Embed Size (px)
Citation preview
BOTUCATU SCHOOL OF MEDICINE, SAO PAULO STATE, BRAZIL
Daniela Ponce
Peritoneal Dialysis:
An Alternate CRRT for AKI?
Faculty Disclosure
X No, nothing to disclose
March 30 - April 2, 2014
Sheraton Sonoma County
Petaluma, California
1- Why to indicate it ?
2- For whom?
3- How to prescribe it?
4- Which complications?
5- Is it better or worse than other methods?
7- Conclusion
Peritoneal Dialysis in AKI
6- PD in AKI: 10 years of Brazilian experience

• simple technique
• no anticoagulation
• low risk of bleeding
• hemodynamically unstable patients
• low risk of electrolyte disorders
• less expensive than CRRT
Advantages of PD
2. Why ?
Disadvantages of PD
Complications related to PD
Low efficiency
UF not controled
Need to peritoneal integrity

Costs of dialysis therapy in AKI
*Canadá
iHD CRRT
0
100
200
300
400
500
US$/dia
CRRT SLED
Manns*
(Crit Care, 2003)
iHD PD
700
600
Berbece*
(Kid Int, 2006)
CRRT
Ponce
(Botucatu, 2010)
iHD PD
Chitalia (Índia)
(Kid Int 2002)
Automatic
Flexible catheter
High volume
40 l/session
Mannual
Rigid Catheter
20 l/session
Manufactured Dialysate
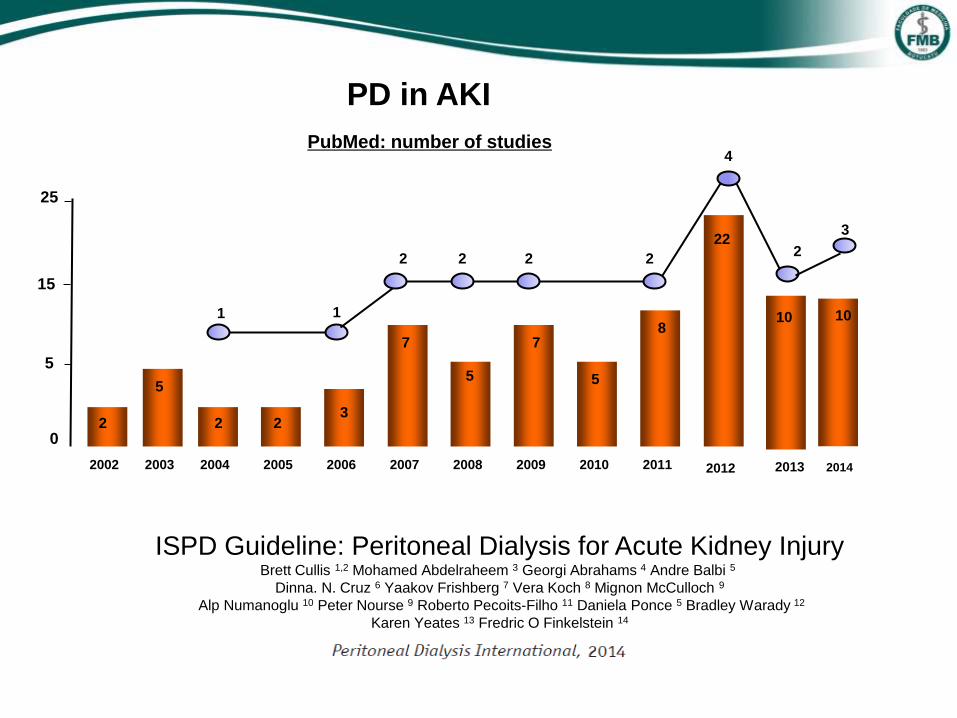
PD in AKI
PubMed: number of studies
0
5
15
25
2 3
7 8
22
2002 2003 2004 2005 2006 2007 2008 2009 2010 2011 2012
5
2 2
7
5 5
1 1
2 2 2 2
4
Artículos de Botucatu
10 10
2013 2014
2
3
ISPD Guideline: Peritoneal Dialysis for Acute Kidney Injury Brett Cullis 1,2 Mohamed Abdelraheem 3 Georgi Abrahams 4 Andre Balbi 5
Dinna. N. Cruz 6 Yaakov Frishberg 7 Vera Koch 8 Mignon McCulloch 9
Alp Numanoglu 10 Peter Nourse 9 Roberto Pecoits-Filho 11 Daniela Ponce 5 Bradley Warady 12
Karen Yeates 13 Fredric O Finkelstein 14

1- Why to indicate it ?
2- For whom?
3- How to prescribe it?
4- Wich complications?
5- Is it better or worsen than other methods?
6- PD in AKI: 10 years of Brazilian experience
7- Conclusion
Peritoneal Dialysis in AKI
Choice of dialysis method in AKI
Indications and contra-indications of each method
Hemodinamic stability and hypercatalism
Nephrology team experience
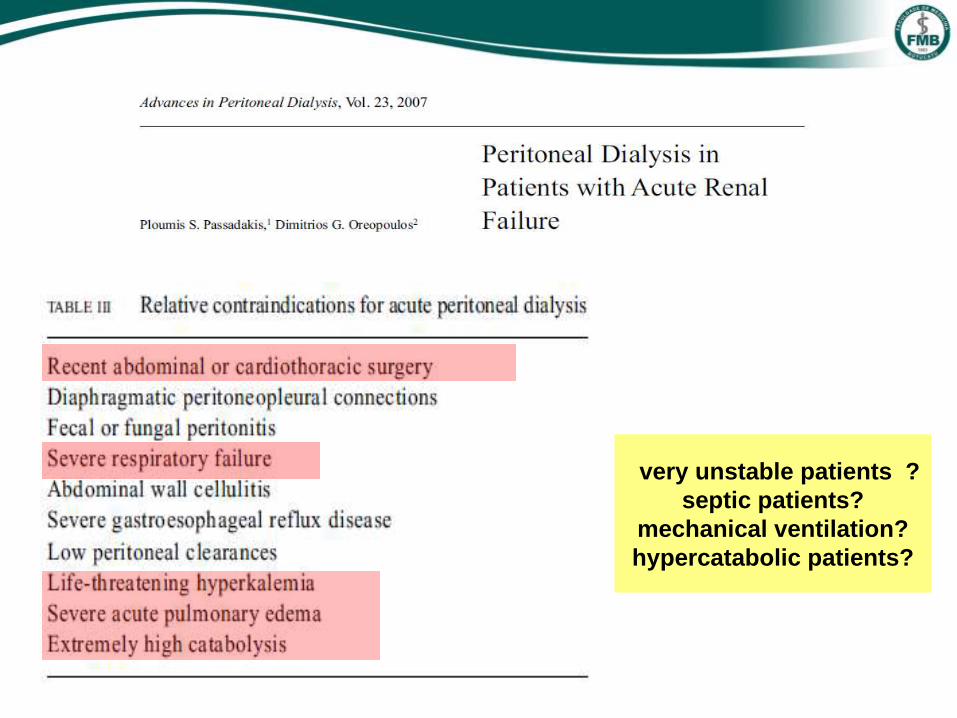
very unstable patients ?
septic patients?
mechanical ventilation?
hypercatabolic patients?
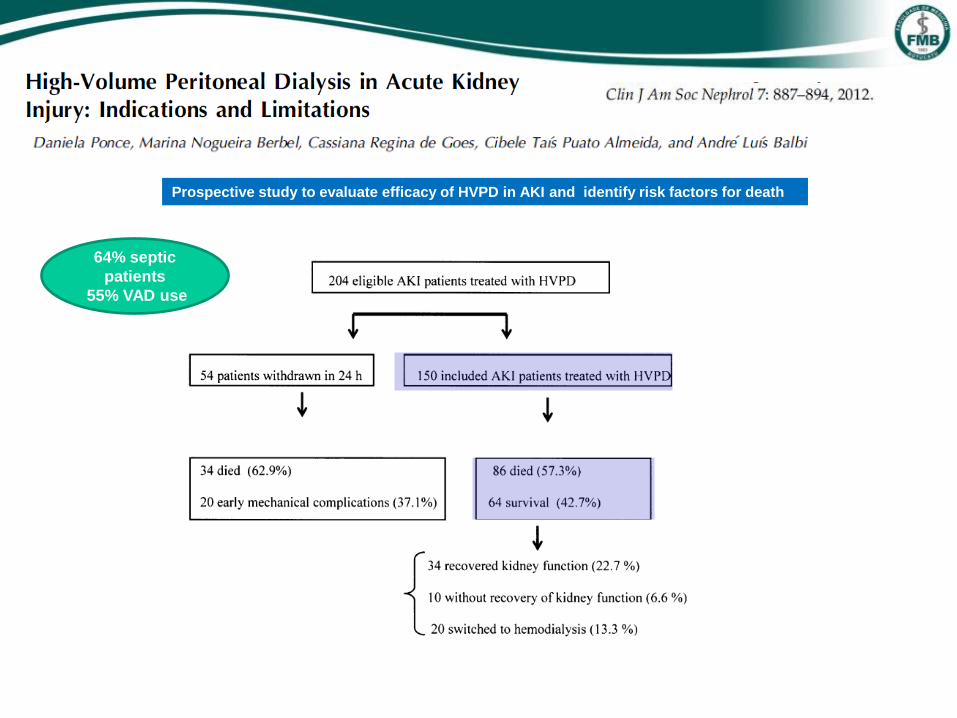
Prospective study to evaluate efficacy of HVPD in AKI and identify risk factors for death
64% septic
patients
55% VAD use
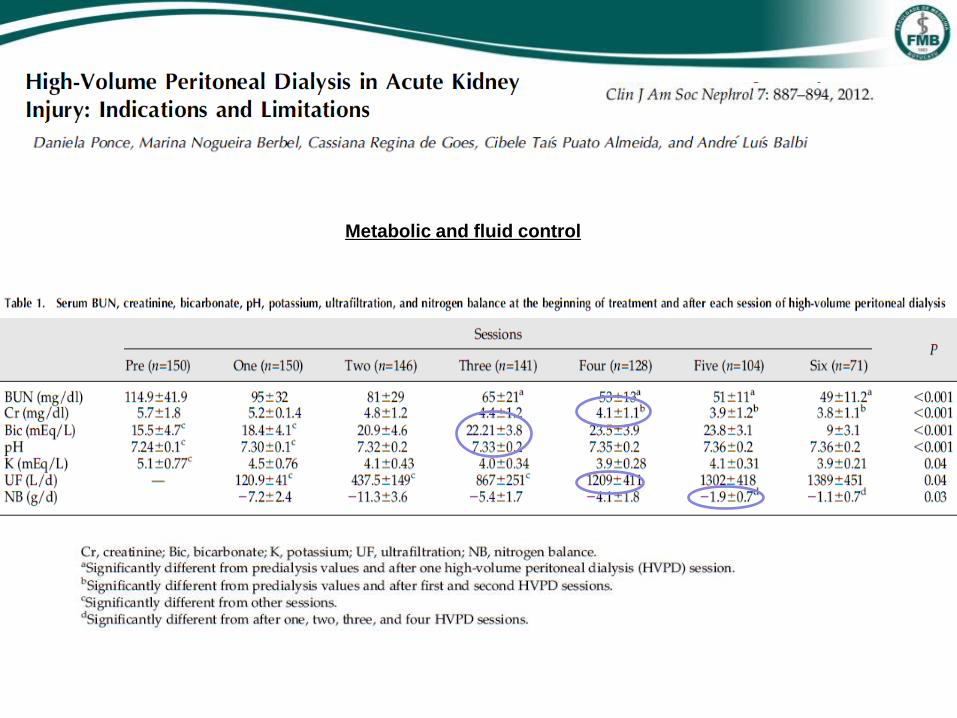
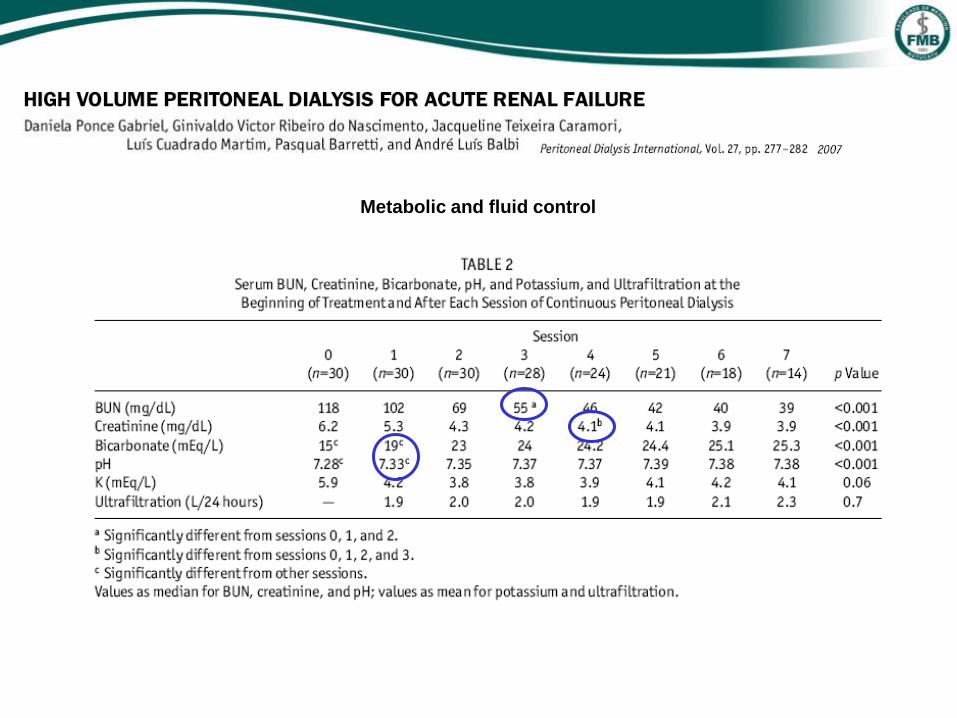
Metabolic and fluid control
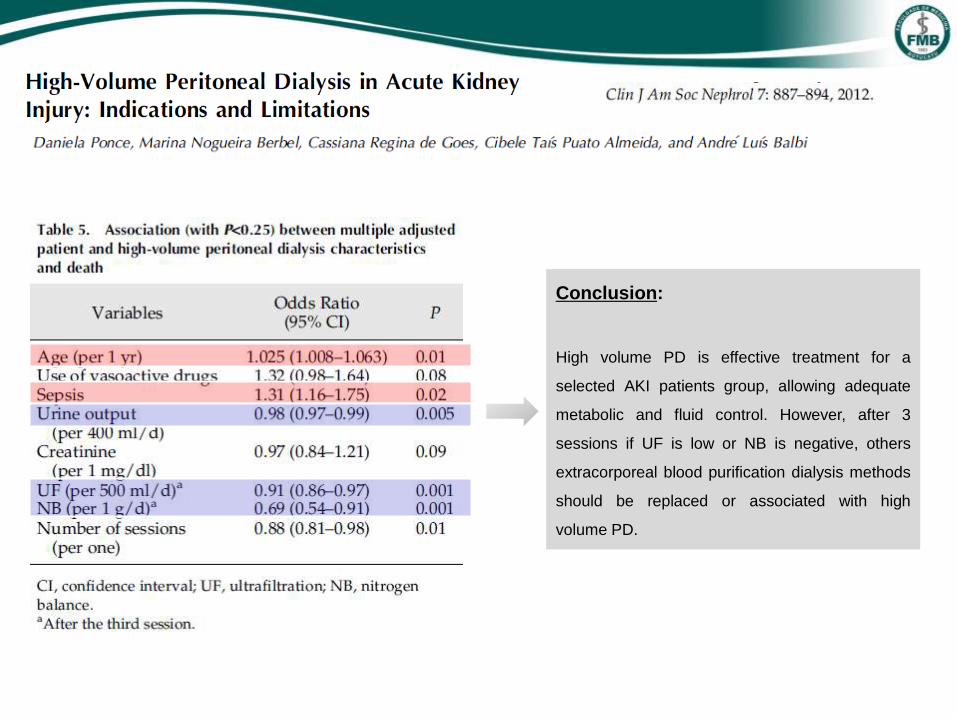
Conclusion:
High volume PD is effective treatment for a
selected AKI patients group, allowing adequate
metabolic and fluid control. However, after 3
sessions if UF is low or NB is negative, others
extracorporeal blood purification dialysis methods
should be replaced or associated with high
volume PD.

This was a prospective cohort study that evaluated respiratory mechanics in 44 HVPD sessions
performed in 20 AKI patients undergoing mechanical ventilation
We evaluated IAP, respiratory mechanics (compliance and respiratory resistance and oxygenation.
Respiratory mechanics and IAP were evaluated at 5 moments during 3 days of dialysis
Under
mechanical
ventilation
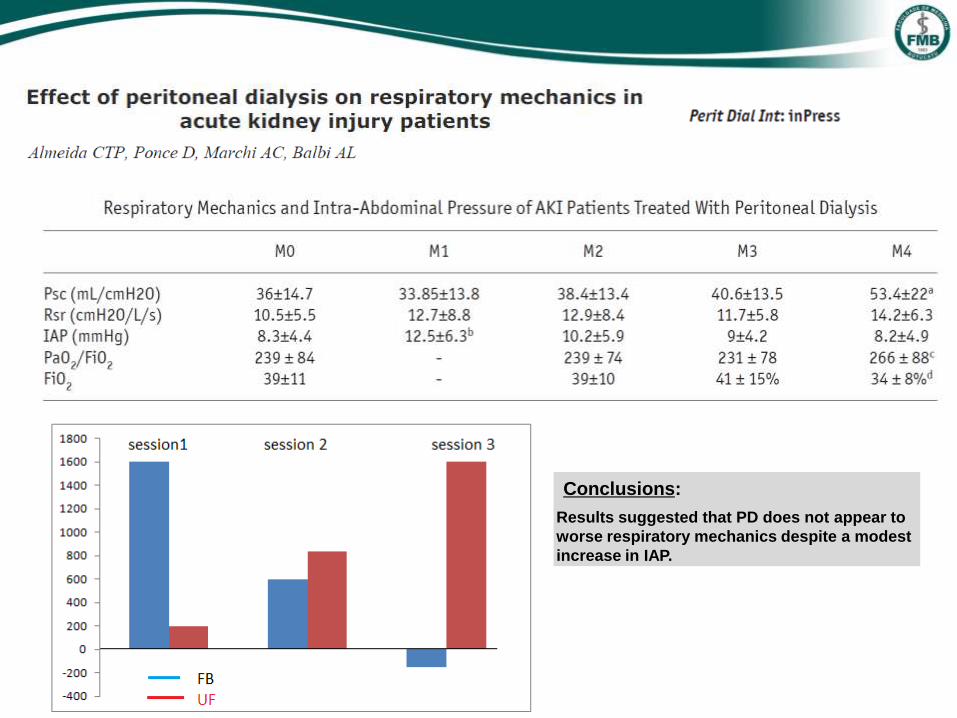
Conclusions:
Results suggested that PD does not appear to
worse respiratory mechanics despite a modest
increase in IAP.
Peritoneal Dialysis in AKI
1- Why to indicate it ?
2- For whom?
3- How to prescribe it?
4- Which complications?
5- Is it better or worsen than other methods?
6- PD in AKI: 10 years of Brazilian experience
7- Conclusion
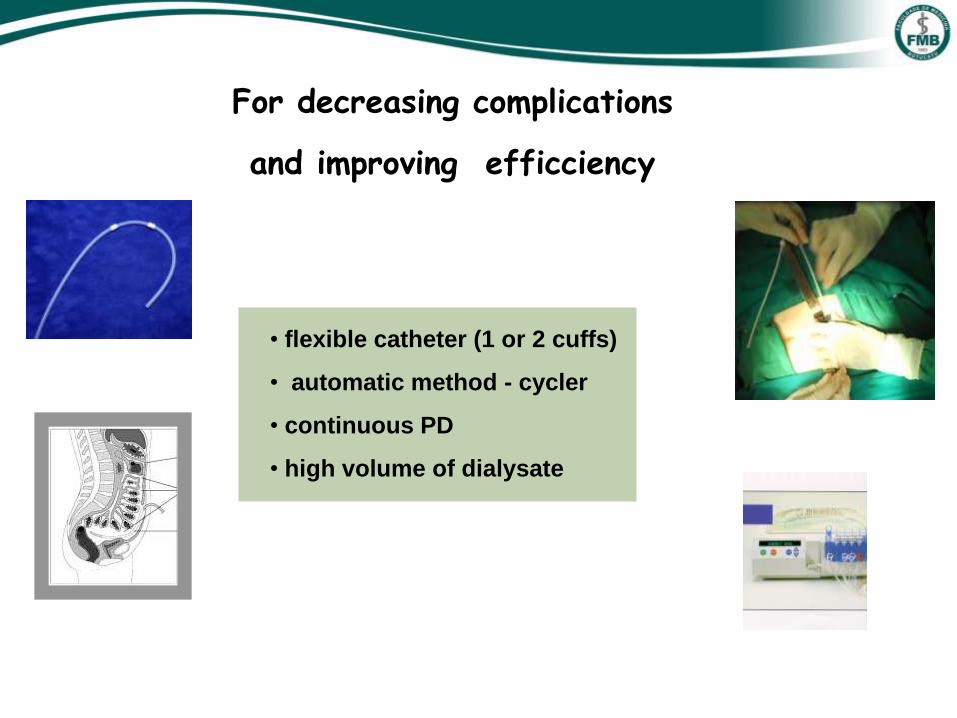
For decreasing complications
and improving efficciency
• flexible catheter (1 or 2 cuffs)
• automatic method - cycler
• continuous PD
• high volume of dialysate
Recommendations
No implantation technique was significantly better than other
Choosing the technique should be based on experience and results of each dialysis center
The involvement of nephrologist in implant procedures should always be considered, as it will be directly
responsible for patient care in the long term.
Flexible catheter in AKI patients
can be inserted by nephrologist using percutaneous technique

The aim was to investigate the early catheter complications and catheter survival according to different percutaneous
methods of catheter implantation performed by nephrologist
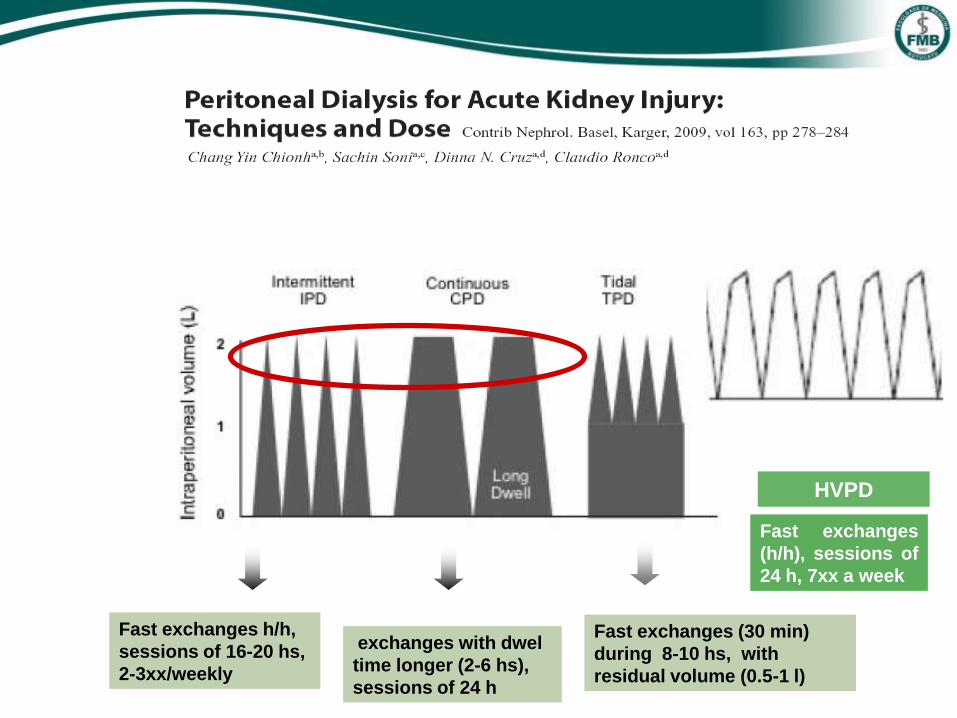
Fast exchanges h/h,
sessions of 16-20 hs,
2-3xx/weekly
exchanges with dwel
time longer (2-6 hs),
sessions of 24 h
Fast exchanges (30 min)
during 8-10 hs, with
residual volume (0.5-1 l)
HVPD
Fast exchanges
(h/h), sessions of
24 h, 7xx a week
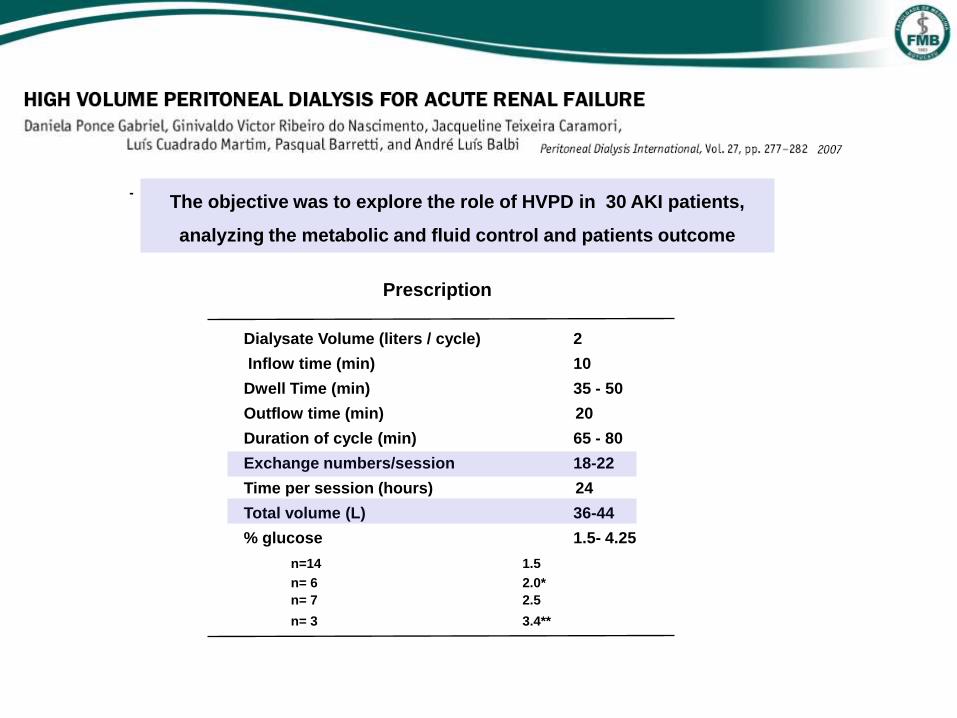
The objective was to explore the role of HVPD in 30 AKI patients,
analyzing the metabolic and fluid control and patients outcome
Dialysate Volume (liters / cycle) 2
Inflow time (min) 10
Dwell Time (min) 35 - 50
Outflow time (min) 20
Duration of cycle (min) 65 - 80
Exchange numbers/session 18-22
Time per session (hours) 24
Total volume (L) 36-44
% glucose 1.5- 4.25
n=14 1.5
n= 6 2.0*
n= 7 2.5
n= 3 3.4**
Prescription
-
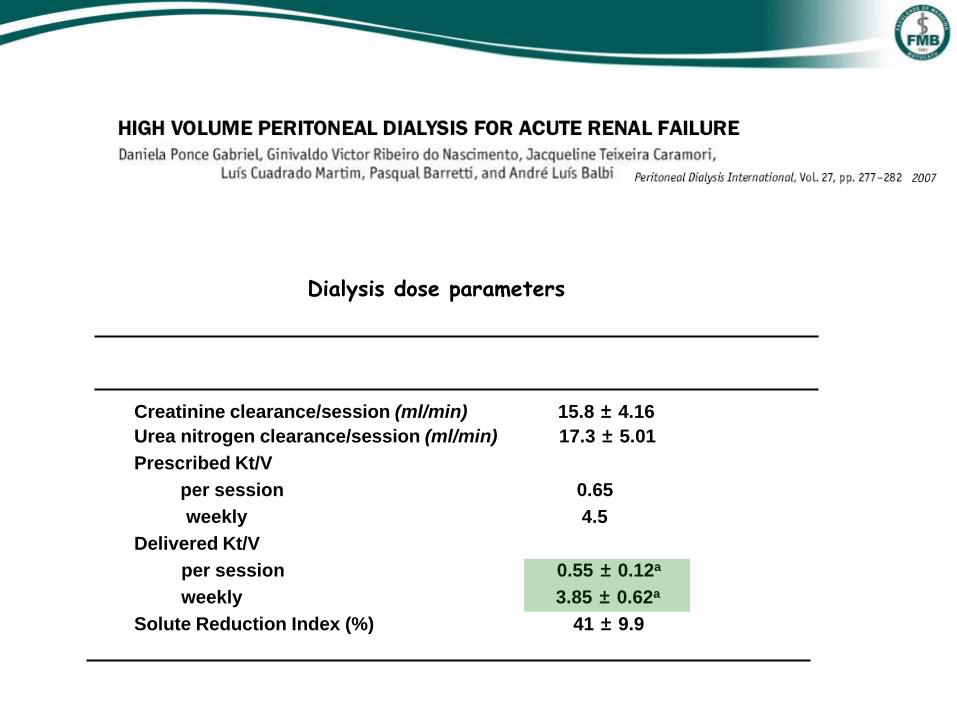
Creatinine clearance/session (ml/min) 15.8 ± 4.16
Urea nitrogen clearance/session (ml/min) 17.3 ± 5.01
Prescribed Kt/V
per session 0.65
weekly 4.5
Delivered Kt/V
per session 0.55 ± 0.12a a
weekly 3.85 ± 0.62a a
Solute Reduction Index (%) 41 ± 9.9
a= p>0.05 from prescribed Kt/V
Variable Median ± SD
Dialysis dose parameters
Metabolic and fluid control
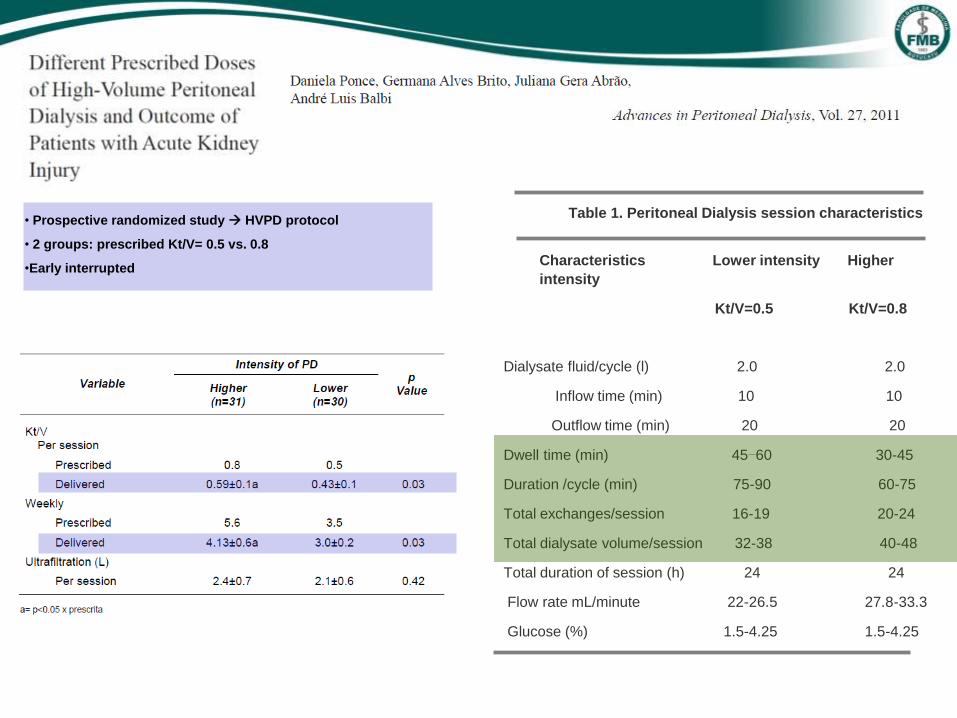
• Prospective randomized study HVPD protocol
• 2 groups: prescribed Kt/V= 0.5 vs. 0.8
•Early interrupted
Table 1. Peritoneal Dialysis session characteristics
Characteristics Lower intensity Higher
intensity
Kt/V=0.5 Kt/V=0.8
Dialysate fluid/cycle (l) 2.0 2.0
Inflow time (min) 10 10
Outflow time (min) 20 20
Dwell time (min) 45–60 30-45
Duration /cycle (min) 75-90 60-75
Total exchanges/session 16-19 20-24
Total dialysate volume/session 32-38 40-48
Total duration of session (h) 24 24
Flow rate mL/minute 22-26.5 27.8-33.3
Glucose (%) 1.5-4.25 1.5-4.25

0
20
40
60
80
100
120
140
BUN
(mg/
dl)
a. BUN (mg/dl)
0
1
2
3
4
5
6
7
Cr
(mg
/dl)
0
5
10
15
20
25
0
1
2
3
4
5
6
b. Creatinine (mg/dl)
c. Bicarbonate (mEq/L) d. Potassium (mEq/L)
Figure 3. Comparison of metabolic control in higher and lower-intensity peritoneal dialysis dose. Median serum levels of (a) BUN, (b) creatinine, (c) bicarbonate, (d) potassium, at the beginning of treatment and after each session.
Metabolic Control
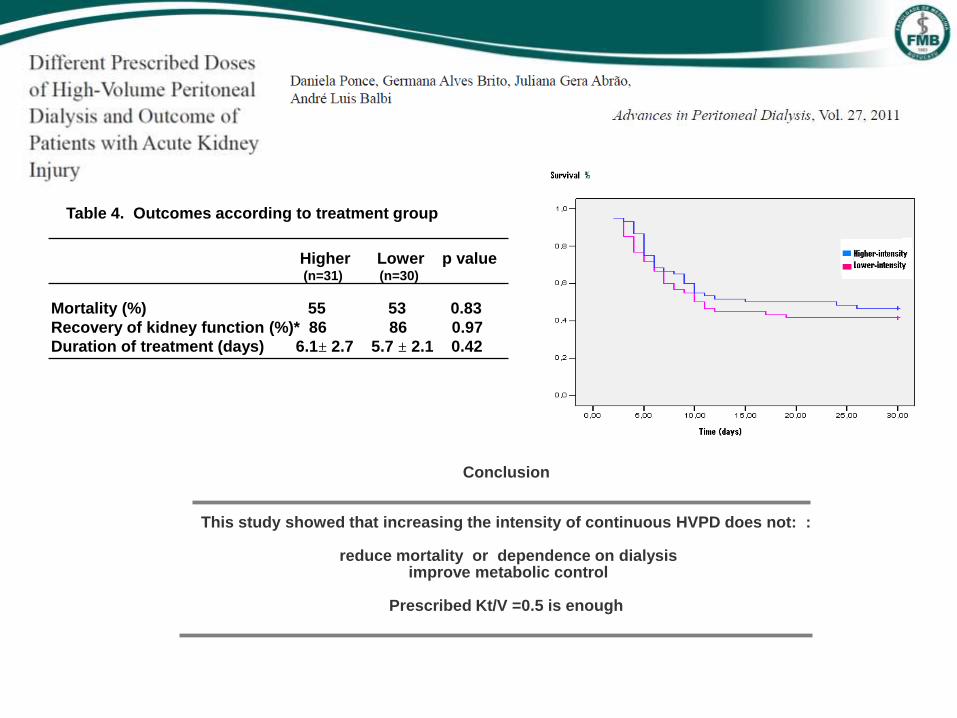
Table 4. Outcomes according to treatment group
Higher Lower p value (n=31) (n=30)
Mortality (%) 55 53 0.83
Recovery of kidney function (%)* 86 86 0.97
Duration of treatment (days) 6.1± 2.7 5.7 ± 2.1 0.42
* Recovery and resolution of kidney function of survivors only Fig 2. Comparison patient survival after 30 days treatment
Conclusion
This study showed that increasing the intensity of continuous HVPD does not: :
reduce mortality or dependence on dialysis improve metabolic control
Prescribed Kt/V =0.5 is enough

Peritoneal Dialysis in AKI
1- Why to indicate it ?
2- For whom?
3- How to prescribe it?
4- Which complications?
5- Is it better or worsen than other methods?
7- Conclusion
6- PD in AKI: 10 years of Brazilian experience
Mechanical
tip catheter migration leakage
Infectious
peritonitis
Metabolic
hyperglicemia hypokalemia
hypercatabolism
0
10
20
30
40
%
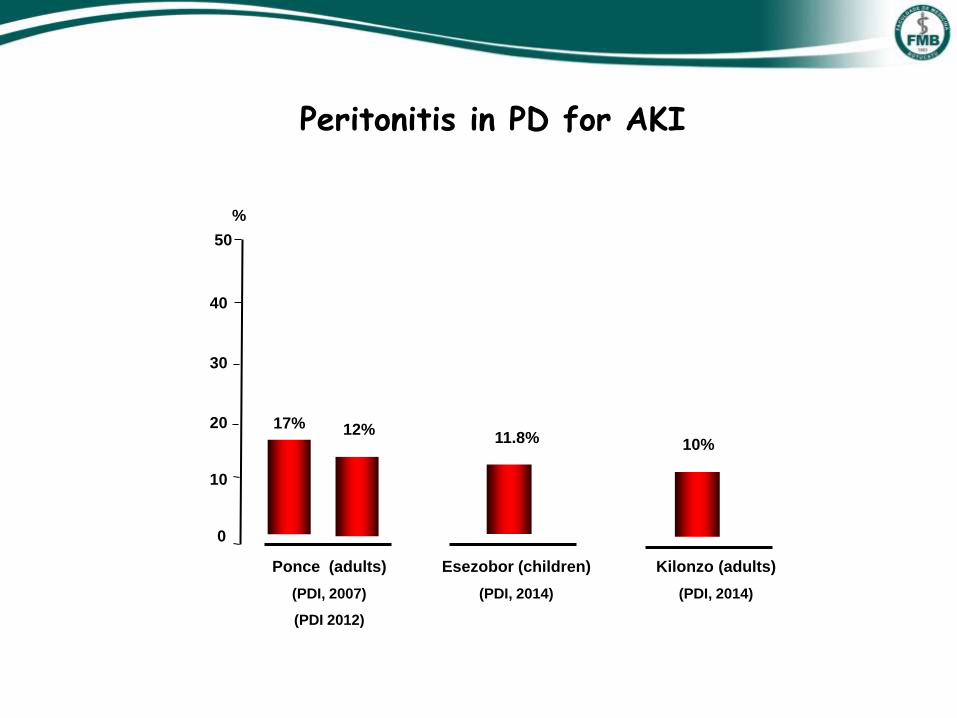
Ponce (adults)
(PDI, 2007)
(PDI 2012)
50
Esezobor (children)
(PDI, 2014)
Kilonzo (adults)
(PDI, 2014)
17% 11.8% 10%
Peritonitis in PD for AKI
12%
0
10
20
30
40
% 50
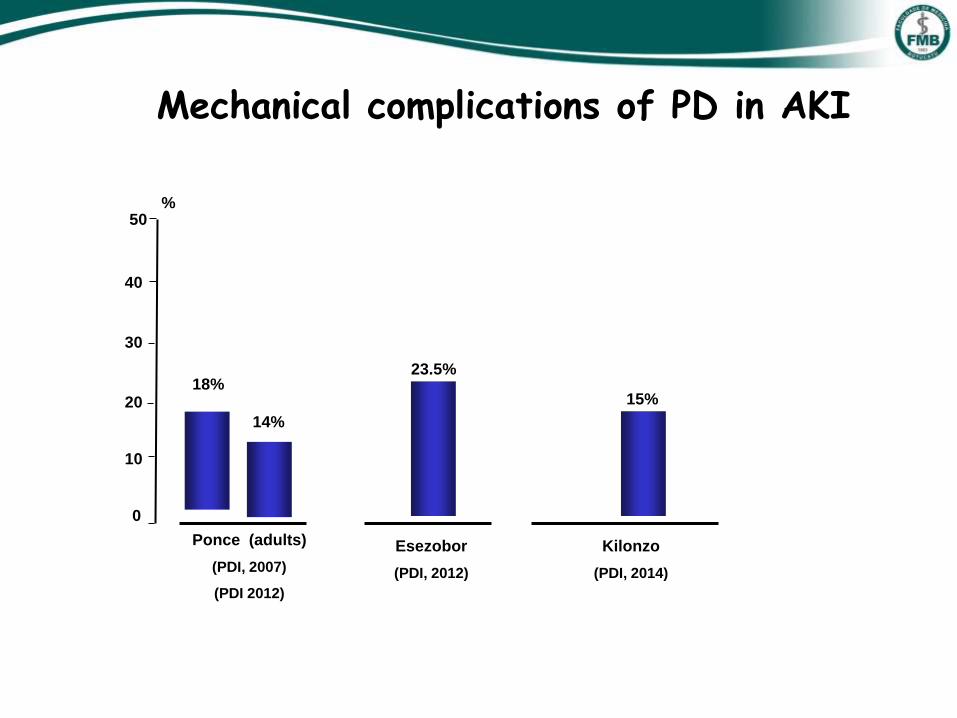
Esezobor
(PDI, 2012)
Kilonzo
(PDI, 2014)
18% 23.5%
15%
Mechanical complications of PD in AKI
14%
Ponce (adults)
(PDI, 2007)
(PDI 2012)
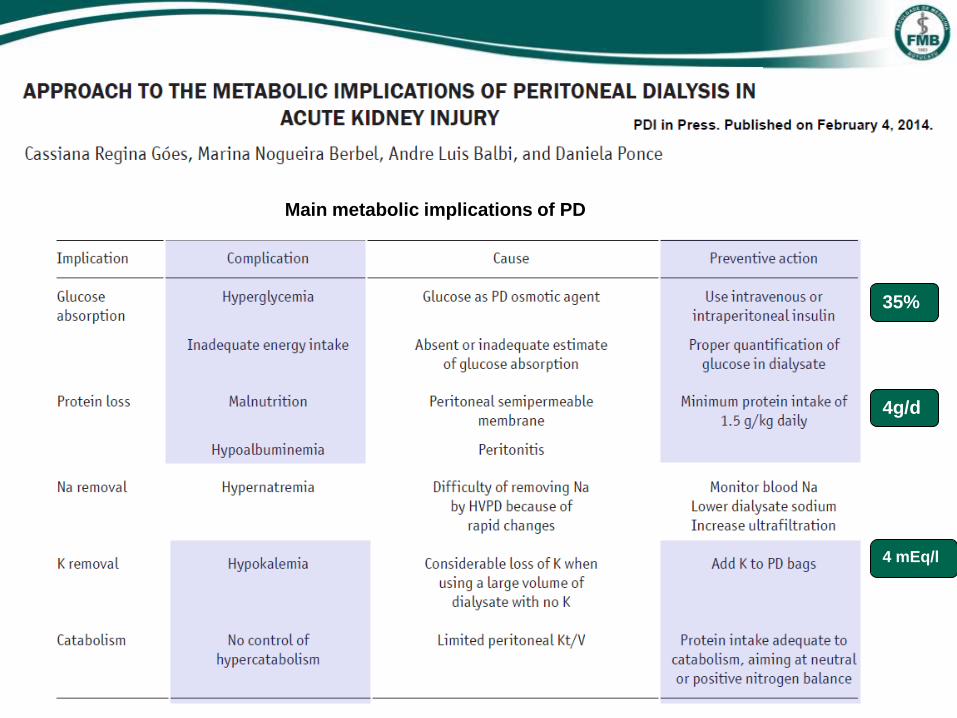
Main metabolic implications of PD
35%
4g/d
4 mEq/l
1- Why to indicate it ?
2- For whom?
3- How to prescribe it?
4- Complications?
5- Is it better or worse than other methods?
6- PD in AKI: 10 years of Brazilian experience
7- Conclusion
Peritoneal Dialysis in AKI
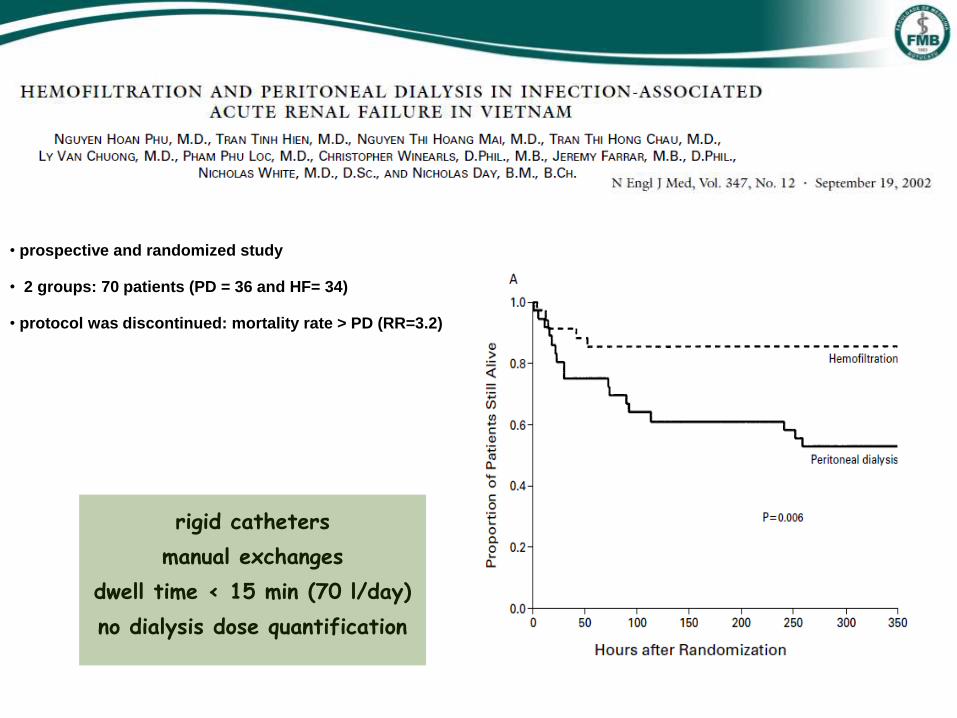
• prospective and randomized study
• 2 groups: 70 patients (PD = 36 and HF= 34)
• protocol was discontinued: mortality rate > PD (RR=3.2)
rigid catheters
manual exchanges
dwell time < 15 min (70 l/day)
no dialysis dose quantification
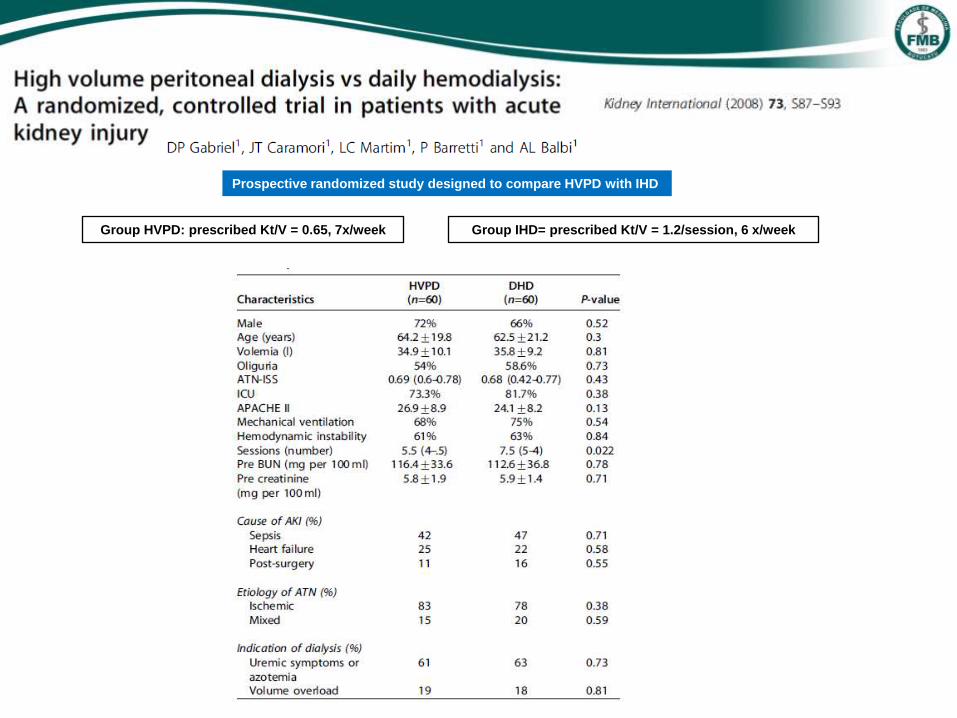
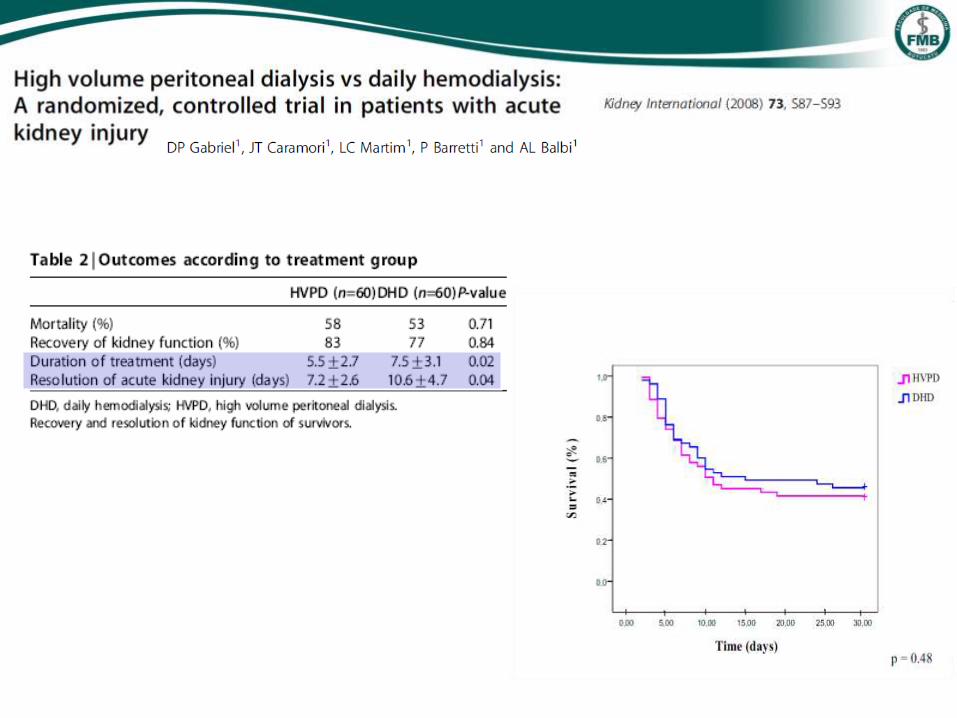
Prospective randomized study designed to compare HVPD with IHD
Group HVPD: prescribed Kt/V = 0.65, 7x/week Group IHD= prescribed Kt/V = 1.2/session, 6 x/week
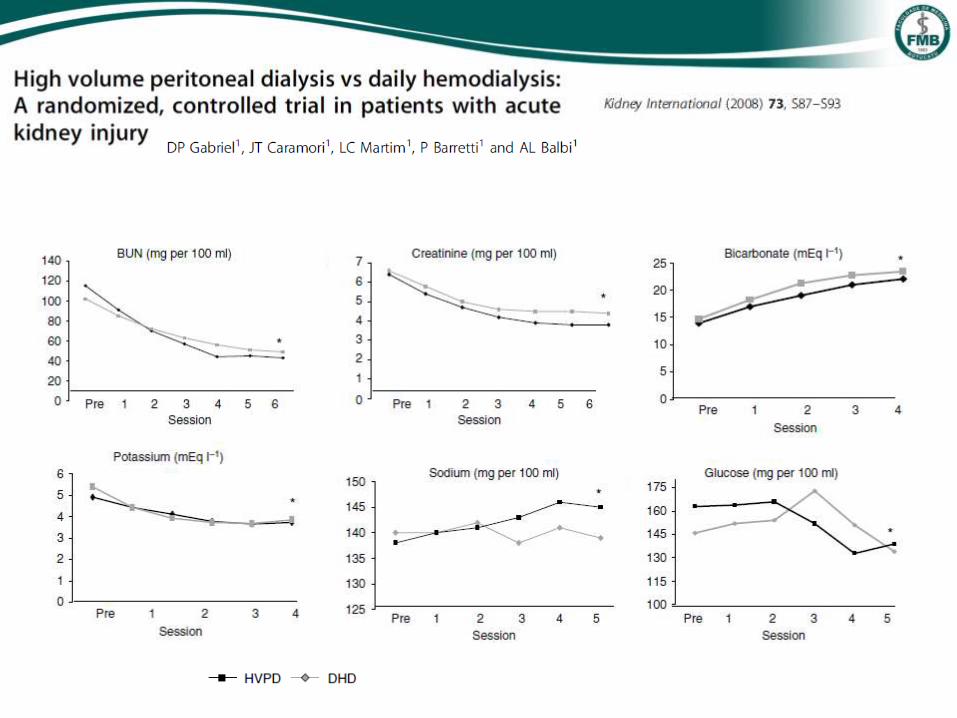
(* p>0.05)
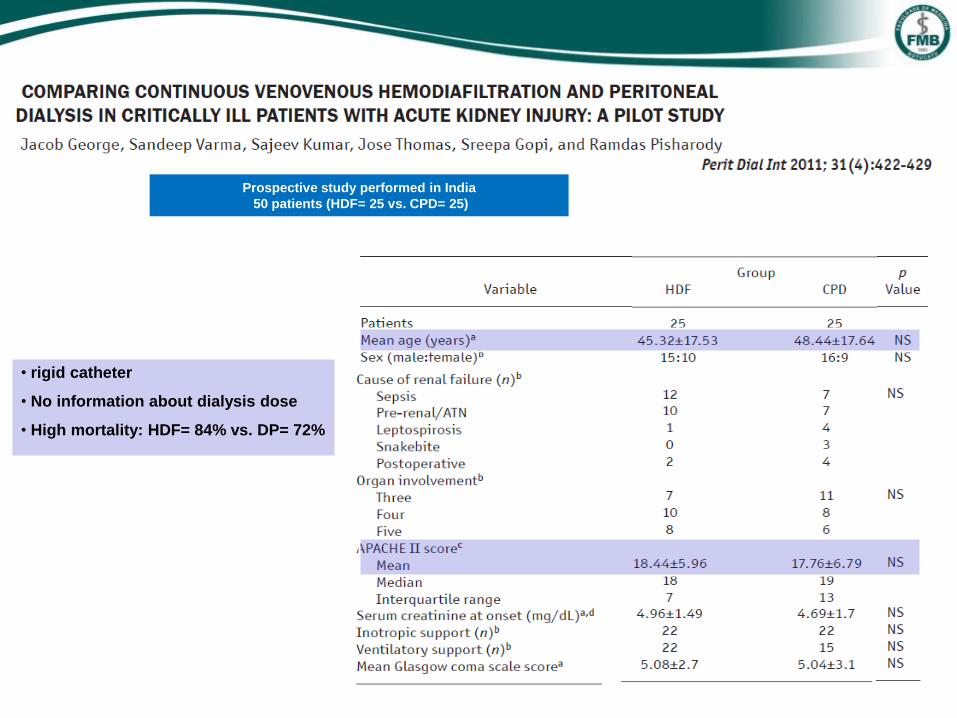
Prospective study performed in India
50 patients (HDF= 25 vs. CPD= 25)
• rigid catheter
• No information about dialysis dose
• High mortality: HDF= 84% vs. DP= 72%
Apoio: FAPESP
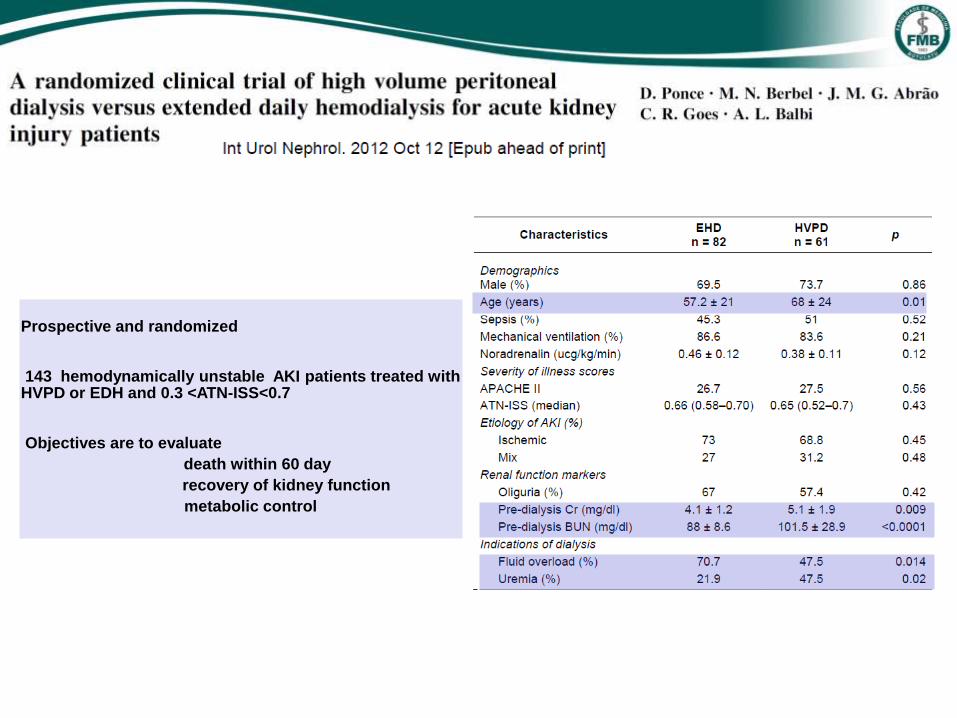
Prospective and randomized 143 hemodynamically unstable AKI patients treated with HVPD or EDH and 0.3 <ATN-ISS<0.7 Objectives are to evaluate
death within 60 day
recovery of kidney function
metabolic control
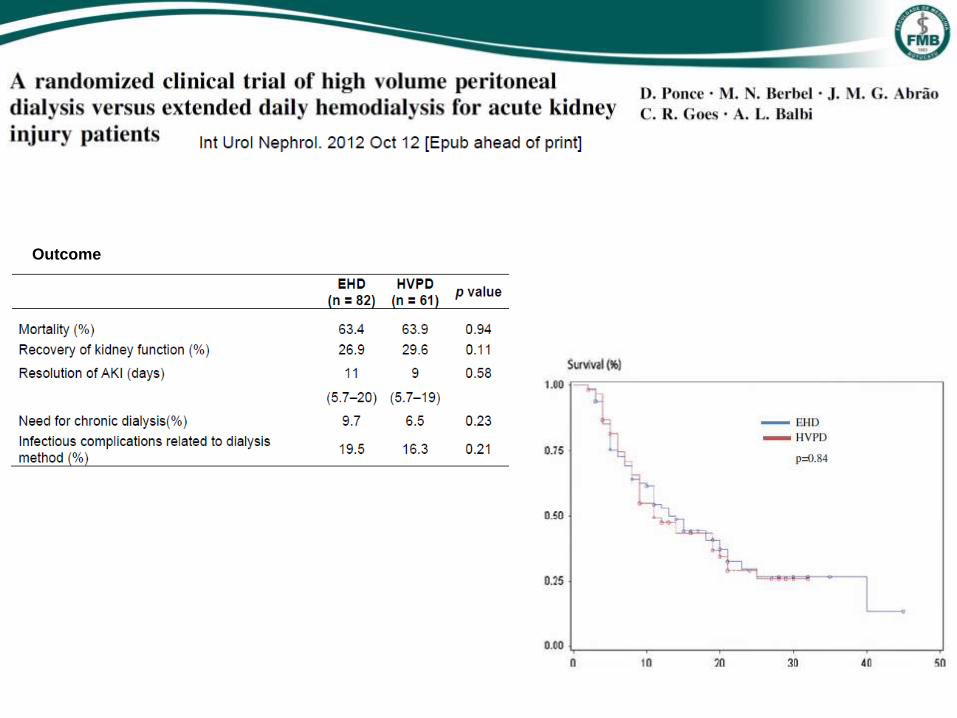
Apoio: FAPESP
Outcome
Sobrevida em 50 dias
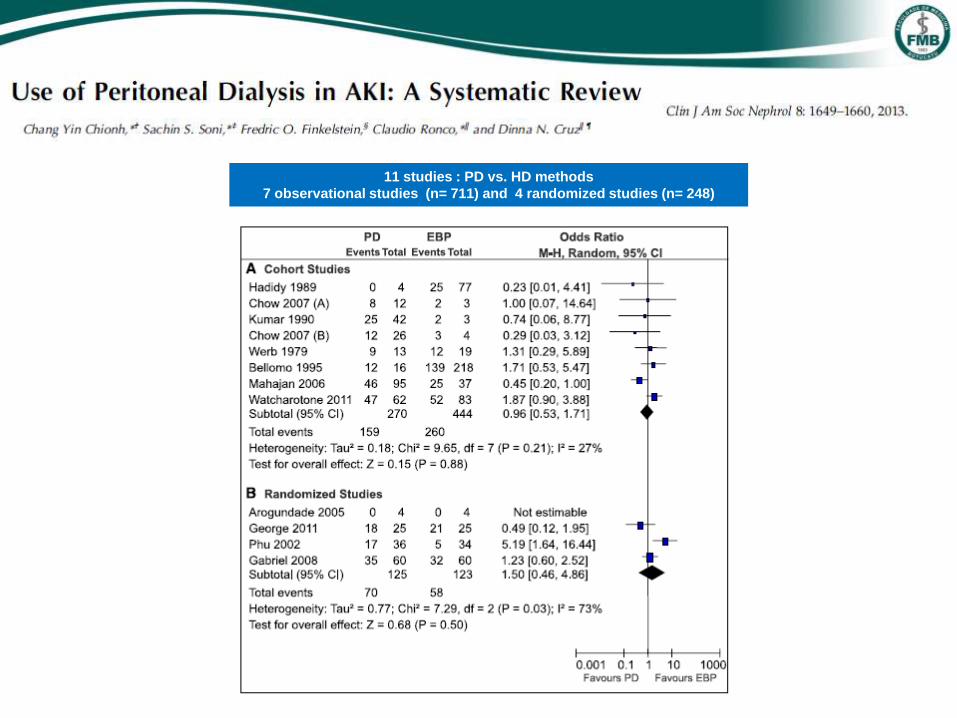
11 studies : PD vs. HD methods
7 observational studies (n= 711) and 4 randomized studies (n= 248)
1- Why to indicate it ?
2- For whom?
3- How to prescribe it?
4- Complications?
5- Is it better or worse than other methods?
6- PD in AKI: 10 years of Brazilian experience
7- Conclusion
Peritoneal Dialysis in AKI
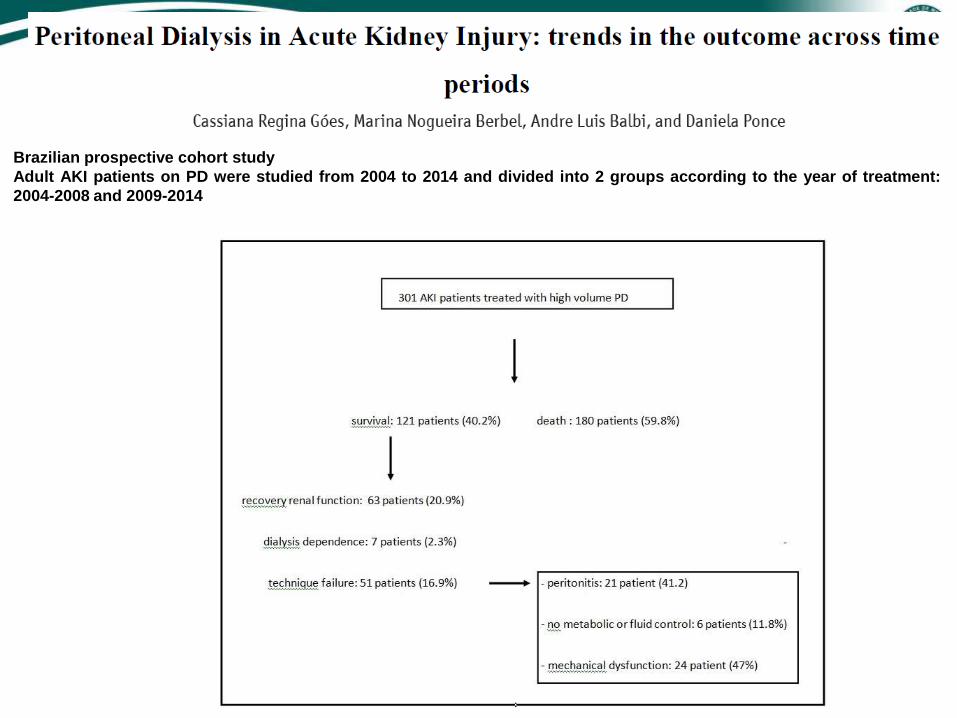
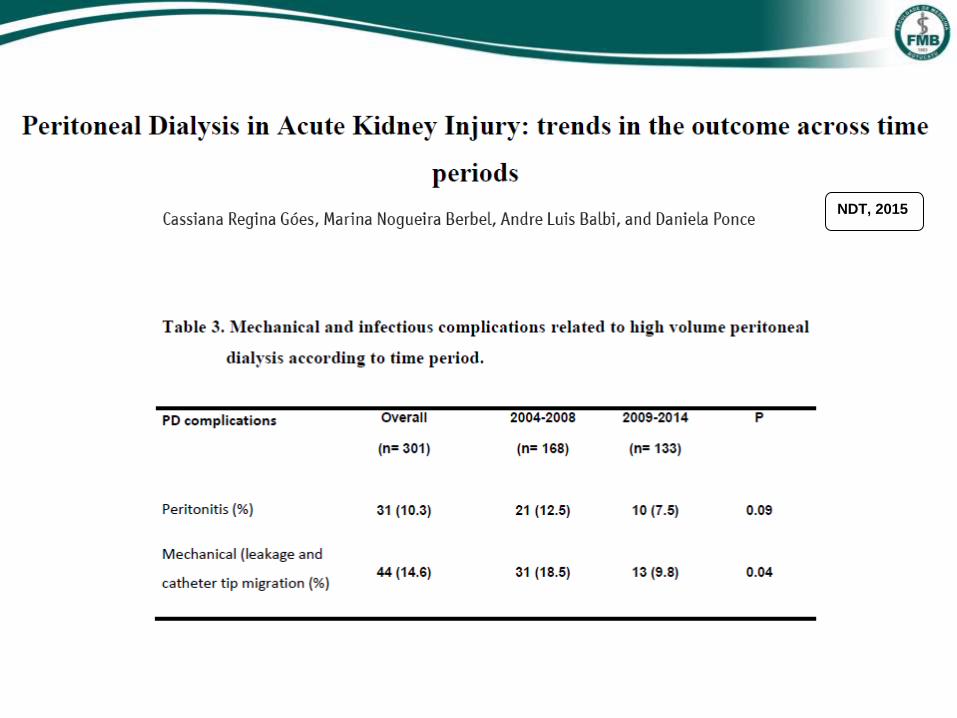
Brazilian prospective cohort study
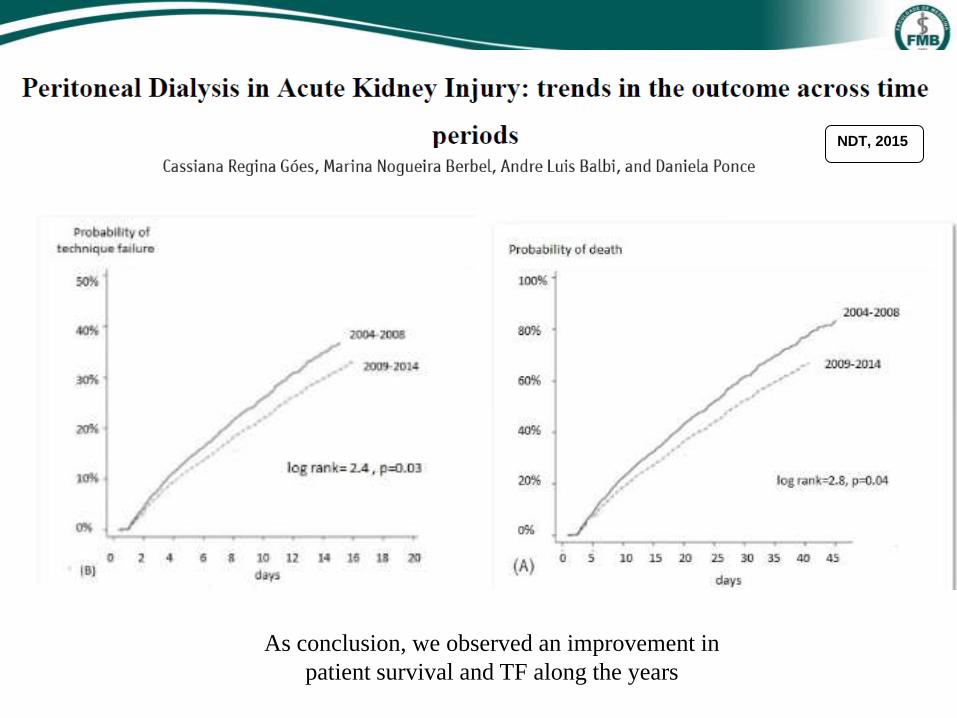
Adult AKI patients on PD were studied from 2004 to 2014 and divided into 2 groups according to the year of treatment:
2004-2008 and 2009-2014

NDT, 2015
NDT, 2015

NDT, 2015

NDT, 2015
NDT, 2015
As conclusion, we observed an improvement in
patient survival and TF along the years
1- Why to indicate it ?
2- For whom?
3- How to prescribe it?
4- Complications?
5- Is it better or worse than other methods?
6- PD in AKI: 10 years of Brazilian experience
7- Conclusion
Peritoneal Dialysis in AKI

There is growing interest in the use of PD in AKI
Because of its simplicity, PD is used in regions with limited resources and sometimes is the only method available
There is no evidence to suggest that the PD is inferior when compared to other methods of dialysis in AKI
However, the success of this method depends on the selection of patients and the team's experience
-
To overcome limitations and if possible, the PD must be performed continuously and automatically, with high volumes
of dialysate and using flexible catheter
The prescription should achieve adequate metabolic and fluid controls
Kt / V of 0.5 per session is enough
Metabolic and mechanical ventilation implications seems to be minimal
It should be discontinued after 3 sessions if no adequate fluid control
We have observed an improvement in patient survival and TF along the years
It is an option to treat AKI patients, mainly in developing countries
• Prof André Luis Balbi
• Nutrit Marina Nogueira Berbel
• Nutrit Cassiana Goes
• Nurse Bianca Albino
• Nurse Mariele Gobo
Thank you very much AKI team
•Tec Enf Elza Maria Januário
• Tec Enf Ana Cristina Paulino Leite
• Tec Enf Vânia Levino
• Tec Tais Pacheco
• Tec Daniele Almeida
Daniela Ponce
BOTUCATU SCHOOL OF MEDICINE, SAO PAULO STATE, BRAZIL