Embed Size (px)
Citation preview

Perceived Exercise Barriers, Enablers, and BenefitsAmong Exercising and Nonexercising Adults WithArthritis: Results From a Qualitative StudySARA WILCOX,1 CHERYL DER ANANIAN,1 JILL ABBOTT,2 JOELLEN VRAZEL,1 CORNELIA RAMSEY,1
PATRICIA A. SHARPE,1 AND TERESA BRADY3
Objective. Rates of participation in regular exercise are lower among individuals with arthritis than those withoutarthritis. This study examined perceived exercise barriers, benefits, and enablers in exercising and nonexercising adultswith arthritis.Methods. Twelve focus groups were conducted with 68 adults with arthritis. Groups were segmented by exercise status,socioeconomic status, and race. Focus group discussions were transcribed verbatim and coded. NVivo software was usedto extract themes for exercisers and nonexercisers.Results. A wide range of physical, psychological, social, and environmental factors were perceived to influence exercise.Some of these factors were similar to those in general adult samples, whereas others were unique to individuals withchronic disease. Symptoms of arthritis were barriers to exercise, yet improvements in these outcomes were also seen aspotential benefits of and motivations for exercise. Exercisers had experienced these benefits and were more likely to haveadapted their exercise to accommodate the disease, whereas nonexercisers desired these benefits and were more likelyto have stopped exercising since developing arthritis. Health care providers’ advice to exercise and the availability ofarthritis-specific programs were identified as needs.Conclusion. This study has implications for how to market exercise to individuals with arthritis and how communitiesand health care professionals can facilitate the uptake of exercise. These implications are discussed.
KEY WORDS. Arthritis; Exercise; Barriers; Benefits.
INTRODUCTION
Arthritis, the leading cause of disability in the UnitedStates, has a negative impact on health-related quality oflife (1). In total, the treatment of arthritis, its complica-tions, and resulting disability cost the United States an
estimated $86 billion per year (1997 US dollars), and thisnumber is expected to increase as the US population ages(2).
The National Arthritis Action Plan (3) and Healthy Peo-ple 2010 (4) underscore the importance of exercise amongpersons with arthritis. Exercise is a critical component ofdisease management (5–7). In randomized clinical trials,exercise (aerobic and resistance training) has been shownto reduce pain; delay disability; improve physical func-tion, postural sway, quality of life, aerobic capacity, andmuscle strength; and reduce the risk of other chronic con-ditions among individuals with arthritis (8–17).
Despite the well-documented benefits of exercise forarthritis management, rates of inactivity are higher in per-sons with arthritis than in those without (18). Althoughmuch research has focused on the correlates of exerciseamong adults in general (19), few studies have focused onunique factors for individuals with arthritis (20). Under-standing these factors among exercisers and nonexercisersmay help researchers and practitioners develop programs,tailor recruitment and retention strategies, and implementhealth communication messages more effectively. There-
The views expressed in this report are not the officialviews of the Centers for Disease Control and Prevention orthe Association of Schools of Public Health.
Supported by a grant from the US Centers for DiseaseControl and Prevention and the Association of Schools ofPublic Health (project S2109-22/22).
1Sara Wilcox, PhD, Cheryl Der Ananian, PhD, JoEllenVrazel, PhD, Cornelia Ramsey, PhD, MSPH, Patricia A.Sharpe, PhD: University of South Carolina, Columbia; 2JillAbbott, DrPH: The Ohio State University ComprehensiveCancer Center, Columbus; 3Teresa Brady, PhD: US Centersfor Disease Control and Prevention, Atlanta, Georgia.
Address correspondence to Sara Wilcox, PhD, Depart-ment of Exercise Science, Arnold School of Public Health,University of South Carolina, 1300 Wheat Street (Blatt),Columbia, SC 29208. E-mail: [email protected].
Submitted for publication June 14, 2005; accepted in re-vised form November 3, 2005.
Arthritis & Rheumatism (Arthritis Care & Research)Vol. 55, No. 4, August 15, 2006, pp 616–627DOI 10.1002/art.22098© 2006, American College of Rheumatology
ORIGINAL ARTICLE
616

fore, the major goal of this project was to understand thebarriers, enablers, and motivations for exercise, as well asthe perceived benefits and outcomes of exercise mostmeaningful to persons with arthritis. Special attention wasgiven to factors that differentiated exercisers from nonex-ercisers.
MATERIALS AND METHODS
Participants. This study was approved by the Univer-sity of South Carolina Institutional Review Board. Partic-ipants responded to advertisements in local newspapers,on local radio stations whose target audience is AfricanAmericans, and in flyers posted throughout communityestablishments. Recruitment was ongoing from May 2003through March 2004.
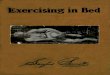
Participants expressing an interest in the study werescreened via telephone after providing oral consent. Eligi-ble participants were ages �18 years with any type ofdiagnosed arthritis and were classified as either exercisersor nonexercisers. All but one participant resided in Lex-ington or Richland County (i.e., greater metro area of Co-lumbia, SC). Groups were segmented by exercise status,socioeconomic status (operationalized as education lessthan or equal to high school versus greater than highschool), and race/ethnicity (Figure 1). Two focus groupswere conducted for each group. Segmentation creates ho-mogeneity along participant characteristics that are poten-tially related to the topic of interest and helps participantsfeel comfortable and willing to talk openly (21).
Procedures. Eleven experts in exercise and/or arthritisconvened via teleconference and provided input on factorsthat influence exercise, personally meaningful outcomesamong persons with arthritis, types of questions to askparticipants, how to segment groups, and how to recruit arepresentative sample. As a result of these calls and areview of the literature (20), 2 moderator’s guides weredeveloped, 1 for exercisers and 1 for nonexercisers. Themoderator’s guides were pilot tested to determine howwell the questions were understood by participants andcaptured participants’ experiences with exercise. At theconclusion of each pilot group, participants provided feed-back on the questions. Because significant changes weremade to the moderator’s guide for exercisers, participantsfrom this pilot group were not included in any analyses.Minimal changes were made to the moderator’s guide fornonexercisers.
Focus groups were moderated by 3 white women withmasters degrees who had training and experience conduct-ing focus groups and indepth interviews (10 groups weremoderated by 1 person). All focus groups were audio re-corded and transcribed verbatim, and transcripts were re-viewed for accuracy.
All individuals directly involved in coding and analysisattended 3 training sessions. All read the 12 focus grouptranscripts and generated a list of themes that were thenorganized into a code book with definitions. Two of 5coders were randomly assigned to code each of the 12focus groups, ensuring that coding pairs differed across thefocus groups. Each person independently coded the tran-script, and the pair met to review all codes and come to a
Figure 1. Recruitment of participants. The boxes at the bottom of the figure indicate the segmentation offocus groups that were completed. Two groups were conducted for each population subgroup. Thenumbers in parentheses indicate the number of persons. Ex � exercise; FG � focus group; PI � privateinvestigator; SES � socioeconomic status.
Exercise and Arthritis 617

consensus. Consensus codes for all focus groups wereentered into NVivo (QSR International, Doncaster, Victo-ria, Australia). Throughout the coding process, new codesand their definitions were discussed, added as needed,and shared with all coders, and previously coded tran-scripts were recoded to reflect these changes.
The focus group (rather than individual participants)was the unit of analysis. In focus groups, participants oftenexpress agreement with one another by nodding and shak-ing their heads, thus an analysis of simple frequencycounts of themes is not a good indicator of the importanceof a theme. Results are reported according to how manygroups of exercisers and nonexercisers expressed thetheme. One limitation of focus groups is that some mem-bers may not feel comfortable expressing contradictoryviews. To minimize this potential, we recruited homoge-neous groups to prevent acquiescence to opinions of indi-viduals with higher status, and the moderators weretrained to prompt individuals who did not respond toquestions or who did not nod in agreement.
Additional measures. Sociodemographics and back-ground information. Participants reported their age, sex,race, educational attainment, income, and employmentstatus. Participants also reported their arthritis type (basedon a physician’s diagnosis) and duration (years).
Physical activity. A modified version of the 2001 Behav-ioral Risk Factor Surveillance System physical activitymodule was administered during the telephone screening(22). The questions were modified to obtain informationon structured exercise only. Participants reported the type,frequency, and duration of their moderate-intensity, vig-orous, and strengthening structured activities.
Participants were classified into 1 of 2 groups. Exercisersparticipated in moderate activities on at least 3 days perweek for �30 minutes per day, vigorous activities on atleast 3 days per week for �20 minutes per day, or strengthtraining on at least 3 days per week for �20 minutes perday. Participating in exercise at this level has been shownto yield health benefits in individuals with arthritis. Non-exercisers were those who exercised (any amount) on 0 or1 day per week, or who exercised for �10 minutes on 2days per week. Those who did not fall into one of these 2groups were ineligible.
RESULTS
Characteristics of participants. The flow of participantsthrough the recruitment process is shown in Figure 1. Ofthe 75 participants who took part in a focus group (includ-ing the 7 who took part in the pilot group of exercisers), themost common recruitment sources were newspaper adver-tisements (n � 26) and fitness and community-based well-ness facilities (n � 14). Characteristics of the 68 focusgroup participants retained in the analyses are shown inTable 1.
Focus group findings: barriers to exercise. Participantsdiscussed barriers to exercise as well as factors that made
exercise more difficult. Themes and illustrative quotationsfor barriers are listed in Tables 2 and 3.
Physical barriers. Pain. Pain was described as a barrierto exercise in all focus groups and was the single mostdiscussed topic. Pain was described in 3 ways: the occur-rence of pain prevented a person from exercising, experi-encing pain during exercise made a person not want toexercise, and pain experienced after exercise decreased aperson’s willingness to participate in future exercise. Al-though similar themes emerged for exercisers and nonex-ercisers, exercisers were more likely to make adaptationsto their exercise (e.g., modify type or intensity, take arespite during arthritis flares) and work through pain toattain benefits, whereas nonexercisers were more likely togive up exercise altogether.
Fatigue. Exercisers and nonexercisers described fatigueas being a barrier to exercise or making exercise moredifficult. Although both groups were willing to modifytheir activities in response to fatigue, nonexercisers moreoften decreased frequency, whereas exercisers were morelikely to adjust other aspects of their exercise, such asintensity. Participants attributed their fatigue to a varietyof factors, including medication, insomnia, and depres-sion.
Mobility. Most commonly, exercisers and nonexercisersdescribed impaired mobility as a major challenge to exer-cise. Nonexercisers also discussed decreased mobility af-ter engaging in exercise.
Comorbid conditions. Comorbid conditions were de-scribed as barriers to exercise more often among exercisersthan nonexercisers. These conditions ranged from muscu-loskeletal to cardiovascular ailments. Nonexercisers andexercisers experienced similar comorbidities; however,only nonexercisers described asthma (2 groups).
Psychological barriers. Attitudes and beliefs. Lack oftime, motivation, and enjoyment of exercise and the sen-timent that “I should but I don’t” were cited by exercisersand nonexercisers alike. Whereas nonexercisers describedthese factors as barriers to exercise, exercisers describedthem as factors that made exercise more difficult.
Exercisers were also more likely than nonexercisers totalk about how other life activities took priority over exer-cise, making it difficult to fit in exercise. Nonexerciserswere much more likely than exercisers to describe theirbelief that they were physically unable to exercise andunskilled to exercise.
Fear. Among nonexercisers, participants’ fear of waterand fear of experiencing pain were barriers. The fear ofwater prevented them from participating in water aerobics,an exercise they believed to be safe and effective for indi-viduals with arthritis.
Perceived negative outcomes. This theme emerged as abarrier for both exercisers and nonexercisers. Almost all ofthe comments were based on actual experiences. The gen-eral consensus was that individuals were going to “pay forit” afterwards, although the outcomes mentioned werevaried and sometimes nonspecific. For some, the potentialnegative outcomes were accepted as part of the exercise
618 Wilcox et al

Table 1. Sociodemographic and physical activity–related characteristics of the sampleby exercise status*
CharacteristicExercisers(N � 36)
Nonexercisers(N � 32)
Type of arthritis (self-reported as physiciandiagnosed), no.†
36 31
Osteoarthritis 16 (44.4) 16 (51.6)Rheumatoid arthritis 14 (38.9) 8 (25.8)Fibromyalgia 6 (16.7) 11 (35.5)Gout 1 (2.8) 2 (6.4)Other (includes those not
sure of type)8 (22.2) 6 (19.4)
Years with arthritis, no.(mean � SD)
31 (12.50 � 10.71) 28 (12.57 � 8.24)
Age, no. (mean � SD years) 36 (58.8 � 15.0) 32 (56.9 � 10.6)Education, no. (mean � SD
years)36 (13.6 � 3.0) 32 (13.1 � 2.2)
Sex‡ 36 32Female 27 (75.0) 30 (93.8)Male 9 (25.0) 2 (6.2)
Marital status§ 36 30Married 13 (36.1) 16 (53.3)Widowed 8 (22.2) 4 (13.3)Divorced or separated 7 (19.5) 7 (23.3)Not married 6 (16.7) 2 (6.7)Living with partner 2 (5.6) 1 (3.3)
Race or ethnicity§ 36 32White 23 (63.9) 15 (46.9)Black/African American 13 (36.1) 13 (40.6)Hispanic 0 (0) 1 (3.1)American Indian 0 (0) 1 (3.1)Not specified 0 (0) 2 (6.3)
Occupational status§ 36 31Employed
Full time 11 (30.5) 5 (16.1)Part time 3 (8.3) 3 (9.7)
Retired 13 (36.1) 13 (41.9)Unemployed 6 (16.7) 6 (19.3)Homemaker 2 (5.6) 2 (6.5)Student 1 (2.8) 2 (6.5)
Income 31 250–$29,999 13 (42.0) 16 (64.0)$30,000–$59,999 9 (29.0) 6 (24.0)�$60,000 9 (29.0) 3 (12.0)
Minutes of physical activityper week, mean � SD
36 32
Total minutes¶ 230.6 � 124.7 9.22 � 20.2Strength minutes¶ 54.9 � 66.1 0.8 � 3.2Moderate minutes¶ 146.1 � 89.9 5.8 � 13.9Vigorous minutes‡ 33.6 � 70.4 2.8 � 15.9
Percentage meeting thephysical activityrecommendations†
Strength 12 (33.3) –Moderate 29 (83.0) –Vigorous 6 (16.7) –
* Values are the number (percentage) unless otherwise indicated.† Categories are not mutually exclusive; therefore, the percentages can add up to greater than 100%.‡ Groups differ significantly (P � 0.05).§ Due to the small sample size in some cells, differences between groups were examined for thepercentage of participants who were white versus nonwhite, employed versus not employed, and marriedor partnered versus neither married nor partnered. No significant differences were found.¶ Groups differ significantly (P � 0.001).
Exercise and Arthritis 619

Tab
le2.
Su
mm
ary
ofp
hys
ical
and
psy
chol
ogic
alba
rrie
rsto
exer
cise
amon
gex
erci
sers
and
non
exer
cise
rsw
ith
arth
riti
s(n
�6
focu
sgr
oup
sea
ch)
Key
them
esan
dsu
bcat
egor
ies
Exe
rcis
ers
Non
exer
cise
rs
nIl
lust
rati
vequ
otat
ion
sn
Illu
stra
tive
quot
atio
ns
Ph
ysic
alP
ain Bef
ore
exer
cise
3“W
hen
you
hav
ea
flar
e-u
pan
dyo
ur
join
tsbe
com
esw
olle
nan
din
flam
ed..
.th
enyo
ure
ally
can
’tex
erci
se.”
5“T
he
reas
onI
hav
en
otm
ade
anat
tem
pt
togo
into
anex
erci
secl
ass
beca
use
,wel
l,I
hu
rtso
bad
.”D
uri
ng
exer
cise
6“I
wou
ldlo
veto
beab
leto
wal
km
uch
ofth
em
all.
..bu
tI
can
wal
ka
litt
lew
hil
ean
dsi
td
own
onon
eof
thos
ebe
nch
esan
dre
stan
dle
tth
ew
orst
ofth
ep
ain
calm
dow
n,a
nd
Ica
nw
alk
ali
ttle
bit
mor
eto
anot
her
ben
ch,a
nd
Im
ake
itth
atw
ay.”
5“[
Art
hri
tis]
isw
hat
mad
eit
sop
ain
ful
now
tod
oth
esa
me
thin
gI
use
tod
o,bu
tI
was
onan
exer
cise
pro
gram
tost
ren
gth
enm
ym
usc
les
and
join
tsbe
cau
seth
eor
thop
edic
told
me
tod
oit
,an
dth
enn
oww
hen
Id
oit
,it’s
like
you
are
stra
inin
gyo
ur
mu
scle
s,an
dyo
uh
urt
mor
e.”
Aft
erex
erci
se5
“Id
olo
veto
dan
ce..
.an
dI
wil
ld
om
ybe
stto
han
gin
ther
ew
ith
ever
ybod
yel
se,k
now
ing
the
con
sequ
ence
sth
en
ext
day
...Y
oukn
owyo
uar
ego
ing
toh
urt
.”
6“W
ell,
exer
cise
for
me
defi
nit
ely
cau
ses
the
pai
n.”
Fat
igu
e5
“Ih
ave
fibr
omya
lgia
,an
dm
yp
robl
emm
ore
than
pai
n,I
mea
n,I
hav
ep
ain
,bu
tto
me,
the
pro
blem
ism
ore
fati
gue,
and
Iu
sed
tori
de
bike
san
dd
om
ore
vigo
rou
sex
erci
se,a
nd
once
Igo
tfi
brom
yalg
ia,I
just
hav
eto
pu
shm
ysel
fto
mak
em
ysel
fex
erci
se.”
5“M
yh
ouse
isal
way
sin
fron
tof
me
like
am
oun
tain
tocl
imb,
and
Id
ow
hat
Ica
nan
dth
enI
got
tosi
td
own
agai
n..
.Aft
era
wh
ile,
som
etim
esyo
uju
stgi
veu
p,a
nd
you
goto
bed
,an
dI’m
sup
pos
edto
beex
erci
sin
g.”
Imp
aire
dm
obil
ity
Imp
edim
ent
toex
erci
se3
“Wh
enit
flar
esu
p..
.Ica
n’t
turn
over
inth
ebe
d.I
can
’tge
tou
tto
wal
k.I’m
like
a90
-yea
rol
dp
erso
nth
atre
ally
can
’tw
alk.
”3
“Now
Ica
n’t
wal
kth
atfa
rbe
cau
sem
ykn
eew
ill
not
allo
wm
eto
wal
k,an
dI
mea
nI
can
’tke
epu
pw
ith
my
hu
sban
d.”
Res
ult
ofex
erci
se1
3“
...
and
Id
on’t
get
the
exer
cise
like
Iw
ould
like
tobe
cau
se,w
hen
Iw
alk
ace
rtai
nd
ista
nce
,Ige
tto
wh
ere
Ica
n’t
har
dly
go..
.an
dif
itge
tsre
alse
vere
,Iu
sual
lyen
du
pin
the
bed
.”C
omor
bid
con
dit
ion
s5
“Bu
tex
erci
seh
ew
ante
dm
eto
do
...h
esa
idit
wou
ldm
ake
itw
orse
beca
use
Ih
adp
sori
asis
onm
ykn
ees
and
my
feet
and
legs
...t
hey
wou
ldcr
ack
and
was
real
sore
,an
dh
esa
idth
eex
erci
seth
ath
ew
ould
wan
tm
eto
do
wou
ldm
ake
itw
orse
.”
3“W
ell,
shou
ldI
goan
dtr
yth
eaq
uat
ics
and
get
exer
cise
,or
shou
ldI
goou
tan
dtr
yto
wal
kag
ain
?B
ut
Ih
ave
asth
ma,
soI
don
’tw
ant
togo
out
inth
ish
eat
and
wal
k.S
o,it
’sli
kea
catc
h-2
2.W
her
ed
oyo
ugo
?”
Psy
chol
ogic
al/b
ehav
iora
lA
ttit
ud
esan
dbe
lief
sL
ack
ofti
me
5“I
don
’th
ave
the
tim
eto
real
lyw
alk
ever
yd
ayan
dth
at’s
wh
atI
wou
ldli
keto
do,
and
that
’son
eof
the
barr
iers
for
me
isth
eti
me.
”3
“If
Ih
adth
eti
me
and
wer
eab
leto
do
thos
eex
erci
ses,
they
wou
ldh
elp
.”
Ish
ould
but
Id
on’t
3“I
pro
babl
yw
ould
not
goif
itw
ere
left
up
tom
e,bu
tn
owI
know
it’s
good
for
me.
”4
“..
.Id
on’t
know
wh
at’s
inm
ym
ind
that
’ske
epin
gm
efr
omit
.On
ed
octo
rto
ldm
e,h
esa
ys,‘
Itm
aym
ean
you
rli
feif
you
exer
cise
.’N
ow,y
outh
ink
that
wou
ldbe
enou
ghm
otiv
atio
n.I
’mst
ill
not
doi
ng
it.I
tbu
gsm
eth
atI’m
such
afa
ilu
reat
that
.”L
ack
ofen
joym
ent
3“T
he
doc
tor
has
just
ord
ered
me
into
anex
erci
secl
ass,
and
I’m,y
oukn
ow,fi
ghti
ng
and
kick
ing
ital
lth
ew
ay..
.Igo
tto
tell
you
,for
the
last
10ye
ars
ofm
yli
fe,I
wou
ldd
op
rett
ym
uch
anyt
hin
gra
ther
than
exer
cise
.”
3“I
hat
eex
erci
se.I
just
hat
eit
.It’s
the
mos
tbo
rin
gth
ing
inth
ew
orld
togo
toa
clu
ban
dp
ick
up
litt
lew
eigh
ts,a
nd
I’ve
don
eit
,an
dit
just
bore
dm
eto
tear
s..
.bor
edom
...e
ven
trie
dth
etr
ead
mil
lin
fron
tof
the
TV
.It’s
aw
aste
ofti
me.
You
don
’tac
com
pli
shan
yth
ing.
”N
ota
pri
orit
y4
“You
hav
eto
take
tim
e.I
hav
eto
beab
leto
god
own
ther
ean
dd
oth
isif
Id
idn
’th
ave
tost
ayh
ome
and
cook
,bu
tyo
ukn
ow,i
t’sju
stti
me
con
sum
ing,
and
itju
stta
kes
away
from
bein
gat
hom
e..
.By
the
end
ofth
ed
ay,I
’ve
had
enou
gh..
..”
2“A
nd
her
eI
amat
hom
eby
mys
elf
and
wh
enI
do
star
tfe
elin
gbe
tter
,you
know
,Ith
ink
I’mm
aybe
In
eed
toex
erci
se..
..Y
oukn
ow,I
’llp
rocr
asti
nat
efo
r,I
mea
n,I
’llev
enco
okw
hic
hI
don
’td
o.I’l
lev
end
oth
atbe
fore
I’ll
exer
cise
.”
Ip
hys
ical
lyca
n’t
14
“Id
idae
robi
cs,a
nd
Ilo
ved
it,b
ut
Ica
n’t
do
aero
bics
.Ica
n’t
do
step
beca
use
Ica
n’t
step
up
and
step
back
beca
use
ofm
yfe
etan
dm
ykn
ees.
Ica
n’t
run
.Ica
n’t
stoo
p.I
can
’tsq
uat
.Ica
n’t
get
dow
non
the
floo
r.If
Ige
ton
the
floo
r,I
can
’tge
tu
p.”
I’mn
otsk
ille
den
ough
14
“Eve
rybo
dy
else
isgo
od,s
oI
don
’tw
ant
tobe
arou
nd
them
,you
know
,an
dI’m
ah
erm
it.”
Fea
r0
3“I
’ve
been
told
totr
yw
ater
aero
bics
,bu
tI’m
not
aw
ater
per
son
.I’m
terr
ified
ofw
ater
,so
that
doe
sn’t
wor
kw
ith
me.
”P
erce
ived
outc
omes
Neg
ativ
eou
tcom
es5
“Cau
seI
fin
d..
.th
atif
Ire
ally
do
goou
t,I
like
tow
alk
atle
ast
3m
iles
.If
I...
som
etim
esif
Id
o3
mil
es,I
’mgo
ing
top
ayfo
rit
,so
Ih
ave
toba
ckof
f.I
can
’td
oas
mu
ch,a
nd
Ih
ave
toge
tth
atin
my
hea
d.”
6“I
fI
wan
tto
...i
fI
feel
like
Ire
ally
wan
tto
do
som
eth
ing
...t
oh
ave
fun
wit
hex
erci
sin
g,I
do
it,a
nd
Isu
ffer
the
con
sequ
ence
sla
ter.
”
Lac
kof
pos
itiv
eou
tcom
es0
4“I
hav
ebe
ensw
imm
ing
and
aero
bics
,bu
tn
one
ofth
ath
elp
edm
eat
all.
Not
hin
g.N
ota
thin
g.I
stil
lh
ave
that
pai
n.”
620 Wilcox et al

Tab
le3.
Su
mm
ary
ofso
cial
and
envi
ron
men
tal
barr
iers
toex
erci
seam
ong
exer
cise
rsan
dn
onex
erci
sers
wit
har
thri
tis
(n�
6fo
cus
grou
ps
each
)
Key
them
esan
dsu
bcat
egor
ies
Exe
rcis
ers
Non
exer
cise
rs
nIl
lust
rati
vequ
otat
ion
sn
Illu
stra
tive
quot
atio
ns
Soc
ial
Lac
kof
sup
por
tL
ack
ofen
cou
rage
men
tfo
rex
erci
se2
“My
hu
sban
d,h
ekn
ows
wh
atI
goth
rou
gh,w
hat
I’ve
had
don
eto
me
and
he’
llsa
y,‘y
ouai
n’t
got
no
busi
nes
sd
oin
gth
at.Y
oukn
ow,y
oukn
owh
owyo
uar
e,yo
ukn
ow.’
So
he
doe
sn’t
enco
ura
gem
e,be
cau
seh
ed
oesn
’tw
ant
the
afte
rmat
hof
it.B
ut
my
dau
ghte
ris
tru
lym
ych
eerl
ead
er.”
3“
...
Id
on’t
hav
ean
ybod
yth
atca
res
wh
atI
do.
Im
ean
,Ili
veby
mys
elf,
and
Iw
ould
imag
ine
ifI
had
am
anor
ifI
had
ach
ild
orso
met
hin
gth
atsa
id,‘
Com
eon
,go,
Mom
’...
You
know
,my
bird
doe
sn’t
care
wh
atI
do
...N
obod
yre
ally
care
s,so
wh
ysh
ould
I...
You
know
,Id
on’t
hav
ean
ybod
ysa
yin
g,‘G
o,ga
l,go
.’”
Lac
kof
ackn
owle
dgm
ent
ofar
thri
tis
12
“Wh
enI
do
wal
kw
ith
my
hu
sban
d,h
e’s
abou
t3
step
sah
ead
ofm
e,an
dh
eke
eps
gett
ing
fart
her
and
fart
her
ahea
dof
me,
and
he
doe
sn’t
un
der
stan
dw
hy
Ica
n’t
keep
up
wit
hh
im.
Th
at’s
wh
yI
amju
stgl
adth
ath
e’s
got
the
lad
ies
inth
en
eigh
borh
ood
he
can
wal
kw
ith
.Now
,Id
on’t
hav
eto
goou
tan
dtr
yto
wal
k.”
Doc
tor
did
not
men
tion
exer
cise
3“T
hey
nev
erm
enti
oned
it.T
he
firs
tth
ing
they
say
is,‘
We
do
abl
ood
test
.Oh
,yo
u’v
ego
trh
eum
atoi
dar
thri
tis.
Her
e,ta
keth
is.’
Oka
y,th
atm
akes
me
sick
.‘O
kay,
take
this
.’T
hat
gave
me
ara
sh.‘
Oka
y,ta
keth
is.’
Th
atgi
ves
me
the
hiv
es.‘
Oka
y,ta
ke2
ofth
ese.
’Oh
,th
at’s
mak
ing
me
swel
l.‘W
ell,
take
ash
otof
this
.’”
3“M
yd
octo
rn
ever
told
me
not
hin
gab
out
itbe
cau
seI
befu
ssin
gw
ith
him
all
the
tim
eab
out
me.
Ica
n’t
wal
k,an
dh
eai
n’t
nev
erte
llm
en
oth
ing
abou
tw
hat
tod
oor
no
pla
ceto
go,y
oukn
oww
hat
Im
ean
...n
oth
ing
like
that
.”
Doc
tor
did
not
refe
rto
pro
gram
s0
3“I
wil
lsa
yth
is..
.th
ere
isve
ryli
ttle
bein
gp
asse
dar
oun
dth
at’ll
tell
you
,‘Y
ouca
ngo
her
e,or
you
can
goth
ere.
’It’s
sort
ofa
wor
d-o
f-m
outh
thin
g.”
Doc
tor
did
not
give
exer
cise
inst
ruct
ion
2“H
ega
vem
ea
pam
ph
let
that
had
mov
emen
tin
it.S
tret
chin
gex
erci
sean
dsi
t-u
ps
and
roll
ing
ina
ball
and
doi
ng
all
that
tost
retc
hyo
ur
back
out,
and
he
did
n’t
real
lysh
owm
eh
owto
do
any.
He
just
give
me
this
pie
ceof
pap
eran
dsa
id,‘
Her
e.’”
0
No
one
toex
erci
sew
ith
3“I
thin
kif
Ih
adso
meb
ody
toex
erci
sew
ith
...s
omet
imes
wh
enI
do
wan
tto
go,I
don
’th
ave
enou
ghm
otiv
atio
n..
.lik
eif
Iw
ant
tow
alk
...S
omet
imes
Id
on’t
hav
ean
ybod
yto
do
anyt
hin
gw
ith
.Th
atge
tsin
the
way
.”
5“I
fI
had
som
eon
e,yo
ukn
ow,a
par
tner
that
Iw
asd
oin
git
wit
h,t
hat
mot
ivat
esm
em
ore
tow
alk
and
exer
cise
...”
Com
pet
ing
role
resp
onsi
bili
ties
2“I
fyo
u’r
ew
orki
ng
and
hav
ea
fam
ily,
it’s
real
lyex
tra,
extr
ah
ard
and
then
ifyo
u’r
eh
urt
ing
besi
des
,Ica
nim
agin
eit
’sev
enm
ore
dif
ficu
lt.”
4“[
Exe
rcis
ing]
exh
aust
sm
e.I
mea
n,i
tw
asba
den
ough
...I
do
the
lau
nd
ryan
dta
kin
gca
reof
the
kid
san
dco
okin
gan
dw
orki
ng
and
ever
y..
.I’d
bed
a’go
ned
ifI
was
gon
na
go,
you
know
,jog
for
am
ile,
you
know
.No,
no,
no.
Not
for
me.
”E
nvi
ron
men
tal
Pro
gram
sor
faci
liti
es:l
ack
ofar
thri
tis-
spec
ific
faci
liti
es5
“Th
ere
are
som
eof
the
oth
erh
ealt
hcl
ubs
and
spas
and
sofo
rth
that
do
wat
erae
robi
cs,b
ut
they
don
’tke
yto
arth
riti
sor
fibr
omya
lgia
orjo
int
rep
lace
men
tli
keth
eyd
oth
ere,
and
it’s
not
wor
kin
gou
tw
ell
wit
hth
embe
cau
seI
had
one
frie
nd
...t
her
ew
asa
pla
ce..
.th
atw
asa
litt
lecl
oser
toh
erh
ouse
,an
dsh
etr
ied
them
,an
dsh
eco
uld
not
do
the
exer
cise
sth
ere.
Th
eyw
ere
not
keye
dto
war
da
per
son
wh
oh
adjo
int
pro
blem
sor
anyt
hin
gli
keth
at,a
nd
you
just
cou
ldn
’td
oth
emw
ith
out
dam
agin
gyo
urs
elf.”
6“I
don
’tkn
own
oth
ing
like
that
arou
nd
her
e.I
hav
en’t
hea
rd.
Ifit
is,I
hav
en’t
hea
rdab
out
it,y
oukn
ow.I
tm
igh
tbe
,bu
tI
hav
en’t
hea
rdab
out
it.”
En
viro
nm
enta
lco
nd
itio
ns
5“[
Rai
n]
mes
ses
up
you
rkn
ees.
Itm
esse
su
pyo
ur
back
.You
don
’tfe
elli
kege
ttin
gu
pan
dd
oin
gan
yth
ing
real
ly.”
4“B
ut
Ih
ave
asth
ma
soI
don
’tw
ant
togo
out
inth
ish
eat
and
wal
k.S
oit
’sli
kea
catc
h-2
2.W
her
ed
oyo
ugo
?”C
ost
2“T
he
oth
eron
ew
asat
the
Yan
dn
um
ber
one
the
Yis
just
too
dar
ned
exp
ensi
vean
ymor
e.”
3“E
very
pla
ceI’v
ech
ecke
d,e
ven
atch
urc
hes
,you
know
,Ica
nn
otaf
ford
itbe
ing
ond
isab
ilit
y.”
Tra
nsp
orta
tion
03
“Wel
l,I
did
n’t
hav
etr
ansp
orta
tion
for
aw
hil
eei
ther
.”
Exercise and Arthritis 621

experience. Both exercisers and nonexercisers concurredthat negative outcomes generally resulted from pushingbeyond one’s limits.
Nonexercisers expressed the theme that exercise mightnot be “worth it” if it did not help their symptoms. Partic-ipants questioned the need for exercise when it did notseem to positively affect their arthritis symptoms.
Social barriers. Lack of support. Not having supportfrom family, friends, and health care providers was ex-pressed in different ways. Some exercisers and nonexer-cisers stated that although their significant others did notdiscourage them from exercise, no one really encouragedthem to do so. Other participants, more commonly nonex-ercisers, expressed the notion that significant others didnot acknowledge their physical limitations and were notsympathetic to their struggles.
Exercisers and nonexercisers also described their healthcare providers’ emphasis on medication and failure tomention exercise. Whereas nonexercisers said that theirphysicians did not refer them to helpful exercise pro-grams, exercisers were more likely to discuss how theirphysicians did not instruct them on how to exercise prop-erly.
No one to exercise with. Although both groups de-scribed how the lack of an exercise partner was a barrier,this theme was more common among nonexercisers. With-out exercise partners, frequency of exercise decreased. Forboth groups, ideal exercise partners were those who pre-ferred similar exercise schedules and who lived close by.Nonexercisers also desired exercise partners with similarabilities.
Competing role responsibilities. Feelings of responsibil-ity to one’s family emerged as a barrier to exercise, espe-cially among nonexercisers. Nonexercisers reported lessenergy as a result of their competing roles, whereas exer-cisers described how they were left with less time to en-gage in exercise.
Environmental barriers. Lack of programs or facilities.In almost all groups, the lack of exercise programs orfacilities specifically for persons with arthritis emerged asa barrier. Although participants acknowledged nearby fit-ness clubs, there were few programs or facilities that mettheir specific needs. Some participants were aware of fa-cilities and programs but said they were too far away toattend regularly. Others described a lack of qualified in-structors, particularly those who understood physical lim-itations.
Environmental conditions. Weather, including hot andcold weather and rain, was the most common environmen-tal barrier cited by exercisers and nonexercisers. Both coldweather and damp, rainy weather were barriers in partbecause they aggravated symptoms of arthritis. Other en-vironmental conditions that impeded exercise includedcongested parking, concrete surfaces, presence of dogs,and lack of sidewalks.
Cost. Cost of programs emerged as a barrier to exerciseamong both groups, but cost seemed to be especially pro-hibitive among nonexercisers who lived on a limited in-
come and sometimes described being uninsured or under-insured, often due to disability.
Transportation. Among nonexercisers, lack of transpor-tation to facilities or programs was a barrier. It was unclearwhether the respondents did not have access to transpor-tation or were not capable of driving because of theirarthritis.
Focus group findings: exercise benefits and enablers.Participants discussed the advantages and benefits thatmay result or have resulted from exercise, identified thesingle outcome that made or would make exercise worthdoing, and described what would motivate them or make iteasier for them to start or continue an exercise program.The themes and illustrative quotations are listed in Tables4 and 5.
Physical benefits and enablers. Symptom management.In all groups, participants described how exercise couldreduce pain. Although some participants quickly notedthat exercise did not stop pain, many stated that it de-creased the severity and intensity of pain enough to makeit more manageable. Those who exercised were generallymore positive because they had experienced pain reduc-tion and other benefits. In contrast, nonexercisers ex-pressed more doubt that exercise would reduce their pain.Approximately half of the responses from nonexercisersresulted from being asked to identify the one outcome thatwould make exercise worth doing or would motivate themto start exercising.
Reduced stiffness was described similar to pain reduc-tion among exercisers and nonexercisers, although it wasmore commonly cited by exercisers. Exercisers also citedincreased energy more often than nonexercisers. Fewergroups described improved sleep, the prevention of dis-ease progression, and decreased use of medications asbenefits.
Mobility and function. Participants in all groups statedthat exercise gave them the ability to move and function,not necessarily at a normal level, but at least at a level thatallowed them to function in life and conduct everydayactivities. Mobility was a critical outcome for enablingthem to cope with arthritis. Exercisers repeatedly ex-pressed the theme of “use it or lose it.” There was animportant distinction between groups. Nonexercisers de-scribed wanting to return to the life they had before arthri-tis when they were able to function normally, whereasexercisers discussed how exercise enabled them to live amore normal life. Many exercisers added that if they didnot move, they would “lock up,” “freeze up,” or “shutdown.” Several participants stated that they would be“crippled” if they did not exercise. Nonexercisers oftenused phrases such as “this is what I hear,” “I don’t knowbut maybe,” or “this is what I understand” to describe themobility and function benefits or desired outcomes.
Strength and flexibility. Increased strength was viewedas an important component to improving mobility andfunctioning by exercisers and nonexercisers alike. Severalnonexercisers noted that building muscles around a jointor strengthening muscles would enhance mobility. In-creased flexibility was a similar theme. In general, both
622 Wilcox et al

Tab
le4.
Su
mm
ary
ofp
erce
ived
ph
ysic
alan
dp
sych
olog
ical
ben
efits
and
enab
lers
ofex
erci
seam
ong
exer
cise
rsan
dn
onex
erci
sers
wit
har
thri
tis
(n�
6fo
cus
grou
ps
each
)
Key
them
esan
dsu
bcat
egor
ies
Exe
rcis
ers
Non
exer
cise
rs
nIl
lust
rati
vequ
otat
ion
sn
Illu
stra
tive
quot
atio
ns
Ph
ysic
alS
ymp
tom
man
agem
ent
Red
uce
dp
ain
6“I
t’sbe
gin
nin
gto
feel
bett
er.N
oth
urt
ing
asba
das
you
did
and
bein
gab
leto
do
thin
gsth
atyo
uco
uld
n’t
do
befo
re.I
’mst
ill
lim
ited
but
man
it’s
sod
iffe
ren
tn
ow.A
nd
that
’sw
hy
Igo
reli
giou
sly
...”
6“S
top
the
pai
n.I
fI
cou
ldge
tso
me
ofth
ere
sult
sI
use
dto
get
befo
reth
ep
ain
,th
atw
ould
mak
em
eke
epgo
ing.
”
Red
uce
dst
iffn
ess
6“I
t’sju
stth
atif
Id
on’t
keep
exer
cisi
ng,
then
ever
ym
orn
ing
I’mst
iffe
rlo
nge
rin
the
mor
nin
gth
anif
Id
on’t
exer
cise
...
Ith
ink
pre
tty
soon
I’dju
stbe
sitt
ing
ina
chai
rn
otab
leto
go.”
4“A
nd
sow
ith
the
mov
emen
tit
reli
eves
som
eof
the
stif
fnes
s.”
Incr
ease
den
ergy
3“
...t
he
mor
eI
pu
shed
mys
elf
tod
oso
met
hin
gli
kest
epcl
ass,
Ico
uld
n’t
beli
eve
how
mu
chen
ergy
Ih
ad.A
nd
wh
enI
slee
pn
owI
don
’tu
sual
lyw
ake
up
.Isl
eep
thro
ugh
the
nig
ht
and
Ica
nge
t9
hou
rsan
dbe
alo
tm
ore
fun
ctio
nal
.”
1
Mob
ilit
yan
dfu
nct
ion
6“T
he
exer
cise
that
Id
o,I
pu
shm
ysel
fto
do
it.B
ecau
seI
know
that
ifI
did
n’t
do
som
eth
ing
that
Iw
ill
even
tual
lybe
crip
ple
d.I
’ve
been
toth
ep
oin
tto
wh
ere
I,yo
ukn
ow,w
asei
ther
had
tobe
ina
wh
eel
chai
r,h
adto
use
aw
alke
r,or
,you
know
,ju
styo
uco
uld
n’t
do
not
hin
g.Y
ouco
uld
n’t
mak
ea
fist
.You
cou
ldn
’tw
alk
oran
yth
ing.
”
6“B
ut
Id
idfi
nd
that
my
orth
oped
icto
ldm
eto
exer
cise
asfa
ras
doi
ng
leg
lift
san
dth
ings
and
that
wou
ldto
buil
dth
em
usc
les
up
arou
nd
my
knee
san
don
ceI
buil
tth
em
usc
les
up
arou
nd
my
knee
s,th
atw
ould
hel
pm
en
otto
bein
such
pai
nor
beab
leto
wal
kan
dbe
mor
em
obil
e.”
Act
ivit
ies
ofd
aily
livi
ng
4“M
ybi
gges
tm
otiv
atio
nI
thin
kis
that
Iw
ant
tobe
able
toco
nti
nu
eto
do
thin
gsm
ysel
f.W
hen
Ifi
rst
cam
ed
own
wit
hm
yar
thri
tis
ther
ew
ere
som
any
thin
gsI
cou
ldn
’td
o.L
ike
azi
pp
eror
do
abu
tton
....
and
the
mor
eI
exer
cise
and
stay
mob
ile
the
mor
eI
can
do
for
mys
elf.”
3“I
wou
ldli
keto
get
back
inth
eli
feth
atI
use
dto
hav
e,to
beab
leto
get
out
and
do
thin
gsw
ith
my
chil
dre
nth
atI
use
dto
do
and
gop
lace
sI
use
dto
goan
dn
otw
orry
abou
th
urt
ing
late
r.E
very
day
thin
gs..
..I’d
like
toge
tou
ton
ed
ayan
dju
stcl
ean
my
wh
ole
hou
se.I
t’sju
stto
tall
yim
pos
sibl
e...
.”S
tren
gth
and
flex
ibil
ity
4“T
obe
nd
dow
nto
pic
kgr
een
bean
sor
som
eth
ing
my
legs
wer
eju
st..
.th
ere’
sn
ost
ren
gth
ther
ean
dth
ere’
sa
big
trem
end
ous
dif
fere
nce
wit
hth
ew
eigh
tm
ach
ines
.So
Igo
3ti
mes
aw
eek
for
abou
tan
hou
rea
chti
me
and
itju
stke
eps
the
mu
scle
sfr
omd
eter
iora
tin
g.”
4“I
thin
kth
atex
erci
seth
atst
ren
gth
ens
you
rbo
dy
...l
ike
wit
har
thri
tis
and
wit
hag
eyo
ust
art
losi
ng
you
rp
ostu
re,
and
Ith
ink
ifyo
uco
uld
do
exer
cise
sm
aybe
like
wei
ght-
bear
ing
exer
cise
sth
atyo
ud
ow
ith
wei
ghts
and
thin
gsth
atw
ould
stre
ngt
hen
som
eof
the
par
tsof
you
rbo
dy
that
wou
ldh
elp
you
hol
dyo
ur
bod
y..
..”
Wei
ght
loss
5“
...i
fI
lose
wei
ght
may
beI’l
lfe
elbe
tter
,may
beI
won
’th
urt
som
uch
...”
4“I
fI
lost
wei
ght
my
arth
riti
sw
ould
n’t
beas
bad
.”
Psy
chol
ogic
al/b
ehav
iora
lIn
dep
end
ence
6“
...b
ecau
sebe
fore
Ist
arte
dd
oin
gth
is[e
xerc
ise]
my
doc
tor
was
tryi
ng
tosc
hed
ule
me
ina
nu
rsin
gh
ome
and
Isa
id,I
said
Iw
ould
not
go..
..af
ter
abou
t3
wee
ksI
cou
ldbe
gin
tose
eth
ed
iffe
ren
ce.
An
dn
ow2
year
sla
ter
I’mfe
elin
gju
stgr
eat
com
par
edto
wh
atI
was
.”
3“B
ut
Ith
ough
tgo
shif
Id
on’t
do
som
eth
ing.
Id
on’t
wan
tto
be..
.Id
on’t
wan
tto
bed
isab
led
.”
Att
itu
des
and
beli
efs
5“
...t
hro
ugh
exer
cise
and
,Im
ean
,th
em
edic
atio
nto
o,bu
tI
hav
ea
wh
ole
dif
fere
nt
outl
ook
onh
avin
gfi
brom
yalg
ia.L
ike
2ye
ars
ago
Iw
asli
ke‘I
don
’tkn
owh
owI’m
goin
gto
live
the
rest
ofm
yli
fed
oin
gth
is..
..I
don
’tkn
owh
owI’m
gon
na
ever
hav
eth
eli
feI
use
dto
hav
ebe
fore
.’A
nd
now
I’mn
ot10
0%bu
tI’m
mak
ing
pro
gres
sge
ttin
gba
ckto
wh
ere
Iw
asbe
fore
.Ikn
owI’m
nev
ergo
nn
abe
the
sam
ep
erso
nas
befo
rebu
tI
thin
kI
can
get
pre
tty
clos
en
ow.”
4“I
thin
kI’v
ed
one
som
eth
ing.
So
itgi
ves
me
am
enta
lbo
ost,
and
then
wh
enm
yw
ife
com
esh
ome,
Isa
y,‘H
ey,I
rod
eth
ebi
keto
day
,Id
idso
me
exer
cise
tod
ay.’
...
It’s
not
hin
gto
som
eon
eel
se,b
ut
tom
eto
beab
leto
take
that
one
pou
nd
wei
ght
and
do
itli
keba
rbel
lsan
dto
rid
eth
atbi
kefo
r10
min
ute
s,it
just
real
lym
akes
me
feel
like
Id
idso
met
hin
g.”
Em
otio
nal
6“M
akes
you
feel
good
wh
enyo
uge
tth
rou
ghw
ith
it.M
akes
you
mor
een
erge
tic
or..
.you
rst
ate
ofm
ind
.It
mak
esyo
ufe
elli
keyo
u’v
ed
one
som
eth
ing
good
for
you
rsel
f.”
6“Y
eah
itd
idm
ake
me
feel
bett
erbu
tit
mak
esm
efe
elbe
tter
but
yet
itbo
ther
sm
e.It
hu
rts
me.
”
En
joym
ent
5“I
like
ever
yth
ing
abou
tex
erci
se.”
5“
...i
fI
feel
like
Ire
ally
wan
tto
do
som
eth
ing
that
’s,y
oukn
ow,t
oh
ave
fun
wit
hex
erci
sin
g,I
do
itan
dI
suff
erth
eco
nse
quen
ces
late
r.”
Beh
avio
ral
enab
lers
3“
...a
nd
tom
eit
’sju
stco
me
dow
nto
it’s
got
tobe
ap
erso
nal
goal
.S
oI’v
ebe
ense
ttin
gti
me
lim
its,
asyo
ust
ated
[nam
e],i
nm
yd
aily
pla
nn
erab
out
wh
ento
mak
eit
ap
rior
ity,
wh
enI
can
pu
tit
in,
tryi
ng
tow
ork
my
life
arou
nd
it.”
1
Exercise and Arthritis 623

Tab
le5.
Su
mm
ary
ofp
erce
ived
soci
alan
den
viro
nm
enta
lbe
nefi
tsan
den
able
rsof
exer
cise
amon
gex
erci
sers
and
non
exer
cise
rsw
ith
arth
riti
s(n
�6
focu
sgr
oup
sea
ch)
Key
them
esan
dsu
bcat
egor
ies
Exe
rcis
ers
Non
exer
cise
rs
nIl
lust
rati
vequ
otat
ion
sn
Illu
stra
tive
quot
atio
ns
Soc
ial
En
joym
ent
ofex
erci
sin
gw
ith
oth
ers
4“I
th
elp
sm
em
enta
lly.
Ith
elp
sm
ep
hys
ical
ly.
It..
.Im
eet
alo
tof
dif
fere
nt
peo
ple
atth
egy
man
dit
’sam
azin
gh
owqu
ick
you
can
form
are
lati
onsh
ipw
ith
peo
ple
that
you
hav
en
ever
met
befo
re.A
nd
it’s
agr
eat
way
tosh
are
tim
ew
ith
oth
erfr
ien
ds.
You
can
get
them
toco
me
toth
egy
mw
ith
you
.”
5“Y
eah
,Ith
ink
like
the
oth
ers
said
Ith
ink
it’s
bein
gw
ith
oth
erp
eop
lew
hen
you
exer
cise
ina
grou
p,i
t’sm
ore
like
aso
cial
thin
gfo
ryo
uto
get
tobe
wit
hot
her
peo
ple
.An
dth
efa
ctth
atit
give
syo
um
ore
ener
gy.
You
feel
hea
lth
ier.
”
En
cou
rage
men
t6
“My
dau
ghte
ris
my
chee
rlea
der
.Sh
eh
asal
way
sen
cou
rage
dm
e.C
ause
som
etim
essh
e’ll
call
and
she,
mor
eth
anan
yon
eca
nte
llw
hen
I’mh
avin
ga
bad
day
.Sh
e’ll
say
‘Ma,
you
mig
ht
nee
dto
just
get
up
and
gofo
ra
litt
lew
alk.
Just
goou
tin
the
yard
Ma.
’You
know
,ju
stw
hat
ever
,sh
e’s
my
chee
rlea
der
.”
6“I
get
alo
tof
gen
eral
sup
por
tin
that
area
.Nob
ody
pu
shes
me
toex
erci
seh
ard
,bu
tev
eryb
ody
sup
por
tsm
eto
do
wh
atev
erI
can
toex
erci
se.”
Som
eon
eto
exer
cise
wit
h5
“Ip
roba
bly
wou
ldn
’tgo
but
my
hu
sban
dgo
esso
Igo
wit
hh
im.I
wou
ldp
roba
bly
beve
ryba
dab
out
exer
cisi
ng
ifI
wer
en’t
goin
gli
keth
at.”
6“W
ord
sd
on’t
mea
nas
mu
chas
go.Y
oukn
owle
t’sgo
,le
t’sd
oit
toge
ther
.”
En
viro
nm
enta
lW
ater
exer
cise
5“
...
Id
idh
ear
som
eth
ing
abou
tth
ere
isa
hea
ted
poo
lov
erat
Har
biso
nan
dth
eyh
ave
wat
erw
orko
uts
for
peo
ple
wit
har
thri
tis
but
Id
on’t
know
ifth
at’s
stil
lgo
ing
onor
not
.”
6“T
hat
’sw
hy
aw
ater
clas
san
dso
met
hin
gli
keth
atw
her
eyo
u’v
ego
tan
inst
ruct
or.S
omeb
ody
ther
eth
atca
nle
adyo
uan
dgi
veyo
u10
exer
cise
sfo
ryo
ur
par
ticu
lar
bod
y.”
Pro
gram
sfo
rp
eop
lew
ith
arth
riti
s3
“..
.wit
har
thri
tis,
and
yes,
you
can
goto
regu
lar
clas
ses,
but
Ith
ink
you
real
lyn
eed
inst
ruct
ors
wh
oar
ego
ing
tou
nd
erst
and
not
som
uch
the
exer
cise
,bu
tth
eli
mit
atio
ns
wh
atw
eh
ave
and
that
isw
hat
’sm
issi
ng.
”
4“
Ith
ink
it’s
like
seve
ral
ofth
emsa
id,fi
nd
ing
ap
lace
togo
tod
oth
eex
erci
sean
dh
avin
gin
stru
ctor
sth
ere
that
know
you
rli
mit
atio
ns
tow
hat
you
can
do
and
wh
atyo
uca
n’t
do
and
how
it’s
goin
gto
affe
ctyo
ur
join
tsin
the
cert
ain
exer
cise
sth
atyo
ud
o.”
Low
cost
4“
...T
he
yoga
once
aw
eek
is$1
5a
mon
than
dyo
u’v
ego
tto
join
[nam
e]fo
r$3
5,an
dI
thin
kit
’sth
ebi
gges
tba
rgai
nar
oun
d.”
2“Y
eah
.An
dit
’s3
tim
esa
wee
kan
dit
’s$3
0fo
r3
tim
esa
wee
kw
hic
his
real
lygo
od.”
Ava
ilab
ilit
yof
equ
ipm
ent
3“S
oI
bou
ght
me
one
ofth
ose
wal
kers
,wh
ere
Ica
nw
alk
inth
eh
ouse
.So
Id
oth
atof
ten
.”3
“An
dso
now
it’s
(th
ebi
ke)
onth
eba
ckp
orch
and
itfa
ces
the
woo
ds
and
soI
sit
up
ther
ean
dI
rid
eit
and
Ih
ave
ali
ttle
tim
erth
atI
fou
nd
and
Ise
tit
for
15m
inu
tes,
then
Iw
alk
for
10m
inu
tes.
I’ve
been
doi
ng
that
like
Isa
ya
mon
thor
son
ow.”
624 Wilcox et al

exercisers and nonexercisers talked about needing to be“more flexible” and described the importance of staying“limber” and “loose.” Exercisers said that an activity suchas swimming “limbers you up,” and yoga “increases yourflexibility.” Several comments related to flexibility alsorelated to the benefit of reduced stiffness described earlier.
Weight loss. Exercisers and nonexercisers described ex-ercise as a way to “keep the weight down” or noted that itwas beneficial to managing the weight that they had gainedover the years. Exercisers perceived that losing weightwould make them feel better or noted that weight loss hadactually helped with their arthritis. Nonexercisers saidthat they wanted weight loss results from exercise and thatit would help them be more motivated to exercise.
Other less common themes. Exercisers described im-provements in comorbid conditions or their symptoms.Several said that they began exercising because of heartconditions, but that it also had a positive impact on theirarthritis. Diabetes and osteoporosis were also raised ascomorbid conditions that prompted them to exercise. Fi-nally, in 2 groups, exercisers described how regular exer-cise decreased the amount of medication needed to man-age the symptoms of arthritis.
Psychological benefits and enablers. Independence. In-dependence was a theme for exercisers and nonexercisers,although it was cited more often by exercisers. Exercisersreported compelling reasons as to why they were moti-vated to exercise regularly, including avoiding becoming“an invalid” or having to be in a wheelchair, fear of havingto go into a nursing home, and, most importantly, beingable to remain “self-sufficient.”
Attitudes and beliefs. Exercisers and nonexercisers de-scribed how exercise improved their attitudes and beliefs.Exercisers noted improvements in self-confidence and anoverall improved attitude toward their disease. Nonexer-cisers, in contrast, liked the feeling of being able to accom-plish something, no matter how small. Whereas exercisersdescribed participating in sufficient exercise to attain ben-efits, nonexercisers struggled to be active but felt that eventhe simplest of efforts were “a really big deal.”
Emotional benefits. All groups described the emotionalbenefits of exercise. Exercisers reported that it made them“feel better” or “feel good” during and after the activity. Inaddition to feeling good, many exercisers described thelink between exercise and both “stress relief” and relax-ation, and said that exercise helped them to forget abouttheir pain. Although many nonexercisers also reportedthat exercise made them “feel good,” there was a distinctdifference in how some viewed this benefit. Some nonex-ercisers implied that the emotional benefit might not out-weigh the pain that exercise caused. Most nonexerciserswho described emotional benefits from exercise referred toexercise experiences before rather than after arthritis.
Enjoyment. In groups of both exercisers and nonexercis-ers, participants described liking exercise or having funwhile exercising, including exercising in a group, with asignificant other, or by themselves. Among nonexercisers,the theme of enjoyment surfaced primarily from discus-sions about their exercise before arthritis. Although some
still described enjoying exercise, they often “paid for itlater” with pain or fatigue.
Behavioral enablers. Exercisers expressed specific be-havioral enablers for exercise, whereas no clear themesemerged for nonexercisers. Exercisers stated that theywere internally motivated to exercise and underscored theimportance of self-regulatory skills, including making ex-ercise a priority, scheduling exercise, and setting goals.
Social benefits and enablers. Exercisers and nonexer-cisers described the enjoyment of exercising with othersand the positive social interaction of being around otherswho exercise. Exercisers mentioned that being in oraround groups of exercisers was a positive social outcome.Social benefits among nonexercisers were typically de-scribed in relation to their exercise experiences beforearthritis. Nonexercisers described the social benefits ofexercise and thought it was a motivating factor.
Exercisers and nonexercisers identified similar socialenablers, including having important others (e.g., friends,family, health care providers) encourage them to exerciseand having someone to exercise with. Exercisers often saidthat they had someone to exercise with, whereas nonexer-cisers said that they did not have this type of support butdesired it. Likewise, nonexercisers expressed the need toreceive external cues or reminders from important othersfor exercise. Having an exercise group of similar otherswas viewed as important for nonexercisers because of theemotional support it provided.
Environmental enablers. Both exercisers and nonexer-cisers stated that a water-based exercise program wouldmake it easier for them to exercise. They also described theneed for programs and instructors who understood issuesrelated to arthritis and exercise. Exercisers were morelikely than nonexercisers to say that low-cost programsenabled them to exercise. Finally, having exercise equip-ment such as a treadmill or a stationary bicycle withinone’s immediate physical environment (i.e., a person’shome or a relative’s home) was perceived as making exer-cise more likely among exercisers and nonexercisers.
DISCUSSION
By recruiting a relatively large sample of individuals witharthritis, measuring exercise participation, and conductingstratified recruitment to ensure a diverse sample of exer-cisers and nonexercisers, our qualitative study extendswhat is known about the perceived barriers, benefits, andenablers of exercise among persons with arthritis. Rela-tively few studies have examined these issues, and evenfewer have been specifically designed with this purpose inmind (20). Furthermore, only 3 studies (all with smallsamples) have used a qualitative approach (23–25), one ofwhich measured physical activity and stratified on thebasis of this measure (23).
Physical, psychological, social, and environmental bar-riers, benefits, and enablers were identified in this study,consistent with social cognitive theory (26) and socialecological models (27,28). While some influences were
Exercise and Arthritis 625

similar to those reported in other general populations (19),others appeared unique to individuals with a chronic dis-ease. Consistent with other studies (25,29), symptoms ofarthritis, including pain, stiffness, fatigue, and mobilityproblems, were perceived as barriers to exercise. Yet im-provements in these outcomes were also seen as potentialbenefits of and motivations for exercise. The role of exer-cise in promoting independence was a salient and highlymotivating benefit, especially among exercisers. Exercisershad experience achieving many benefits, whereas nonex-ercisers described these potential benefits as outcomes thatwould motivate them to exercise. Nonexercisers expressedsome doubt that they would benefit from exercise andthought that increased pain, even if temporary, may not beworth the benefits.
A number of our findings have direct implications forhow to market exercise to individuals with arthritis andhow communities and clinicians can facilitate participa-tion in exercise. First, individuals with arthritis value theinformation provided by health care providers (24,25).Receiving such information has been shown to predicthigher levels of physical activity among adults with rheu-matoid arthritis (30). The perceived lack of advice, instruc-tion, and referrals was cited in our study as a barrier.Providers may feel ill prepared to prescribe exercise (24)and may need additional assistance to make exercise rec-ommendations and specific referrals. In addition, resultsfrom research trials take time to influence practice (31),and the lack of advice, instruction, and referrals may re-flect this lag in evidence-based practice.
Second, wider availability and awareness of arthritis-specific programs is needed for individuals with arthritisand health care providers. The lack of arthritis-specificprograms and knowledgeable instructors was identified asa major barrier, especially among nonexercisers. Consid-ering the prevalence of arthritis, community programs andfacilities should be encouraged to expand their program-ming to individuals with arthritis and to publicize suchprograms. Program characteristics that build self-efficacy,facilitate social support, encourage individuals to work attheir own pace, and are led by quality instructors areparticularly important (29).
Third, exercisers and nonexercisers identified similarbarriers to exercise. What differentiated these groups wasthat exercisers were less likely to allow these barriers toprevent exercise and often modified their exercise to ac-commodate physical limitations. Nonexercisers were morelikely to have given up exercise altogether or to havegreatly reduced its frequency when faced with arthritis-specific barriers. Print and other forms of messages mightbe more effective if they emphasize ways in which indi-viduals with arthritis can modify exercise to accommodatetheir disease.
Fourth, most exercisers and nonexercisers alike wereaware of the benefits of exercise, yet nonexercisers werenot engaging in it. These findings indicate that knowledge-based approaches alone are unlikely to affect behavior(19,32), and techniques to increase self-efficacy (33), prob-lem-focused coping, and self-regulatory skills are impor-tant for changing behavior.
Fifth, pain relief and improved mobility from exercise
were the major motivators for exercisers and nonexercis-ers. However, pain was the primary reason why nonexer-cisers had quit an exercise program. Pain is consistentlyassociated with lower rates of exercise across arthritistypes, despite the fact that a substantial number of con-trolled, randomized trials of exercise in persons with ar-thritis have reported reductions in pain (11,34,35). In oneintervention study (36), improvements in pain predictedsubsequent exercise participation, suggesting that this out-come may be critical to exercise adherence. Recruitmentand program messages might need to explain to personswith arthritis that pain may increase during and immedi-ately after exercise, but that overall pain management canbe enhanced. Many exercisers voiced this message. Inter-ventions might also need to include pain managementstrategies.
Finally, in addition to traditional outcome measures,personally meaningful outcomes for individuals with ar-thritis (e.g., pain reduction, increased mobility, decreasedstiffness, independence) should be emphasized in inter-vention materials and assessed in research and practicesettings. These outcomes are what matter most to the in-dividuals with arthritis and are likely to predict subse-quent adherence.
As is common in qualitative research, a purposive sam-ple of participants was recruited. Key stratification factorsexpected to affect the discussion were used to structure thecomposition of groups and to create homogeneous groups.To increase the generalizability of findings, we used avariety of recruitment strategies to reach the entire com-munity. Nonetheless, participants who volunteer in such astudy may differ from those who do not volunteer alongpotentially important variables such as disease severity,attitudes about health and exercise, and sociodemograph-ics. Furthermore, local communities vary widely in theavailability of resources and programs for individuals witharthritis, and our findings may not be as applicable incommunities with more such resources or in rural areaswith substantially fewer resources. To limit the number ofgroups conducted, groups were not segmented by age ordisease type. Also, we recruited a small number of men,particularly those who were nonexercisers. It is likely thatbarriers, attitudes, and beliefs differ by age (or generation),sex, and disease type. Therefore, we are not able to makesex-, age-, and disease-specific conclusions. Finally, not allpotentially pertinent characteristics of participants weremeasured (e.g., personality traits).
Despite potential limitations, our findings provide use-ful information for understanding the experiences withand beliefs about exercise among persons with arthritisand informing recruitment and intervention strategies.
ACKNOWLEDGMENTSWe would like to thank Carol Rheaume for her assistancein pilot testing the moderator’s guide and Billy Oglesby forproviding qualitative training and consultation. We alsogratefully acknowledge each of the individuals who tookpart in our focus groups.
626 Wilcox et al

REFERENCES
1. Centers for Disease Control and Prevention. Prevalence ofdisabilities and associated health conditions among adults:United States, 1999 [published erratum appears in MMWRMorb Mortal Wkly Rep 2001;50:149]. MMWR Morb MortalWkly Rep 2001;50:120–5.
2. Yelin E, Cisternas MG, Pasta DJ, Trupin L, Murphy L, HelmickCG. Medical care expenditures and earnings losses of personswith arthritis and other rheumatic conditions in the UnitedStates in 1997: total and incremental estimates. ArthritisRheum 2004;50:2317–26.
3. Arthritis Foundation Association of State and TerritorialHealth Officials and Centers for Disease Control and Preven-tion. National arthritis action plan: a public health strategy.Atlanta (GA): Centers for Disease Control and Prevention;1999.
4. US Department of Health and Human Services. Healthy Peo-ple 2010: understanding and improving health. 2nd ed. Wash-ington (DC): US Government Printing Office; 2000.
5. Calkins E. Management of rheumatoid arthritis and the otherautoimmune rheumatic diseases. In: Hazzard WR, Blass JP,Ettinger WH, Halter JB, Ouslander JG, editors. Principles ofgeriatric medicine and gerontology. New York: McGraw-Hill;1999. p. 1135–53.
6. Creamer P, Hochberg MC. Management of osteoarthritis. In:Hazzard WR, Blass JP, Ettinger WH, Halter JB, Ouslander JG,editors. Principles of geriatric medicine and gerontology. NewYork: McGraw-Hill; 1999. p. 1155–62.
7. Hochberg MC, Altman RD, Brandt KD, Clark BM, Dieppe PA,Griffin MR, et al. Guidelines for the medical management ofosteoarthritis. Part II. Osteoarthritis of the knee. ArthritisRheum 1995;38:1541–6.
8. Van Baar ME, Assendelft WJ, Dekker J, Oostendorp RA, Bi-jlsma JW. Effectiveness of exercise therapy in patients withosteoarthritis of the hip or knee: a systematic review of ran-domized clinical trials. Arthritis Rheum 1999;42:1361–9.
9. Hall J, Skevington SM, Maddison PJ, Chapman K. A random-ized and controlled trial of hydrotherapy in rheumatoid ar-thritis. Arthritis Care Res 1996;9:206–15.
10. Hakkinen A, Sokka T, Kotaniemi A, Hannonen P. A random-ized two-year study of the effects of dynamic strength trainingon muscle strength, disease activity, functional capacity, andbone mineral density in early rheumatoid arthritis. ArthritisRheum 2001;44:515–22.
11. Ettinger WH Jr, Burns R, Messier SP, Applegate W, RejeskiWJ, Morgan T, et al. A randomized trial comparing aerobicexercise and resistance exercise with a health education pro-gram in older adults with knee osteoarthritis: the FitnessArthritis and Seniors Trial (FAST). JAMA 1997;277:25–31.
12. Messier SP, Royer TD, Craven TE, O’Toole ML, Burns R,Ettinger WH Jr. Long-term exercise and its effect on balance inolder, osteoarthritic adults: results from the Fitness, Arthritis,and Seniors Trial (FAST). J Am Geriatr Soc 2000;48:131–8.
13. Minor MA. Physical activity and management of arthritis.Ann Behav Med 1991;13:117–24.
14. Rossy LA, Buckelew SP, Dorr N, Hagglund KJ, Thayer JF,McIntosh MJ, et al. A meta-analysis of fibromyalgia treatmentinterventions. Ann Behav Med 1999;21:180–91.
15. Penninx BW, Messier SP, Rejeski WJ, Williamson JD, DiBariM, Cavazzini C, et al. Physical exercise and the prevention ofdisability in activities of daily living in older persons withosteoarthritis. Arch Intern Med 2001;161:2309–16.
16. US Department of Health and Human Services. Physical ac-tivity and health: a report of the surgeon general. Atlanta(GA): National Center for Chronic Disease Prevention andHealth Promotion, Centers for Disease Control and Preven-tion, US Department of Health and Human Services; 1996.
17. Friedenreich CM. Physical activity and cancer prevention:from observational to intervention research. Cancer Epide-miol Biomarkers Prev 2001;10:287–301.
18. Hootman JM, Macera CA, Ham SA, Helmick CG, Sniezek JE.Physical activity levels among the general US adult popula-tion and in adults with and without arthritis. Arthritis Rheum2003;49:129–35.
19. Trost SG, Owen N, Bauman AE, Sallis JF, Brown W. Corre-lates of adults’ participation in physical activity: review andupdate. Med Sci Sports Exerc 2002;34:1996–2001.
20. Wilcox S, der Ananian C, Sharpe PA, Robbins J, Brady T.Correlates of physical activity in persons with arthritis: re-view and recommendations. J Phys Activ Health 2005;2:230–52.
21. Morgan DL. Planning focus groups. Volume 2. ThousandOaks (CA): Sage; 1998. p. 139.
22. Centers for Disease Control and Prevention. Targetingarthritis: the nation’s leading cause of disability. Atlanta (GA):Department of Health and Human Services, Centers for Dis-ease Control and Prevention; 2001.
23. Eurenius E, Biguet G, Stenstrom CH. Attitudes toward phys-ical activity among people with rheumatoid arthritis. Phys-iother Theory Pract 2003;19:53–62.
24. Lambert BL, Butin DN, Moran D, Zhao SZ, Carr BC, Chen C, etal. Arthritis care: comparison of physicians’ and patients’views. Semin Arthritis Rheum 2000;30:100–10.
25. Kamwendo K, Askenbom M, Wahlgren C. Physical activity inthe life of the patient with rheumatoid arthritis. PhysiotherRes Int 1999;4:278–92.
26. Bandura A. Social foundations of thought and action: a socialcognitive theory. Englewood Cliffs (NJ): Prentice-Hall; 1986.p. 617.
27. McLeroy KR, Bibeau D, Steckler A, Glanz K. An ecologicalperspective on health promotion programs. Health Educ Q1988;15:351–77.
28. Sallis JF, Bauman A, Pratt M. Environmental and policy in-terventions to promote physical activity. Am J Prev Med1998;15:379–97.
29. Schoster B, Callahan LF, Meier A, Mielenz T, DiMartino L.The People with Arthritis Can Exercise (PACE) program: aqualitative evaluation of participant satisfaction. PrevChronic Dis [serial online]. 2005;2(3). URL: http://www.cdc.gov/pcd/issues/2005/jul/05_0009.htm.
30. Terpstra SJ, de Witte LP, Diederiks JP. Compliance of patientswith an exercise program for rheumatoid arthritis. PhysiotherCan 1992;44:37–41.
31. Institute of Medicine. Crossing the quality chasm: a newhealth system for the 21st century. Washigton (DC): NationalAcademy Press; 2001.
32. Marcus BH, King TK, Clark MM, Pinto BM, Bock BC. Theoriesand techniques for promoting physical activity behaviours.Sports Med 1996;22:321–31.
33. Bandura A. Self-efficacy mechanism in human agency. AmPsychol 1982;37:122–47.
34. American Geriatrics Society Panel on Exercise and Osteoar-thritis. Exercise prescription for older adults with osteoarthri-tis pain: consensus practice recommendations: a supplementto the AGS Clinical Practice Guidelines on the management ofchronic pain in older adults [published erratum appears inJ Am Geriatr Soc 2001;49:1400]. J Am Geriatr Soc 2001;49:808–23.
35. Stenstrom CH, Minor MA. Evidence for the benefit of aerobicand strengthening exercise in rheumatoid arthritis. ArthritisRheum 2003;49:428–34.
36. Minor MA, Brown JD. Exercise maintenance of persons witharthritis after participation in a class experience. Health EducQ 1993;20:83–95.
Exercise and Arthritis 627