Embed Size (px)
Citation preview
Supplement to Podiatry Today® and Vascular Disease Management® Preventing Critical Limb Ischemia 1
Preventing Critical Limb IschemiaExperts Discuss Podiatric and Cardiovascular Interdisciplinary Care
Supported by
Supplement to Vascular Disease Management®
Cannot be reprinted without
permission of HMP Communications
2 Preventing Critical Limb Ischemia Supplement to Podiatry Today® and Vascular Disease Management®
Introduction: A Primer on Critical Limb IschemiaJoseph Caporusso, DPM ..................................................................................................................... pg. 3
New Treatment Paradigm: The Angiosome ConceptKanwar P. Singh, MD, FACC .............................................................................................................. pg. 4
Holistic Patient Management: Working With an InterventionalistPeter A. Soukas, MD, FACC, FSVM, FSCAI, RPVI, and Harold B. Glickman, DPM ...................................... pg. 8
Amputation Prevention: A Multidisciplinary ApproachJ. A. Mustapha, MD, FACC, FSCAI; Desmond Bell, DPM, CWS; Yazan Khatib, MD, FACC, FSCAI, FSVMB, FABVM; Fadi Saab, MD; Carmen M. Heaney, BSN, RN, CCRC, CIP ........................................................ pg. 12
Diagnosing CLI: The Role of the PodiatristJoseph Caporusso, DPM ..................................................................................................................... pg.18
Comprehensive Wound Care ManagementRasesh M. Shah, MD, FACS, and John Steinberg, DPM, FACFAS ............................................................... pg. 21
Desmond Bell, DPM, CWSExecutive Director, Save A Leg, Save A Life FoundationCEO, Limb Salvage InstituteJacksonville, FL
Joseph Caporusso, DPMChairmanPAD CoalitionMcAllen, TX
Harold B. Glickman, DPMPast President, American Podiatric Medical AssociationChairman Dept. Podiatric SurgerySibley Memorial Hospital Washington, DC
Carmen M. Heaney, BSN, RN, CCRC, CIPDirector of Clinical ResearchMetro Health Hospital Wyoming, MI
Yazan Khatib, MD, FACC, FSCAI, FSVMB, FABVMCo-Founder, First Coast Cardiovascular InstituteCo-Founder, Save A Leg, Save A Life Founda-tionJacksonville, FL
J. A. Mustapha, MD, FACC, FSCAIDirector of Endovascular InterventionsDirector of Cardiovascular Research Metro Health HospitalWyoming, MI
Fadi Saab, MDMetro Heart & VascularWyoming, MI
Rasesh M. Shah, MD, FACSSentara Vascular SpecialistsVirginia Beach, VA
Kanwar P. Singh, MD, FACCAssistant Professor of MedicineDirector, Vascular Medicine and InterventionCo-Director, Interventional CardiologyUniversity of Connecticut Health CenterFarmington, CT
Peter A. Soukas, MD, FACC, FSVM, FSCAI, RPVIDirector, Vascular Medicine and Interventional Peripheral Vascular LabDirector, Brown Vascular & Endovascular MedicineFellowship ProgramAssistant Professor of MedicineWarren Alpert School of Medicine of Brown UniversityThe Miriam and Rhode Island HospitalsProvidence, RI
John Steinberg, DPM, FACFASAssociate Professor/Department of Plastic SurgeryCo-Director, Center for Wound HealingGeorgetown University School of Medicine Georgetown University Hospital Washington, DC
Authors
Table of Contents
Disclaimer: The authors of the articles contained in this Supplement to Podiatry Today® and Vascular Disease Management® are paid consultants for Cordis Corporation. These articles contain the techniques, approaches and opinions of the individual authors. It does not constitute recommendations or medical advice of Cordis Corporation. Cordis does not provide medical advice. Cordis has no independent knowledge concerning the information contained in any of the articles, and the studies, findings and conclusions expressed are those reached by the authors. This Cordis-sponsored publication is not intended to be used as a training guide. Before using any medical device, please review all relevant package inserts with particular attention to the indications, contraindica-tions, warnings and precautions, and steps for use of the device(s).
Cannot be reprinted without
permission of HMP Communications
Supplement to Podiatry Today® and Vascular Disease Management® Preventing Critical Limb Ischemia 3
Lower-extremity peripheral artery disease (PAD) is a major health concern worldwide. PAD prevalence has been estimated to be between 4.3% and 29%.1–5 Older populations have higher rates of PAD and, in most age
groups, males have higher PAD rates than females.3
PAD natural history includes asymptomatic PAD, atypical leg pain, claudication and critical limb ischemia (CLI). CLI presents in 1–2% of the PAD population and is defined as ischemic rest pain, nonhealing wounds or gangrene.6,7 The degree and developmen-tal chronicity of CLI determine patients’ clinical manifestations. The Rutherford and Fontaine clinical classification systems offer insight into ischemic classification and limb salvageability. CLI presents with multifocal areas of occlusion in a lower extremity’s arterial tree; the disease process is usually symmetrical.
CLI is most commonly caused by obstructive atheroscle-rotic arterial disease. Other causes include atheroembolic or thromboembolic disease, trauma, and vasculitis. Disease chronicity plays a role in CLI’s formation instead of acute limb ischemia’s. Conditions such as diabetes and severe low-cardiac output reduce blood flow to the microvascular beds and can exacerbate or contribute to CLI development.
CLI is associated with very high intermediate-term mor-bidity and mortality. Patients with PAD are at 3 to 5 times greater risk of cardiovascular mortality than those without PAD.7 Advanced PAD and CLI greatly increase the risk of cardiovascular ischemic events. Given that this devastating disease can — and, in many cases, will — end in primary amputation, early detection and intervention are crucial.
The ischemic rest pain associated with CLI typically occurs at night and continuously in more severe cases. Patients will often present with a history of pain while asleep and waking to massage the foot and/or walk around the room to try to achieve relief. In some cases, partial relief occurs with dependency of the limb. When patients with pain have reached a point where the pain does not permit sleep in a supine position, their general physical and psychological conditions further decline.
Ischemic ulceration is an ominous sign in CLI. Ischemic ulcer-ations have vastly different presentations than neuropathic ulcer-ations. Instead of the healthy, granular base seen with neuropathic ulceration, ischemic ulceration presents with a necrotic/fibrotic base. The hyperkeratotic covering or rim is also absent and has a more “punched out” appearance.
Gangrene is the end-stage of tissue loss. This is the most feared complication of CLI due to the treatment indicated for this pro-
cess. Amputation before or after revascularization is most likely needed. The literature has highlighted the downward spiral that occurs after that first pedal amputation.8 The stresses and increased pressures applied to the contralateral limb after amputation puts the remaining extremity at an increased risk for amputation. For these reasons, it’s extremely important that the length of the am-putated limb be preserved as distally as possible. The energy the patient needs to ambulate greatly increases as the amputation level becomes more proximal. Patients are increasingly aware of the sequelae and are demanding limb salvage at all costs.
The devastating effects of CLI warrant a team approach to its evaluation and treatment. The podiatrist working with the vas-cular specialist can increase the chance of limb salvage and lessen the horrific consequences of CLI. Appropriate revascularization of the affected limb — along with appropriate wound care, de-bridement and/or lesser amputation — can let the patient func-tion very close to his/her normal level. n
References
1. Selvin E, Erlinger TP. Prevalence of and risk factors for peripheral arterial disease in the United States: results from the National Health and Nutrition Examination Survey, 1999-2000. Circulation. 2004;110(6):738–743.
2. Criqui MH, Fronek A, Barrett-Connor E, et al. The prevalence of periph-eral arterial disease in a defined population. Circulation. 1985;71(3):510–515.
3. Diehm C, Schuster A, Allenberg JR, et al. High prevalence of peripheral ar-terial disease and comorbidity in 6880 primary care patients: cross-sectional study. Atherosclerosis. 2004;172(1):95–105.
4. Meijer WT, Hoes AW, Rutgers D, et al. Peripheral arterial disease in the el-derly: The Rotterdam Study. Arterioscler Thromb Vasc Biol. 1998;18(2):185–192.
5. Hirsch AT, Criqui MH, Treat-Jacobson D, et al. Peripheral arterial dis-ease detection, awareness, and treatment in primary care. JAMA. 2001;286(11):1317–1324.
6. Dormandy JA, Rutherford RB. Management of peripheral arterial dis-ease (PAD). TASC Working Group. TransAtlantic Inter-Society Consensus (TASC). J Vasc Surg. 2000;31(1 Pt 2):S1–S296.
7. Hirsch AT, Haskal ZJ, Hertzer NR, et al; American Association for Vascular Sur-gery; Society for Vascular Surgery; Society for Cardiovascular Angiography and In-terventions; Society for Vascular Medicine and Biology; Society of Interventional Radiology; ACC/AHA Task Force on Practice Guidelines; American Association of Cardiovascular and Pulmonary Rehabilitation; National Heart, Lung, and Blood In-stitute; Society for Vascular Nursing; TransAtlantic Inter-Society Consensus; Vascular Disease Foundation. ACC/AHA 2005 guidelines for the management of patients with peripheral arterial disease (lower extremity, renal, mesenteric, and abdominal aortic): executive summary a collaborative report from the American Association for Vascular Surgery/Society for Vascular Surgery, Society for Cardiovascular Angi-ography and Interventions, Society for Vascular Medicine and Biology, Society of Interventional Radiology, and the ACC/AHA Task Force on Practice Guidelines (Writing Committee to Develop Guidelines for the Management of Patients With Peripheral Arterial Disease) endorsed by the American Association of Cardiovascular and Pulmonary Rehabilitation; National Heart, Lung, and Blood Institute; Society for Vascular Nursing; TransAtlantic Inter-Society Consensus; and Vascular Disease Foundation. J Am Coll Cardiol. 2006;47(6):1239–1312.
8. Izumi Y, Satterfield K, Lee S, Harkless LB. Risk of reamputation in diabetic patients stratified by limb and level of amputation: a 10-year observation. Diabetes Care. 2006;29(3):566–570.
Introduction: A Primer on Critical Limb IschemiaJoseph Caporusso, DPM
Cannot be reprinted without
permission of HMP Communications

4 Preventing Critical Limb Ischemia Supplement to Podiatry Today® and Vascular Disease Management®
As discussed throughout this supplement, critical limb ischemia (CLI) is the most severe form of peripheral arterial disease (PAD). It occurs when the resting metabolic need of tissue is not met by
the arterial supply. The anatomic substrate of CLI typically consists of severe, multi-level occlusive or stenotic athero-sclerotic disease, including combinations of aorto-iliac, fem-oral, popliteal and tibial vessels. The conditions of patients with CLI are typically complicated by medically significant comorbidities including advanced age, diabetes, renal insuf-ficiency, coronary artery disease, and cerebrovascular disease, among others. Such patients are at increased risk of surgi-cal revascularization complications, rendering percutaneous options more attractive. However, these same medical issues may complicate percutaneous revascularization.
Taylor and Palmer published the angiosome concept in 1987,1 describing a three-dimensional model of human anatomy segregated into 40 blocks of tissue fed by source ar-teries. Its initial clinical application was centered on healing surgical graft sites for operative wounds and plastic surgery reconstructions. More recently, the angiosome concept has been shown to help successfully guide tibial vessel selection in optimizing revascularization strategies for surgical and en-dovascular CLI therapies.
The angiosome concept is part of a new paradigm in the treatment of CLI that aims to simplify these com-plex cases and gives the vascular specialist a framework to guide therapies.
Traditional Approach to CLIThe first issue in treating CLI is determining the acuity of
the clinical scenario. In truly acute presentations, it’s urgent that patency of the affected vessels be restored. With subacute or more chronic presentations, the traditional approach has been to consider staged or sequential revascularizations, fo-cusing first on inflow and subsequently on infrainguinal and infrapopliteal lesions.
Indeed, the 2011 American College of Cardiology/Amer-ican Heart Association update to the guidelines for manag-ing patients with PAD suggests that patients with CLI should undergo outflow interventions only after an incomplete re-sponse to inflow therapy, a recommendation carried over from the 2005 document. This recommendation is afforded
Class I status despite having the lowest caliber of evidence (Level C, expert opinion).2
However, staged vascular procedures carry additional risks: vascular access, sedation, contrast, radiation, healthcare costs, and disruption of patient’s lives. Additionally, patients are (appropriately) often reluctant to accept a wait-and-see approach and wish for definitive procedures. So in many cases, I choose to optimize the endovascular treatment with a single procedure to re-establish inflow and the key tibial vessel. The angiosome model drives the choice of tibial run-off target.
The Angiosome ModelThe human body has been divided into 40 discrete angio-
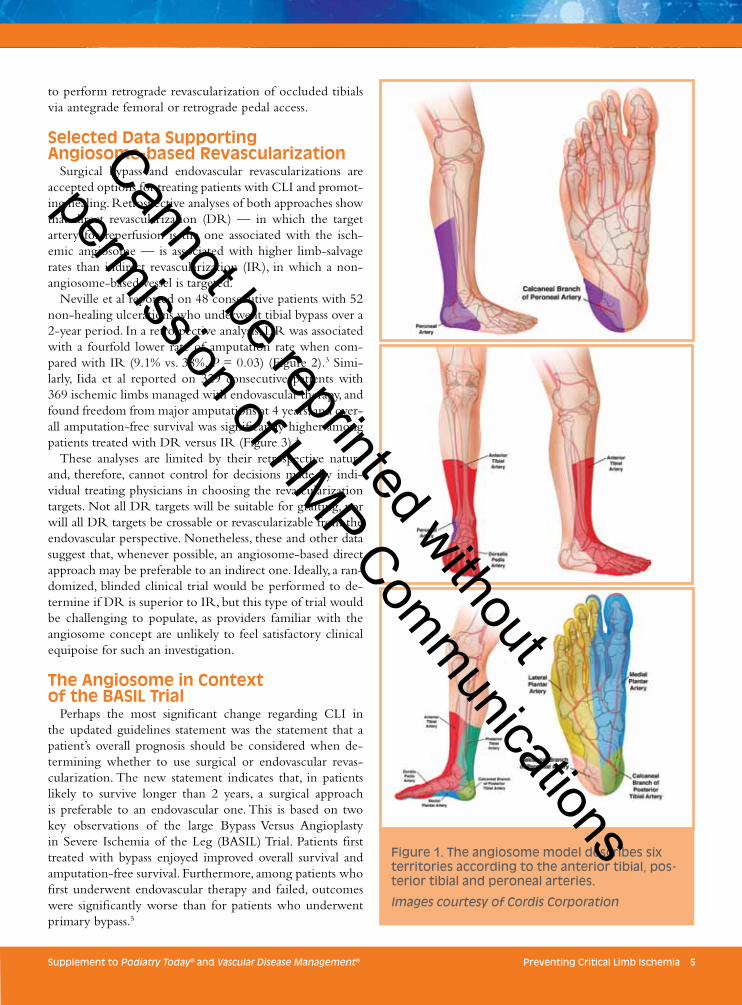
somes. With regard to foot ulcerations, six territories are de-scribed according to the anterior tibial (ATA), posterior tibial (PTA) and peroneal (PA) arteries (see Figure 1 on page 5).
The ATA arises from the popliteal artery and courses an-terolaterally in the anterior compartment, then crosses the dorsal aspect of the shin and over the ankle joint, where it becomes the familiar dorsalis pedis (DP) pulse. With this anatomic path in mind, it becomes easy to identify the an-terior tibial angiosome.
The popliteal artery continues after the ATA separates and becomes the tibioperoneal trunk (TPT). From here, the TPT divides into the PTA and PA. The PTA travels in the deep posterior compartment and follows the medial aspect of the tibia. It tucks behind the medial malleolus, where it’s typically identified on exam, and wraps along the plantar surface of the heel. Under the heel, it gives off medial calcaneal branches, and then divides into a medial plantar and lateral plantar arteries. These two arteries feed the plantar aspect of the foot (Figure 1).
The PA is the other branch of the TPT, running along the posterior side of the fibula in the superficial posterior compartment. As it terminates at the ankle, it gives off lat-eral calcaneal branches for its own angiosome distribution, as well as named collaterals that perfuse the AT and PTA. One of the PA’s key aspects is that it’s the most in-line con-tinuation of the popliteal artery. When the popliteal artery is occluded and there are no visible tibial targets, crossing catheters and wires will most commonly enter the PA, al-lowing revascularization. PA collaterals can at times be used
New Treatment Paradigm: The Angiosome ConceptKanwar P. Singh, MD, FACC
Cannot be reprinted without
permission of HMP Communications
Supplement to Podiatry Today® and Vascular Disease Management® Preventing Critical Limb Ischemia 5
to perform retrograde revascularization of occluded tibials via antegrade femoral or retrograde pedal access.
Selected Data Supporting Angiosome-based Revascularization
Surgical bypass and endovascular revascularizations are accepted options for treating patients with CLI and promot-ing healing. Retrospective analyses of both approaches show that direct revascularization (DR) — in which the target artery for reperfusion is the one associated with the isch-emic angiosome — is associated with higher limb-salvage rates than indirect revascularization (IR), in which a non-angiosome-based vessel is targeted.
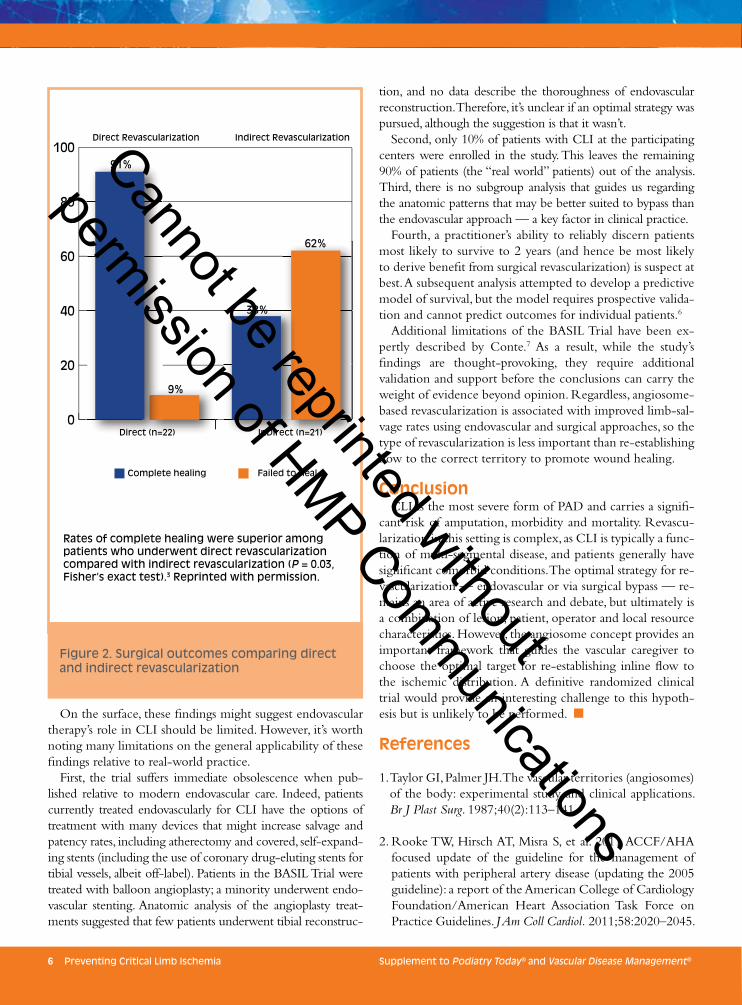
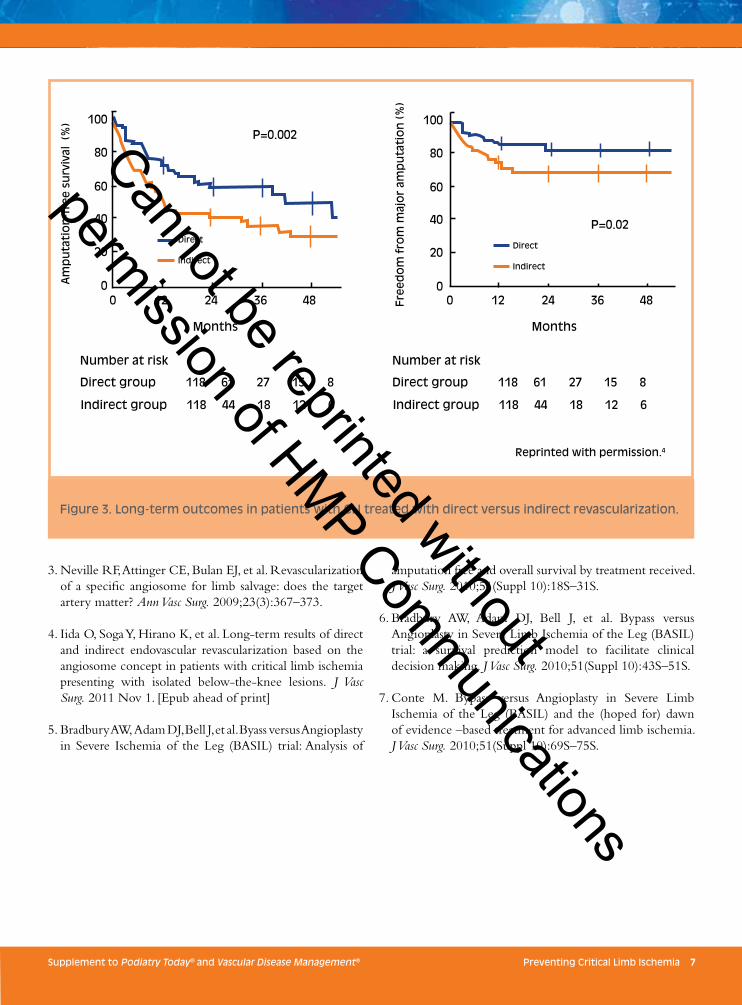
Neville et al reported on 48 consecutive patients with 52 non-healing ulcerations who underwent tibial bypass over a 2-year period. In a retrospective analysis, DR was associated with a fourfold lower rate of amputation rate when com-pared with IR (9.1% vs. 38%, P = 0.03) (Figure 2).3 Simi-larly, Iida et al reported on 329 consecutive patients with 369 ischemic limbs managed with endovascular therapy, and found freedom from major amputations at 4 years, and over-all amputation-free survival was significantly higher among patients treated with DR versus IR (Figure 3).4
These analyses are limited by their retrospective nature and, therefore, cannot control for decisions made by indi-vidual treating physicians in choosing the revascularization targets. Not all DR targets will be suitable for grafting, nor will all DR targets be crossable or revascularizable from the endovascular perspective. Nonetheless, these and other data suggest that, whenever possible, an angiosome-based direct approach may be preferable to an indirect one. Ideally, a ran-domized, blinded clinical trial would be performed to de-termine if DR is superior to IR, but this type of trial would be challenging to populate, as providers familiar with the angiosome concept are unlikely to feel satisfactory clinical equipoise for such an investigation.
The Angiosome in Context of the BASIL Trial
Perhaps the most significant change regarding CLI in the updated guidelines statement was the statement that a patient’s overall prognosis should be considered when de-termining whether to use surgical or endovascular revas-cularization. The new statement indicates that, in patients likely to survive longer than 2 years, a surgical approach is preferable to an endovascular one. This is based on two key observations of the large Bypass Versus Angioplasty in Severe Ischemia of the Leg (BASIL) Trial. Patients first treated with bypass enjoyed improved overall survival and amputation-free survival. Furthermore, among patients who first underwent endovascular therapy and failed, outcomes were significantly worse than for patients who underwent primary bypass.5
Figure 1. The angiosome model describes six territories according to the anterior tibial, pos-terior tibial and peroneal arteries.
Images courtesy of Cordis Corporation
Cannot be reprinted without
permission of HMP Communications
6 Preventing Critical Limb Ischemia Supplement to Podiatry Today® and Vascular Disease Management®
On the surface, these findings might suggest endovascular therapy’s role in CLI should be limited. However, it’s worth noting many limitations on the general applicability of these findings relative to real-world practice.
First, the trial suffers immediate obsolescence when pub-lished relative to modern endovascular care. Indeed, patients currently treated endovascularly for CLI have the options of treatment with many devices that might increase salvage and patency rates, including atherectomy and covered, self-expand-ing stents (including the use of coronary drug-eluting stents for tibial vessels, albeit off-label). Patients in the BASIL Trial were treated with balloon angioplasty; a minority underwent endo-vascular stenting. Anatomic analysis of the angioplasty treat-ments suggested that few patients underwent tibial reconstruc-
tion, and no data describe the thoroughness of endovascular reconstruction. Therefore, it’s unclear if an optimal strategy was pursued, although the suggestion is that it wasn’t.
Second, only 10% of patients with CLI at the participating centers were enrolled in the study. This leaves the remaining 90% of patients (the “real world” patients) out of the analysis. Third, there is no subgroup analysis that guides us regarding the anatomic patterns that may be better suited to bypass than the endovascular approach — a key factor in clinical practice.
Fourth, a practitioner’s ability to reliably discern patients most likely to survive to 2 years (and hence be most likely to derive benefit from surgical revascularization) is suspect at best. A subsequent analysis attempted to develop a predictive model of survival, but the model requires prospective valida-tion and cannot predict outcomes for individual patients.6
Additional limitations of the BASIL Trial have been ex-pertly described by Conte.7 As a result, while the study’s findings are thought-provoking, they require additional validation and support before the conclusions can carry the weight of evidence beyond opinion. Regardless, angiosome-based revascularization is associated with improved limb-sal-vage rates using endovascular and surgical approaches, so the type of revascularization is less important than re-establishing flow to the correct territory to promote wound healing.
ConclusionCLI is the most severe form of PAD and carries a signifi-
cant risk of amputation, morbidity and mortality. Revascu-larization in this setting is complex, as CLI is typically a func-tion of multi-segmental disease, and patients generally have significant comorbid conditions. The optimal strategy for re-vascularization — endovascular or via surgical bypass — re-mains an area of active research and debate, but ultimately is a combination of lesion, patient, operator and local resource characteristics. However, the angiosome concept provides an important framework that guides the vascular caregiver to choose the optimal target for re-establishing inline flow to the ischemic distribution. A definitive randomized clinical trial would provide an interesting challenge to this hypoth-esis but is unlikely to be performed. n
References
1. Taylor GI, Palmer JH. The vascular territories (angiosomes) of the body: experimental study and clinical applications. Br J Plast Surg. 1987;40(2):113–141.
2. Rooke TW, Hirsch AT, Misra S, et al. 2011 ACCF/AHA focused update of the guideline for the management of patients with peripheral artery disease (updating the 2005 guideline): a report of the American College of Cardiology Foundation/American Heart Association Task Force on Practice Guidelines. J Am Coll Cardiol. 2011;58:2020–2045.
0
20
40
60
80
100Direct Revascularization Indirect Revascularization
91%
9%
62%
38%
Direct (n=22) InDirect (n=21)
Complete healing Failed to heal
Figure 2. Surgical outcomes comparing direct and indirect revascularization
Rates of complete healing were superior among patients who underwent direct revascularization compared with indirect revascularization (P = 0.03, Fisher’s exact test).3 Reprinted with permission.
Cannot be reprinted without
permission of HMP Communications
Supplement to Podiatry Today® and Vascular Disease Management® Preventing Critical Limb Ischemia 7
3. Neville RF, Attinger CE, Bulan EJ, et al. Revascularization of a specific angiosome for limb salvage: does the target artery matter? Ann Vasc Surg. 2009;23(3):367–373.
4. Iida O, Soga Y, Hirano K, et al. Long-term results of direct and indirect endovascular revascularization based on the angiosome concept in patients with critical limb ischemia presenting with isolated below-the-knee lesions. J Vasc Surg. 2011 Nov 1. [Epub ahead of print]
5. Bradbury AW, Adam DJ, Bell J, et al. Byass versus Angioplasty in Severe Ischemia of the Leg (BASIL) trial: Analysis of
amputation free and overall survival by treatment received. J Vasc Surg. 2010;51(Suppl 10):18S–31S.
6. Bradbury AW, Adam DJ, Bell J, et al. Bypass versus Angioplasty in Severe Limb Ischemia of the Leg (BASIL) trial: a survival prediction model to facilitate clinical decision making. J Vasc Surg. 2010;51(Suppl 10):43S–51S.
7. Conte M. Bypass versus Angioplasty in Severe Limb Ischemia of the Leg (BASIL) and the (hoped for) dawn of evidence –based treatment for advanced limb ischemia. J Vasc Surg. 2010;51(Suppl 10):69S–75S.
P=0.002
P=0.02
MonthsMonths
Fre
ed
om
fro
m m
ajo
r am
pu
tati
on
(%
)
Direct
Indirect
100
80
60
40
20
00 12 24 36 48
Direct
Indirect
Am
pu
tati
on
-fre
e s
urv
ival
(%
) 100
80
60
40
20
00 12 24 36 48
Number at risk
Direct group 118 61 27 15 8
Indirect group 118 44 18 12 6
Number at risk
Direct group 118 61 27 15 8
Indirect group 118 44 18 12 6
Reprinted with permission.4
Figure 3. Long-term outcomes in patients with CLI treated with direct versus indirect revascularization.
Cannot be reprinted without
permission of HMP Communications
8 Preventing Critical Limb Ischemia Supplement to Podiatry Today® and Vascular Disease Management®
Critical limb ischemia (CLI) results from severe com-promise of blood flow to the affected extremity and manifests as rest pain, ulceration or gangrene. It’s usually caused by multi-segmental obstructive
atherosclerosis, but may be caused by atheroembolic, throm-boembolic or vasculitic disease (Table 1). With the stagger-ing increase in the number of CLI cases, primarily due to smoking and the diabetes pandemic, it’s vital that a dedicated multidisciplinary team treat patients to save limbs and lives. A successful team should feature a strong partnership between the podiatrist and the interventionalist.
Scope of the ProblemIn 2003, more than 2.5 million Americans had CLI, and
there were more than 240,000 amputations in the United States and Europe.1 Primary amputation was the initial treat-ment in 67% of these patients and, surprisingly, 50% were performed without angiography or even an ABI.1
Risk factors for developing CLI include age (older than 65), hypertension, hyperlipidemia and abnormal ABI. The most lethal risk factors for CLI are smoking and diabetes. The number of cases of diabetes mellitus (DM) has swelled from 30 million to 230 million in the last 20 years. Diabetes increases CLI risk fourfold; smoking triples the risk.2 Dia-betic patients with CLI are 10 times more likely to require amputation than non-diabetics.3 Worldwide, a limb is lost every 30 seconds to diabetes.4
Fate of the CLI PatientThe CLI patient faces a poor prognosis, principally due
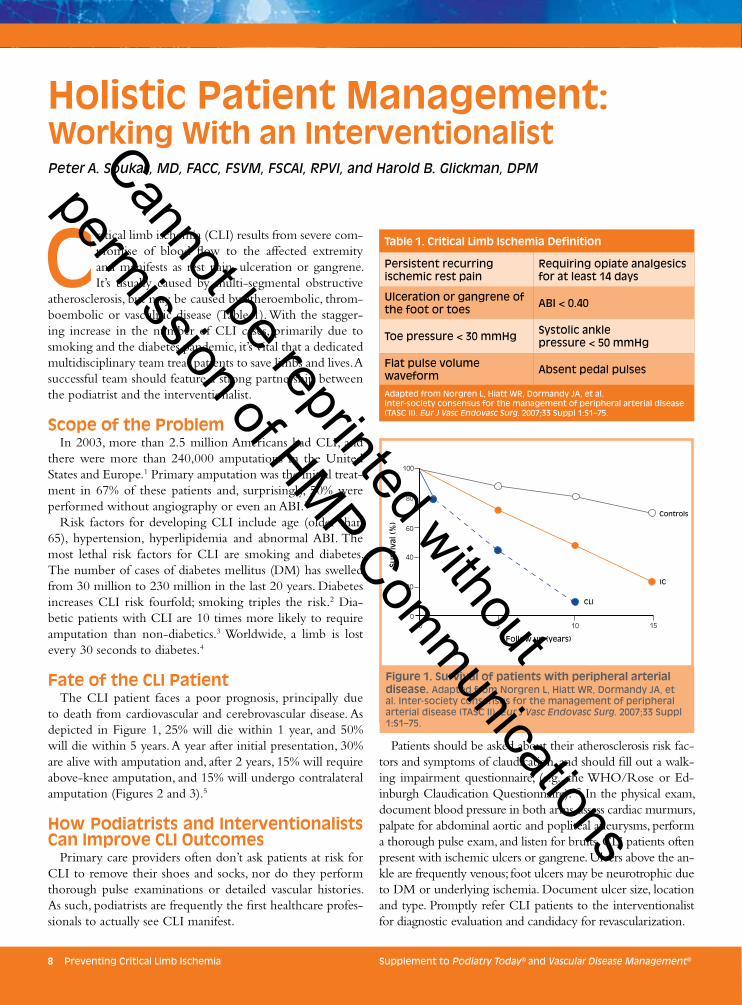
to death from cardiovascular and cerebrovascular disease. As depicted in Figure 1, 25% will die within 1 year, and 50% will die within 5 years. A year after initial presentation, 30% are alive with amputation and, after 2 years, 15% will require above-knee amputation, and 15% will undergo contralateral amputation (Figures 2 and 3).5
How Podiatrists and Interventionalists Can Improve CLI Outcomes
Primary care providers often don’t ask patients at risk for CLI to remove their shoes and socks, nor do they perform thorough pulse examinations or detailed vascular histories. As such, podiatrists are frequently the first healthcare profes-sionals to actually see CLI manifest.
Patients should be asked about their atherosclerosis risk fac-tors and symptoms of claudication, and should fill out a walk-ing impairment questionnaire, (e.g., the WHO/Rose or Ed-inburgh Claudication Questionnaire).6,7 In the physical exam, document blood pressure in both arms, assess cardiac murmurs, palpate for abdominal aortic and popliteal aneurysms, perform a thorough pulse exam, and listen for bruits. CLI patients often present with ischemic ulcers or gangrene. Ulcers above the an-kle are frequently venous; foot ulcers may be neurotrophic due to DM or underlying ischemia. Document ulcer size, location and type. Promptly refer CLI patients to the interventionalist for diagnostic evaluation and candidacy for revascularization.
Holistic Patient Management: Working With an InterventionalistPeter A. Soukas, MD, FACC, FSVM, FSCAI, RPVI, and Harold B. Glickman, DPM
100
80
60
40
20
00 5 10 15
Controls
CLI
IC
Surv
ival
(%
)
Follow up (years)
Figure 1. Survival of patients with peripheral arterial disease. Adapted from Norgren L, Hiatt WR, Dormandy JA, et al. Inter-society consensus for the management of peripheral arterial disease (TASC II). Eur J Vasc Endovasc Surg. 2007;33 Suppl 1:S1–75.
Table 1. Critical Limb Ischemia Definition
Persistent recurring ischemic rest pain
Requiring opiate analgesics for at least 14 days
Ulceration or gangrene of the foot or toes ABI < 0.40
Toe pressure < 30 mmHg Systolic ankle pressure < 50 mmHg
Flat pulse volumewaveform Absent pedal pulses
Adapted from Norgren L, Hiatt WR, Dormandy JA, et al. Inter-society consensus for the management of peripheral arterial disease (TASC II). Eur J Vasc Endovasc Surg. 2007;33 Suppl 1:S1–75.
Cannot be reprinted without
permission of HMP Communications

Supplement to Podiatry Today® and Vascular Disease Management® Preventing Critical Limb Ischemia 9
Diagnostic EvaluationDiagnostic evaluation usually begins with an ankle-brachial
index (ABI). Evaluate toe pressure or transcutaneous oxygen tension in patients for whom ABI may be unreliable (e.g., those with medial calcinosis, DM or renal failure). Reduced ABI has been shown to be a powerful predictor of future cardiovascular events; the lower the ABI, the higher the risk.8 Duplex ultra-sound and pulse volume recordings are useful for defining the severity and level of disease, and to plan intervention. CT and magnetic resonance angiographies can better evaluate aorto-iliac and distal infrapopliteal diseases, respectively. If the patient is deemed a candidate for revascularization, angiography can be used to confirm the diagnosis and define treatment options.
Treatment of CLIThe primary goals of CLI treatment are to relieve ischemic
pain, heal ulcers, prevent limb loss, and improve function and
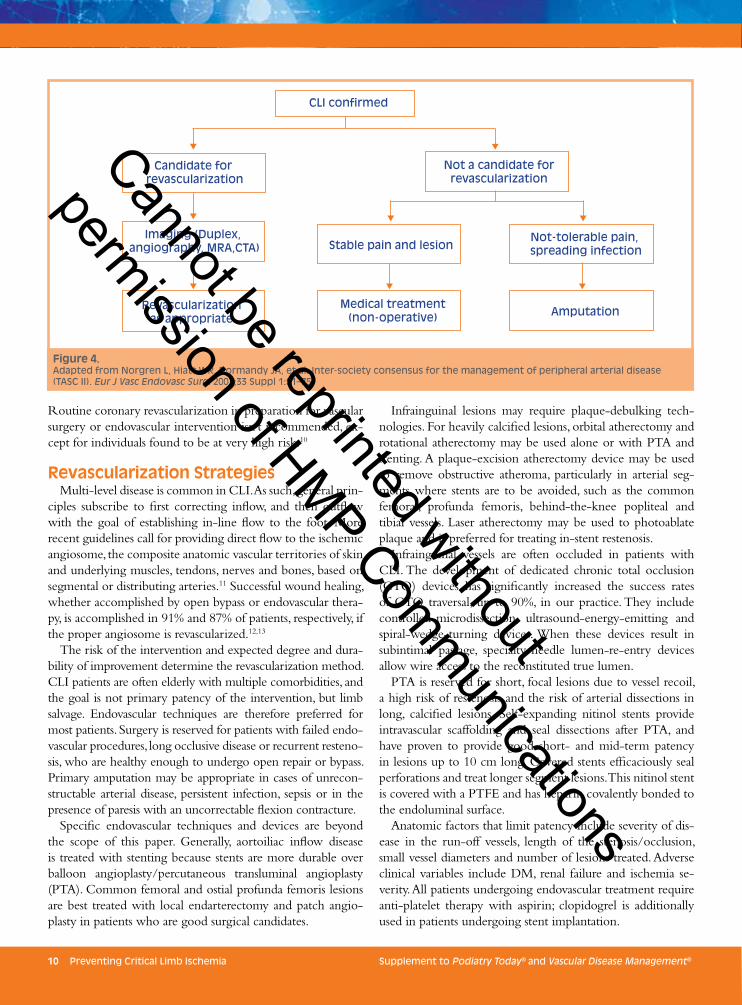
quality of life for the patient. CLI patients who develop cellu-litis or spreading infection require systemic antibiotic therapy. Figure 4 presents a general treatment algorithm for the CLI patient. Podiatrists are vital to implementing limb-loss preven-tion strategies including: education about self-care of the feet; provision of conforming orthotics and shoes; and aggressive wound care, such as debridement, dressings and skin grafting.
Before revascularization, all patients should undergo risk-factor modification, such as smoking cessation, statin therapy to reduce LDL cholesterol to < 100 mg/dl, glucose control to achieve HgA1c < 7.0%, BP <140/90 mmHg, BP < 130/80 if diabetic or renal disease, and antiplatelet therapy with aspirin or clopidogrel. Given the high prevalence of coronary artery disease (CAD) in patients with CLI, evaluate for evidence of CAD. Manage patients with clinical evidence of heart dis-ease — as manifested by angina, congestive heart failure or symptomatic arrhythmias — according to current guidelines.9
Primary treatment A year later
Primaryamputation
25%
Medicaltreatment only
25%
ContinuingCLI20%
Dead25%
CLIresolved
25%
Alive with amputation
30%
Revascularization50%
Figure 3. Fate of patients with below-knee amputation. Adapted from Norgren L, Hiatt WR, Dormandy JA, et al. Inter-society consensus for the management of peripheral arterial disease (TASC II). Eur J Vasc Endovasc Surg. 2007;33 Suppl 1:S1–75.
Figure 2. Fate of patients presenting with CLI. Adapted from Norgren L, Hiatt WR, Dormandy JA, et al. Inter-society consensus for the management of peripheral arterial disease (TASC II). Eur J Vasc Endovasc Surg. 2007;33 Suppl 1:S1–75.
Early After 2 years
1o healing60%
Above-kneeamputation
15%
2o healing15%
Perioperativedeath10%
Full mobility40%
Above-knee
amputation
15%
Contralateralamputation
15%
Dead30%
Cannot be reprinted without
permission of HMP Communications
10 Preventing Critical Limb Ischemia Supplement to Podiatry Today® and Vascular Disease Management®
Routine coronary revascularization in preparation for vascular surgery or endovascular intervention isn’t recommended, ex-cept for individuals found to be at very high risk.10
Revascularization StrategiesMulti-level disease is common in CLI. As such, general prin-
ciples subscribe to first correcting inflow, and then outflow with the goal of establishing in-line flow to the foot. More recent guidelines call for providing direct flow to the ischemic angiosome, the composite anatomic vascular territories of skin and underlying muscles, tendons, nerves and bones, based on segmental or distributing arteries.11 Successful wound healing, whether accomplished by open bypass or endovascular thera-py, is accomplished in 91% and 87% of patients, respectively, if the proper angiosome is revascularized.12,13
The risk of the intervention and expected degree and dura-bility of improvement determine the revascularization method. CLI patients are often elderly with multiple comorbidities, and the goal is not primary patency of the intervention, but limb salvage. Endovascular techniques are therefore preferred for most patients. Surgery is reserved for patients with failed endo-vascular procedures, long occlusive disease or recurrent resteno-sis, who are healthy enough to undergo open repair or bypass. Primary amputation may be appropriate in cases of unrecon-structable arterial disease, persistent infection, sepsis or in the presence of paresis with an uncorrectable flexion contracture.
Specific endovascular techniques and devices are beyond the scope of this paper. Generally, aortoiliac inflow disease is treated with stenting because stents are more durable over balloon angioplasty/percutaneous transluminal angioplasty (PTA). Common femoral and ostial profunda femoris lesions are best treated with local endarterectomy and patch angio-plasty in patients who are good surgical candidates.
Infrainguinal lesions may require plaque-debulking tech-nologies. For heavily calcified lesions, orbital atherectomy and rotational atherectomy may be used alone or with PTA and stenting. A plaque-excision atherectomy device may be used to remove obstructive atheroma, particularly in arterial seg-ments where stents are to be avoided, such as the common femoral, profunda femoris, behind-the-knee popliteal and tibial vessels. Laser atherectomy may be used to photoablate plaque and is preferred for treating in-stent restenosis.
Infrainguinal vessels are often occluded in patients with CLI. The development of dedicated chronic total occlusion (CTO) devices has significantly increased the success rates of CTO traversal, up to 90%, in our practice. They include controlled-microdissection, ultrasound-energy-emitting and spiral-wedge-turning devices. When these devices result in subintimal passage, specialty-needle lumen-re-entry devices allow wire access to the reconstituted true lumen.
PTA is reserved for short, focal lesions due to vessel recoil, a high risk of restenosis and the risk of arterial dissections in long, calcified lesions. Self-expanding nitinol stents provide intravascular scaffolding and seal dissections after PTA, and have proven to provide good short- and mid-term patency in lesions up to 10 cm long. Covered stents efficaciously seal perforations and treat longer segment lesions. This nitinol stent is covered with a PTFE and has heparin covalently bonded to the endoluminal surface.
Anatomic factors that limit patency include severity of dis-ease in the run-off vessels, length of the stenosis/occlusion, small vessel diameters and number of lesions treated. Adverse clinical variables include DM, renal failure and ischemia se-verity. All patients undergoing endovascular treatment require anti-platelet therapy with aspirin; clopidogrel is additionally used in patients undergoing stent implantation.
CLI confirmed
Candidate for revascularization
Imaging (Duplex, angiography, MRA,CTA)
Revascularizationas appropriate
Not a candidate forrevascularization
Stable pain and lesionNot-tolerable pain, spreading infection
Medical treatment(non-operative) Amputation
Figure 4. Adapted from Norgren L, Hiatt WR, Dormandy JA, et al. Inter-society consensus for the management of peripheral arterial disease (TASC II). Eur J Vasc Endovasc Surg. 2007;33 Suppl 1:S1–75.
Cannot be reprinted without
permission of HMP Communications

Supplement to Podiatry Today® and Vascular Disease Management® Preventing Critical Limb Ischemia 11
Post-Revascularization ManagementAfter revascularization, the interventionalist must commu-
nicate with his/her podiatric colleague to review the angio-graphic findings and revascularization procedures. The new medical regimen is reviewed, and the timing of any additional procedures is discussed. Coordination of wound care and ad-junctive therapies — such as hyperbaric oxygen treatment, systemic antibiotics and possible need for amputation — are discussed and agreed upon.
The podiatrist again assumes the primary role in success-ful limb salvage. Pre- and post-revascularization, the podiatrist treats the ulcer patient with offloading, achieved by several methods, including shoe modifications, orthotics and casting techniques. Although discussing each ulcer product in depth is beyond the scope of this article, the principles of wound care should be faithfully followed. Chief among them is removing infected/necrotic tissue from the ulcer, treating infection, and maintaining a moist environment to promote ulcer healing.
The interventionalist must routinely follow the CLI pa-tient with ABI and duplex ultrasound surveillance to assess the patency of the endovascular or surgical bypass site. Return of claudication or rest pain, drop in ABI or elevated Doppler velocities at the treated segment likely represents restenosis, mandating prompt angiography and repeat revascularization to avoid vessel re-occlusion.
The podiatrist can frequently recognize impending treat-ment site failure by noting slowed wound healing, worsen-ing pulse exam, elevation pallor and dependent rubor, ulcer growth, or new areas of ischemia on the toes and foot. In such a case, the interventionalist should be contacted to assess vessel patency.
Both the podiatrist and interventionalist should use every office visit to reinforce risk factor reduction strategies, medica-tion compliance, and engage patients in playing active roles in their care. By partnering, the interventionalist and podiatrist can save both limbs and lives.
Partnering for Interdisciplinary CareWhen the podiatrist recognizes and diagnoses CLI and
PAD, and there’s a lesion such as a wound on one or both feet, the podiatrist should properly treat and debride the wound, then refer the patient to the vascular specialist for examination and treatment of the PAD. Similarly, the vas-cular interventionalist should refer the patient back to the podiatric physician for continued treatment of the lower-extremity wound. This is the ideal path for overcoming the patient’s disease state.
To that end, it’s critical that the podiatric physician who has diagnosed CLI and PAD maintain a working relationship with the vascular interventionalist. This relationship should be based on competency, knowledge, trust and friendship. Face-to-face contact between the podiatrist and interventionalist is the easiest and best way to start a working relationship.
In our experience, podiatric and vascular interventionalist practices complement one another. They not only can refer patients back and forth, but prevent lower-extremity ampu-tations in many diabetic and non-diabetic patients.
In the large urban area where we practice, it’s very easy to find this type of approach to CLI. It might not be that way in smaller communities. Either the podiatrist or interventional-ist must take the initiative to start such a relationship. Don’t hesitate to pick up the phone to discuss referring patients to one another. This team approach is critical to preventing lower-extremity amputations, and patients’ lives may depend on it. n
References1. Allie DE, Hebert CJ, Lirtzman MD, et al. Critical limb ischemia: a global
epidemic. A critical analysis of current treatment unmasks the clinical
and economic costs of CLI. EuroIntervention. 2005;1:75–84.
2. Dormandy J, Verstraete M, Andreani D, et al. Second European consen-
sus document on chronic critical leg ischemia. Circulation. 1991;84(Suppl
4):1–26.
3. DeBakey ME, Crawford ES, Garrett E, et al. Occlusive disease of
the lower extremities in patients 16 to 37 years of age. Ann Surg.
1964;159:873–890.
4. International Working Group on the Diabetic Foot, available at www.
iwgdf.org
5. Norgren L, Hiatt WR, Dormandy JA, et al. Inter-Society Consensus
for the Management of Peripheral Arterial Disease (TASC II). Eur J Vasc
Endovasc Surg. 2007;33 Suppl 1:S1–75.
6. Rose G, McCartney P, Reid DD. Self-administration of a question-
naire on chest pain and intermittent claudication. Br J Prev Soc Med.
1977;31(1):42–48.
7. Leng G, Fowkes F. The Edinburgh claudication questionnaire: an im-
proved version of the WHO/Rose questionnaire for use in epidemio-
logical surveys. J Clin Epidemiol. 1992;45(10):1101–1109.
8. Resnick HE, Lindsay RS, McDermott MM, et al. Relationship of high and
low ankle brachial index to all-cause and cardiovascular disease mortality:
the Strong Heart Study. Circulation. 2004;109(6):733–739.
9. Eagle KA, Berger PB, Calkins H, et al. ACC/AHA guideline update
for perioperative cardiovascular evaluation for non-cardiac surgery-
executive summary: a report of the American College of Cardiology/
American Heart Association Task Force on Practice Guidelines. J Am
Coll Cardiol. 2002;39(3):542–553.
10. McFalls EO, Ward HB, Moritz TE, et al. Coronary artery revas-
cularization before elective major vascular surgery. N Engl J Med.
2004;351(27):2795–2804.
11. Taylor GI, Palmer JH. The vascular territories (angiosomes) of the
body: experimental study and clinical applications. Br J Plast Surg.
1987;40(2):113–141.
12. Neville RF, Attinger CE, Bulan EJ, et al. Revascularization of a specific
angiosome for limb salvage: does the target artery matter? Annals of
Vasc Surg. 2009;(3):367–373.
13. Iida O, Nanto S, Uematsu M, et al. Importance of the angiosome con-
cept for endovascular therapy in patients with critical limb ischemia.
Catheter Cardiovasc Interv. 2010;75(6):830–836.
Cannot be reprinted without
permission of HMP Communications

12 Preventing Critical Limb Ischemia Supplement to Podiatry Today® and Vascular Disease Management®
Amputation is no longer an acceptable first option for patients with critical limb ischemia (CLI). This is primarily because rapidly evolving technol-ogy, including less-invasive endovascular and hy-
brid (combined surgical and endovascular) procedures, and clinical follow-up with podiatry and wound care specialists are more likely to lead to amputation prevention. Due to post-amputation consequences, immediate revascularization should be the first step in treating patients with CLI to pre-vent the comorbidity associated with limb loss.
Unfortunately, this primary goal is achieved in only a mi-nority of patients. In a recent series, only 40% of patients with CLI received prompt revascularization.1 This low rate is explained partly by late referrals and the fact there’s no agreed upon definition of a non-salvageable limb.
With currently available, swift vascular therapeutic options, the issue remains how to identify and refer CLI patients early to ensure the complete benefit of early revascularization in conjunction with podiatric, wound care and diabetic special-ists. The answer lies in a multidisciplinary team approach, which we believe has been shown to lower amputation rates.
Evolution of Centralized CareThe term “wound care center” was not part of the special-
ty’s vocabulary as recently as approximately 20 years ago. The
concept of a central location where individuals with chronic or non-healing wounds could receive intensive care and ad-vanced treatment has gone from a novel medical concept to a well-established service and has become a common term in the process. By taking the team approach found in other areas of medicine (stroke teams, burn teams) and applying it to wound care, we have not only improved outcomes for many suffering patients, but raised the bar by creating a de-mand for greater research, clinical practice, standardization and improved outcomes.
The team approach to wound care has been validated through retrospective analyses and the number of positively affected lives. Evidence has shown that a team approach to managing diabetes is an effective way to avoid or postpone the onset of serious complications.2 The Nashville, TN, Department of Veterans Affairs Medical Center used the Preservation Amputation Care and Treatment program and demonstrated a 40% decrease in the number of lower-ex-tremity amputations over the past 5 years. The program has decreased the costs of pharmaceuticals by 48%, lab studies by 32% and inpatient bed days by 44%.3 Concomitant to the team approach, lower-extremity preservation and the use of limb salvage, limb preservation and amputation prevention has increased.
The acute risk of mortality and morbidity facing patients with CLI necessitates critical urgency for limb preservation, particularly given the aging population and the number of pa-tients with diabetes increasing at an alarming rate, both in the United States and worldwide. The financial impact and the in-herent issues associated with lower-extremity amputation com-pound the importance of lower-extremity preservation.
Patients suffering from non-healing, lower-extremity wounds and CLI often have multiple comorbidities requir-ing multiple specialties. Patients with CLI are among the most complicated to treat and, as a result, a specialized team is best suited for managing limb-threatening complications.
Better understanding of the need for limb preservation and development of breakthrough technologies have given rise to a concept similar to that of wound care centers — increasingly referred to as limb-salvage, limb-preservation or amputation-prevention centers. This model inherently in-corporates the need for a team approach. Not that the team members need work under the same roof. Rather, the con-cept should be community-centered — whether hospital-
Amputation Prevention: A Multidisciplinary ApproachJ. A. Mustapha, MD, FACC, FSCAI; Desmond Bell, DPM, CWS; Yazan Khatib, MD, FACC, FSCAI, FSVMB, FABVM; Fadi Saab, MD; Carmen M. Heaney, BSN, RN, CCRC, CIP
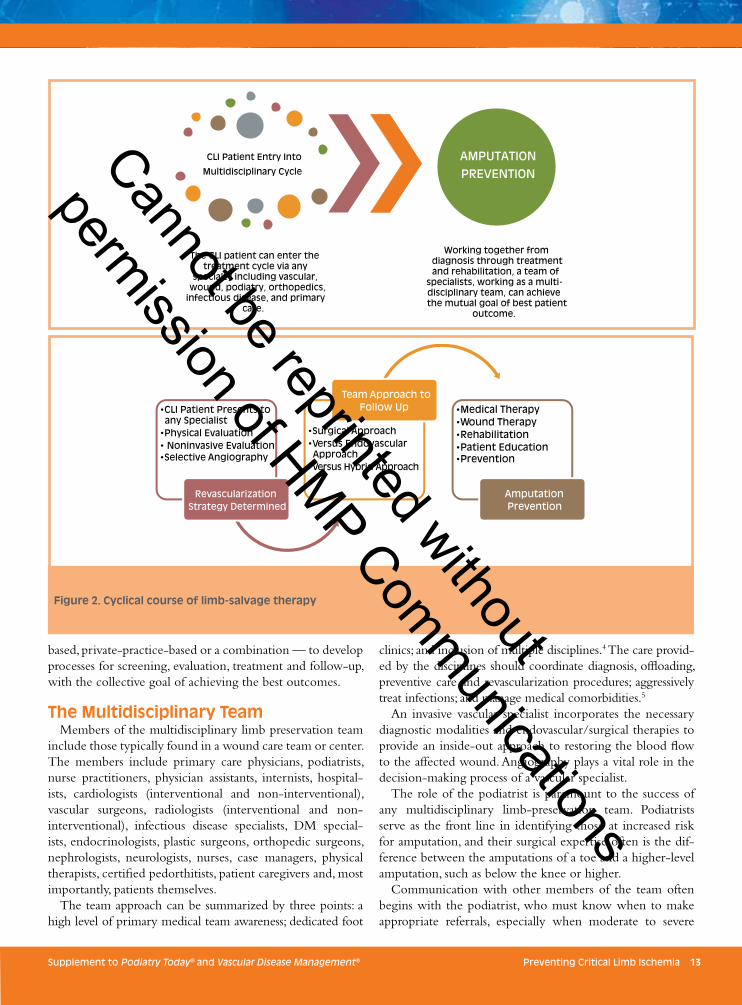
Figure 1. In a multidisciplinary therapeutic treatment flow, the cycle of therapy does not always start in the office of the same specialist.
Patients enter
the cycle
Non-invasive andphysical testing
Evaluated byhealth care
provider
Initiate revascularization
plan
Initiate pharmacological treatment plan
Cannot be reprinted without
permission of HMP Communications
Supplement to Podiatry Today® and Vascular Disease Management® Preventing Critical Limb Ischemia 13
based, private-practice-based or a combination — to develop processes for screening, evaluation, treatment and follow-up, with the collective goal of achieving the best outcomes.
The Multidisciplinary TeamMembers of the multidisciplinary limb preservation team
include those typically found in a wound care team or center. The members include primary care physicians, podiatrists, nurse practitioners, physician assistants, internists, hospital-ists, cardiologists (interventional and non-interventional), vascular surgeons, radiologists (interventional and non-interventional), infectious disease specialists, DM special-ists, endocrinologists, plastic surgeons, orthopedic surgeons, nephrologists, neurologists, nurses, case managers, physical therapists, certified pedorthitists, patient caregivers and, most importantly, patients themselves.
The team approach can be summarized by three points: a high level of primary medical team awareness; dedicated foot
clinics; and inclusion of multiple disciplines.4 The care provid-ed by the disciplines should coordinate diagnosis, offloading, preventive care and revascularization procedures; aggressively treat infections; and manage medical comorbidities.5
An invasive vascular specialist incorporates the necessary diagnostic modalities and endovascular/surgical therapies to provide an inside-out approach to restoring the blood flow to the affected wound. Angiography plays a vital role in the decision-making process of a vascular specialist.
The role of the podiatrist is paramount to the success of any multidisciplinary limb-preservation team. Podiatrists serve as the front line in identifying those at increased risk for amputation, and their surgical expertise often is the dif-ference between the amputations of a toe and a higher-level amputation, such as below the knee or higher.
Communication with other members of the team often begins with the podiatrist, who must know when to make appropriate referrals, especially when moderate to severe
CLI Patient Entry Into
Multidisciplinary Cycle
The CLI patient can enter the treatment cycle via any
specialty including vascular, wound, podiatry, orthopedics,
infectious disease, and primary care.
AMPUTATION PREVENTION
Working together from diagnosis through treatment and rehabilitation, a team of
specialists, working as a multi-disciplinary team, can achieve the mutual goal of best patient
outcome.
Figure 2. Cyclical course of limb-salvage therapy
•CLI Patient Presents to any Specialist •Physical Evaluation • Noninvasive Evaluation •Selective Angiography
Revascularization Strategy Determined
•Surgical Approach •Versus Endovascular Approach •Versus Hybrid Approach
Team Approach to Follow Up •Medical Therapy
•Wound Therapy •Rehabilitation •Patient Education •Prevention
Amputation Prevention
Cannot be reprinted without
permission of HMP Communications
14 Preventing Critical Limb Ischemia Supplement to Podiatry Today® and Vascular Disease Management®
peripheral arterial disease (PAD) is suspected or observed. Developing a working relationship with a vascular interven-
tionalist (cardiologist, vascular surgeon or radiologist) should be mutually beneficial and ultimately benefit patients at high risk for amputation.
In a multidisciplinary therapeutic treatment flow, the cycle of therapy does not always start in the office of the same spe-cialist (Figure 1). A patient with CLI may enter the multidis-ciplinary cycle via a podiatry office, primary care practitio-ner, wound clinic or vascular specialist. Whatever the point of entry into the cycle (Figure 2), the patient should receive the appropriate care each specialist can offer.
Approach to Patient EvaluationThe success of a patient’s experience (including evaluation,
therapy and recovery) who presents with critical limb isch-emia requires a collaborative approach to all aspects of care using the following criteria.
Thorough Physical ExamThe physical examination can significantly increase the
diagnostic accuracy in patients evaluated for suspected PAD. A systematic approach using palpation, auscultation and in-spection is quite effective. Blood pressure should be mea-sured in both arms. The examiner should palpate the femoral, popliteal, dorsalis pedis and posterior tibial pulses, and note the amplitude and symmetry in each territory. Carefully in-spect the extremities and note the color (e.g., cyanosis, pal-lor), temperature, distribution of hair growth, and presence of trophic skin or muscle changes.
PAD and CLI remain clinical diagnoses that should be classified for severity according to either the Rutherford or Fontaine classification. Multiple modalities can aid CLI diagnosis, particularly when examining peripheral pulses at baseline. A provider who is unable to palpate pulses should document the pulse by an arterial doppler (triphasic, bipha-sic, monophasic). An ankle-brachial index (ABI) is an ad-equate starting point to assess the significance of the disease. An ABI test can be easily performed and interpreted by the performing discipline. A transcutaneous partial pressure of oxygen (TcPO
2) is another measurement that can be used in
a podiatry or wound clinic setting. A TcPO2 less than 30–50
mmHg is consistent with CLI and poor healing. Currently available technology lets skin-perfusion pressure be done within 4 minutes and doesn’t require the recalibration need-ed with older-generation TcPO
2 machinery. Skin-perfusion
pressure should be routinely measured in all patients with Rutherford grades IV–VI.
Computerized Tomography and Magnetic Resonance Angiographies Computerized tomography angiography (CTA) and mag-
netic resonance angiography (MRA) are two noninvasive modalities that can, despite their limitations, better define the vascular anatomy of patients with CLI.
Multiple studies have demonstrated that CTA of the ex-
0
50
100
150
200
250
Based on ICD-9 codes for Ischemia 440.20 and Ischemia Gangrene 440.24
2004 2005 2006 2007 2008Projection
ULCER
GANGRENE
87
36
123
22
28
50
73
65
26
91
19
17
36
55
43
29
72
20
18
38
34
126
43
169
28
19
47
122
172
32
204
20
24
44
160
TOTAL CLI-
AKA
BKA
TOTAL AMP
TOTAL SALVAGE
ULCER
GANGRENE
TOTAL CLI-
AKA
BKA
TOTAL AMP
TOTAL SALVAGE
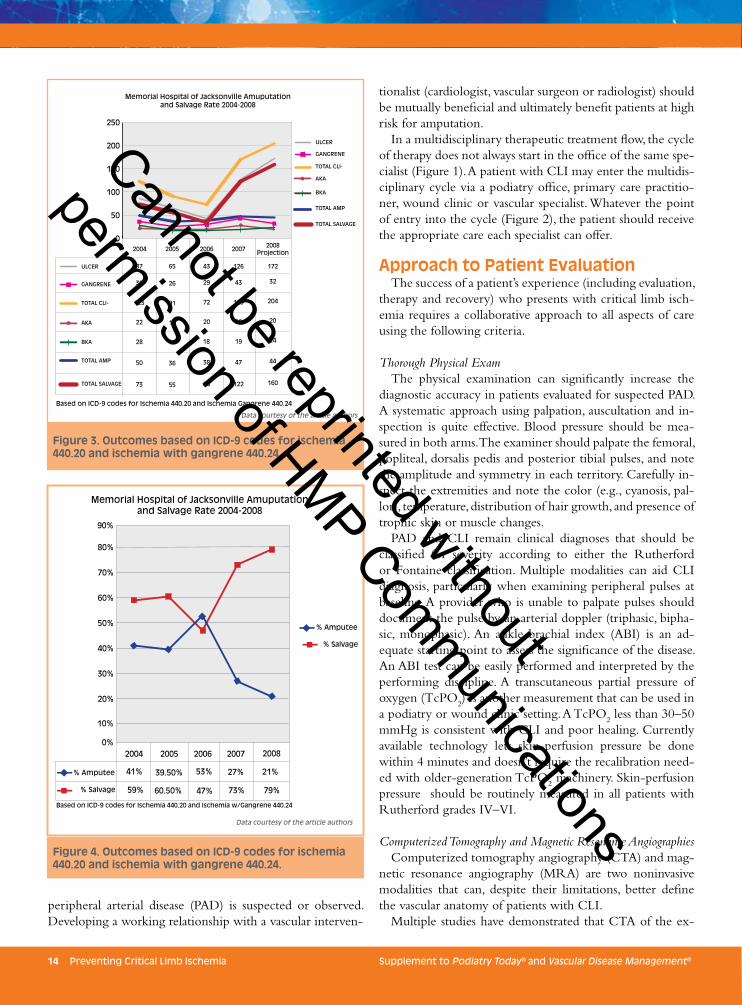
Memorial Hospital of Jacksonville Amuputationand Salvage Rate 2004-2008
20%
30%
40%
50%
60%
70%
80%
90%
10%
0%2004 2005
Based on ICD-9 codes for Ischemia 440.20 and Ischemia w/Gangrene 440.24
2006 2007 2008
41% 39.50% 53% 27% 21%
79%73%47%60.50%59%
% Amputee
% Salvage
% Amputee
% Salvage
Figure 4. Outcomes based on ICD-9 codes for ischemia 440.20 and ischemia with gangrene 440.24.
Figure 3. Outcomes based on ICD-9 codes for ischemia 440.20 and ischemia with gangrene 440.24.
Data courtesy of the article authors
Data courtesy of the article authors
Cannot be reprinted without
permission of HMP Communications

Supplement to Podiatry Today® and Vascular Disease Management® Preventing Critical Limb Ischemia 15
tremities accurately detects arterial occlusions and stenosis > 50%.5 CTA usually requires an IV injection of 100–200 ml of iodinated contrast, and exposure to radiation. CTA is limited by poor visualization of vessels with heavy calcifica-tion, artifact from stented vessels, venous opacification, and decreased spatial resolution when compared to digital sub-traction angiography.
MRA with gadolinium contrast enhancement is very ef-fective for diagnosing the anatomic location and degree of stenosis in PAD. A recent meta-analysis demonstrated MRA’s superior accuracy compared to arterial duplex ultrasound in detecting arterial stenosis > 50%.6 Limitations of MRA in-clude mainly an overestimation of the degree of stenosis due to turbulence, artifact due to metal clips, and association of gadolinium toxicity in patients with renal insufficiency.
Arteriogram With Run-OffArteriogram (or CTA, MRA) with run-off to the digital
branches of the foot is done primarily to evaluate the aorto-iliac and superficial femoral arteries. Arteriogram has shown to less accurately visualize the tibial arteries and their col-laterals, especially, the communicating collaterals. The pedal vessels are also under-visualized in most cases. In the authors’ opinion, retrograde angiography using tibial access might highlight different vascular conduits.
Selective AngiographySelective angiography with and without vasodilators must
be performed. Amputation should never be recommended without having performed combined antegrade retrograde selective angiography.
Tibio-pedal Access and Angiography With and Without VasodilatorsThis is an absolute must in all CLI cases previously deemed
not salvageable. The data collected from retrograde access al-most always changes the therapy path from major amputa-tion to either minor or no amputation. Another important element is determining the true lesions and lesion lengths. It lets operators accurately visualize the length of the chronic total occlusion (CTO).
A single tibial access angiogram usually opacifies most of the tibial arteries and their branches. The antegrade flow is delayed to the tibio-pedal bed due to either high-grade ste-nosis or CTO. This causes low-pressure states in the tibio-pedal vessels distal to the lesion, which can cause vasospasm and a low-flow state, which causes it not to fill the entire length of its patent vessel. This appears to be a long CTO when the reality is a short CTO or subtotal occlusion.
Angiosome MappingCutaneous and arterial angiosome mapping is easy to per-
form. Cutaneous angiosome is straightforward and should be done on all patients with Rutherford V and VI ischemic tis-
sue. Antegrade angiosome arterial mapping defines whether blood perfusion is reaching the target tissue via direct or indirect arterial flow. In our experience, a long tibio-pedal CTO can easily be reduced to a short-segment CTO just by adding a retrograde angiogram via tibio-pedal access.
TreatmentInterdisciplinary discussions and referrals, advances in
pharmacological therapy and wound care treatment, and more successful foot surgery provide more options for treat-ing complex disease. Excellent femoral, tibial and hybrid en-dovascular procedures provided by multiple specialties have improved revascularization success in critically ischemic limbs that otherwise would have been unsalvageable a few years ago.
Outcomes/Follow-UpIt’s difficult to identify objective performance goals in pa-
tients with CLI. The Society of Vascular Surgery has pro-
Figure 5. An arteriogram is done primarily to evaluate the aortoiliac and superficial femoral arteries.
Imag
e c
ou
rte
sy o
f th
e a
rtic
le a
uth
ors
Cannot be reprinted without
permission of HMP Communications

16 Preventing Critical Limb Ischemia Supplement to Podiatry Today® and Vascular Disease Management®
posed the use of major adverse limb events (MALEs) as a primary end-point to determine such goals.7 MALEs include amputation or any major vascular intervention with 30 days. With the rapidly evolving techniques and the significant impact of revascularization on a patient’s life, clinical trials should focus on quality of life as a primary measure to evaluate outcomes.
Podiatrists and wound clinics should closely follow up with CLI patients who undergo complex revascularization. It’s important to document treatment response and the healing process, particularly in patients with non-healing foot ulcers. There are multiple questionnaires that can help with this. By the same token, deterioration or therapy fail-ure can be recognized by the patient’s wound care special-ist or podiatrist, and triage to appropriate therapy can be initiated. Reasonable follow-up modalities include post-procedure ABIs, screening arterial Doppler ultrasound and measuring tissue oxygenation.
Successes of the Team ApproachSystem changes have had a major impact on management
of the diabetic foot during the past decades. Comprehen-sive multidisciplinary foot-care programs have been shown to increase quality of care and reduce amputation rates by 36% to 86%.8
Take, for example, the work of the Save a Leg, Save a Life Foundation. The foundation — originally a local, informal, lunch-and-learn/journal club — was later incorporated as a non-profit. Its primary purpose is to increase education among healthcare providers, specifically in wound care and PAD. Through a series of local meetings, initially focusing on home health nurses, the message quickly spread to other providers who were similarly interested in these topics. In approximately 1 year, the group grew from 15 members to more than 100.
The regular gatherings began to form relationships within the community. In turn, these relationships positively affect-
Figure 6. Selective angiography with and without vasodilators must be performed.
Figure 7. A single tibial access angiogram usually opacifies most of the tibial arteries and their branches.
Imag
e c
ou
rte
sy o
f th
e a
rtic
le a
uth
ors
Imag
e c
ou
rte
sy o
f th
e a
rtic
le a
uth
ors
Cannot be reprinted without
permission of HMP Communications
Supplement to Podiatry Today® and Vascular Disease Management® Preventing Critical Limb Ischemia 17
ed quality of care. The desire to quantify this impact was the impetus for gathering data regarding lower-extremity am-putation rates for the period from 2 years before and 2 years after the organization’s founding.
Data were obtained from the Agency of Health Care Ad-ministration, the Duval County Department of Health (Jack-sonville, FL) and local hospitals, and amputation rates for the 4-year period were analyzed (Figure 3). The most striking data revealed some unanticipated and significant findings, centering on Memorial Hospital of Jacksonville. Among our conclusions were that the multidisciplinary approach, expe-dited by regular educational meetings, helped develop rela-tionships — and the teams within a community had lowered amputation rates and increased limb-salvage rates (Figure 4).
In Singapore, the LEAP (lower extremity amputation prevention) group showed its multidisciplinary approach to amputation prevention resulted in a lower amputation rate (29% versus 76 %, P = 0.00001), lower related death rate (1% versus 19 %, P = 0.00001) and fewer in-hospital days per patient (17.8 days versus 23.16 days, P = 0.048) as compared to the standard clinical practice group.9
The LEAP strategy also generated significant cost sav-ings per patient during admission when compared with the pre-LEAP approach. The LEAP strategy dominated standard practice in the management of patients with DM and CLI. In essence, the implementation of this multidisciplinary ap-proach significantly improved patient outcomes and reduced hospital stays.9
ConclusionApproximately 30,000 to 40,000 Americans undergo am-
putation annually. In 2008, an estimated 1.6 million Ameri-cans were living with an amputation, and it is estimated that by 2050, 3.6 million will be living with an amputation.10 With the advancements described herein, does it make sense to perform major amputations (above- or below-knee) with-out fully evaluating other options? We emphatically say “No.”
In addition, we’re facing a major ethical dilemma. Many limb-salvage specialists are successfully revascularizing pa-tients who have been told they had no options. Unfortu-nately, many of these patients had received gloomy recom-mendations without the benefit of an adequate evaluation (selective angiography, etc.). Today, no patient should under-go amputation without a full amputation-prevention assess-ment followed by attempted revascularization using the ap-propriate surgical, endovascular or hybrid approach. In short, amputation should be the treatment of last resort, used only when all other options have been exhausted, and should be described as treatment failure.11 n
References1. O’Hare AM, Bertenthal D, Sidawy AN, et al. Renal in-
sufficiency and use of revascularization among a national cohort of men with advanced lower extremity peripheral arterial disease. Clin J Am Soc Nephrol. 2006;1(2):297–304.
2. Agency for Healthcare Research and Quality. Improving care for diabetes patients through intensive therapy and a team approach. Research in Action. 2001:2:1–12. Available from 2http://www.ahrq.gov/research/diabria/diabetes.htm
3. Hinkes M. Diabetes: taking steps to prevent amputa-tion. Lower Extremity Review. August 2009. Available from www.lowerextremityreview.com/article/diabetes-taking-steps-to-prevent-amputation
4. Bass A. [Prevention is the name of the game]. Harefuah. 2010;149(12):782–3, 811. Hebrew.
5. Ofer A, Nitecki SS, Linn S, et al. Multidetector CT an-giography of peripheral vascular disease: a prospective comparison with intraarterial digital subtraction angiog-raphy. Am J Roentgenol. 2003;180(3):719–724.
6. Visser K, Hunink MG. Peripheral arterial disease: gadolinium-enhanced MR angiography versus col-or-guided duplex US — a meta-analysis. Radiology. 2000;216(1):67–77.
7. Conte MS. Technical factors in lower-extremity vein by-pass surgery: how can we improve outcomes? Semin Vasc Surg. 2009;22(4):227–233.
8. Sanders LJ, Robbins JM, Edmonds ME. History of the team approach to amputation prevention: pioneers and milestones. J Am Podiatr Med Assoc. 2010;100(5):317–334.
9. Tan ML, Feng J, Gordois A, Wong ES. Lower extremity amputation prevention in Singapore: Economic analysis of results. Singapore Med J. 2011;52(9):662–668
10. Ziegler-Graham K, MacKenzie EJ, Ephraim PL, et al. Es-timating the prevalence of limb loss in the United States: 2005 to 2050. Arch Phys Med Rehabil. 2008;89(3):422–429.
11. Gardner BA, Chenchen H, Sing H, Adams G. Amputation as a last resort. A look at critical limb ischemia and the treatment options available before amputation is the only remaining option. Endovasc Today. 2011;10(8):38–44.
Cannot be reprinted without
permission of HMP Communications

18 Preventing Critical Limb Ischemia Supplement to Podiatry Today® and Vascular Disease Management®
Diagnosing a patient with critical limb ischemia (CLI) requires the podiatrist to perform a detailed history along with physical, vascular laboratory and possible referral angiographic examinations.
Although the evaluation is not as urgent with CLI as it is in acute limb ischemia, thoroughly evaluating each of these areas in a semi-urgent manner can prevent tissue loss and a more distal amputation (should it come to that).
History and Initial Physical EvaluationThe patient’s presentation history plays an important role in
the evaluation of CLI. The onset of the disease process needs to be known to help differentiate CLI from acute limb isch-emia. This distinction is quite important, because the progno-sis, evaluation and treatment differ between the two scenarios. An abrupt change in foot color — bluish discoloration, with an acute onset of foot pain — could very well point to an acute ischemic event of that lower limb. These events, com-pared to the more chronic in nature CLI changes, must be treated as an acute emergency to avoid limb loss.
The vascular history should include evaluation for arterial disease in other sites (e.g., carotid, coronary), global risk factors for atherosclerosis, and history of trauma or other incident that may have caused skin breakdown. Shoe wear can be the incit-ing element and should be evaluated both in the history and
the exam. Patients who have exhibited CLI symptoms previ-ously remain at risk for recurrent symptoms or signs of CLI. Prior bouts of CLI, along with their treatments and outcomes, can assist the clinician with the current episode.1
The physical examination of the lower extremity with sus-pected CLI begins with an overall perusal of the bilateral lower extremities. Signs of chronic ischemia include depen-dent rubor, lack of hair growth, pallor on elevation, atrophic shiny skin, nail dystrophy and delayed capillary refill time.1 In our experience, an ominous sign of peripheral aterial disease (PAD)/CLI is when subcutaneous tissue atrophy can be seen at the ends of the toes (Figure 1). The atrophy and the loss of elasticity of the subcutaneous tissues prevent rebounding of the subcutaneous tissues when pressure is applied to the end of the toe. We liken this sign to a baked potato that has been over-baked and lost its shape (Figure 2).
Palpation of PulsesPalpation of the lower-extremity pulses is another aspect
of the physical exam necessary for diagnosing CLI. Although there are several grading systems for lower-extremity pulses — such as the four-level grading system — a simple “pal-pable” or “not palpable” will suffice. The literature has re-ported variance between clinicians when palpitating pulses.2 There may be times when one clinician believes a pedal
Diagnosing CLI: The Role of the PodiatristJoseph Caporusso, DPM
Figure 1. An ominous sign of peripheral aterial disease/critical limb ischemia is when subcutaneous tissue atrophy can be seen at the ends of the toes.
Figure 2. Atrophy and loss of subcutaneous-tissue elas-ticity prevent rebounding of the subcutaneous tissues when pressure is applied to end of the toe — much like an over-baked potato that has lost its shape.
Imag
e c
ou
rte
sy o
f Jo
sep
h C
apo
russ
o, D
PM
Imag
e c
ou
rte
sy o
f Jo
sep
h C
apo
russ
o, D
PM
Cannot be reprinted without
permission of HMP Communications
Supplement to Podiatry Today® and Vascular Disease Management® Preventing Critical Limb Ischemia 19
pulse can be felt, while another clinician doesn’t. This sub-jectivity is to be considered when palpating pedal pulses. Note that both the posterior tibial and the dorsalis pedis arteries have accepted rates of anatomical absences.2
Capillary refill time is another indication of PAD/CLI. The longer it takes the capillaries to refill after the application of pressure indicates the presence of vascular disease. Less than three seconds indicates a normal capilliary refill time.3
Ulceration ClassificationAny ulceration that’s present should be classified as to
its etiology. Distinction should be made between ischemic (arterial), neuropathic, mixed and venous ulcerations. De-termining classification is extremely important to ensure appropriate treatment of the ulceration. Each type of ulcer-ation has a unique presentation, letting the clinician differ-entiate one from another.
Ischemic (arterial) ulcerations occur at the ends of the digits and in the heel area. They’re usually extremely painful, although some patients who have diabetes and peripheral neuropathy may not experience the pain associated with these ulcerations. The ulcer base demonstrates an unhealthy appearance with necrosis present. A hyperkertotic rim isn’t usually associated with an arterial ulcer. Rather, the neuro-pathic ulceration presents with a base that is granular and healthy in appearance, usually with a hyperkeratotic rim or covering that rules out a purely ischemic ulcer.
Calculating the Ankle Brachial IndexThe calculation of an ankle brachial index (ABI) is the
next step in evaluating the patient with CLI. The ABI has been reported to be 95% sensitive to and 99% specific for PAD.4 Performing the ABI helps define the at-risk popula-tion clinically and epidemiologically. An ABI index of less than or equal to 0.40 is consistent with CLI.1,4
Although a very useful test, the ABI does have limitations. First, when there are incompressible arteries, the ABI can be falsely elevated. In such cases, use the toe brachial index to provide more information regarding the PAD/CLI spec-trum. The ABI also isn’t designed to define the degree of functional limitation. Segmental pressures and pulse-volume recordings in conjunction with the ABI can provide the cli-nician with further information.
Vascular Laboratory and ImagingThe vascular laboratory can further help the clinician
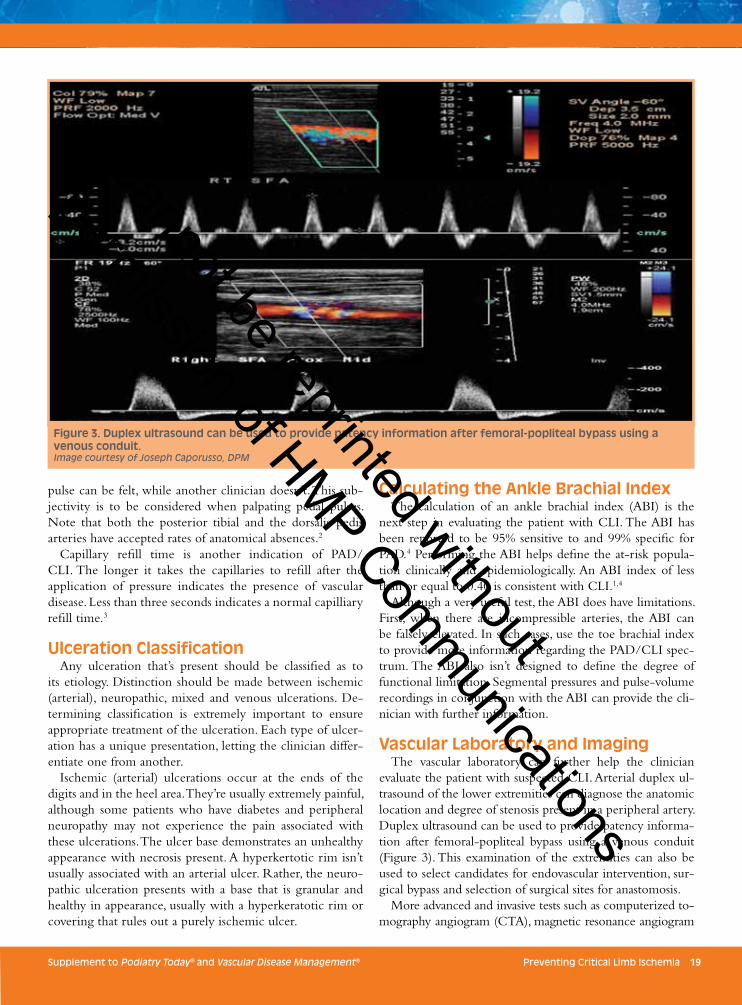
evaluate the patient with suspected CLI. Arterial duplex ul-trasound of the lower extremities can diagnose the anatomic location and degree of stenosis present in a peripheral artery. Duplex ultrasound can be used to provide patency informa-tion after femoral-popliteal bypass using a venous conduit (Figure 3). This examination of the extremities can also be used to select candidates for endovascular intervention, sur-gical bypass and selection of surgical sites for anastomosis.
More advanced and invasive tests such as computerized to-mography angiogram (CTA), magnetic resonance angiogram
Figure 3. Duplex ultrasound can be used to provide patency information after femoral-popliteal bypass using a venous conduit. Image courtesy of Joseph Caporusso, DPM
Cannot be reprinted without
permission of HMP Communications

20 Preventing Critical Limb Ischemia Supplement to Podiatry Today® and Vascular Disease Management®
(MRA) and traditional contrast angiography can be used to further detail the extent of the PAD. Each exam has its pros and cons. A complete description is beyond the scope of this work, but a cursory view will be given of each.
The angiographic image produced by CTA is constructed by multiple cross-sectional images, and then presented in a projection similar to that of a standard arteriogram. This projection can be rotated three dimensionally to view any oblique projection, a potential diagnostic advantage when compared to catheter angiography. A possible disadvantage of CTA versus catheter angiography is the lower spatial reso-lution. CTA does offer patients with pacemakers, defibrilla-tors, metal clips stands and prostheses an alternative to MRA. CTA also has a higher resolution than MRA, which can pro-vide images of calcification within the vessel wall. CTA scan times are significantly faster than those of MRA.
MRA is based on imaging the arteries similar to stan-dard arteriography, and has evolved and improved over the years. MRA accuracy depends on the technique used and the standard against which it’s compared. The MRA literature provides somewhat mixed results compared to catheter angiography.4
Contrast angiography has been considered the gold standard for defining both normal and abnormal vascular anatomy. It’s widely available and the most used technique, partly because physicians can easily interpret the images. The addition of digital subtraction techniques enhances image quality to allow better detection of abnormalities. The technological advances in angiography instrumentation have further enhanced the patient safety profile of this technique, although potential complications remain. These include bleeding, infection, vessel disruption, contrast reaction and nephrotoxicity. Less common complications could include artheroembolization, dissection, and vessel wall disruption or perforation.4
The choice of an advanced or invasive arterial angiographic technique may depend on availability on instrumentation/devices, physician experience and regional practice preferences.
ConclusionWhen it comes to the treatment of foot ulceration and/or
gangrene caused by CLI, the podiatric physician plays the role of both diagnostician and interventionalist. Many times, the podiatric physician is the first to discover the effects of CLI on the feet and, in doing so, sets the necessary mechanisms in motion to help the patient. Coordination of care with the vas-
cular specialist is paramount to successful outcomes. The treat-ment of CLI and its pedal complications is yet another ex-ample of how the multidisciplinary team approach yields the best results. The podiatrist, working in conjunction with the vascular team, affords the patient the necessary holistic care. n
References1. Norgren L, Hiatt WR, Dormandy JA, Nehler MR, Har-
ris KA, Fowkes FG, et al. Inter-society consensus for the management of peripheral arterial disease (TASC II). J Vasc Surg. 2007;45(Suppl S):S5–S67.
2. Kazmers A, Koski ME, Groehn H, et al. Assessment of noninvasive lower extremity arterial testing versus pulse exam. Am Surg. 1996;62(4):315–319.
3. Ikem R, Ikem I, Adebayo O, Soyoye D. An assessment of peripheral vascular disease in patients with diabetic foot ulcer. Foot (Edinb). 2010;20(4):114–117.
4. Hirsch AT, Haskal ZJ, Hertzer NR, et al; American Asso-ciation for Vascular Surgery; Society for Vascular Surgery; Society for Cardiovascular Angiography and Interven-tions; Society for Vascular Medicine and Biology; Society of Interventional Radiology; ACC/AHA Task Force on Practice Guidelines; American Association of Cardio-vascular and Pulmonary Rehabilitation; National Heart, Lung, and Blood Institute; Society for Vascular Nursing; TransAtlantic Inter-Society Consensus; Vascular Disease Foundation. ACC/AHA 2005 guidelines for the manage-ment of patients with peripheral arterial disease (lower extremity, renal, mesenteric, and abdominal aortic): execu-tive summary a collaborative report from the American Association for Vascular Surgery/Society for Vascular Sur-gery, Society for Cardiovascular Angiography and Inter-ventions, Society for Vascular Medicine and Biology, Soci-ety of Interventional Radiology, and the ACC/AHA Task Force on Practice Guidelines (Writing Committee to Develop Guidelines for the Management of Patients With Peripheral Arterial Disease) endorsed by the American Association of Cardiovascular and Pulmonary Rehabilita-tion; National Heart, Lung, and Blood Institute; Society for Vascular Nursing; TransAtlantic Inter-Society Consen-sus; and Vascular Disease Foundation. J Am Coll Cardiol. 2006;47(6):1239–1312.
Cannot be reprinted without
permission of HMP Communications

Supplement to Podiatry Today® and Vascular Disease Management® Preventing Critical Limb Ischemia 21
Peripheral arterial disease (PAD) affects nearly 9 mil-lion Americans and significantly increases the risk of heart attack, stroke, and death in that population. PAD can present as leg pain that’s often mistakenly
attributed to old age or arthritis. The most serious presenta-tion of PAD is critical limb ischemia (CLI), defined as isch-emic rest pain or tissue loss present for more than 2 weeks and arterial insufficiency corroborated by objective testing (see below). Approximately 300,000 patients a year present with this advanced degree of ischemia in the United States. Patients presenting with CLI face a prognosis worse than that of many cancers (Figure 1), yet CLI is often underdiagnosed and not aggressively treated.
Two demographic features suggest that the prevalence of CLI will increase over the next two decades. First, the number of persons 65 or older is expected to increase from 46 million to 80 million.1 Aging alone may account for a nearly 50% increase in the number of patients presenting with CLI.2 Sec-ond, as the incidence of diabetes mellitus continues to increase, so too will the number of patients with CLI. Optimum care of these patients needs to be multidisciplinary. These patients must have very aggressive treatment of all atherosclerotic risk factors, expeditious revascularization, and meticulous wound management to achieve the ultimate goal of limb salvage.
Restoration of InflowThe pathophysiology of CLI is quite simple. Tissue nutri-
tive demand is greater than the supply, with arterial lesions limiting perfusion of the affected area. This typically occurs in patients with multi-level occlusive disease that affects the aortoiliac, femoral-popliteal, and tibial segments. Microcir-culatory defects can also affect flow-regulatory and defense mechanisms. There’s often a combination of contributing factors, including endothelial dysfunction, altered hemorhe-ology and activation of white blood cell count with inflam-mation. CLI therapy’s goals are relieving ischemic rest pain, healing the wound, preventing limb loss, and improving pa-tient function/quality of life.
Adequate tissue perfusion is necessary for healing ischemic ulcerations. Restoration of inflow must take priority over at-tempted wound healing or tissue debridement unless there is concern for deep or ascending infection with systemic signs. Objective criteria for defining ischemia include ABI < 0.50, ankle systolic pressure < 50 mm Hg, toe systolic pressure < 30 mm Hg, and transcutaneous oxygen tension <30 mm Hg. The presence of even one of these factors in a patient with a non-healing, lower-extremity wound should dictate that revascularization be achieved to ensure healing.
The natural history of ischemic wounds has been studied
Comprehensive Wound Care ManagementRasesh M. Shah, MD, FACS, and John Steinberg, DPM, FACFAS
Within 3 months of presentation
Mortality
Amputation12%
Mortality9%
10 years70%
3 years31.6%2 years
21%
5 years50%
Presistent CLI18% Myocardial
infarction1%
Cerebral Vascular accident
1%
Figure 1. Prognosis for patients with critical limb ischemia. Adapted from Norgren L, Hiatt WR, Dormandy JA, Nehler MR, Harris KA, Fowkes FG, et al. Inter-society consensus for the management of peripheral arterial disease (TASC II). J Vasc Surg. 2007;45(Suppl S):S5–S67.
Cannot be reprinted without
permission of HMP Communications
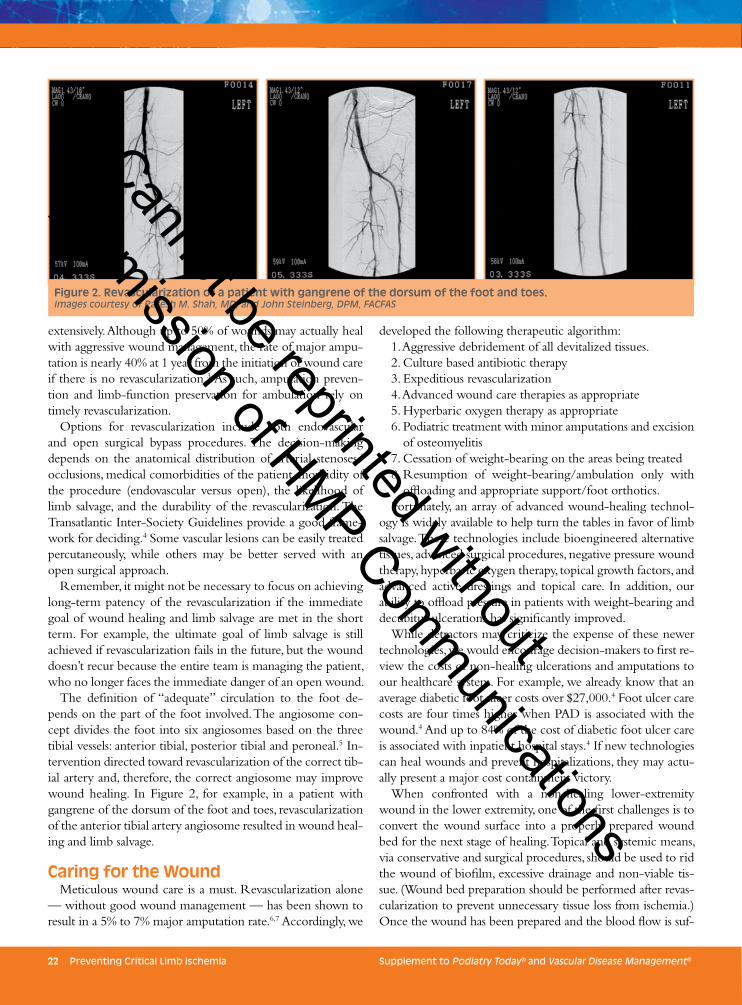
22 Preventing Critical Limb Ischemia Supplement to Podiatry Today® and Vascular Disease Management®
extensively. Although up to 50% of wounds may actually heal with aggressive wound management, the rate of major ampu-tation is nearly 40% at 1 year from the initiation of wound care if there is no revascularization.3 As such, amputation preven-tion and limb-function preservation for ambulation rely on timely revascularization.
Options for revascularization include both endovascular and open surgical bypass procedures. The decision-making depends on the anatomical distribution of arterial stenoses/occlusions, medical comorbidities of the patient, morbidity of the procedure (endovascular versus open), the likelihood of limb salvage, and the durability of the revascularization. The Transatlantic Inter-Society Guidelines provide a good frame-work for deciding.4 Some vascular lesions can be easily treated percutaneously, while others may be better served with an open surgical approach.
Remember, it might not be necessary to focus on achieving long-term patency of the revascularization if the immediate goal of wound healing and limb salvage are met in the short term. For example, the ultimate goal of limb salvage is still achieved if revascularization fails in the future, but the wound doesn’t recur because the entire team is managing the patient, who no longer faces the immediate danger of an open wound.
The definition of “adequate” circulation to the foot de-pends on the part of the foot involved. The angiosome con-cept divides the foot into six angiosomes based on the three tibial vessels: anterior tibial, posterior tibial and peroneal.5 In-tervention directed toward revascularization of the correct tib-ial artery and, therefore, the correct angiosome may improve wound healing. In Figure 2, for example, in a patient with gangrene of the dorsum of the foot and toes, revascularization of the anterior tibial artery angiosome resulted in wound heal-ing and limb salvage.
Caring for the WoundMeticulous wound care is a must. Revascularization alone
— without good wound management — has been shown to result in a 5% to 7% major amputation rate.6,7 Accordingly, we
developed the following therapeutic algorithm:1. Aggressive debridement of all devitalized tissues.2. Culture based antibiotic therapy3. Expeditious revascularization4. Advanced wound care therapies as appropriate5. Hyperbaric oxygen therapy as appropriate6. Podiatric treatment with minor amputations and excision
of osteomyelitis7. Cessation of weight-bearing on the areas being treated8. Resumption of weight-bearing/ambulation only with
offloading and appropriate support/foot orthotics.Fortunately, an array of advanced wound-healing technol-
ogy is widely available to help turn the tables in favor of limb salvage. These technologies include bioengineered alternative tissues, advanced surgical procedures, negative pressure wound therapy, hyperbaric oxygen therapy, topical growth factors, and advanced active dressings and topical care. In addition, our ability to offload pressure in patients with weight-bearing and decubitus ulcerations has significantly improved.
While detractors may criticize the expense of these newer technologies, we would encourage decision-makers to first re-view the costs of non-healing ulcerations and amputations to our healthcare system. For example, we already know that an average diabetic foot ulcer costs over $27,000.4 Foot ulcer care costs are four times higher when PAD is associated with the wound.4 And up to 84% of the cost of diabetic foot ulcer care is associated with inpatient hospital stays.4 If new technologies can heal wounds and prevent hospitalizations, they may actu-ally present a major cost containment victory.
When confronted with a non-healing lower-extremity wound in the lower extremity, one of the first challenges is to convert the wound surface into a properly prepared wound bed for the next stage of healing. Topical and systemic means, via conservative and surgical procedures, should be used to rid the wound of biofilm, excessive drainage and non-viable tis-sue. (Wound bed preparation should be performed after revas-cularization to prevent unnecessary tissue loss from ischemia.) Once the wound has been prepared and the blood flow is suf-
Figure 2. Revascularization of a patient with gangrene of the dorsum of the foot and toes. Images courtesy of Rasesh M. Shah, MD, and John Steinberg, DPM, FACFAS
Cannot be reprinted without
permission of HMP Communications

Supplement to Podiatry Today® and Vascular Disease Management® Preventing Critical Limb Ischemia 23
ficient, ultimate wound closure should be achieved via grafting, secondary intention or surgical means. “Reconstructive ladder” is a term that refers to the stepwise decision-making process that should be used to determine the most appropriate way to heal a given wound.
After revascularization comes excisional debridement of the non-healing wound. Remove all necrotic and non-viable tis-sue from the wound base and the wound margins so that the exudate is reduced to moderate levels, the margins are no lon-ger undermined, and the wound is free from excessive bacte-rial load. Negative pressure wound therapy (NPWT) is a key technology used in combination with surgical debridement. NPWT applies sub-atmospheric pressure to the wound in the form of an active, closed-suction drain. The negative pressure is also responsible for reduced bacterial count, stimulation of angiogenesis, exercise of the cell membrane and re-approxi-mation of the wound edges. Bioengineered alterative tissues and advanced surgical reconstruction techniques can be ap-plied when the wound is deemed properly prepared for closure.
It’s imperative to determine the wound etiology early in the diagnostic workup. Many diabetic foot ulcers occur on the plantar aspect of the foot, primarily due to abnormal bio-mechanics during the gait cycle. Given that one of the key goals of limb salvage is that a patient be able to use a limb after wound healing, more than skin coverage is needed at the wound site. Unless the underlying tendon, bone or me-chanical abnormality is corrected as part of the comprehensive treatment plan, the patient is almost certainly doomed to suffer wound recurrence after returning to a weight-bearing status.
Case Study In Figure 3, the patient presents with a non-healing wound
after a partial third ray amputation. This wound is fibrotic and probes deeply, but shows no evident abscess formation or ascending infection. Given the relatively stable nature of the wound, a timely vascular consultation is done before any debridement or advanced wound care attempts.
The center photo shows the wound after revasculariza-tion and subsequent surgical debridement. Now the advanced wound care technologies can be safely applied in the face of restored tissue oxygenation. For this example, bioengineered alternative tissues were combined with NPWT to ultimately provide wound closure and successful amputation prevention/limb salvage.
ConclusionCommunication and teamwork are paramount to limb sal-
vage. This is a high-stakes pathology — major morbidity and mortality are associated with even very distal amputation in the extremity. Literature reviews have repeatedly shown that comprehensive amputation prevention teams can lower the rates of proximal leg amputation significantly.8 While some-one should direct a patient’s care process, there’s no room for
ego-driven decisions or isolationism. The team approach si-multaneously and rapidly tackles the problem, reassures the family and patient everything possible is being done, and helps spread the liability associated with these challenging case types. Individuals routinely involved in limb salvage include vascu-lar specialists, podiatrists, plastic surgeons, orthopedists, nurse practitioners, physical therapists, infectious disease specialists, rheumatologists, endocrinologists, nephrologists, hospitalists and prosthetists/orthotists. n
References1. Population Division, Department of Economic and Social
Affairs, United Nations. World Population Ageing 1950-2050. 2002. Available at http://www.un.org/esa/popula-tion/publications/worldageing19502050/
2. Jensen SA, Vatten LJ, Myhre HO. The prevalence of chron-ic critical lower limb ischemia in a population of 20,000 subjects 40–69 years of age. Eur J Vasc Endovasc Surg. 2006;32:60–65.
3. Norgren L, Hiatt WR, Dormandy JA, Nehler MR, Har-ris KA, Fowkes FG, et al. Inter-society consensus for the management of peripheral arterial disease (TASC II). J Vasc Surg. 2007;45(Suppl S):S5–S67.
4. Hunt NA, Liu GT, Lavery LA. The economics of limb salvage in diabetes. Plast Reconstr Surg. 2011;127 Suppl 1:289S–295S.
5. Taylor GI, Palmer JH. The vascular territories (angio-somes) of the body: experimental study and clinical ap-plications. Br J Plast Surg. 1987;40(2):113-141.
6. Samson RH, Sprayregen S, Veith FJ, et al. Management of angioplasty complications, unsuccessful procedures and early and late failures. Ann Surg. 1984;199(2):234–240.
7. Karacagil S, Almgren B, Bowald S, Eriksson I. Angiographic criteria for prediction of early graft failure of secondary in-frainguinal bypass surgery. J Vasc Surg. 1990;12(2):131–138.
8. Centers for Disease Control and Prevention. 2011 Na-tional Diabetes Fact Sheet. 2011. Available at www.cdc.gov/diabetes/pubs/factsheet11.htm
Figure 3. The patient presented with a non-healing wound after a partial third ray amputation.
Images courtesy of Rasesh M. Shah, MD, and John Steinberg, DPM, FACFAS
155-7889 22354 01/12
Cannot be reprinted without
permission of HMP Communications
Cannot be reprinted without
permission of HMP Communications