Embed Size (px)
Citation preview

Original article / Article original
Percutaneous treatment of sciatica caused by a herniated disc:
An exploratory study on the use of gaseous discography and
Discogel1 in 79 patients
Traitement des sciatiques par hernie discale : experience de la disco-manometrie aerique et duDiscogel1. A propos de 79 patients traites
M. de Seze a,*, L. Saliba b, J.-M. Mazaux a
a EA 4136 handicap et systeme nerveux, service de MPR, unite de medecine orthopedique, hopital Tastet-Girard, CHU de Bordeaux,
universite de Bordeaux Segalen, place Amelie-Raba-Leon, 33076 Bordeaux cedex, Franceb Pharmacie des dispositifs medicaux steriles, hopital Haut-Leveque, avenue de Magellan, 33604 Pessac cedex France
Received 13 March 2012; accepted 22 January 2013
Abstract
Objectives. – Sciatica is a common disease; between 13% and 40% of the general population will experience at least one episode of sciatica due to
spinal disc herniation and nerve root irritation. In some specialist centres, percutaneous intradiscal techniques can be applied as an intermediate
measure between conservative treatment and surgery, with a view to avoiding the adverse events associated with surgical discectomy. Discogel1 is
a percutaneously implanted medical device for the treatment of lumbar sciatica due to a herniated disc. We performed an open, prospective,
observational study in order to (a) determine whether the prior use of air disc manometry could limit the risk of nerve root irritation reportedly
associated with nucleolysis and administration of Discogel1 and (b) investigate the technique’s efficacy and safety.
Method. – A total of 79 Discogel1-treated patients were systematically reviewed. A nurse anaesthetist evaluated each patient’s pain levels during
the procedure itself. The therapist assessed the patient on inclusion and 8 weeks after the Discogel1 procedure. A third assessment was based on a
telephone interview (by an independent assessor) at least 4 months after the procedure.
Results. – Pain levels immediately after the Discogel1 procedure (1.7 � 2.0) were markedly lower than before the procedure (5.5 � 2.3). There
were no complications. Two months after Discogel1 administration, the initial pain level had fallen by an average of 74 � 34%. The outcome was
quite stable over time (mean follow-up: 8 months). At the end of the follow-up period, 60.7% of the patients were free of pain, 76% considered the
treatment outcome to be good or very good, 74% had returned to work and 76% would recommend the treatment to a friend.
Conclusion. – The favourable outcomes associated with the procedure should now be confirmed in a controlled trial.
# 2013 Published by Elsevier Masson SAS.
Keywords: Sciatica; Nerve root irritation; Percutaneous technique
Resume
Objectifs. – Entre 13 % et 40 % de la population generale presenteront au cours de leur vie un episode de sciatique par conflit disco-radiculaire.
Dans quelques centres specialises, les techniques percutanees intra-discales sont proposees. Leur objectif est de reduire les effets secondaires lies a
la discectomie. Le Discogel1 est un dispositif medical intra-discal utilise dans ce contexte pour securiser davantage la procedure therapeutique.
Nous avons conduit une etude prospective observationnelle sur une serie de 79 patients traites consecutivement : (a) pour observer la capacite d’une
disco-manometrie aerique a reduire le risque d’irritation radiculaire decrit lors des nucleolyses et de l’utilisation du Discogel1 (b) pour examiner
l’efficacite et la tolerance de ce dispositif.
Patients et methode. – Un suivi systematique a ete effectue chez les 79 premiers patients traites par Discogel1 dans notre centre. Une infirmiere
anesthesiste procedait aux evaluations de la douleur en periode perioperatoire. Ces donnees etaient completees par une evaluation clinique a huit
semaines et telephonique a plus de quatre mois.
Available online at
www.sciencedirect.com
Annals of Physical and Rehabilitation Medicine 56 (2013) 143–154
* Corresponding author.
E-mail address: [email protected] (M. de Seze).
1877-0657/$ – see front matter # 2013 Published by Elsevier Masson SAS.
http://dx.doi.org/10.1016/j.rehab.2013.01.006

Resultats. – Le suivi perioperatoire montre des intensites douloureuses moyennes qui diminuent rapidement (5,5 � 2,3 en preoperatoire,
1,7 � 2,0 en postoperatoire immediat) et l’absence de complications. La douleur a diminue de 74 � 34 % deux mois apres la procedure d’injection
du Discogel1. Au terme de l’evaluation, 60,7 % des patients sont asymptomatiques, 76 % considerent le traitement comme efficace, 74 %
retrouvent leurs activites professionnelles et 76 % recommanderaient ce traitement a des proches.
Conclusion. – Cette procedure et ces resultats meritent d’etre confirmes lors d’une etude controlee.
# 2013 Publie par Elsevier Masson SAS.
Mots cles : Lombosciatique ; Conflit disco-radiculaire ; Technique percutanee ; Nucleolyse ; Disco-manometrie aerique
M. de Seze et al. / Annals of Physical and Rehabilitation Medicine 56 (2013) 143–154144
1. English version
1.1. Introduction
Sciatica is a common condition; between 13% and 40% of
the general population will experience at least one episode of
sciatica due to nerve root irritation at some point in their life.
The annual incidence of this condition ranges from 1% to
5%, depending on the study in question [13]. A review of the
literature shows that the pain levels associated with sciatica
do not decrease over the long-term (5 years) – regardless of
whether the patient has been treated or not. The treatment
goals are therefore limited to relieving all the symptoms in
the short- to mid-term and reducing functional disability in
the mid- to long-term [29,30]. In fact, this is a rather
ambitious objective because it seeks to help patients to
maintain their professional activity and avoid periods of time
off work caused by pain.
At present, there is a hierarchy of treatments for sciatica
caused by nerve root irritation as a result of disc herniation; oral
treatments may be followed by the spinal infiltration of
corticoids, which in turn may be followed by surgery. In certain
specialist centres, percutaneous intradiscal techniques (nucleo-
lysis and nucleotomy) can be used after conservative treatment
and as an alternative to surgery. These developments are driven
by the need for techniques that are less aggressive than
discectomy; in sciatica, positive outcomes for discectomy are
often compromised by chronic, invalidating, lower back pain and
the occurrence of serious postoperative complications [24–
27,32,41,51,57]. Nucleolysis is defined as the injection of
compounds into the middle of the intervertebral disc, with a view
to dissolving all or part of the nucleus pulposus. Nucleotomy is
defined as the creation of a small cavity within the nucleus
pulposus by physical means, such as intradiscal needle aspiration
and laser or radiofrequency vaporization. These percutaneous
techniques are based on the same supposed principle of action; by
destroying or reducing the volume of the nucleus pulposus, they
tend to limit the nerve root irritation induced by compression of
the nucleus pulposus and its suffusion through the annulus
fibrosus [16,17]. In the 1970s, chemopapain was the first
substance to be used in disc nucleolysis. This is the only
percutaneous technique to have been validated by a sufficient
number of controlled studies [7,10,28,34,55]. Even though
chemopapain has now been withdrawn from the market,
it is still considered as the reference technique. Researchers
have since investigated a number of other options
[1,4,6,9,14,15,18,19,35,40,42,44,50,54,59]. In nucleolysis, the
risk of radiculitis (related to epidural leakage of the injected
product) is a constant concern [2,44,54]. Theron et al. have
reported several cases of radiculitis (with the occurrence of a
burning sensation) during the intradiscal injection of rectified
spirit [54]. With a view to limiting the risk of diffusion outside the
disc, a viscous gel containing ethylcellulose and tungsten
radiopaque suspended in 95% ethanol has been developed [54].
This gel has been approved as a percutaneously administered,
CE-marked implantable device (Discogel1) for the treatment of
lumbar sciatica caused by a herniated disc. According to the
product information sheet, Discogel1 has two mechanisms of
action. It combines a chemical effect (in which the rectified spirit
causes local necrosis of the nucleus pulposus) [44] with a
mechanical effect that may be related to the ethylcellulose’s
hydrophilic properties (via dehydration of the turgescent,
protruding disc).
The tungsten-containing gel can be visualized radiographi-
cally. Even when the injection is fluoroscopically guided,
leakage is always possible and, indeed, has been reported
during vertebroplasty with radiopaque cement [31]. Theron
et al. have reported cases of resurgent pain during injection,
although he did not specify the number of cases or the intensity
of the pain [54]. In fact, Theron et al. suggested that the pain
was related to the injection speed [44,54]. This type of painful
episode relates to distension of the disc, which can be revealed
by discography [60]. However, when the lumbar or radicular
pain occurs during the intradiscal injection of a product that is
possibly toxic for the nerve roots, it is difficult to rule our
epidural leakage if the disc’s renitence has not been checked
beforehand. In theory, discography could be used to check the
disc’s renitence a few days before the injection, although this
type of procedure would make the treatment more burdensome
and would probably increase the risk of infection. On the other
hand, intradiscal injection of contrast agent prior to injection of
Discogel1 appears to be poorly compatible in terms of the
limited disc volume and dilution of the subsequently injected
Discogel1. Furthermore, this procedure appears to be poorly
effective because it does not prevent the occurrence of benign
radiculitis in 3.7% of cases and severe neurological complica-
tions in 0.45% of nucleolysis procedures [2].
Given this context, we performed an open, observational
study designed to:
� test the ability of an air discography procedure to limit the
risks of epidural leakage;
� establish the efficacy and safety of Discogel1 injection by a
second medical team.

Rehabilitation Medicine 56 (2013) 143–154 145
1.2. Method
1.2.1. Study population
Patients were followed up as part of their routine medical
care, which was provided in our department in most cases. A
total of 79 consecutive patients met the inclusion criteria, i.e. an
indication for the treatment of lumbar sciatica via the
percutaneous injection of Discogel1.
1.2.2. Eligibility criteria
Inclusion criteria:
� lumbar sciatica due to nerve root irritation;
� onset at least 8 weeks previously;
� lack of response to optimal medical treatment;
� at least two epidural injections, including at least one under
fluoroscopic guidance.
Exclusion criteria:
� the presence of herniation with the extrusion or migration of
disc material;
� observation of markedly narrow pinched intervertebral discs
on CT or MRI.
1.2.3. Procedures and techniques
The procedures were performed with neurosedation during
day hospitalization in a day surgery service. Using a posterior-
lateral approach on the painful body side, an 18-gauge needle
(length: 10 cm) was introduced under fluoroscopic guidance.
This needle was used as a conduit for the disc puncture. The
disc was then punctured with a finer needle (22-gauge, 15 cm in
length), the tip of which was located in the centre of the
intervertebral disc (as checked by frontal and lateral fluoro-
scopy). In order to increase the procedure’s safety and efficacy
and check the disc’s renitence, filtered air discography was
performed with a 10 mL syringe and a bacterial filter. The disc’s
renitence was considered to be satisfactory if:
� resistance to injection was felt before 10 mL of air had been
injected;
� the syringe’s piston recoiled by at least two graduations once
finger pressure had been released.
Next, in accordance with Discogel1’s recommendations for
use, 0.7 mL of gel was injected slowly (0.1 mL every
30 seconds, under fluoroscopic guidance). Once the injection
had been completed, the needle’s inner shaft guide was put back
in place and the needle was left in position for 2 minutes (in
order to limit the risk of leakage at the time of removal).
The patients were monitored for 3 hours immediately after
the procedure, while the effects of neurosedation dissipated.
The patients left hospital with a prescription for a week’s
course of anti-inflammatories and analgesics. They were told
not to remain seated for long periods. As is generally the case
for surgical discectomy procedures, 6 weeks of sick leave
were always prescribed. However, the patients were told
M. de Seze et al. / Annals of Physical and
that they could return to work after 3 weeks if they felt able
to do so.
1.2.4. Efficacy criteria
In order to evaluate the percutaneous procedure, we first
assessed immediate perioperative pain. A nurse anaesthetist
surveyed overall perioperative and immediate postoperative
pain levels in the patients. The pain intensity was rated verbally
on a numeric scale from 0 (no pain) to 10 (the worst pain
imaginable). The pain was rated three times during the
procedure and then once an hour during the 3-hour monitoring
period in the recovery room.
In a second step, we assessed the change in pain levels over
time. In the first 66 patients treated, a nurse anaesthetist
evaluated overall pain levels by means of a telephone survey
one week after the injection. Furthermore, the physician
evaluated the intensity of lumbar and radicular pain during
consultations at inclusion and 8 weeks after the injection. A
third evaluation (a telephone survey) was performed by an
independent assessor at least 4 months after the procedure.
Again, the intensities of lumbar and radicular pain were rated
verbally on a scale of 0 (no pain) to 10 (the worst pain
imaginable). The patients were also invited to reply to the
following three questions:
� How would you now describe the treatment outcome: very
good, good, average or poor?
� Did the treatment enable you to resume your previous
professional activities?
� Would you recommend this treatment to a friend or family
member with the same problem?
1.3. Results
In all, 79 patients (40 women and 39 men; mean age:
40 � 12 years) were included in the study. On average, they had
been suffering from lumbar sciatica for 14 � 12 months. The
injected discs were L4-L5 in 40 patients, L5-S1 in 31 patients
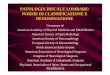
and at two sites in eight patients. Fig. 1 gives an illustrative
example of a procedure with an L5-S1 disc: disc puncture
(Fig. 1A), discography through air injection (Fig. 1B) and disc
opacification induced by injection of Discogel1 (Fig. 1C) into
the intradiscal air space. The air discography procedure
prompted the discovery of a non-renitent disc in two patients
(3.7%) and thus Discogel1 was not injected in these cases. The
change in perioperative pain over time is described in Table 1.
For the 79 treated patients as a whole, the mean perioperative
and immediate postoperative pain levels were significantly
lower than the mean preoperative level (P < 0.0001). During
the perioperative period, overall pain levels increased in five
patients (by 1 point in two patients and by 2 points in three
patients). None of these occurrences prompted a change in the
procedure. In the immediate postoperative period, three
patients reported an increase pain levels (by 1 point in one
patient, by 2 points in one patient and by 4 points in one
patient). Again, none of the temporary increases in pain
prompted a change in treatment. No sensory or motor

Fig. 1. The main steps in discographic verification. A. Puncture of the L5-S1
intervertebral disc. B. Discography with filtered air. C. Discography following
the injection of Discogel1.
M. de Seze et al. / Annals of Physical and Rehabilitation Medicine 56 (2013) 143–154146
impairments were reported during the immediate postoperative
period.
The evaluation one week after the procedure revealed a
significant decrease in the mean pain level, relative to the mean
preoperative level (P < 0.0001, Table 1). However, pain levels
increased in four patients (by 1 point in one patient, by 2 points
in two patients and by 4 points in one patient). None of these
increases in pain required treatment other than that planned in
the protocol.
Fifteen patients had undergone Discogel1 injection less
than 4 months before collection of the data presented here and
thus were not contacted by telephone following the clinical
evaluation 8 weeks after the procedure. The other 64 patients
were contacted by telephone after a mean (SD) time interval of
8.5 � 4.5 months (D255). The intensities of nerve root pain and
lumbar pain are reported in Table 2; both values fell
significantly between D0 and D60 (P < 0.0001) and between
D0 and D255. We did not observe a statistically significant
change in pain intensity between D60 and D255 (P > 0.05).
Two months after the Discogel1 administration, the mean
reduction in the initial pain level was 74 � 34%. Table 3 (giving
the percentage of patients as a function of the degree of pain
relief) shows that the results were relatively stable over the
8 months follow-up period. The variations observed during the
follow-up period highlighted a tendency for:
� initially unsatisfactory outcomes to worsen;
� further improvement in patients reporting more than a 50%
decrease in pain nerve root during the first 2 months.
Only three patients (3.7%) with extreme initial pain levels
reported the resurgence of pain during long-term follow-up. At
the end of the follow-up period, 60.7% of the patients no longer
experienced any pain, 76% considered that the treatment
outcome was good or very good (Table 4), 74% had returned to
work and 76% would have recommended the treatment to a
friend. During follow-up, none of the patients reported the
occurrence of sensory or motor impairments.
1.4. Discussion
Our study results emphasized the value of performing air
discography prior to percutaneous disc treatments and
confirmed the previously reported therapeutic value of
Discogel1 in the treatment of sciatica [53,54]. The air
discography procedure prompted the discovery of a non-
renitent disc in two cases (3.7%) and so the latter patients did
not receive an injection of Discogel1. No per- or post-
procedural pain suggestive of nerve root damage or epidural
leakage was observed and none of the Discogel1 injections had
to be abandoned once initiated. In the present series, 3.7% of
the injections were cancelled because of poor disc renitence.
This value corresponds very closely to the proportion of
patients with radiculitis reported during papain-based nucleo-
lysis [2]. This similarity suggests that our air discography
procedure enabled us to prevent this type of complication from
occurring.
For the five patients who reported the recrudescence of
preoperative pain, the observed disc renitence and the
preoperative aerogram suggested to us that the pain was
related to disc distension [60]; we were therefore able to

Table 1
Overall pain levels, measured on a verbal numeric scale.
Preoperative pain Perioperative pain Immediate postoperative pain After one week
Overall pain level (mean � standard deviation) 5.2 � 2.3 2.6 � 2.5a 1.7 � 2.0a 3.0 � 1.9a
0: no pain; 10: the worst pain imaginable.a A significant difference (P < 0.0001) relative to the preoperative pain level.
M. de Seze et al. / Annals of Physical and Rehabilitation Medicine 56 (2013) 143–154 147
continue the Discogel1 injection without fear of epidural
leakage. Only one patient reported lasting, resurgent pain in the
postoperative period (with a 2 point increase that prompted the
patient to rate the overall perioperative pain level as 10 out of
10). This extreme pain level was suggestive of radiculitis.
Nevertheless, other data collected during follow-up argued
against this diagnosis because no immediate change in
treatment was required and the check-up after a week revealed
a 50% pain decrease (relative to the initial pain level). Hence, in
this case, there was a dissociation between the clinical
presentation noted in the medical records and our evaluation.
It would have been interesting to study the pain’s characteristics
because discogenic pain is predominantly lumbar and radicular
pain is mainly felt in the legs (i.e. along the nerve path) [60].
Above all, this recrudescence of pain revealed the limitations of
Table 2
Pain levels, measured on a verbal numeric scale.
D0 (n = 79) D60 (n = 79) D255 (n = 64)
Nerve root pain 6.7 � 1.6 2.0 � 2.5a 2.7 � 3a
Lower back pain 6.6 � 2.1 2.7 � 2.5a 3.0 � 3a
0: no pain; 10: the worst pain imaginable.a A significant difference (P < 0.0001), relative to D0.
Table 4
The patients’ assessment of efficacy during telephone follow-up.
The patient’s assessment Percentage (n = 64)
Poor 17.7
Average 6.3
Good 12.6
Very good 63.2
Total 100
Table 3
Distribution of the patients as a function of the degree of pain relief (relative to
the initial level of nerve root pain).
Reduction in
pain (relative
to the initial level)
Percentage of patients
in each class after
2 months (n = 79)
Percentage of patients in
each class at the time of the
telephone follow-up (n = 64)
0% 12.6 16.4
1–24% 0 1.3
25–50% 6.3 6.3
51–75% 11.4 10.1
76–99% 11.4 5.0
100% 58.2 60.7
Total 100 100
our procedure for gathering perioperative data; we had chosen
to evaluate overall pain and thus simplify assessment of the
patients during each step in the therapeutic procedure.
Discogel1 has much the same advantages and constraints as
nucleolysis. However, according to the product information
supplied with Discogel1, its viscous, radiopaque nature
reduces the risks of epidural leakage enough to be able to
dispense with the discography that is generally recommended
before nucleolysis [2,44]. The absence of serious adverse
events in published series appears to confirm the basis of this
approach for avoiding serious neurological complications
[53,54]. However, the literature has also mentioned the
occurrence of radiculitis linked to Discogel1 leakage [54].
Nucleolysis is generally less feasible when epidural leakage
is discovered during discography with contrast agent. Hence, in
this context (including the injection of Discogel1), disc
manometry with filtered air appears to be able to limit both the
risk of epidural leakage and the need to inject contrast agent –
the use of which is likely of dilute the nucleolytic agent or delay
the injection until the excess intradiscal pressure subsides.
In the present series, 75% of the outcomes were judged to be
good or very good by the patients (Table 4). The corresponding
values reported by Theron et al. range from 82% to 91.4%
(overall average: 89%) [54]. Hence, in comparison, our results
appear to be less good. This difference may be due to two
parameters. Firstly, there were differences in the treatment
procedures. Theron et al. evaluated the effect of a Discogel1
injection combined with a local corticoid injection at a
posterior, epidural or foraminal site (chosen as a function of the
patient’s symptoms and the imaging data). We did not use a
local corticoid injection. Secondly, there were differences
between the two sets of treated patients. In our series, the
patients had been in pain for an average of 14 months; this is
longer than the period of 6 to 8 months post-onset during which
the relief of nerve root compression appears to be most effective
[36,37,56,58]. In contrast, patients in previously reported series
were eligible for Discogel1 injection after just 3 months of
nerve root pain.
The 75% reduction in pain reported by the patients treated
here agrees well with the literature data. In fact, the reported
efficacy of chemopapain ranged between 80% and 85%
[8,11,12,16,22,46], although the techniques intended to replace
chemopapain are associated with values nearer to 70%
[1,4,6,9,14,15,18–20,35,40,42,44,50,54,59].
The extent of pain relief in our series appears to be lower
than that reported in the surgical series [16]. This difference
may be due to the anatomy of the herniated disc treated in the
respective studies. In principle, percutaneous techniques are
only indicated for sciatica caused by a subligamentous

M. de Seze et al. / Annals of Physical and Reh148
herniated disc, which is known to be predictive of a poor
prognosis in terms of both progression of the sciatica and
responsiveness to treatment [5,36,56].
The creation of an intradiscal cavity (in order to decrease
nerve root compression) is often cited as the mechanism of
action of the percutaneous intradiscal techniques [42,43,50].
In that case, and given that the disc is a compressible
structure, how then can one imagine that resumption of a
weight-bearing posture would not lead to the rapid (or even
immediate) recurrence of pain? From a mechanical point of
view, the achievement of sustained relief would require the
destruction of all of the nucleus pulposus (as occurs
with chemopapain); this would lead to pinching of the
intervertebral disc [16]. In contrast, the new percutaneous
techniques are known not to induce narrowing of
the intervertebral disc [1,4,6,9,14,15,18,19,35,40,42,44,50,
54,59]. One must therefore envisage a mechanism capable of
sustainably reducing inflammatory reactions induced by
contact between extruded nucleus pulposus and the nerve
roots [3,23,33,38,39,45,49,52]. This is one of the putative
mechanisms of action in ozone-alcohol nucleolysis, which
appears to be capable of reducing the production of nucleus
pulposus and thus limiting its suffusion through the annulus
fibrosus [19,44]. However, the absence of an effect on the
permeability of the annulus fibrosus exposes the patient to
early relapses and creates the need for repeated injections
[6,15,59]. In our series, fewer than 5% of the patients
suffered a long-term relapse after a single injection. These
results are concordant with the relapse rates associated with
thermal (vaporization) techniques [9,17,18,20,48]. It has
been suggested that the sustained efficacy of thermal
techniques is related to heat-induced scarring of the annulus
fibrosus and thus a reduction of the latter’s permeability to
the nucleus pulposus [21,47]. Studies of the CT-guided
injection of Discogel1 suggest that viscous gel can migrate
towards the herniated breaches and thus reduce the local
porosity [53,54].
Hence, Discogel1’s efficacy appears to be based on two
mechanisms of action:
� the immediate effect of alcohol-based nucleolysis on the
nucleus pulposus;
� the longer-term sealing of the annulus fibrosus.
However, animal studies must now be performed in order to
better understand the device’s mechanisms of action. Our
ability to draw conclusions on the basis of our present results
was limited by:
� the absence of a topographic pain analysis during the
perioperative period (which would probably have enabled us
to better differentiate between discogenic pain and nerve root
pain);
� the absence of a control group (which would probably have
enabled us to better evaluate the air discography’s impact on
the occurrence of pain during administration and thus better
assess Discogel1’s therapeutic effect).
1.5. Conclusion
Our present results emphasize the increased safety and ease
of use associated with the performance of air discography prior
to nucleolysis via Discogel1 injection. The long-term follow-
up results (with a cure rate of 60.7%) are encouraging in terms
of efficacy and safety and thus encourage us to perform a
controlled study.
Disclosure of interest
The main author, Mathieu de Seze has a contract of advice
(council) with the laboratories Mertz Pharma France which
market the discogel in France.
None of the other authors has conflict of interest.
2. Version francaise
2.1. Introduction
La sciatique est une pathologie frequente. Entre 13 % et
40 % des personnes presenteront au moins un episode de
sciatique par conflit disco-radiculaire durant leur vie. L’inci-
dence annuelle correspondante est comprise entre 1 % et 5 %
[13]. La revue de la litterature medicale fait apparaıtre que
l’evolution douloureuse des sciatiques est la meme a long terme
(cinq ans), que les patients aient beneficies ou non d’un
traitement. L’objectif des traitements peut ainsi etre limite a
l’amelioration de l’ensemble des symptomes a court et a moyen
terme et a reduire les incapacites fonctionnelles a moyen et a
long terme [29,30]. Il s’agit d’un objectif en realite ambitieux
car il est de nature a eviter la desinsertion professionnelle des
patients, liee aux limitations d’activite induites par des periodes
douloureuses trop longues.
Il existe actuellement une hierarchie therapeutique qui passe
du traitement medical a la chirurgie en passant par les
infiltrations rachidiennes de corticoıdes. Dans certains centres
specialises les techniques percutanees intra-discales, nucleo-
lyses et nucleotomies, prennent leur place entre les soins
conservateurs et la chirurgie. Le developpement de ces
techniques repose sur la volonte de proposer des techniques
moins ‘agressives’ que la discectomie chirurgicale dont le
resultat positif sur la sciatique et souvent greve par des
lombalgies chroniques invalidantes et par la survenue de
complications graves [24–27,32,41,51,57]. Les nucleolyses
sont definies par l’injection de substances chimiques au sein du
disque intervertebral visant a dissoudre tout ou partie du
nucleus pulposus. Les nucleotomies sont definies par la
creation d’une cavitation partielle au sein du nucleus pulposus
par des moyens physiques telle que l’aspiration intra-discale ou
la vaporisation du nucleus par une onde laser ou par
radiofrequence. Ces techniques percutanees reposent sur le
meme principe d’action theorique : elles tendent, par la
reduction du volume du nucleus pulposus et par sa denatura-
tion, a limiter l’irritation des racines nerveuses induite par la
compression et les suffusions de nucleus pulposus au travers de
l’annulus discal [16,17]. La chemopapaıne fut la premiere
abilitation Medicine 56 (2013) 143–154

M. de Seze et al. / Annals of Physical and Rehabilitation Medicine 56 (2013) 143–154 149
substance utilisee pour realiser des nucleolyses discales dans
les annees 1970. C’est la seule technique percutanee qui a
beneficie d’un nombre suffisant d’etudes controlees pour
confirmer son interet [7,10,28,34,55]. Malgre l’arret de sa
commercialisation, elle est toujours consideree comme
technique de reference. Les praticiens ont cherche des solutions
alternatives nombreuses [1,4,6,9,14,15,18,19,35,40,42,44,
50,54,59]. En ce qui concerne les nucleolyses, le risque de
radiculite liee a une fuite epidurale du produit injecte est un
souci constant [2,44,54]. Theron et al. ont rapporte quelques cas
de radiculites lors d’injection intra-discale d’alcool a 95 %, se
traduisant par la survenue de sensations de brulures radiculaires
intenses pendant l’injection de solution alcoolique a 95 % [54].
Pour tenter de limiter les risques de diffusion extra-discale, il a
propose d’utiliser un gel compose d’ethyl-cellulose contenant
de l’alcool a 95 % et une suspension de tungstene radio-opaque
[54]. Il s’agit depuis 2008 d’un dispositif implantable
(Discogel1), mis en place par voie percutanee, qui a recu
une certification de conformite au marquage CE, propose pour
le traitement des lombosciatiques par hernie discale. Selon la
notice d’utilisation, le mode d’action decrit est double. Il
combine une action chimique induite par l’ethanol a 95 %, a
l’origine d’une necrose locale du nucleus pulposus [44], et une
action d’ordre mecanique qui serait liee aux proprietes
hydrophiles de l’ethyl-cellulose, via une deshydratation du
disque turgescent et protuberant.
Ce gel est visualisable radiologiquement grace a l’adjonc-
tion de tungstene en suspension. Cependant, malgre la
visualisation du produit au cours de l’injection, une fuite
demeure possible, comme cela a ete rapporte lors des
techniques de vertebroplasties utilisant des substances radio-
opaques [31]. Theron et al. rapportent des cas de recrudescence
douloureuse durant l’injection sans en preciser le nombre et
l’intensite [54]. Il met ces douleurs en relation avec la vitesse de
l’injection du produit [44,54]. Le processus douloureux evoque
est ici est une distension discale comme cela se voit lors des
discographies [60]. Cependant, lorsque des douleurs lombaires
ou radiculaires surviennent au cours de l’injection intra-discale
d’un produit possiblement toxique pour les racines nerveuses, il
est difficile d’exclure un processus de fuites epidurales si on ne
s’est pas assure de la continence discale avant l’injection intra-
discale. Dans ce but, la realisation d’une discographie quelques
jours auparavant est theoriquement envisageable mais cette
procedure alourdie la prise en charge therapeutique et en
augmentant le nombre d’abord discal augmente le risque
infectieux. En revanche, l’injection d’un produit de contraste
intra-discal avant l’injection du Discogel1 semble peu
compatible pour des raisons de volume discal limite et de
dilution du dispositif injecte. De plus, cette procedure s’avere
imparfaitement efficace puisqu’elle n’empeche pas la survenue
de radiculites benignes dans 3,7 % des cas et de complications
neurologiques severes dans environ 0,45 % des nucleolyses [2].
Dans ce cadre, nous avons propose une etude observation-
nelle ouverte dont l’objectif etait :
� de tester une procedure de discographie aerique pour limiter
les risques de fuites epidurales ;
� de renseigner l’efficacite et la tolerance du Discogel1 par une
deuxieme equipe.
2.2. Methode
2.2.1. Population
Le suivi des patients s’inscrivait dans un schema de soins
courants habituellement delivre au sein de notre equipe. Il a ete
propose consecutivement a 79 patients repondant aux indica-
tions des traitements des lombosciatiques par voie percutanee
de beneficier du Discogel1.
2.2.2. Criteres d’eligibilite
Criteres d’inclusion :
� patients souffrant de lombosciatique par conflit disco-
radiculaire ;
� depuis au moins huit semaines ;
� resistant au traitement medical bien conduit ;
� incluant au moins deux infiltrations epidurales, dont au moins
une realisee sous controle scopique.
Criteres de non-inclusion :
� presence d’une hernie exclue ou migree ;
� observation de disques intervertebraux tres pinces sur
l’imagerie TDM ou IRM.
2.2.3. Procedure et technique
Le geste etait realise au cours d’une journee d’hospitalisa-
tion, au sein d’un service de chirurgie ambulatoire, sous
neurosedation. Le disque traite etait aborde sous controle
scopique, a l’aiguille (18-G, 10 cm), par voie postero-laterale,
du cote de la douleur du patient. L’aiguille mise en place servait
de guide pour la ponction discale. Le disque etait alors
ponctionne au moyen d’une aiguille plus fine (22-G, 15 cm)
dont l’extremite etait situee au centre du disque intervertebral
par un controle scopique de face et de profil. Pour augmenter la
securite du geste sans risquer de diminuer l’efficacite du
dispositif, une discographie a l’air filtre etait realisee avec une
seringue de 10 mL et un filtre bacterien, afin de s’assurer de la
renitence du disque. La renitence discale etait jugee
satisfaisante si :
� une sensation de resistance a l’injection survenait avant les
10 mL de volume de la seringue ;
� au relachement de la pression manuelle, le piston de la
seringue revenait d’au moins deux graduations.
Puis, selon les recommandations du Discogel1, 0,7 mL du
dispositif etait injecte lentement (0,1 mL toutes les 30 secondes
sous controle scopique). A la fin de l’injection, le guide de
l’aiguille etait remis en place et l’aiguille etait laissee en
position pendant deux minutes, pour limiter le risque de fuite au
moment du retrait.
Apres l’intervention, les patients etaient surveilles trois
heures, le temps que les effets de la neurosedation se dissipent.

Fig. 1. Principales etapes du controle discographique. A. Ponction du disque
intervertebral L5-S1. B. Discographie a l’air filtre. C. Discographie secondaire a
l’injection de Discogel1.
M. de Seze et al. / Annals of Physical and Rehabilitation Medicine 56 (2013) 143–154150
Les patients sortaient avec une prescription d’anti-inflamma-
toire et d’antalgique pour huit jours. Ils avaient pour consigne
d’eviter les stations assises prolongees. Par mesure systema-
tique et de maniere similaire aux procedures de discectomie
chirurgicale, un arret de travail etait prescrit pour une duree de
six semaines mais les patients etaient informes de la possibilite
de reprise professionnelle au bout de trois semaines s’ils s’en
sentaient capables.
2.2.4. Criteres de jugement
Pour evaluer la procedure percutanee nous nous sommes en
premier lieu interesse a la douleur perioperatoire immediate.
L’ensemble des patients a beneficie d’une evaluation globale de
la douleur ressentie en peroperatoire et en postoperatoire
immediat par l’infirmiere anesthesiste. L’intensite de la douleur
etait evaluee au moyen d’une echelle verbale numerique
(0 = pas de douleur ; 10 = douleur maximale imaginable). La
question etait posee trois fois pendant l’intervention et une fois
par heure lors des trois heures de surveillance en salle de reveil.
En second lieu nous avons suivi l’evolution des douleurs.
Chez les 66 premiers patients injectes, une evaluation de la
douleur globale etait realisee, par une infirmiere anesthesiste,
par appel telephonique au huitieme jour apres l’intervention.
Deux evaluations portant sur l’intensite des douleurs lombaire
et radiculaires etaient faites par le therapeute au cours de
consultation, le jour de l’inclusion et huit semaines apres le
geste. Une troisieme evaluation etait effectuee par remplissage
d’un questionnaire telephonique, soumis au moins quatre mois
apres le geste par un evaluateur independant. Les parametres
alors evalues etaient les intensites des douleurs lombaires et
radiculaires, recueillies au moyen d’une echelle verbale
numerique (0 = pas de douleur, 10 = douleur maximale
imaginable). Les patients repondaient egalement aux trois
questions suivantes :
� Avec le recul que vous avez, comment qualifieriez-vous le
resultat de ce traitement : tres bon, bon, moyen, mauvais ?
� Ce traitement vous a-t-il permis de reprendre votre vie
professionnelle anterieure ?
� Est-ce que vous recommanderiez ce traitement a un ami ou
quelqu’un de votre entourage proche qui aurait le meme
probleme ?
2.3. Resultats
Soixante dix-neuf patients (40 femmes et 39 hommes, age
moyen 40 � 12 ans) ont ete inclus. Ils souffraient en moyenne
depuis 14 � 12 mois. Les disques injectes etaient aux niveaux
L4-L5 chez 40 patients, L5-S1 chez 31 patients et aux deux
niveaux chez huit patients. La Fig. 1 montre un exemple de
procedure sur le disque L5-S1 : la ponction du disque (Fig. 1A),
l’aerogramme discal obtenu par l’injection aerique (Fig. 1B) et
l’opacification discale induite par le Discogel1 en place
(Fig. 1C) venant prendre la place de l’aerogramme discal. La
procedure de discographie aerique a amene a la decouverte
d’un disque non renitent chez deux patients (3,7 %), chez
lesquels le Discogel1 n’a donc pas ete injecte. L’evolution des
douleurs perioperatoires est rapportee dans le Tableau 1. Parmi
les 79 patients injectes, les intensites moyennes des douleurs
peroperatoires et postoperatoires immediates diminuaient de
maniere significative par rapport a l’intensite moyenne de la

Tableau 1
Intensite douloureuse globale mesuree par echelle verbale numerique.
Preoperatoire Peroperatoire Postoperatoire immediat j8
Intensite douloureuse globale (moyenne � ecart-type) 5,2 � 2,3 2,6 � 2,5a 1,7 � 2,0a 3,0 � 1,9a
0 : pas de douleur ; 10 : douleur maximale imaginable.a Difference significative avec un p < 0,0001 par rapport a la douleur preoperatoire.
M. de Seze et al. / Annals of Physical and Rehabilitation Medicine 56 (2013) 143–154 151
douleur preoperatoire ( p < 0,0001). Durant la periode per-
operatoire, la douleur globale augmentait chez cinq patients
(1 point chez deux patients et 2 points chez trois patients).
Aucune de ces douleurs n’a necessite un ajustement de la
procedure. En periode, postoperatoire immediate, trois patients
ont rapporte une augmentation de leur douleur (1 point chez un
patient, 2 points chez un patient et 4 points chez un patient).
Aucune des ces augmentations douloureuses temporaires n’a
necessite un ajustement therapeutique. Aucun deficit sensitif ou
moteur n’a ete rapporte pendant cette periode perioperatoire
immediate.
L’evaluation huit jours apres l’intervention montrait une
diminution significative de la moyenne de l’intensite doulour-
euse par rapport a celle rapportee en preoperatoire ( p < 0,0001,
Tableau 1). La douleur augmentait neanmoins chez
Tableau 2
Valeurs des intensites douloureuses mesuree par echelle verbale numerique.
j0 (n = 79) j60 (n = 79) j255 (n = 64)
Radiculalgie 6,7 � 1,6 2,0 � 2,5a 2,7 � 3a
Lombalgie 6,6 � 2,1 2,7 � 2,5a 3,0 � 3a
0 : pas de douleur ; 10 : douleur maximale imaginable.a Difference significative avec un p < 0,0001 par rapport a J0
Tableau 4
Estimation de l’efficacite par les patients lors du suivi telephonique.
Estimation du patient Pourcentage (n = 64)
Mauvaise 17,7
Moyenne 6,3
Bonne 12,6
Tres bonne 63,2
Total 100
Tableau 3
Repartition des patients par classe de reduction de la douleur radiculaire initiale.
Classes de reduction de
la douleur par rapport a
l’intensite initiale
Pourcentage de patients
par classe a 2 mois
d’evolution (n = 79)
Pourcentage de patients
par classe lors du suivi
telephonique (n = 64)
0 % 12,6 16,4
1–24 % 0 1,3
25–50 % 6,3 6,3
51–75 % 11,4 10,1
76–99 % 11,4 5,0
100 % 58,2 60,7
Total 100 100
quatre patients (1 point chez un patient, 2 points chez deux
patients, 4 points chez un patient). Aucune de ces augmenta-
tions douloureuses n’a necessite une prise en charge autre que
celle prevue dans le protocole (confere procedure et methode).
Quinze patients avaient beneficie du Discogel1 moins de
quatre mois avant le recueil des donnees presentees, et n’ont
donc pas ete recontactes par telephone apres l’evaluation
clinique a huit semaines postoperatoires. Les 64 autres patients
ont donc ete contactes par telephone avec un delai moyen de
8,5 � 4,5 mois (j255). L’intensite des douleurs radiculaires et
lombaires est rapportee dans le Tableau 2. L’intensite des
douleurs radiculaires et lombaires diminuait significativement
entre j0 et j60 ( p < 0,0001) ainsi qu’entre j0 et j255. On ne
constatait aucune difference statistiquement significative dans
l’intensite des douleurs entre j60 et j255 ( p > 0,05). Deux mois
apres l’administration du Discogel1, il existait une reduction
de la douleur initiale moyenne de 74 � 34 %. Le Tableau 3,
exprime en pourcentage de patients par classe de soulagement,
montre une relative stabilite des resultats dans le temps avec un
suivi moyen de huit mois. Les variations observees lors du suivi
soulignent une tendance a :
� la deterioration des resultats initialement insuffisants ;
� l’amelioration des patients rapportant une diminution de plus
de 50 % de la douleur radiculaire dans les deux premiers
mois.
Seulement trois patients (3,7 %) initialement completement
soulages declaraient une recidive lors du suivi prolonge. Au
terme du suivi, 60,7 % des patients ne presentaient plus aucune
douleur, 76 % jugeaient l’effet du traitement bon ou tres bon
(Tableau 4), 74 % avaient repris leurs activites professionnelles
et 76 % conseilleraient ce traitement a un ami. Au cours du
suivi, aucun patient n’a signale la survenue d’un deficit sensitif
ou moteur.
2.4. Discussion
Les resultats de cette etude confirment l’interet de la
pratique d’une discographie aerique lors des techniques
percutanees et l’interet therapeutique precedemment rapporte
du Discogel1 dans le traitement des sciatiques [53,54]. La
procedure de discographie aerique a amene a la decouverte
d’un disque non renitent chez deux patients (3,7 %), chez
lesquels le Discogel1 n’a donc pas ete injecte. Aucune douleur
per- ou post-procedural pouvant faire evoquer une souffrance
radiculaire liee a une fuite epidurale n’a ete rapportee et aucune
injection n’a ete arretee precocement. Dans notre serie, le taux

M. de Seze et al. / Annals of Physical and Rehabilitation Medicine 56 (2013) 143–154152
d’eviction des injections en raison de l’incontinence discale est
de 3,7 %. Il correspond exactement au taux de radiculites
rapporte lors de la realisation des nucleolyses a la papaıne [2].
Cette similitude suggere que notre procedure de discographie
aerique a permis d’eviter la survenue de ce genre de
complications.
Parmi les cinq patients qui rapportaient une recrudescence
douloureuse preoperatoire, la renitence discale et l’aero-
gramme visualise precedemment nous ont permis de rapporter
ces douleurs a la distension discale [60] et de continuer le geste
sans redouter de fuite epidurale. Un seul d’entre eux rapportait
une persistance de la recrudescence douloureuse en periode
postoperatoire qui augmentait encore de 2 points, l’amenant a
evaluer la douleur globale peroperatoire a 10/10. L’intensite de
cette douleur peut faire craindre une radiculite. Neanmoins, les
elements du suivi venaient s’opposer a ce diagnostic puisque
aucune adaptation therapeutique immediate n’a ete necessaire
et le suivi a huit jours montrait une diminution de 50 % de
l’intensite douloureuse par rapport a la douleur initiale. Il y a
donc dans ce cas une dissociation entre la presentation clinique
rapportee dans le dossier medical et l’evaluation que nous
avons recueillie. Un rapport specifique du type de douleur
aurait permis de mieux differencier une douleur d’origine
discogenique montrant des douleurs predominant au niveau
lombaire d’une origine radiculaire predominant sur le trajet
nerveux [60]. Cette recrudescence revele surtout les limites de
notre recueil de donnees perioperatoire, pour lequel nous avons
utilise une evaluation de la douleur globale afin de faciliter
l’interrogation du patient durant toutes les etapes de la
procedure therapeutique.
Le Discogel1 presente des avantages et contraintes
similaires a celles de la nucleolyse. Mais, selon la notice
d’utilisation du Discogel1 son caractere radio-opaque et
visqueux limite suffisamment les risques de fuites epidurales
pour pouvoir, lors de son administration intra-discale, se passer
de la discographie habituellement recommandee avant les
nucleolyses [2,44]. L’absence d’effet indesirable grave rapporte
lors des series publiees semble confirmer le bien fonde de cette
attitude pour eviter les complications neurologiques graves
[53,54]. Cependant, au cours des etudes precedentes, il a ete
rapporte la possibilite de radiculites liees a des fuites de
Discogel1 [54].
La faisabilite des nucleolyses est principalement reduite par
la presence d’une fuite epidurale decouverte lors d’une
discographie au produit de contraste. Ainsi, dans ce contexte,
incluant l’injection de Discogel1, une disco-manometrie a l’air
filtre semble pouvoir limiter le risque de fuite epidurale, tout en
limitant le recours a l’injection d’un produit de contraste, dont
l’utilisation est susceptible de diluer l’effet de l’agent chimique
de la nucleolyse ou de differer l’injection du dispositif a cause
de l’hyperpression discale induite.
Dans notre serie, le pourcentage de bons et tres bons
resultats est de 75 % (Tableau 4). Le taux de bons a tres bons
resultats rapporte par Theron varie de 82 % a 91,4 % (moyenne
globale = 89 %) [54]. Par comparaison, les resultats de notre
serie semblent moins bons. Cette difference est peut-etre
expliquee par deux phenomenes. En premier lieu, la difference
observee peut etre induite par des differences de procedures
therapeutiques. En effet Theron et al. ont evalue l’effet de
l’injection du Discogel1 en association avec une injection
locale de corticoıde dont le site dependait de la symptoma-
tologie et de l’imagerie (articulaire posterieure, epidurale ou
foraminale) que nous n’avons pas utilisees. En second lieu,
cette difference peut provenir d’une difference de population
traitee dans les deux series. En effet, dans notre serie la duree
moyenne de douleur etait de 14 mois et depassait largement la
periode de six a huit mois au-dela de laquelle l’efficacite d’une
levee de compression radiculaire semble diminuer
[36,37,56,58], tandis que dans la serie precedente, la periode
de souffrance radiculaire necessaire pour beneficier du
Discogel1 etait egale a trois mois.
Le taux de soulagement de 75 % des patients traites decrit ici
semble s’accorder avec l’ensemble des donnees de la
litterature. En effet, l’efficacite rapportee de la chemopapaıne
oscillait entre 80 et 85 % [8,11,12,16,22,46], mais celles des
techniques qui visent a la remplacer se rapprochent de 70 %
[1,4,6,9,14,15,18–20,35,40,42,44,50,54,59].
Le taux de soulagement dans notre serie semble inferieur a
celui rapporte dans les series chirurgicales [16]. L’anatomie des
hernies discales traitees peut expliquer ces differences de
resultats. En effet, le champ d’application des techniques
percutanees est, par principe, reserve aux sciatiques par hernies
discales sous-ligamentaires dont on sait qu’elles constituent un
facteur de mauvais pronostic tant pour l’evolution naturelle de
la sciatique que pour leur reponse aux traitements [5,36,56].
La creation d’une cavite discale propre a diminuer la
compression radiculaire est souvent evoquee comme meca-
nisme d’action des techniques percutanees intra-discales
[42,43,50]. Dans ce cas, le disque etant une structure
compressible, comment ne pas imaginer que la remise en
charge du patient entraınerait une recidive douloureuse
rapide voir immediate ? D’un point de vue mecanique, pour
obtenir un soulagent durable, il faudrait detruire l’ensemble du
nucleus pulposus ce qui, a l’instar de la chemopapaıne, induirait
un pincement du disque intervertebral [16]. Hors a l’inverse, les
nouvelles techniques percutanees sont connues pour ne pas
entraıner de pincement discal [1,4,6,9,14,15,18,19,35,40,42,
44,50,54,59]. Il faut donc retenir un mecanisme capable de
reduire de maniere durable les reactions inflammatoires
induites par les suffusions du nucleus pulposus au contact
des racines nerveuses [3,23,33,38,39,45,49,52]. C’est l’un des
mecanismes d’action retenu pour les nucleolyses a l’ozone et a
l’alcool, qui semblent capables de reduire la production de
nucleus pulposus et de limiter ainsi sa suffusion au travers de
l’annulus fibrosus [19,44]. Cependant, l’absence de systeme
agissant sur la permeabilite de l’annulus fibrosus expose a des
recidives precoces et induit la necessite de pratiquer des
injections repetees [6,15,59]. Dans notre serie, les recidives a
long terme sont inferieures a 5 % apres une injection unique.
Ces resultats paraissent en accord avec les taux de recidives
observees dans les techniques thermiques [9,17,18,20,48].
L’effet durable des techniques thermiques a ete mis en relation
avec des modifications cicatricielles de l’annulus fibrosus,
induites par l’elevation temporaire de temperature, qui le

M. de Seze et al. / Annals of Physical and Rehabilitation Medicine 56 (2013) 143–154 153
rendraient plus etanche vis-a-vis du nucleus pulposus [21,47].
Les suivis scannographiques des injections de Discogel1
suggerent la presence d’une migration du dispositif visqueux
vers les breches herniaires qui reduirait leur porosite [53,54].
Ainsi, deux mecanismes d’action semblent pouvoir etre
retenus pour expliquer l’effet du Discogel1 :
� une action immediate de nucleolyse alcoolique sur le nucleus
pulposus ;
� une action differee de colmatage de l’annulus fibrosus.
Des etudes experimentales doivent cependant etre menees
pour mieux comprendre les mecanismes d’action de ce
dispositif.
Les conclusions que nous pouvons tirer a partir de cette
etude sont limitees par :
� l’absence d’analyse de la topographie douloureuse en periode
perioperatoire (qui aurait permis de mieux differencier les
douleurs discogeniques d’eventuelles douleurs d’origine
radiculaire) ;
� l’absence de groupe temoin dont la presence aurait permis de
mieux evaluer l’impact de la discographie aerique sur la
survenue de douleurs procedurales et de mieux evaluer l’effet
therapeutique du Discogel1.
2.5. Conclusion
Ces resultats soulignent l’aspect securisant et pratique de la
realisation d’une discographie aerique avant la realisation
d’une nucleolyse incluant l’injection de Discogel1. Le suivi
prolonge, montrant un taux de guerison de 60,7 % des patients,
est encourageant sur le plan de l’efficacite, rassurant sur le plan
de la tolerance, et nous incitent a proposer une etude controlee.
Declaration d’interets
L’auteur principal, Mathieu de Seze, a un contrat de conseil
aupres des laboratoires Mertz Pharma France qui commercia-
lisent le Discogel1 en France.
Aucun des autres auteurs n’a de conflit d’interet.
References
[1] Andreula CF, Simonetti L, De Santis F, Agati R, Ricci R, Leonardi M.
Minimally invasive oxygen-ozone therapy for lumbar disk herniation.
AJNR Am J Neuroradiol 2003;24:996–1000.
[2] Bouillet R. Treatment of sciatica. A comparative survey of complications
of surgical treatment and nucleolysis with chymopapain. Clin Orthop
Relat Res 1990;251:144–1452.
[3] Brisby H, Balague F, Schafer D, Sheikhzadeh A, Lekman A, Nordin M,
et al. Glycosphingolipid antibodies in serum in patients with sciatica.
Spine 2002;27:380–6.
[4] Buric J, Molino Lova R. Ozone chemonucleolysis in non-contained
lumbar disc herniations: a pilot study with 12 months follow-up. Acta
Neurochir Suppl 2005;92:93–7.
[5] Bush K, Cowan N, Katz DE, Gishen P. The natural history of sciatica
associated with disc pathology. A prospective study with clinical and
independent radiologic follow-up. Spine 1992;17:1205–12.
[6] Clavo B, Robaina F, Kovacs F, Urrutia GR, Gazzeri R, Galarza M, et al.
Fulminating septicemia secondary to oxygen-ozone therapy for lumbar
disc herniation: case report. Spine 2007;32:E121–3 [Spine 2007;32:2036;
author reply 7].
[7] Crawshaw C, Frazer AM, Merriam WF, Mulholland RC, Webb JK. A
comparison of surgery and chemonucleolysis in the treatment of sciatica.
A prospective randomized trial. Spine 1984;9:195–8.
[8] Dabezies EJ, Langford K, Morris J, Shields CB, Wilkinson HA. Safety and
efficacy of chymopapain (Discase) in the treatment of sciatica due to a
herniated nucleus pulposus. Results of a randomized, double-blind study.
Spine 1988;13:561–5.
[9] Dupuy R, Lavignolle B, Vignes R. Traitement de la lombosciatique par
nucleotomie laser : a propos de 56 patients suivis 12 mois. Rachis
2003;15:321–7.
[10] Ejeskar A, Nachemson A, Herberts P, Lysell E, Andersson G, Irstam L,
et al. Surgery versus chemonucleolysis for herniated lumbar discs. A
prospective study with random assignment. Clin Orthop Relat Res
1983;174:236–42.
[11] Feldman J, Menkes CJ, Pallardy G, Chevrot A, Horreard P, Zenny JC, et al.
Double-blind study of the treatment of disc lumbosciatica by chemonu-
cleolysis. Rev Rhum Mal Osteoartic 1986;53:147–52.
[12] Fraser RD. Chymopapain for the treatment of intervertebral disc hernia-
tion. A preliminary report of a double-blind study. Spine 1982;7:608–12.
[13] Frymoyer JW. Back pain and sciatica. N Engl J Med 1988;318:291–300.
[14] Gangi A, Dietemann JL, Ide C, Brunner P, Klinkert A, Warter JM. Percuta-
neous laser disk decompression under CT and fluoroscopic guidance: indica-
tions, technique, and clinical experience. Radiographics 1996;16:89–96.
[15] Gazzeri R, Galarza M, Neroni M, Esposito S, Alfieri A. Fulminating
septicemia secondary to oxygen-ozone therapy for lumbar disc herniation:
case report. Spine 2007;32:E121–3.
[16] Gibson JN, Waddell G. Surgery for degenerative lumbar spondylosis:
updated Cochrane Review. Spine 2005;30:2312–20.
[17] Goupille P, Mulleman D, Mammou S, Griffoul I, Valat JP. Percutaneous
laser disc decompression for the treatment of lumbar disc herniation: a
review. Semin Arthritis Rheum 2007;37:20–30.
[18] Gronemeyer DH, Buschkamp H, Braun M, Schirp S, Weinsheimer PA,
Gevargez A. Image-guided percutaneous laser disk decompression for
herniated lumbar disks: a 4-year follow-up in 200 patients. J Clin Laser
Med Surg 2003;21:131–8.
[19] Han HJ, Kim JY, Jang HY, Lee B, Yoon JH, Jang SK, et al. Fluoroscopic-
guided intradiscal oxygen-ozone injection therapy for thoracolumbar
intervertebral disc herniations in dogs. In Vivo 2007;21:609–13.
[20] HAS : Haute Autorite de sante. Destruction d’un disque intervertebral par
laser (Nucleotomie) par voie transcutanee avec guidage radiologique. In:
professionnels Seeda, ed. Paris; 2005:1–35.
[21] Hecht P, Hayashi K, Cooley AJ, Lu Y, Fanton GS, Thabit 3rd G, et al. The
thermal effect of monopolar radiofrequency energy on the properties of
joint capsule. An in vivo histologic study using a sheep model. Am J
Sports Med 1998;26:808–14.
[22] Javid MJ, Nordby EJ, Ford LT, Hejna WJ, Whisler WW, Burton C, et al.
Safety and efficacy of chymopapain (Chymodiactin) in herniated nucleus
pulposus with sciatica. Results of a randomized, double-blind study.
JAMA 1983;249:2489–94.
[23] Kawaguchi S, Yamashita T, Katahira G, Yokozawa H, Torigoe T, Sato N.
Chemokine profile of herniated intervertebral discs infiltrated with mono-
cytes and macrophages. Spine 2002;27:1511–6.
[24] Kawaguchi Y, Matsui H, Gejo R, Tsuji H. Preventive measures of back
muscle injury after posterior lumbar spine surgery in rats. Spine
1998;23:2282–7 [discussion 8].
[25] Kawaguchi Y, Matsui H, Tsuji H. Back muscle injury after posterior
lumbar spine surgery. Part 1: histologic and histochemical analyses in rats.
Spine 1994;19:2590–7.
[26] Kawaguchi Y, Matsui H, Tsuji H. Back muscle injury after posterior
lumbar spine surgery. Part 2: histologic and histochemical analyses in
humans. Spine 1994;19:2598–602.
[27] Kawaguchi Y, Matsui H, Tsuji H. Back muscle injury after posterior
lumbar spine surgery. A histologic and enzymatic analysis. Spine
1996;21:941–4.

M. de Seze et al. / Annals of Physical and Rehabilitation Medicine 56 (2013) 143–154154
[28] Lavignolle B, Vital JM, Baulny D, Grenier F, Castagnera L. Comparative
study of surgery and chemonucleolysis in the treatment of sciatica caused
by a herniated disk. Acta Orthop Belg 1987;53:244–9.
[29] Legrand E, Bouvard B, Audran M, Fournier D, Valat JP. Sciatica from disk
herniation: medical treatment or surgery? Joint Bone Spine 2007;74:
530–5.
[30] Luijsterburg PA, Verhagen AP, Ostelo RW, van Os TA, Peul WC, Koes
BW. Effectiveness of conservative treatments for the lumbosacral radicu-
lar syndrome: a systematic review. Eur Spine J 2007;16:881–99.
[31] Martin DJ, Rad AE, Kallmes DF. Prevalence of extravertebral cement
leakage after vertebroplasty: procedural documentation versus CT detec-
tion. Acta Radiol 2012;53:569–72.
[32] Mayer TG, Vanharanta H, Gatchel RJ, Mooney V, Barnes D, Judge L, et al.
Comparison of CT scan muscle measurements and isokinetic trunk
strength in postoperative patients. Spine 1989;14:33–6.
[33] McCarron RF, Wimpee MW, Hudkins PG, Laros GS. The inflammatory
effect of nucleus pulposus. A possible element in the pathogenesis of low
back pain. Spine 1987;12:760–4.
[34] Muralikuttan KP, Hamilton A, Kernohan WG, Mollan RA, Adair IV. A
prospective randomized trial of chemonucleolysis and conventional disc
surgery in single level lumbar disc herniation. Spine 1992;17:381–7.
[35] Muto M, Andreula C, Leonardi M. Treatment of herniated lumbar disc by
intradiscal and intraforaminal oxygen-ozone (O2-O3) injection. J Neuror-
adiol 2004;31:183–9.
[36] Ng LC, Sell P. Predictive value of the duration of sciatica for lumbar
discectomy. A prospective cohort study. J Bone Joint Surg Br
2004;86:546–9.
[37] Nygaard OP, Kloster R, Solberg T. Duration of leg pain as a predictor of
outcome after surgery for lumbar disc herniation: a prospective cohort
study with 1-year follow-up. J Neurosurg 2000;92:131–4.
[38] Nygaard OP, Mellgren SI, Osterud B. The inflammatory properties of
contained and non-contained lumbar disc herniation. Spine
1997;22:2484–8.
[39] Onozawa T, Atsuta Y, Sato M, Ikawa M, Tsunekawa H, Feng X. Nitric
oxide induced ectopic firing in a lumbar nerve root with cauda equina
compression. Clin Orthop Relat Res 2003;408:167–73.
[40] Paradiso R, Alexandre A. The different outcomes of patients with disc
herniation treated either by microdiscectomy, or by intradiscal ozone
injection. Acta Neurochir Suppl 2005;92:139–42.
[41] Rantanen J, Hurme M, Falck B, Alaranta H, Nykvist F, Lehto M, et al. The
lumbar multifidus muscle five years after surgery for a lumbar interverte-
bral disc herniation. Spine 1993;18:568–74.
[42] Revel M. Value of percutaneous treatments of the lumbar spine in back and
nerve root pain. Semin Musculoskelet Radiol 1997;1:349–54.
[43] Revel M, Payan C, Vallee C, Laredo JD, Lassale B, Roux C, et al.
Automated percutaneous lumbar discectomy versus chemonucleolysis in
the treatment of sciatica. A randomized multicenter trial. Spine
1993;18:1–7.
[44] Riquelme C, Musacchio M, Mont’Alverne F, Tournade A. Chemonucleo-
lysis of lumbar disc herniation with ethanol. J Neuroradiol 2001;28:219–29.
[45] Saal JS, Franson RC, Dobrow R, Saal JA, White AH, Goldthwaite N. High
levels of inflammatory phospholipase A2 activity in lumbar disc hernia-
tions. Spine 1990;15:674–8.
[46] Schwetschenau PR, Ramirez A, Johnston J, Wiggs C, Martins AN.
Double-blind evaluation of intradiscal chymopapain for herniated lumbar
discs. Early results. J Neurosurg 1976;45:622–7.
[47] Shah RV, Lutz GE, Lee J, Doty SB, Rodeo S. Intradiskal electrothermal
therapy: a preliminary histologic study. Arch Phys Med Rehabil
2001;82:1230–7.
[48] Singh V, Manchikanti L, Benyamin RM, Helm S, Hirsch JA. Percutaneous
lumbar laser disc decompression: a systematic review of current evidence.
Pain Physician 2009;12:573–88.
[49] Stafford MA, Peng P, Hill DA. Sciatica: a review of history, epidemiology,
pathogenesis, and the role of epidural steroid injection in management. Br
J Anaesth 2007;99:461–73.
[50] Stevenson RC, McCabe CJ, Findlay AM. An economic evaluation of a
clinical trial to compare automated percutaneous lumbar discectomy with
microdiscectomy in the treatment of contained lumbar disc herniation.
Spine 1995;20:739–42.
[51] Styf JR, Willen J. The effects of external compression by three different
retractors on pressure in the erector spine muscles during and after
posterior lumbar spine surgery in humans. Spine 1998;23:354–8.
[52] Takahashi H, Suguro T, Okazima Y, Motegi M, Okada Y, Kakiuchi T.
Inflammatory cytokines in the herniated disc of the lumbar spine. Spine
1996;21:218–24.
[53] Theron J, Cuellar H, Sola T, Guimaraens L, Casasco A, Courtheoux P.
Percutaneous treatment of cervical disk hernias using gelified ethanol.
AJNR Am J Neuroradiol 2010;31:1–3.
[54] Theron J, Guimaraens L, Casasco A, Sola T, Cuellar H, Courtheoux P.
Percutaneous treatment of lumbar intervertebral disk hernias with radi-
opaque gelified ethanol: a preliminary study. J Spinal Disord Tech
2007;20:526–32.
[55] van Alphen HA, Braakman R, Bezemer PD, Broere G, Berfelo MW.
Chemonucleolysis versus discectomy: a randomized multicenter trial. J
Neurosurg 1989;70:869–75.
[56] Vucetic N, Astrand P, Guntner P, Svensson O. Diagnosis and prognosis in
lumbar disc herniation. Clin Orthop Relat Res 1999;361:116–22.
[57] Weber BR, Grob D, Dvorak J, Muntener M. Posterior surgical approach to
the lumbar spine and its effect on the multifidus muscle. Spine
1997;22:1765–72.
[58] Weber H, Holme I, Amlie E. The natural course of acute sciatica with
nerve root symptoms in a double-blind placebo-controlled trial evaluating
the effect of piroxicam. Spine 1993;18:1433–8.
[59] Wei CJ, Li YH, Chen Y, Wang JY, Zeng QL, Zhao JB, et al. Percutaneous
intradiscal oxygen-ozone injection for lumbar disc herniation: no need of
perioperative antibiotic prophylaxis. Nan Fang Yi Ke Da Xue Xue Bao
2007;27:384–6.
[60] Yu Y, Liu W, Song D, Guo Q, Jia L. Diagnosis of discogenic low back pain
in patients with probable symptoms but negative discography. Arch
Orthop Trauma Surg 2012;132:627–32.