Embed Size (px)
Citation preview
Gastrointestinal
Solving the Puzzle:
Respira
tory
Psychosocial
Diabetes
CF Clinical Research
• Needs
• Active Studies
• Opportunities
• “Personalized” Care
Undernutrition
Pandora’s BoxChris Landon M.D FAAP, FCCP.Pediatric Diagnostic CenterVentura, California
CF Clinical Research 2001
CF Clinical Research Needs
• “Better” Clinical Trials - Series of Cochrane Library reports- Cheng et al. Pediatr Pulmonol, 2000
• Research Mandates - Adequate power - Appropriate duration - Meaningful outcome measures - Multicenter design
- Account for individual variation
• Rapid Testing of New Treatments- Clinical trial networks
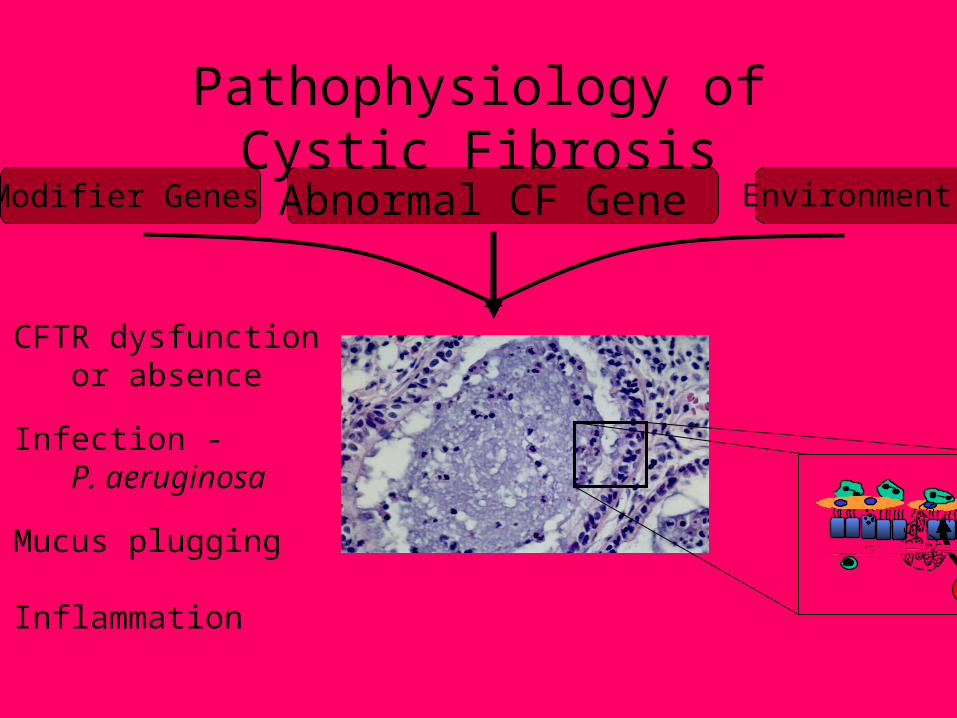
Modifier Genes
• CFTR dysfunction or absence
• Infection - P. aeruginosa
• Mucus plugging
• Inflammation
Abnormal CF Gene Environment
Pathophysiology of Cystic Fibrosis
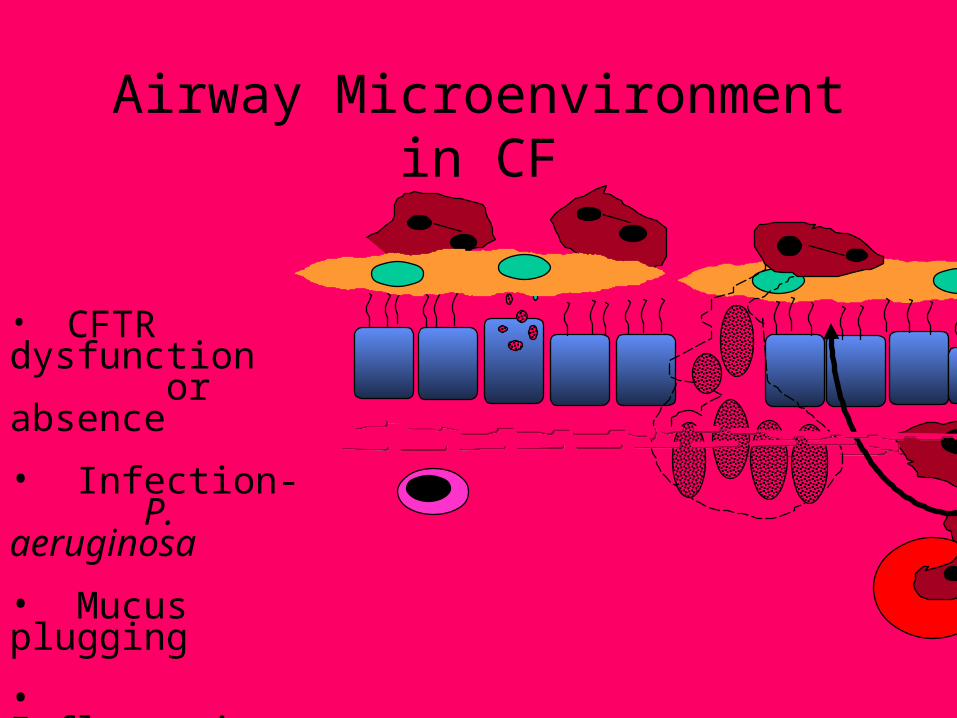
• CFTR dysfunction or absence
• Infection- P. aeruginosa
• Mucus plugging
• Inflammation
Airway Microenvironment in CF
• Inhaled tobramycin - Tobi® (Pathogenesis/Chiron)- Compelling results from follow-up of multicenter trials
• RSV vaccine - (Wyeth-Lederle, P. Hiatt et al)- Multicenter trial
- Potential for short and long term reduction in morbidity
• Dextran - (D. Speert et al) - Multiple actions including - Interference with Pseudomonas attachment to epithelium.
• Xylitol - (J. Zabner et al)- 5 carbon sugar, improves antimicrobial properties of
airway surface liquid.
Improving Antimicrobial Activity in the CF Airway
• Airway Secretion Clearance Study (American Biosystems Inc., CFF)
- Comparison of Conventional Chest Physical
Therapy, Flutter Device, and High Frequency Chest Wall Oscillation
- 22 centers
• Inhaled Hypertonic Saline - Disrupts ionic bonds in airway secretions- Multicenter trial in Australia (P. Bye et al.)
• Purinergic Agonists - (Inspire Pharmaceuticals Inc.) - Activate alternative chloride channel- Increase ciliary activity- Phase I trial (P. Noone et al.)
Improving Mucociliary Clearance in CF
• Dornase alfa - Pulmozyme® (Genentech Inc.)- Does early administration of rhDnase slow the decline in lung function?- Multicenter, International trial
• Elastase inhibitors- Recombinant alpha-one-antitrypsin (PPL Therapeutics plc) - DMP 777 - specific intracellular inhibitor- rMNEI - Monocyte/Neutrophil Elastase
Inhibitor (CBRI)
Modulating Airway Inflammation in CF
• Treatment of stop mutations - (Wilschanski et al.)- Aminoglycoside treatment (e.g. gentamicin) overcomes stop mutations e.g. G542X
• Correcting trafficking defects - (P. Zeitlin et al)- Short chain fatty acids can assist trafficking
through endoplasmic reticulum- Aimed at F508 mutation
Correcting CFTR Dysfunction
• Lipid abnormalities in CF (S. Freedman and J. Alvarez) - AA is increased in CF cells - DHA is decreased in CF cells
- AA is pro-inflammatory- DHA treatment in murine models protects against lung infection.
• Lipid abnormality confirmed in:- Murine models- Tissue culture- Human epithelial cells
• Lumarel® (Genzyme, Inc.) – no longer under development
DHA (Docosahexanoic acid) in CF
• Acquisition of P. aeruginosa- Early intermittent colonization with different strains- Later, one predominant strain
(J. Burns et al., Multicenter BAL trial; P. Farrell, M. Rock et al. Wisconsin studyD. Armstrong et al.)
• Early Diagnosis through Newborn Screening - Improves growth and nutrition - Avoids complications of infancy
(P. Farrell et al.)
• Link Between Early Impaired Growth and Later Decreased Pulmonary Function.
(W. Morgan, and the ESCF)
Early Treatment in CF
• CF Related Diabetes- Improved definition (A. Moran et al.)- Links to lung disease (C. Milla et al.)
• CF Liver Disease- Guidelines (R. Sokol et al.)- Modifier genes (K. Friedman et al.)
• CF Bone Disease- Diagnosis and treatment (R. Aris et al.)
• Adult Centers- Reproduction- Psychosocial stresses
CF Clinical Research andComprehensive Care
+ =
• Genomics - Microarrays
• Proteomics
. . . .
. . . .
. . . .
. . . . . . . . . . . . .. . . . . . . . .
• Modifier Genes
• Pathways of Injury
• Individual Variation
• New Treatments
• Individual Treatment Approaches
Towards “Personalized” CF Care:Genomics and Proteomics
• New treatments are being added to the regimen
~ time
~ complexity
• Need to Measure Adherence
~ new electronic monitors (Doser, Nebulizer Monitor)
~ daily diary measure
• Include Quality of Life as Secondary Outcome
Advances in CF Treatment
Pandemonium - All The Demons
• Physician• Clinical Nurse Specialist• Dietitian• Respiratory Therapist• Physical Therapist• Pediatric Pulmonologist• Adult Pulmonologist• Pharmacist
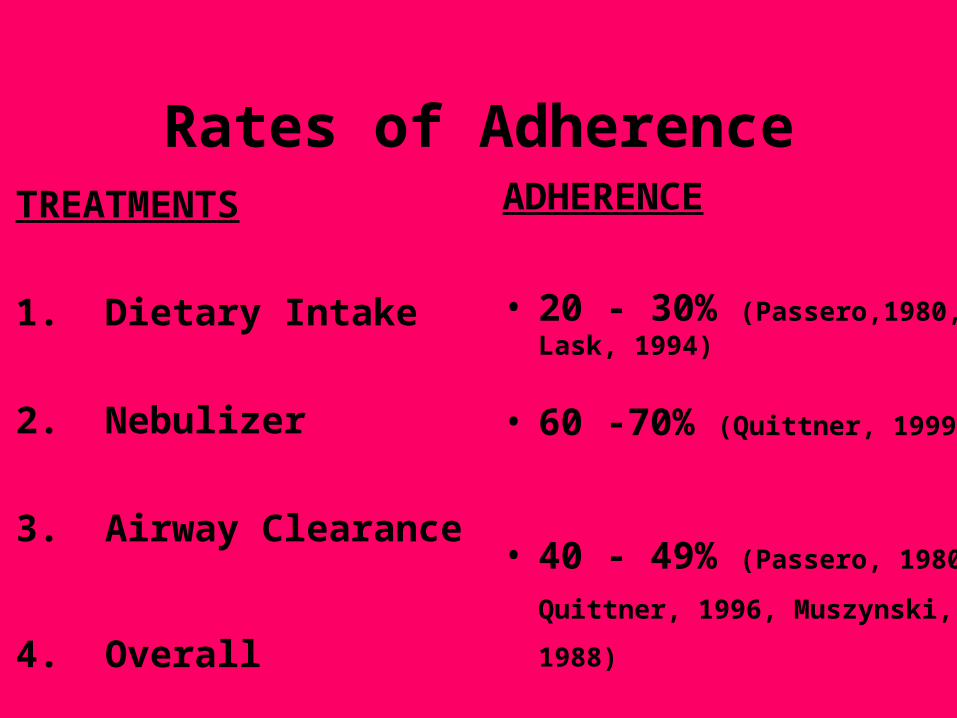
TREATMENTS
1. Dietary Intake
2. Nebulizer
3. Airway Clearance
4. Overall
ADHERENCE
• 20 - 30% (Passero,1980, Lask, 1994)
• 60 -70% (Quittner, 1999)
• 40 - 49% (Passero, 1980,
Quittner, 1996, Muszynski, 1988)
• 50% (Gudas , 1991)
Rates of Adherence
Pre, Post, 6, 12, & 18 Months:
1. Improved Adherence to:
~ Nebulized Treatments
~ Metered Dosed Inhalers
~ Airway Clearance
~ Enzymes
2. Reduced Morbidity (Days in hospital, IV’s)
3. Reduced Family Conflict
4. Increased Quality of Life
Outcome Measures
Mob Action
Peer Pressure in the Bacterial World
• (N. Hoiby and J. W. Costerton)• What is a Biofilm?
- A structured community of bacterial cells enclosed in a self-produced polymeric matrix.
- Biofilms are a protective mode of growth that allow survival in hostile environments.
- Bacteria in biofilms are inherently resistant to killing.
Hypothesis: P. aeruginosa infections of the CF lung are biofilm infections
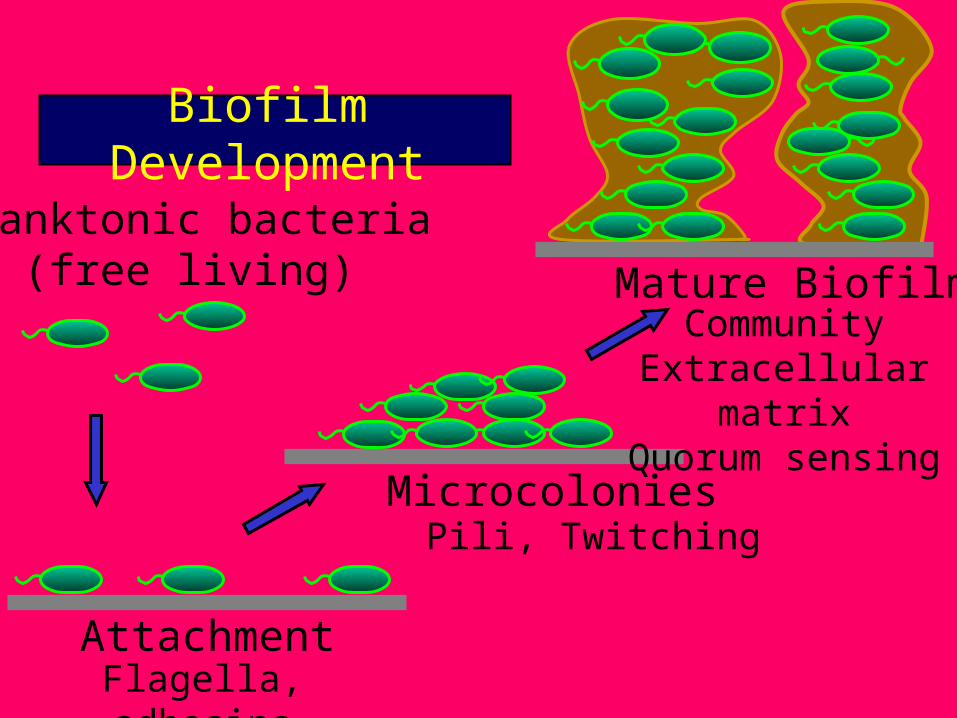
Planktonic bacteria(free living)
AttachmentFlagella, adhesins
MicrocoloniesPili, Twitching
CommunityExtracellular matrix
Quorum sensing
Mature Biofilm
Biofilm Development
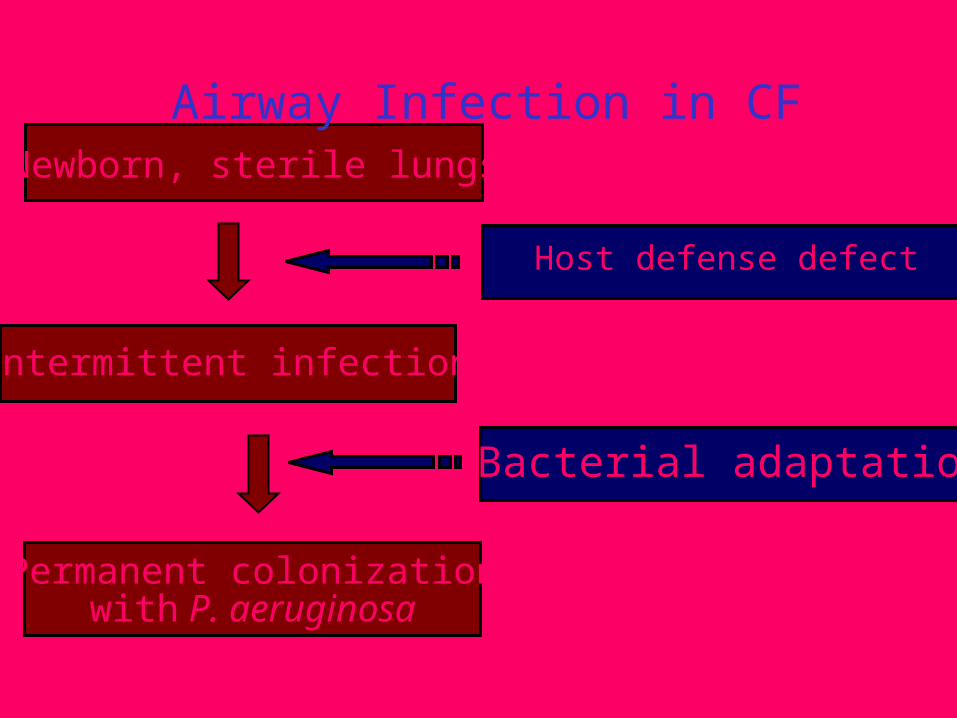
Newborn, sterile lungs
Permanent colonizationwith P. aeruginosa
Intermittent infection
Bacterial adaptation
Host defense defect
Airway Infection in CF
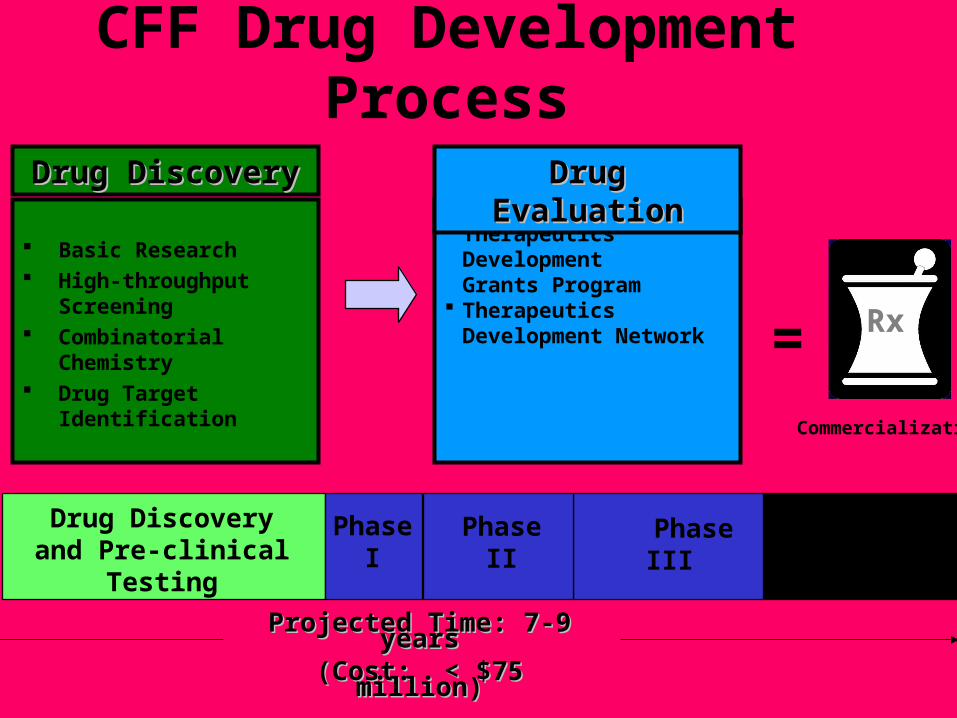
Basic Research High-throughput
Screening Combinatorial Chemistry Drug Target Identification
Drug DiscoveryDrug Discovery
Commercialization
= Rx
Therapeutics DevelopmentGrants Program
TherapeuticsDevelopment Network
Drug EvaluationDrug Evaluation
Drug Discoveryand Pre-clinical
Testing
Projected Time: 7-9 yearsProjected Time: 7-9 years(Cost: < $75 million)(Cost: < $75 million)
PhaseIII
Submission and
Approval
PhaseII
PhaseI
CFF Drug Development Process

Plasmin DNA Complexes Copernicus Gene System, Inc.
CPX SciClone Pharmaceuticals, Inc.
Moli1901 (Duramycin) Molichem Medicines
Inositol induced chloride secretion Inologic, Inc.
Long-acting Sodium Channel blocker CYFI, Inc.
Anti-Protease Therapy Center for Blood ResearchTyloxapol Discovery Laboratories, Inc.P-113: antimicrobial peptide PeriodontixPa 1806 PathoGenesis Corporation
Acid-stable digestive enzyme therapy Altus Biologics, Inc.Other
AbnormalGene
AbnormalProtein
Altered IonTransportAbnormalMucousSecretion
Infection &InflammationTissueDestruction
Therapeutics DevelopmentProgram Grants
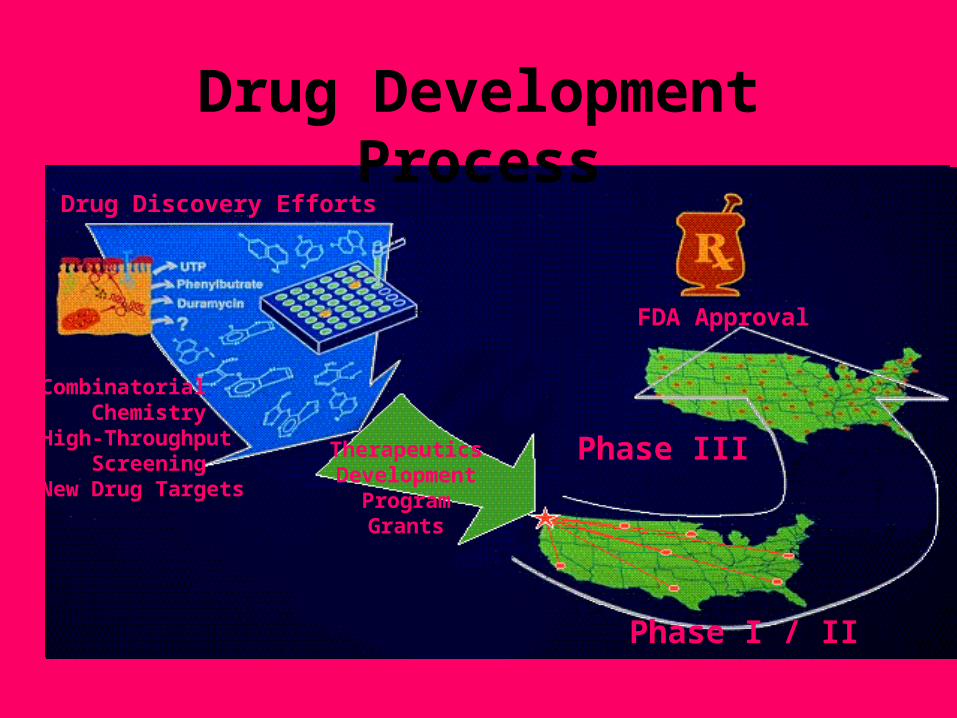
FDA Approval
Phase III
Phase I / II
Drug Discovery Efforts
Combinatorial ChemistryHigh-Throughput ScreeningNew Drug Targets
TherapeuticsDevelopment
ProgramGrants
Drug Development Process
CF Clinical Research
• Needs
• Active Studies
• Opportunities
• “Personalized” Care
ClinicalResearch
Basic ResearchGenomicsProteomics
Center Care
?
?
Solving the Puzzle