a high quality of life for them as theiremory declines. Simultaneously, caregivers must dealith their own burnout and declining health resulting from
he extreme demands of caregiving. Professional caregivers,linicians, and researchers face challenges in diagnosingnd treating the disease. Often, people suffering from ADnd their families avoid early diagnosis and intervention outf fear, stigma, and denial. Additionally, traditional diag-ostics fail to provide much help in early diagnosis orifferentiation.
Modern computing, consumer electronics, and tele-ommunications technologies have the potential to im-rove the quality of life for both AD patients and theiraregivers. They also hold the promise of creating inno-ative approaches for detecting the disease and its pro-ression. The Everyday Technologies for Alzheimer’sare (ETAC) initiative was launched in 2003 to bring
isibility to early, pioneering research efforts in thists reserved.

dpsgpp
2
idon
vmapstmtiSsccta2dpA
nmeusoacffimibdd
3
p
amdsstsdlmtaadcthooaartasct
vochanBes
ftmatronbmcfiTsoS
228 E. Dishman and M.C. Carrillo / Alzheimer’s & Dementia 3 (2007) 227–234
omain, and to accelerate multidisciplinary research ap-roaches to investigating the potential of ICTs in fourpecific areas: disease diagnosis, tracking disease pro-ression, disease treatment, and caregiver assistance. Theortfolio of ETAC-funded grants thus far shows greatromise in these four interrelated domains.
. Technologies for disease diagnosis
Many AD patients consider the current neuropsycholog-cal tests very onerous, especially as their cognitive functioneclines. These tests also poorly distinguish different typesf dementia. The ICTs offer promising new ways to diag-ose and differentiate AD.
Virtual reality (VR) technology can be used to measureisuospatial ability, and may be both less burdensome andore probative than traditional two-dimensional (2D) pen
nd pencil tests. Virtual reality can be used in two classicaradigms that asses visual-spatial memory. First, the clas-ic Vandenberg shape-comparison test, in which one men-ally rotates images of test shapes to determine which oneatches a standard shape, can be performed through VR
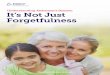
echnology which allows the participant to “see” the objectsn three dimensions (3D) and physically manipulate them.econd, the Morris water maze, a commonly used test ofpatial learning and memory for animal models of dementia,an also be performed in 3D space (Fig. 1) [2,3]. These testsan be performed with relatively inexpensive VR machineshat use special eyeglasses called shutter glasses that rapidlynd alternately occlude the eyes. Virtual reality tests, in bothD and 3D, are currently under evaluation to see if they canetect AD symptoms earlier than traditional pencil andaper tests, and if they can predict how well persons withD can orient themselves in their environment.Similarly, music technologies may offer valuable diag-
ostic information because they probe neuropsychologicalarkers for the episodic domains shown to be sensitive to
arly detection of cognitive decline [4], while offeringnique opportunities for community-wide use. Music washown to arouse individuals in late-stage AD who weretherwise not very responsive [5]. Hyperscore, a computerpplication that allows people with no musical education toompose their own music, has spurred people sufferingrom AD to overcome physical limitations and start usingne motor control to interact with the interface [6]. Newusic tools are being developed to move neuropsycholog-
cal testing into the auditory domain, where melodies areeing used to probe associative memory and thereby helpistinguish early AD from other diseases such as semanticementia or depression.
. Technologies for tracking disease progression
Wireless audiovisual networks and pocket personal com-
uter (PC) technology can be used both to monitor people’s hctivity over time, and to look for behavioral changes thatight be indicative of dementia or show progression of
isease. These monitoring systems can be combined withimple magnetic switches on appliances and pressure padwitches on furniture to get a picture of the types of activityhat people engage in during their daily routines. Suchystems offer many advantages to people suffering from theisease and to caregivers. When those affected by AD areiving alone, the systems can provide caregivers and familyembers with the peace of mind that comes from knowing
here is a system in place to monitor their loved one [7]. Inn institutional or nursing-home setting, these systems canlso provide valuable backup, since they operate 24 hours aay, 7 days a week. In nursing homes, where professionalaregivers are often overworked or may be unfamiliar withhe medical history of their charges, monitoring systemsave the potential to identify anomalous behavior that mighttherwise be missed. Families and facilities will have theption of choosing monitoring technologies that vary alongcontinuum of intrusiveness. For example, once installed
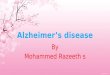
nd activated, in-home sensors will monitor movement,oom use, and device use. This tends to be intrusive, al-hough the opportunity to turn off the sensors may bevailable. Data entry devices such as the PocketPC Buddyystem will only accumulate and transmit information that aaregiver has entered, thus falling on the nonintrusive end ofhe continuum (Fig. 2) [8].
Feasibility studies indicate that monitoring systems areery beneficial. For example, in a small pilot trial conductedn eight adults over 10 days in a nursing home, videoamera technology found three episodes of aggressive be-avior that had been missed by staff members, and sixttempts to wander outside the building that had gone un-oticed. In the first in-home usability test of the Pocket-uddy system, one caregiver’s responses identified him asxtremely stressed, resulting in the recruitment of additionalupport [9].
A substantial amount of information may be gleanedrom these systems. Basic individual welfare can be ascer-ained. Medication status can determine if persons beingonitored are taking their prescription medications at the
ppropriate times and correct dosages. The system can po-entially recognize a problem indicative of dementia, e.g.,epeatedly opening and closing a refrigerator door, or somether activity that would not be expected of cognitivelyormal individuals. Disease monitoring could also warn ifehavior is indicative of disease progression. For example,ore frequent aggressive symptoms may signal a significant
hange in health status. This type of monitoring can bene-tuned to both gradual and dramatic behavioral changes.hese systems can be used to detect household maintenanceuch as running faucets and showers, to detect blocked orverflowing toilets, and to monitor household appliances.ystems and technologies have the potential to detect be-
aviors and events that warn of global safety issues and
dtnba
Omlcptoiawtwtt
icerthcamrbs
ucebaartwopta
4
ith
4
uwettrivprpbgostsc
4
mvstistjth
Fpi
229E. Dishman and M.C. Carrillo / Alzheimer’s & Dementia 3 (2007) 227–234
angerous risks. For example, doors left open, backed-upoilets, or stove burners left operating may all pose a sig-ificant risk. Actual reports of falls, wandering, and otherehaviors through interactive systems provide similar safetylarms.
However, potential problems exist with these systems.ne of the major difficulties with this type of technology isapping, i.e., it can be difficult to pinpoint the precise
ocation of the participant. With video-based systems, thisan be overcome by using multiple cameras to build a 3Dicture of the living space. With radiofrequency-based sys-ems, which are not very accurate at measuring distances,ne can focus on the shape of the trajectory of participantsn their environment rather than on their exact location. Thisllows the identification of frequently occupied locationsithin the “trajectory shape,” which can then be calibrated
o exact locations by comparing reported activity (e.g.,atching television, sleeping, or eating in the kitchen) with
he position of a participant in the trajectory map at thatime.
Several other technical difficulties with electronic mon-toring exist, including signal interference, technology in-ompatibility, and data-review limitations. Signal interfer-nce from a variety of household electronics andadiofrequency transmitters can be troublesome for moni-oring systems. Appliances such as microwaves, householdeating and cooling sensors, wireless phones, and wirelessomputer networks cause problems and can result in falselarms. This problem is likely to become worse asore appliances and applications become wireless. For
adiofrequency-based systems, the selection of a frequencyand that is interference-free is important. In the case of
ig. 1. Humans, like rats and mice, use room cues to find submergedlatform. Humans with hippocampal damage show severe spatial memorympairments on this task (Astur et al., 2004).
ystems that rely on off-the-shelf software and hardware, w
pdates from manufacturers can often be detrimental be-ause they may introduce incompatibilities or new interfer-nce patterns. Dedicated systems such as the pocket PC-ased PocketBuddy use custom-written software withutomatic updating [9]. With video monitoring systems, themount of data collected can be too cumbersome for manualeview. Software-based reviews will need to be developedhat can handle trillions of frames of video per day. Like-ise, systems need careful adjustment to reduce the numberf false positives. With video-based surveillance systems,rivacy is of primary concern [10]. A possible future solu-ion, allowing monitoring systems to maintain an individu-l’s privacy, is to monitor infrared wavelengths only.
. Technologies for treatment
People with AD may benefit from modern technologiesn many ways, from multimedia to help with identity reten-ion, and to interactive body and mind exercises that canelp with cognitive rehabilitation.
.1. Multimedia
Interactive websites that offer online support groups arender development to help families, caregivers, and peopleith neurodegenerative diseases. These websites provide
ducational videos and handbooks. In addition, multimediaechnology is being developed to assist people with cogni-ive and memory problems. The initial projects focus onemembering and reminiscing in people with mild cognitivempairment and mild to mid-stage AD. The aim is to de-elop multimedia DVDs that store and play patient biogra-hies. By regularly viewing these DVDs, participants betteretain their sense of identity, and the multimedia format alsorovides nurturing and emotional support for family mem-ers. These DVDs also have the advantage of giving care-ivers who are not family members a better understandingf the persons for whom they are caring [11,12]. There areome hurdles to overcome in the production of these rela-ively short (40-minute) biographies. Determining how toummarize a person’s life can be challenging, and conflictsan arise in families over content.
.2. Interactive exercises
Interactive programs under development fall into twoain categories: video-based and electrophysiological. The
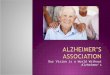
ideo system relies on a television and monitoring system tohow and monitor exercises, respectively. This system faceshe same problem as other video monitoring technologies,.e., the difficulty in accurately tracking the participant. Oneolution currently being explored is to dovetail the camerao a computerized model of the human torso that has 14ointed segments (Fig. 3). By mapping these segments onhe person, and then comparing their actual movements withow they should be moving, the system can decipher how
ell the person is performing the exercise. Robust prompts
afsmi
(sMoimmtwephpfitr[mir
iAdnnrp
vs
5
cepcpst
trgta
Fdd ealthca
230 E. Dishman and M.C. Carrillo / Alzheimer’s & Dementia 3 (2007) 227–234
re being developed that will help this system provideeedback to the participant. Algorithms are also being de-igned so that the system can cope with extraneous bodyovements that could otherwise confuse and crash the
nterface.Magnetoencephalography (MEG)/electroencephalagram
EEG)-based systems that measure brain activity noninva-ively are also being developed for cognitive training. TheEG/EEGs can record the full spatiotemporal orchestration
f the brain while it is occupied with a specific task, and candentify networks of brain areas that are essential to funda-ental cognitive processes such as attention and workingemory [13]. These approaches also allow measurement of
wo or more different brain processes simultaneously,hich is something that behavioral tasks cannot do. A prime
xample of this is attending-and-ignoring. People who areaying attention to one object while ignoring another mayave two different types of activity going on in differentarts of the brain at the same time, reflecting the processesor attending something of interest while simultaneouslygnoring other things that are distracting. Until recently,here was no physiological evidence for a separate processelated to ignoring irrelevant or distracting information14,15]. Now there is evidence that aging (and perhaps AD)ay differentially influence our ability to ignore irrelevant
nformation more than it affects our ability to attend toelevant information [16].
Buddy CoordinatAging in Place Initiatives for Alzhe
PocketBuddy events and messages provide caregiving support
Poc
Caregiver enters patient data into PocketBuddy
From
Mea
How
YE
WebBuddy Com
ig. 2. The PocketPC (PocketBuddy) technology provides portable, noninuring daily caregiving activities. PocketBuddy is capable of recording behata can be made accessible to a virtual network of family, friends, and h
The MEG/EEG measures can help tailor cognitive train- h
ng. For example, they could be used to identify and helpD patients whose brain networks do not interact robustlyuring cognitive tasks. This may be used to identify sensoryetworks, sensory-motor networks, and cognitive-controletworks that are engaged during specific tasks, and byecording how the brain is responding, may help trackrogress during cognitive therapies.
Currently, the main focus for this technology is on de-eloping the interface and algorithms needed for complexignal detection and brain network identification [17,18].
. Technologies for caregiver assistance
Monitoring can be a two-way street. In addition to re-eiving monitoring information about a person with AD,veryday technologies can also be used to contact and assisteople in managing their everyday lives, thus giving theiraregivers respite. Technologies that are actively being ex-lored include verbal live systems, digital television, andimple cell-phone interfaces that give individuals promptso help them cope with activities of daily living.
Live systems based on video monitoring are designed torack people engaged in specific tasks (e.g., making tea), toecognize if they get stuck at a particular point, and thenive them a verbal prompt. The development of software forhis type of system can be extremely challenging. Considersimple task such as drying one’s hands, for example. The
althcare System Disease Patients and Caregivers
ddy Component
Network access in the home transmits data to central data source
Central Data Source
tPatient data is accessible via the Web to support network of family, friends, caregivers, and healthcare personnel
support for gathering data about the Alzheimer patient and the caregiverand emotional changes observed by the caregiver. Using Web technology,re professionals.
ed Heimer’s
ketBu
: Linda
l delivery
’s Dad?
S NO
ponen
vasiveavioral
ands will often be covered by the towel or by each other,

mtoae[
fietrassvga
dmmcsToo
cTedta
Fof with the
231E. Dishman and M.C. Carrillo / Alzheimer’s & Dementia 3 (2007) 227–234
aking it extremely difficult for the video system to keeprack. Sophisticated software algorithms are being devel-ped to ensure that tracking systems are accurate and widelypplicable, so that new models need not be reinvented forach specific task that one may want to monitor (Fig. 4)19–21].
Digital television prompting systems may be very usefulor people affected by AD who tend to spend a lot of timen front of the television. This type of system may bextremely useful not only to the person living alone, but alsoo those living with caregivers, because this system canelieve some of the “prompting” burden from the caregivernd help reduce conflict. The prompts can range from veryubtle (images of food near mealtimes) to explicit (a mes-age to take a particular medication), but must be scheduledia an easy-to-use control interface. Requirements-athering and system design are real challenges, calling forrange of coordinated methodologies [22].Cell phones are relatively simple, light, and wearable
evices that can be used to communicate with individuals,ainly as a reminding device [23,24]. A week’s or aonth’s worth of short video messages, recorded with a
omputer and webcam, can be loaded into the phones andet to deliver appropriate messages at the appropriate time.he system design can also accommodate a certain degreef flexibility, so that messages can be updated or substituted
ig. 3. In the Interactive Video Exercise project, the image analysis algorithf body parts, with panels 2 and 3 showing the fit of the segmented modeedback messages for elders as they perform their chair exercises along
n the go. This may be particularly useful for the busy
aregiver who may have to delay visits or alter schedules.hese systems are being designed backwards, from thend-user. Appropriate target activities will be identified andeveloped via interviews with people affected by AD andheir caregivers. These will then be tested in the field, andppropriate adjustments will be made.
Problems and areas for future development include:
● What to prompt? Choosing the best prompt that ismost likely to get the desired response is important.
● How to prompt? Prompts can be images, an engi-neered machine voice, a recorded human voice, or atone. Voice prompts have the advantage of being ableto deliver very specific messages. Recorded humanvoices may be less irritating and more comforting,especially those of a family member or primary care-giver. However, populating systems with recordedmessages may take considerable time.
● How to input prompts? If systems are flexible enoughthat prompts can be customized, the input interfacemust be user-friendly.
● How to cope with ignored prompts? The systemsshould be flexible enough to recognize when users areignoring prompts, and respond appropriately. Devel-oping this capability may be challenging.
● How to handle data volume? Monitoring systems will
el the user with body segments and joints. Panel 1 shows the segmentationrecognition of exercise movements provides input for real-time tailoredcoach on video.
ms model. The
contain a high number of variables, and the volume of

6
etts
6
w
pfigdpwcwd
6
Fla
232 E. Dishman and M.C. Carrillo / Alzheimer’s & Dementia 3 (2007) 227–234
data generated for analysis will be considerable. Sys-tems must be robust enough to cope.
. General considerations and conclusions
Regardless of the application, some overarching consid-rations apply to the development and dissemination of allypes of ICTs that might be used to improve the lives ofhose dealing with AD. Some topics worthy of future re-earch and discussion are outlined below.
.1. Ethical issues
We found that many Institutional Review Boards (IRBs)
Task started
Rinse hands
Task
U
D
Use soap
Turn on
Turn off
Dry hands
ig. 4. A probabilistic temporal model of hand washing: The features are coosely grouped using flocking constraints. The module consists of actionnd towel positions; Timeout; Water sensor.
ere ill-equipped to provide timely review of ETAC-related E
rojects, often because they use drug trials as their modelor evaluating risk, though many ICT-enabled protocolsnvolve little to no participant risk. The development of aeneral strategy or white paper that describes the concepts,evelopment, and potential benefits of technological ap-roaches would be useful for IRBs that may be unfamiliarith the technology, and that may have ethical or privacy
oncerns. Given the cultural differences involved in livingith AD and the varying privacy concerns, understandingifferences across nations and cultures would also be useful.
.2. Proprietary issues
System integration and the technology challenges of
Wet hands
n on
soap
ands
n off
ristics of the local appearance of the person’s hands to be tracked and areothing; Prompt (min, med, max); Call caregiver and Observations: Hand
Tur
se
ry h
Tur
haractes: Do n
TAC-type grants often require partnership with industry,

wispeiinilp
6
pttpfiibaivat
6
tbssouancttlt
6r
pesbsunr
rwtbaAsc
6
ohrimntsmoahitrut
R
233E. Dishman and M.C. Carrillo / Alzheimer’s & Dementia 3 (2007) 227–234
hich may mean that researchers face restrictions on shar-ng information. The interoperability of these technologyystems is key if we are to achieve the size and scale ofilots required to prove return on investment (ROI) andfficacy of ICTs for AD. A guideline for researchers andndustry partners on how to navigate confidentiality andntellectual property issues would be helpful. Given theeed to accelerate the pace of discovery, reduce redundancyn research, and produce larger data sets for statistical va-idity, we believe that open-source hardware and softwarelatforms may help solve some of these issues.
.3. Funding
Because the field is relatively new, members of fundinganels and organizations may be unaware of the value ofhis type of research for AD and other age-related condi-ions. Many ETAC researchers, even when armed withositive, promising research results from their initial pilots,nd it impossible to gain additional funding for larger stud-
es. Often they “fall between the cracks” of technology-ased funding initiatives and clinically based funding initi-tives that do not support cross-disciplinary and appliednvestigation. We believe it is imperative to bring moreisibility to assistive technology research programs, and todvocate nationally for increased funding of clinical andechnological research focused on innovative uses of ICTs.
.4. Integration and ease of use
Through ETAC, we have found that many research cen-ers are spending significant amounts of time and money touild technologies that may already exist. Often, these re-earchers fail to obtain much pilot data in the field becauseo much of their funding is spent on technology integrationr on making technologies usable by frail individuals andntrained family members. We must find ways to cooperatend prevent the simultaneous development of similar tech-ologies, thus preserving resources while accelerating out-omes studies. Over the long term, integrating researchechnologies from numerous universities and research cen-ers into shared research platforms can alleviate this prob-em, with the caveat that this could restrict novelty if pushedoo aggressively in the early stages of the field.
.5. Developing a community of researchers andeviewers
One of the most significant challenges facing the ETACrogram has been to find reviewers with mixed-disciplinexpertise to evaluate research proposals. Most ETAC re-earchers have reportedly been rejected for follow-up grantsy technical reviewers who clearly have no clinical under-tanding of AD, and by clinical reviewers who do notnderstand assistive technologies. As with any new field orontraditional research domain, building a community of
esearchers and reviewers takes time, and scaling to largeresearch pilots will remain a challenge without creativeays to increase the research community. The ETAC ini-
iative, in a short period of time, has played a central role inringing visibility and momentum to this emerging field,nd will look to ICTs not only to help people suffering fromD and their caregivers, but to help the researchers them-
elves collaborate better across borders, disciplines, andultures.
.6. Stigmatization of older people
Finally, perhaps the “grand challenge” of ETAC is tovercome the cultural stigma and denial about aging thatas kept these topics from rising to the top of nationalesearch agendas, in spite of the imminent age wave and itsnevitable economic impacts. Stigma and denial take nu-erous forms, from funding agencies that ignore the unique
eeds of aging populations to companies that refuse to haveheir brand associated with “old people.” The ETAC re-earchers have routinely found that other researchers, familyembers, social workers, and policymakers assume that
lder people and people with AD are incapable of learningnd using ICTs. The portfolio of ETAC grants thus farighlights promising directions that we cannot afford tognore. This portfolio offers demonstrable evidence thatoday’s older members of society—and certainly tomor-ow’s, who will be even more “tech-savvy”—are eager tose and to co-invent new information and communicationechnologies that hold promise to improve their lives.
eferences
[1] Dishman E. Inventing wellness systems for aging in place. IEEEComput 2004;34–41.
[2] Astur RS, Tropp J, Sava S, Constable RT, Markus ET. Sex differ-ences in a virtual Morris water task and a virtual eight-arm maze.Behav Brain Res 2004;151:103–15.
[3] Parsons TD, Larson P, Kratz K, Thiebaux M, Bluestein B, Buck-walter JG, et al. Sex differences in mental rotation and spatial rotationin a virtual environment. Neuropsychologia 2004;42:555–62.
[4] de Jager CA, Milwain E, Budge M. Early detection of isolatedmemory deficits in the elderly: the need for more sensitive neuropsy-chological tests. Psychol Med 2002;2:483–91.
[5] Cuddy LL, Duffin J. Music, memory, and Alzheimer’s disease: ismusic recognition spared in dementia, and how can it be assessed?Med Hypotheses 2005;64:229.
[6] Machover T. Shaping minds musically. BT Technol J 2004;22:171–9.[7] Mahoney DF, Tarlow B. Workplace response to virtual caregiver
support and remote home monitoring of elders: the WIN project. StudHealth Technol Informatics 2006;122:676–80.
[8] Becker SA, Webbe FM. Designing for older adult users of handheldtechnology. In. Proceedings of the 28th IEEE Engineering in Medi-cine and Biology Society Annual International Conference; 2006:3297–300.
[9] Becker SA, Webbe F. Use of handheld technology by older adultcaregivers as part of a virtual support network. In. Proceedings of theFirst International Conference on Pervasive Computing Technologies
for Healthcare; 2006: article 56.
[
[
[
[
[
[
[
[
[
[
[
[
[
[
[
234 E. Dishman and M.C. Carrillo / Alzheimer’s & Dementia 3 (2007) 227–234
10] Bharucha AJ, London AJ, Barnard D, Wactlar H, Dew MA, ReynoldsCF III. Ethical considerations in the conduct of electronic surveillanceresearch. J Law Med Ethics 2006;34:611–9.
11] Baecker RM, Marziali E, Cohene T, Mindy S, Ramdeen K, ChatlandS. Multimedia biographies for individuals with Alzheimer’s diseaseand their families [abstract]. In. Proceedings of the World Congresson Internet in Medicine (MEDNET); 2006. Available at: http://www.mednetcongress.org/ocs/viewabstract.php?id�188.
12] Cohene T, Baecker RM, Marziali E, Mindy S. Memories of a life: adesign case study for Alzheimer’s disease. In: Lazar J, ed. UniversalUsability. New York: John Wiley & Sons; 2007, p. 357–88.
13] Dale AM, Liu AK, Fischi RB, Buckner RL, Belliveau JW, LewineJD, et al. Dynamic statistical parametric mapping: combining fMRIand MEG for high-resolution imaging of cortical activity. Neuron2000;26:55–67.
14] Worden MS, Foxe JJ, Wang N, Simpson GV. Anticipatory biasing ofvisuospatial attention indexed by retinotopically specific alpha-bandEEG increases over occipital cortex. J Neurosci 2000;20:1–6.
15] Pantazis D, Weber DL, Dale CL, Nichols TE, Simpson GV, LeahyRM. Imaging of oscillatory behavior in event-related MEG studies.Proc SPIE Comput Imag III 2005:674:55–63.
16] Gazzaley A, Cooney JW, Rissman J, D’Esposito M. Top-down sup-pression deficit underlies impairment in normal aging. Nat Neurosci2005;8:1298–300.
17] Ahammad P, Bajcsy R, Simpson GV, Sastry S. Tools for character-ization and classification of brain activity via magnetoencephalogra-phy. In. Engineering principles in biological systems, Cold Spring
Harbor symposium. 2006.18] Darvas F, Hui H, Dale C, Simpson GV, Leahy RM. Linear andnon-linear directional interaction measures applied to paced and self-paced finger movements. an MEG study. In: Proceedings of 15thInternational Conference on BioMagnetism; 2006, p. 109.
19] Boger J, Hoey J, Poupart P, Boutilier C, Fernie G, Mihailidis A. Aplanning system based on Markov decision processes to guide peoplewith dementia through activities of daily living. IEEE Trans InformTechnol Biomed 2006;10:323–33.
20] Hoey J, von Bertoldi A, Poupart P, Mihailidis A. Tracking usingflocks of features, with application to assisted handwashing. In. Pro-ceedings of British Machine Vision Conference 2006:367–76.
21] Hoey J, von Bertoldi A, Poupart P, Mihailidis A. Assisting personswith dementia during handwashing using a partially observableMarkov decision process. The 5th International Conference onComputer Vision Systems; 2007. Available at: http://biecoll.ub.uni-bielefeld.de/volltexte/2007/12.
22] Newell AF, Carmichael A, Gregor P, Alm N. Information technologyfor cognitive support. In: Jacko J, Sears A, eds. The human-computerinteraction handbook, 2nd ed. Mahweh (NJ): Lawrence ErlbaumAssociates; 2007:464–81.
23] Oriani M, Moniz-Cook E, Binetti G, Zanieri G, Frisoni GB, GeroldiC, et al. An electronic memory aid to support prospective memory inpatients in the early stages of Alzheimer’s disease: a pilot study.Aging Mental Health 2003;7:22–7.
24] Lekeu F, Wojtasik V, Van der Linden M, Slamon E. Training earlyAlzheimer patients to use a mobile phone. Acta Neurol Belg 2002;
102:114–21.