Embed Size (px)
Citation preview
7th November 2018
Lyudmil NinovEPF Project Officer
Personalised Medicine:
A Cross-Disease Patient Perspective
Stanhope Hotel, Brussels, Belgium

About us:• Umbrella across chronic
diseases
• Founded in 2003
• Independent, non-governmental
• Focus on EU-level
The European Patients’ Forum
Our Vision!
“All patients with chronic conditions in Europe have equal access to high quality, patient-centred health and related care.”
Our Mission!“To be the collective, influential patient voice in European health and related policies and a driving force to advance patient empowerment and patient access in Europe.”

• Right to healthcare based on individual needs – not “one-size-fits-all”
• Tailored solutions integrated as part of a holistic approach – treating the person, not the disease
• In this sense, all medicine should already be personalised – BUT
• PM as now understood (i.e. medicine using genomic and other molecular information) adds a vital building block to realising a truly holistic approach towards individualised medicine
All health care should be personalised
Definition of PM by EUPATI:
“a medical model that proposes to customise medical decisions, practices
and treatments for the individual patient. It uses targeted medicines
aimed at specific molecules that are involved in the patient’s disease and takes genetic, clinical, environmental and lifestyle information about the patient into account. The aim is to
select the best therapies for the individual patient to ensure the best
outcome and reduce risk of side effects.”

• Everyone has an individual molecular profile → treatment could be optimised without need for “trial and error” in “one size fits all” model
• The concept of disease itself is changing – e.g., “cancer” is no longer one disease
• This is a complete paradigm shift in science from organ-based definition of disease to molecular mechanisms
• Personalised prevention – the “ultimate” personalised medicine?
The promise of PM
Expectations from PM:
- Personalised prevention strategies:
- How not to become a patient at all?
- Life style changes
- Preventive interventions…
- Accurate and earlier diagnosis
- The “right treatment” in the “right dose” at the “right time” for each patient
- Fewer side effects
- Accurate dosing based on knowledge of individual metabolism
- Avoiding ineffective treatments (“non-responders”)
- More certainty that a given treatment will work “for me”

• Health literacy – accurate, up-to-date, unbiased information on evidence-base, benefits and risks
• A new patient-professional relationship & participatory care
• Having meaningful conversations that enable meaningful decisions
• Equitable access to prevention, diagnosis and treatment
Challenges of personalised medicine
As well as promise and hope, PM also presents questions and challenges for patients
So
urc
e: C
ori
ell
Pe
rso
nal
ize
d M
ed
icin
e C
olla
bo
rati
ve

• Scientific developments in medicine are increasingly complex to communicate
• Information overload, mis- and disinformation (media coverage, Dr Google…)
• Patients look for answers everywhere
Health literacy implications of PM
Today's paradox: people are asked to take more responsibility for their health –but we must make choices in an ever-more complex context
• PM will only achieve its true potential if patients understand their options!
• Accurate, evidence-based, easy to understand and relatable to each individual’s situation
HLS-EU survey: around half of Europeans have inadequate health literacy

• Professionals need to be trained – how many GPs/specialists know about enough about PM or genomics to discuss meaningfully with patients?
• Shared decision-making is not “optional” any more, but vital!
HCP education and training, attitudes need to reflect this
Meaningful conversations
PM necessitates a fundamental shift in medical culture, professional and patient roles: from paternalistic to participatory
✓ HCPs need to understand personalised medicine
✓ HCPs need to embrace patient empowerment and be skilled in communication and participatory care
Patients need access to high-quality, relevant information
✓ Online information
✓ Decision aids

• How clinical evidence is presented can affect thepatient’s perception of benefits and risks (harms)
• Patients must have full understanding of the evidenceto make informed choices
– People fear the wrong things (bathtubs vs. sharks)
– Patients (and physicians) overestimate benefits andunderestimate risks of medical interventions
– Patients’ preferences & tolerance of risk can be differentto professionals
• Well-chosen and clearly designed visual aids can help enhance understanding of text
• Uncertainties of medical tests need to be communicated accurately
Communicating benefits/risks
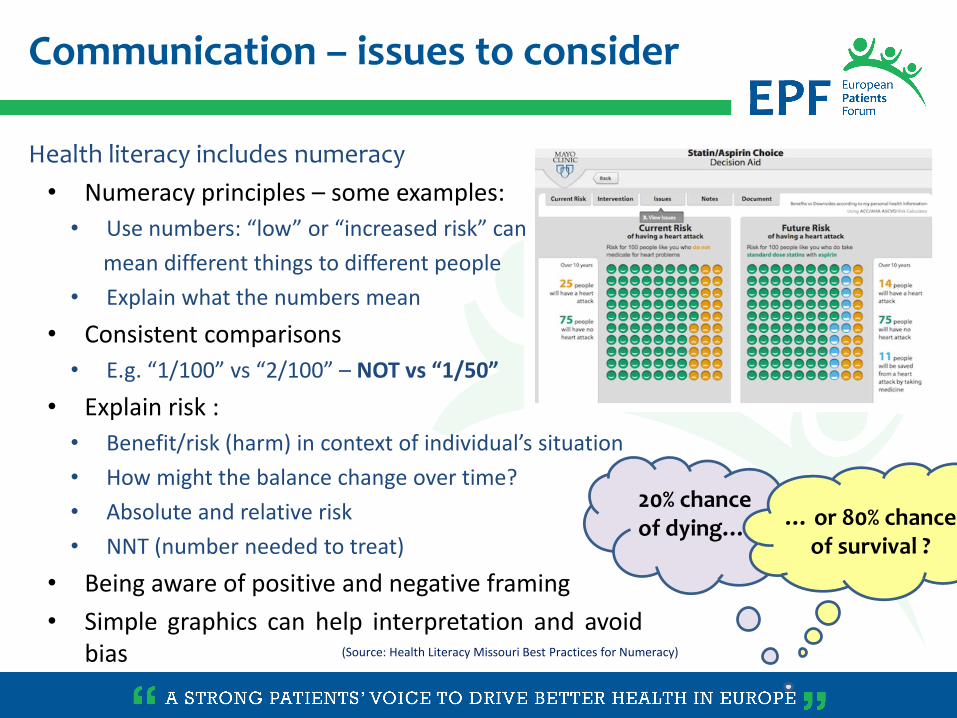
Communication – issues to consider
(Source: Health Literacy Missouri Best Practices for Numeracy)
20% chance of dying… … or 80% chance
of survival ?
Health literacy includes numeracy
• Numeracy principles – some examples:
• Use numbers: “low” or “increased risk” can
mean different things to different people
• Explain what the numbers mean
• Consistent comparisons
• E.g. “1/100” vs “2/100” – NOT vs “1/50”
• Explain risk :
• Benefit/risk (harm) in context of individual’s situation
• How might the balance change over time?
• Absolute and relative risk
• NNT (number needed to treat)
• Being aware of positive and negative framing
• Simple graphics can help interpretation and avoidbias

• We are not there yet – evolution, not quite “revolution”
• Communication challenges:
– Danger of over-hyping modest advances by media – raised expectations, false hope
– Patient/lay-friendly information urgently needed
– Having the data =/= knowing what it means, let alone knowing what action should be taken
– Sometimes tests fail to provide answers or provide unexpected answers → learning how to deal with uncertainty, variations of unknown significance, incidental findings
– Risk of over-medicalisation / genetic determinism
Reality check
“There’s very little research on the
impact of uncertain results on
families yet – the technology is
just too new”
– The Guardian -

• Patients want and have a right to be involved in decisions about their treatment – including prevention
• Patients need to understand the benefits and risks (harms) of different options – including option to do nothing
• Good communication about benefits and risks/harms is needed to help patients assess their options and make informed choices according to their values and preferences
Conclusions (I)

Conclusions (II)
• HCPs need training on personalised medicine
• HCPs need training on communication with patients
• Patients need communication & education strategies to increase awareness and health literacy
– Different target audiences with different needs (“patient experts” to general public)
• When genetic testing offers a “substantial and quantifiable risk estimate” and when meaningful prevention action can be taken, testing should be made available
– Important to give information and communicate in an ethical and sensitive manner
– Professional genetic counselling should be available to patients and family members

Thank you!
From ‘doing to’ … to doing (better) with patients
From “patient-centred” healthcare … to participatory healthcare

/europeanpatientsforum
/eupatientsforum
More [email protected]
THANK YOU FOR YOUR ATTENTION!
Follow us on Social Media!
/eupatient
eu-patient.eu/blog





























