Embed Size (px)
DESCRIPTION
FOR MORE MEDICAL PRESENTATIONS AND VIDEOS http://medicalpresentation.blogspot.in/
Citation preview

64 yr old male with previous history of
heart attack came to casualty with c/o sudden onset of pain in the right leg below the knee.
On examination….



Absent popliteal and lower pulsations Decreased sensations Inability to move toes

Acute limb ischemia

EtiologyEtiology of of acute limb ischemiaacute limb ischemia
Acute arterial embolism:
Acute traumatic ischemia:
Of a relatively Of a relatively health arterial treehealth arterial tree
Acute arterial thrombosis: Of a previously Of a previously diseased arterial treediseased arterial tree


Patho-pysiologyPatho-pysiology

Acute Embolic IschemiaAcute Embolic Ischemia
An embolus suddenly
occludes a relatively
healthy arterial tree
It usually arrest at arterial
bifurcation
Aortic bifurcation
Iliac bifurcation
Femoral bifurcation
Popliteal trifurcation
An embolus can originate from the heart (MS with atrial fibrillation, MI with mural
thrombus) or dilated diseased arteries (aortic aneurism)

Example of acute arterial embolus
“Saddle” Embolus of right iliac artery

Acute Thrombotic Acute Thrombotic IschemiaIschemia
AtherosclerosisAtherosclerosis causes
progressive narrowing of the
arterial tree
Sluggish flow & rough surface will favor acute
thrombosis
Stimulates development of
collaterals

Clinical PictureClinical Picture

Clinical Evaluation of Acute Ischemia Clinical Evaluation of Acute Ischemia (Clinical Picture)(Clinical Picture)
Signs of acute ischemiaSigns of acute ischemia
5P5PsPainPain: symptom
++
PulselessPulseless
PalePale
ParasthesiaParasthesia
ParalysisParalysis
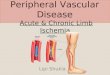
InspectionInspection
COLOR:
EarlyEarly: pale
LaterLater: cyanosed mottling fixed mottling & cyanosis
Pallor
Reversible mottling
An area of fixed cyanosis
surrounded by reversible mottling
Empty veins: compare the Rt. (ischemic) & Lt. (normal)
Fixed mottling & cyanosis

Clinical Evaluation of Acute Ischemia Clinical Evaluation of Acute Ischemia (Clinical Picture)(Clinical Picture)
Signs of acute ischemiaSigns of acute ischemia
5P5PsPainPain: symptom
++
PulselessPulseless
PalePale
ParasthesiaParasthesia
ParalysisParalysis
PalpationPalpation
FemoralFemoral PoplitealPopliteal
Posterior tibialPosterior tibial Dorsalis pedisDorsalis pedis
Palpate peripheral pulsesPalpate peripheral pulses, compare with the other side & write it down on a sketch
TemperatureTemperature: the limb is cold with a level of temperature change (compare the two limbs)
Slow capillary refillingSlow capillary refilling of the skin after finger pressure

Clinical Evaluation of Acute Ischemia Clinical Evaluation of Acute Ischemia (Clinical Picture)(Clinical Picture)
Signs of acute ischemiaSigns of acute ischemia
5P5PsPainPain: symptom
++
PulselessPulseless
PalePale
ParasthesiaParasthesia
ParalysisParalysis
PalpationPalpation
Loss of sensory function
Numbness will progress to anesthesia
Progress of Sensory loss
Light touch
Vibration sense
Proprioreception
Deep pain
Pressure sense LateLate

Clinical Evaluation of Acute Ischemia Clinical Evaluation of Acute Ischemia (Clinical Picture)(Clinical Picture)
Signs of acute ischemiaSigns of acute ischemia
5P5PsPainPain: symptom
++
PulselessPulseless
PalePale
ParasthesiaParasthesia
ParalysisParalysis
PalpationPalpation
Loss of motor function:Loss of motor function:
Indicates advancedadvanced limb threatening ischemia
Late irreversible ischemia: Muscle turgidity
Intrinsic foot muscles are affected first, followed by the leg muscles
Detecting early muscle weakness is difficult because toes movements are produced mainly by leg muscles


Investigations
The severity and duration of The severity and duration of ischemia at the time of ischemia at the time of presentation provides a presentation provides a
narrow margin of timenarrow margin of time for for investigationsinvestigations

general investigations CK [Patients with a
suspected hypercoagulable state will need additional studies seeking:]
Anticardiolipin antibodies
Elevated homocysteine concentration
Antibodies to platelet factor IV

Doppler USDoppler US
to assess the level of obstruction & severity of ischemia

What are welooking for?
NORMAL• Multiphasic
• Pulsatile• Regular amplitude
An audible Doppler signal assures some blood flow No Doppler signals, a vascular surgeon should be immediately consulted


0.7 to 0.9 is mild disease,0.5 to 0.69 is moderate disease,< 0.5 is severe disease.


ArteriographyArteriography
If the differentiation between embolic & thrombotic ischemia is not clear clinically, and if the limb condition permits,
DO ANGIOGRAPHYDO ANGIOGRAPHY

Value of angiographyValue of angiography Localizes the obstruction Visualize the arterial tree & distal run-
off Can diagnose an embolus: Sharp cutoff, reversed meniscus or clot
silhouette

WWW.SMSO.NET
Embolism:
obvious cardiac source
No hx of cluadication
Normal pulses in contralateral limb
Angiogram: minimal atherosclerotic
Few collateral
Thrombosis:
No obvious cardiac source.
history of cluadication.
abnormal pulses in contralateral limb.
Angiogram: diffuse atherosclerotic
Well developed collateral

CategoryCategory DescriptionDescription Cap. refillCap. refill ParalysisParalysis Sensory Sensory lossloss
AA VV
II ViableViable Not immediately Not immediately threatenedthreatened
IntactIntact -- -- AudAud AudAud
IIaIIa ThreatenedThreatened Salvagable if Salvagable if treatedtreated
Intact/slowIntact/slow -- PartialPartial __ AudAud
IIbIIb ThreatenedThreatened Salvagable if Salvagable if treated treated emergentlyemergently
Slow/absentSlow/absent PartialPartial PartialPartial __ AudAud
IIIIII IrreversibleIrreversible Primary Primary amputation req.amputation req.
AbsentAbsent CompleteComplete CompleteComplete __ __
DopplerDoppler


TREATMENT
Goals of therapy include restoration of blood flow,
preservation of limb and life, and prevention of recurrent
thrombosis

IMMEDIATE CARE
THROMBOLYTICS
SURGERY

A. Immediate care
Anticoagulation Analgesia measures to improve existing perfusion treatment of associated cardiac
conditions

B B Catheter directed Catheter directed thrombolysisthrombolysis
Agents used: Streptokinase, Urokinase, tissue plasminogen
activator
IndicationsIndications:
1. Viable or marginally threatened limb (class I, IIa)
2. Recent acute thrombosis (not suitable for embolism or old thrombi)
3. Avoid patients with contraindications

ContraindicationsContraindications::
AbsoluteAbsolute:
1. Cerebro-vascular stroke within previous 2 months
2. Active bleeding or recent GI bleeding within previous 10 days
3. Intracranial trauma or neurosurgery within previous 3 months
RelativeRelative:
1. Cardio-pulmonary resuscitation within previous 10 days
2. Major surgery or trauma within previous 10 days
3. Uncontrolled hypertension

SURGERY
OPERATIVE REVASCULARISATION AMPUTATION

Fogarty balloon catheter (with post-op anti coagulants)



Surgery [Surgery may be considered in trauma, where there
are contraindications to CDT, or where CDT is not available.
The method of revascularization (open surgicalor endovascular) may differ depending on:
Anatomic location of occlusion Etiology of ALI Contraindications to open or endovascular
treatment Local practice patterns]

Amputation
for irreversible ischemia with permanent tissue damage

Clinical outcomes• Mortality -15–20%.
• Major morbidities include:
1. Due to major bleeding 10–15% of patients require transfusion/and or operative intervention
2. Amputation (25–30% of patients)3. Fasciotomy (5–25% of patients)4. Renal insufficiency (up to 20% of patients)

Follow-up care
warfarin, often for 3–6 months or longer.
Patients with thromboembolism will need long-term anticoagulation, possibly lifelong.
If contraindicated due to bleeding risk factors>> platelet inhibition therapy


Algorithm to be followed…
Patient with suspected ischemia
History Examination investigations
Acute limb ischemia confirmed and staged

Heparin
I IIA IIb III
AMPUTATION
EMERGENCYOPERATIVE
RE-VASCULARISATION
EARLY INTERVENTION
NO YES
TREAT FORCHRONIC ISCHEMIA
SAME AS FOR IIa

Management of IIa
ARTERIOGRAPHY
No lesion
Discrete localized lesions
Multiple extensive lesions