Embed Size (px)
Citation preview

JOBNAME: No Job Name PAGE: 1 SESS: 17 OUTPUT: Tue Jun 8 20:09:19 2010 SUM: 81DB65EE/v2503/blackwell/journals/jasp_v40_i8/jasp_653
Perfectionistic Self-Presentation and Trait Perfectionism inSocial Problem-Solving Ability and Depressive Symptoms1
Avi Besser2
Department of Behavioral SciencesCenter for Research in Personality, Life
Transitions, and Stressful Life EventsSapir Academic College, Israel
Gordon L. FlettYork University
Toronto, Ontario, Canada
Paul L. HewittUniversity of British Columbia
Vancouver, British Columbia, Canada
This study examined social problem solving and perfectionistic self-presentation,and assessed whether social problem solving mediates the association between per-fectionism and depression. A sample of 200 community members completed mea-sures of perfectionistic self-presentation, trait perfectionism, social problem-solvingability, and depression. Correlational analyses confirmed that perfectionistic self-presentation and socially prescribed perfectionism are both associated with a nega-tive problem-solving orientation. Tests of mediating effects revealed that negativeproblem-solving ability mediates the associations of socially prescribed perfection-ism and perfectionistic self-presentation with depressive symptoms, particularlyamong women. The findings support further exploration of mediational modelslinking perfectionism, problem-solving ability, and depression and suggest thatpeople who display high perfectionistic self-presentation are particularly vulnerableto stress and distress and should benefit from problem-solving training.jasp_653 2123..2157
Over the past 30 years, there has been sustained and growing interest inthe study of individual differences in the ability to solve personal problems(see Heppner, Witty, & Dixon, 2004). In part, this interest reflects the resultsof several studies that have found that social problem-solving ability is aconsistent correlate of positive mental health (D’Zurilla, 1986; Heppner,1978; Nezu, 1987). In addition, the general importance of problem solving toproblems in living is widely acknowledged. Most individuals are frequentlyfaced with a number of environmental circumstances that require effective
1Gordon Flett was supported by the Canada Research Chair Program. The authorsacknowledge Einat Biton and Natali Lev of Sapir Academic College for their invaluableassistance with data collection.
2Correspondence concerning this article should be addressed to Avi Besser, Department ofBehavioral Sciences, Sapir Academic College, D. N. Hof Ashkelon, 79165 Israel. E-mail:[email protected]
2123
Journal of Applied Social Psychology, 2010, 40, 8, pp. 2123–2156.© 2010 Copyright the AuthorsJournal compilation © 2010 Wiley Periodicals, Inc.
1
2
3
4
5
6
7
89
10
11
12
13
14151617181920212223242526
27
28
29
30
31
32
33
34
35
36
373839404142
JOBNAME: No Job Name PAGE: 2 SESS: 17 OUTPUT: Tue Jun 8 20:09:19 2010 SUM: 4D08EACA/v2503/blackwell/journals/jasp_v40_i8/jasp_653
responses (D’Zurilla & Goldfried, 1971; Spivack, Platt, & Shure, 1976), andineffective problem-solving responses in these situations may seriouslyimpair a person’s ability to cope with his or her environment and may leadto severe emotional distress (Butler & Meichenbaum, 1981; D’Zurilla &Goldfried, 1971).
The current paper examines the association between perfectionism andsocial problem-solving ability. One theme found in the literature on the topicof problem solving is that personality factors such as perfectionism may serveas antecedents of a negative problem-solving orientation. For instance,research has explored the link between problem-solving appraisals and TypeA behavior (Heppner, Kampa, & Brunning, 1987), and a negative problem-solving orientation has been linked with several personality factors, includingan external locus of control (Heppner & Petersen, 1982; Nezu, 1985), sociot-ropy (Haaga, Fine, Terrill, Stewart, & Beck, 1995), and a depressive attribu-tional style (Heppner, Baumgardner, & Jackson, 1985; Spence, Sheffield, &Donovan, 2002).
Attempts to examine perfectionism and problem-solving ability are com-plicated at both the conceptual and empirical levels because perfectionism isa multidimensional construct. For example, Frost and associates developed ameasure entitled the Multidimensional Perfectionism Scale (see Frost &Marten, 1990; Frost, Marten, Lahart, & Rosenblate, 1990). This scale con-sists of six subscales that measure personal aspects of perfectionism (i.e.,personal standards, concern for mistakes, doubts about actions, organiza-tion) and the familial aspects of perfectionism (i.e., high parental expecta-tions, parental criticism). Frost and associates (DiBartolo, Frost, Chang,LaSota, & Grills, 2004; Frost, Heimberg, Holt, Mattia, & Neubauer, 1993;Frost et al., 1990) have shown that the concern-for-mistakes subscale is theperfectionism dimension that is linked most consistently with depressivesymptoms.
Similarly, Hewitt and Flett (1991b, 2004) developed another measure ofperfectionism that is also called the Multidimensional Perfectionism Scale(MPS). This scale measures three dimensions of perfectionism—self-orientedperfectionism, other-oriented perfectionism, and socially prescribed perfec-tionism. Whereas self-oriented perfectionism entails a relentless striving forpersonal standards of perfection, other-oriented perfectionism involves afocus on the capabilities of others. As such, other-oriented perfectionism isassociated with hostility and extrapunitive tendencies toward others, ratherthan negative self-judgments (Hewitt & Flett, 1991b).
The third dimension of perfectionism—socially prescribedperfectionism—is the aspect of perfectionism that is most consistently relatedto maladjustment. Socially prescribed perfectionism entails the belief thatothers have high expectations and perfectionistic motives for one’s own
2124 BESSER ET AL.
1
2
3
4
5
6
7
8
9
10
11
12
13
14
15
16
17
18
19
20
21
22
23
24
25
26
27
28
29
30
31
32
33
34
35
36
37
38
39
40
41
42
JOBNAME: No Job Name PAGE: 3 SESS: 17 OUTPUT: Tue Jun 8 20:09:19 2010 SUM: 4AAFC1AF/v2503/blackwell/journals/jasp_v40_i8/jasp_653
behavior, as well as the belief that others will be satisfied only when thesestandards are attained. Socially prescribed perfectionism is associated with awide variety of psychological problems, including depression, anxiety, stress,suicidal tendencies, and personality disorders (Dean & Range, 1996; Dean,Range, & Goggin, 1996; Flett, Besser, & Hewitt, 2005; Frost et al., 1993;Hewitt & Flett, 1991a, 1991b, 1993; Hewitt, Flett, & Endler, 1995; Sherry,Hewitt, Flett, & Harvey, 2003).
Perfectionism and Social Problem-Solving Ability
Flett, Hewitt, Blankstein, Solnik, and Van Brunschot (1996) introducedthe idea that perfectionists may suffer from deficits in social problem solvingbecause they are highly defensive and believe that problems must be perfectlyresolved. These researchers conducted initial empirical investigations ofdimensions of perfectionism and problem-solving ability. Their first studyexamined associations between the MPS (Hewitt & Flett, 1991b) and theoriginal version of the Social Problem-Solving Inventory (SPSI; seeD’Zurilla & Nezu, 1990).
The SPSI provides two general measures of problem-solving orientationand specific problem-solving skills. The problem-solving orientation scaleconsists of three subscales measuring orientation in terms of cognitive, emo-tional, and behavioral responses. The problem-solving skill subscale consistsof four subscales measuring phases of the problem-solving process, includingproblem definition, the generation of alternative solutions, decision making,and solution implementation. The main hypothesis guiding this initialresearch was that socially prescribed perfectionism includes elements of help-lessness and hopelessness that are antithetical to the problem-solving process,and this ought to contribute to a negative problem-solving orientation.
In their first study, Flett et al. (1996) analyzed data from 168 under-graduate students and found that socially prescribed perfectionism was theonly perfectionism trait dimension that was significantly associated withindexes of negative problem orientation (rs ranging from -.34 to -.39). Inaddition, both self-oriented perfectionism and other-oriented perfectionismwere associated with positive appraisals of overall problem-solving ability.
In their second study, Flett et al. (1996) re-examined the link between traitdimensions of perfectionism and scores on the SPSI in a sample of 114university students. Participants also completed measures of anxiety anddepression. Once again, socially prescribed perfectionism was found to beassociated with the negative problem-solving orientation subscales (rsranging from -.26 to -.32). As for problem-solving skills, other-orientedperfectionism, but not self-oriented perfectionism, was associated with more
PERFECTIONISM AND SOCIAL PROBLEM-SOLVING ABILITY 2125
1
2
3
4
5
6
7
8
91011
12
13
14
15
16
17
18
19
20
21
22
23
24
25
26
27
28
29
30
31
32
33
34
35
36
37
38
39
40
41
JOBNAME: No Job Name PAGE: 4 SESS: 17 OUTPUT: Tue Jun 8 20:09:19 2010 SUM: 4EBB7067/v2503/blackwell/journals/jasp_v40_i8/jasp_653
positive appraisals of problem-solving skills. Partial correlational analysesinvolving the measures of anxiety and depression showed that the linkbetween socially prescribed perfectionism and negative problem-solving ori-entation could still be detected after controlling for the link between negativeproblem-solving orientation and psychological distress.
As part of the discussion of their findings, Flett et al. (1996) suggested theneed for future studies to examine whether social problem-solving abilitycontributes to the association between perfectionism and psychologicaldistress. They suggested that perfectionists with poor problem-solvingorientations would be especially susceptible to distress because they wouldexperience high levels of prolonged stress. The possibility that poor problemsolving underscores the link between perfectionism and elevated levels ofdistress is in keeping with observations (e.g., Nezu & Ronan, 1988) thatproblem solving functions as part of a complex process, alongside othervariables. The roles of coping and problem-solving variables as mediators ormoderators of the link between perfectionism and psychological distress wereincorporated into a theoretical model of perfectionism, stress, and copingthat was described by Hewitt and Flett (2002).
Subsequent research by Chang (1998) addressed the link between perfec-tionism and social problem solving as part of a broader study of predictors ofsuicide risk in Caucasian and Asian American college students. A sample of148 participants completed the SPSI–Revised (D’Zurilla, Nezu, & Maydeu-Olivares, 1996) and Frost et al.’s (1990) MPS. This revised problem-solvingmeasure assesses negative problem-solving orientation, positive problem-solving orientation, rational problem solving, an impulsive/careless problem-solving style, and an avoidance style. They found that the high personalstandards factor was not significantly associated with the problem-solvingmeasures. However, measures of concern for mistakes, parental criticism,and doubts about action were positively associated with a negative problem-solving orientation, with the caveat that some correlations did not attainsignificance because of a stringent Bonferroni correction.
A more recent investigation by Chang (2002) evaluated an integrativemodel in which both perfectionism and social problem solving were hypoth-esized to have additive and interactive effects in predicting depression andsuicide ideation. A sample of 385 university students in the midwesternUnited States completed Frost et al.’s (1990) MPS and the short form of theSPSI–Revised, as well as measures of depression and suicide ideation. Analy-ses focused on total scores on the social problem-solving measure and onFrost et al.’s MPS. Thus, the results were not presented for the separateperfectionism dimensions. A small, negative association between perfection-ism and problem-solving ability was reported (r = -.13, p < .05). Chang alsofound that perfectionism and problem-solving ability did, indeed, interact to
2126 BESSER ET AL.
1
2
3
4
5
6
7
8
9
10
11
12
13
14
15
16
17
18
19
20
21
22
23
24
25
26
27
28
29
30
31
32
33
34
35
36
37
38
39
40
41
42
JOBNAME: No Job Name PAGE: 5 SESS: 17 OUTPUT: Tue Jun 8 20:09:19 2010 SUM: 46582091/v2503/blackwell/journals/jasp_v40_i8/jasp_653
predict significant unique variance in both depression and suicide ideation.As expected, students jointly characterized by elevated perfectionism andlower problem-solving ability had elevated levels of depression and suicideideation.
Cheng (2001) examined perfectionism and problem-solving ability in asample of 138 university students from Hong Kong. Participants completeda brief 11-item perfectionism measure comprised of items from Frost et al.’s(1990) subscales assessing concern over mistakes and doubts about actions.They also completed Heppner and Petersen’s (1982) Problem-Solving Inven-tory, and measures of hopelessness and depression. Cheng reported a signifi-cant link between perfectionism and perceived deficits in problem solving(r = .30).
Finally, in a more recent investigation, Argus and Thompson (2008)examined associations among perfectionism, social problem-solving ability,perceived mindfulness, and depression in a clinical sample. This study foundlittle evidence of any link between perfectionistic self-standards and socialproblem-solving ability, but it did find that perceived deficits in socialproblem-solving ability were associated with perceived discrepancies betweenperfectionistic standards and the attainment of these standards. Other resultsof this study confirmed a link between depression and negative perceptions ofsocial problem-solving ability. Extensive research has attested to the roleof negative problem-solving orientations in depression (see Nezu, Nezu, &Clark, 2008). Nezu et al.’s recent review of this literature led Argus andThompson (2008) to conclude that intervention focused on fostering a morepositive orientation toward problem solving is an important way of reducinglevels of depression and vulnerability to subsequent bouts of depression.
The Present Study
To our knowledge, further tests of the association between perfectionismand social problem-solving ability have not been reported. The current studyis designed to extend existing research in several ways. First, we seek tore-examine the association between trait perfectionism and social problem-solving ability in a community sample of Israeli adults. Perfectionism wasassessed using Hewitt and Flett’s (1991b) MPS. Flett et al.’s (1996) studiesare the only ones thus far to use this particular perfectionism measure inconjunction with a social problem-solving measure, and that research wasconducted with university students in Canada.
Our interest in re-examining the link between social problem solving andlevels of self-oriented, other-oriented, and socially prescribed perfectionismstem, in part, from certain inconsistencies in the findings of the two studies
PERFECTIONISM AND SOCIAL PROBLEM-SOLVING ABILITY 2127
1
2
3
4
5
6
7
8
9
10
11
12
13
14
15
16
17
18
19
20
21
22
23
24
25
26
27
282930
31
32
33
34
35
36
37
38
39
40
41
JOBNAME: No Job Name PAGE: 6 SESS: 17 OUTPUT: Tue Jun 8 20:09:19 2010 SUM: 5335A054/v2503/blackwell/journals/jasp_v40_i8/jasp_653
described by Flett et al. (1996). Specifically, self-oriented perfectionism wassignificantly associated with positive appraisals of problem-solving skills intheir first study, but not in their second study. It is important to re-examinethis issue in light of the growing controversy about the extent to whichself-oriented perfectionism has an adaptive aspect (see Bieling, Israeli,Smith, & Antony, 2003).
Another unique feature of the current study is its focus on a relativelynew aspect of the perfectionism construct known as perfectionistic self-presentation (see Hewitt et al., 2003). Perfectionistic self-presentation isbased on the premise that certain perfectionists are highly invested in cover-ing up their mistakes and are preoccupied with trying to present themselvesas perfect (i.e., self-promotion) or defensively minimizing the number ofmistakes that are on display for others to see. Hewitt et al. hypothesized thatthere are stable individual differences in the tendency to engage in perfec-tionistic self-presentation. The Perfectionistic Self-Presentation Scale (PSPS;Hewitt et al., 2003) was developed to assess three aspects of perfectionisticself-presentation; namely, perfectionistic self-promotion, unwillingness todisplay imperfections, and unwillingness to disclose imperfections to others.This third dimension would involve avoidance of personal communicationabout issues that could reveal the perfectionist’s flaws.
Initial research has indicated that perfectionistic self-presentation is,indeed, a multidimensional construct (Hewitt et al., 2003). Although perfec-tionistic self-presentation is significantly correlated with trait perfectionism,a perfectionistic self-presentational style predicts unique variance in psy-chological distress after taking into account the variance attributable toperfectionism, as assessed by the respective MPSs. That is, perfectionisticself-presentation predicts unique variance over and above the variance attrib-utable to maladaptive trait dimensions of perfectionism, such as sociallyprescribed perfectionism (see Hewitt et al., 2003; Sherry, Hewitt, Flett, Lee-Baggley, & Hall, 2007). This outcome follows, given that not all individualswho feel a great pressure from imposed expectations will respond necessarilyby trying to seem perfect when in public.
Other research with the PSPS (Hewitt et al., 2003) has indicated thatperfectionistic self-presentation is associated with low levels of appearanceself-esteem (Hewitt, Flett, & Ediger, 1995), personality dysfunction (Sherryet al., 2007), self-conscious anxiety among students in dating relationshipsand relationship difficulties in married couples (Flett, Hewitt, Shapiro, &Rayman, 2000–2001; Habke, Hewitt, & Flett, 1999), and tendencies towardself-silencing and reduced emotional expressiveness (Geller, Cockell, Hewitt,Goldner, & Flett, 2000). Patients with eating disorders are also characterizedby highly perfectionistic self-presentations (Cockell et al., 2002). Elevationsin perfectionistic self-presentation are correlated with facets of the anxiety
2128 BESSER ET AL.
1
2
3
4
5
6
7
8
9
10
11
12
13
14
15
16
17
18
19
20
21
22
23
24
25
26
27
28
29
30
31
32
33
34
35
36
37
38
39
40
41
42
JOBNAME: No Job Name PAGE: 7 SESS: 17 OUTPUT: Tue Jun 8 20:09:19 2010 SUM: 4C002140/v2503/blackwell/journals/jasp_v40_i8/jasp_653
sensitivity construct, including a fear of expressing publicly observable symp-toms of anxiety (Flett, Greene, & Hewitt, 2004).
Although the association between perfectionistic self-presentation andperceived problem-solving ability has not been investigated in previousresearch, perfectionistic self-presentation should be associated with a nega-tive problem-solving orientation for many reasons. Problem-solving orienta-tion was defined by Nezu, Nezu, and Lombardo (2004) as “a set of relativelystable cognitive-affective schemas that represent a person’s generalizedbeliefs, attitudes, and emotional reactions about problems in living and one’sability to successfully cope with such problems” (p. 277).
By definition, people who are highly perfectionistic in their self-presentation are characterized as highly neurotic and defensive individualswho feel that they must overcompensate for deficits in their own selves byportraying a false image and trying to appear as perfect as possible. Hewittet al. (2003) suggested that perfectionistic self-presentation is a highly neu-rotic style that is a way of overcompensating for feelings of inferiority. Thissuggestion is consistent with the views outlined by classic theorists, such asAdler (1956) and Horney (1950). A possible link between perfectionisticself-presentation and deficits in problem solving can be extrapolated fromHorney’s (1945) seminal analysis of inner conflict. Horney (1945) described aneurotic style of individuals with a profound fear of disclosure and of beingidentified as frauds, who engage in bluffing and pretense as a projection of anideal self. She suggested that this neurotic style and associated fear of disclo-sure are not conducive to “constructive work” (p. 45) and would work inopposition to behaviors (including problem solving) that could result inexposure and public humiliation if efforts prove to be unsuccessful.
Given that perfectionistic self-presentation has been empirically linkedwith diminished self-esteem (Hewitt, Flett, & Ediger, 1995), as well as the factthat perfectionistic self-presentation is a highly neurotic orientation andneuroticism is linked with negative appraisals of problem-solving ability(Elliott, Herrick, MacNair, & Harkins, 1994), it follows that perfectionisticself-presentation is most likely associated with negative problem-solvingappraisals. This defensiveness may also be reflected in a negative orientationtoward personal problems, because the existence of these problems andacknowledgment of these problems would only serve to highlight imperfec-tions in the self, perhaps in ways that make these personal imperfectionsmore visible to significant others.
Another unique aspect of the current investigation is that our sampleincluded enough men and women to conduct meaningful tests of possiblegender differences. In general, gender differences have seldom been testedin the perfectionism literature (for a related discussion, see Blankstein,Lumley, & Crawford, 2007). In the current instance, it is quite conceivable
PERFECTIONISM AND SOCIAL PROBLEM-SOLVING ABILITY 2129
1
2
3
4
5
6
7
8
9
10
11
12
13
14
15
16
17
18
19
20
21
22
23
24
25
26
27
28
29
30
31
32
33
34
35
36
37
38
39
40
41
42
JOBNAME: No Job Name PAGE: 8 SESS: 17 OUTPUT: Tue Jun 8 20:09:19 2010 SUM: 4CE3E5D7/v2503/blackwell/journals/jasp_v40_i8/jasp_653
that there are gender differences in the importance and relevance of perfec-tionistic self-presentation.
Previous research on perfectionistic self-presentation, including theoriginal research performed by Hewitt et al. (2003), has not systematicallyevaluated gender differences. This lack of any systematic focus on genderdifferences is unfortunate, given that issues related to presentation of self,image construction, and appearance are seemingly more relevant for females(see Pliner, Chaiken, & Flett, 1990), and it has been observed that thereare clear differences in self-presentational norms for females and males(see Leary, 1996). In addition, there is some evidence suggesting thatself-presentation varies in significance for adolescent girls, as compared toadolescent boys (see Elliott, 1982).
Although this issue has not been tested often, those few studies in whichgender differences have been explored have yielded evidence that perfection-istic self-presentation may have different nomological networks in men andwomen. For instance, Habke et al. (1999) found that perfectionistic self-presentation is associated with self-reports of diminished dyadic adjustmentamong women, but not among their male partners. Similarly, Sherry, Hewitt,Lee-Baggley, Flett, and Besser (2004) reported that perfectionistic self-presentation is significantly correlated with thoughts about cosmetic surgeryamong university women, but not among university men. This clearly illus-trates the need to incorporate a focus on possible gender differences.
A central goal of the current study is to test a mediation model that linksperfectionism, social problem-solving ability, and depression. Given thatnegative perceptions of social problem-solving ability are consistently linkedwith depression (see Nezu et al., 2008), it follows that personality variableslinked consistently with depression (e.g., socially prescribed perfectionism orSPP) may be associated with distress, in part, because of deficits in socialproblem-solving ability and related processes (e.g., cognitive-emotional regu-lation strategies; see Rudolph, Flett, & Hewitt, 2007).
A main hypothesis guiding our study is that perfectionism is associatedwith negative appraisals of social problem-solving ability and that thesenegative appraisals of problem-solving ability mediate the link between per-fectionism and depressive symptoms. This hypothesis is extrapolated fromother research showing that maladaptive coping styles, in general, mediatethe link between maladaptive dimensions of perfectionism and psychologi-cal distress (e.g., Dunkley, Blankstein, Halsall, Williams, & Winkworth,2000; Dunkley, Zuroff, & Blankstein, 2003; O’Connor & O’Connor, 2003)and related research suggesting that negative self-appraisals mediate thelink between perfectionism and depression (Rice, Ashby, & Slaney, 1998).According to the theoretical suggestions outlined by Hewitt and Flett(2002), perfectionism is associated with distress, in part, because certain
2130 BESSER ET AL.
1
2
3
4
5
6
7
8
9
10
11
12
13
14
15
16
17
18
19
20
21
22
23
24
25
26
27
28
29
30
31
32
33
34
35
36
37
38
39
40
41
42
JOBNAME: No Job Name PAGE: 9 SESS: 17 OUTPUT: Tue Jun 8 20:09:19 2010 SUM: 40BF8D58/v2503/blackwell/journals/jasp_v40_i8/jasp_653
perfectionists respond to stress with maladaptive coping and problem-solving tendencies that perpetuate and exacerbate negative affect andrelated symptoms of distress.
Method
Participants
Our sample consisted of 200 Israeli community sample participants (100men, 100 women). They responded to our call for volunteers to take part ina study of “attitudes, attributions, and mood.” Participants were a commu-nity sample of young adults in their mid-20s (M = 24.2 years, SD = 2.8). Allparticipants had more than 12 years of formal education (M = 12.4 years,SD = 0.9).
Measures
Multidimensional Perfectionism Scale (MPS). The MPS (Hewitt & Flett,1991b, 2004) has three subscales of 15 items each. Respondents rated state-ments reflecting self-oriented perfectionism (e.g., “One of my goals is to beperfect in every thing I do”), other-oriented perfectionism (e.g., “I have highexpectations for the people who are important to me”), and socially pre-scribed perfectionism (e.g., “My family expects me to be perfect”) on a7-point scale. Extensive evidence has confirmed the multidimensionality ofthis instrument, as well as the reliability and validity of the subscales (Flett,Sawatzky, & Hewitt, 1995; Frost et al., 1993; Hewitt & Flett, 1991b, 2004;Hewitt, Flett, Turnbull-Donovan, & Mikail, 1991).
Perfectionistic Self-Presentation Scale (PSPS; Hewitt et al., 2003). ThePSPS is a 27-item multidimensional scale that assesses an individual’s needto appear perfect to others (Hewitt et al., 2003). The PSPS has three sub-scales that assess perfectionistic self-promotion (i.e., need to appear perfectto others; e.g., “I strive to look perfect to others”), nondisplay of imper-fection (i.e., need to avoid appearing imperfect to others; e.g., “I do notcare about making mistakes in public,” reverse-scored), and nondisclosureof imperfection (i.e., need to avoid disclosing imperfections to others; e.g.,“Admitting failure to others is the worst possible thing”). Extensiveresearch has attested to the reliability and validity of the PSPS (Hewittet al., 2003).
Perfectionistic self-presentation has been linked with other relevant con-structs, such as public self-consciousness, fear of negative evaluation, and a
PERFECTIONISM AND SOCIAL PROBLEM-SOLVING ABILITY 2131
1
2
3
4
567
8
9
10
11
12
13
14
15
16
17
18
19
20
21
22
23
24
25
26
27
28
29
30
31
32
33
34
35
36
37
38
39
40
JOBNAME: No Job Name PAGE: 10 SESS: 17 OUTPUT: Tue Jun 8 20:09:19 2010 SUM: 4F39A493/v2503/blackwell/journals/jasp_v40_i8/jasp_653
sense of impostorism (Ferrari & Thompson, 2006; Hewitt et al., 2003). It hasalso been associated significantly with self-concealment, as might beexpected, but not to the degree that perfectionistic self-presentation andself-concealment are redundant with each other (see Hewitt et al., 2003).
Research has indicated that the three PSPS factors have adequate levels ofinternal consistency and are significantly correlated with the MPS factors,but the PSPS factors account for a significant degree of unique variance inmeasures of self-esteem (Hewitt et al., 1995). The authors also reported thatthe three PSPS factors had high levels of test–retest reliability over a 2-monthperiod, with test–retest correlations ranging from .74 to .84.
Social Problem-Solving Inventory (SPSI; D’Zurilla & Nezu, 1990;D’Zurilla et al., 1996). The SPSI is a 70-item, multidimensional measure ofself-perceived problem-solving ability. The SPSI was selected for use in thisstudy, instead of briefer measures, to facilitate comparisons of the currentresults with those reported by Flett et al. (1996).
The SPSI is comprised of two major scales, referred to as the ProblemOrientation Scale (POS) and the Problem-Solving Skills Scale (PSSS). ThePOS consists of three subscales measuring cognitive orientation (e.g., “WhenI am faced with a difficult problem, I usually believe that I will be able tosolve the problem on my own if I try hard enough”), emotion orientation(e.g., “I am generally able to remain ‘cool, calm, and collected’ when I amsolving problems”), and behavior orientation (e.g., “I usually confront myproblems ‘head on,’ instead of trying to avoid them”).
The PSSS consists of four subscales measuring problem definition andformulation (e.g., “When I am faced with a large, complex problem, I oftentry to break it down into smaller problems that I can solve one at a time”),generation of alternative solutions (e.g., “When I am attempting to solve aproblem, I often try to be creative and think of original or unconventionalsolutions”), decision making (e.g., “When making decisions, I generally use asystematic method for judging and comparing alternatives”), and solutionimplementation and verification (e.g., “After carrying out a solution to aproblem, I usually try to analyze what went right and what went wrong”).The POS and the PSSS can also be combined to provide a summary score forthe entire SPSI.
Although the SPSI is a relatively new instrument, initial evidence hasattested to the validity and reliability of the measure as a whole, as well asthat of its subscales (see D’Zurilla & Nezu, 1990). For instance, the 3-weektest–retest reliabilities for the POS, PSSS, and SPSI were .87 or greater, andthe alpha coefficients were .92 or greater.
Center for Epidemiological Studies Depression Scale (CES-D; Radloff,1977). The CES-D is a well-known 20-item inventory with items thatmeasure the affective and somatic symptoms of depression. Scores range
2132 BESSER ET AL.
1
2
3
4
5
6
7
8
9
10
11
12
13
14
15
16
17
18
19
20
21
22
23
24
25
26
27
28
29
30
31
32
33
34
35
36
37
38
39
40
41
42
JOBNAME: No Job Name PAGE: 11 SESS: 17 OUTPUT: Tue Jun 8 20:09:19 2010 SUM: 3E326F27/v2503/blackwell/journals/jasp_v40_i8/jasp_653
from 0 to 60, with higher scores indicating more severe depression. Althoughthe scale is typically used as a continuous measure, a score of 16 or higher isregarded as the clinical cutoff for at least a mild case of depression (Radloff,1977). The CES-D is well suited for administration to adults from the generalpopulation. Respondents indicate the frequency with which they have expe-rienced each symptom over the past week on a 4-point scale ranging from0 to 3.
The CES-D has acceptable levels of internal consistency and convergentvalidity. Extensive evidence from a variety of samples attests to the psy-chometric properties of the CES-D (see Eaton, Muntaner, Smith, Tien, &Ybarra, 2004).
Procedure
Participants were initially contacted through advertisements in publicplaces asking for volunteers to take part in a study on “attitudes, attributions,and mood.” Participants were young Israeli adults who were from the area insouthern Israel in which they were recruited. Participants completed thequestionnaire package individually. The order of presentation of the ques-tionnaires was randomized.
Results
Descriptive Analyses
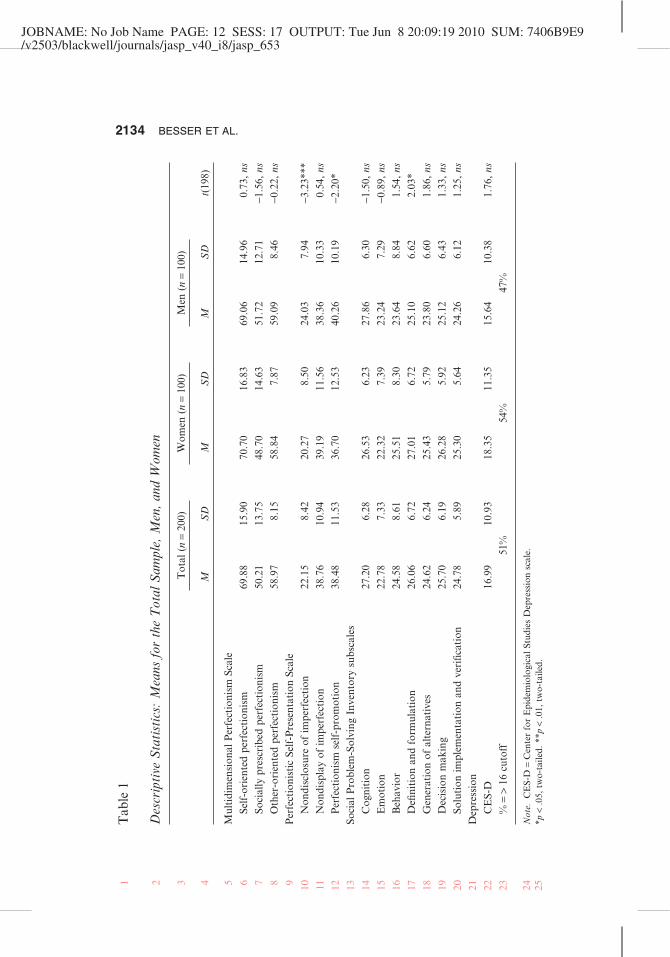
Means and standard deviations for each of the measures for men,women, and the total sample are shown in Table 1. The data presented inTable 1 represent some normative information for the use of these mea-sures in Israel, since measures such as the PSPS have not been studiedextensively thus far.
As shown in Table 1, there were no significant differences in mean scoreson the MPS (Hewitt & Flett, 1991b, 2004). In contrast, men had significantlyhigher scores on the PSPS (Hewitt et al., 2003) subscales assessing perfec-tionistic self-promotion and the need to avoid disclosing imperfections. Therewas only one significant gender difference in mean scores on the SPSI(D’Zurilla & Nezu, 1990), and there was no significant gender difference inmean scores on the CES-D (Radloff, 1977) scale. Note that the total sampleCES-D mean of 16.99 exceeds the threshold of 16 that is used as a cutoff formild depression.
PERFECTIONISM AND SOCIAL PROBLEM-SOLVING ABILITY 2133
1
2
3
4
5
6
7
8
9
10
11
12
13
14
15
16
17
18
19
20
21
222324
25
26
27
28
29
30
31
32
33
34
35
36
37
38
39
JOBNAME: No Job Name PAGE: 12 SESS: 17 OUTPUT: Tue Jun 8 20:09:19 2010 SUM: 7406B9E9/v2503/blackwell/journals/jasp_v40_i8/jasp_653
Tab
le1
Des
crip
tive
Sta
tist
ics:
Mea
nsfo
rth
eT
otal
Sam
ple,
Men
,and
Wom
en
Tot
al(n
=20
0)W
omen
(n=
100)
Men
(n=
100)
t(19
8)M
SD
MS
DM
SD
Mul
tidi
men
sion
alP
erfe
ctio
nism
Scal
eSe
lf-o
rien
ted
perf
ecti
onis
m69
.88
15.9
070
.70
16.8
369
.06
14.9
60.
73,
nsSo
cial
lypr
escr
ibed
perf
ecti
onis
m50
.21
13.7
548
.70
14.6
351
.72
12.7
1-1
.56,
nsO
ther
-ori
ente
dpe
rfec
tion
ism
58.9
78.
1558
.84
7.87
59.0
98.
46-0
.22,
nsP
erfe
ctio
nist
icSe
lf-P
rese
ntat
ion
Scal
eN
ondi
sclo
sure
ofim
perf
ecti
on22
.15
8.42
20.2
78.
5024
.03
7.94
-3.2
3***
Non
disp
lay
ofim
perf
ecti
on38
.76
10.9
439
.19
11.5
638
.36
10.3
30.
54,
nsP
erfe
ctio
nism
self
-pro
mot
ion
38.4
811
.53
36.7
012
.53
40.2
610
.19
-2.2
0*So
cial
Pro
blem
-Sol
ving
Inve
ntor
ysu
bsca
les
Cog
niti
on27
.20
6.28
26.5
36.
2327
.86
6.30
-1.5
0,ns
Em
otio
n22
.78
7.33
22.3
27.
3923
.24
7.29
-0.8
9,ns
Beh
avio
r24
.58
8.61
25.5
18.
3023
.64
8.84
1.54
,ns
Defi
niti
onan
dfo
rmul
atio
n26
.06
6.72
27.0
16.
7225
.10
6.62
2.03
*G
ener
atio
nof
alte
rnat
ives
24.6
26.
2425
.43
5.79
23.8
06.
601.
86,
nsD
ecis
ion
mak
ing
25.7
06.
1926
.28
5.92
25.1
26.
431.
33,
nsSo
luti
onim
plem
enta
tion
and
veri
ficat
ion
24.7
85.
8925
.30
5.64
24.2
66.
121.
25,
nsD
epre
ssio
nC
ES-
D16
.99
10.9
318
.35
11.3
515
.64
10.3
81.
76,
ns%
=>
16cu
toff
51%
54%
47%
Not
e.C
ES-
D=
Cen
ter
for
Epi
dem
iolo
gica
lStu
dies
Dep
ress
ion
scal
e.*p
<.0
5,tw
o-ta
iled.
**p
<.0
1,tw
o-ta
iled.
2134 BESSER ET AL.1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 18 19 20 21 22 23 24 25
JOBNAME: No Job Name PAGE: 13 SESS: 17 OUTPUT: Tue Jun 8 20:09:19 2010 SUM: 52550594/v2503/blackwell/journals/jasp_v40_i8/jasp_653
Correlational Analyses
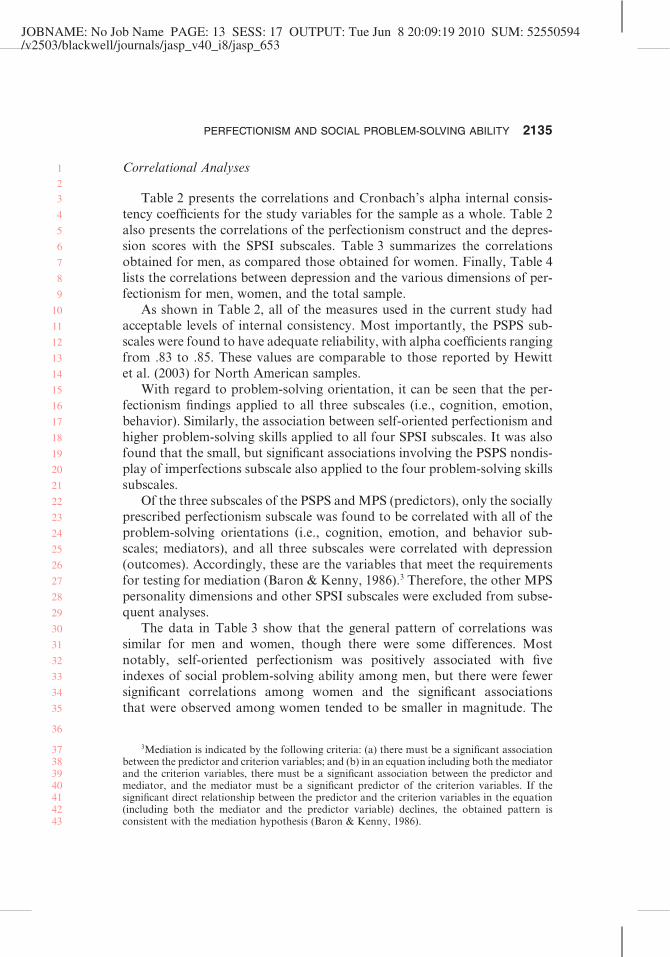
Table 2 presents the correlations and Cronbach’s alpha internal consis-tency coefficients for the study variables for the sample as a whole. Table 2also presents the correlations of the perfectionism construct and the depres-sion scores with the SPSI subscales. Table 3 summarizes the correlationsobtained for men, as compared those obtained for women. Finally, Table 4lists the correlations between depression and the various dimensions of per-fectionism for men, women, and the total sample.
As shown in Table 2, all of the measures used in the current study hadacceptable levels of internal consistency. Most importantly, the PSPS sub-scales were found to have adequate reliability, with alpha coefficients rangingfrom .83 to .85. These values are comparable to those reported by Hewittet al. (2003) for North American samples.
With regard to problem-solving orientation, it can be seen that the per-fectionism findings applied to all three subscales (i.e., cognition, emotion,behavior). Similarly, the association between self-oriented perfectionism andhigher problem-solving skills applied to all four SPSI subscales. It was alsofound that the small, but significant associations involving the PSPS nondis-play of imperfections subscale also applied to the four problem-solving skillssubscales.
Of the three subscales of the PSPS and MPS (predictors), only the sociallyprescribed perfectionism subscale was found to be correlated with all of theproblem-solving orientations (i.e., cognition, emotion, and behavior sub-scales; mediators), and all three subscales were correlated with depression(outcomes). Accordingly, these are the variables that meet the requirementsfor testing for mediation (Baron & Kenny, 1986).3 Therefore, the other MPSpersonality dimensions and other SPSI subscales were excluded from subse-quent analyses.
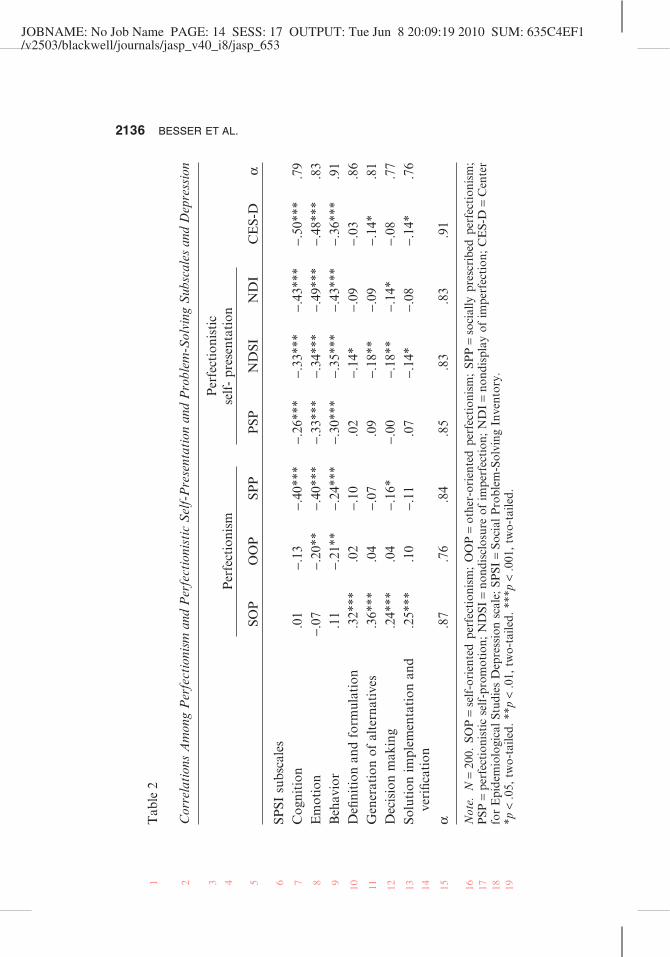
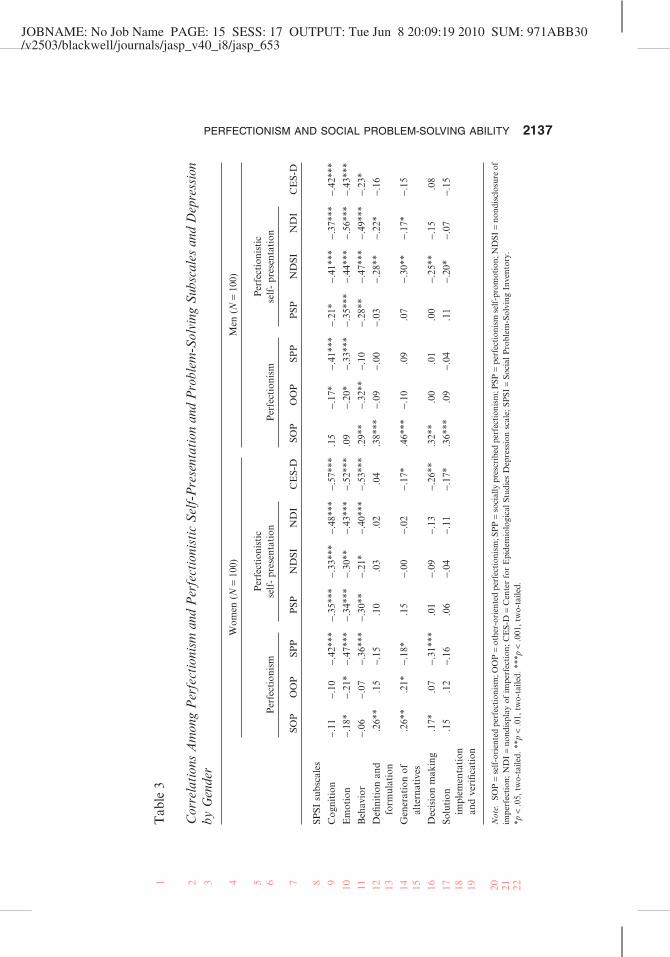
The data in Table 3 show that the general pattern of correlations wassimilar for men and women, though there were some differences. Mostnotably, self-oriented perfectionism was positively associated with fiveindexes of social problem-solving ability among men, but there were fewersignificant correlations among women and the significant associationsthat were observed among women tended to be smaller in magnitude. The
3Mediation is indicated by the following criteria: (a) there must be a significant associationbetween the predictor and criterion variables; and (b) in an equation including both the mediatorand the criterion variables, there must be a significant association between the predictor andmediator, and the mediator must be a significant predictor of the criterion variables. If thesignificant direct relationship between the predictor and the criterion variables in the equation(including both the mediator and the predictor variable) declines, the obtained pattern isconsistent with the mediation hypothesis (Baron & Kenny, 1986).
PERFECTIONISM AND SOCIAL PROBLEM-SOLVING ABILITY 2135
1
2
3
4
5
6
7
8
9
10
11
12
13
14
15
16
17
18
19
20
21
22
23
24
25
26
27
28
29
30
31
32
33
34
35
36
37383940414243
JOBNAME: No Job Name PAGE: 14 SESS: 17 OUTPUT: Tue Jun 8 20:09:19 2010 SUM: 635C4EF1/v2503/blackwell/journals/jasp_v40_i8/jasp_653
Tab
le2
Cor
rela
tion
sA
mon
gP
erfe
ctio
nism
and
Per
fect
ioni
stic
Sel
f-P
rese
ntat
ion
and
Pro
blem
-Sol
ving
Sub
scal
esan
dD
epre
ssio
n
Per
fect
ioni
smP
erfe
ctio
nist
icse
lf-
pres
enta
tion
CE
S-D
aSO
PO
OP
SPP
PSP
ND
SIN
DI
SPSI
subs
cale
sC
ogni
tion
.01
-.13
-.40
***
-.26
***
-.33
***
-.43
***
-.50
***
.79
Em
otio
n-.
07-.
20**
-.40
***
-.33
***
-.34
***
-.49
***
-.48
***
.83
Beh
avio
r.1
1-.
21**
-.24
***
-.30
***
-.35
***
-.43
***
-.36
***
.91
Defi
niti
onan
dfo
rmul
atio
n.3
2***
.02
-.10
.02
-.14
*-.
09-.
03.8
6G
ener
atio
nof
alte
rnat
ives
.36*
**.0
4-.
07.0
9-.
18**
-.09
-.14
*.8
1D
ecis
ion
mak
ing
.24*
**.0
4-.
16*
-.00
-.18
**-.
14*
-.08
.77
Solu
tion
impl
emen
tati
onan
dve
rific
atio
n.2
5***
.10
-.11
.07
-.14
*-.
08-.
14*
.76
a.8
7.7
6.8
4.8
5.8
3.8
3.9
1
Not
e.N
=20
0.SO
P=
self
-ori
ente
dpe
rfec
tion
ism
;O
OP
=ot
her-
orie
nted
perf
ecti
onis
m;
SPP
=so
cial
lypr
escr
ibed
perf
ecti
onis
m;
PSP
=pe
rfec
tion
isti
cse
lf-p
rom
otio
n;N
DSI
=no
ndis
clos
ure
ofim
perf
ecti
on;
ND
I=
nond
ispl
ayof
impe
rfec
tion
;C
ES-
D=
Cen
ter
for
Epi
dem
iolo
gica
lStu
dies
Dep
ress
ion
scal
e;SP
SI=
Soci
alP
robl
em-S
olvi
ngIn
vent
ory.
*p<
.05,
two-
taile
d.**
p<
.01,
two-
taile
d.**
*p<
.001
,tw
o-ta
iled.
2136 BESSER ET AL.
1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 18 19
JOBNAME: No Job Name PAGE: 15 SESS: 17 OUTPUT: Tue Jun 8 20:09:19 2010 SUM: 971ABB30/v2503/blackwell/journals/jasp_v40_i8/jasp_653
Tab
le3
Cor
rela
tion
sA
mon
gP
erfe
ctio
nism
and
Per
fect
ioni
stic
Sel
f-P
rese
ntat
ion
and
Pro
blem
-Sol
ving
Sub
scal
esan
dD
epre
ssio
nby
Gen
der
Wom
en(N
=10
0)M
en(N
=10
0)
Per
fect
ioni
smP
erfe
ctio
nist
icse
lf-
pres
enta
tion
CE
S-D
Per
fect
ioni
smP
erfe
ctio
nist
icse
lf-
pres
enta
tion
CE
S-D
SOP
OO
PSP
PP
SPN
DSI
ND
ISO
PO
OP
SPP
PSP
ND
SIN
DI
SPSI
subs
cale
s
Cog
niti
on-.
11-.
10-.
42**
*-.
35**
*-.
33**
*-.
48**
*-.
57**
*.1
5-.
17*
-.41
***
-.21
*-.
41**
*-.
37**
*-.
42**
*
Em
otio
n-.
18*
-.21
*-.
47**
*-.
34**
*-.
30**
-.43
***
-.52
***
.09
-.20
*-.
33**
*-.
35**
*-.
44**
*-.
56**
*-.
43**
*
Beh
avio
r-.
06-.
07-.
36**
*-.
30**
-.21
*-.
40**
*-.
53**
*.2
9**
-.32
**-.
10-.
28**
-.47
***
-.49
***
-.23
*
Defi
niti
onan
dfo
rmul
atio
n.2
6**
.15
-.15
.10
.03
.02
.04
.38*
**-.
09-.
00-.
03-.
28**
-.22
*-.
16
Gen
erat
ion
ofal
tern
ativ
es.2
6**
.21*
-.18
*.1
5-.
00-.
02-.
17*
.46*
**-.
10.0
9.0
7-.
30**
-.17
*-.
15
Dec
isio
nm
akin
g.1
7*.0
7-.
31**
*.0
1-.
09-.
13-.
26**
.32*
*.0
0.0
1.0
0-.
25**
-.15
.08
Solu
tion
impl
emen
tati
onan
dve
rific
atio
n
.15
.12
-.16
.06
-.04
-.11
-.17
*.3
6***
.09
-.04
.11
-.20
*-.
07-.
15
Not
e.SO
P=
self
-ori
ente
dpe
rfec
tion
ism
;OO
P=
othe
r-or
ient
edpe
rfec
tion
ism
;SP
P=
soci
ally
pres
crib
edpe
rfec
tion
ism
;PSP
=pe
rfec
tion
ism
self
-pro
mot
ion;
ND
SI=
nond
iscl
osur
eof
impe
rfec
tion
;ND
I=
nond
ispl
ayof
impe
rfec
tion
;CE
S-D
=C
ente
rfo
rE
pide
mio
logi
calS
tudi
esD
epre
ssio
nsc
ale;
SPSI
=So
cial
Pro
blem
-Sol
ving
Inve
ntor
y.*p
<.0
5,tw
o-ta
iled.
**p
<.0
1,tw
o-ta
iled.
***p
<.0
01,t
wo-
taile
d.
PERFECTIONISM AND SOCIAL PROBLEM-SOLVING ABILITY 2137
1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 18 19 20 21 22
JOBNAME: No Job Name PAGE: 16 SESS: 17 OUTPUT: Tue Jun 8 20:09:19 2010 SUM: 634E6E7D/v2503/blackwell/journals/jasp_v40_i8/jasp_653
significant negative correlations between perfectionistic self-presentation andsocial problem-solving ability tended to be stronger for women and certainassociations were only evident among women. For instance, the PSPS dimen-sion assessing the need to avoid displaying imperfection was associated withall four problem-solving skills subscales, but these associations were notsignificantly correlated among men. Similarly, depression was negativelyassociated with three of the problem-solving skills subscales among women,but not among men.
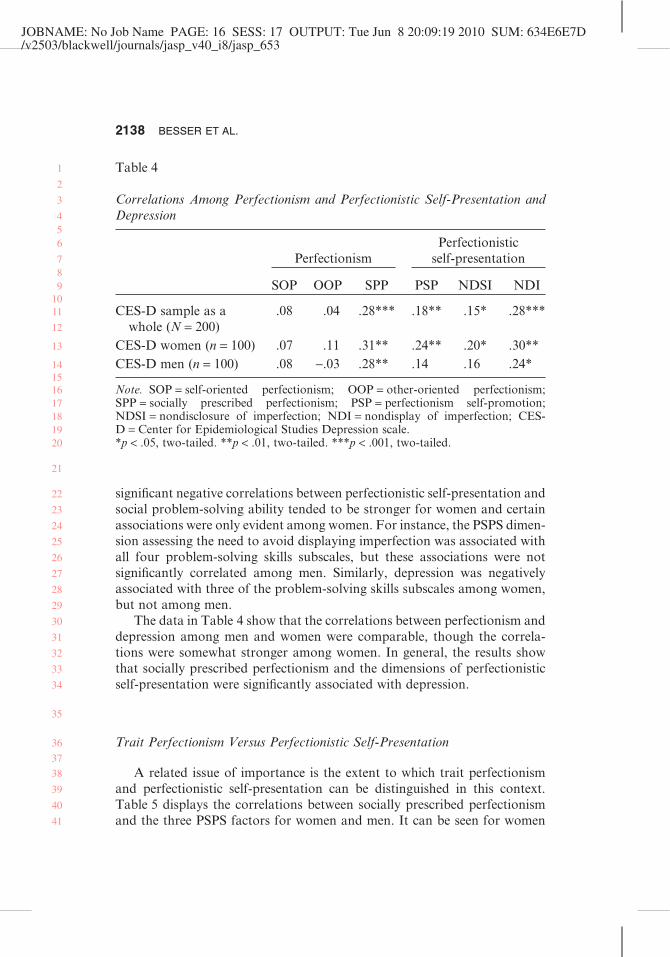
The data in Table 4 show that the correlations between perfectionism anddepression among men and women were comparable, though the correla-tions were somewhat stronger among women. In general, the results showthat socially prescribed perfectionism and the dimensions of perfectionisticself-presentation were significantly associated with depression.
Trait Perfectionism Versus Perfectionistic Self-Presentation
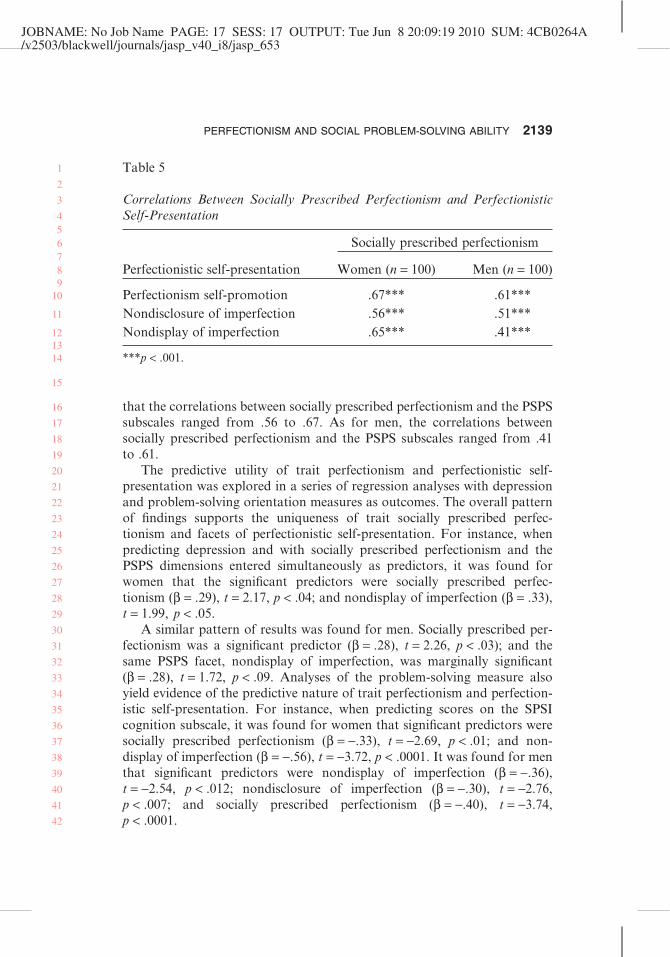
A related issue of importance is the extent to which trait perfectionismand perfectionistic self-presentation can be distinguished in this context.Table 5 displays the correlations between socially prescribed perfectionismand the three PSPS factors for women and men. It can be seen for women
Table 4
Correlations Among Perfectionism and Perfectionistic Self-Presentation andDepression
PerfectionismPerfectionistic
self-presentation
SOP OOP SPP PSP NDSI NDI
CES-D sample as awhole (N = 200)
.08 .04 .28*** .18** .15* .28***
CES-D women (n = 100) .07 .11 .31** .24** .20* .30**CES-D men (n = 100) .08 -.03 .28** .14 .16 .24*
Note. SOP = self-oriented perfectionism; OOP = other-oriented perfectionism;SPP = socially prescribed perfectionism; PSP = perfectionism self-promotion;NDSI = nondisclosure of imperfection; NDI = nondisplay of imperfection; CES-D = Center for Epidemiological Studies Depression scale.*p < .05, two-tailed. **p < .01, two-tailed. ***p < .001, two-tailed.
2138 BESSER ET AL.
1
2
3
456
789
1011
12
13
14151617181920
21
22
23
24
25
26
27
28
29
30
31
32
33
34
35
36
37
38
39
40
41
JOBNAME: No Job Name PAGE: 17 SESS: 17 OUTPUT: Tue Jun 8 20:09:19 2010 SUM: 4CB0264A/v2503/blackwell/journals/jasp_v40_i8/jasp_653
that the correlations between socially prescribed perfectionism and the PSPSsubscales ranged from .56 to .67. As for men, the correlations betweensocially prescribed perfectionism and the PSPS subscales ranged from .41to .61.
The predictive utility of trait perfectionism and perfectionistic self-presentation was explored in a series of regression analyses with depressionand problem-solving orientation measures as outcomes. The overall patternof findings supports the uniqueness of trait socially prescribed perfec-tionism and facets of perfectionistic self-presentation. For instance, whenpredicting depression and with socially prescribed perfectionism and thePSPS dimensions entered simultaneously as predictors, it was found forwomen that the significant predictors were socially prescribed perfec-tionism (b = .29), t = 2.17, p < .04; and nondisplay of imperfection (b = .33),t = 1.99, p < .05.
A similar pattern of results was found for men. Socially prescribed per-fectionism was a significant predictor (b = .28), t = 2.26, p < .03); and thesame PSPS facet, nondisplay of imperfection, was marginally significant(b = .28), t = 1.72, p < .09. Analyses of the problem-solving measure alsoyield evidence of the predictive nature of trait perfectionism and perfection-istic self-presentation. For instance, when predicting scores on the SPSIcognition subscale, it was found for women that significant predictors weresocially prescribed perfectionism (b = -.33), t = -2.69, p < .01; and non-display of imperfection (b = -.56), t = -3.72, p < .0001. It was found for menthat significant predictors were nondisplay of imperfection (b = -.36),t = -2.54, p < .012; nondisclosure of imperfection (b = -.30), t = -2.76,p < .007; and socially prescribed perfectionism (b = -.40), t = -3.74,p < .0001.
Table 5
Correlations Between Socially Prescribed Perfectionism and PerfectionisticSelf-Presentation
Perfectionistic self-presentation
Socially prescribed perfectionism
Women (n = 100) Men (n = 100)
Perfectionism self-promotion .67*** .61***Nondisclosure of imperfection .56*** .51***Nondisplay of imperfection .65*** .41***
***p < .001.
PERFECTIONISM AND SOCIAL PROBLEM-SOLVING ABILITY 2139
1
2
3
456789
10
11
121314
15
16
17
18
19
20
21
22
23
24
25
26
27
28
29
30
31
32
33
34
35
36
37
38
39
40
41
42
JOBNAME: No Job Name PAGE: 18 SESS: 17 OUTPUT: Tue Jun 8 20:09:19 2010 SUM: 3DDA245A/v2503/blackwell/journals/jasp_v40_i8/jasp_653
Mediational Models
Structural equation modeling (SEM) was employed to examine our pro-posed mediational model. Analyses were conducted using the Version 4.01of the AMOS program (Arbuckle, 1999). Model fit was assessed usingthe following indexes: chi square divided by degrees of freedom (c2/df),non-normed fit index (NNFI; Bentler & Bonett, 1980), comparative fit index(CFI; Bentler, 1990), and root mean square error of approximation(RMSEA; Steiger, 1980).
Although a nonsignificant p value has traditionally been used as a crite-rion for not rejecting an SEM, this criterion is overly strict and is too sensitivefor models containing many variables (Kelloway, 1998). Therefore, in thepresent study, alternative criteria that reflect real-world conditions were alsoused. A model in which c2/df was �5, CFI and NNFI were greater than .90,and RMSEA was between .00 and .08 (Hu & Bentler, 1998, 1999) wasdeemed acceptable. These moderately stringent acceptance criteria clearlyreject inadequate or poorly specified models, while accepting for consider-ation models that meet real-world criteria for reasonable fit and representa-tion of the data (Kelloway, 1998).
In addition, to test the mediating effects further, statistics were computedto examine the significance of the indirect relationships via the hypothesizedmediator. As indicated earlier, correlations among the variables and theirmeans and standard deviations are presented in Table 2.
First, we used SEM to examine the direct effect of perfectionistic self-presentation, a latent construct defined by three indicators: perfectionisticself-promotion, nondisplay of imperfection, and nondisclosure of imperfec-tion (Predictor 1) or of the observed variable SPP (Predictor 2) on depression(outcome). Next, we used SEM to examine the mediational models in whichthe mediating role of social problem-solving ability was a latent constructdefined by three indicators: cognition, emotion, and behavior (mediator).Models were run separately for men and for women.
Direct-Effect Models
The direct-effect models of the effect of perfectionistic self-presentationon depression fit the data well: women, c2(2) = 1.97, c2/df = 0.94(NNFI = .99, CFI = .10, RMSEA = .0000); men, c2(2) = 1.51, c2/df = 0.47(NNFI = .99, CFI = .10, RMSEA = .0000). Perfectionistic Self-Presentationpredicted higher levels of depression: women, b = .28, t = 2.73, p < .006; men,b = .24, t = 2.21, p < .027. This model explained 8% and 6% of the variance indepression among women and men, respectively.
2140 BESSER ET AL.
1
2
3
4
5
6
7
8
9
10
11
12
13
14
15
16
17
18
19
20
21
22
23
24
25
26
27
28
29
30
31
32
33
34
35
36
37
38
39
40
41
JOBNAME: No Job Name PAGE: 19 SESS: 17 OUTPUT: Tue Jun 8 20:09:19 2010 SUM: 2A821B44/v2503/blackwell/journals/jasp_v40_i8/jasp_653
The direct-effect models of the effect of socially prescribed perfectionismon depression indicates that socially prescribed perfectionism predictedhigher levels of depression: women, b = .31, t = 3.23, p < .001; men, b = .28,t = 2.85, p < .004. This model explained 10% and 8% of the variance indepression among women and men, respectively.
Mediational Effect Models
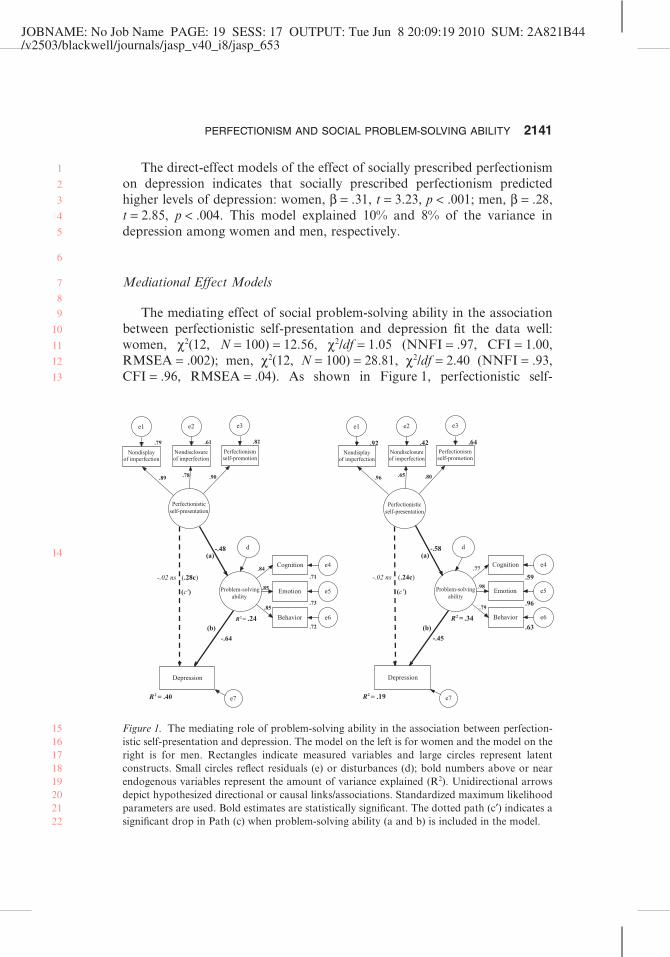
The mediating effect of social problem-solving ability in the associationbetween perfectionistic self-presentation and depression fit the data well:women, c2(12, N = 100) = 12.56, c2/df = 1.05 (NNFI = .97, CFI = 1.00,RMSEA = .002); men, c2(12, N = 100) = 28.81, c2/df = 2.40 (NNFI = .93,CFI = .96, RMSEA = .04). As shown in Figure 1, perfectionistic self-
Perfectionisticself-presentation
.92 Nondisplay
of imperfection
e1
.42 Nondisclosureof imperfection
e2
.64 Perfectionismself-promotion
e3
R2 = .19
Depression
e7
R2 = .34
Problem-solvingability
.59
Cognition e4.77
.96
Emotion e5.98
.63
Behavior e6
.79
-.58
-.45
d
.65 .80.96
(a)
(b)
(c')
-.02 ns (.24c)
.79
Nondisplayof imperfection
e1
.61
Nondisclosureof imperfection
e2
.82
Perfectionismself-promotion
e3
R2 = .40
Depression
e7
R2 = .24
.71
Cognition e4.84
.73
Emotion e5.85
.72
Behavior e6
.85
-.48
-.64
d
.78 .90 .89
(a)
(b)
(c')
-.02 ns (.28c)
Perfectionisticself-presentation
Problem-solvingability
Figure 1. The mediating role of problem-solving ability in the association between perfection-istic self-presentation and depression. The model on the left is for women and the model on theright is for men. Rectangles indicate measured variables and large circles represent latentconstructs. Small circles reflect residuals (e) or disturbances (d); bold numbers above or nearendogenous variables represent the amount of variance explained (R2). Unidirectional arrowsdepict hypothesized directional or causal links/associations. Standardized maximum likelihoodparameters are used. Bold estimates are statistically significant. The dotted path (c′) indicates asignificant drop in Path (c) when problem-solving ability (a and b) is included in the model.
PERFECTIONISM AND SOCIAL PROBLEM-SOLVING ABILITY 2141
1
2
3
4
5
6
7
8
9
10
11
12
13
14
1516171819202122
JOBNAME: No Job Name PAGE: 20 SESS: 17 OUTPUT: Tue Jun 8 20:09:19 2010 SUM: 3FDEEB92/v2503/blackwell/journals/jasp_v40_i8/jasp_653
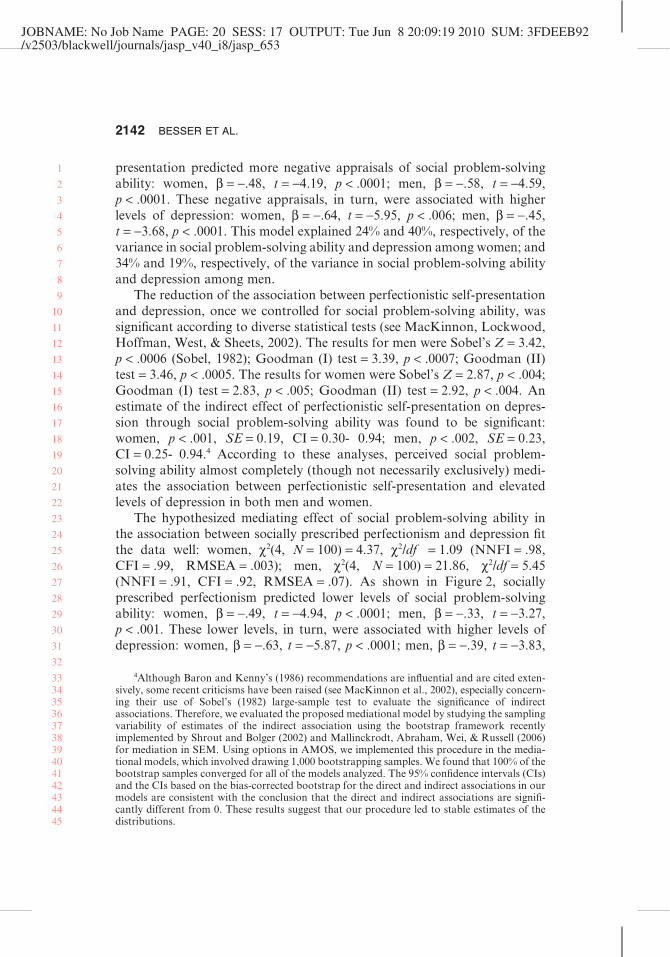
presentation predicted more negative appraisals of social problem-solvingability: women, b = -.48, t = -4.19, p < .0001; men, b = -.58, t = -4.59,p < .0001. These negative appraisals, in turn, were associated with higherlevels of depression: women, b = -.64, t = -5.95, p < .006; men, b = -.45,t = -3.68, p < .0001. This model explained 24% and 40%, respectively, of thevariance in social problem-solving ability and depression among women; and34% and 19%, respectively, of the variance in social problem-solving abilityand depression among men.
The reduction of the association between perfectionistic self-presentationand depression, once we controlled for social problem-solving ability, wassignificant according to diverse statistical tests (see MacKinnon, Lockwood,Hoffman, West, & Sheets, 2002). The results for men were Sobel’s Z = 3.42,p < .0006 (Sobel, 1982); Goodman (I) test = 3.39, p < .0007; Goodman (II)test = 3.46, p < .0005. The results for women were Sobel’s Z = 2.87, p < .004;Goodman (I) test = 2.83, p < .005; Goodman (II) test = 2.92, p < .004. Anestimate of the indirect effect of perfectionistic self-presentation on depres-sion through social problem-solving ability was found to be significant:women, p < .001, SE = 0.19, CI = 0.30- 0.94; men, p < .002, SE = 0.23,CI = 0.25- 0.94.4 According to these analyses, perceived social problem-solving ability almost completely (though not necessarily exclusively) medi-ates the association between perfectionistic self-presentation and elevatedlevels of depression in both men and women.
The hypothesized mediating effect of social problem-solving ability inthe association between socially prescribed perfectionism and depression fitthe data well: women, c2(4, N = 100) = 4.37, c2/df = 1.09 (NNFI = .98,CFI = .99, RMSEA = .003); men, c2(4, N = 100) = 21.86, c2/df = 5.45(NNFI = .91, CFI = .92, RMSEA = .07). As shown in Figure 2, sociallyprescribed perfectionism predicted lower levels of social problem-solvingability: women, b = -.49, t = -4.94, p < .0001; men, b = -.33, t = -3.27,p < .001. These lower levels, in turn, were associated with higher levels ofdepression: women, b = -.63, t = -5.87, p < .0001; men, b = -.39, t = -3.83,
4Although Baron and Kenny’s (1986) recommendations are influential and are cited exten-sively, some recent criticisms have been raised (see MacKinnon et al., 2002), especially concern-ing their use of Sobel’s (1982) large-sample test to evaluate the significance of indirectassociations. Therefore, we evaluated the proposed mediational model by studying the samplingvariability of estimates of the indirect association using the bootstrap framework recentlyimplemented by Shrout and Bolger (2002) and Mallinckrodt, Abraham, Wei, & Russell (2006)for mediation in SEM. Using options in AMOS, we implemented this procedure in the media-tional models, which involved drawing 1,000 bootstrapping samples. We found that 100% of thebootstrap samples converged for all of the models analyzed. The 95% confidence intervals (CIs)and the CIs based on the bias-corrected bootstrap for the direct and indirect associations in ourmodels are consistent with the conclusion that the direct and indirect associations are signifi-cantly different from 0. These results suggest that our procedure led to stable estimates of thedistributions.
2142 BESSER ET AL.
1
2
3
4
5
6
7
8
9
10
11
12
13
14
15
16
17
18
19
20
21
22
23
24
25
26
27
28
29
30
31
32
33343536373839404142434445
JOBNAME: No Job Name PAGE: 21 SESS: 17 OUTPUT: Tue Jun 8 20:09:19 2010 SUM: 396E2E0B/v2503/blackwell/journals/jasp_v40_i8/jasp_653
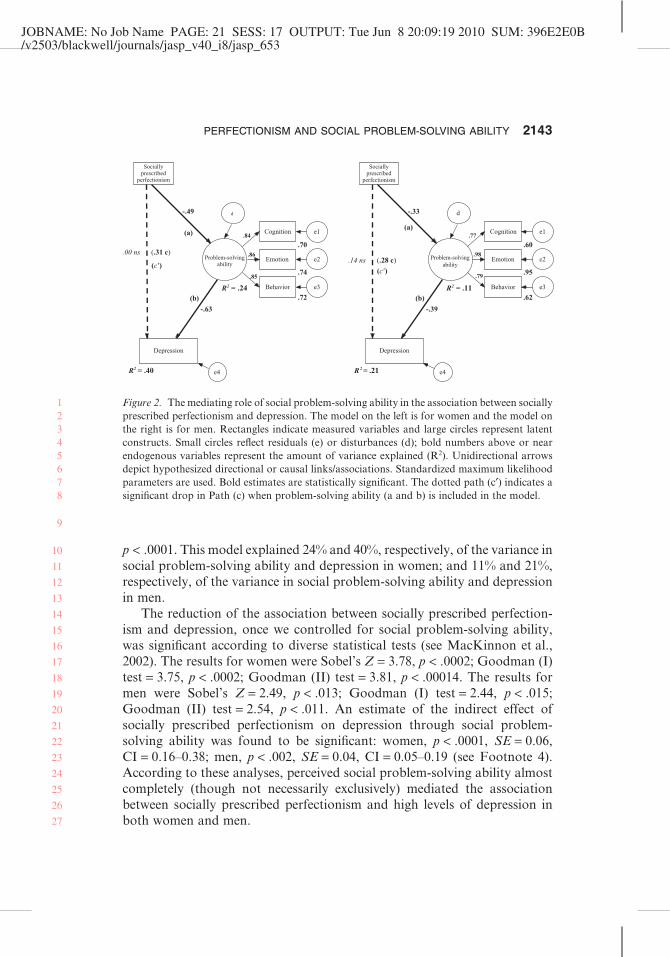
p < .0001. This model explained 24% and 40%, respectively, of the variance insocial problem-solving ability and depression in women; and 11% and 21%,respectively, of the variance in social problem-solving ability and depressionin men.
The reduction of the association between socially prescribed perfection-ism and depression, once we controlled for social problem-solving ability,was significant according to diverse statistical tests (see MacKinnon et al.,2002). The results for women were Sobel’s Z = 3.78, p < .0002; Goodman (I)test = 3.75, p < .0002; Goodman (II) test = 3.81, p < .00014. The results formen were Sobel’s Z = 2.49, p < .013; Goodman (I) test = 2.44, p < .015;Goodman (II) test = 2.54, p < .011. An estimate of the indirect effect ofsocially prescribed perfectionism on depression through social problem-solving ability was found to be significant: women, p < .0001, SE = 0.06,CI = 0.16–0.38; men, p < .002, SE = 0.04, CI = 0.05–0.19 (see Footnote 4).According to these analyses, perceived social problem-solving ability almostcompletely (though not necessarily exclusively) mediated the associationbetween socially prescribed perfectionism and high levels of depression inboth women and men.
Sociallyprescribed
perfectionism
R2 = .40
Depression
e4
R2 = .24
.70
Cognition e1 .84
.74
Emotion e2.86
.72
Behavior e3
.85
-.63
d -.49
(a)
(b)
(c')
.00 ns (.31 c) Problem-solving
ability
Sociallyprescribed
perfectionism
R 2 = .21
Depression
e4
R2 = .11
.60
Cognition e1.77
.95
Emotion e2.98
.62
Behavior e3
.79
-.39
d-.33
(b)
(a)
(c')
.14 ns (.28 c) Problem-solvingability
Figure 2. The mediating role of social problem-solving ability in the association between sociallyprescribed perfectionism and depression. The model on the left is for women and the model onthe right is for men. Rectangles indicate measured variables and large circles represent latentconstructs. Small circles reflect residuals (e) or disturbances (d); bold numbers above or nearendogenous variables represent the amount of variance explained (R2). Unidirectional arrowsdepict hypothesized directional or causal links/associations. Standardized maximum likelihoodparameters are used. Bold estimates are statistically significant. The dotted path (c′) indicates asignificant drop in Path (c) when problem-solving ability (a and b) is included in the model.
PERFECTIONISM AND SOCIAL PROBLEM-SOLVING ABILITY 2143
12345678
9
10
11
12
13
14
15
16
17
18
19
20
21
22
23
24
25
26
27

JOBNAME: No Job Name PAGE: 22 SESS: 17 OUTPUT: Tue Jun 8 20:09:19 2010 SUM: 496B089F/v2503/blackwell/journals/jasp_v40_i8/jasp_653
Discussion
The purpose of the current study was to extend the existing research onperfectionism and self-reported problem-solving ability by examining thelink between perfectionism and problem-solving ability in a communitysample of Israeli adults. This study adopted a broader focus than previousresearch on this topic by including measures of perfectionistic self-presentation, in addition to trait measures of perfectionism. The currentstudy also incorporated a focus on gender differences and included empiricaltests of whether social problem-solving ability mediates the links betweenperfectionism dimensions (i.e., trait perfectionism, perfectionistic self-presentation) and depression.
Consistent with past research with university students, our results (for thetotal sample) confirmed that socially prescribed perfectionism is associatedwith a negative problem-solving orientation. Socially prescribed perfection-ism was correlated significantly with a negative problem-solving orientationin terms of the overall scale, as well as all three SPSI subscales (i.e., affect,behavior, and cognition).
In contrast, self-oriented and other-oriented perfectionism are not asso-ciated with the problem-solving orientation measures. The obtained associa-tion between a negative problem orientation and socially prescribedperfectionism is generally in keeping with observations that emphasize theimportance of viewing an individual’s problem-solving ability from a social-cognitive perspective (see Bandura, 1986; D’Zurilla & Nezu, 1990). Someinvestigators (e.g., Nezu et al., 2004; Spence et al., 2002) have concluded thata negative problem-solving orientation may actually constitute a cognitivediathesis for depression, in part because a negative problem-solving orienta-tion incorporates negative cognitive and motivational reactions to life prob-lems. Our results suggest that individuals with high levels of sociallyprescribed perfectionism and a negative problem-solving orientation may beparticularly at risk.
The data from our total sample also show that self-oriented perfectionismis associated with positive appraisals, in terms of the SPSI subscales assessingactual problem-solving skills, especially among men. This clarifies earlierresearch by Flett et al. (1996), who reported that this association was evidentin only one of their two studies with university students. The current findingsare in accordance with previous research linking self-oriented perfectionismwith learned resourcefulness and self-control in university students (Flett,Hewitt, Blankstein, & O’Brien, 1991). Our new data are interesting andpotentially important in light of accumulating evidence that self-orientedperfectionism can sometimes be adaptive in nonclinical samples (see Bielinget al., 2003; Slaney, Rice, & Ashby, 2002).
2144 BESSER ET AL.
123
4
5
6
7
8
9
10
11
12
13
14
15
16
17
18
19
20
21
22
23
24
25
26
27
28
29
30
31
32
33
34
35
36
37
38
39
40
41
42
JOBNAME: No Job Name PAGE: 23 SESS: 17 OUTPUT: Tue Jun 8 20:09:19 2010 SUM: 4EE4C87F/v2503/blackwell/journals/jasp_v40_i8/jasp_653
Although self-oriented perfectionism is sometimes associated with posi-tive outcomes in students, this is not always the case. An experimentalinvestigation showed that students with high self-oriented perfectionismhad negative cognitive and affective responses to failure feedback on anego-involving performance task (Besser, Flett, & Hewitt, 2004). Moreover,other evidence from studies involving psychiatric patients has suggested thatself-oriented perfectionism is associated with dispositional self-criticism(Hewitt & Flett, 1993), and self-oriented perfectionism combined with theexperience of life stress is often associated with depression (see Flett, Hewitt,Blankstein, & Mosher, 1995; Hewitt & Flett, 1993; Hewitt, Flett, & Ediger,1996). Perhaps it is the presence of positive problem-solving skills andresourcefulness that sometimes protects certain self-oriented perfectionistsfrom maladjustment.
A unique finding of the current study is that perfectionistic self-presentation is robustly associated with a negative problem-solving orienta-tion. All dimensions of perfectionistic self-presentation were linked withoverall scores on the measure of negative problem-solving orientation, as wellas the affect, cognition, and behavior subscales. Thus, perfectionistic self-presenters seem to have cognitive, emotional, and behavioral characteristicsand responses that tend to undermine their ability to solve personal prob-lems. Examination of the PSPS subscales indicated in the total sample thatthe nondisplay of imperfections subscale had the strongest link with themeasures of problem-solving orientation, but all three PSPS had significantassociations with the problem-solving orientation subscales. In contrast,weaker results were evident with the problem-solving skills measure, with thenondisclosure of imperfections subscale being the only PSPS subscale linkedwith deficient problem-solving skills.
Although past research has not examined the possibility that perfection-istic self-presentation may be associated with maladaptive problem-solvingand coping orientations, the pervasive link between perfectionistic self-presentation and poor problem-solving orientation in the current study wasexpected, given that acknowledging and confronting personal problems in atask-focused manner is not in keeping with the perfectionist’s need to avoiddisclosing personal mistakes and shortcomings. Also, perfectionistic self-presentation can be considered an extremely neurotic form of self-presentation, and neurotic tendencies in general have been linked withnegative appraisals of problem-solving ability (Elliott et al., 1994). Theobtained associations between perfectionistic self-presentation and variousindexes of negative problem orientation are consistent with more generalfindings suggesting that perfectionistic self-presenters are at risk for psycho-logical problems, and that they have negative self-evaluative tendencies anddiminished self-esteem (see Hewitt et al., 2003).
PERFECTIONISM AND SOCIAL PROBLEM-SOLVING ABILITY 2145
1
2
3
4
5
6
7
8
9
10
11
12
13
14
15
16
17
18
19
20
21
22
23
24
25
26
27
28
29
30
31
32
33
34
35
36
37
38
39
40
41
42
JOBNAME: No Job Name PAGE: 24 SESS: 17 OUTPUT: Tue Jun 8 20:09:19 2010 SUM: 4C55F7B5/v2503/blackwell/journals/jasp_v40_i8/jasp_653
In light of Horney’s (1945) suggestion that those who are preoccupiedwith a fear of disclosure may be unwilling to engage proactively in behaviorsthat could entail exposure to humiliation and ridicule, it is possible that thelink between perfectionistic self-presentation and negative problem-solvingorientation is actually a reflection of a more general avoidance tendency, anddisengagement from activities and situations that could reveal flaws in theself. As a recent study by Hewitt, Habke, Lee-Baggley, Sherry, and Flett(2008) indicated, this defensiveness and avoidance can have very negativeimplications for people with high levels of perfectionistic self-presentationwho are receiving treatment. The tendency to distance and disengage isreflected in a poorer therapeutic alliance, as might be expected if there islimited self-disclosure.
It remains to be established in future behavioral investigations whetherindividuals with high levels of perfectionistic self-presentation are actuallyless able to solve problems, or if this is merely their perception. It is quitepossible that perfectionistic self-presenters have a problem in terms of cog-nitive appraisals of their own problem-solving abilities, rather than actualskill deficits. Perhaps this is a result of their evaluating themselves accordingto exceptionally stringent criteria. Previous research by Blankstein, Flett, andJohnston (1992) found that depressed university students gave negativeappraisals of their problem-solving ability, even though their scores on theMeans–End Problem-Solving Test indicated no actual deficits in the qualityof their solutions to problems.
As expected, our results show that higher levels of depression are associ-ated with socially prescribed perfectionism, perfectionistic self-presentation,and a negative problem-solving orientation. In this study, the most robustassociation with depression involved the cognitive subscale tapping problem-solving orientation and depression. A key aspect of the current studyinvolved tests of a mediational model linking perfectionism, social problem-solving ability, and depression. Our analyses confirm that social problem-solving ability does, indeed, mediate the link between perfectionism anddepressive symptoms. Perfectionism is defined in one analysis as a constructcomprised of the three facets of perfectionistic self-presentation versussocially prescribed perfectionism in another analysis. Thus, people with highlevels of socially prescribed perfectionism and perfectionistic self-presentation are prone to depression, in part, because they have a negativeproblem-solving orientation in terms of their cognitive, emotional, andbehavioral problem-solving orientations.
Analyses were conducted separately for men and women, and supportwas obtained for the mediational model in both instances. However, it wasalso evident that the model was substantially stronger for women, andthe associations between the predictor and the mediator and between the
2146 BESSER ET AL.
1
2
3
4
5
6
7
8
9
10
11
12
13
14
15
16
17
18
19
20
21
22
23
24
25
26
27
28
29
30
31
32
33
34
35
36
37
38
39
40
41
42
JOBNAME: No Job Name PAGE: 25 SESS: 17 OUTPUT: Tue Jun 8 20:09:19 2010 SUM: 49919214/v2503/blackwell/journals/jasp_v40_i8/jasp_653
mediator and the outcome variable for women and men were very different.Although these results should be replicated and examined in longitudinalstudies, the results of our analyses suggest that perfectionism and perceiveddeficits in social problem-solving ability may play a greater role in women’sexperience of depressive symptoms. These findings further underscore theneed to consider possible gender differences in terms of the nomologicalnetwork of the perfectionism construct.
Implications of the Current Findings
The current findings involving individual differences in perfectionismhave several implications of theoretical and practical importance. At thetheoretical level, the current findings support recent conceptualizations andempirical attempts to examine coping moderators and mediators of the asso-ciation between perfectionism and maladjustment (see Dunkley et al., 2003;Hewitt & Flett, 2002; Hewitt, Flett, & Endler, 1995; O’Connor & O’Connor,2003). In addition, it is evident that our results varied as a function of theperfectionism dimension in question, and this further underscores the useful-ness of conceptualizing and assessing perfectionism as a multidimensionalconstruct.
At the practical level, the current findings have clear implications for thesocial problem-solving process. Our results indicate that distressed individu-als who are characterized by the interpersonal aspects of perfectionism arelikely to benefit substantially from problem-solving interventions designed toincrease their sense of efficacy in dealing with important life problems. Ingeneral, problem-solving therapy for depression has proven quite effective(see Bell & D’Zurilla, 2009).
At the same time, it is reasonable to expect that these same perfectionistswill be quite defensive, especially if they have the perfectionistic self-presentational style. They may react quite strongly to potentially embarrass-ing situations. They may also react poorly to unrealistic problem-solvinggoals that they perceive as unattainable or overly demanding. Clearly, a keytask for therapists is to get beyond this defensiveness, to help foster a moreadaptive approach to problem solving.
Research on the effectiveness of problem-solving interventions in adoles-cents has found that a preventive program that emphasizes problem solvingis initially successful in reducing levels of depression (see Hussian &Lawrence, 1981; Nezu, 1986), but the successes of this intervention may notnecessarily be maintained over time (e.g., Spence, Sheffield, & Donovan,2003). Our findings suggest that certain perfectionists may benefit greatlyfrom prevention programs focused on improving their problem-solving
PERFECTIONISM AND SOCIAL PROBLEM-SOLVING ABILITY 2147
1
2
3
4
5
6
7
8
9
10
11
12
13
14
15
16
17
18
19
20
21
22
23
24
25
26
27
28
29
30
31
32
33
34
35
36
37
38
39
40
41
JOBNAME: No Job Name PAGE: 26 SESS: 17 OUTPUT: Tue Jun 8 20:09:19 2010 SUM: 444BE152/v2503/blackwell/journals/jasp_v40_i8/jasp_653
orientation and problem-solving skills, but it would be substantially better ifsuch preventive efforts also incorporated an emphasis on the potentialdeleterious effects of various dimensions of perfectionism.
Limitations of the Current Study
The limitations of the current study must be acknowledged. First andforemost, it will be important in subsequent research to incorporate a lon-gitudinal element, so that it can be determined whether dimensions ofperfectionism interact with poor problem-solving ability to predict vulner-ability to psychological distress. Given evidence that social problem solvingmoderates the link between stress and depression (see Nezu & Ronan, 1985,1988; Spence et al., 2002), as well as the moderational role of life stress inperfectionism and depression (see Hewitt & Flett, 2002), it is clear thatfuture longitudinal investigations in this area should also focus on indi-vidual differences in the experience and appraisal of negative life events andlife problems.
Another issue that should be evaluated is whether certain findings arespecific to the experience of depressive symptoms or generalize to otherforms of psychological distress. It is quite likely that perfectionism anddeficient problem solving both contribute to various forms of maladjust-ment. In fact, it is important to acknowledge that the general model linkingperfectionism and problem-solving deficits should be relevant to an under-standing of suicidal tendencies, given the established link between problem-solving deficits and suicidality (see Clum & Febbraro, 1994, 2004). In thisregard, Chang (2002) found that the interaction of perfectionism andproblem solving was more predictive of suicide ideation than it was ofdepressive symptoms. Forman, Berk, Henriques, Brown, and Beck (2004)showed that deficits in problem solving are linked with repeated suicideattempts.
Finally, the current results are based solely on self-report measures, andmore rigorous methods could be incorporated into future investigations.Research on perfectionism is just beginning to include observer ratings, andmost existing data are based on self-reports (for a discussion, see Flett et al.,2005). Future research should examine whether similar findings are detectedwhen various types of data (e.g., observer ratings) are utilized. In this regard,existing research has suggested that observers (peers and clinicians) canreliably assess individual differences in perfectionistic self-presentation (seeHewitt et al., 2003).
In summary, the results of the present study attest to the usefulness ofexamining perfectionism and perceptions of social problem solving. We
2148 BESSER ET AL.
1
2
3
4
5
6
7
8
9
10
11
12
13
14
15
16
17
18
19
20
21
22
23
24
25
26
27
28
29
30
31
32
33
34
35
36
37
38
39
40
41
JOBNAME: No Job Name PAGE: 27 SESS: 17 OUTPUT: Tue Jun 8 20:09:19 2010 SUM: 892C3176/v2503/blackwell/journals/jasp_v40_i8/jasp_653
found that socially prescribed perfectionism and all dimensions of perfec-tionistic self-presentation are associated with reports of poorer problem-solving orientation. In addition, our results support the view that socialproblem solving mediates the link between perfectionism and depression.Our results also provide some indication of the need for a nuanced approachthat takes possible gender differences into account because the mediationalmodel was more predictive for women.
Overall, these findings demonstrate the usefulness of investigating indi-vidual differences in perfectionists’ self-perceptions of problem-solvingability, and suggest the need for intervention strategies that are designed toenhance the perceived problem-solving abilities of individuals who feel thatthey must be perfect when in public and who feel a great pressure to meet theperfectionistic expectations of other people. More positive perceptions ofproblem-solving ability should play a key role in alleviating some of thepsychological distress experienced by certain perfectionists.
References
Adler, A. (1956). The neurotic dispositions. In H. L. Ansbacher & R. R.Ansbacher (Eds.), The individual psychology of Alfred Adler (pp. 239–262). New York: Harper.
Arbuckle, J. L. (1999). AMOS: A structural equation modeling program.Chicago: Small Waters.
Argus, G., & Thompson, M. (2008). Perceived social problem solving ability,perfectionism, and mindful awareness in clinical depression: An explor-atory study. Cognitive Therapy and Research, 32, 745–757.
Bandura, A. (1986). Social foundations of thought and action: A socialcognitive theory. Englewood Cliffs, NJ: Prentice Hall.
Baron, R. M., & Kenny, D. A. (1986). The moderator–mediator variabledistinction in social psychological research: Conceptual, strategic, andstatistical considerations. Journal of Personality and Social Psychology,51, 1173–1182.
Bell, A. C., & D’Zurilla, T. J. (2009). Problem-solving therapy for depression:A meta-analysis. Clinical Psychology Review, 29, 348–353.
Bentler, P. M. (1990). Comparative fit indexes in structural models. Psycho-logical Bulletin, 107, 238–246.
Bentler, P. M., & Bonett, D. G. 1980. Significance tests and goodness-of-fit inthe analysis of covariance structures. Psychological Bulletin, 88, 588–606.
Besser, A., Flett, G. L., & Hewitt, P. L. (2004). Perfectionism, cognition,and affect in response to performance failure versus success. Journal ofRational-Emotive and Cognitive-Behavior Therapy, 22, 297–324.
PERFECTIONISM AND SOCIAL PROBLEM-SOLVING ABILITY 2149
1
2
3
4
5
6
7
8
9
10
11
12
13
14
15
16
171819
20
21
22
23
24
25
26
27
28
29
30
31
32
33
34
35
36
37
38
39
40
41
JOBNAME: No Job Name PAGE: 28 SESS: 17 OUTPUT: Tue Jun 8 20:09:19 2010 SUM: C9DF3313/v2503/blackwell/journals/jasp_v40_i8/jasp_653
Bieling, P. J., Israeli, A., Smith, J., & Antony, M. M. (2003). Making thegrade: The behavioral consequences of perfectionism in the classroom.Personality and Individual Differences, 35, 163–178.
Blankstein, K. R., Flett, G. L., & Johnston, M. E. (1992). Depression,problem-solving appraisals, and problem-solving ability. Journal of Clini-cal Psychology, 48, 749–759.
Blankstein, K. R., Lumley, C. H., & Crawford, A. (2007). Perfectionism,hopelessness, and suicide ideation: Revisions to diathesis-stress and spe-cific vulnerability models. Journal of Rational-Emotive and Cognitive-Behavior Therapy, 25, 279–319.
Butler, L., & Meichenbaum, D. (1981). The assessment of interpersonalproblem-solving skills. In P. C. Kendall & S. D. Hollon (Eds.), Assess-ment strategies for cognitive-behavioral interventions (pp. 197–225). SanDiego, CA: Academic Press.
Chang, E. C. (1998). Cultural differences, perfectionism, and suicidal risk ina college population: Does social problem-solving still matter? CognitiveTherapy and Research, 22, 237–254.
Chang, E. C. (2002). Examining the link between perfectionism and psycho-logical maladjustment: Social problem-solving as a buffer. CognitiveTherapy and Research, 26, 581–595.
Cheng, S. K. (2001). Life stress, problem-solving, perfectionism, and depres-sive symptoms in Chinese. Cognitive Therapy and Research, 25, 303–310.
Clum, G. A., & Febbraro, G. A. R. (1994). Stress, social support, andproblem-solving appraisal/skills: Prediction of suicide severity within acollege sample. Assessment, 16, 69–83.
Clum, G. A., & Febbraro, G. A. R. (2004). Social problem-solving andsuicide risk. In E. C. Chang, T. J. D’Zurilla, & L. J. Sanna (Eds.), Socialproblem-solving: Theory, research, and training (pp. 67–72). Washington,DC: American Psychological Association.
Cockell, S. J., Hewitt, P. L., Seal, B., Sherry, S. B., Goldner, E. M., Flett, G.L., et al. (2002). Trait and self-presentational dimensions of perfectionismamong women with anorexia nervosa. Cognitive Therapy and Research,26, 745–758.
Dean, P. J., & Range, L. M. (1996). The escape theory of suicide andperfectionism in college students. Death Studies, 20, 415–424.
Dean, P. J., Range, L. M., & Goggin, W. C. (1996). The escape theory ofsuicide in college students: Testing a model that includes perfectionism.Suicide and Life-Threatening Behavior, 26, 181–186.
DiBartolo, P. M., Frost, R. O., Chang, P., LaSota, M., & Grills, A. E. (2004).Shedding light on the relationship between personal standards and psy-chopathology: The case for contingent self-worth. Journal of Rational-Emotive and Cognitive-Behavior Therapy, 22, 237–250.
2150 BESSER ET AL.
1
2
3
4
5
6
7
8
9
10
11
12
13
14
15
16
17
18
19
20
21
22
23
24
25
26
27
28
29
30
31
32
33
34
35
36
37
38
39
40
41
42
JOBNAME: No Job Name PAGE: 29 SESS: 17 OUTPUT: Tue Jun 8 20:09:19 2010 SUM: BD9E2309/v2503/blackwell/journals/jasp_v40_i8/jasp_653
Dunkley, D. M., Blankstein, K. R., Halsall, J., Williams, M., & Winkworth,G. (2000). The relation between perfectionism and distress: Hassles,coping, and perceived social support as mediators and moderators.Journal of Counseling Psychology, 47, 437–453.
Dunkley, D. M., Zuroff, D. C., & Blankstein, K. R. (2003). Self-criticalperfectionism and daily affect: Dispositional and situational influences onstress and coping. Journal of Personality and Social Psychology, 84, 234–252.
D’Zurilla, T. J. (1986). Problem-solving therapy: A social competenceapproach to clinical intervention. New York: Springer.
D’Zurilla, T. J., & Goldfried, M. R. (1971). Problem-solving and behaviormodification. Journal of Abnormal Psychology, 78, 107–126.
D’Zurilla, T. J., & Nezu, A. M. (1990). Development and preliminary evalu-ation of the Social Problem-Solving Inventory (SPSI). PsychologicalAssessment: A Journal of Consulting and Clinical Psychology, 2, 156–163.
D’Zurilla, T. J., Nezu, A. M., & Maydeu-Olivares, A. (1996). Manual for theSocial Problem-Solving Inventory—Revised. Unpublished manuscript,State University of New York at Stony Brook, Stony Brook, NY.
Eaton, W. W., Muntaner, C., Smith, C., Tien, A., & Ybarra, M. (2004).Center For Epidemiologic Studies Depression Scale: Review and revision(CESD and CESDR). In M. E. Maruish (Ed.), The use of psychologicaltesting for treatment planning and outcomes assessment (3rd ed., pp. 363–378). Mahwah, NJ: Lawrence Erlbaum.
Elliott, G. C. (1982). Self-esteem and self-presentation among the young as afunction of age and gender. Journal of Youth and Adolescence, 11, 135–153.
Elliott, T. R., Herrick, S. M., MacNair, R. R., & Harkins, S. W. (1994).Personality correlates of self-appraised problem-solving orientation:Problem orientation and trait affectivity. Journal of Personality Assess-ment, 63, 489–505.
Ferrari, J. R., & Thompson, T. (2006). Impostor fears: Links with self-presentational concerns and self-handicapping behaviors. Personality andIndividual Differences, 40, 341–352.
Flett, G. L., Besser, A., & Hewitt, P. L. (2005). Perfectionism, ego defensestyles, and depression: A comparison of self versus informant ratings.Journal of Personality, 73, 1355–1396.
Flett, G. L., Greene, A., & Hewitt, P. L. (2004). Dimensions of perfectionismand anxiety sensitivity. Journal of Rational-Emotive and Cognitive-Behavior Therapy, 22, 37–55.
Flett, G. L., Hewitt, P. L., Blankstein, K. R., & Mosher, S. W. (1995).Perfectionism, life events, and depressive symptoms: A test of a diathesis-stress model. Current Psychology, 14, 112–137.
PERFECTIONISM AND SOCIAL PROBLEM-SOLVING ABILITY 2151
1
2
3
4
5
6
7
8
9
10
11
12
13
14
15
16
17
18
19
20
21
22
23
24
25
26
27
28
29
30
31
32
33
34
35
36
37
38
39
40
41
42
JOBNAME: No Job Name PAGE: 30 SESS: 17 OUTPUT: Tue Jun 8 20:09:19 2010 SUM: CA3D9F31/v2503/blackwell/journals/jasp_v40_i8/jasp_653
Flett, G. L., Hewitt, P. L., Blankstein, K. R., & O’Brien, S. (1991). Perfec-tionism and learned resourcefulness in depression and self-esteem.Personality and Individual Differences, 12, 61–68.
Flett, G. L., Hewitt, P. L., Blankstein, K. R., Solnik, M., & Van Brunschot,M. (1996). Perfectionism, social problem-solving ability, and psychologi-cal distress. Journal of Rational-Emotive and Cognitive-Behavior Therapy,14, 245–275.
Flett, G. L., Hewitt, P. L., Shapiro, B., & Rayman, J. (2000–2001). Perfec-tionism, beliefs, and adjustment in dating relationships. Current Psychol-ogy, 20, 289–311.
Flett, G. L., Sawatzky, D. L., & Hewitt, P. L. (1995). Dimensions of perfec-tionism and goal commitment: A further comparison of two perfection-ism measures. Journal of Psychopathology and Behavioral Assessment, 17,111–124.
Forman, E. M., Berk, M. S., Henriques, G. R., Brown, G. K., & Beck, A. T.(2004). History of multiple suicide attempts as a behavioral marker ofsevere psychopathology. American Journal of Psychiatry, 161, 437–443.
Frost, R. O., Heimberg, R., Holt, C., Mattia, J., & Neubauer, A. (1993). Acomparison of two measures of perfectionism. Personality and IndividualDifferences, 14, 119–126.
Frost, R., & Marten, P. (1990). Perfectionism and evaluative threat. Cogni-tive Therapy and Research, 14, 559–572.
Frost, R. O., Marten, P. A., Lahart, C., & Rosenblate, R. (1990). Thedimensions of perfectionism. Cognitive Therapy and Research, 14, 449–468.
Geller, J., Cockell, S. J., Hewitt, P. L., Goldner, E. M., & Flett, G. L. (2000).Inhibited expression of negative emotions and interpersonal orientationin anorexia nervosa. International Journal of Eating Disorders, 28, 8–19.
Haaga, D. A. F., Fine, J. A., Terrill, D. R., Stewart, B. L., & Beck, A. T.(1995). Social problem-solving deficits, dependency, and depressivesymptoms. Cognitive Therapy and Research, 19, 147–158.
Habke, A. M., Hewitt, P. L., & Flett, G. L. (1999). Perfectionism and sexualsatisfaction in intimate relationships. Journal of Psychopathology andBehavioral Assessment, 21, 307–322.
Heppner, P. P. (1978). A review of the problem-solving literature and itsrelationship to the counseling process. Journal of Counseling Psychology,25, 366–375.
Heppner, P. P., Baumgardner, A. H., & Jackson, S. A. (1985). Problem-solving, self-appraisal, depression, and attributional style: Are theyrelated? Cognitive Therapy and Research, 9, 105–113.
2152 BESSER ET AL.
1
2
3
4
5
6
7
8
9
10
11
12
13
14
15
16
17
18
19
20
21
22
23
24
25
26
27
28
29
30
31
32
33
34
35
36
37
38
39
40
41
42
JOBNAME: No Job Name PAGE: 31 SESS: 17 OUTPUT: Tue Jun 8 20:09:19 2010 SUM: C1D84BED/v2503/blackwell/journals/jasp_v40_i8/jasp_653
Heppner, P. P., Kampa, M., & Brunning, L. (1987). The relationship betweenproblem-solving self-appraisal and indices of physical and psychologicalhealth. Cognitive Therapy and Research, 11, 155–168.
Heppner, P. P., & Petersen, C. H. (1982). The development and implicationsof a personal problem-solving inventory. Journal of Counseling Psychol-ogy, 29, 66–75.
Heppner, P. P., Witty, T. E., & Dixon, W. A. (2004). Problem-solvingappraisal and human adjustment: A review of 20 years of research usingthe Problem-Solving Inventory. Counseling Psychologist, 32, 344–428.
Hewitt, P. L., & Flett, G. L. (1991a). Dimensions of perfectionism in unipolardepression. Journal of Abnormal Psychology, 100, 98–101.
Hewitt, P. L., & Flett, G. L. (1991b). Perfectionism in the self and socialcontexts: Conceptualization, assessment, and association with psychopa-thology. Journal of Personality and Social Psychology, 60, 456–470.
Hewitt, P. L., & Flett, G. L. (1993). Dimensions of perfectionism, daily stress,and depression: A test of the specific vulnerability hypothesis. Journal ofAbnormal Psychology, 102, 58–65.
Hewitt, P. L., & Flett, G. L. (2002). Perfectionism and stress in psychopa-thology. In G. L. Flett & P. L. Hewitt (Eds.). Perfectionism: Theory,research, and treatment (pp. 255–284). Washington, DC: AmericanPsychological Association.
Hewitt, P. L., & Flett, G. L. (2004). The Multidimensional PerfectionismScale: Technical manual. Toronto, Ontario, Canada: Multi-HealthSystems.
Hewitt, P. L., Flett, G. L., & Ediger, E. (1995). Perfectionism traits andperfectionistic self-presentation in eating disorder attitudes, characteris-tics, and symptoms. International Journal of Eating Disorders, 18, 327–336.
Hewitt, P. L., Flett, G. L., & Ediger, E. (1996). Perfectionism and depression:Longitudinal assessment of a specific vulnerability hypothesis. Journal ofAbnormal Psychology, 105, 276–280.
Hewitt, P. L., Flett, G. L., & Endler, N. S. (1995). Perfectionism, coping, anddepression symptomatology in a clinical sample. Clinical Psychology andPsychotherapy, 2, 47–58.
Hewitt, P. L., Flett, G. L., Sherry, S. B., Habke, M., Parkin, M., Lam, R. W.,et al. (2003). The interpersonal expression of perfection: Perfectionisticself-presentation and psychological distress. Journal of Personality andSocial Psychology, 84, 1303–1325.
Hewitt, P. L., Flett, G. L., Turnbull-Donovan, W., & Mikail, S. (1991). TheMultidimensional Perfectionism Scale: Reliability, validity, and psycho-metric properties in psychiatric samples. Psychological Assessment: AJournal of Consulting and Clinical Psychology, 3, 464–468.
PERFECTIONISM AND SOCIAL PROBLEM-SOLVING ABILITY 2153
1
2
3
4
5
6
7
8
9
10
11
12
13
14
15
16
17
18
19
20
21
22
23
24
25
26
27
28
29
30
31
32
33
34
35
36
37
38
39
40
41
42
JOBNAME: No Job Name PAGE: 32 SESS: 17 OUTPUT: Tue Jun 8 20:09:19 2010 SUM: B8FC8524/v2503/blackwell/journals/jasp_v40_i8/jasp_653
Hewitt, P. L., Habke, A. M., Lee-Baggley, D. L., Sherry, S. B., & Flett, G. L.(2008). The impact of perfectionistic self-presentation on the cognitive,affective, and physiological experience of a clinical interview. Psychiatry,71, 93–122.
Horney, K. (1945). Our inner conflicts. New York: Norton.Horney, K. (1950). Neurosis and human growth: The struggle towards self-
realization. New York: Norton.Hu, L. T., & Bentler, P. M. (1998). Fit indices in covariance structure
modeling: Sensitivity and underparamaterized model misspecification.Psychological Methods, 3, 424–453.
Hu, L. T., & Bentler, P. M. (1999). Cutoff criteria for fit indexes in covariancestructure analysis: Conventional criteria versus new alternatives. Struc-tural Equation Modeling, 6, 1–55.
Hussian, R. A., & Lawrence, P. S. (1981). Social reinforcement of activityand problem-solving training in the treatment of depressed institutional-ized elderly patients. Cognitive Therapy and Research, 5, 57–69.
Kelloway, E. K. (1998). Using LISREL for structural equation modeling: Aresearcher’s guide. Newbury Park, CA: Sage.
Leary, M. R. (1996). Self-presentation: Impression management and interper-sonal behavior. Boulder, CO: Westview.
MacKinnon, D. P., Lockwood, C. M., Hoffman, J. M., West, S. G., &Sheets, V. (2002). A comparison of methods to test mediation and otherintervening variable effects. Psychological Methods, 7, 83–104.
Mallinckrodt, B., Abraham, T. W., Wei, M., & Russell, D. W. (2006).Advance in testing statistical significance of mediation effects. Journal ofCounseling Psychology, 53, 372–378.
Nezu, A. M. (1985). Differences in psychological distress between effectiveand ineffective problem solvers. Journal of Counseling Psychology, 32,135–138.
Nezu, A. M. (1986). Efficacy of a social problem-solving therapy approachfor unipolar depression. Journal of Consulting and Clinical Psychology, 54,196–202.
Nezu, A. M. (1987). A problem-solving formulation of depression: Literaturereview and proposal of a pluralistic model. Clinical Psychology Review, 7,121–144.
Nezu, A. M., Nezu, C. M., & Clark, M. A. (2008). Social problem solvingas a risk factor for depression. In K. S. Dobson & D. J. A. Dozois(Eds.), Risk factors in depression (pp. 263–286). New York: AcademicPress.
Nezu, A. M., Nezu, C. M., & Lombardo, E. (2004). Cognitive-behavioral caseformulation and treatment design: A problem-solving approach. New York:Springer.
2154 BESSER ET AL.
1
2
3
4
5
6
7
8
9
10
11
12
13
14
15
16
17
18
19
20
21
22
23
24
25
26
27
28
29
30
31
32
33
34
35
36
37
38
39
40
41
42
JOBNAME: No Job Name PAGE: 33 SESS: 17 OUTPUT: Tue Jun 8 20:09:19 2010 SUM: D18BB6DB/v2503/blackwell/journals/jasp_v40_i8/jasp_653
Nezu, A. M., & Ronan, G. F. (1985). Life stress, current problems, problemsolving, and depressive symptoms: An integrative model. Journal of Con-sulting and Clinical Psychology, 53, 693–697.
Nezu, A. M., & Ronan, G. F. (1988). Social problem-solving as a moderatorof stress-related depressive symptoms: A prospective analysis. Journal ofCounseling Psychology, 35, 134–138.
O’Connor, R. C., & O’Connor, D. B. (2003). Predicting hopelessness andpsychological distress: The role of perfectionism and coping. Journal ofCounseling Psychology, 50, 363–372.
Pliner, P., Chaiken, S., & Flett, G. L. (1990). Gender differences in concernwith body weight and physical appearance over the lifespan. Personalityand Social Psychology Bulletin, 16, 263–273.
Radloff, L. S. (1977). A self-report depression scale for research in thegeneral population. Applied Psychological Measurement, 1, 385–401.
Rice, K. G., Ashby, J. S., & Slaney, R. B. (1998). Self-esteem as a mediatorbetween perfectionism and depression: A structural equations analysis.Journal of Counseling Psychology, 45, 304–314.
Rudolph, S. G., Flett, G. L., & Hewitt, P. L. (2007). Perfectionism anddeficits in cognitive emotion regulation. Journal of Rational-Emotive andCognitive-Behavior Therapy, 25, 343–357.
Sherry, S. B., Hewitt, P. L., Flett, G. L., & Harvey, M. (2003). Perfectionismdimensions, perfectionistic attitudes, dependent attitudes, and depressionin psychiatric patients and university students. Journal of Counseling Psy-chology, 50, 373–386.
Sherry, S. B., Hewitt, P. L., Flett, G. L., Lee-Baggley, D. L., & Hall, P. A.(2007). Trait perfectionism and perfectionistic self-presentation in person-ality pathology. Personality and Individual Differences, 42, 477–490.
Sherry, S. B., Hewitt, P. L., Lee-Baggley, D. L., Flett, G. L., & Besser, A.(2004). Perfectionism and thoughts about having cosmetic surgery per-formed. Journal of Applied Biobehavioral Research, 9, 244–257.
Shrout, P. E., & Bolger, N. (2002). Mediation in experimental and nonex-perimental studies: New procedures and recommendations. PsychologicalMethods, 7, 422–445.
Slaney, R. B., Rice, K. G., & Ashby, J. S. (2002). A programmatic approachto measuring perfectionism: The Almost Perfect Scales. In G. L. Flett &P. L. Hewitt (Eds.), Perfectionism: Theory, research, and treatment (pp.63–88). Washington, DC: American Psychological Association.
Sobel, M. E. (1982). Asymptotic intervals for indirect effects in structuralequations models. In S. Leinhart (Ed.), Sociological methodology, 1982(pp. 290–312). San Francisco: Jossey-Bass.
Spence, S. H., Sheffield, J., & Donovan, C. (2002). Problem-solving orienta-tion and attributional style: Moderators of the impact of negative life
PERFECTIONISM AND SOCIAL PROBLEM-SOLVING ABILITY 2155
1
2
3
4
5
6
7
8
9
10
11
12
13
14
15
16
17
18
19
20
21
22
23
24
25
26
27
28
29
30
31
32
33
34
35
36
37
38
39
40
41
42
JOBNAME: No Job Name PAGE: 34 SESS: 17 OUTPUT: Tue Jun 8 20:09:19 2010 SUM: 2C6D8375/v2503/blackwell/journals/jasp_v40_i8/jasp_653
events on the development of depressive symptoms in adolescence?Journal of Clinical Child Psychology, 31, 219–229.
Spence, S. H., Sheffield, J. K., & Donovan, C. L. (2003). Preventing adoles-cent depression: An evaluation of the Problem-Solving for Life Program.Journal of Consulting and Clinical Psychology, 71, 3–13.
Spivack, G., Platt, J. J., & Shure, M. B. (1976). The problem-solving approachto adjustment. San Francisco: Jossey-Bass.
Steiger, J. H. (1980). Tests for comparing elements of a correlation matrix.Psychological Bulletin, 87, 245–251.
2156 BESSER ET AL.
1
2
3
4
5
6
7
8
9
JOBNAME: No Job Name PAGE: 35 SESS: 17 OUTPUT: Tue Jun 8 20:09:19 2010 SUM: 0779709E/v2503/blackwell/journals/jasp_v40_i8/jasp_653
Toppan Best-set Premedia LimitedJournal Code: JASP Proofreader: EmilyArticle No: 653 Delivery date: 8 June 2010Page Extent: 24