()Anatomy: A Cost-Effective Intelligent Decision Support
System in Surgery for More Effective Treatment of
Gastrointestinal Diseases through Optimal Surgical
Procedures
Collaborating Principal Investigator
1 Overall Objectives
Crohn’s disease is a clinically challenging inflammatory condition
capable of afflicting the entire gastro-intestinal tract.
Surgically, Crohn’s disease with multiple narrow strictures is
treated not by resection but by changing the intestinal geometry
using a procedure called the Heineke-Mikulicz (HM) strictureplasty.
There is growing appreciation that mechanical stresses influence
the development and progression of pathology. I hypothesize that
the wall mechanical strain and stress fields generated by the
strictureplasty geometry as well as certain types of anastomosis
(end-to-end, side-to-side, end-to-side) may predispose the
intestinal wall to mechanical instability states, and this can lead
to intestinal maladaptation and subsequent surgical failure, e.g.
anastomotic leak or recurrence of disease. The overall goal of this
proposal is to design and implement an intelligent decision support
system (IDSS) in surgery that will be able to identify those points
of mechanical instability and will provide the surgeon with
alternative optimal surgical procedures that could alleviate the
risk of surgical failure, thus improving the quality of life of
children and adults affected by this disease and reducing the
re-operative rates that are known to be associated with significant
patient morbidity in inflammatory bowel diseases (IBD). The IDSS
will model the strain and stress fields in the segment of the
patient-specific intestinal wall around the suture line and
far-field from it under varied loading conditions and with given
anastomotic geometries.
∗Address: Department of Bioengineering, Center for Vascular
Remodeling and Regeneration, McGowan
Institute for Regenerative Medicine, University of Pittsburgh, 300
Technology Drive, Pittsburgh, PA 15213,
United States; phone: 650-796-8846; fax: 412-383-8788; e-mail:
[email protected] †Address: Department of Surgery, University of
Pittsburgh Medical Center, 200 Lothrop Street, Pitts-
burgh, PA 15213, United States, e-mail:
[email protected]
1
2 Specific Aims
I have formulated the following hypotheses and designed the
associated specific aims to test them: Hypothesis #1: The
intestinal wall response to the surgical geometry depends on its
material properties. Specific Aim #1: Measure either ex-vivo or
intra-operatively the intestinal wall material properties in
different locations such as duodenum, jejunum, ileum, appendix,
colon, and rectum, and correlate the measured material properties
with known patient-specific clinical factors, e.g. smoking,
malnutrition, chemo-radiation treatment, lead- ing to increased
risks of surgical anastomoses failure. Hypothesis #2: The location
of multiple strictureplasties and the intraluminal pressure and
flow can make the intestinal wall susceptible to recurrence of
Crohn’s disease. Specific Aim #2: Improve the current model of
single HM strictureplasty to account for the effect of multiple
strictureplasties and the pressure and flow profiles on mechanical
instability states in a patient-specific geomet- rical setting.
Hypothesis #3: Side-to-side anastomosis can serve as a point of
reversible obstruction and lead to increased symptoms in Crohn’s
patients. Specific Aim #3: Model the strain and stress fields in
different geometries of anastomosis, i.e. end-to-end, side-to-
side, and end-to-side, to reveal states of mechanical instability
that would predispose the initiation of surgical failure.
Hypothesis #4: Patient anatomic factors, such as length of sigmoid
colon, length of inferior mesenteric artery and vein, can play a
role in the mechanical stability of low colorectal anastomosis.
Specific Aim #4: Integrate the specific mechanical constraints that
far-field patient anatomy, such as length of sigmoid colon and
mesentery, imposes on the local anastomotic mechanical
fields.
3 Background
Crohn’s disease is a clinically challenging inflammatory condition
capable of afflicting the entire gastro-intestinal (GI) tract [1].
The pathology is part of a wider set of conditions termed
inflammatory bowel disease (IBD). Due to the multi-focal nature of
Crohn’s in- flammation, multiple non-adjoining areas of localized
luminal narrowing are commonly en- countered upon surgical
exploration [2]. Surgically, Crohn’s disease with multiple narrow
strictures (Figure 1) is treated not by resection but by changing
the intestinal geometry using a procedure called the
Heineke-Mikulicz (HM) strictureplasty, in hopes of preserving the
intestinal length in a patient population at high risk for
short-gut syndrome [2, 3]. Tech- nically, the procedure involves
making a longitudinal incision on the anti-mesenteric side (top
side, opposite from where the blood vessels enter the intestinal
wall) across the stric- tured portion of intestine (Figure 2A),
then juxtaposing the two vertices of the incision (Figure 2B-C),
and closing the incision transversely (Figure 2D).
Mechanical forces play an intricate role in biological systems from
the tissue and organ level down to individual cells and even
proteins [4, 5, 6]. There is growing appreciation that mechanical
stresses influence the development and progression of pathology.
For example, in the much studied cardiovascular system, arteries
are known to be sensitive to the local mechanical environment to
which they are exposed, and it is well established in the
literature that variation in the mechanical stresses can cause
growth and remodeling in the arterial wall [7, 8, 9]. Less work has
been done in the GI system [10, 11, 12]. However, small
animal
2
Alkiviadis Tsamis
studies have shown that intestinal tissue also undergoes active
remodeling as a function of increased mechanical stress [10, 12,
13]. Surgeons empirically understand that mechanical forces play an
important role in healing. In GI surgery, tension on an anastomosis
plays an important role and is strongly linked to poor anastomotic
healing and tissue breakdown [14]. Likewise, plastic surgeons
strive to decrease the degree of tension (in-plane stretching) in
skin flaps to avoid tissue death [15]. Surgery by definition leads
to reconstruction of tissues in non-native geometries that alter
the mechanical environment of those tissues.
Figure 1: Multiple small bowel strictures. Figure taken from
[3].
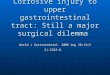
Figure 2: Heineke-Mikulicz (HM) strictureplasty procedure performed
in a patient with focal stricturing. (A.) Linear incision is made
along the anti-mesenteric border, extending proximally (a) and
distally (a’) across the stricture into healthy bowel. (B. and C.)
The incision is closed transversely with the approximation of
vertex points a and a’, which initially were separated by the
length of the incision. (D.) Completed HM strictureplasty. Figure
taken from [16].
3
3.1 Previous work in the area by others
Bowel preserving Crohn’s colitis surgery in the form of HM
strictureplasties introduces new anatomy (geometry) to a local part
of the intestine. This new anatomy can be indicative of buckling
modes which can undergo limit point instability states [17].
Buckling of thin plates with through cracks has been studied in
compressive loading [18, 19, 20, 21], bending loading [22], and
tensile loading [20, 21, 22]. Of note, buckling in tensile loading,
which is not directly evident, can occur in compressed regions
especially around cracks or holes [20]. It has been reported that,
if a thin plate is bent in one direction and deformed in the other
direction, similar to the combined loading conditions generated by
the strictureplasty, this may generate limit point instabilities or
singularities [23].
3.2 Previous work by Pocivavsek et al. [16]
Prior work by Pocivavsek et al [16] focused on the purely geometric
components of the HM strictureplasty procedure, concluding that the
transverse closure generates a saddle-like ge- ometry with a
central point carrying −2π Gaussian curvature condensation (Figure
3A, black circle) flanked by +π cones (Figure 3A, red circles).
Simple elastic modeling of the anti-mesenteric surface showed that
these purely geometric factors could account for the overall
strictureplasty shape. A key conclusion of this work was a
connection between the saddle-like geometry and its effect on
luminal cross-sectional area (Figure 3B), a parameter closely tied
to Crohn’s pathology. Immediately underneath the transverse suture
line there was pronounced dilation (Figure 3B, green shaded area,
top image), as expected from the highly successful clinical
application of strictureplasty to alleviate obstructions. How-
ever, just proximal and distal to this dilation, there were areas
of contracture (Figure 3B, green shaded area, bottom left and right
images). Pocivavsek et al [16] hypothesized that the
geometry-induced luminal narrowing proximal and distal to the
strictureplasty may serve to promote disease recurrence: first,
increased propensity for bowel content stasis prox- imal to the
strictureplasty leading to potential overgrowth and inflammation,
and secondly, given an already compromised lumen, the need for less
disease-specific narrowing prior to clinical re-presentation of
obstruction. In summary, the geometric analysis of HM stricture-
plasties argues for altered luminal flow (fluid mechanics) as a
potential explanation of disease recurrence patterns after
successful strictureplasty.
3.3 Previous work by Tsamis et al. [24, 25]
With Crohn’s disease, surgeons have noted that pathology tends to
recur not at the site of transverse closure but at some distance
proximal or distal to it [26, 27], and recurrence rates are higher
in the inter-plasty regions [28]. I hypothesize that the stress
distributions generated by the non-linear HM strictureplasty
geometry may serve as the nidus of disease recurrence. In
particular, the recurrence of Crohn’s disease can be associated
with remodeling of the mesenteric wall (bottom side, where the
blood vessels enter the intestine) which can be driven by
stress-induced alteration in blood perfusion or in interstitial
pressure [7]. To test the hypothesis, I used finite element
simulations to reproduce the highly non-linear geometries of the HM
strictureplasty and at the same time calculate mechanical stress
fields
4
Alkiviadis Tsamis
around the suture line and far-field from it. My aim is to study
and understand the mechanics of these non-linear geometries in
idealized materials, and to formulate a general framework upon
which further layers of complexity can subsequently be added.
Figure 3: Models of single enterotomy Heineke-Mikulicz (HM)
strictureplasties of varying length. (A.) CT derived
three-dimensional reconstructions of final Heineke-Mikulicz geome-
tries generated from 2, 3, and 4cm linear enterotomies. (B.) Shows
the relative cross-sectional areas of the three models from distal
to proximal ends and across the HM strictureplasty sites as a
function of arc length. Figure taken from [16].
I designed the HM strictureplasty finite element models in Abaqus
(Version 6.12-3, c© Dassault Systemes, 2012) to simulate the
above-mentioned surgical procedure which is displacement-driven. I
modeled the intestine as a 3D deformable extruded cylindrical shell
of diameter 2cm and length 10cm [16] (Figure 4A). The surgical cut
(enterotomy) was gen- erated by an extruded linear cut on the
anti-mesenteric side (Figure 4A, inset). The linear cut length
varied from 0.5-2 times the diameter, with a gap width of 2µm in
the middle of the cut length. The two edges of the cut were formed
by 2 spline curves as shown in Figure 4B. For all simulations tube
diameter was fixed to 2cm, while enterotomy length was varied. The
wall material was assumed linearly elastic, isotropic and
incompressible. The enterotomy was closed transversely in twenty
consecutive steps. The governing dimensionless parameters in the
problem were α=cylinder thickness/cut length and φ=tube
diameter/cut length.
I tested the above-mentioned hypothesis by analyzing the variation
of the wall stress across the wall thickness on both the
anti-mesenteric and mesenteric surfaces, knowing that bending
stresses in the middle surface of the thickness (neutral surface)
are close to zero. The measure of stress that I used in the model
is the equivalent tensile stress or von Mises stress
σMises =
xy + σ2 yz + σ2
Alkiviadis Tsamis
which is frequently used to describe the stress field of materials
under multiaxial loading conditions. The σxx, σyy , and σzz are the
normal components, and the σxy, σyz , and σzx are the shear
components, of the Cauchy stress tensor
σ =
X
Y
Z
X
Z
Figure 4: (A.) The intestinal wall was modeled as a 3D deformable
extruded cylindrical shell of diameter 2cm and length 10cm [16].
The surgical cut (enterotomy) was simulated as an extruded linear
cut (0.5-2 times diameter) on the anti-mesenteric side that was
formed by 2 spline curves separated by a small gap of 2µm in the
middle of the length of the model cylinder (A., inset). (A.) also
shows 1 partition on the X-Z plane, 1 partition on the Y-Z plane,
and 41 equi-distanced circular partitions on the X-Y plane along
the length of the linear cut to provide locations for displacement
boundary conditions. (B.) Shows the 2 spline curves that are used
to form the two edges of the cut.
Stress distributions on the inner, middle, and outer shell surfaces
are shown for φ = 1.3 with α = 0.033 (Figure 5A) and α = 0.067
(Figure 5B), and for φ = 0.5 with α = 0.013 (Figure 6A) and α =
0.025 (Figure 6B). By setting the middle surface as the origin (z =
0) allows us to define the outer shell surface as z = +t/2 and
inner shell surface as z = −t/2, where t is shell thickness. On the
anti-mesenteric half, the pattern of stress distribution is similar
for all cases, with a high stress middle plane core σij |z=0 around
the HM strictureplasty vertex, while outside this core σij |z=0 ∼
0. The core size is most sensitive to shell thickness and
relatively insensitive to enterotomy length as seen by comparing
Figure 5 and Figure 6. Moving onto the inner and outer shell
planes, the stress magnitude increases and the distribution
encompasses a larger area of the anti-mesenteric surface: σij
|z=±t/2 >> σij |z=0. These stresses are distributed in a
floret pattern along the peaks and valleys of the hyperbolic saddle
generated by the HM strictureplasty and, again, their magnitude is
most sensitive to shell thickness.
On the mesenteric half a very different pattern of stress
distribution is seen compared to the anti-mesentery. First, the
stress magnitudes are highly sensitive to enterotomy length.
6
Alkiviadis Tsamis
For φ = 1.3, the mesenteric surface in nearly stress-free across
shell thickness (see Figure 5). However, as the enterotomy length
is quadrupled (φ = 0.5 and Figure 6), a semi-elliptical ring of
stress around a stress-free central zone located underneath the
transverse closure appears. In contrast to the nodal distribution
of stress magnitude observed on the anti- mesentery, the mesenteric
stresses are more uniformly distributed throughout shell thickness:
σij |z=−t/2 ∼ σij |z=0 ∼ σij |z=+t/2. It should be noted that the
mesenteric stresses are highest at points distal and proximal to
the HM strictureplasty suture line.
INNER MIDDLE OUTER
A.
B.
stress
Figure 5: Stress distributions on the inner, middle, and outer
shell surfaces for φ = 1.3 with α = 0.033 (A.) and α = 0.067 (B.).
On the anti-mesenteric half, both shells showed the same pattern of
high stress focused only at the vertex core for the middle surface
but high stress regions distributed along the peaks and valleys of
the hyperbolic saddle on the inner and outer surfaces (floret type
distribution). On the mesenteric half, there was trace stress only
along the middle surface.
Furthermore, the luminal area distal and proximal to the transverse
closure collapsed for φ=0.5 and underwent a phase transition as the
strictureplasty was formed. The model suggests that under long
enterotomy lengths, the stresses on the mesenteric wall may lead to
focal areas of hypo-perfusion and may trigger the initiation of
tissue adaptation and possi- ble recurrence of Crohn’s disease
distal and proximal to the HM strictureplasty suture line. Bending
modes of deformation in the anti-mesentery and stretching modes of
deformation in the mesentery suggest that, ideally, an optimal
combination of bending, tensile and compres-
7
Alkiviadis Tsamis
sive loads might provide an anatomy in which the developed strains
and stresses could be minimal. Finally, based on our analysis, the
stitch connecting the enterotomy vertices seems to be the
controlling stitch, which sets not only the global geometry but
also the overall energy of the deformation. Furthermore, the force
in this stitch becomes minimal after a critical value of enterotomy
length (Figure 7, diameter/cut length∼0.8).
INNER MIDDLE OUTER
A.
B.
stress
Figure 6: Stress distributions on the inner, middle, and outer
shell surfaces for φ = 0.5 with α = 0.013 (A.) and α = 0.025 (B.).
On the anti-mesenteric half, the stress distribution again showed a
pattern of stress-focusing at the vertex core for the middle
surface, with high stress regions covering nearly the whole half on
the inner and outer surfaces. On the mesenteric half, stresses were
present throughout the thickness of the shell and distributed in a
semi-elliptical ring around a stress-free central zone located
underneath the transverse closure.
8
Alkiviadis Tsamis
0 0.5 1 1.5 2 2.5 3 3.5 4 4.5 5 0
0.05
0.1
0.15
0.2
0.25
0.3
displacement
F z
Φ = 2.00
Φ = 1.30
Φ = 1.00
Φ = 0.80
Φ = 0.66
Φ = 0.57
Φ = 0.50
Figure 7: Force (z − component) versus displacement curves for
vertex point closure with different values of enterotomy length φ
and thickness 0.06. For small enterotomy length (φ > 1.3), the
curves were indicative of Euler buckling. However, with increasing
enterotomy length (φ ≤ 1.3), the force-displacement curves were
indicative of limit point instability. It is interesting that the
maximum force did not change for φ ≤ 0.8 and remained lower than
the maximum force corresponding to smaller enterotomy lengths (φ
> 0.8).
4 Detailed Research Plan
The overall goal of this proposal is to design and implement an
intelligent decision support system (IDSS) in surgery that will
provide the surgeon with patient-specific optimal surgi- cal
geometries for more effective treatment of GI disease. Our approach
initially focuses on Crohn’s surgeries such as the strictureplasty,
however the tools developed will easily be broad- ened to other
common GI surgical procedures. The methodology is based on the
hypothesis that the wall mechanical strain and stress distributions
generated by the non-linear geom- etry of the strictureplasty as
well as certain types of anastomosis (end-to-end, side-to-side,
end-to-side) may serve as the nidus of surgical failure, e.g.
anastomotic leak or recurrence of GI disease. More specifically,
the anatomy of a surgical geometry can predispose the GI wall to
mechanical instability states under varied loading conditions, and
this can lead to GI mal- adaptation and subsequent surgical
failure. The personalized IDSS will be able to identify points of
mechanical instability that can be caused by the intended surgical
intervention, and will provide the surgeon with alternative optimal
surgical procedures that would alleviate the risk of surgical
failure within the patient-specific tissue properties and anatomy,
thus
9
Alkiviadis Tsamis
improving the treatment of Crohn’s disease and the quality of life
of children and adults affected by this disease, and reducing the
re-operative rates that are known to be associated with significant
patient morbidity in IBD. The IDSS will be finite element-based to
reproduce the highly non-linear geometries of the strictureplasty
and anastomosis. It will model the strain and stress fields in the
segment of the patient-specific GI wall around the suture line and
far-field from it under varied loading conditions and with given
anastomotic geometries, eventually incorporating realistic material
properties to give a true biomechanics picture. The IDSS will be
formulated on a general framework upon which further layers of
complexity can subsequently be added, such as material
heterogeneity, the effect of splenic mobilization, the effect of
mesenteric attachments (inferior mesenteric artery and vein
ligation), intra-luminal intestinal fluid mechanical stresses
(effect of diverting loop ileostomy), and the contact of the GI
wall with surrounding abdominal tissue.
4.1 Hypothesis #1
The GI wall response to the non-linear surgical geometry is
dependent on its anisotropic non- linear material properties.
Specific Aim #1a: Measure either ex-vivo or intra-operatively the
GI wall anisotropic non-linear material properties in different
locations of the GI tract such as duodenum, jejunum, ileum,
appendix, colon, and rectum. Specific Aim #1b: Correlate measured
material properties with known patient-specific clinical factors,
e.g. smoking, mal- nutrition, chemo-radiation treatment, leading to
increased risks of surgical anastomoses fail- ure. The GI wall
anisotropic non-linear material properties will be measured either
ex-vivo, using fresh (non-fixed) tissue samples obtained from
surgical resections under IRB-approved protocols, or
intra-operatively. The ex-vivo characterization of elastic moduli
will be done using biaxial testing machine, as well as
compressional tensiometer to obtain bulk moduli. The clinical
control parameters could be: albumin, pre-albumin, age, sex,
smoking status, immuno-modulatory medications, cancer status,
history of chemotherapy, history of radi- ation, and history of
IBD, as well as nutritional status of patients. The intra-operative
characterization of tissue properties could be done using optical
methods such as elastogra- phy.
4.2 Hypothesis #2
The location of multiple strictureplasties and the dynamics of
pressure and flow in the lumen of the GI tract can make the GI wall
susceptible to recurrence of Crohn’s disease. Specific Aim #2:
Improve the current model of single HM strictureplasty [24, 25] to
account for the effect of multiple strictureplasties and the
pressure and flow profiles on mechanical in- stability states in a
patient-specific geometrical setting. Strains and stresses in the
surgical GI anatomy will be obtained using finite element analysis
in ABAQUS (Version 6.12-3, c© Dassault Systemes, 2012). The current
model of single HM strictureplasty will be improved to include
realistic wall thickness, anisotropic non-linear material
properties, multiple HM strictureplasties within one model tube,
effect of internal pressure (positive or negative) on HM
strictureplasty geometry and stresses, and flow profiles through
one or multiple HM strictureplasties to couple the
elasticity-derived geometry with flow of fluid or solid material in
the intestinal lumen. Simulations will be repeated using
patient-specific intestinal geome-
10
Alkiviadis Tsamis
tries obtained from CT images under IRB-approved protocols. The 3D
geometries will then be reconstructed using commercially available
software (IDL, MATLAB, RHINOCEROS, TRUEGRID) and be input in
ABAQUS.
4.3 Hypothesis #3
Side-to-side anastomosis can serve as a point of reversible
obstruction (un-published clinical data provided by Dr. David
Binion, Department of Medicine, GI Section, UPMC) and lead to
increased symptoms in Crohn’s patients. Specific Aim #3: Model the
strain and stress fields in different geometries of anastomosis,
i.e. end-to-end, side-to-side, and end-to-side, to reveal states of
mechanical instability that would predispose the initiation of
surgical failure. Depending on the anatomy of Crohn’s disease,
surgeons often perform anastomosis instead of HM strictureplasty.
Anastomosis can be end-to-end, side-to-side, or end-to-side.
Side-to-side geometry can create a high resistance zone along the
length of the intestine. This may serve as a point of reversible
obstruction and lead to increased symptoms in Crohn’s patients. The
strain and stress fields in different anastomotic geometries would
be very important in this regard, and therefore should be studied
and modeled separately. I will model the three cases of anastomosis
in ABAQUS using two cylinders with radii r1 = r2 and r1 6= r2. A
multitude of ratios ζ = r1/r2 can be studied (0.8 ≤ ζ ≤ 1.2). The
integrity of all cases of anastomosis will then be tested under
different loading conditions: (A) tension, (B) twist, (C) pressure,
(D) fluid flow and shear, (E) coupling of elastic loads and flow.
The tests will be repeated using patient-specific intestinal
geometries as described in Specific Aim #2.
4.4 Hypothesis #4
Patient-derived anatomic factors, such as length of sigmoid colon,
length of inferior mesen- teric artery and vein, can play a role in
the mechanical stability of low colorectal anastomosis. Specific
Aim #4: Integrate the specific mechanical constraints that
far-field patient anatomy, such as length of sigmoid colon and
mesentery, imposes on the local anastomotic mechan- ical fields.
All above simulations will be integrated to explore the effect of
patient-specific anatomic factors, such as length of sigmoid colon,
length of inferior mesenteric artery and vein, on the mechanical
field of low colorectal anastomosis. The far-field patient anatomy
will be obtained from CT images under IRB-approved protocols. The
3D geometry will then be reconstructed using commercially available
software (IDL, MATLAB, RHINOCEROS, TRUEGRID) and be input in ABAQUS
to be in assembly with the introduced patient- specific intestinal
geometries.
5 Significance and Relevance of the Proposed Research
to Crohn’s Disease
Crohn’s disease is marked by its chronic and at times highly morbid
nature. The past decades have seen wonderful progress in the
medical management of Crohn’s, however, surgical inter- vention
remains a mainstay even at a time when the majority of patients
continue to receive disease modifying treatment post-primary
resection. Certain subsets of highly aggressive
11
Alkiviadis Tsamis
Crohn’s such as the diffusely stricturing disease often require
multiple re-operative interven- tions. It is well appreciated that
every re-hospitalization and especially re-operation carries with
it great morbidity and increasing risk of life-long disability for
the patient. Thirty years ago, pioneering work was done by IBD
surgeons in the United States in using the classic Heineke-Mikulicz
strictureplasty (commonly used for pyloric stenosis in children and
post- vegotomy procedures) to treat Crohn’s strictures in the small
intestine. This bowel sparing procedure decreased the incidence of
short gut syndrome, a dreaded complication in patients with diffuse
Crohn’s. However, disease recurrence remains a problem
post-strictureplasty particularly in tissue distal or proximal to
the prior operation. The challenge of mod- ern surgery and
especially complex gastro-intestinal re-construction is
understanding the inherent biomechanical environment that the new
surgically altered anatomy imposes on surrounding tissue. However,
such understanding necessitates advanced modeling and study using
engineering tools. The primary focus of this grant is building such
a tool set, with a particular focus on Crohn’s re-constructive
surgeries. Imagine the surgeon having at his/her fingertips in the
pre-operative setting a detailed set of simulations among different
possi- ble re-constructions derived using patient-specific anatomic
and physiologic data (CT scans, upper GI studies, pre-albumin
level, existing treatment, etc.). Using these simulations, the
surgeon in discussion with the patient and other members of their
healthcare team could plan out the most appropriate, safest, and
optimal procedure.
6 Facilities Available and Important Collaborations to
Carry Out the Proposed Studies
I strongly believe that the University of Pittsburgh, Department of
Bioengineering, will be an ideal place for me to carry out the
proposed research plan, because it affords me the valuable
experience of interfacing directly with strong clinical
collaborators, yet it demonstrates what it takes to navigate the
barriers that come with multi-disciplinary research. Dr. David Vorp
(Vascular Bioengineering Laboratory) will provide me with
laboratory resources to support the work outlined in the proposed
research plan. In this work I will make use solely of human
intestinal tissue and CT images collected under IRB-approved
protocols. All tissue samples and CT images will be de-identified
through an established process using an honest broker. The human
intestinal tissue and CT images will be provided to me by Dr. Luka
Pocivavsek from the University of Pittsburgh Medical Center, with
whom I have established strong interdisciplinary collaboration
within the frame of the proposed research project. Dr. Pocivavsek
is my Collaborating Principal Investigator. He will provide me with
valuable clinical data, his experience and expertise in IBD
research, and through him I will interact directly with his strong
clinical collaborators, including Dr. Anthony Bauer and Dr. Kenneth
Lee. Further, my current affiliation with the McGowan Institute for
Regenerative Medicine has developed collaboration with Dr. Antonio
D’Amore and Dr. William Wagner. Within the frame of this
collaboration, I will be able to use the biaxial tensile testing
device in Dr. Wagner’s laboratory to measure the material
properties of the human intestinal tissue with Crohn’s disease and
under multiple loading and geometrical constraints.
12
References
[1] Brunicardi, F. C., Andersen, D. K., Billiar, T. R., Dunn, D.
L., Hunter, J. G., Matthews, J. B., and Pollock, R. E., 2009,
Schwartz’s Principles of Surgery, Chapter 22, ”Thoracic Aneurysms
and Aortic Dissection”, McGraw-Hill.
[2] Hurst, R. D. and Michelassi, F., 1998, “Strictureplasty for
crohn’s disease: techniques and long-term results,” World Journal
of Surgery, 22(4), pp. 359–363.
[3] Fichera, A. and Michelassi, F., 2007, “Surgical treatment of
crohn’s disease,” Journal of Gastrointestinal Surgery, 11(6), pp.
791–803.
[4] Fung, Y., 1993, Biomechanics: mechanical properties of living
tissues, Springer-Verlag.
[5] Shiu, Y. T., 2006, Mechanical Forces on Cells. In: Bronzino, J.
D. (Eds.), The Biomed- ical Engineering Handbook: Tissue
Engineering and Artificial Organs, CRC/Taylor- Francis.
[6] Boal, D. and Boal, D. H., 2012, Mechanics of the Cell,
Cambridge University Press.
[7] Tsamis, A., Rachev, A., and Stergiopulos, N., 2011, “A
constituent-based model of age-related changes in conduit
arteries,” American Journal of Physiology-Heart and Circulatory
Physiology, 301(4), pp. H1286–H1301.
[8] Rachev, A. and Gleason Jr, R. L., 2011, “Theoretical study on
the effects of pressure- induced remodeling on geometry and
mechanical non-homogeneity of conduit arteries,” Biomechanics and
Modeling in Mechanobiology, 10(1), pp. 79–93.
[9] Humphrey, J. and Rajagopal, K., 2003, “A constrained mixture
model for arterial adaptations to a sustained step change in blood
flow,” Biomechanics and Modeling in Mechanobiology, 2(2), pp.
109–126.
[10] Liao, D.-H., Zhao, J.-B., and Gregersen, H., 2009,
“Gastrointestinal tract modelling in health and disease,” World
Journal of Gastroenterology, 15(2), pp. 169–176.
[11] Glagov, S., Newman, W. P. I., and Schaffer, S. A., 1990,
Pathobiology of the Human Atherosclerotic Plaque, Springer.
[12] Gregersen, H. and Kassab, G., 1996, “Biomechanics of the
gastrointestinal tract,” Neu- rogastroenterology & Motility,
8(4), pp. 277–297.
[13] Zhao, J., Liao, D., Yang, J., and Gregersen, H., 2010,
“Biomechanical remodelling of obstructed guinea pig jejunum,”
Journal of Biomechanics, 43(7), pp. 1322–1329.
[14] Davis, B. and Rivadeneira, D. E., 2013, “Complications of
colorectal anastomoses: leaks, strictures, and bleeding.” The
Surgical Clinics of North America, 93(1), pp. 61–87.
[15] Chasmar, L. R., 2007, “The versatile rhomboid (limberg) flap,”
The Canadian Journal of Plastic Surgery, 15(2), pp. 67–71.
13
[16] Pocivavsek, L., Efrati, E., Lee, K. Y., and Hurst, R. D.,
2013, “Three-dimensional geometry of the heineke-mikulicz
strictureplasty,” Inflammatory Bowel Diseases, 19(4), pp.
704–711.
[17] Timoshenko, S. P. and Gere, J. M., 1961, Theory of elastic
stability, McGraw-Hill, New York.
[18] Haghpanah Jahromi, B. and Vaziri, A., 2012, “Instability of
cylindrical shells with single and multiple cracks under axial
compression,” Thin-Walled Structures, 54, pp. 35–43.
[19] Putra, I. S., Dirgantara, T., Sucipto, A., and Jusuf, A.,
2006, “Buckling analysis of cylindrical shells having a
longitudinal crack,” Key Engineering Materials, 306, pp.
49–54.
[20] Brighenti, R., 2005, “Buckling of cracked thin-plates under
tension or compression,” Thin-Walled Structures, 43(2), pp.
209–224.
[21] Estekanchi, H. and Vafai, A., 1999, “On the buckling of
cylindrical shells with through cracks under axial load,”
Thin-Walled Structures, 35(4), pp. 255–274.
[22] Shats’kyi, I. and Makoviichuk, M., 2009, “Analysis of the
limiting state of cylindrical shells with cracks with regard for
the contact of crack lips,” Strength of Materials, 41(5), pp.
560–564.
[23] Boudaoud, A., Patrcio, P., Couder, Y., and Amar, M. B., 2000,
“Dynamics of singu- larities in a constrained elastic plate,”
Nature, 407(6805), pp. 718–720.
[24] Tsamis, A., Pocivavsek, L., and Vorp, D. A., 2013, “Elasticity
and geometry: a compu- tational model of the heineke-mikulicz
strictureplasty,” Inflammatory Bowel Diseases, submitted.
[25] Tsamis, A., Pocivavsek, L., and Vorp, D. A., 2012, “Effect of
geometry on wall stresses in a computational model of the
heineke-mikulicz strictureplasty,” Proceedings, 2012 Annual Meeting
of the Biomedical Engineering Society. Georgia World Congress
Center, Atlanta, Georgia.
[26] Kono, T., Ashida, T., Ebisawa, Y., Chisato, N., Okamoto, K.,
Katsuno, H., Maeda, K., Fujiya, M., Kohgo, Y., and Furukawa, H.,
2011, “A new antimesenteric functional end- to-end handsewn
anastomosis: surgical prevention of anastomotic recurrence in
crohn’s disease,” Diseases of the Colon & Rectum, 54(5), pp.
586–592.
[27] Munoz-Juarez, M., Yamamoto, T., Wolff, B. G., and Keighley, M.
R., 2001, “Wide- lumen stapled anastomosis vs. conventional
end-to-end anastomosis in the treatment of crohn’s disease,”
Diseases of the Colon & Rectum, 44(1), pp. 20–26.
[28] Greenstein, A. J., Zhang, L. P., Miller, A. T., Yung, E.,
Branco, B. C., Sachar, D. B., and Greenstein, A. J., 2009,
“Relationship of the number of crohn’s strictures and stric-
tureplasties to postoperative recurrence,” Journal of the American
College of Surgeons, 208(6), pp. 1065–1070.
14
Previous work by Tsamis et al. tsamis2013strictureplasty,
tsamis2012bmes
Detailed Research Plan