Embed Size (px)
Citation preview

tvpjournal.comToday’s Veterinary Practice July/August 201416
Keratoconjunctivitis sicca (KCS) is a relatively common condition in dogs. Although KCS can be diagnosed readily with a thorough ophthalmic examination, the diagnosis is often overlooked.
KCS is an inflammatory condition of the cornea and conjunctiva, secondary to a deficiency of the precorneal tear film (PTF). KCS is cat-egorized by tear film defi-ciency: • Quantitative KCS is a
decrease in the aqueous component of the tear film as measured with the Schirmer tear test (STT); it is recognized more commonly in veterinary medicine.
• Qualitative KCS is a decrease in the lipid or mucin components of the tear film and diag-nosed by document-ing decreased tear film breakup time (TBUT).
PATHOPHySIOLOGyTear film deficiencies lead to: •Chronic inflammation of
the ocular surface sec-ondary to increased sur-face friction
• Secondary infection•Dehydration and malnu-
trition of the corneal and
conjunctival epithelium. This latter combination makes ulcerations more
prone to infection, possibly resulting in keratomala-cia and perforation.
Diagnosis & Treatment of Keratoconjunctivitis Sicca in DogsLori J. Best, DVM; Diane V.H. Hendrix, DVM, Diplomate ACVO; and Daniel A. Ward, DVM, PhD, Diplomate ACVOUniversity of Tennessee
PEER REVIEWED
THE LACRIMAL SySTEM & TEAR FILMnormal PTf is estimated to be anywhere from 3 to 45 microns thick in humans and, in most species, is composed of aqueous, lipid, and mucin layers, which were once thought to be present in a laminar arrangement (Table 1).1,2 more recent evidence suggests that PTf may resemble a muco-aqueous pool covered in a very thin lipid layer rather than a trilaminar structure.3
lacrimal secretion is stimulated via sensory input from the cornea, periocular structures, and globe. The ophthalmic and maxillary divisions of the trigeminal nerve serve as the afferent part of the reflex arc; then motor input travels to the lacrimal glands via the parasympathetic division of the facial nerve as the efferent arc. Tears are then secreted following contraction of lacrimal acinar myoepithelium.
Table 1. structure of Precorneal Tear filmAREA OF
PRODUCTIONFUNCTION
TyPE OF DEFICIENCy
DIAGNOSTIC TEST
LIPID meibomian glands
• limits evaporation • binds tear film to
cornea • Provides surface
tension to prevent tear film overflow
Qualitative Decrease in TbuT
AQUEOUS orbital and nictitans lacrimal glands
•Provides corneal nutrition, surface lubrication, and smooth surface for optical clarity
•removes waste material and bacteria
Quantitative Decrease in sTT value
MUCIN conjunctival goblet cells
•enhances spread of tear film
Qualitative Decrease in TbuT
July/August 2014 Today’s Veterinary Practice 17
Diagnosis & TreaTmenT of KeraToconjuncTiViTis sicca in Dogs |
tvpjournal.com
Chronic surface irritation results in: •Conjunctival hyperemia• Squamous metaplasia of the surface epithelium•Hyperkeratinization of the surface epithelium •Thickening of the corneal epithelium.
Inflammatory cells and blood vessels enter the anterior corneal stroma, depositing pigment, lip-ids, and calcium. The vascularization and deposits stabilize the cornea and make it less susceptible to ulceration; however, their presence can result in vision loss.
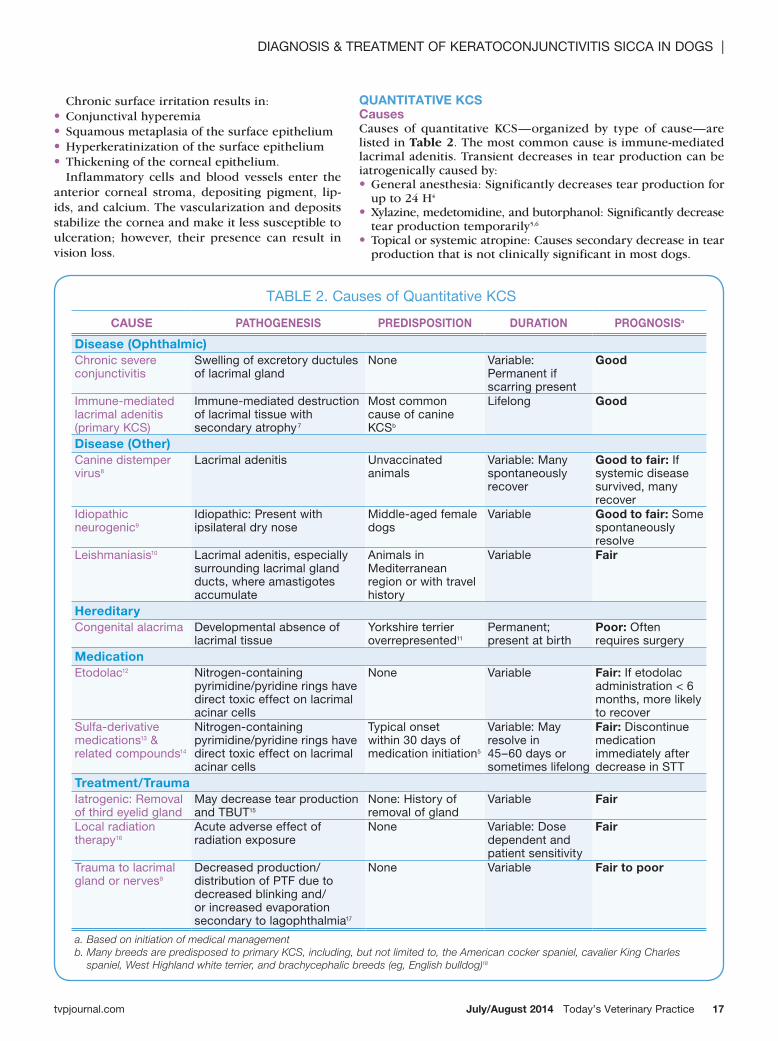
Table 2. causes of Quantitative Kcs
CAUSE PATHOGENESIS PREDISPOSITION DURATION PROGNOSISa
Disease (Ophthalmic)chronic severe conjunctivitis
swelling of excretory ductules of lacrimal gland
none Variable: Permanent if scarring present
Good
immune-mediated lacrimal adenitis (primary Kcs)
immune-mediated destruction of lacrimal tissue with secondary atrophy7
most common cause of canine Kcsb
lifelong Good
Disease (Other)canine distemper virus8
lacrimal adenitis unvaccinated animals
Variable: many spontaneously recover
Good to fair: if systemic disease survived, many recover
idiopathic neurogenic9
idiopathic: Present with ipsilateral dry nose
middle-aged female dogs
Variable Good to fair: some spontaneously resolve
leishmaniasis10 lacrimal adenitis, especially surrounding lacrimal gland ducts, where amastigotes accumulate
animals in mediterranean region or with travel history
Variable Fair
Hereditarycongenital alacrima Developmental absence of
lacrimal tissueYorkshire terrier overrepresented11
Permanent; present at birth
Poor: often requires surgery
Medicationetodolac12 nitrogen-containing
pyrimidine/pyridine rings have direct toxic effect on lacrimal acinar cells
none Variable Fair: if etodolac administration < 6 months, more likely to recover
sulfa-derivative medications13 & related compounds14
nitrogen-containing pyrimidine/pyridine rings have direct toxic effect on lacrimal acinar cells
Typical onset within 30 days of medication initiation5
Variable: may resolve in 45–60 days or sometimes lifelong
Fair: Discontinue medication immediately after decrease in sTT
Treatment/Traumaiatrogenic: removal of third eyelid gland
may decrease tear production and TbuT15
none: History of removal of gland
Variable Fair
local radiation therapy16
acute adverse effect of radiation exposure
none Variable: Dose dependent and patient sensitivity
Fair
Trauma to lacrimal gland or nerves9
Decreased production/ distribution of PTf due to decreased blinking and/or increased evaporation secondary to lagophthalmia17
none Variable Fair to poor
a. Based on initiation of medical managementb. Many breeds are predisposed to primary KCS, including, but not limited to, the American cocker spaniel, cavalier King Charles
spaniel, West Highland white terrier, and brachycephalic breeds (eg, English bulldog)18
QUANTITATIVE KCSCausesCauses of quantitative KCS—organized by type of cause—are listed in Table 2. The most common cause is immune-mediated lacrimal adenitis. Transient decreases in tear production can be iatrogenically caused by:•General anesthesia: Significantly decreases tear production for
up to 24 H4 •Xylazine, medetomidine, and butorphanol: Significantly decrease
tear production temporarily5,6 •Topical or systemic atropine: Causes secondary decrease in tear
production that is not clinically significant in most dogs.
| Diagnosis & TreaTmenT of KeraToconjuncTiViTis sicca in Dogs
Today’s Veterinary Practice July/August 201418 tvpjournal.com
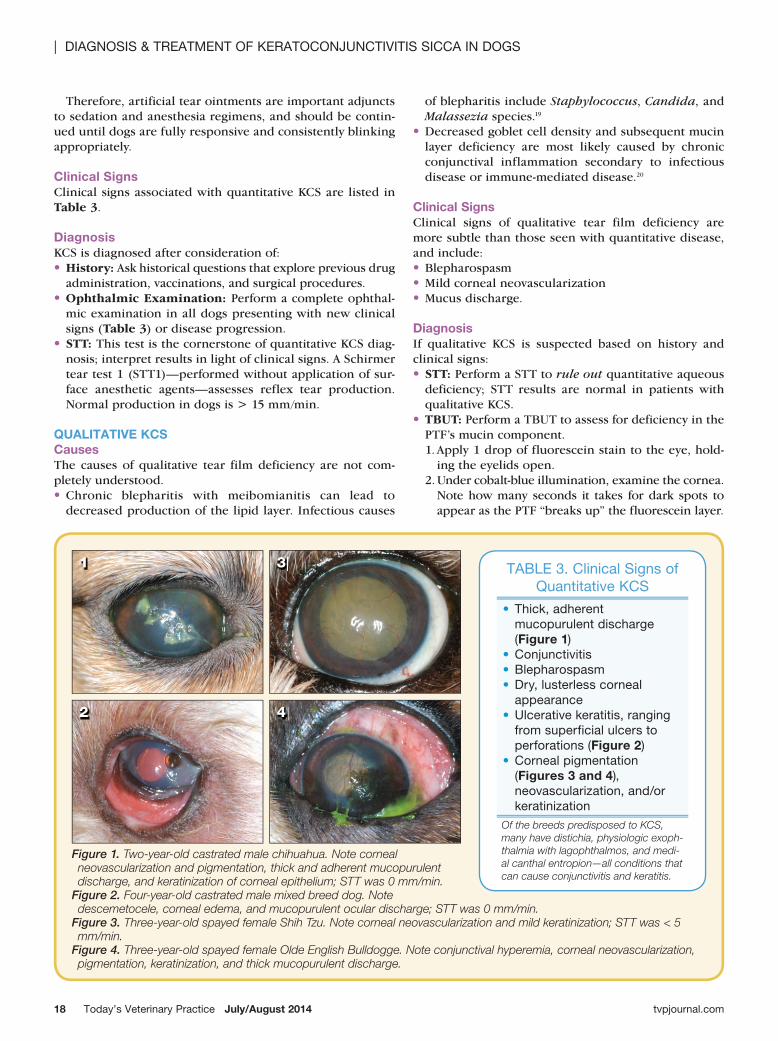
Figure 1. Two-year-old castrated male chihuahua. Note corneal neovascularization and pigmentation, thick and adherent mucopurulent discharge, and keratinization of corneal epithelium; STT was 0 mm/min.
Figure 2. Four-year-old castrated male mixed breed dog. Note descemetocele, corneal edema, and mucopurulent ocular discharge; STT was 0 mm/min.
Figure 3. Three-year-old spayed female Shih Tzu. Note corneal neovascularization and mild keratinization; STT was < 5 mm/min.
Figure 4. Three-year-old spayed female Olde English Bulldogge. Note conjunctival hyperemia, corneal neovascularization, pigmentation, keratinization, and thick mucopurulent discharge.
1
2 4
3 Table 3. clinical signs of Quantitative Kcs
•Thick, adherent mucopurulent discharge (Figure 1)
•conjunctivitis•blepharospasm•Dry, lusterless corneal
appearance•ulcerative keratitis, ranging
from superficial ulcers to perforations (Figure 2)
•corneal pigmentation (Figures 3 and 4), neovascularization, and/or keratinization
Of the breeds predisposed to KCS, many have distichia, physiologic exoph-thalmia with lagophthalmos, and medi-al canthal entropion—all conditions that can cause conjunctivitis and keratitis.
Therefore, artificial tear ointments are important adjuncts to sedation and anesthesia regimens, and should be contin-ued until dogs are fully responsive and consistently blinking appropriately.
Clinical SignsClinical signs associated with quantitative KCS are listed in Table 3.
Diagnosis KCS is diagnosed after consideration of: •History: Ask historical questions that explore previous drug
administration, vaccinations, and surgical procedures. •Ophthalmic Examination: Perform a complete ophthal-
mic examination in all dogs presenting with new clinical signs (Table 3) or disease progression.
•STT: This test is the cornerstone of quantitative KCS diag-nosis; interpret results in light of clinical signs. A Schirmer tear test 1 (STT1)—performed without application of sur-face anesthetic agents—assesses reflex tear production. Normal production in dogs is > 15 mm/min.
QUALITATIVE KCSCausesThe causes of qualitative tear film deficiency are not com-pletely understood. •Chronic blepharitis with meibomianitis can lead to
decreased production of the lipid layer. Infectious causes
of blepharitis include Staphylococcus, Candida, and Malassezia species.19
•Decreased goblet cell density and subsequent mucin layer deficiency are most likely caused by chronic conjunctival inflammation secondary to infectious disease or immune-mediated disease.20
Clinical SignsClinical signs of qualitative tear film deficiency are more subtle than those seen with quantitative disease, and include: •Blepharospasm•Mild corneal neovascularization•Mucus discharge.
DiagnosisIf qualitative KCS is suspected based on history and clinical signs:•STT: Perform a STT to rule out quantitative aqueous
deficiency; STT results are normal in patients with qualitative KCS.
•TBUT: Perform a TBUT to assess for deficiency in the PTF’s mucin component. 1. Apply 1 drop of fluorescein stain to the eye, hold-
ing the eyelids open. 2. Under cobalt-blue illumination, examine the cornea.
Note how many seconds it takes for dark spots to appear as the PTF “breaks up” the fluorescein layer.
July/August 2014 Today’s Veterinary Practice 19
Diagnosis & TreaTmenT of KeraToconjuncTiViTis sicca in Dogs |
tvpjournal.com
3. A normal TBUT is ≥ 20 seconds. Animals with quanti-tative deficiencies often have a TBUT of < 5 seconds, which indicates an unstable PTF.20
•Conjunctival Biopsy: In cases of suspected mucin defi-ciency, obtain a conjunctival biopsy specimen to quanti-tate conjunctival goblet cell density.
•Eyelid Margin Examination: With a focus light and magnifying source, carefully examine the eyelid margin to identify deficiencies of the lipid component, which often occur secondary to blepharitis (Figure 6) or mei-bomianitis.
MEDICAL MANAGEMENT OF KCSPrimary medical therapy of both quantitative and qualita-tive KCS consists of tear stimulants and tear replacements. Topical antibiotics and anti-inflammatory drugs are also commonly used.
Dogs with KCS may have increased sensitivity to pain associated with topical medications, because abnormal PTF cannot provide a reflex dilution effect. This may be espe-cially problematic with frequent application of tear replace-ment medications that contain preservatives; some artificial tear products are available without preservatives, but the lack of preservatives requires single-use ampules, which most owners find inconvenient.
In most patients with KCS, topical therapy is required indefinitely. Clients should be educated about the chronic-ity of KCS and the necessity of lifelong therapy.
Tear Stimulation1. Cyclosporine A (CsA)
Mechanism of action. Cyclosporine is an immunomodu-lator that blocks normal production of interleukin-2, which
inhibits proliferation of T-helper and cytotoxic T cells in the lacrimal gland and allows normal lacrimation.21
Cyclosporine also acts as an anti-inflammatory, decreases pigmentation, normalizes goblet cell mucin secretion,22 and directly stimulates lacrimation, but the latter mechanism is still poorly understood.23
Efficacy. Topical preparations are very effective for tear stimulation and reducing inflammation, with 81.8% of dogs showing improvement (Figure 7, page 20).24,25 Dogs with a STT < 2 mm/min respond with increased tear secretion in approximately 50% of cases, while dogs with a STT ≥ 2 mm/min have an approximately 80% chance of responding.18
Formulation. CsA is available as Optimmune 0.2% oph-thalmic ointment (merck-animal-health-usa.com). Com-pounded formulations are available in 1% and 2% corn or
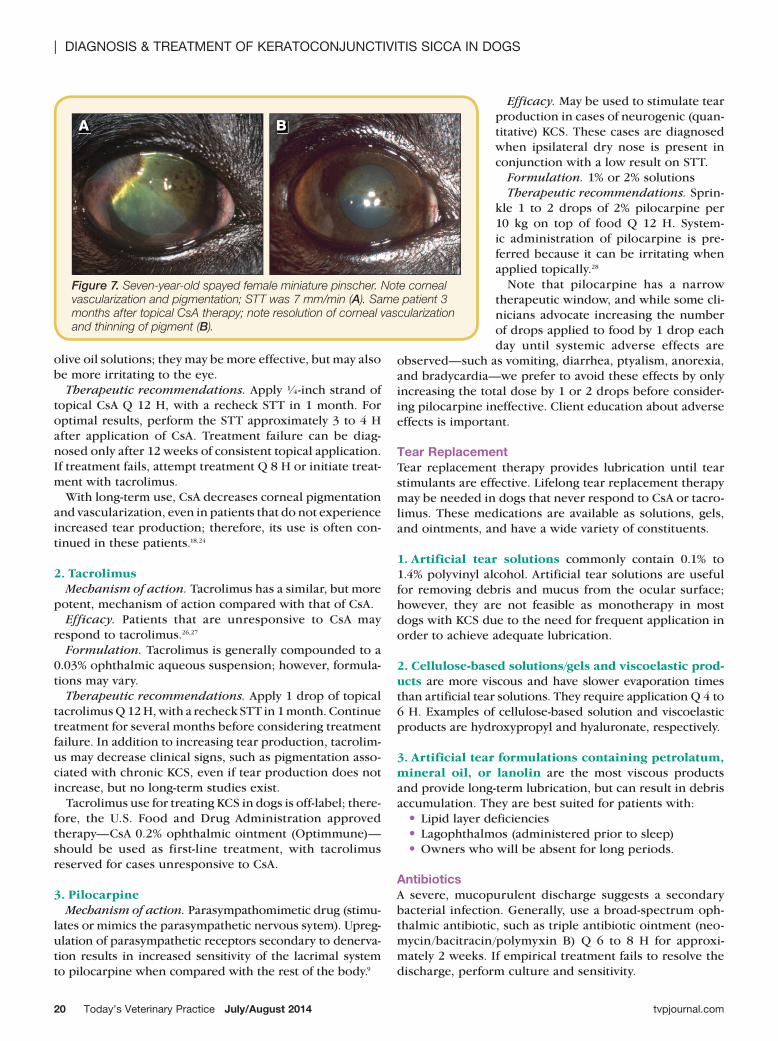
Figure 6. Four-year-old castrated male Chihuahua with acute blepharitis.
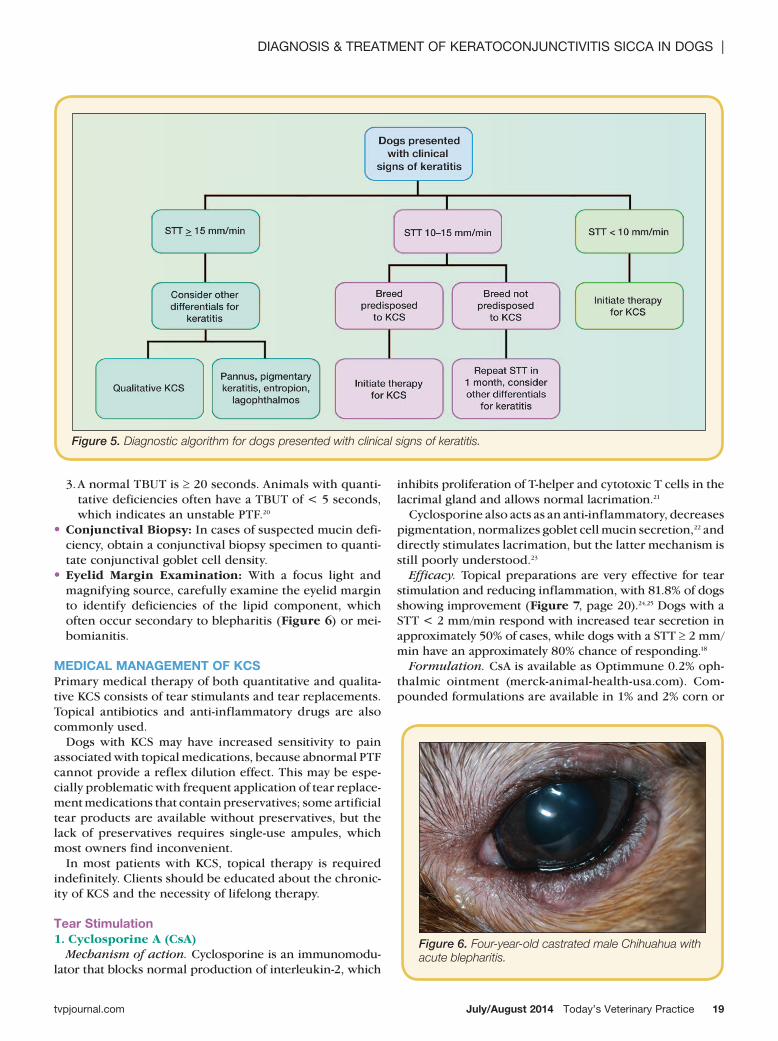
Figure 5. Diagnostic algorithm for dogs presented with clinical signs of keratitis.
| Diagnosis & TreaTmenT of KeraToconjuncTiViTis sicca in Dogs
Today’s Veterinary Practice July/August 201420 tvpjournal.com
olive oil solutions; they may be more effective, but may also be more irritating to the eye.
Therapeutic recommendations. Apply ¼-inch strand of topical CsA Q 12 H, with a recheck STT in 1 month. For optimal results, perform the STT approximately 3 to 4 H after application of CsA. Treatment failure can be diag-nosed only after 12 weeks of consistent topical application. If treatment fails, attempt treatment Q 8 H or initiate treat-ment with tacrolimus.
With long-term use, CsA decreases corneal pigmentation and vascularization, even in patients that do not experience increased tear production; therefore, its use is often con-tinued in these patients.18,24
2. TacrolimusMechanism of action. Tacrolimus has a similar, but more
potent, mechanism of action compared with that of CsA.Efficacy. Patients that are unresponsive to CsA may
respond to tacrolimus.26,27 Formulation. Tacrolimus is generally compounded to a
0.03% ophthalmic aqueous suspension; however, formula-tions may vary.
Therapeutic recommendations. Apply 1 drop of topical tacrolimus Q 12 H, with a recheck STT in 1 month. Continue treatment for several months before considering treatment failure. In addition to increasing tear production, tacrolim-us may decrease clinical signs, such as pigmentation asso-ciated with chronic KCS, even if tear production does not increase, but no long-term studies exist.
Tacrolimus use for treating KCS in dogs is off-label; there-fore, the U.S. Food and Drug Administration approved therapy—CsA 0.2% ophthalmic ointment (Optimmune)— should be used as first-line treatment, with tacrolimus reserved for cases unresponsive to CsA.
3. PilocarpineMechanism of action. Parasympathomimetic drug (stimu-
lates or mimics the parasympathetic nervous sytem). Upreg-ulation of parasympathetic receptors secondary to denerva-tion results in increased sensitivity of the lacrimal system to pilocarpine when compared with the rest of the body.9
Efficacy. May be used to stimulate tear production in cases of neurogenic (quan-titative) KCS. These cases are diagnosed when ipsilateral dry nose is present in conjunction with a low result on STT.
Formulation. 1% or 2% solutionsTherapeutic recommendations. Sprin-
kle 1 to 2 drops of 2% pilocarpine per 10 kg on top of food Q 12 H. System-ic administration of pilocarpine is pre-ferred because it can be irritating when applied topically.28
Note that pilocarpine has a narrow therapeutic window, and while some cli-nicians advocate increasing the number of drops applied to food by 1 drop each day until systemic adverse effects are
observed—such as vomiting, diarrhea, ptyalism, anorexia, and bradycardia—we prefer to avoid these effects by only increasing the total dose by 1 or 2 drops before consider-ing pilocarpine ineffective. Client education about adverse effects is important.
Tear ReplacementTear replacement therapy provides lubrication until tear stimulants are effective. Lifelong tear replacement therapy may be needed in dogs that never respond to CsA or tacro-limus. These medications are available as solutions, gels, and ointments, and have a wide variety of constituents.
1. Artificial tear solutions commonly contain 0.1% to 1.4% polyvinyl alcohol. Artificial tear solutions are useful for removing debris and mucus from the ocular surface; however, they are not feasible as monotherapy in most dogs with KCS due to the need for frequent application in order to achieve adequate lubrication.
2. Cellulose-based solutions/gels and viscoelastic prod-ucts are more viscous and have slower evaporation times than artificial tear solutions. They require application Q 4 to 6 H. Examples of cellulose-based solution and viscoelastic products are hydroxypropyl and hyaluronate, respectively.
3. Artificial tear formulations containing petrolatum, mineral oil, or lanolin are the most viscous products and provide long-term lubrication, but can result in debris accumulation. They are best suited for patients with: • Lipid layer deficiencies• Lagophthalmos (administered prior to sleep)•Owners who will be absent for long periods.
AntibioticsA severe, mucopurulent discharge suggests a secondary bacterial infection. Generally, use a broad-spectrum oph-thalmic antibiotic, such as triple antibiotic ointment (neo-mycin/bacitracin/polymyxin B) Q 6 to 8 H for approxi-mately 2 weeks. If empirical treatment fails to resolve the discharge, perform culture and sensitivity.
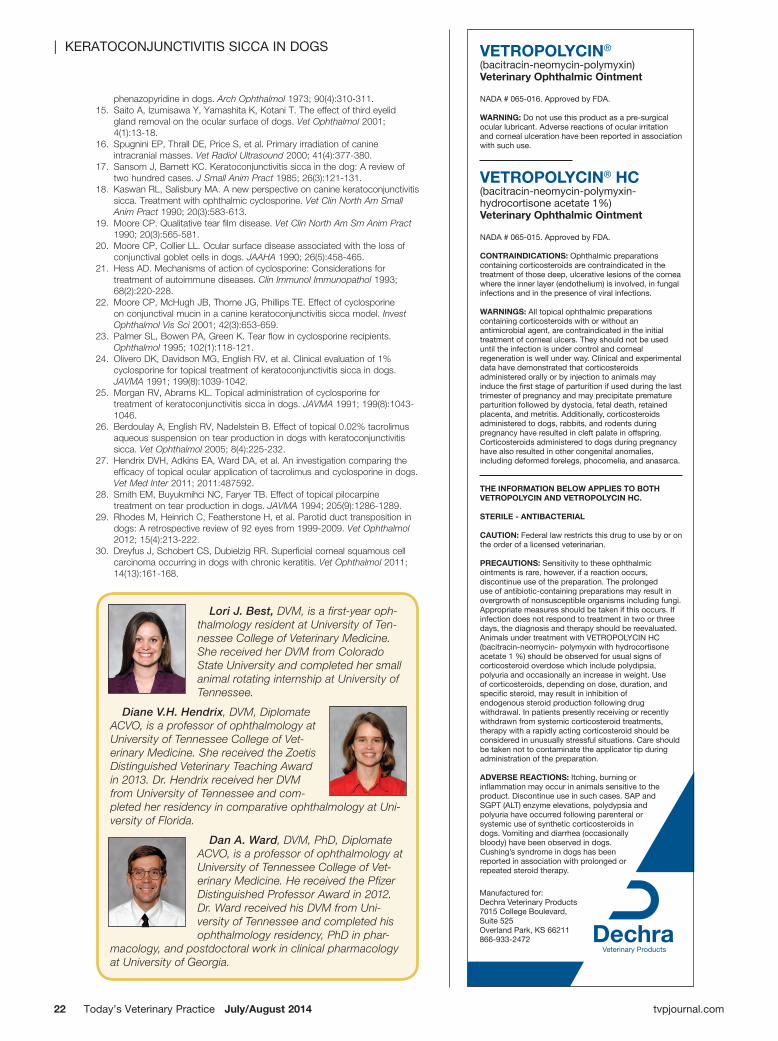
Figure 7. Seven-year-old spayed female miniature pinscher. Note corneal vascularization and pigmentation; STT was 7 mm/min (A). Same patient 3 months after topical CsA therapy; note resolution of corneal vascularization and thinning of pigment (B).
A B

July/August 2014 Today’s Veterinary Practice 21
Diagnosis & TreaTmenT of KeraToconjuncTiViTis sicca in Dogs |
tvpjournal.com
Anti-Inflammatory AgentsAnti-inflammatory therapy may be useful if conjunctival inflammation is severe, possibly occluding lacrimal excre-tory ducts. Corticosteroids can be used on a short-term basis (1–4 weeks); discontinue if patient is nonresponsive. Only consider using them, though, in animals with no uptake of fluorescein dye.
Apply topical prednisolone acetate 1% or dexamethasone 0.1% topically Q 6 to 8 H. Use caution when using topical corticosteroids because dogs with KCS can develop ulcer-ative keratitis, infection, and keratomalacia.
MucolyticsIf a patient with KCS has copious mucopurulent discharge, acetylcysteine 5% is often administered; however, its use is not common due to its expense and toxicity to the epithe-lium. In addition, the mucous layer provides some protec-tion to the cornea. Frequent flushing with sterile eyewash, instead, simply removes mucus without side effects.
SURGICAL MANAGEMENT OF KCSAfter 3 to 6 months of medical therapy with no response, surgical treatment for KCS can be considered. Surgery is not always successful and, even when it is, patients often need ongoing topical therapy.29
Treatment of ChoiceParotid duct transposition—in which the parotid duct and papilla are dissected free of the oral mucosa, mobilized, and transposed to the inferior cul-de-sac—is the surgical treatment of choice. Open and closed methods have been described.
ChallengesThis surgery is often performed by a board-certified oph-thalmologist due to the difficulty of the procedure in some dogs and often complicated aftercare. Potential complica-tions include severance of the duct, occlusion of the duct secondary to scar formation, development of white miner-al crystalline corneal deposits, facial dermatitis, periocular pyoderma, and excessive saliva production.
PROGNOSIS & MONITORINGPrognosis depends on the underlying etiology of KCS and the patient’s response to treatment (Table 2). If KCS does not respond to medical therapy, the prognosis is worse for vision retention. In addition, most patients will require life-long therapy with topical immunosuppressive medications.
Recently, chronic keratitis treated long-term with tacroli-mus or CsA has been tenuously associated with increased risk for corneal squamous cell carcinoma.30 However, because the study was retrospective, clinical data are lack-ing, and KCS alone may have resulted in a predisposition to this condition. While this study is interesting, KCS should be treated as described in this article.
Dogs with a diagnosis of KCS should be evaluated every 6 to 12 months to assess effect of treatment and progres-sion of disease. n
csa = cyclosporine a; Kcs = keratoconjunctivitis sicca; PTf = precorneal tear film; sTT = schirmer tear test; sTT1 = schirmer tear test 1; TbuT = tear film breakup time
References1. King-Smith PE, Fink BA, Fogt N, et al. The thickness of the human
precorneal tear film: Evidence from reflection spectra. Invest Ophthalmol Vis Sci 2000; 41(11):3348-3359.
2. Prydall JI, Artal P, Wood H, Campbell FW. Study of human precorneal tear film thickness and structure using laser interferometry. Invest Ophthalmol Vis Sci 1992; 33(6):2006-2011.
3. Franzco IC. Fluids of the ocular surface: Concepts, functions, and physics. Clin Exp Ophthalmol 2012; 40(6):634-643.
4. Herring IP, Pickett JP, Champagne ES, Marini M. Evaluation of aqueous tear production in dogs following general anesthesia. JAAHA 2000; 36(5):427-430.
5. Dodam JR, Branson KR, Martin DD. Effects of intramuscular sedative and opioid combinations on tear production in dogs. Vet Ophthalmol 1998; 1(1):57-59.
6. Sanchez RF, Mellor D, Mould J. Effects of medetomidine and medetomidine-butorphanol combination on Schirmer tear test 1 readings in dogs. Vet Ophthalmol 2006; 9(1):33-37.
7. Kaswan RL, Martin CL, Chapman WL. Keratoconjunctivitis sicca: Histopathologic study of nictitating membrane and lacrimal glands from 28 dogs. Am J Vet Res 1984; 45(1):112-118.
8. Martin CL, Kaswan R. Distemper-associated keratoconjunctivitis sicca. JAAHA 1985; 21(3):355-359.
9. Matheis FL, Walder-Reinhardt L, Spiess BM. Canine neurogenic keratoconjunctivitis sicca: 11 cases (2006-2010). Vet Ophthalmol 2012; 15(4):288-290.
10. Naranjo C, Fondevila D, Leiva M, et al. Characterization of lacrimal gland lesions and possible pathogenic mechanisms of keratoconjunctivitis sicca in dogs with leishmaniosis. Vet Parasit 2005; 133(1):37-47.
11. Westermeyer HD, Ward DA, Abrams K. Breed predisposition to congenital alacrima in dogs. Vet Ophthalmol 2009; 12(1):1-5.
12. Klauss G, Giuliano EA, Moore CP, et al. Keratoconjunctivitis sicca associated with administration of etodolac in dogs: 211 cases (1992-2002). JAVMA 2007; 230(4):541-547.
13. Trepanier LA, Danhoff R, Troll J, Watrous D. Clinical findings in 40 dogs with hypersensitivity associated with administration of potentiated sulfonamides. J Vet Intern Med 2003; 17(5):647-652.
14. Bryan GM, Slatter DH. Keratoconjunctivitis sicca induced by
ULCER THERAPyWhile superficial, uncomplicated ulcers can be treated with triple antibiotic ointment, csa, and lubricants, ulcers secondary to Kcs are usually complicated and require more intensive therapy.
1. Perform culture and cytology on stromal ulcers and ulcers with a cellular infiltrate.
2. Apply topical antibiotics Q 2 H to infected ulcers until the cornea stabilizes. appropriate antibiotics include:• ciprofloxacin 0.03% ophthalmic solution, or
other ophthalmic fluoroquinolones, used alone or
• Tobramycin 0.03% ophthalmic solution and cefazolin (33 mg/ml in artificial tear solution).
3. Use topical atropine to dilate the pupil and decrease ciliary spasm, even though it is associ-ated with decreased tear production. if the patient remains uncomfortable while on atropine therapy, the addition of oral nsaiDs may be considered.
4. Consider conjunctival graft placement in addition to Kcs therapy and frequent antibiotic therapy for deep ulcers.
| KeraToconjuncTiViTis sicca in Dogs
Today’s Veterinary Practice July/August 201422 tvpjournal.com
phenazopyridine in dogs. Arch Ophthalmol 1973; 90(4):310-311. 15. Saito A, Izumisawa Y, Yamashita K, Kotani T. The effect of third eyelid
gland removal on the ocular surface of dogs. Vet Ophthalmol 2001; 4(1):13-18.
16. Spugnini EP, Thrall DE, Price S, et al. Primary irradiation of canine intracranial masses. Vet Radiol Ultrasound 2000; 41(4):377-380.
17. Sansom J, Barnett KC. Keratoconjunctivitis sicca in the dog: A review of two hundred cases. J Small Anim Pract 1985; 26(3):121-131.
18. Kaswan RL, Salisbury MA. A new perspective on canine keratoconjunctivitis sicca. Treatment with ophthalmic cyclosporine. Vet Clin North Am Small Anim Pract 1990; 20(3):583-613.
19. Moore CP. Qualitative tear film disease. Vet Clin North Am Sm Anim Pract 1990; 20(3):565-581.
20. Moore CP, Collier LL. Ocular surface disease associated with the loss of conjunctival goblet cells in dogs. JAAHA 1990; 26(5):458-465.
21. Hess AD. Mechanisms of action of cyclosporine: Considerations for treatment of autoimmune diseases. Clin Immunol Immunopathol 1993; 68(2):220-228.
22. Moore CP, McHugh JB, Thorne JG, Phillips TE. Effect of cyclosporine on conjunctival mucin in a canine keratoconjunctivitis sicca model. Invest Ophthalmol Vis Sci 2001; 42(3):653-659.
23. Palmer SL, Bowen PA, Green K. Tear flow in cyclosporine recipients. Ophthalmol 1995; 102(1):118-121.
24. Olivero DK, Davidson MG, English RV, et al. Clinical evaluation of 1% cyclosporine for topical treatment of keratoconjunctivitis sicca in dogs. JAVMA 1991; 199(8):1039-1042.
25. Morgan RV, Abrams KL. Topical administration of cyclosporine for treatment of keratoconjunctivitis sicca in dogs. JAVMA 1991; 199(8):1043-1046.
26. Berdoulay A, English RV, Nadelstein B. Effect of topical 0.02% tacrolimus aqueous suspension on tear production in dogs with keratoconjunctivitis sicca. Vet Ophthalmol 2005; 8(4):225-232.
27. Hendrix DVH, Adkins EA, Ward DA, et al. An investigation comparing the efficacy of topical ocular application of tacrolimus and cyclosporine in dogs. Vet Med Inter 2011; 2011:487592.
28. Smith EM, Buyukmihci NC, Faryer TB. Effect of topical pilocarpine treatment on tear production in dogs. JAVMA 1994; 205(9):1286-1289.
29. Rhodes M, Heinrich C, Featherstone H, et al. Parotid duct transposition in dogs: A retrospective review of 92 eyes from 1999-2009. Vet Ophthalmol 2012; 15(4):213-222.
30. Dreyfus J, Schobert CS, Dubielzig RR. Superficial corneal squamous cell carcinoma occurring in dogs with chronic keratitis. Vet Ophthalmol 2011; 14(13):161-168.
Lori J. Best, DVM, is a first-year oph-thalmology resident at University of Ten-nessee College of Veterinary Medicine. She received her DVM from Colorado State University and completed her small animal rotating internship at University of Tennessee.
Diane V.H. Hendrix, DVM, Diplomate ACVO, is a professor of ophthalmology at University of Tennessee College of Vet-erinary Medicine. She received the Zoetis Distinguished Veterinary Teaching Award in 2013. Dr. Hendrix received her DVM from University of Tennessee and com-pleted her residency in comparative ophthalmology at Uni-versity of Florida.
Dan A. Ward, DVM, PhD, Diplomate ACVO, is a professor of ophthalmology at University of Tennessee College of Vet-erinary Medicine. He received the Pfizer Distinguished Professor Award in 2012. Dr. Ward received his DVM from Uni-versity of Tennessee and completed his ophthalmology residency, PhD in phar-
macology, and postdoctoral work in clinical pharmacology at University of Georgia.
VETROPOLYCIN® (bacitracin-neomycin-polymyxin) Veterinary Ophthalmic Ointment
NADA # 065-016. Approved by FDA.
WARNING: Do not use this product as a pre-surgical ocular lubricant. Adverse reactions of ocular irritation and corneal ulceration have been reported in association with such use.
VETROPOLYCIN® HC (bacitracin-neomycin-polymyxin- hydrocortisone acetate 1%)Veterinary Ophthalmic Ointment
NADA # 065-015. Approved by FDA.
CONTRAINDICATIONS: Ophthalmic preparations containing corticosteroids are contraindicated in the treatment of those deep, ulcerative lesions of the cornea where the inner layer (endothelium) is involved, in fungal infections and in the presence of viral infections.
WARNINGS: All topical ophthalmic preparations containing corticosteroids with or without an antimicrobial agent, are contraindicated in the initial treatment of corneal ulcers. They should not be used until the infection is under control and corneal regeneration is well under way. Clinical and experimental data have demonstrated that corticosteroids administered orally or by injection to animals may induce the first stage of parturition if used during the last trimester of pregnancy and may precipitate premature parturition followed by dystocia, fetal death, retained placenta, and metritis. Additionally, corticosteroids administered to dogs, rabbits, and rodents during pregnancy have resulted in cleft palate in offspring. Corticosteroids administered to dogs during pregnancy have also resulted in other congenital anomalies, including deformed forelegs, phocomelia, and anasarca.
THE INfORmATION bELOW APPLIES TO bOTH VETROPOLYCIN AND VETROPOLYCIN HC.
STERILE - ANTIbACTERIAL
CAUTION: Federal law restricts this drug to use by or on the order of a licensed veterinarian.
PRECAUTIONS: Sensitivity to these ophthalmic ointments is rare, however, if a reaction occurs, discontinue use of the preparation. The prolonged use of antibiotic-containing preparations may result in overgrowth of nonsusceptible organisms including fungi. Appropriate measures should be taken if this occurs. If infection does not respond to treatment in two or three days, the diagnosis and therapy should be reevaluated. Animals under treatment with VETROPOLYCIN HC (bacitracin-neomycin- polymyxin with hydrocortisone acetate 1 %) should be observed for usual signs of corticosteroid overdose which include polydipsia, polyuria and occasionally an increase in weight. Use of corticosteroids, depending on dose, duration, and specific steroid, may result in inhibition of endogenous steroid production following drug withdrawal. In patients presently receiving or recently withdrawn from systemic corticosteroid treatments, therapy with a rapidly acting corticosteroid should be considered in unusually stressful situations. Care should be taken not to contaminate the applicator tip during administration of the preparation.
ADVERSE REACTIONS: Itching, burning or inflammation may occur in animals sensitive to the product. Discontinue use in such cases. SAP and SGPT (ALT) enzyme elevations, polydypsia and polyuria have occurred following parenteral or systemic use of synthetic corticosteroids in dogs. Vomiting and diarrhea (occasionally bloody) have been observed in dogs. Cushing’s syndrome in dogs has been reported in association with prolonged or repeated steroid therapy.
Manufactured for:Dechra Veterinary Products7015 College Boulevard, Suite 525Overland Park, KS 66211866-933-2472

As with all drugs, side effects may occur. In field studies, the most common side effects reported were ocular itching, burning, or inflammation in animals sensitive to the product. Prolonged use may result in the overgrowth of non-susceptible organisms including fungi. VETROPOLYCIN ONLY— Do not use as a pre-surgical ocular lubricant. VETROPOLYCIN HC ONLY— This product is not for use in animals with corneal ulcers, fungal infections, or viral infections. Patients should be monitored for signs of corticosteroid overdose. The safe use of this product has not been evaluated in pregnant animals. Refer to the prescribing information for VETROPOLYCIN and VETROPOLYCIN HC for complete details or visit www.dechra-us.com.
Now you can treat your canine and feline patients with
the trusted ophthalmic products, VETROPOLYCIN®
(bacitracin-neomycin-polymyxin) and VETROPOLYCIN® HC
(bacitracin-neomycin-polymyxin-hydrocortisone acetate 1%), that
are FDA-CVM approved for use in dogs and cats. The
choice is clear. Contact your Dechra Representative or
your Veterinary Distributor
for more information.
24 Hour Technical Support available from trained Veterinary Professionals. | 866-933-2472
Buy 9, get 3 freeSome restrictions apply. Details are available from your Veterinary Distributor.
Limited time Offer
Dechrao p h t h a l m i c
o i n t m e n t s
a r e b a c k
Dechra Veterinary Products, 7015 College Blvd., Suite 525, Overland Park, Kansas 66211, 866-933-2472 www.dechra-us.com