Embed Size (px)
Citation preview

DepartmenFrance.
CorrespondVascular SurgRue Pierre D�echu-nice.fr
Ann Vasc Surhttp://dx.doi.or� 2013 Elsevi
Manuscript rec
11, 2013.
894
Percutaneous Angioplasty of Long TibialOcclusions in Critical Limb Ischemia
Nirvana Sadaghianloo, Elix�ene Jean-Baptiste, Serge Declemy, Aur�elien Mousnier,
Sophie Brizzi, and R�eda Hassen-Khodja, Nice, France
Background: The aim of this study was to assess the midterm results of percutaneousangioplasty in patients with critical limb ischemia (CLI) and long tibial occlusions.Methods: Between January and September 2011, 34 consecutive patients with patent femoro-popliteal artery and 49 segmental tibial occlusions >8 cm were included in our prospective,single-center cohort study. Clinical success (defined as wound healing and survival withoutmajor amputation), patency, and freedom from target vessel revascularization (TVR) wereexamined.Results: The median age of the patients was 75 (53e89) years, 74% were diabetic, and 89%of the limbs studied were Rutherford 5 and 6. Median follow-up was 12.5 (1e15) months. The1-year clinical success rate was 65%, higher among patients with technical success (76% vs.25%, P ¼ 0.01) and patients with 2 or 3 patent tibial arteries after the procedure (90% vs.41% in patients with only 1 patent artery, P ¼ 0.003). At 1 year, primary and secondary patencyrates were 13% and 32%, respectively (24% and 58% without technical failures). The 1-yearfreedom-from-TVR rate was 34%.Conclusions: Despite high technical failure rates and the need for repeat procedures,percutaneous angioplasty of long tibial occlusions enhances wound healing, especially whenintegrated into a maximal revascularization approach.
INTRODUCTION
In the recent European guidelines for critical limb
ischemia (CLI), percutaneous angioplasty has been
recognized as a reasonable first-line therapeutic
modality for patients with CLI and infrapopliteal
lesion, in the majority of cases.1 Distal surgical
bypass is a well-acknowledged therapeutic modality
and must be considered for more complex anatomic
lesions of tibial arteries or in cases of endovascular
failure and persisting clinical symptoms of CLI.1,2
However, without a specific classification of infra-
popliteal arterial disease, the role of endovascular
t of Vascular Surgery, University Hospital of Nice, Nice,
ence to: R�eda Hassen-Khodja, MD, Department ofery, University Hospital of Nice, Hopital Saint Roch, 5voluy, 06000 Nice, France; E-mail: hassen-khodja.r@
g 2013; 27: 894–903g/10.1016/j.avsg.2013.02.008er Inc. All rights reserved.
eived: December 8, 2012; manuscript accepted: February
treatment in complex anatomic lesions remains
unclear. Recent studies have shown high technical
success rates and better limb-salvage rates in
patients undergoing angioplasty of heterogeneous
infrapopliteal lesions, with however, an inconstant
proportion of long tibial occlusions and various defi-
nitions of success.3,4 The objective of our single-
center study was to prospectively assess the 1-year
clinical and patency results of percutaneous angio-
plasty in a specific cohort of patients with CLI and
long tibial occlusions.
METHODS
Between January and September 2011, all consecu-
tive patients admitted to our vascular surgery
department with CLI and infrapopliteal arterial
disease were assessed for revascularization. Defini-
tion of CLI followed the current consensus: presence
of ischemic rest pain for >2 weeks (Fontaine stage
III, Rutherford class 4) or ischemic tissue loss associ-
ated with an absolute ankle pressure of <50 mm Hg

Vol. 27, No. 7, October 2013 Angioplasty in tibial occlusions 895
or great toe pressure of <30 mm Hg (Fontaine stage
IV, Rutherford class 5 or 6).
Endovascular treatmentwas thefirst-line strategy
for all patients whenever technically achievable.
Patients who underwent primary major amputa-
tion owing to irreversible ischemic damage were
primarily excluded from our database. In nonambu-
latory patients with limited life expectancy, CLI
was managed conservatively by the best medical
treatment, including analgesic, antibiotic, statin,
and antiplatelet therapy, and their data were also
excluded from analyses.
Patients with patent femoropopliteal arteries and
segmental tibial occlusions >8 cm, diagnosed by
angiography and eligible for endovascular treat-
ment,were included in our prospective cohort study.
Exclusion criteria were acute limb ischemia,
recent (<6 months) ipsilateral revascularization,
concomitant open vascular surgery, endovascular
treatment of venous bypasses, isolated nonocclusive
stenoses and short occlusions (<8 cm) of tibial
arteries, long occlusions without distal vessel visu-
alization, and isolated below-the-ankle arterial
occlusions.
The study was conducted according to the Decla-
ration of Helsinki, and the institutional ethics
committee of our hospital approved this protocol.
Patients gave informed consent before inclusion in
the study.
Treatment Protocol
Before the intervention, a nephron-protection
protocol was commenced in all patients with creat-
inine clearance <30 mL/min: a 3-mL/kg/hr sodium
bicarbonate infusion 1 hr before and 1 mL/kg/hr for
6 hours after the procedure.
All procedures were performed in the operating
room by an experienced vascular surgeon, under
local, regional, or general anesthesia, according to
patient’s age and comorbidities.
After anterograde puncture of the ipsilateral
common femoral artery, we attempted to recanalize
all selected long occlusions via a 5F sheath by a trans-
luminal or subintimal approach, using dedicated
0.014-in. below-the-knee wires (Pilot 200 and
Winn 200T; Abbott Vascular, Abbott Park, IL).
Angioplasty was performed using dedicated low-
profile balloons (Armada 0.14 [Abbott Vascular]
and Advance 0.14 [Cook Medical, Inc., Blooming-
ton, IL]). In successfully recanalized arteries,
stenting (Xpert; Abbott Vascular) was only used in
the case of a flow-limiting dissection that was not
resolved by 5-min balloon inflation.
At the beginning of the procedure, 3500e5000 IU
of heparin was administered based on the patient’s
weight. At the end of the procedure, the access site
was closed using a percutaneous suture device
(StarClose SE; Abbott Vascular). Surgical treatment
to remove necrotic tissue and drain the abscess
was performed at the end of the interventional
procedure when necessary, and this was always
accompanied by broad-spectrum antibiotic therapy.
After the intervention, all patients received
75 mg/d of aspirin for life, with an additional
75mg/d of clopidogrel for 1month. Optimalmedical
treatment for vascular risk factors and additional
wound care were given to all patients.
Assessment of the peripheral circulation was
systematically performed by a duplex scan during
follow-up at 1, 3, and 6 months, or more frequently
depending on individual clinical needs; repeated
angiography was limited to patients with symp-
tomatic recurrent stenosis/occlusion or additional
arterial lesions that were suspected clinically.
Outcome Measures and Definitions
Revascularization of at least one of the 3 leg arteries
with reestablishment of a direct arterial flow to the
foot was considered a technical success. The main
outcome measure was the clinical success rate.
Clinical success was defined as complete tissue loss
healingwithoutmajor amputation (Rutherford class
5 and 6 patients) or upward shift of at least 2 clinical
symptom categories according to the Rutherford
classification (Rutherford class 4 patients).
Secondary outcome measures were patency and
freedom from target vessel revascularization (TVR).
Primary patency was defined as uninterrupted
patency with no additional procedures performed
on or at the margins of the treated segment. Assisted
primary patency was used when patency was not
lost but maintained by prophylactic intervention.
Secondary patency concerns any patent revascular-
ization, even after a reintervention.5
Statistical Method
Statistical analysis was performed with StatView
software, version 5.0 (SAS Institute, Inc., Cary,
NC). Nominal variables were expressed as a number
and a percentage of patients. Differences of categor-
ical variables were assessed by the 2-tailed Fisher’s
exact test. Continuous variables were expressed
as the mean standard deviation or the range for
non-Gaussian distributions. Differences between
continuous variables were assessed by 2-tailed
unpaired t-test. Differences with a value of P <0.10 were statistically controlled by logistic

Fig. 1. Initial treatment of patients with critical limb ischemia.
Table I. Population characteristics
Number of patients 34
Male 23 68%
Female 11 32%
Risk factors
Hypertension 25 74%
Diabetes 25 74%
Current smoking (<3 years) 6 18%
Hyperlipidemia 17 50%
Comorbid diseases
Severe renal insufficiency 9 27%
ESRD on dialysis 4 12%
BMI >30 7 21%
COPD 3 9%
Coronary artery disease 16 47%
Cerebrovascular disease 5 15%
Medication
Antiplatelet 32 94%
Statin 29 85%
Beta-blocker 20 59%
ACE inhibitor 12 35%
Oral glucose-lowering medication 15 44%
Insulin therapy 15 44%
Mode of presentation (37 limbs)
Rutherford 4 4 11%
Rutherford 5 30 81%
Rutherford 6 3 8%
ACE, angiotensin-converting enzyme; BMI, body mass index;
COPD, chronic obstructive pulmonary disease; ESRD, end-
stage renal disease.
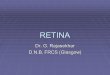
Fig. 2. (A) Long occlusion of both anterior and posterior
tibial artery. (B) Successful recanalization of anterior
tibial artery. The posterior tibial artery was not attempted
(no distal vessel visualization).
896 Sadaghianloo et al. Annals of Vascular Surgery
regression analysis. The KaplaneMeier life-table
method was used to calculate patency curves. Bivar-
iate assessment of interdependency of gender and
patency was performed by applying log-rank tests.

Table II. Predictive factors of technical failure:
Univariate analysis of 49 recanalization attempts
Success Failure
Pn % n %
Total (N ¼ 49) 27 55% 22 45% dGender
Male 15 47% 17 53% 0.14
Female 12 71% 5 29%
Age (years) 71.5 ± 10.5 75.8 ± 10.1 0.15
Comorbid diseases
Hypertension 21 58% 15 42% 0.52
Diabetes 24 65% 13 35% 0.02
Severe renal
insufficiency
9 69% 4 31% 0.33
Fontaine stage
III 1 20% 4 80% 0.15
IV 26 59% 18 41%
Rutherford
classification
4 1 20% 4 80%
5 23 58% 17 42% 0.20
6 3 67% 1 33%
Occlusion
length (cm)
14.7 ± 5.8 18.3 ± 4.2 0.01
Table III. Predictive factors of clinical success:
Univariate analysis of 37 limbs
Success Failure
Pn % n %
Total (N ¼ 37) 24 65% 13 35% dGender
Male 14 56% 11 44% 0.14
Female 10 83% 2 17%
Age (years) 73 ± 11.1 76.5 ± 9.3 0.33
Comorbid diseases
Hypertension 19 70% 8 30% 0.27
Diabetes 19 70% 8 30% 0.27
Severe renal
insufficiency
8 80% 2 20% 0.43
Coronary artery
disease
14 78% 4 22% 0.17
Medication
Antiplatelet 23 66% 12 34% >0.99
Statin 21 68% 10 32% 0.64
Beta-blocker 15 71% 6 29% 0.48
ACE inhibitor 9 69% 4 31% 0.73
Oral glucose-lowering
medication
9 60% 6 40% 0.73
Insulin therapy 14 82% 3 18% 0.38
Occlusion length (cm) 15.2 ± 6.8 18.1 ± 6.7 0.13
Technical success
(29 of 37)
22 76% 7 24% 0.01
ACE, angiotensin-converting enzyme.
Table IV. Predictive factors of clinical success
Vol. 27, No. 7, October 2013 Angioplasty in tibial occlusions 897
The Cox proportional hazards regression model was
used to control potentially confounding factors for
censored variables. Differences are expressed
as hazard ratio (HR) with 95% confidence interval
(CI). P< 0.05was considered statistically significant.
among Fontaine stage IV limbs (N ¼ 33)
Success Failure
Pn % n %
Number of patent arteries
at end of procedure
1 5 35% 9 65% 0.006
2 15 88% 2 12%
2 15 88% 2 12% >0.99
3 2 100% 0 0%
Patency of angiosome
arteries
At least 1 artery 16 73% 6 27% 0.43
No artery 6 55% 5 43%
RESULTS
Between January and September 2011, 153 consec-
utive patients were admitted to our vascular surgery
department with CLI and infrapopliteal arterial
disease. Thirty patients were excluded from our
study: 22 with irreversible ischemic tissue loss who
underwent primary major amputation, and 8 with
limited life expectancy who were managed conser-
vatively. Treatment concerning the remaining 123
patients with CLI and eligible for revascularization
are summarized in Figure 1.
According to our selected criteria, 34 patients
presenting with 37 CLI and long tibial occlusion
(Fontaine stage IV, Rutherford class 5 and 6)
(89%) were included in our cohort study (Fig. 1).
The median age was 75 (range 53e89) years, and
23 (68%) of the patients were men. Patients’ demo-
graphic data, mode of presentation, risk factors for
arteriosclerosis, and comorbidities are summarized
in Table I.
Forty-nine occluded tibial arteries with a mean
length of 16.2 ± 5.9 cm were considered for either
transluminal or subintimal angioplasty (Fig. 2)
among the 34 patients. Twenty-two artery recanali-
zation attempts failed, owing to the inability to cross
or dilate highly calcified lesions (n¼ 17), an absence
of tibial blood flow at the time of final angiography
(n ¼ 4), or tibial artery rupture (n ¼ 1). In the
univariate analysis (Table II), the length of the
lesion was significantly higher in the failed

Fig. 3. Clinical evolution of patients with ischemic tissue loss.
898 Sadaghianloo et al. Annals of Vascular Surgery
recanalization attempts group (16.3 ± 6.1 cm vs.
11 ± 3 cm; P ¼ 0.02 [t-test]). Technical failures
were also more common in nondiabetic patients
than in diabetic ones (75% vs. 35%; P ¼ 0.01).
Multivariate logistic regression analysis showed
that lesion length (odds ratio [OR] ¼ 1.19; 95%
confidence interval [CI] 1.03e1.38; P ¼ 0.01)
and nondiabetic patients (OR ¼ 8.02; 95% CI
1.61e39.89; P ¼ 0.01) were independent predictors
of technical failure. Of note, the length of the lesion
was similar in diabetic and nondiabetic patients
(16.5 ± 4 cm vs. 15.7 ± 5.8 cm; P ¼ 0.63 [t-test]).
Further clinical characterization of this nondiabetic
subgroup could not be achieved because of the
small sample size and insufficient data collection.
With respect to the number of limbs treated,
the technical success rate was 78% (29 of 37)
(Table III). Five stents were implanted in this series
because of residual stenosis (n ¼ 3) or vessel dissec-
tion (n ¼ 2). The final angiography showed no
improvement in 8 limbs, despite revascularization
attempts on at least 1 occluded artery.
The 30-day complication rate was 9% (1 retro-
peritoneal hematoma, 1 calf hematoma after arterial
perforation, and 1 myocardial infarction). No death
occurred during this period.
Median follow-up was 12.5 (range 1e15)
months. One patient was unavailable for follow-
up. Patient survival rate was 91% at 12 months.
Four patients (12%) died within the follow-up
period (1 multiorgan failure, 1 respiratory failure,
1 heart failure, 1 mesenteric infarction).
The clinical success rate at 1 year, defined as
wound healing without major amputation, was
65%. Clinical success was higher among patients
with 2 patent tibial arteries after the first procedure
(88%) versus patients with only 1 patent artery
(35%) (P ¼ 0.006 by Fisher’s exact test). Given
that there were only 2 patients with 3 patent tibial
arteries, comparison between patients with 2 vs.
3 patent arteries was not significant (P < 0.99
by Fisher’s exact test) (Table IV). The clinical evolu-
tion of patients with ischemic tissue loss showed
improvement within the first 3 months, and
progressive wound healing within 6 months
(Fig. 3).
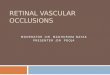
Primary patency rates at 6 months and 1 year
were 27% and 13%, assisted primary patency rates
were 41% and 28%, and secondary patency rates
were 47% and 32%, respectively. When consid-
ering only those patients with an initial technical
success, primary patency rates at 6 months and 1
year were 48% and 24%, assisted primary patency
rates were 74% and 52%, and secondary patency
rates were 85% and 58%, respectively (Fig. 4).
During follow-up, 14 TVRs were performed on 10
patients (12 limbs) with delayed healing. Seven
patients who healed in spite of restenosis did not
undergo any further revascularization procedures.
Freedom from TVR was 34% at 1 year.
The occlusion lengthwas associatedwith resteno-
sis or thrombosis in the univariate analysis (16.3 ±
6.1 cm vs. 11 ± 3 cm; P ¼ 0.02 [Fisher’s exact test])
(Table V), but not in the multivariate analysis
(hazard ratio [HR] ¼ 1.06; 95% CI 0.98e1.14;
P ¼ 0.11 [Cox model]). In both the univariate and
multivariate analyses, male gender was an indepen-
dent predictor of higher primary patency
(HR ¼ 0.32; 95% CI 0.12e0.87; P ¼ 0.02 [Cox
model]) (Fig. 5). Gender-related outcome was no
longer significant in secondary patency rates (HR ¼0.46; 95% CI 0.18e1.22; P ¼ 0.11 [Cox model]).

Fig. 4. (A) KaplaneMeier analysis of patency. (B) KaplaneMeier analysis of patency (without primary technical
failures).
Vol. 27, No. 7, October 2013 Angioplasty in tibial occlusions 899
DISCUSSION
In this cohort of patients with CLI and long tibial
occlusions, the technical success rate of angioplasty
was 78%. To the best of our knowledge, this is the
first series dealing with CLI and long tibial artery
occlusion simultaneously. Other series have either
excluded long tibial occlusions, contained cases
with mixed short and long tibial occlusions, or

Table V. Predictive factors of patency loss:
Univariate analysis of 27 recanalized arteries
Patency loss Patent arteries
Pn % n %
Total (N ¼ 27) 19 70% 8 30% dGender
Male 8 53% 7 47% 0.04
Female 11 92% 1 8%
Age (years) 73.8 ± 9.6 66 ± 11.3 0.07
Comorbid diseases
Hypertension 16 76% 5 24% 0.31
Diabetes 16 67% 8 33% 0.53
Severe renal
insufficiency
8 100% 0 0% 0.06
Medication
Antiplatelet 19 70% 8 30% dStatin 14 64% 8 36% 0.27
Beta-blocker 13 81% 3 19% 0.20
ACE inhibitor 9 90% 1 10% 0.18
Oral glucose-lowering
medication
7 58% 5 42% 0.39
Insulin therapy 9 60% 6 40% 0.23
Occlusion length (cm) 16.3 ± 6.1 11 ± 3 0.02
ACE, angiotensin-converting enzyme.
900 Sadaghianloo et al. Annals of Vascular Surgery
included many patients with tibial stenosis.6e13 In
a previous meta-analysis, Romiti et al. reported
a mean technical success rate of 84% in heteroge-
neous series with tibial occlusions and stenoses.3
In our series, limited to tibial occlusions, we failed
to recanalize 22 of 49 occluded tibial arteries
(45%), which seems to be a poor result; however,
this is comparable to findings reported by Ferraresi
et al., who had a technical success rate of 48%
when treating 281 stenosed or occluded tibial
arteries.10 The length of the lesion was predictive
of technical failure in our series. Vraux et al.
reported similar results with occlusions >10 cm.6
Postoperative and long-term complications were
similar to previously published data.14 Only 1 death
occurred within the first 6 months of follow-up.
Therefore, endovascular treatment of long tibial
occlusions may not increase morbidity and
mortality.
Limb salvage and amputation-free-survival rates
are often considered as primary end-points in
similar studies.15,16 However, focusing on wound
healing is at least as important to evaluate midterm
results of a revascularization technique in patients
with ischemic tissue loss. Considering the high rate
of primary technical failure in long tibial occlusions,
the clinical success rate in our series seems discor-
dant, although similar, to some published literature
findings (55e80%).6,7,17e19 Our analysis of clinical
success predictors shows that the number of patent
tibial arteries at the end of the procedure may be
of paramount importance in wound healing. Two
patent tibial arteries will lead to a higher rate of clin-
ical success than only 1 patent tibial artery
(P¼ 0.006). Iida et al. reported quite similar findings
when evaluating the angiosome concept in CLI.16
Considering the positive wound-healing outcome
and the infrequency of postoperative complications,
we may advocate, when possible, the revasculariza-
tion of at least 2 tibial arteries, instead of limiting
attempts to 1 artery.
In our series, specific direct revascularization of
the angiosome did not prove efficient in terms of
wound healing (Table III). Iida et al. reported a 4-
year amputation-free survival rate of 49% in a direct
revascularization group compared with 29% in an
indirect group (P ¼ 0.0002).20 However, the angio-
some theory remains controversial.21e23 in CLI
because one given wound often covers several
angiosomes. Therefore, direct revascularization of
all supplying arteries is probably the best approach
for the patient.
In addition to these findings, we found that the
length of the occlusion was predictive of restenosis.
Lazaris et al. demonstrated that the length of occlu-
sion and the number of run-off vessels were the
main determinants of patency after subintimal
angioplasty of infrainguinal arteries, but they
included only 6 isolated infrapopliteal angioplasties
in their cohort.24
Patency was assessed by duplex scan in all recan-
alized arteries of our series, and even by angiog-
raphy for some patients (61%). Our patency rates
are low, mostly due to a high primary technical
failure, and comparison of our patency rates with
those of previously published heterogeneous
cohorts remains difficult. Interestingly, 74% of our
patients are diabetic and in the recent European
guidelines for CLI, Dick et al. noted that, in diabetic
patients, primary patency rates are quite poor, but
with close follow-up and reinterventions one can
attain acceptable secondary patency and
amputation-free survival rates.25 Our results are
consistent with this statement.
In our study, we have shown female gender to be
predictive of poor primary patency. Gender-related
outcome in peripheral occlusive vascular disease
has already been described after carotid and femoro-
popliteal artery surgery26e29 Pomposelli et al. also
found that 5-year vein graft patency after a dorsalis
pedis bypass was worse in women.2 Although our
study was not designed primarily with this aim in

Fig. 5. (A) Log-rank analysis of gender-related primary patency. (B) Log-rank analysis of gender-related secondary
patency.
Vol. 27, No. 7, October 2013 Angioplasty in tibial occlusions 901

902 Sadaghianloo et al. Annals of Vascular Surgery
mind, we suggest closer follow-up after angioplasty
of long tibial occlusions in women.
Study Limitations
This prospective, non-randomized, single-center
study has several limitations. We assessed a small
number of patients, which makes statistical
interpretation difficult. However, our restrictive
inclusion criteria allowed us to assess outcomes
for a specific type of lesion.
Another limitation was that patency was deter-
mined by conventional angiography in only 61%
of cases during follow-up. Our personal experience
and some recent literature have shown that Duplex
ultrasound only has a limited value for the investi-
gation of infrapopliteal lesions.30 However, the use
of a noninvasive technique seemed preferable in
our high-risk population.
In conclusion, despite high technical failure rates
and the need for repeated procedures, endovascular
treatment of long tibial occlusions does enhance
wound healing. Our data also suggest that patients
with 2 patent tibial arteries have higher clinical
success rates than patients with only 1 patent artery.
In our specific subset of patients, female gender was
predictive of patency loss. Although described in
previous studies on other arteries, gender-related
outcome in infrapopliteal arteries should be assessed
further in a larger study population.
REFERENCES
1. Setacci C, de Donato G, Teraa M, et al. Chapter IV: treatment
of critical limb ischaemia. Eur J Vasc Endovasc Surg
2011;42(Suppl. 2):S43e59.
2. Pomposelli FB, Kansal N, Hamdan AD, et al. A decade of
experience with dorsalis pedis artery bypass: analysis of
outcome in more than 1,000 cases. J Vasc Surg 2003;37:
307e15.
3. Romiti M, Albers M, Brochado-Neto FC, Durazzo AES,
Pereira CAB, De Luccia N. Meta-analysis of infrapopliteal
angioplasty for chronic critical limb ischemia. J Vasc Surg
2008;47:975e81.
4. Ihnat DM, Mills JL Sr. Current assessment of endovascular
therapy for infrainguinal arterial occlusive disease in patients
with diabetes. J Vasc Surg 2010;52(Suppl. 3):S92e5.
5. Rutherford RB, Baker JD, Ernst C, et al. Recommended
standards for reports dealing with lower extremity ischemia:
revised version. J Vasc Surg 1997;26:517e38.
6. Vraux H, Bertoncello N. Subintimal angioplasty of tibial
vessel occlusions in critical limb ischaemia: a good opportu-
nity? Eur J Vasc Endovasc Surg 2006;32:663e7.7. Vraux H, Hammer F, Verhelst R, Goffette P, Vandeleene B.
Subintimal angioplasty of tibial vessel occlusions in the
treatment of critical limb ischaemia: mid-term results. Eur
J Vasc Endovasc Surg 2000;20:441e6.8. Nydahl S, Hartshorne T, Bell PR, Bolia A, London NJ.
Subintimal angioplasty of infrapopliteal occlusions in
critically ischaemic limbs. Eur J Vasc Endovasc Surg
1997;14:212e6.9. Ingle H, Nasim A, Bolia A, et al. Subintimal angioplasty of
isolated infragenicular vessels in lower limb ischemia:
long-term results. J Endovasc Ther 2002;9:411e46.10. Ferraresi R, Centola M, Ferlini M, et al. Long-term outcomes
after angioplasty of isolated, below-the-knee arteries in
diabetic patients with critical limb ischaemia. Eur J Vasc
Endovasc Surg 2009;37:336e42.11. Dorros G, Jaff MR, Dorros AM, Mathiak LM, He T. Tibioper-
oneal (outflow lesion) angioplasty can be used as primary
treatment in 235 patients with critical limb ischemia: five-
year follow-up. Circulation 2001;104:2057e62.12. Bosiers M, Hart JP, Deloose K, Verbist J, Peeters P. Endovas-
cular therapy as the primary approach for limb salvage in
patients with critical limb ischemia: experience with 443
infrapopliteal procedures. Vascular 2006;14:63e9.
13. Faglia E, Mantero M, Caminiti M, et al. Extensive use of
peripheral angioplasty, particularly infrapopliteal, in the
treatment of ischaemic diabetic foot ulcers: clinical results
of a multicentric study of 221 consecutive diabetic subjects.
J Intern Med 2002;252:225e32.
14. Met R, van Lienden KP, Koelemay MJW, Bipat S,
Legemate DA, Reekers JA. Subintimal angioplasty for
peripheral arterial occlusive disease: a systematic review.
Cardiovasc Intervent Radiol 2008;31:687e97.
15. Engelhardt M, Boos J, Bruijnen H, et al. Critical limb
ischaemia: initial treatment and predictors of amputation-
free survival. Eur J Vasc Endovasc Surg 2012;43:55e61.
16. Iida O, Soga Y, Hirano K, et al. Midterm outcomes and risk
stratification after endovascular therapy for patients with
critical limb ischaemia due to isolated below-the-knee
lesions. Eur J Vasc Endovasc Surg 2012;43:313e21.
17. Giles KA, Pomposelli FB, Spence TL, et al. Infrapopliteal
angioplasty for critical limb ischemia: relation of Trans-
Atlantic InterSociety Consensus class to outcome in 176
limbs. J Vasc Surg 2008;48:128e36.
18. Kudo T, Chandra FA, Ahn SS. The effectiveness of percuta-
neous transluminal angioplasty for the treatment of critical
limb ischemia: a 10-year experience. J Vasc Surg 2005;41:
423e35.
19. Hanna GP, Fujise K, Kjellgren O, et al. Infrapopliteal trans-
catheter interventions for limb salvage in diabetic patients:
importance of aggressive interventional approach and role
of transcutaneous oximetry. J Am Coll Cardiol 1997;30:
664e9.20. Iida O, Soga Y, Hirano K, et al. Long-term results of direct
and indirect endovascular revascularization based on the
angiosome concept in patients with critical limb ischemia
presenting with isolated below-the-knee lesions. J Vasc
Surg 2012;55:363e70.
21. Varela C, Acın F, de Haro J, Bleda S, Esparza L, March JR.
The role of foot collateral vessels on ulcer healing and
limb salvage after successful endovascular and surgical
distal procedures according to an angiosome model. Vasc
Endovasc Surg 2010;44:654e60.
22. Varela C, Acın F, de Haro J, Bleda S, Esparza L, March JR.
Factors influencing wound healing of critical ischaemic
foot after bypass surgery: is the angiosome important in
selecting bypass target artery? Eur J Vasc Endovasc Surg
2012;43:322e8.23. Alexandrescu V, S€oderstr€om M, Venermo M. Angiosome
theory: fact or fiction? Scand J Surg 2012;101:125e31.
24. Lazaris AM, Salas C, Tsiamis AC, et al. Factors affecting
patency of subintimal infrainguinal angioplasty in patients

Vol. 27, No. 7, October 2013 Angioplasty in tibial occlusions 903
with critical lower limb ischemia. Eur J Vasc Endovasc Surg
2006;32:668e74.25. Dick F, Ricco J-B, Davies AH, et al. Chapter VI: follow-up
after revascularisation. Eur J Vasc Endovasc Surg 2011;
42(Suppl. 2):S75e90.26. Maca T, Ahmadi R, Derfler K, et al. Elevated lipoprotein(a)
and increased incidence of restenosis after femoropopliteal
PTA. Rationale for the higher risk of recurrence in females?
Atherosclerosis 1996;127:27e34.27. Shammas NW, Shammas G, Bryan D, Rauba J, Dippel E,
Jerin M. Predictors of target lesion revascularization in
patients undergoing lower extremity percutaneous inter-
ventions. J Invasive Cardiol 2009;21:266e9.
28. Pulli R, Dorigo W, Pratesi G, Fargion A, Angiletta D,
Pratesi C. Gender-related outcomes in the endovascular
treatment of infrainguinal arterial obstructive disease. J
Vasc Surg 2012;55:105e12.
29. DeRubertis BG, Vouyouka A, Rhee SJ, et al. Percuta-
neous intervention for infrainguinal occlusive disease in
women: equivalent outcomes despite increased severity
of disease compared with men. J Vasc Surg 2008;48:
150e7.30. Favaretto E, Pili C, Amato A, et al. Analysis of agreement
between Duplex ultrasound scanning and arteriography in
patients with lower limb artery disease. J Cardiovasc Med
(Hagerstown) 2007;8:337e41.