Embed Size (px)
Citation preview
ORIGINAL ARTICLE
Percutaneous trans uminal septal myocardial
ablation (PTSMA) for symptomatic patients
with hypertrophic obstructive cardio-
myopathy: first experience
J.M. ten Berg, H.H.D. Idzerda, W. Jaarsma
Background. Recently, percutaneous transluminalseptal myocardial ablation (PTSMA) has beenintroduced as treatment for symptomatic patientswith hypertrophic obstructive cardiomyopathy(HOCM).Methods. We describe our first experience in 24patients who were treated in our institution duringthe year 2000.Results. The procedure was initially successful inall but one patient. In that patient the septal branchthat was perfusing the proximal septum could notbe found. The procedure was complicated in threepatients. One patient died suddenly on the secondday after the procedure. Two additional patientsneeded a permanent pacemaker for persisting totalheart block. In the other 22 patients the procedurewas successful with an acute decrease ofthe meanoutflow tract gradient from 89±43 mmHg to21±19 mmlHg. In those 19 patients who had afollow-up of at least three months (mean follow-up 172±87 days), the meanNYHA class decreasedfrom 2.7±0.7 beforePTSMA to 0.6±0.9 at the lastfollow-up. The echocardiographic gradient de-creased from 92±39 mmHg before the procedureto 26±23 mmHg at the last follow-up.Conclusions. Our preliminary results demonstratethat PTSMA is an effective treatment forsymptomatic patients with HOCM. (Neth HeartJ2001;9:318-22.)
Keywords: Hypertrophic obstructive cardiomyopathy(HOCM), percutaneous transluminal septal myo-cardial ablation (PTSMA)
J.M. ten Berg.H.H.D. Idzerda.W. Jaarsma.Department of Cardiology, St. Antonius Hospital,Koekoekslaan 1, 3435 CM Nieuwegein.
Address for correspondence: J.M. ten Berg.E-mail: [email protected].
Patients with hypertrophic obstructive cardio-myopathy (HOCM) who remain symptomatic
despite optimal medication are candidates to undergoa Morrow septal myectomy."-2 Although this procedureis safe when performed by experienced surgeons, it isinvasive with the need for thoracotomy and extra-corporal circulation. A percutaneous technique hasrecently been introduced: percutaneous transluminalseptal myocardial ablation (PTSMA) using alcohol tolocally ablate the septal hypertrophy. In this reportwe describe our first experience with this techniqueand review the literature.
Patients and methods
Patient selectionWe consider patients to be candidates for PTSMAwhen they remain symptomatic (NYHA functionalclass >II) despite maximal tolerated doses of (-blockers, verapamil, or disopyramide and have a restingor provocable - post-ventricular extrasystole or withValsalva - left ventricular outflow tract gradient over50 mmHg. Also patients previously unsuccessfullytreated with a DDD-pacemaker or myectomy arecandidates.
How to perform PTSMAEncouraged by previous results of other groups, westarted to perform PTSMA in February 2000 usingthe technique developed and described by Seggewissand colleagues.4 In short: a complete angiogram isperformed and a temporary pacemaker is placed in theright ventricle to intercept possible total heart block.Then the gradient is measured using an angioplastycatheter in the aorta ascendens and a pigtail catheterin the left ventricular apex. The gradient is measuredat rest, after a post-ventricular extrasystole and duringa Valsalva manoeuvre. Next, the presumed target septalbranch is wired.Ashort balloon, 10mm over the wire,is introduced into the septal branch to prevent leakageof alcohol into the left anterior descending coronaryartery (LAD) and sized not to cause dissection oftheseptal branch when inflated. The inflated balloon is
Ne3hehd ands Heart Journal, Volume 9, Number 8, Novenber 2001318
Percutaneous transluminal septal myocardial ablation (PTSMA) for symptomatic patients with hypertrophic obstructive cardiomyopathy
checked to ensure that it does not occlude the LAD.After retrieval ofthe wire, angiographic contrast (1 ml)is introduced through the inflated balloon to excludeleakage into the LAD and then echo contrast (1 mlLevovist®) is injected to confirm, by 2D echo-cardiography, that the selected septal branch perfusesonly the target myocardial area and no other structures.After correct positioning ofthe catheter and balloon,two to four dosages of 1 ml of96% alcohol are slowlyintroduced through the inflated balloon under rhythmcontrol and with direct echocardiographic visualisationof the alcohol, which is very echogenic. The amountofalcohol used depends on the mass ofthe septum aswell as the acute haemodynamic changes (dis-appearance of systolic anterior movement, gradientand mitral regurgitation) during the procedure. Thedevelopment of a total heart block also ends theprocedure. After the last dose, the balloon remains inplace for ten minutes to ensure that no alcohol entersthe LAD when removing the balloon. During theprocedure the patient is given analgesic medication.After the procedure an angiogram of the LAD isperformed to ensure patency ofthe LAD and closureof the septal branch. Post-procedure, the patient ismonitored for at least 48 hours to intercept late totalheart block and any other complications.
ResultsDuring the year 2000, 31 patients with HOCM werereferred for intervention. Of these, one patientunderwent Morrow resection in combination withmitral valve replacement for endocarditis. Six patientswere in NYHA functional class .Il and for this reasondid not undergo intervention. In these six patientsoptimisation ofmedicationwas suggested. In the year2000, 24 patients were treated by PTSMA in ourinstitution. The procedure was initially successful in allbut one patient. In that patient the septal branch thatwas perfusing the proxunmal septum could not be found.The procedure was complicated in three patients. A42-year-old man underwent PTSMA for dyspnoeaNYHA class III and a gradient at rest of 50 mmHg.The procedure was successful with a drop of thegradient to 20 mmHg, but a total heart block devel-oped. The next day normal conduction returned andthe temporary pacemakerwas removed. Later that day,total heart block recurred with rapidly progressingheart failure for which the temporary pacemaker wasreintroduced. After the patient had recovered withpacing and diuretics, an electromechanical dissociationdeveloped during the night and the patient died.Autopsy showed septal infarction and congestion ofthe lungs. Two additional patients needed a permanent
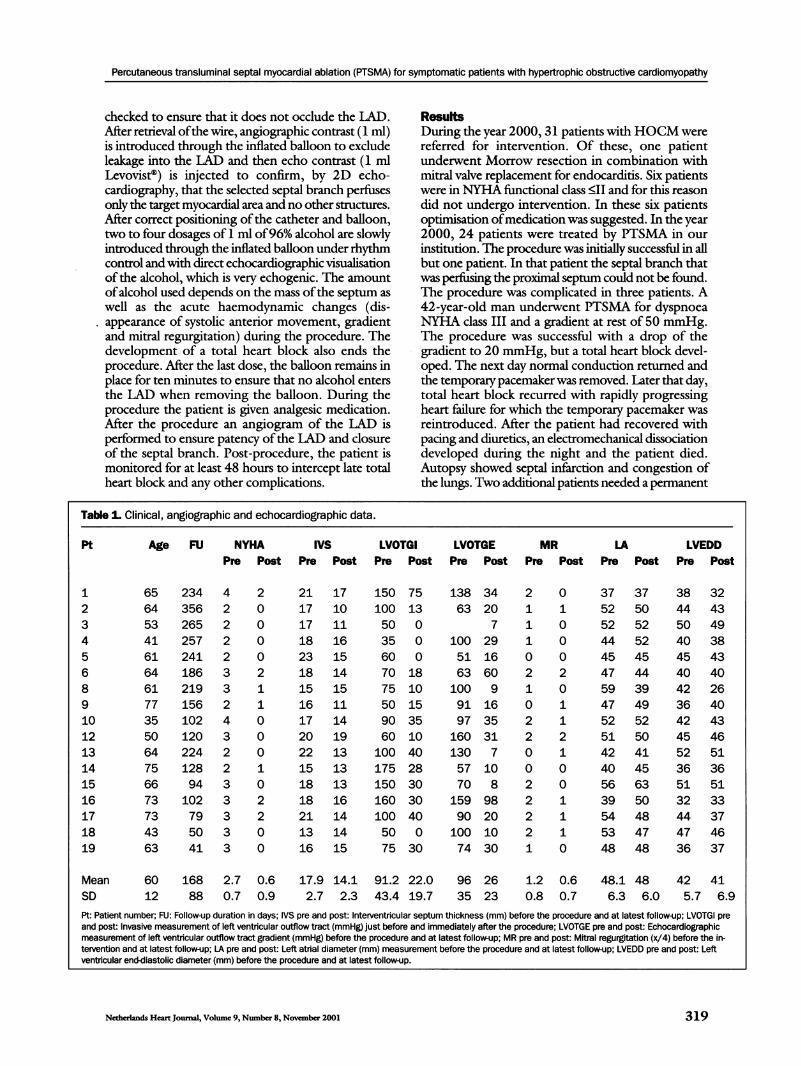
Table 1. Clinical, angiographic and echocardiographic data.
Age FU NYHA IVS LVOTGI LVOTGE MR LA LVEDDPre Post Pre Post Pre Post Pre Post Pre Post Pre Post Pre Post
6564534161646177355064756673734363
234 4 2356 2 0265 2 0257 2 0241 2186 3219 3156 2102 4120 3224 2128 294 3102 379 350 341 3
0
2110
0
0
10
220
0
21 1717 1017 1118 1623 1518 1415 1516 1117 1420 1922 1315 1318 1318 1621 1413 1416 15
150 75100 1350 035 060 070 1875 1050 1590 3560 10100 40175 28150 30160 30100 4050 075 30
138 3463 20
7
100 2951 1663 60100 991 1697 35160 31130 757 1070 8
159 9890 20100 1074 30
21110
210
220
0
22221
0
10
0
0
20
11210
0
1110
37 3752 5052 5244 5245 4547 4459 3947 4952 5251 5042 4140 4556 6339 5054 4853 4748 48
38 3244 4350 4940 3845 4340 4042 2636 4042 4345 4652 5136 3651 5132 3344 3747 4636 37
Mean 60SD 12
168 2.7 0.688 0.7 0.9
17.9 14.1 91.2 22.0 96 26 1.2 0.62.7 2.3 43.4 19.7 35 23 0.8 0.7
48.1 48 42 416.3 6.0 5.7 6.9
Pt: Patient number; FU: Follow-up duration in days; IVS pre and post: Interventricular septum thickness (mm) before the procedure and at latest follow-up; LVOTGI preand post: Invasive measurement of left ventricular outflow tract (mmHg) just before and immediately after the procedure; LVOTGE pre and post: Echocardiographicmeasurement of left ventricular outflow tract gradient (mmHg) before the procedure and at latest follow-up; MR pre and post: Mitral regurgitation (x/4) before the in-tervention and at latest follow-up; LA pre and post: Left atral diameter (mm) measurement before the procedure and at latest follow-up; LVEDD pre and post: Leftventricular end-diastolic diameter (mm) before the procedure and at latest follow-up.
Netherlands Heart Journal, Volume 9, Number 8, November 2001
Pt
12345689101213141516171819
319
Percutaneous transluminal septal myocardial ablation (PTSMA) for symptomatic patients with hypertrophic obstructive cardiomyopathy
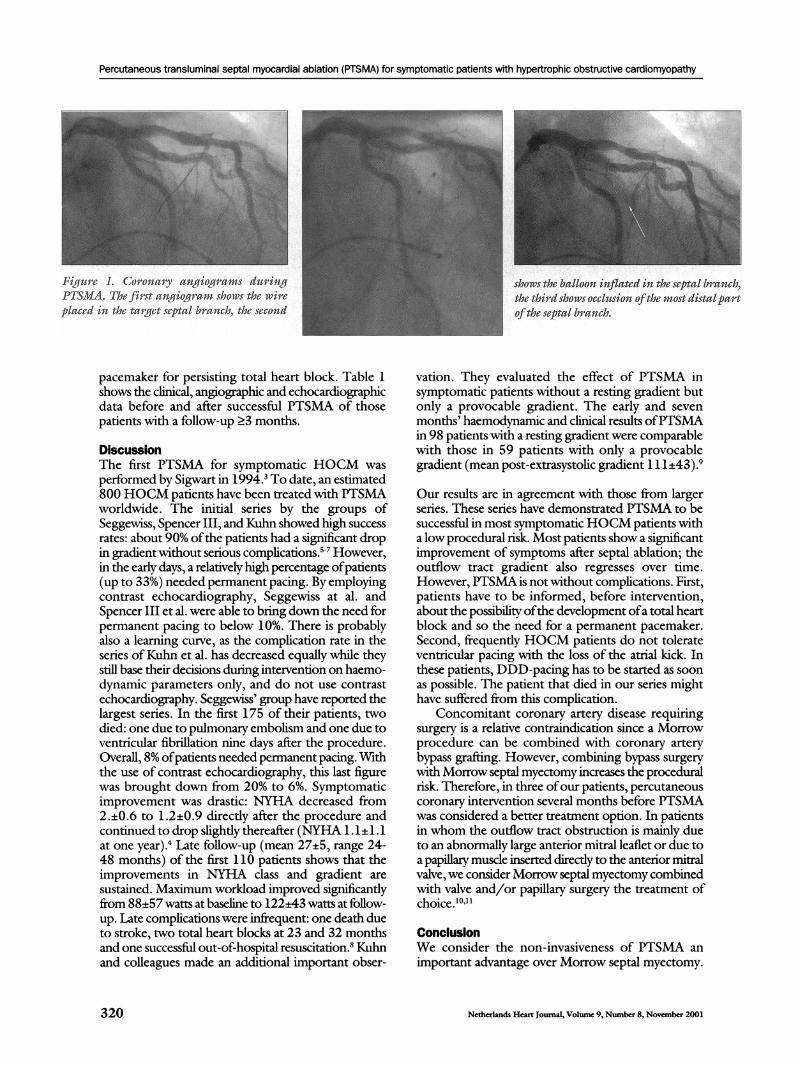
Figure 1. Coronary angiogramns duringPTSMA. The first angiogram shows the wireplaced in the target septal branch, the second
pacemaker for persisting total heart block. Table 1shows the clinical, angiographic and echocardiographicdata before and after successful PTSMA of thosepatients with a follow-up >3 months.
DiscussionThe first PTSMA for symptomatic HOCM wasperformed by Sigwart in 1994.3 To date, an estimated800 HOCM patients have been treated with PTSMAworldwide. The initial series by the groups ofSeggewiss, Spencer III, and Kuhn showed high successrates: about 90% ofthe patients had a significant dropin gradient without serious complications.57 However,in the early days, a relatively high percentage ofpatients(up to 33%) needed permanent pacing. By employingcontrast echocardiography, Seggewiss at al. andSpencer III et al. were able to bring down the need forpermanent pacing to below 10%. There is probablyalso a learning curve, as the complication rate in theseries ofKuhn et al. has decreased equally while theystill base their decisions during intervention on haemo-dynamic parameters only, and do not use contrastechocardiography. Seggewiss' group have reported thelargest series. In the first 175 of their patients, twodied: one due to pulmonary embolism and one due toventricular fibrillation nine days after the procedure.Overall, 8% ofpatients needed permanent pacing. Withthe use of contrast echocardiography, this last figurewas brought down from 20% to 6%. Symptomaticimprovement was drastic: NYHA decreased from2.±0.6 to 1.2±0.9 directly after the procedure andcontinued to drop slightly thereafter (NYHA 1.1±1.1at one year).4 Late follow-up (mean 27±5, range 24-48 months) of the first 110 patients shows that theimprovements in NYHA class and gradient aresustained. Maximum workload improved significantlyfrom 88±57 watts at baseline to 122±43 watts at follow-up. Late complications were infrequent: one death dueto stroke, two total heart blocks at 23 and 32 monthsand one successful out-of-hospital resuscitation.8 Kuhnand colleagues made an additional important obser-
shows the balloon inflated in the septal brancb,the third shows occlusion ofthe most distalpartofthe septal branch.
vation. They evaluated the effect of PTSMA insymptomatic patients without a resting gradient butonly a provocable gradient. The early and sevenmonths' haemodynamic and clinical results ofPTSMAin 98 patients with a resting gradient were comparablewith those in 59 patients with only a provocablegradient (mean post-extrasystolic gradient 111±43).9
Our results are in agreement with those from largerseries. These series have demonstrated PTSMA to besuccessful in most symptomaticHOCM patients witha low procedural risk. Most patients show a significantimprovement of symptoms after septal ablation; theoutflow tract gradient also regresses over time.However, PTSMA is not without complications. First,patients have to be informed, before intervention,about the possibility ofthe development ofa total heartblock and so the need for a permanent pacemaker.Second, frequently HOCM patients do not tolerateventricular pacing with the loss of the atrial kick. Inthese patients, DDD-pacing has to be started as soonas possible. The patient that died in our series mighthave suffered from this complication.
Concomitant coronary artery disease requiringsurgery is a relative contraindication since a Morrowprocedure can be combined with coronary arterybypass graffing. However, combining bypass surgerywith Morrow septal myectomy increases the proceduralrisk. Therefore, in three ofour patients, percutaneouscoronary intervention several months before PTSMAwas considered a better treatment option. In patientsin whom the outflow tract obstruction is mainly dueto an abnormally large anterior mitral leaflet or due toa papillary muscle inserted directly to the anterior mitralvalve, we consider Morrow septal myectomy combinedwith valve and/or papillary surgery the treatment ofchoice.'0"'1
ConclusionWe consider the non-invasiveness of PTSMA animportant advantage over Morrow septal myectomy.
Netherlands Heart Joumal, Volume 9, Number 8, November 2001320
Percutaneous transluminal septal myocardial ablation (PTSMA) for symptomatic patients with hypertrophic obstructive cardiomyopathy
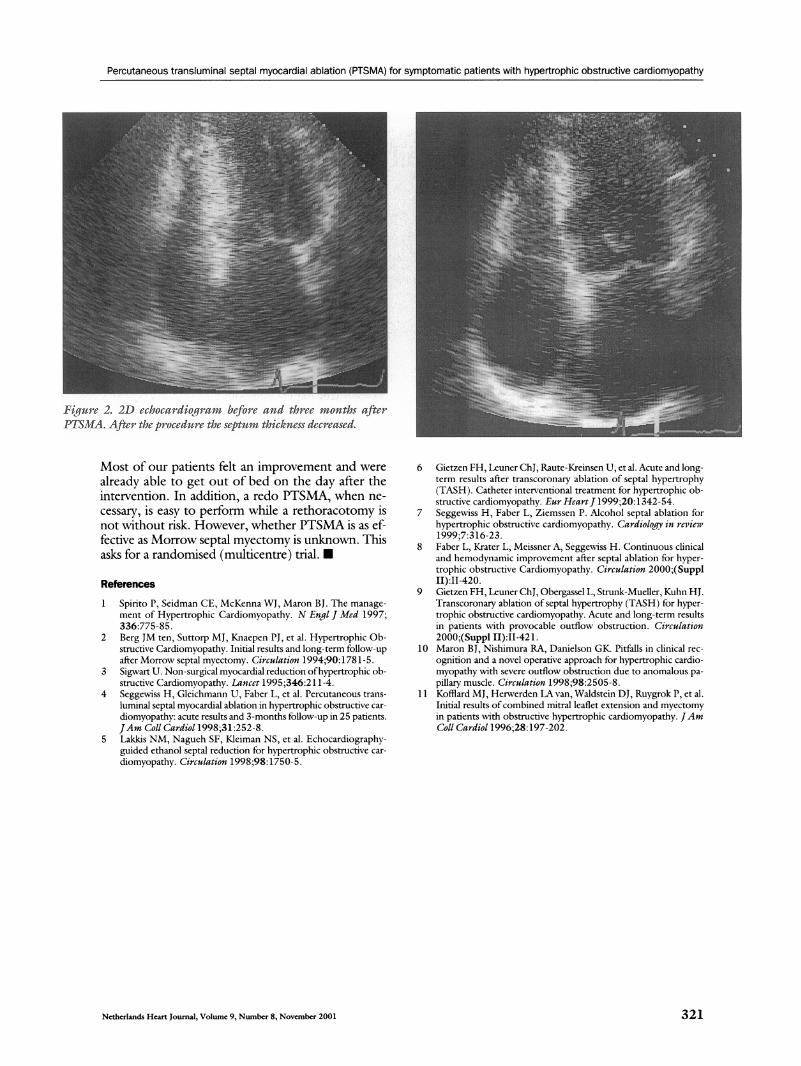
Fiqurc 2. 21) cchoctnidioqi-a befoict and threc months after-PTI7SU'IA. After- tht pi ocedniti- the septnmili thjicknssc decreased.
Most of our patients felt an improvement and werealready able to get out of bed on the day after theintervention. In addition, a redo PTSMA, when ne-cessary, is easy to perform while a rethoracotomy isnot without risk. However, whether PTSMA is as ef-fective as Morrow septal myectomy is unknown. Thisasks for a randomised (multicentre) trial. c
References
1 Spirito P, Seidman CE, McKenna WJ, Maron BJ. The manage-ment of Hypertrophic Cardiomyopathy. N Engl J Med 1997;336:775-85.
2 Berg JM ten, Suttorp MJ, Knaepen PJ, et al. Hypertrophic Ob-structive Cardiomyopathy. Initial results and long-term follow-upafter Morrow septal myectomy. Circulation 1994;90:1781-5.
3 Sigwart U. Non-surgical myocardial reduction ofhypertrophic ob-structive Cardiomyopathy. Lancet 1995;346:21 1-4.
4 Seggewiss H, Gleichmann U, Faber L, et al. Percutaneous trans-luminal septal myocardial ablation in hypertrophic obstructive car-diomyopathy: acute results and 3-months follow-up in 25 patients.JAm Coll Cardiol 1998;31:252-8.
5 Lakkis NM, Naguch SF, Kleiman NS, et al. Echocardiography-guided ethanol septal reduction for hypertrophic obstructive car-diomyopathy. Circulation 1998;98:1750-5.
6 Gietzen FH, Leuner ChJ, Raute-Kreinsen U, et al. Acute and long-term results after transcoronary ablation of septal hypertrophy(TASH). Catheter interventional treatment for hypertrophic ob-structive cardiomyopathy. Eur HeartJ 1999;20:1342 - 54.
7 Seggewiss H, Faber L, Ziemssen P. Alcohol septal ablation forhypertrophic obstructive cardiomyopathy. Cardiology in review1999;7:316-23.
8 Faber L, Krater L, Meissner A, Seggewiss H. Continuous clinicaland hemodynamic improvement after septal ablation for hyper-trophic obstructive Cardiomyopathy. Circulation 2000;(SupplII):II-420.
9 Gietzen FH, Leuner ChJ, Obergassel L, Strunk-Mueller, Kuhn HJ.Transcoronary ablation of septal hypertrophy (TASH) for hyper-trophic obstructive cardiomyopathy. Acute and long-term resultsin patients with provocable outflow obstruction. Circulation2000;(Suppl II):II-421.
10 Maron BJ, Nishimura RA, Danielson GK. Pitfalls in clinical rec-ognition and a novel operative approach for hypertrophic cardio-myopathy with severe oufflow obstruction due to anomalous pa-pillary muscle. Circulation 1998;98:2505-8.
11 Kofflard MJ, Herwerden LA van, Waldstein DJ, Ruygrok P, et al.Initial results ofcombined mitral leaflet extension and myectomyin patients with obstructive hypertrophic cardiomyopathy. JAmColl Cardiol 1996;28:197-202.
Netherlands Heart Journal, Volume 9, Number 8, November 2001 321














![Percutaneous image-guided ablation of bone and soft tissue ... · oid osteoma [23, 24]. Ever since, for the therapy of this benign tumour, thermal ablation constitutes a first-line](https://img.pdfslide.us/doc/110x75/5cbf758888c9932c128b8add/percutaneous-image-guided-ablation-of-bone-and-soft-tissue-oid-osteoma-23.jpg)













