Embed Size (px)
Citation preview

lable at ScienceDirect
Seminars in Fetal & Neonatal Medicine 20 (2015) 262e271
Contents lists avai
Seminars in Fetal & Neonatal Medicine
journal homepage: www.elsevier .com/locate/s iny
Review
Persistent pulmonary hypertension of the newborn: Advances indiagnosis and treatment
Amish Jain a, Patrick J. McNamara b, c, *
a Department of Pediatrics, Mount Sinai Hospital, Toronto, Ontario, Canadab Division of Neonatology, Hospital for Sick Children, Toronto, Ontario, Canadac Departments of Pediatrics and Physiology, University of Toronto, Toronto, Canada
Keywords:Pulmonary hypertensionPersistent pulmonary hypertension of thenewborn (PPHN)NewbornPhenotypic expressionEchocardiography
* Corresponding author. Address: Department of NChildren, 555 University Avenue, Toronto, Ontario M5813 5773x6345; fax: þ1 (416) 813 5245.
E-mail address: [email protected] (P.J
http://dx.doi.org/10.1016/j.siny.2015.03.0011744-165X/Crown Copyright © 2015 Published by Els
s u m m a r y
Persistent pulmonary hypertension of the newborn (PPHN) is a frequent cause for admission to theneonatal intensive care unit and is associated with mortality and variable morbidities. It is primarily astate of oxygenation failure representing a failure of the normal postnatal decline in pulmonary vascularresistance that may be associated with right ventricular dysfunction. Enhanced knowledge of thepathophysiologic contributors to this syndrome helps clinicians understand its phenotypic expressionand facilitates more focused intensive care decision-making. The approach to treatment should be basedon alleviation of the elevation in pulmonary vascular resistance and should include optimization of lungrecruitment and judicious use of pulmonary vasodilators. When response to inhaled nitric oxide issuboptimal, the physiologic contributors to impaired oxygenation need further investigation. Targetedneonatal echocardiography provides novel physiologic insights; in particular, it may help assess theadequacy of right ventricular performance, the relative contribution of the fetal shunts and themagnitude of the overall impairment to cardiac output. This information may facilitate therapeutic nextsteps and whether adjunctive vasodilators or drugs to augment ventricular function are preferable. Thisarticle provides a comprehensive overview of the pathological contributors to PPHN, the physiologicconstituents of its phenotypic expression, standard approach to therapeutic intervention, and the role ofbedside echocardiography in enhancing the decision-making process.
Crown Copyright © 2015 Published by Elsevier Ltd. All rights reserved.
1. Introduction
Pulmonary hypertension (PHT) is a serious cardiopulmonarydisorder characterized by elevated mean pulmonary artery pres-sure (mPAP) and prolonged exposure of the right ventricle to highafterload. Physiologically, mPAP is directly related to pulmonaryblood flow (PBF), pulmonary vascular resistance (PVR) and pul-monary capillary wedge pressure (PCWP) by the equation:
mPAP¼ (PBF � PVR) þ PCWP.
Although PHT may result from high PBF (e.g., large left-to-rightshunts, severe chronic anemia) or rise in PCWP (e.g., left ventricular
eonatology, Hospital for SickG 1X8, Canada. Tel.: þ1 (416)
. McNamara).
evier Ltd. All rights reserved.
dysfunction), the vast majority of cases are secondary to high PVR.In neonates, PHT is almost always secondary to dysregulation ofPVR. PHT is a frequent diagnosis in tertiary neonatal intensive careunits and may arise secondary to a wide range of diseases. Broadly,PHT in neonates can be described as acute or chronic (Fig. 1), whichare distinguished by intrinsic differences in their pathophysiologyand clinical presentation [1]. While acute episodes of neonatal PHTmay occur later in neonatal illnesses (e.g., secondary to sepsis), themost usual presentation is in the immediate postnatal period,secondary to abnormal transition of the pulmonary circulationfrom a high-resistance intrauterine to a low-resistance extrauterinecircuit. This characteristic presentation of acute pulmonary hyper-tensive crises is widely referred to as persistent pulmonary hy-pertension of the newborn (PPHN). Chronic PHT, on the other hand,occurs due to secondary rise in PVR following initial successfulpostnatal transition, and is seen most frequently as a secondarycomplication of chronic neonatal lung disease in prematurely bornneonates [2,3]. The majority of research in neonatal PHT hasfocused on PPHN, yet knowledge gaps remain and core physiologic

Fig. 1. Pulmonary hypertension in neonates can be classified as acute or chronic and may arise from a variety of underlying disorders. RDS, respiratory distress syndrome; TTN,transient tachypnea of newborn; MAS, meconium aspiration syndrome; CDH, congenital diaphragmatic hernia; HIE, hypoxiceischemic encephalopathy; AV, arteriovenous; NSAID,non-steroidal anti-inflammatory drug; SSRI, selective serotonin reuptake inhibitors; SIRS, systemic inflammatory response syndrome; NEC, necrotizing enterocolitis; ACDMPV,alveolar capillary dysplasia with misalignment of pulmonary veins; CNLD, chronic neonatal lung disease; CDH, congenital diaphragmatic hernia; ASD, atrial septal defect; VSD,ventricular septal defect; PDA, patent ductus arteriosus. Reproduced with permission from Chapter 29, Avery's neonatology: pathophysiology and management of the newborn, 7thed (in press).
A. Jain, P.J. McNamara / Seminars in Fetal & Neonatal Medicine 20 (2015) 262e271 263
concepts are oftentimes neglected; in addition, the relativecontribution of chronic PHT to adverse clinical outcomes is justbeginning to be realized.
Persistent pulmonary hypertension of the newborn is one of themost challenging acute disorders of postnatal transition with sub-stantial morbidity and mortality. Perinatal asphyxia, meconiumaspiration syndrome and sepsis account for the majority of cases;irreversible causes are fortunately rare. Occasionally, PPHN may bethe primary diagnosis when no other underlying pathology can beidentified. Although improved obstetric care has considerablyreduced the incidence of these perinatal pathologies, PPHN con-tinues to be an important clinical problem accounting for up to 4%of all admissions to some tertiary neonatal units. The incidence indeveloped countries ranges from one to two per 1000 live birthswith a mortality rate of ~10% [4,5]. Surviving neonates often requireprolonged cardiorespiratory support, have a long hospital stay, andare at high risk of long-term adverse neurodevelopmental out-comes [6]. The incidence and burden of disease is likely to be muchhigher in the developing world. Although treatment with exoge-nous inhaled nitric oxide (iNO), the only approved pulmonaryvasodilator in neonates, has reduced the need for extracorporealmembrane oxygenation (ECMO), these benefits have not translatedinto a survival advantage or minimization of long-term neuro-disability [5,7]. Given the relatively high prevalence of these dis-orders in tertiary NICUs, it is imperative that clinicians caring forthese babies familiarize themselves with the disease-specificphysiology and associated hemodynamic alterations. Promptrecognition and early effective management is important for opti-mizing patient outcomes. In this article we suggest the need toreconsider PPHN as a physiologic continuum, with cardiopulmo-nary consequences that vary between patients and according toprecipitating causes; in addition we attempt to justify the need toperform a thoughtful and comprehensive appraisal of actual
physiology as an essential prerequisite of the clinical decision-making process.
2. Pathophysiology
2.1. Cellular pathways
Several cellular pathways involved in regulation of pulmonaryvascular tone have been identified over the last two decades (Fig. 2)[1,8]. It is important for clinicians to be aware of these pathways,which modulate pathophysiological progression and clinicalimpact. Although inter-pathway interactions exist and relation-ships may be complex in nature, for the sake of simplicity, therelevant pathways could be described under following headings:(A) nitric oxide (NO)-soluble guanylate cyclase‒cyclic guanylmonophosphate (cGMP); (B) prostaglandin‒prostacyclin‒cyclicadenosine monophosphate (cAMP); (C) rho-A/rho-kinase; (D)endothelin; (E) free radicals. Among these pathways, pathways (A),(B) and (D) have been the subjects of most interest. Oxygen and NOrepresent mediators of pulmonary vasodilatation translated intostandard clinical practice. Subsequently, a number of other medi-ators have been identified, prompting the development ofadjunctive/alternate therapeutic agents. Whereas successful use ofmany alternate therapeutic agents have been described in PPHN,the relative contributory role of each mediator in enabling suc-cessful physiological transition after birth and under pathologicalconditions has not been completely elicited. Pulmonary vasodila-tation has been shown to occur in response to stimulation by nitricoxide (NO) [7], prostacyclin (PGI2) [9,10] and soluble guanyl cyclase(sGC) [11] and inhibition of phosphodiesterase 3 and/or 5 (PDE 3/5)[12e14], endothelin 1 (ET 1) [15,16], reactive oxygen species (ROS)[17], and rho-kinase [18,19]. A basic knowledge of these regulatorypathways and target mediators is necessary for clinicians involved
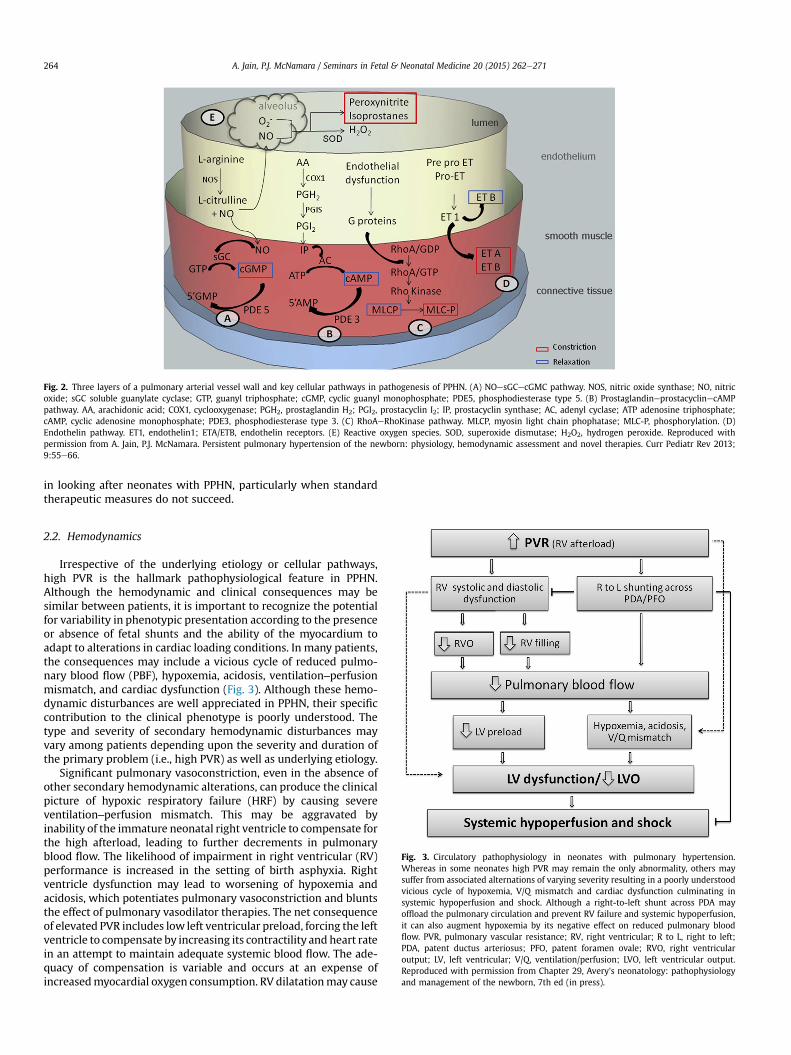
Fig. 2. Three layers of a pulmonary arterial vessel wall and key cellular pathways in pathogenesis of PPHN. (A) NOesGCecGMC pathway. NOS, nitric oxide synthase; NO, nitricoxide; sGC soluble guanylate cyclase; GTP, guanyl triphosphate; cGMP, cyclic guanyl monophosphate; PDE5, phosphodiesterase type 5. (B) ProstaglandineprostacyclinecAMPpathway. AA, arachidonic acid; COX1, cyclooxygenase; PGH2, prostaglandin H2; PGI2, prostacyclin I2; IP, prostacyclin synthase; AC, adenyl cyclase; ATP adenosine triphosphate;cAMP, cyclic adenosine monophosphate; PDE3, phosphodiesterase type 3. (C) RhoAeRhoKinase pathway. MLCP, myosin light chain phophatase; MLC-P, phosphorylation. (D)Endothelin pathway. ET1, endothelin1; ETA/ETB, endothelin receptors. (E) Reactive oxygen species. SOD, superoxide dismutase; H2O2, hydrogen peroxide. Reproduced withpermission from A. Jain, P.J. McNamara. Persistent pulmonary hypertension of the newborn: physiology, hemodynamic assessment and novel therapies. Curr Pediatr Rev 2013;9:55e66.
A. Jain, P.J. McNamara / Seminars in Fetal & Neonatal Medicine 20 (2015) 262e271264
in looking after neonates with PPHN, particularly when standardtherapeutic measures do not succeed.
Fig. 3. Circulatory pathophysiology in neonates with pulmonary hypertension.Whereas in some neonates high PVR may remain the only abnormality, others maysuffer from associated alternations of varying severity resulting in a poorly understoodvicious cycle of hypoxemia, V/Q mismatch and cardiac dysfunction culminating insystemic hypoperfusion and shock. Although a right-to-left shunt across PDA mayoffload the pulmonary circulation and prevent RV failure and systemic hypoperfusion,it can also augment hypoxemia by its negative effect on reduced pulmonary bloodflow. PVR, pulmonary vascular resistance; RV, right ventricular; R to L, right to left;PDA, patent ductus arteriosus; PFO, patent foramen ovale; RVO, right ventricularoutput; LV, left ventricular; V/Q, ventilation/perfusion; LVO, left ventricular output.Reproduced with permission from Chapter 29, Avery's neonatology: pathophysiologyand management of the newborn, 7th ed (in press).
2.2. Hemodynamics
Irrespective of the underlying etiology or cellular pathways,high PVR is the hallmark pathophysiological feature in PPHN.Although the hemodynamic and clinical consequences may besimilar between patients, it is important to recognize the potentialfor variability in phenotypic presentation according to the presenceor absence of fetal shunts and the ability of the myocardium toadapt to alterations in cardiac loading conditions. In many patients,the consequences may include a vicious cycle of reduced pulmo-nary blood flow (PBF), hypoxemia, acidosis, ventilation‒perfusionmismatch, and cardiac dysfunction (Fig. 3). Although these hemo-dynamic disturbances are well appreciated in PPHN, their specificcontribution to the clinical phenotype is poorly understood. Thetype and severity of secondary hemodynamic disturbances mayvary among patients depending upon the severity and duration ofthe primary problem (i.e., high PVR) as well as underlying etiology.
Significant pulmonary vasoconstriction, even in the absence ofother secondary hemodynamic alterations, can produce the clinicalpicture of hypoxic respiratory failure (HRF) by causing severeventilation‒perfusion mismatch. This may be aggravated byinability of the immature neonatal right ventricle to compensate forthe high afterload, leading to further decrements in pulmonaryblood flow. The likelihood of impairment in right ventricular (RV)performance is increased in the setting of birth asphyxia. Rightventricle dysfunction may lead to worsening of hypoxemia andacidosis, which potentiates pulmonary vasoconstriction and bluntsthe effect of pulmonary vasodilator therapies. The net consequenceof elevated PVR includes low left ventricular preload, forcing the leftventricle to compensate by increasing its contractility and heart ratein an attempt to maintain adequate systemic blood flow. The ade-quacy of compensation is variable and occurs at an expense ofincreasedmyocardial oxygen consumption. RV dilatationmay cause
A. Jain, P.J. McNamara / Seminars in Fetal & Neonatal Medicine 20 (2015) 262e271 265
leftward deviation of the interventricular septum, thereby reducingthe left ventricular filling capacity and compliance. Systolicdysfunction of the right ventricle, by virtue of ventricular‒ventric-ular interaction through shared myocardial fibers between the twoventricles, may adversely affect LV systolic function [20]. Further,non-PVR related factors might also contribute to the myocardialdysfunction. These factors include the underlying etiology (e.g.sepsis, perinatal asphyxia), systemic hypovolemia, invasive venti-lation with high mean airway pressure and medications (e.g. pul-monary vasoconstriction from high-dose epinephrine anddopamine, low preload secondary to systemic vasodilatation frommilrinone) [21]. Furthermore, the role of fetal shunts needsthoughtful consideration. A large PDA, if present, may shunt bloodfrom the pulmonary to systemic circulation; on one hand, this mayprotect theneonatal rightventricle byoffloading thehigh-resistancepulmonary circuit and support postductal systemic perfusion, butmay also potentiate hypoxemia by promoting low PBF. Similarly thepresence of a right-to-left transatrial shunt may support preductalcardiac output and cerebral perfusion when pulmonary venous re-turn and left heart preload are severely compromised, but at theexpense of lower blood oxygenation. The merits/harm of fetalchannels need broad consideration according to the unique patho-physiological circumstances. Regardless, if uncorrected, the clinicalpicture in PPHN may rapidly progress to a state of refractory hyp-oxemia and severe systemic hypoperfusion and shock.
2.3. Right ventricular performance and PPHN
The right ventricle plays an essential role in supporting pulmo-nary bloodflowduring the normal neonatal transition. The ability ofthe right ventricle to maintain or augment its performance in thesetting of PPHN, where there is failure of the normal postnataldecline in PVR, is an important component of the adaptive response.
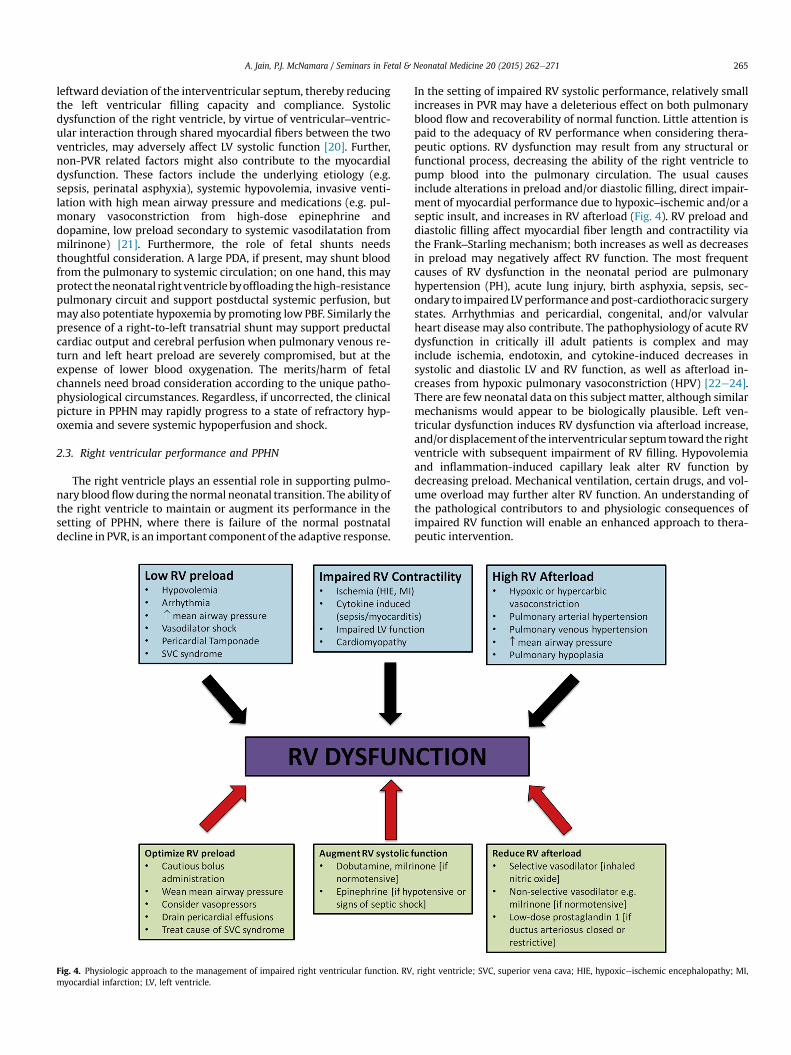
Fig. 4. Physiologic approach to the management of impaired right ventricular function. RVmyocardial infarction; LV, left ventricle.
In the setting of impaired RV systolic performance, relatively smallincreases in PVR may have a deleterious effect on both pulmonaryblood flow and recoverability of normal function. Little attention ispaid to the adequacy of RV performance when considering thera-peutic options. RV dysfunction may result from any structural orfunctional process, decreasing the ability of the right ventricle topump blood into the pulmonary circulation. The usual causesinclude alterations in preload and/or diastolic filling, direct impair-ment of myocardial performance due to hypoxic‒ischemic and/or aseptic insult, and increases in RV afterload (Fig. 4). RV preload anddiastolic filling affect myocardial fiber length and contractility viathe Frank‒Starling mechanism; both increases as well as decreasesin preload may negatively affect RV function. The most frequentcauses of RV dysfunction in the neonatal period are pulmonaryhypertension (PH), acute lung injury, birth asphyxia, sepsis, sec-ondary to impaired LVperformance andpost-cardiothoracic surgerystates. Arrhythmias and pericardial, congenital, and/or valvularheart disease may also contribute. The pathophysiology of acute RVdysfunction in critically ill adult patients is complex and mayinclude ischemia, endotoxin, and cytokine-induced decreases insystolic and diastolic LV and RV function, as well as afterload in-creases from hypoxic pulmonary vasoconstriction (HPV) [22e24].There are few neonatal data on this subject matter, although similarmechanisms would appear to be biologically plausible. Left ven-tricular dysfunction induces RV dysfunction via afterload increase,and/ordisplacementof the interventricular septumtoward the rightventricle with subsequent impairment of RV filling. Hypovolemiaand inflammation-induced capillary leak alter RV function bydecreasing preload. Mechanical ventilation, certain drugs, and vol-ume overload may further alter RV function. An understanding ofthe pathological contributors to and physiologic consequences ofimpaired RV function will enable an enhanced approach to thera-peutic intervention.
, right ventricle; SVC, superior vena cava; HIE, hypoxiceischemic encephalopathy; MI,

A. Jain, P.J. McNamara / Seminars in Fetal & Neonatal Medicine 20 (2015) 262e271266
3. Clinical evaluation and diagnosis
Classically, diagnosis of PPHN is clinically suspected in neonatespresentingwith signs of respiratory distress andHRF during the firstfew days of age, especially when it occurs in the context of incrimi-nating clinical history. Indeed, PPHN occurs more frequently sec-ondary to an underlying etiology. A careful appraisal of the clinicalscenario, which includes careful elicitation of a detailed case historyand completion of a thorough clinical examination, may provideimportant etiological clues. Clinical assessment will usually have tobe quick and performed alongside resuscitative measures to ensuretimely stabilization. For example, a history of fetal distress, severemetabolic acidosis in cord blood, low Apgar scores and/or the pres-ence of meconium in amniotic fluid and/or in the neonate's larynxvisualized on direct laryngoscopy along with typical chest X-rayfindings suggest a significant perinatal hypoxic‒ischemic event orseries of events. Meconium aspiration syndrome may also occur inthe setting of significant perinatal asphyxia; history of prolongedrupture of membranes, group B streptococcus colonization, orpresence of chorioamnioitis suggest infection. In addition to theclinical features of septic shock or the presence of bronchopneu-moniaonchest radiograph,blood, urineorcerebrospinalfluid testingmay reveal evidence of acute systemic inflammation. A history ofelective cesarean section and radiological finding of fluid in inter-lobar fissures suggests transient tachypnea of the newborn. Other,relatively less frequent etiologies include respiratory distress syn-drome, especially in late-preterm and term neonates born tomothers with poorly controlled diabetes; antenatal drug exposure(e.g. delayed transition from selective serotonin reuptake inhibitors,antenatal closure of ductus arteriosus from non steroidal anti-inflammatory drugs); chromosomal anomalies; pulmonary hypo-plasia (secondary to congenital diaphragmatic hernia or severe longstanding oligohydramnios). A family history positive for previousneonatal deaths from respiratory failure and/or a history of consan-guinity may point towards surfactant protein deficiency. A neonatewho appeared well at birth with normal Apgar scores but presentsminutes or hours later with severe respiratory distress and HRFwhich is relatively unresponsive to medical management may sug-gest alveolar capillary dysplasia with misalignment of pulmonaryveins, a rare genetic disorder characterized by maldevelopment ofthe capillary vascular bed around the alveoli in the lungs. Enhancedappreciation of the likely etiology may enable a more focused anddisease-specific approach to therapeutic interventions. This is highlyrelevant for unique situations such as hypoxiceischemic encepha-lopathy where the benefits of therapeutic hypothermia in mini-mizing the risk of brain injury need to be carefully balanced againstthe resultant aggravation of PVR. Regardless, therapeutic hypother-mia is a post-stabilization intervention.
Establishing the relative contribution of parenchymal lung dis-ease versus high PVR to the clinical picture of HRF can be chal-lenging, especially as they often coexist. The clinical features whichsuggest high PVR as the major contributor include severity ofoxygenation failure characterized by an oxygenation index of �15(more commonly >25) despite optimization of lung recruitment,presence of lability of systemic oxygenation and a pre-to-postductal saturation difference of >10% on pulse oximetry (SpO2).Adequacy of invasive ventilation may be judged according toarterial partial pressure of carbon dioxide, qualitative assessment oflung expansion/aeration on chest radiograph and failure ofimprovement in oxygenation independent of appropriate increasesin mean airway pressure. Oxygen lability refers to the clinicalobservation of decrements in oxygenation associatedwith agitationor handling and is suggestive of excessive pulmonary vaso-reactivity. Continuous pre-to-post ductal SpO2 monitoring is awidely used investigation to screen for and monitor treatment
response in PPHN in patients with a patient ductus arteriosus.Higher pre-than post-ductal SpO2 values relate to increasedshunting of blood from the main pulmonary artery to descendingaorta through a patent ductus arteriosus (PDA) and indicate higherPVR in comparison to systemic vascular resistance (SVR). It isimportant that pre-ductal SpO2 is measured in the right upper limband post-ductal in one of the lower limbs, as the arterial supply tothe left arm may be either pre- or post-ductal in origin. Although apositive screen is strongly suggestive of PPHN, negative screen doesnot rule it out since the ductus arteriosusmay not be patent [25,26].Further, clinicians should be aware that left-sided obstructive heartdefects (coarctation of aorta; interrupted aortic arch; hypoplasticleft heart syndrome) might demonstrate a ‘false’ positive screenand that treatment strategies aimed to lower PVR may cause clin-ical deterioration in these patients.
3.1. Role of echocardiography in diagnosing PPHN
Techniques such as cardiac catheterization and MRI for assess-ment of pulmonary vascular resistance, blood flow and myocardialfunction are currently not feasible in a sick newborn. Echocardiog-raphy is the only presently feasible bedside clinical investigation andis routinely used to confirm the diagnosis of PPHN and to monitordisease progression or response to therapies. It is a simple, non-invasive, bedside test, which can be performed even in the mostunstable patients. For older children and adults, PHT is usuallydiagnosed by echocardiography if pulmonary artery peak systolicpressure is > 35 mmHg [27]. Although this definition may be usefulfor infants with late-onset, acute or chronic PHT, it is not applicablefor diagnosing acute PPHN during the early neonatal period. This isbecause even under physiological conditions, pulmonary pressuresare expected to be high at birth and decline thereafter. The decline islikely to be most rapid over the first few hours to days of age [28]. Anumber of echocardiography indices of PVR and PHT have beenvalidated in adult patients [29,30]. Enhancements in imaging tech-niques and wide dissemination of echocardiography equipmentallow timely assessment of these indices in neonates; yet theirclinical use in PPHN is limited by the relative paucity of normativeneonatal data. Re-characterization of normal transitional physiologyusing echocardiography in a time-sensitive manner during earlypostnatal period can further inform its scientific use inmanagementof neonates with PPHN. Nevertheless, echocardiographic findingsconsistent with suprasystemic pulmonary pressures, if present, areconsidereddiagnostic of PPHN. Themostwidely usedmeasurementsinclude peak systolic RV pressure calculated frommeasured velocityof tricuspid regurgitant jet, presence of pure right-to-left shunt at theductal or atrial level, and paradoxical interventricular septal motionat end-systole. On the other hand, findings suggestive of high pul-monary pressures at levels which are not suprasystemic, such asbidirectional shunts or flat interventricular septal motion, should beconsidered supportive at best, of diagnosis of PPHN, especially wheninterpreted in context of the clinical symptoms. It should be notedthat presence of significant RV systolic dysfunction may lead to un-derestimation and false ‘normalization’ of many echocardiographicindices of PHT which are pressure dependent e hence the impor-tance of payingmore attention to anddevelopingenhancedmethodsof qualitative and quantitative evaluation of RV systolic function inneonates with PPHN.
3.2. Congenital heart defect versus PPHN
Timely evaluation, to rule out a critical cyanotic congenital heartdefect (CHD), is of critical importance for neonates suspected tohave PPHN. The possibility of a duct-dependent pulmonary bloodflow disorder should be considered in all neonates presenting with

A. Jain, P.J. McNamara / Seminars in Fetal & Neonatal Medicine 20 (2015) 262e271 267
HRF during the neonatal period, particularly when symptoms fail toresolve after resuscitation and standard treatment [31]. Delays inestablishment of the correct diagnosis and implementation ofappropriate treatment may worsen prognosis [32]. The clinicalfactors which may point towards critical cyanotic CHD includefamily history, relative absence of signs of respiratory distress,presence of cardiovascular findings such as murmur, weak lowerlimb pulsations, abnormal heart shape on chest radiograph andabnormal electrocardiograph, relatively fixed SpO2, absence ofsystemic hypotension in spite of severe prolonged hypoxemia,presence of reverse differential cyanosis (i.e., post-ductalSpO2 > pre-ductal by � 10%) as it may indicate right-to-leftshunting of oxygenated blood across PDA [e.g., total anomalouspulmonary venous connections (TAPVC), transposition of great ar-teries], ‘failed’ hyperoxia test and failure to respond to or worseningwith vasodilator therapies. Although these clinical features mayprovide important clues regarding underlying etiology, theirinherent sensitivity and specificity remain low. The hyperoxia testhas been widely accepted in clinical practice, but may also beequivocal in the setting of critically low PBF due to severe PPHN.Further, PPHN is known to be an associated finding at presentationof certain critical CHDs, making clinical distinction even moredifficult. As referred to earlier, therapeutic strategies used to reducePVR may compromise patients with certain forms of heart defects,particularly disorders associated with excessive pulmonary bloodflow (e.g., TAPVC; double outlet right ventricle) or duct-dependentsystemic blood flow lesions (e.g., hypoplastic left heart syndrome),although this list is not absolute. A comprehensive structuralechocardiography assessment performed by an experienced oper-ator is the only accepted definitive test in routine clinical practice.Ideally all cases suspected of PPHN should have an echocardiogramas soon as possible to confirm the diagnosis and rule out CHD;unfortunately 24/7 echocardiography services and pediatric cardi-ology expertise are not be available in many centers and hospitals.It is our opinion that patients with a presumptive diagnosis ofPPHN, where HRF continues in spite of standard treatment orwhere the likelihood of duct-dependent CHD is considered high,require urgent evaluation by an experienced pediatric cardiologist.If delays in cardiology consultation are anticipated or illnessseverity is high, it may be desirable to maintain ductal patency byintravenous infusion of prostaglandins until a diagnosis is reached.
4. Management
4.1. General approach
For neonates presenting with HRF after birth, early identifica-tion of symptoms, timely resuscitation, close post-resuscitationmonitoring, and appropriate escalation of cardiorespiratory in-terventions are essential management steps prior to embarking ona trial of specific pulmonary vasodilator therapies. In some patients,resolution of HRF may ensue without the need for further escala-tion of treatment. The resuscitation should be provided using thesequential ‘airwayebreathingecirculation’ approach as recom-mended in standard neonatal resuscitation algorithms. The ma-jority of neonates with significant PPHN are expected to requireinvasive ventilatory support. Whereas a short trial of non-invasiveventilation may be acceptable, close clinical monitoring is essentialto ensure timely escalation. The ventilation strategy should befocused to establish adequate alveolar recruitment and carbon di-oxide clearance while avoiding lung hyper-expansion. This mayrequire escalation to high-frequency modes of ventilation andshould be confirmed and followed with chest radiograph andarterial blood gas. The goal of circulatory assessment is to ascertainadequacy of systemic perfusion and to titrate treatments
accordingly. Non-specific but frequently monitored clinical featuressuggestive of inadequate systemic blood flow include prolongedcapillary filling time, low pulse volume, and systolic hypotension;the presence of sustained metabolic acidosis due to high arteriallactate is a rather specific sign of decreased tissue oxygen delivery.Establishment of secure venous and arterial access is essential.Antibiotic treatment, if indicated, should be initiated at the earliestopportunity. Pre- and post-ductal pulse oximetry monitoringshould be initiated to assess and monitor the magnitude of anyright-to-left ductal shunt as well as the possibility of cyanotic CHD.The oxygenation index (OI) should be calculated, if feasible, toassess and document the severity of oxygenation failure. Neonatesin whom HRF persists in spite of establishing adequate ventilationand circulatory resuscitation in the absence of CDH with an OI of>15 are considered candidates for trial of specific pulmonaryvasodilator therapy.
4.2. Oxygen therapy
The target oxygen concentration ideal for optimizing outcomesfor neonates with PPHN is not established. Traditionally clinicianshave aimed to maintain above-normal oxygen content whilemanaging babies with PPHN, presumably prompted by the dis-covery of oxygen as an important mediator in the physiologicaldrop in PVR at birth and the fact that hypoxia induces a vasocon-strictor response in the pulmonary vascular bed. Although the useof oxygen to correct hypoxia and minimize hypoxic pulmonaryvasoconstriction are important clinical goals in managing neonateswith PPHN, maintaining higher than normal blood oxygen contenthas not been scientifically shown to confer any additional benefits,and may be potentially harmful [33]. The relationship between PVRand arterial partial pressure of oxygen (PaO2) has been investigatedin a number of experiments using neonatal animal models. In 1966,Rudolph and Yuan measured PVR and pulmonary arterial pressureusing invasive methods in normal newborn calves as PaO2 wasgradually decreased from 100 mmHg [34]. Interestingly, PVRremained low and did not change across a range of PaO2 valuesbetween 50 and 100 mmHg. However, further reductions in PaO2<50 mmHg lead to an exponential increase in both PVR and meanpulmonary arterial pressure. These findings were reconfirmed in arecent experiment in normal newborn lambs [35]. In addition, therelationship between PVR and PaO2 at birth remained unchangedeven when PPHN was induced experimentally by intrauterineductal ligation [36]. Further, studies in the same model demon-strated that prior exposure to hyperoxia led to exaggerated pul-monary vasoconstriction after a hypoxic insult and bluntedvasodilatory effects of iNO. Treatment with recombinant superox-ide dismutase reversed this effect, suggesting a role of oxygen freeradicals [37]. Additionally, oxygen free radicals have been shown tointeract with iNO producing peroxynitrite, an NOmetabolite that isimplicated in mediating pulmonary vasoconstriction and rightventricular dysfunction [38]. Given the current state of evidence,avoidance of both hypoxia and hyperoxia, and maintenance of ox-ygen levels within physiologically normal range (PaO2 between 60and 100 mmHg) appear to be the safest and most appropriateclinical approaches in neonates with PPHN.
4.3. Standard of care
Inhaled nitric oxide (iNO) and extracorporeal membraneoxygenation (ECMO) are two therapeutic options that have un-dergone rigorous evaluation and have scientifically proven benefitsfor infants with PPHN who fail to respond to ventilation andresuscitation measures [7,39]. Among various pulmonary vaso-dilatory therapeutic agents, iNO is the only agent approved by the

A. Jain, P.J. McNamara / Seminars in Fetal & Neonatal Medicine 20 (2015) 262e271268
US Food and Drug Administration for use in neonates with PPHN,and, when available, should always be the first-line treatment. iNOtreatment should be initiated at a dose of 20 parts per million(ppm), as it identifies the majority of ‘responsive’ cases and is rarelyassociated with side-effects [40]. Although some neonates mayrespond to doses up to 40 ppm, further escalation of the dose is notrecommended as it has not been shown to provide any additionalbenefit and increases the risk of significant methemoglobinemia[41]. It is important to remember that iNO has only been shown toimprove clinical outcomes in neonates with HRF and OI levels be-tween 15 and 40. In clinical situations where OI remains >40despite resuscitation and optimizing ventilatory management, itmay be appropriate to try treatment with iNO but it should notdelay consultation with a regional ECMO center regarding thesuitability of transfer. An urgent echocardiogram to confirm diag-nosis, evaluate cardiac function, and rule out cyanotic CHD is highlydesirable in all neonates with persistent HRF, but is mandatory ifECMO is being considered.
4.4. Potential adjunctive treatments
Several randomized controlled trials and subsequent meta-analysis have demonstrated that treatment with iNO reduces theneed for ECMO in term and near-term neonates with HRF, butwithout any beneficial effect on overall mortality rate and long-term morbidities [4,6,7]. In ~30e35% cases of PPHN, use of iNO iseither clinically ineffective or provides only transient improvement.Additionally, the escalating cost and need for special deliveryapparatus make it a non-viable option in many centers in thedeveloping world, where both the incidence and mortality associ-ated with PPHN is suspected to be higher. These considerationshave prompted clinicians to try other alternate/adjunctive pulmo-nary vasodilator therapies. With the discovery of other target me-diators, several therapeutic agents have been developed, many ofwhich are used routinely in clinical practice for children and adultswith PHT. Successful use of alternate drugs has been reported inmanagement of PPHN but their efficacy and safety have not beentested in large clinical trials (Fig. 5) [8,12,19,21,27]. Further, thereare no data available on the effect of these treatments on long-termneurodevelopmental outcomes. Although a short trial of alternatetherapeutic agents may be justified in settings where iNO is un-available or is ineffective, this should not delay transfer of patients
Fig. 5. Several alternate/adjunctive therapies have been developed based on identified celluthe only established vasodilatory therapies for infants with PPHN and should be used ainvestigation. Cgmp, cyclic guanyl monophosphate; PDE5, phosphodiesterase type 5; sGC,domized control trial.
to an ECMO facility for definitive management. One of the majordrawbacks of these therapies is the need for systemic administra-tion and, hence, higher potential of adverse effects. Caution shouldbe exercisedwhile administrating systemic vasodilator therapies asit may precipitate severe hypotension, which may worsen pulmo-nary blood flow as well as cardiac function. Recently, successful useof inhaled prostacyclin, administered as a continuous in-linenebulization, has been described in a case series of neonates withPPHN [10]. Although this raises the possibility of selective pulmo-nary administration of adjunctive therapy, it requires testing inrandomized trials.
4.5. Role of vasopressors in management of PPHN
One of the postulated mechanisms of HRF in neonates withPPHN is reduced PBF secondary to high PVR:SVR ratio resulting inshunting of blood away from the pulmonary circulation at theductal level. Hence in theory, if SVR is therapeutically increased, itmay reduce the PVR:SVR ratio and augment net PBF with a resul-tant improvement in ventilation perfusion mismatch and oxygen-ation. Historically, this strategy has been widely employed byclinicians when faced with clinical situations where therapies tolower PVR are unsuccessful. An ideal therapeutic agent to achievethe goal of reducing PVR:SVR ratio should increase SVR withsimultaneous reduction or at least having no effect on PVR. There isanimal experimental evidence that commonly used non-selectivevasopressor agents such as dopamine and epinephrine may in-crease SVR, but are unlikely to improve PBF due to their potentialvasoconstrictive effects on a labile pulmonary vascular bed [42];the net consequence of increased PVR is unaltered or theoreticallyaugmented PVR:SVR ratio, which would appear to be counter-intuitive clinically. A small case series evaluating the effect ofnorepinephrine in neonates with PPHN reported that althoughnorepinephrine caused an increase in both PVR and SVR, theincrement in PVRwas relatively less pronounced, causing an overalldecline in the PVR:SVR ratio which was clinically associated withimproved oxygenation [43]. Another agent with properties poten-tially suited to alter PVR:SVR ratio in PPHN is arginine vasopressin(AVP) [44]. It primarily exerts its vasoconstrictor effect by bindingto V1 receptors in the vascular smooth muscle and activating cal-cium channels. However, recent evidence suggests that effect ofAVP is not uniform across all vascular beds. Low-dose AVP has been
lar mediators involved in regulation of pulmonary vascular tone. Oxygen and iNO ares first-line therapies. Other therapeutic agents are currently under various stages ofsoluble guanylate cyclase; PDE3, phosphodiesterase type 3; ET, endothelin; RCT, ran-
A. Jain, P.J. McNamara / Seminars in Fetal & Neonatal Medicine 20 (2015) 262e271 269
shown to produce selective vasodilatation in coronary, cerebral,pulmonary, and renal vascular beds likely by stimulating release ofendothelial nitric oxide while causing vasoconstriction in othervascular beds [45]. Systemic AVP therapy is widely used in treat-ment of refractory vasodilatory shock in adults and pediatric pa-tients and more recently has been successfully used formanagement of refractory hypotension in extremely low birthweight infants [46,47]. In addition, a retrospective study of neo-nates with PPHN who were unresponsive to iNO therapy and whoreceived treatment with AVP (received iNO for �4 h with noimprovement in oxygenation) found a temporal association be-tween AVP treatment and improvement in oxygenation with theeffect starting within 3 h of initiating treatment [48]. Although AVP,by virtue of its biological properties, appears to be a promisingagent for use in PPHN, it needs further systematic prospectiveevaluation. In our experience, a targeted approach to physiologicmanagement is only effective in the setting of a patent ductusarteriosus with a right-to-left or bidirectional shunt, presumablysecondary to its contribution to reduced PBF.
4.6. Management of RV dysfunction
Integral to the management of RV dysfunction is the determi-nation of the relative contribution of altered RV loading conditionsversus impaired myocardial performance. In some situations, theapproach to treatment may include broad physiologic consider-ation. There are few clinical indicators of the adequacy of RV per-formance in neonates. Until recently direct visual assessment of RVperformance by echocardiography was the most widely usedmethod, but this is highly subjective and does not consider ven-tricular loading conditions. Novel techniques using tricuspidannular plane systolic excursion index, tissue Doppler imaging, andthe change in ventricular cavity fractional area can provide addi-tional insights into the adequacy of RV systolic performance, andnormative data have recently been described for neonates duringthe transitional period [49]. Treatment strategies for acute RVdysfunction are derived from the pathogenic entities outlined pre-viously. Major components include volume optimization, RV ino-tropy enhancement, and RV afterload reduction (Fig. 4). As RVperformance is highly volume dependent, it is important to correcthypovolemia as itmay limit the pulmonary bloodflow in a pressure-passive circulation. However, excessive augmentation of RV preloadmayhaveanegative impacton cardiac output by increasing leftwarddeviation of the interventricular septum, limiting LV filling.Adequate oxygenation and lung recruitment are important tominimize hypoxic pulmonary vasoconstriction episodes, whichfurther augment RV afterload and prohibit recovery of myocardialperformance. Due to potential adverse hemodynamic effects, me-chanical ventilation needs to be administered with caution andexpertise. Higher tidal volume and positive end-expiratory pressuremay increase pulmonary arterial pressure, worsen tricuspid regur-gitation, and increase RV afterload [50]. In addition, positive end-expiratory pressure may decrease RV pre-load by diminishingvenous return. The decision to provide support directly augmentingRV systolic performance versus reducing RV afterload is challenging.In the setting of high oxygen requirements and echocardiographyevidence of PPHN, initiation of iNO treatment to reduce RV afterloadwould appear prudent, although this has not been formally inves-tigated. Low-dose intravenous prostaglandin E1 should be consid-eredwhen the ductus arteriosus is closed or small andwhen there isevidence of impaired cardiac output. As discussed earlier, main-taining a right-to-left shunt across the fetal channelswill offload theRV and will augment systemic blood flow, albeit at the expense ofblood oxygenation. The selection of an inotrope to augment ven-tricular performance is dependent on systemic arterial pressure.
Dobutamine, the inotrope traditionallyused in cardiac pump failure,works through primarily b1-adrenoreceptor-mediated increases inmyocardial contractility and is the first-line agent in normotensivepatients. Concomitant stimulation of b1-adrenoreceptor stimula-tion in the systemic circulation induces vasodilation and decreasesafterload in a developmentally regulatedmanner [51]. In adultswithacute PH, there is evidence that low-dose dobutamine (2 to 5 mg/kg/min) increases CO and decreases PVR, whereas higher doses (5 to10 mg/kg/min) only induce tachycardia and increase myocardialoxygen consumption without further improvements in PAP [52].Higher doses of dobutamine might also impair diastolic functionand thus decrease ventricular filling. Milrinone, a selectivephosphodiesterase-3 (PDE3) inhibitor, also exerts inotropic andvasodilatory properties and improves diastolic performance [1].However, milrinone's inotropic effect might be developmentallyregulated because of the differential expression of phosphodies-terase isoforms between fetal and postnatal life [53]. Althoughdecreasing PVR and increasing RV systolic performance may bedesirable in the setting of a failing right ventricle and acute PPHN,milrinone's use in the immediate postnatal period is thus limited bysystemic vasodilation and hypotension. Like dobutamine, milrinonecan be combined with iNO to augment pulmonary vasodilationwhileminimizing hypotension and tachyarrhythmias. There is someexperimental evidence that, in the setting of 100% oxygen admin-istration, iNO upregulates PDE3 expression [54]. Theoretically co-administration of milrinone in this setting would appear to havebiological plausibility through augmenting cAMP-related pulmo-nary vasodilation. Epinephrine and/or norepinephrine increasesinotropy through b1-adrenoreceptor agonism. Concomitant stimu-lation of b1-adrenoreceptor increases RV perfusion pressure andcardiac output, but, according tofindings in the developing swine, itmight also increase in PVR and pulmonary artery pressure [55].Epinephrine. Finally, similar but not identical to the effects ofepinephrine are the cardiovascular actions of dopamine, anothervasopressor-inotrope often used in hypotensive neonates withPPHN in the clinical practice.
5. Role of targeted neonatal echocardiography in PPHN
Increasingly, neonatologists around the world are beginning touse bedside targeted neonatal echocardiography (TnECHO) orfunctional echocardiography to facilitate clinical decision-makingfor critically ill neonates in neonatal intensive care units [56,57].A TnECHO is an ultrasound scan of the heart focused on acquiringclinically relevant real-time hemodynamic information related tocardiovascular health of the newborn. A major benefit of TnECHO isthe ability to perform short longitudinal studies to help monitordisease progression and response to clinical interventions [58]. Asthe measurements are mostly obtained by physicians experiencedin performing and interpreting TnECHO and directly involved inpatient care, clinical integration of the acquired information iseasier. Complete technical details of TnECHO training and meth-odology are beyond the scope of this review and have beendescribed elsewhere [58]. Given the non-specific nature of symp-toms in neonates and low sensitivity and specificity of clinical signs,clinical integration of information obtained from a TnECHO studycan help establish diagnosis, define the true nature and severity ofthe associated physiological derangements and provide measuresto monitor response to treatments. As highlighted earlier, althoughPPHN is primarily a disorder of high PVR, it can be associated with anumber of secondary hemodynamic alterations of varying severity.Whereas in some patients high PVRmay be the only abnormality, inothers it may be complicated by reduced PBF, right and/or leftventricular dysfunction and low systemic blood flow and perfusionpressure. Further, in some patients, failure of improvement with

Table 1Use of targeted neonatal echocardiography in PPHN.a
Assessment of pulmonary artery resistance and pressure Assessment of impact on left heart functionand systemic circulation
Assessment of right heart function andpulmonary blood flow
Quantitative:Calculation of RV systolic pressure using modifiedBernoulli's equation from measurement of peakvelocity of TR or Doppler of PDA flow.
Semiquantitative:Monitor progress using serial measurements ofDoppler-derived time interval characteristics ofsystolic blood flow in main pulmonary artery e
pulmonary artery acceleration time and its ratiowith RV ejection time.
Qualitative:Estimation of RV systolic pressure in comparison tosystemic systolic pressure e interventricular septalpositioning at end systole; pattern of blood flowacross PDA and PFO.
LV preload:Subjective assessment of Doppler ofpulmonary venous flow and Doppler offlow across mitral valve in diastole.
LV contractility:Quantitative evaluation using well-establishedindices e fractional shortening, ejection fractionusing Simpson's biplane method and meanvelocity of circumferential fibre shorteningcorrected for heart rate; qualitative assessmentof contractility.
Systemic blood flow:Quantitative measurement of LV output andstroke distance in ascending aorta.
RV contractility:Quantitative evaluation using recentlydescribed indices e measurement oftricuspid annular plane systolic excursion,tissue Doppler-derived peak systolicmyocardial velocity at the base of theright ventricle and fractional area change;qualitative assessment of RV contractilityand dilatation.
Pulmonary blood flow:Quantitative measurement of RV outputand stroke distance in main pulmonaryartery.
TR, tricuspid regurgitation; PDA, patent ductus arteriosus; PFO, patent foramen ovale; LV, left ventricle; RV, right ventricle.a Reproduced with permission from Chapter 29, Avery's neonatology: pathophysiology and management of the newborn, 7th ed (in press).
Practice points
� Persistent pulmonary hypertension represents a failure of
the normal postnatal decline in pulmonary vascular
resistance, which should form the basis for therapeutic
interventions.
� Targeted neonatal echocardiography may provide novel
physiologic insights, particularly when standard-of-care
treatment options fail.
� Therapeutic strategies should focus on optimization of
lung recruitment, pulmonary vasodilation, and support-
ing cardiac output.
Research directions
� Need to investigate the mechanistic role of right ventric-
ular performance in refractory patients.
� Evidence for alternative therapies is limited to pharma-
cological and caseecontrol studies and, despite the
recognized logistical difficulties to perform well-designed
RCTs on neonates with PPHN, this should be another area
of future clinical research focus.
A. Jain, P.J. McNamara / Seminars in Fetal & Neonatal Medicine 20 (2015) 262e271270
vasodilator therapies may be because high PVR is truly unrespon-sive to treatment, whereas in others it may be due to absence ofsignificant PPHN, as the cause of HRF was parenchymal lung dis-ease. In addition, therapies not leading to immediate clinicalimprovement in oxygenation are often deemed as a ‘failure’. In ourexperience, TnECHO can facilitate identification of a subclinicalresponse, where there are measureable improvements in cardio-pulmonary indices even though the clinical picture does not changeimmediately. It is plausible that in such patients the use of physi-ologically appropriate adjunctive treatment may be a betterapproach than discontinuation of the therapy perceived to beineffective. The TnECHO assessment in neonates with PPHN and astructurally normal heart include: evaluation of pulmonary he-modynamics; assessment of impact on systemic circulation; andassessment of impact on right ventricular performance (Table 1). Itis important to be comprehensive, as any single echocardiographicmarker, when used in isolation, is unlikely to yield informationleading to clinical benefits. This problem is potentiated in neonates,due to the small size of the anatomic structures interrogated,therein increasing the possibility for erroneous results as well as ahigher degree of inter- and intra-observer variability. In addition,there is a lack of validation studies and normative data for some ofthe measurements in the neonate. Nevertheless, when the infor-mation gathered from TnECHO is integrated with the clinical situ-ation, it can provide significant physiological insights, allowingclinicians to take better-informed decisions. Accordingly, targetedneonatal echocardiography should be used to complement ratherthan replace clinical judgment.
6. Conclusion
In summary, PPHN is a widespread neonatal problem whosehallmark clinical feature is oxygenation failure, yet it represents aspectrum of physiologic contributors that must be considered whenmaking clinical decisions. Neonatal intensivists must recognize andfollow the standard therapeutic approach including the judicious useof oxygen, the administration of iNO and achievement of appropriatelung recruitment. It is equally important not to lose sight of thefundamental physiologic rationale, which forms the basis of thisapproach and is based on management of elevated PVR. The latter ismost relevant when considering alternative pulmonary vasodilatorsor drugs to support right ventricular performance. The use of TnECHOmay provide novel physiologic insights in patients who are criticallyill or refractory to standard approaches, enabling a more physiologi-cally relevant approach to therapeutic interventions.
Conflict of interest statement
None declared.
Funding sources
None.
References
[1] Jain A, McNamara PJ. Persistent pulmonary hypertension of the newborn:physiology, hemodynamic assessment and novel therapies. Curr Pediatr Rev2013;9:55e66.
[2] Jensen EA, Schmidt B. Epidemiology of bronchopulmonary dysplasia. BirthDefects Res 2014;100:145e57.
[3] Mourani PM, Abman SH. Pulmonary vascular disease in bronchopulmonarydysplasia: pulmonary hypertension and beyond. Curr Opin Pediatr 2013;25:329e37.
A. Jain, P.J. McNamara / Seminars in Fetal & Neonatal Medicine 20 (2015) 262e271 271
[4] Walsh-Sukys MC, Tyson JE, Wright LL, Bauer CR, Korones SB, Stevenson DK,et al. Persistent pulmonary hypertension of the newborn in the era beforenitric oxide: practice variation and outcomes. Pediatrics 2000;105(1 Pt 1):14e20.
[5] Lipkin PH, Davidson D, Spivak L, Straube R, Rhines J, Chang CT. Neuro-developmental and medical outcomes of persistent pulmonary hypertensionin term newborns treated with nitric oxide. J Pediatr 2002;140:306e10.
[6] Hosono S, Ohno T, Kimoto H, Shimizu M, Takahashi S, Harada K. Develop-mental outcomes in persistent pulmonary hypertension treated with nitricoxide therapy. Pediatrics Int 2009;51:79e83.
[7] Finer NN, Barrington KJ. Nitric oxide for respiratory failure in infants born at ornear term. Cochrane Database Syst Rev 2006;(4):CD000399.
[8] Gao Y, Raj JU. Regulation of the pulmonary circulation in the fetus andnewborn. Physiol Rev 2010;90:1291e335.
[9] Golzand E, Bar-Oz B, Arad I. Intravenous prostacyclin in the treatment ofpersistent pulmonary hypertension of the newborn refractory to inhaled ni-tric oxide. Isr Med Assoc J 2005;7:408e9.
[10] Kelly LK, Porta NF, Goodman DM, Carroll CL, Steinhorn RH. Inhaled prosta-cyclin for term infants with persistent pulmonary hypertension refractory toinhaled nitric oxide. J Pediatr 2002;141:830e2.
[11] Grimminger F, Weimann G, Frey R, Voswinckel R, Thamm M, B€olkow D, et al.First acute haemodynamic study of soluble guanylate cyclase stimulator rio-ciguat in pulmonary hypertension. Eur Resp J 2009;33:785e92.
[12] McNamara PJ, Shivananda SP, Sahni M, Freeman D, Taddio A. Pharmacology ofmilrinone in neonates with persistent pulmonary hypertension of thenewborn and suboptimal response to inhaled nitric oxide. Pediatr Crit CareMed 2013;14:74e84.
[13] McNamara PJ, Laique F, Muang-In S, Whyte HE. Milrinone improvesoxygenation in neonates with severe persistent pulmonary hypertension ofthe newborn. J Crit Care 2006;21:217e22.
[14] Shah PS, Ohlsson A. Sildenafil for pulmonary hypertension in neonates.Cochrane Database Syst Rev 2007;(3):CD005494.
[15] Krishnan U, Krishnan S, Gewitz M. Treatment of pulmonary hypertension inchildren with chronic lung disease with newer oral therapies. Pediatr Cardiol2008;29:1082e6.
[16] Nakwan N, Choksuchat D, Saksawad R, Thammachote P, Nakwan N. Successfultreatment of persistent pulmonary hypertension of the newborn withbosentan. Acta Paediatr 2009;98:1683e5.
[17] Firth AL, Yuan JX. Bringing down the ROS: a new therapeutic approach forPPHN. Am J Physiol Lung Cell Mol Physiol 2008;295:L976e8.
[18] Nossaman BD, Kadowitz PJ. The role of the RhoA/rhoekinase pathway inpulmonary hypertension. Curr Drug Discov Technol 2009;6:59e71.
[19] Fujita H, Fukumoto Y, Saji K, Sugimura K, Demachi J, Nawata J, et al. Acutevasodilator effects of inhaled fasudil, a specific Rho-kinase inhibitor, in pa-tients with pulmonary arterial hypertension. Heart Vess 2010;25:144e9.
[20] Members ATF, Gali�e N, Hoeper MM, Humbert M, Torbicki A, Vachiery JL, et al.Guidelines for the diagnosis and treatment of pulmonary hypertension: the TaskForce for the Diagnosis and Treatment of Pulmonary Hypertension of the Euro-pean Society of Cardiology (ESC) and the European Respiratory Society (ERS),endorsed by the International Society of Heart and Lung Transplantation (ISHLT).Eur Heart J 2009;30:2493e537.
[21] Haddad F, Hunt SA, Rosenthal DN, Murphy DJ. Right ventricular function incardiovascular disease. Part I: Anatomy, physiology, aging, and functionalassessment of the right ventricle. Circulation 2008;117:1436e48.
[22] Haddad F, Doyle R, Murphy DJ, Hunt SA. Right ventricular function in car-diovascular disease. Part II: pathophysiology, clinical importance, and man-agement of right ventricular failure. Circulation 2008;117:1717e31.
[23] Moenkemeyer F, Patel N. Right ventricular diastolic function measured bytissue Doppler imaging predicts early outcome in congenital diaphragmatichernia. Pediatr Crit Care Med 2014;15:49e55.
[24] Bogaard HJ, Abe K, Vonk Noordegraaf A, Voelkel NF. The right ventricle underpressure: cellular and molecular mechanisms of right-heart failure in pul-monary hypertension. Chest 2009;135:794e804.
[25] Ochikubo CG,Waffarn F, Turbow R, KanakriyehM. Echocardiographic evidenceof improved hemodynamics during inhaled nitric oxide therapy for persistentpulmonary hypertension of the newborn. Pediatr Cardiol 1997;18:282e7.
[26] Skinner JR, Hunter S, Hey EN. Haemodynamic features at presentation inpersistent pulmonary hypertension of the newborn and outcome. Archs DisChildh Fetal Neonatal Ed 1996;74:F26e32.
[27] Galie N, Torbicki A, Barst R, Dartevelle P, Haworth S, Higenbottam T, et al.Guidelines on diagnosis and treatment of pulmonary arterial hypertension.The Task Force on Diagnosis and Treatment of Pulmonary Arterial Hyper-tension of the European Society of Cardiology. Eur Heart J 2004;25:2243e78.
[28] Shiraishi H, Yanagisawa M. Pulsed Doppler echocardiographic evaluation ofneonatal circulatory changes. Br Heart J 1987;57:161e7.
[29] Grapsa J, Dawson D, Nihoyannopoulos P. Assessment of right ventricularstructure and function in pulmonary hypertension. J Cardiovasc Ultrasound2011;19:115e25.
[30] Rudski LG, Lai WW, Afilalo J, Hua L, Handschumacher MD, Chandrasekaran K,et al. Guidelines for the echocardiographic assessment of the right heart inadults: a report from the American Society of Echocardiography endorsed bythe European Association of Echocardiography, a registered branch of theEuropean Society of Cardiology, and the Canadian Society of Echocardiogra-phy. J Am Soc Echocardiogr 2010;23:685e713. quiz 786e8.
[31] Long WA. Structural cardiovascular abnormalities presenting as persistentpulmonary hypertension of the newborn. Clin Perinatol 1984;11:601e26.
[32] Brown KL, Miles F, Sullivan ID, Hoskote A, Verhulst L, Ridout DA, et al.Outcome in neonates with congenital heart disease referred for respiratoryextracorporeal membrane oxygenation. Acta Paediatr 2005;94:1280e4.
[33] Farrow KN, Wedgwood S, Lee KJ, Czech L, Gugino SF, Lakshminrusimha S, et al.Mitochondrial oxidant stress increases PDE5 activity in persistent pulmonaryhypertension of the newborn. Resp Physiol Neurobiol 2010;174:272e81.
[34] Rudolph AM, Yuan S. Response of the pulmonary vasculature to hypoxia andHþ ion concentration changes. J Clin Invest 1966;45:399e411.
[35] Lakshminrusimha S, Russell JA, Steinhorn RH, Swartz DD, Ryan RM, Gugino SF,et al. Pulmonary hemodynamics in neonatal lambs resuscitated with 21%, 50%,and 100% oxygen. Pediatr Res 2007;62:313e8.
[36] Lakshminrusimha S, Swartz DD, Gugino SF, Ma CX, Wynn KA, Ryan RM, et al.Oxygen concentration and pulmonary hemodynamics in newborn lambs withpulmonary hypertension. Pediatr Res 2009;66:539e44.
[37] Farrow KN, Lakshminrusimha S, Reda WJ, Wedgwood S, Czech L, Gugino SF, et al.Superoxide dismutase restores eNOS expression and function in resistance pul-monaryarteries fromneonatal lambswithpersistentpulmonaryhypertension.AmJ Physiol 2008;295:L979e87.
[38] Jankov RP, Lewis P, Kantores C, Ivanovska J, Xu EZ, Van Vliet T, et al. Perox-ynitrite mediates right-ventricular dysfunction in nitric oxide-exposed juve-nile rats. Free Rad Biol Med 2010;49:1453e67.
[39] UKCollaborativeECMOTrialGroup.UKcollaborative randomised trial ofneonatalextracorporeal membrane oxygenation. Lancet 1996;348(9020):75e82.
[40] DiBlasi RM, Myers TR, Hess DR. Evidence-based clinical practice guideline:inhaled nitric oxide for neonates with acute hypoxic respiratory failure. RespCare 2010;55:1717e45.
[41] Salguero KL, Cummings JJ. Inhaled nitric oxide and methemoglobin in full-term infants with persistent pulmonary hypertension of the newborn. Pul-mon Pharmacol Ther 2002;15:1e5.
[42] Sakamoto H, Takenoshita M, Asakura Y, Ibara S, Ikenoue T. Comparison ofcirculatory effects between arginine vasopressin (AVP) and dopamine inconscious newborn goats. J Vet Med Sci 1996;58:511e4.
[43] Tourneux P, Rakza T, Bouissou A, Krim G, Storme L. Pulmonary circulatoryeffects of norepinephrine in newborn infants with persistent pulmonary hy-pertension. J Pediatr 2008;153:345e9.
[44] Tayama E, Ueda T, Shojima T, Akasu K, Oda T, Fukunaga S, et al. Argininevasopressin is an ideal drug after cardiac surgery for the management of lowsystemic vascular resistant hypotension concomitant with pulmonary hy-pertension. Interact Cardiovasc Thoracic Surg 2007;6:715e9.
[45] Holmes CL, Patel BM, Russell JA, Walley KR. Physiology of vasopressin relevantto management of septic shock. Chest 2001;120:989e1002.
[46] Russell JA. Bench-to-bedside review: vasopressin in the management of septicshock. Crit Care 2011;15:226.
[47] Ikegami H, Funato M, Tamai H, Wada H, Nabetani M, Nishihara M. Low-dosevasopressin infusion therapy for refractory hypotension in ELBW infants.Pediatr Int 2010;52:368e73.
[48] Mohamed A, Nasef N, Shah V, McNamara PJ. Vasopressin as a rescue therapyfor refractory pulmonary hypertension in neonates: case series. Pediatr CritCare Med 2014;15:148e54.
[49] Jain A, Mohamed A, El-Khuffash A, Connelly KA, Dallaire F, Jankov RP, et al.A comprehensive echocardiographic protocol for assessing neonatal rightventricular dimensions and function in the transitional period: normativedata and Z scores. J Am Soc Echocardiogr 2014;27:1293e304.
[50] Jardin F, Vieillard-Baron A. Right ventricular function and positive pressureventilation in clinical practice: from hemodynamic subsets to respirator set-tings. Intensive Care Med 2003;29:1426e34.
[51] Noori S, Seri I. Neonatal blood pressure support: the use of inotropes, lusi-tropes, and other vasopressor agents. Clin Perinatol 2012;39:221e38.
[52] Kerbaul F, Rondelet B, Motte S, Fesler P, Hubloue I, Ewalenko P, et al. Effects ofnorepinephrine and dobutamine on pressure load-induced right ventricularfailure. Crit Care Med 2004;32:1035e40.
[53] Akita T, Joyner RW, Lu C, Kumar R, Hartzell HC. Developmental changes inmodulation of calcium currents of rabbit ventricular cells by phosphodies-terase inhibitors. Circulation 1994;90:469e78.
[54] Chen B, Lakshminrusimha S, Czech L, Groh BS, Gugino SF, Russell JA, et al.Regulation of phosphodiesterase 3 in the pulmonary arteries during theperinatal period in sheep. Pediatr Res 2009;66:682e7.
[55] Cheung PY, Barrington KJ. The effects of dopamine and epinephrine on he-modynamics and oxygen metabolism in hypoxic anesthetized piglets. CritCare 2001;5:158e66.
[56] Mertens L, Seri I, Marek J, Arlettaz R, Barker P, McNamara P, et al. Targetedneonatal echocardiography in the neonatal intensive care unit: practiceguidelines and recommendations for training. Writing Group of the AmericanSociety of Echocardiography (ASE) in collaboration with the European Asso-ciation of Echocardiography (EAE) and the Association for European PediatricCardiologists (AEPC). J Am Soc Echocardiogr 2011;24:1057e78.
[57] El-Khuffash A, Herbozo C, Jain A, Lapointe A, McNamara PJ. Targeted neonatalechocardiography (TnECHO) service in a Canadian neonatal intensive careunit: a 4-year experience. J Perinatol 2013;33:687e90.
[58] El-Khuffash AF, McNamara PJ. Neonatologist-performed functional echocar-diography in the neonatal intensive care unit. Semin Fetal Neonat Med2011;16:50e60.