Embed Size (px)
DESCRIPTION
Citation preview

Application of Pharmacogenomics To Personalised Medicine and R & D
Dr Harsukh ParmarGlobal Discovery Medicine
Respiratory & Inflammation Therapy [email protected]

U.S. Drug Industry R&D Expenditures and Drug Approvals, 1963-2000
U.S. Drug Industry R&D Expenditures and Drug Approvals, 1963-2000
0
20
40
60
1963
1965
1967
1969
1971
1973
1975
1977
1979
1981
1983
1985
1987
1989
1991
1993
1995
1997
1999
NC
E A
ppro
vals
0
9
18
27
R&
D Expenditures
(Billions of 2000$)
Source: Tufts CSDD Approved NCE Database, PhRMAR&D expenditures adjusted for inflation
R&D Expenditures
NCE Approvals

Main Reasons for Termination of Development LACK OF EFFICACY & SAFETY !
One Size Does NOT Fit ALL !Toxicology
19.4%
Other6.2%
Various10%
Clinical Efficacy22.5%
PortfolioConsiderations
21.7%
Clinical Safety20.2% Clinical
Pharmacokinetics/Bioavailability
3.1%
Preclinical efficacy3.1%
PreclinicalPharmacokinetcs/
Bioavailability1.6%
Formulation0.8%
Patent or CommercialLegal0.8%
Regulatory0.8%


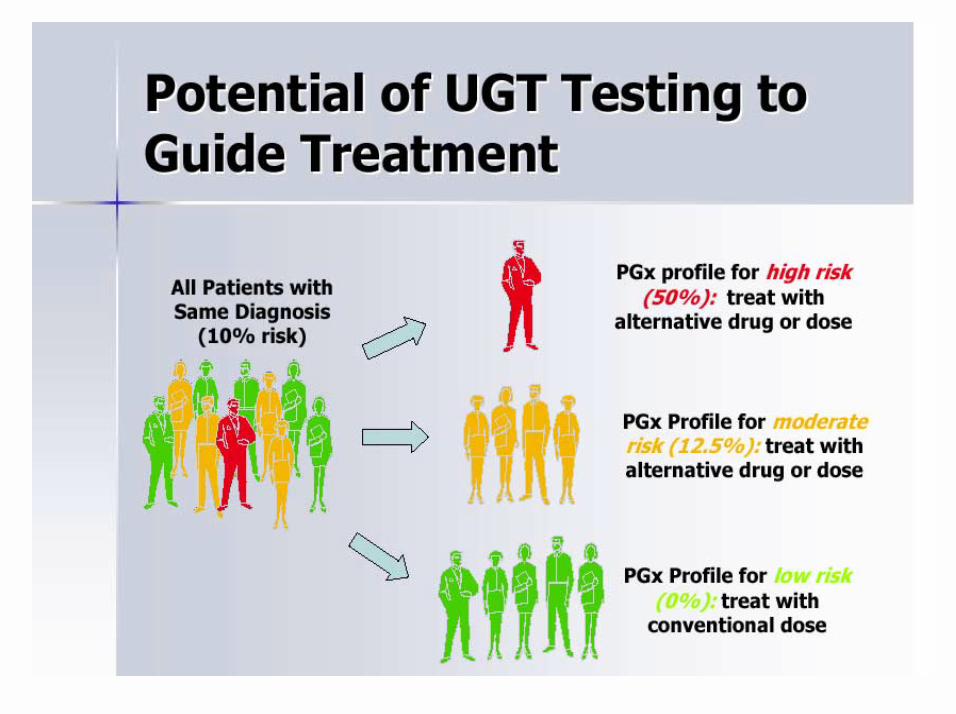
The co-existence of genetic polymorphisms in drug metabolizing enzymes, targets, receptors, and transporters, in the context of drug and non-drug influences, may result in high frequencies of unusual drug reaction phenotypes.

Current Treatment is Population Based

What is Personalised Medicine?Personalised Medicine links the patient to a disease (segment or part of the disease) to a drug using a diagnostic or biomarker orclinical test that:
• Defines the disease and/or• Predicts response and risk and/or• Determines dose
Leading to improved patient outcomes, targeted therapies and newcommercial opportunities. Personalised Medicine involves testing patients prior to treatment to enable clinicians to prescribe:
• The Right Drug• At the Right Dose• For the Right Disease• To the Right Patient

Pharmacogenomics –Making Personalised Medicines

Patient Segmentation is Not New
•Historically we have always done this usingClinical and Biochemical features:
!Inclusion/Exclusion Criteria in ClinicalTrials
!Regulatory Approved Data sheets oftendefine the approved indications andsubset of patients suitable for theapproved therapy

•The vast array of technology to define patient subgroups•These range from biochemical, immunocytochemistry,genetics, proteomics, to new evolving technology such asreal time chemotaxis assays•Molecular re-classification of disease through genotype•Better understanding & use of biomarkers for patientstratification•Better understanding & use of biomarkers for patient segmentation & enriched clinical trials•Greater societal expectation on efficacy and safety•Increasing costs leading to better targeted therapies
So What Has Changed ?

Pharmacogenomics Promise
•New diagnostic procedures (pharmacogenomic tests)
•Better matches between patient, disease, therapy and outcome
•Impact on R&D as well as Sales and Marketing
Individualized Medicine


• BMS - Taxol: first cancer blockbuster, now facing generic competition
• Novel taxane about to enter market
• Beta-tubulin gene contains mutations that predict for patterns of response and resistance
• Beta-tubulin pharmacogenomic test for differential prescription:Taxol or taxane
0
10
20
30
40
Wild-TypeN=33
MutatedN=16
Taxol Response rate(%)Median survival(months)
Genotype
NSCLC treatment with TAXOL
2
10
39
0
Importance is clear and growing

20/04/2005 15
Discovery MedicineUtilize and Integrate Human
Pathophysiology and Disease Models
Annots
GO
Prot
einD
omai
n
Cyt
oban
d
NS
HS
CO
PD0
15 19 18 9 16 2
CO
PD1
CO
PD2
NA
•Validated targets•Pathophysiologicalunderstanding•Biological Mechanism•Disease stratification•Biomarkers•Patient segmentation
Platforms•Genetics•Genomics•Proteomics•Metabonomics•Lipidomics•Glycomics•Imaging•Epidemiology•Physiology Bioinformatics and Informatics
Clinical DataTarget Validation
Deliverables


Rheumatoid Arthritis

GENE EXPRESSION ANALYSIS USING GENELOGIC DATA

!Pathways that are significant to the pathophysiology of
Rheumatoid Arthritis and Anti-TNF treatments have been
highlighted in the table.
!Knowledge of immune response genes can potentially be
useful for identification of surrogate markers of clinical endpoint
or disease/treatment/response markers according to the project
needs.
GenelogicTM Expression Data

Overview of Analysis• Gene expression data from three types of sample
populations analyzed:
!WBC samples from Normal individuals!WBC samples from Rheumatoid Arthritis patients.!WBC samples from RA patients, 6 weeks after
Remicade Infusion.
• Set of 25 genes were identified as a marker set for patient stratification in future novel NME target discovery and development.

Micro-array Analysis in RA-Treated with Steroids• Analysis of covariance. The
distribution of p-values allowed identification of genes with altered gene expression on steroids.
Experimental MedicineDr H Parmar
CD68100x
pre post
prednisolone
placebo
CD68 Immunohistochemistry

Biomarkers of disease progression
COPD

Gene ontology
annotation
campaign (GOAC)FEV1/FVC ratio
Brushings (bronchial epithelial cells)
Microarrays Microarrays
Identify differentially expressed genes
Identify differentially expressed genes
Functional assaysCytokine production
Differentiation, ProliferationSecretion, Motility
Candidate Targets Candidate Targets
Define the biochemical pathways initiated by COPD related stresses•Smoke (CSE)
Primary cell-based model
Non-smokers
Smokerswith/without
COPD
Bronchial biopsies
Bioinformatics&
Statistical analysis
IHC/in situ
Confirm expression in in disease tissue
Confirm expression in in disease tissue
Clinical data
Generate hypotheses, identify targetable
molecules in pathways
Generate hypotheses, identify targetable
molecules in pathways
Analysis of Epithelial Gene Expression in COPD

Annots
GO
Prot
einD
omai
n
NAMEnuclear factor of kappa light polypeptide gene enhancer in B-cells 2 (p49/tubulin, gamma 1carboxylesterase 1 (monocyte/macrophage serine esterase 1)carboxyl ester lipase (bile salt-stimulated lipase)cholesterol 25-hydroxylaseSPARC-like 1 (mast9, hevin)low density lipoprotein receptor (familial hypercholesterolemia)prostate stem cell antigencarboxypeptidase Egastrin-releasing peptidefer-1-like 3, myoferlin (C. elegans)killer cell lectin-like receptor subfamily C, member 3DEAD/H (Asp-Glu-Ala-Asp/His) box polypeptide, Y chromosomeribosomal protein S4, Y-linkedkiller cell lectin-like receptor subfamily C, member 3small inducible cytokine A5 (RANTES)small inducible cytokine A5 (RANTES)secreted phosphoprotein 1 (osteopontin, bone sialoprotein I, early T-lympsecreted phosphoprotein 1 (osteopontin, bone sialoprotein I, early T-lympCluster Incl. AF070536:Homo sapiens clone 24566 mRNA sequence /cdS100 calcium binding protein A10 (annexin II ligand, calpactin I, light polymucin 1, transmembranealdehyde dehydrogenase 1 family, member A3cytochrome P450, subfamily I (aromatic compound-inducible), polypeptidcytochrome P450, subfamily I (dioxin-inducible), polypeptide 1 (glaucomacytochrome P450, subfamily I (dioxin-inducible), polypeptide 1 (glaucomaannexin A3transmembrane 4 superfamily member 1transcobalamin I (vitamin B12 binding protein, R binder family)cystatin A (stefin A)uroplakin 1BS100 calcium binding protein Pclaudin 10carcinoembryonic antigen-related cell adhesion molecule 5carcinoembryonic antigen-related cell adhesion molecule 6 (non-specific carbonyl reductase 1UDP glycosyltransferase 2 family, polypeptide Bubiquitin carboxyl-terminal esterase L1 (ubiquitin thiolesterase)hypothetical protein MGC13523Pirinaldo-keto reductase family 1, member B10 (aldose reductase)malic enzyme 1, NADP(+)-dependent, cytosolicglutathione peroxidase 2 (gastrointestinal)phosphogluconate dehydrogenasethioredoxinaldo-keto reductase family 1, member C1 (dihydrodiol dehydrogenase 1; alcohol dehydrogenase 7 (class IV), mu or sigma polypeptidetransaldolase 1aldo-keto reductase family 1, member C3 (3-alpha hydroxysteroid dehydNAD(P)H dehydrogenase, quinone 1
Cyt
oban
d
Disease progression cluster (Gene Expresion)(GOLD 0,1 &2; decreasing FEV1)
NS
HS
CO
PD0
15 19 18 9 16 2
CO
PD1
CO
PD2
NA
• Hierarchical clustering of genes• Subjects ordered in disease progression• N=79, Expression data from U133A&B

Human Knock-Out Initiated Projects, Entered Phase III





Disease reclassification at the molecular level

!Genes distinguishing ALL from AML The 50 genes that correlate most highly between ALL and AML are shown.
!The top panel shows genes that are highly expressed in ALL, whereas the bottom panel shows genes more highly expressed in AML.
!While as a group, these genes are correlated with pathologic class, no single gene is uniformly expressed across the class, illustrating the value of whole-genome expression analysis in class prediction
Molecular classification of Acute LeukaemiaGolub TR et al. Science 1999; 286: 531









Nanosphere, Inc - Novel technology detects human DNA mutations


Speed and Simplicity
Since it is based on direct genomic detection and not target amplification, ClearRead makes molecular testing faster and simpler. Current methods require highly specialized scientists and lab technicians for processing and interpretation, while ClearReadassays are easy to perform and produce definitive results.
Verigene Mobile
!The next generation Verigene Mobile will transfer the power and accuracy of the Verigene AutoLab to an affordable, hand-held device.
!Its portability will make it ubiquitous at point-of-care settings such as doctor's offices, hospital bedsides and even in patients' homes.



Herceptin






Drugs with Personalised Medicine Properties/Potential
•Herceptin in Oncology •Protease Inhibitors in HIV•Protease Inhibitors in HCV•Diabetic Treatment & Monitoring•Neuroamidase Inhibitors in Influenza e.g. Tamiflu, Relenza•Rituximab, Anti-CD20 in NHL, RA etc•Xolair, Anti-IgE in asthma•Anti-TNF’s & Anti-IL1 in RA•Campostar in Oncology•Xeloda, Gemcitabine, Velcade in Oncology•Taxol & Taxanes in Oncology•UDF in Oncology•EGFR Antibodies & TK inhibitors e.g. Tarceva, Iressa•Potentially VEGF Antibodies (Avastin) and TK inhibitors•Various Monoclonal Antibody Targets