Embed Size (px)
Citation preview

Pain, 35 (1988) 155-169
Elsevier
155
PAI 01291
Personalised evaluation of self-hypnosis as a treatment of chronic pain: a repertory grid analysis
Robert G. Large * and Frances R. James * *
Departments of * Psychiatry and Behavioural Science and * * Psychology, University of Auckland, and Pain Clinic,
Auckland Hospital, Auckland (New Zealand)
(Received 16 December 1988, revision received and accepted 19 May 1988)
SummarY Self-hypnosis was taught to 5 highly hypnotisable patients referred to Auckland Hospital Pain Clinic. Evaluation
included the Illness Self-Concept Repertory Grid (ISCRG) and follow-up was at 1 and 6 months post treatment. Consensus grids
indicated the subjects initially identified with physical illness but this association decreased over the course of the study. There
appeared, therefore, to be a shift in self-concept away from physical illness, in association with the learning and practice of
self-hypnosis. This change was especially evident in the grids of those subjects who experienced the most pain relief.
An association between pain reduction and self-concepts is thus noted. This study does not identify whether self-concepts merely
reflect therapeutic change or whether strong self-identification with physical illness indicates a poor prognosis for pain relief. This is a
question which deserves further study.
Key words: Self-hypnosis; Personal&d evaluation; Chronic pain; Grid analysis
Introduction
The role construct repertory grid was devised by George Kelly [6] as a means of exploring an individual’s view of the world. Grid technique has since been adapted to a variety of purposes and good overviews of this literature are provided by Bannister and Fransella [l] and by Beail [2] in- cluding some discussion on the validity and relia- bility of repertory grids.
A form of the repertory grid has been used in Auckland to explore self-concepts in patients with chronic pain, viz., the Illness Self-Concept Reper-
Correspondence to: Dr. R.G. Large, Dept. Psychiatry and Behavioural Science, School of Medicine, University of Auck-
land PB, Auckland, New Zealand.
tory Grid (ISCRG), which is described in 2 previ- ous papers. The distance between ‘self’ and ‘ideal self concepts predicted outcome in a trial of EMG feedback [7] and self-concepts shifted in associa- tion with a pain management programme utilising education and cognitive-behavioural techniques
PI. In this study we were interested in tracking
shifts in self-concepts associated with self-hypno- sis (SH) training. Further details of the design and execution of the study are described in a compa- nion paper [4]. Hypnosis has been said to alter an individual’s emotional reaction and attitude to- wards pain [3,9] and the ISCRG is a sensitive instrument in defining attitudes towards the self and towards illness.
03043959/88/$03.50 0 1988 Elsevier Science Publishers B.V. (Biomedical Division)

150
TABLt I
SUBJt’(‘T DETAILS
Subject Sex Age Location Duration SHC’S of pal” of pain
(years)
I RG F 45 L. chest I 5 2 K<; F 21 L. head 1 4 3 PD M 31 R. shoulder 10 5 4DM F 22 R. knee I 5 5 IC‘ M 51 Low back 5 5
___
Methods
A series of 28 new patients at Auckland
Hospital Pain Clinic were assessed using the Stan-
ford Hypnotic Clinical Scale (SHCS) [ll]. Five were selected for high hypnotisability, clinical sui- tability and interest in learning self-hypnosis. Each subject had tried other forms of treatment in-
cluding medication, acupuncture, physiotherapy and a wide range of alternative therapies. Subject details are presented in Table I. Apart from sub- ject 2, who saw a local electro-acupuncturist, none of the patients had any other therapy apart from
learning self-hypnosis during the course of the
study.
Subjects 1, 3 and 5 had chronic musculoskeletal pain, otherwise not specified. Subject 2 had con-
stant left parietal headache for which no cause
could be found, and subject 4 had a post-trau- matic neuralgia. All subjects were judged to have
psychological factors affecting their physical con- dition, but no other psychiatric diagnosis.
The purpose of this study was to attempt con- trolled clinical assessment of the use of self-hyp- nosis in the management of chronic pain per se. We therefore selected from a consecutive series of patients attending the clinic for the first time with chronic non-malignant pain regardless of diagno- sis. We preferred to apply the most appropriate treatment programme for each individual, as we wished to test the utility of hypnosis as it is applied in the field, rather than a standardised treatment package. Consequently, single-case de- sign was most appropriate to this study; to allow individual variation in treatment strategy to exist,
aud he controlled for [14]. Specificity of effect MX~ ttvaluated by using a hatterc of questionnaires in addition to daily pain. medication and sleep rcc- ords and interview data.
Treatment was administered in the context of a multiple baseline design across subjects with a delay of 1 week between subjects. The advantages of single-case designs in clinical research and the
range of designs available are discussed in Kazdin
151. All patients were seen by the same therapist (RGL) who worked individually with each person
to arrive at a suitable self-hypnosis strategy for
each to use in their own time. The average length of treatment was 5.2 one hour sessions, with a 1
month follow-up. Two of the patients were taught
the technique of glove anaesthesia. two used rc- taxation techniques and the final subject used
distraction imagery. Assessment included questionnaires. daily mea-
sures and interview findings. Research interviews
were conducted independently of the therapist by the researcher (FRJ) and consisted of the McGill Pain Questionnaire (MPQ) [lo], the Health Locus of Control survey (HLC) [13] and the Illness Self- Concept Repertory Grid (ISCRG). Interviews oc- curred prior to treatment. and at the end of the treatment phase with follow-up at 1 and 6 months
post treatment. The MPQ was also completed at the initial assessment for inclusion in the study.
Subjects were asked about the effect of pain on their daily life. Daily self-report measures in- cluded: rating of pain intensity on a numerical
scale O- 10, rating quality of sleep as: (1) uninter-
rupted; (2) interrupted: (3) very bad: or (4) no sleep at all. Details of the analgesic medication required each day and of self-hypnosis practice
were recorded. The ISCRG has 6 elements which are rated
against 8 constructs. Constructs are presented as bipolar visual analog scales. Elements and con- structs are detailed in Appendix A.
ISCRG data were analysed using lngrid 72. This program was developed by Patrick Slater and has been carefully described in great detail in his 2 volume work on the measurement of intra-per-
sonal space [12]. The output from each grid analy- sis is very extensive and space would not permit us to give all of these data on the 16 grids described

157
in this paper. Instead, the grids will be presented in the form of composite diagrams and Appendix B is attached as an example of the data output on
one grid. Essentially, Ingrid 72 performs a prin-
cipal component analysis on the raw data, which are the ratings of each element against each of the
bipolar constructs. These data form the grid ma- trix from which the components are computed. In effect, there are 2 mathematical ‘spaces,’ a con-
struct space and an element space. The elements can be defined in terms of their positions in the construct space whilst the constructs can be de- fined in terms of their positions in the element space. The components are computed by a sub- routine applied to the covariance matrix between the elements. It is condensed into a tridiagonal
matrix with the same latent roots and its k roots are all obtained simultaneously by direct solution
of the determinantal equation. Finally, the ele-
ment vectors are derived and stored as an m x k array. Construct vectors are then calculated from
these results. The components therefore describe the connections between the construct and ele- ment spaces. The orientation of the component
axes is determined in the construct space by the element vectors and in the element space by the construct vectors. In grids of the size described in this paper, most of the variance is accounted for by the first 2 or 3 principal components. It is therefore possible to represent the data succinctly and with acceptable accuracy in the form of com- posite diagrams according to Siater’s method. Here
the first 2 principal components are taken as the horizontal and vertical axes of the graph. The constructs are plotted as angles to the components and are represented as bipolar points at the cir-
cumference of a circle drawn at a convenient
radius around the intersection of the component axes. The elements are plotted as points within this construct space. It is possible to represent the relationship of each element with each construct by simply dropping a perpendicular line from the element point to the construct axis - thus depict- ing the position of the element along the dimen- sion of the bipolar construct [8,12].
The ISCRG was recently evaluated on a sample of 21 ‘well’ volunteers. Test-retest reliability of the ISCRG, with 1 week delay, was found to be
0.80. These data are being prepared for pub- lication.
Results
This section consists of a brief summary of the
overall results of the study followed by discussion
of the ISCRG. There was a great deal of variation in response
to treatment, even in this small sample. An overall reduction of pain was indicated by the decrease in the MPQ scales of ‘Number of words chosen’ and ‘Pain rating index.’ Breakdown of the PRI indi- cated there was a specific decrease in the affective
and the evaluative dimensions of pain. There was no overall decrease in daily measures of pain. Pain-related measures of medication intake, qual-
ity of sleep and daily activity levels suggest that
some improvement in lifestyle did occur. There
was a significant increase in personal locus of
control across all subjects. On an individual level,
two of the subjects totally removed their pain, two showed some improvement and one experienced no change in pain intensity.
There are 3 aspects to the discussion of the ISCRG. First the consensus findings, second the
analysis of consensus change over time, and fi- nally the grids from 2 patients will be discussed to highlight the variation which existed between sub- jects.
Consensus grids
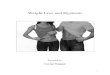
The consensus grids from each assessment time
are displayed in Fig. 1. Appendix B gives a con- densed version of the output from a single grid
using the pre-treatment grid of subject 4 as an
example. The output includes the raw scores, cor- relations between constructs, distances between
elements, latent roots of the principal components and loadings of the constructs and elements on the first 2 components.
The pre-treatment grid is an example of the typical response of an individual who has chronic pain. There is an identification of the self as physically ill, a rejection of the concept of hypo- chondriac, with its implications of psychological factors in the illness, and an expression of iso- lation from friends and family (‘others’). The doc-

CONSENSUS GRID
Pre treatment Post treatment
One Month Follow up Six Month Follow up
Fig. 1. The consensus grids for all 5 patients are shown at the 4 occasions of testing. The horizontal axis represents the first principal component and the vertical axis the second principal component. Constructs are represented as directional arrows at the
circumference of the circle and may be drawn by completing the line through opposing arrows and the mid-point of the graph. The
positive poles are unsigned. The negative poles are signed. Elements are represented by the open circles. Both elements and constructs
are labelled according to the list shown in Appendix A.
tor is seen as understanding that they are physi- cally ill.
The series of post-treatment and follow-up grids represent the move towards feeling understood by others and of rejecting the concept of physical illness. Physical illness becomes associated with the hypochondriac at the negative poles of the constructs.
The final assessment at 6 months post treat- ment indicates that they now feel understood by both doctor and family. The ‘doctor’ believes that they bottle feelings up while ‘others’ believe that they express feelings more than they do. It is of interest that the ‘physically ill’ element and the ‘ideal self’ are both more expressive of feelings than the patients see themselves.

159
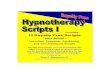
Time series grids from each test occasion, on 1 grid. The results The dimensions of the grid are determined by indicate both changes in the conception of an
each set of data. This means that distances be- element across time and changes in the rela-
tween elements for different grids may not be tionship between the elements (Fig. 2). Note that
directly comparable. To obtain further informa- the construct alignment is identical and that dis- tion about the changes in self-concept we plotted tances are now directly comparable. the self, ideal self, and the physically ill element, Within elements. The concept of self changed
TIME SERIES CONSENSUS GRID
Pretreatment
One Month Follow up
A : as I am
Post treatment
Six Month Follow up
B : as f would like to be C : like a physically ill person
Fig. 2. The grids are displayed using the same conventions as Fig. 1. On this occasion construct alignment is kept constant, negative
poles are unsigned, and only 3 elements are plotted for each test occasion.

160
from being irritable, with many problems other I’he concept of ideal self remained consistent than pain, to being less worried about their illness, during the study and was a rather idealised picture
less depressed and less anxious and notably to- of health. with no problems and no emotional
wards being able to express feelings. distress.
SUBJECT FOUR
Pre treatment Post treatment
b
5
7 7
- 4
One Month Follow up Six Month Follow up
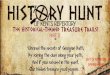
Fig. 3. Individual grids for subject 4 are shown using the same conventions as Fig. 1. Only the construct poles on the left of each grid are labelled. Positive poles are unsigned, negative poles are signed.

Initially the physically ill element was pre- having an emotional component to the pain and sented as worried about illness, anxious and de- as bottling feelings. It is interesting that the rating pressed. At the post-treatment assessment this al- of physical illness at this stage corresponds with tered and the physically ill person was seen as the rating of self initially, After 1 month the
SUBJECT FfVE
c
i 4 7 -8
Pre treatment Post treatment
One Month Follow up Six Month Follow up
Fig. 4. Individual grids for subject 5 are shown using the same conventions as Fig. 1. Only the construct poles on the left of each grid
are labelled. Positive poles are unsigned, negative poles are signed.

physically ill element is rated at the extremes of illness, worry and distress but by the 6 month assessment it has returned to the initial position.
Between elements. During the treatment phase of the study there is a close association of the self
and physically ill element. This changes during the
follow-up phase as the self begins to be identified
more positively. There is also a slight increase in
the distance between the ideal self and the physi-
cally ill element at the end of the study. The change in orientation of the elements at post
treatment indicates that the constructs on which
they vary have altered. The actual self is separated from the idea1 by being less emotionally expres-
sive, having more outside problems and having a greater emotional component to the pain. The
actual self is now less worried about the pain, less anxious and less depressed than the physically ill person. The ideal self has less emotional problems and more expression of emotion than the physi-
cally ill person.
Subject 4. A cluster of the elements ‘as I am,’ ‘as others see me,’ ‘ as the doctor sees me’ and ‘like
a physically ill person’ was found for both subjects
2 and 4. The ’ ideal self’ and ‘ hypochondriac’ were
positioned at the positive and negative poles of the constructs, respectively (Fig. 3). These subjects showed the least improvement, although they both
demonstrated pain control during the treatment sessions. They identified themselves by their health
problem. Unlike the other patients in this study these two felt understood by their family and friends. Feeling understood may, for these individ- uals, have trapped them in the role of patient.
There was little variation in subject 4’s grid during the study, although the physically ill ele- ment was more closely associated with the self at
the end of the study. Subject 5. The notable feature about subject 5 is
that initially he had a small distance between the elements of ‘actual’ and ‘ideal’ self which were
both aligned with the ‘hypochondriac.’ The ‘physically ill person’ was at the extreme on the
worry and distress constructs (Fig. 4). At the end of treatment this has changed and
the ‘ideal self’ is associated with the ‘physically ill’
person. The ‘actual self’ is now aligned with ‘as the doctor sees me.‘ This suggests that subject 5 now sees himself as wanting to be physically ill rather than believing himself a hypochondriac.
The hypochondriac element ia at the negative ex- treme of the grid.
At the 1 month follow-up the actual self is now associated with both ‘as my doctor sees me’ and
with ‘as others see me.’ The ideal self has moved away from this cluster having more non-pain
problems than the actual self. At this assessment both the hypochondriac and the physically ill ele- ment have moved to the edge of the distress scales.
whilst, at 6 months, both elements moved to the extreme of the grid, representing 2 poles of nega- tive attributes and the actual self was more closelv associated with the ideal.
This subject experienced chronic low back pain as the result of an injury. He was involved in a legal battle with the Accident Compensation Cor- poration over the validity of his claim. They argued that there had been no precipitant injury. As he
continued with the treatment this patient became more convinced of the validity of his claim, as
expressed by the separation between hypo- chondriac and self and the association of ideal self
and physically ill. By the 1 month assessment he
had significantly improved the pain and had ceased to identify himself as ill. Relationships with his family had improved and he reported feeling un- derstood by both others and the doctor. This situation was repeated at 6 months, with some increase in distance between himself and his
family.
Discussion
The patients who took part in this study were deliberately selected for high hypnotisability in order to maximise the effects of SH. Despite this selection and despite the fact that all subjects experienced some alteration in their pain during therapy sessions, improvement was variable. Two patients had complete remission of pain, one re- mained unchanged but continued to work and function adequately and two continued to suffer disabling pain. The consensus grids suggested ini-

163
tial identification of the self-concept with physical illness, with a loosening of this identification in
the follow-up phase. Since the Health Locus of Control scale showed a significant shift towards
personal locus of control [4], it is tempting to interpret these findings as indicating a cognitive shift away from perceiving oneself as a helpless
victim of illness towards a self-concept of relative wellness, with an ability to alter one’s pain experi- ence. This interpretation would view the grid
changes as being a consequence of the experience of being able to alter pain by using a self-directed
technique. When one considers the individual grids, how-
ever, an alternative interpretation presents itself.
The 2 patients whose grids are described in detail
illustrate the extremes of the patterns of changes found. Subject 4 saw herself at the start of the
study much as she believed her doctor and others did, i.e., as a physically ill person. At the 6 month follow-up little had changed, even though this
patient could experience dramatic pain relief dur- ing therapy sessions. She could experience pro- found glove anaesthesia and could transfer this sensation to her painful knee, but the effect re- mained transient and she remained unconvinced
of her ability to help herself. In contrast, subject 5 saw himself closer to being a hypochondriac than a physically ill person and felt alienated from others whom, he felt, viewed him as being healthy. At follow-up his self-view was more congruent
with that of others, but closer to wellness and a considerable distance away from physical illness or hypochondriasis. He had experienced good
success using hypnotically mediated imagery of relaxing and healing his back muscles and now
felt well in control of the situation.
Subject 2, who stopped using SH and gained little benefit, showed a very similar grid pattern to
subject 4, whilst subjects 1 and 3 showed marked increases in the distances between the self and physical illness elements. This happened for sub- ject 3 despite little change in his level of pain. One
might hypothesise, therefore, that subjects 2 and 4 found themselves ‘locked’ into a self-view of being physically ill and this being congruent with the way they believed their doctor and others viewed them.
It is possible that the experience of pain relief using hypnosis created a sense of cognitive disso- nance which was resolved by preserving the self- concept of physical illness and negating the effects
of self-hypnosis; for subject 2 by ceasing to prac- tice and for subject 4 by reducing the reliability
and durability of the hypnotically induced pain relief. The latter is not suggested as being a de- liberate and considered action, but this patient
had a history of dissociative symptoms, including amnesia and brief fugue states. She was caught up in compensation issues and remained angrily re-
sentful towards the person who had injured her and caused her pain problem. Clinically it did not
seem unreasonable to suggest that classical con-
version mechanisms were operating to produce
and maintain psychogenic pain.
Clearly, this small group study cannot be used
to draw any valid conclusions on this matter, but it does raise a potentially important clinical and research question. Essentially this is whether the
experience of pain relief can so powerfully alter
self-concepts that the self-view will shift from illness to wellness; or alternatively whether a fixed self-view of illness neutralises treatments such as hypnosis, which are aimed at producing subjective pain relief. We suggest that this issue could use- fully be explored using the ISCRG with extended
groups of patients in trials of pain relieving proce- dures.
The ISCRG is a useful research tool in that it is highly flexible and yet can produce quantifiable
data which allows comparison across both individ- uals and time. Clinically it provides insight into
the individual and can be used to guide the clini-
cian in evaluating and planning treatment. The results of this study are similar, but not identical,
to our findings in a study of a small group pain management programme [8]. In that study there was a clear shift towards viewing illness as an undesirable state. There was some shift away from viewing the self as physically ill but this was not statistically significant. It may be that the shifts in attitude shown in the pain management sample were a reflection of the educational content of the programme whilst the samples reported here were more influenced by the change in their pain expe- rience. The fact that the ISCRG has once again

identified clinically meaningful change> III self- concepts is further evidence of the utility of this
method.
Acknowledgements
Our thanks to the patients who took part in this study and to Mr. John West and Dr. Alex Serge-
jew for help in computer programming.
References
1 Bannister. D. and Fransella, F., Inquiring Man: The Psy-
chology of Personal Constructs. 2nd edition, Penguin Books.
New York. 1980.
2 Beail. N., Consensus grids: what about the variance? Br. J.
Med. Psychol.. 57 (1984) 193-195.
3 C‘ovino. N.A. and Warfield, C.A., Hypnosis and the
management of pain, Hosp. Pratt.. 20 (1985) 48g-48t.
4 James, F.R. and Large. R.G., Self-hypnosis in chronx pain:
a multiple baseline study. Submitted for publication.
5 Kazdin. A.E.. Single-Case Research Designs: Methods for
Clinical and Applied Settings. Oxford University Press.
New York. 1982.
(1
7
8
Y
IO
11
12
13
14
I.arge. R.G. Prcdlcrlon of treatment response in pam pa-
tlents: the ~llnebs self-concept repertory grid .tncl EM(;
feedback. Pam. 21 (1985) 27% 2x8.
I..lrge. R.G.. Self-concept> and illness attitudes m chronrc
pain A repertoq grid study of ;\ pain management pro-
gramme. Pain. 23 (19X5) 113 119.
1x,1. P.A.. Ware. P.D. and Monroe. R.R.. The hypnotic
control of intractable pun. Am. J (‘Iin. Hypnox.. 3 (1960)
: h.
Melzack. R.. l‘he McG11l Pain Questionnaire: maJor prop-
crtw and scoring methods. Pam. 1 (1980) 277 ~299.
Morgan, A.H. and Hilgard, J.R., The Stanford Hypnotic
Clinical Scale for Adults. Am. J. Clin. Hypnw.. 21 (1979)
I34- 147.
Slater. P. (Ed.). The Measurement of Intrapersonal Space
by Grid Technique. Vols. 1 and 2, Wiley, London, 1976.
Wallston, B.S., Wallston, K.A., Kaplan, G.D. and Maides.
S.A.. Development and validation of the Health Locus of
Control (HLC) scale. J. Cons. Clin. Psychol., 44 (1976)
580.-588.
Wilson, B., Single-case experimental designs In neuropsy-
chological rehabilitation. J. Clin. Exp. Neuropsvchol.. 9
(1 Y87) 527-544.
Appendix A: elements and constructs of the ISCRG form A
Elements
A=Asl am C = As others see me E = Like a hypochondriac
Constructs
B = As 1 would like to be D = As my doctor sees me F = Like a physically ill person
1.
2.
3.
4.
5.
6.
7.
8.
I am worried about illness in general: Not at all . a great deal.
I see my illness or pain as:
Extremely serious . . . . not serious.
The part emotions play in causing or maintaining my pain or illness is:
Not important . most important.
Regarding feelings I : Bottle all feelings up . . express all feelings regardless of consequences
The extent of my depression is: Nil . . . so severe that suicide is contemplated
My degree of anxiety is: So severe that I am panic stricken . . . . I have problems apart from my pain which are: Not important . .
My irritability is Extreme .
nil
most important.
nil

165
Appendix B: sample output of Ingrid 72
It! SUBjiCT 4 - PRETRERTHiNi
'f~'?~Tii!l# ,I A
5c!:.5050
7:59.:m 5046.9333 8090 .@OC:I 527j.5010 502i.X; Si23r1,OOOi' 10~40.3~~j
AS PER CEN 9.60
14.49 9.66
15.49 lO.!C 9.61
1i.3
19.30

166

167
ELEHENT 3 4 0.!98 : 0.134 6 -0.159
ELMENT 4 5 _(),2;2 b -,>,!5Z
ELEKNi 5 b -0.9:4


169
l.-il.!39 2 -0.928 3 0.360 CONSTRUCT 2 WITH ELEiYENT
1 0.363 2 -0.942 3 O-63? CWTRUCT 3 Y!lH ELEHENT
1 -O.!% 2 -0.921 3 0.354 C!J#SiCliCT 4 WITH ELEYEK
1 -0.906 2 -0 .d 055 3 -0.603 CMiRUCi 5 YITlf ELKIT
1 Ij . !J" *I 2 -53.981 3 0.557
Ci?!~WUii 6 MIT!! ELEWT 1 -s.113 2 -0.913 3 0x1 ..Jd CW!RUii ! llIiH ELEXE!dT
1 -c.;i: 2 -0.79.i ; 6.X? CWSTRUCT S KiX iLiYE!T
! C.5!7 2 -O.B?‘j ; n li?C “.__,
4 -0.020
4 0.347
4 -G.OO?
4 -0.845
4 O.l!Z
4 0.020
4 -G.Z4
4 0.66:
5 c.955 6 -0.090
5 0.603 6 -0.002
5 0.953 6 -0.113
5 0.674 6 0.X
: O,SiE 6 -O.??l
5 0.943 6 -C.OS7
5 0 ., C,4 6 -C .‘A. 171
5 0.207 6 X0.676
CCl;SiLsCT 1 UiTh) ELEREfii
! 93.5 2 !5?.! 3 64.9 PNSTRUCT 2 kiilH ELE?!ENT
I 68.1 2 160.4 3 511.3 CCHSiRtlCT 3 EITK ELEZi#i
! 99.0 2 !57.! 3 69.3 CWTRUCi 4 Ir'iTH ELEW!T
1 154.9 2 94.9 3 !27.1 CFHSiRKT 5 YiiH ELXNT
1 37.! 2 1t9.9 3 A.! COHSTFJCT 6 Yii!! ilE$E?T
1 96.5 2 i58.9 3 69.4 C3NSTRUCi ! WITH ELEMENT
1 !12.!j 2 142.5 3 X.6 CONSKL!C: 8 !+'I%! ELXXT
1 58.9 2 !49.1 3 34.9
4 91.1 : 17.2 6 95.1
4 69.7 : 52.9 6 9L1.1
4 FC.5 5 16.6 6 96.5
4 !4;.6 5 4i.6 6 67.!
4 7?.9 5 ZS.6 6 lc:.!
4 93.9 5 !F.4 6 95.?
4 lG3.G j !3.1 6 5ib.9
4 4'1.4 5 59.5 6 132.5

















![Hypnosis William Hewitt - Hypnosis for Beginners[2003]](https://img.pdfslide.us/doc/110x75/552115f3497959734d8b4612/hypnosis-william-hewitt-hypnosis-for-beginners2003.jpg)