Embed Size (px)
Citation preview

DOI: 10.1542/peds.2011-1663; originally published online March 12, 2012; 2012;129;e1060Pediatrics
Thomas O. CarpenterMichelle B. Vanstone, Sharon E. Oberfield, Laurel Shader, Laleh Ardeshirpour and
Hypercalcemia in Children Receiving Pharmacologic Doses of Vitamin D
http://pediatrics.aappublications.org/content/129/4/e1060.full.html
located on the World Wide Web at: The online version of this article, along with updated information and services, is
of Pediatrics. All rights reserved. Print ISSN: 0031-4005. Online ISSN: 1098-4275.Boulevard, Elk Grove Village, Illinois, 60007. Copyright © 2012 by the American Academy published, and trademarked by the American Academy of Pediatrics, 141 Northwest Pointpublication, it has been published continuously since 1948. PEDIATRICS is owned, PEDIATRICS is the official journal of the American Academy of Pediatrics. A monthly
at Indonesia:AAP Sponsored on January 13, 2013pediatrics.aappublications.orgDownloaded from

Hypercalcemia in Children Receiving PharmacologicDoses of Vitamin D
abstractVitamin D deficiency causes rickets, requiring vitamin D at dosesgreater than daily dietary intake. Several treatment regimens arefound in the literature, with wide dosing ranges, inconsistent monitor-ing schedules, and lack of age-specific guidelines. We describe 3 chil-dren, ages 2 weeks to 2 and 9/12 years, who recently presented to ourinstitution with hypercalcemia and hypervitaminosis D (25-hydroxy-vitamin D levels.75 ng/mL), associated with treatment of documentedor suspected vitamin D-deficient rickets. The doses of vitamin D usedwere within accepted guidelines and believed to be safe. The patientsrequired between 6 weeks and 6 months to correct the elevatedserum calcium, with time to resolution of hypercalcemia related toage and peak serum calcium, but not to peak 25-hydroxyvitamin Dlevel. With recent widespread use of vitamin D in larger dosages inthe general population, we provide evidence that care must be takenwhen using pharmacologic dosing in small children. With limiteddosing guidelines available on a per weight basis, the administrationof dosages to infants that are often used in older children and adultshas toxic potential, requiring a cautious approach in dose selectionand careful follow-up. Dosage recommendations may need to bereassessed, in particular, where follow-up and monitoring may becompromised. Pediatrics 2012;129:e1060–e1063
AUTHORS: Michelle B. Vanstone, MD,a Sharon E. Oberfield,MD,b Laurel Shader, MD,c Laleh Ardeshirpour, MD,a andThomas O. Carpenter, MDa
aDepartment of Pediatrics (Endocrinology), Yale University Schoolof Medicine, New Haven, Connecticut; bDivision of PediatricEndocrinology, Morgan Stanley Children’s Hospital of New York,Columbia University Medical Center, New York, New York; andcFairhaven Community Health Center, New Haven, Connecticut
KEY WORDShypervitaminosis D, hypercalcemia, rickets
ABBREVIATIONS1,25(OH)2D—1,25-dihydroxyvitamin D25-OHD—25-hydroxyvitamin DRDA—Recommended Dietary Allowance
www.pediatrics.org/cgi/doi/10.1542/peds.2011-1663
doi:10.1542/peds.2011-1663
Accepted for publication Nov 14, 2011
Address correspondence to Thomas O. Carpenter, MD,Department of Pediatrics, Yale University School of Medicine, POBox 208064, New Haven, CT 06520-8064. E-mail: [email protected]
PEDIATRICS (ISSN Numbers: Print, 0031-4005; Online, 1098-4275).
Copyright © 2012 by the American Academy of Pediatrics
FINANCIAL DISCLOSURE: The authors have indicated they haveno financial relationships relevant to this article to disclose.
FUNDING: No external funding.
e1060 VANSTONE et al at Indonesia:AAP Sponsored on January 13, 2013pediatrics.aappublications.orgDownloaded from

Pharmacologic dosages of vitamin Dare used to treat infants and childrenwith vitamin D deficiency rickets or hy-pocalcemia. One suggested treatmentregimen for symptomatic vitamin Ddeficiency in children recommends3000 to 15 000 IU daily for 4 to 6 weeks.1
Others suggest dosing by age: 1000 IU/day for infants ,1 month old, 1000 to5000 IU/day for 1- to 12-month-oldinfants, and .5000 IU/day for chil-dren .12 months old.2 With radio-graphic evidence of healing rickets, thedose may be reduced, but the sug-gested duration of pharmacologicdosing is as long as 2 to 3 months.Timely biochemical monitoring is crit-ical in avoiding hypercalcemia, andmost guidelines suggest documentingmarkers of a therapeutic response af-ter 1 month of treatment.
We describe mild hypercalcemia in 3children inwhomvitaminD therapywasprescribed for suspected nutritionalvitamin D deficiency. These cases raisethe concern that even recommendedtreatment doses have potential for tox-icity, especially if administered inap-propriately, or for too long a period oftime without biochemical monitoring.Recommended dose ranges have lim-ited data to support their use and mayexceed upper tolerable limits for in-fants and children.
CASE REPORTS
Case 1
This infantgirlwasbornat37.5weeksofgestation to a 34-year-old mother viaemergent cesarean delivery for mater-nal preeclampsia. There was no ma-ternal history of diabetes, excessivealcohol use or smoking, but a limiteddietary intake of dairy products. Sheself-administered prenatal vitamins, butreceived no other medications. Reviewof the mother’s medical record revealedhypocalcemia, elevated serum alkalinephosphatase activity, increased hepatictransaminases, and an elevated intact
serum PTH level (77 pg/mL, normal 10-65). An older sibling was healthy, andthe family had no history of musculo-skeletal disorders.
Craniotabes was noted on the first dayof life. Weight and length were at thefifth and 28th centiles, respectively. Nodysmorphic features or bone deform-ities were evident, and the results of theremainder of the physical examinationwere normal. Radiographs suggesteddecreased calvarial ossification, but acomprehensive skeletal survey wasotherwise unremarkable. The totalserum calcium level at birth was ap-propriate for the first 36 hours of life(8.2 mg/dL), and increased to typicallevels by day 3 (Table 1). Serum 1,25-dihydroxyvitamin D (1,25[OH]2D) levelwas 74 pg/mL (normal for age); a 25-hydroxyvitamin D (25-OHD) level wasnot obtained. On day 7, she receiveda single 1000-IU oral dose of vitamin D3.At 2 weeks of age, the serum 25-OHDlevel was 21 ng/mL, and she was as-sumed to have inadequate vitamin Dstores. Thus, she was prescribed 1000IU/day of vitamin D3, in addition to amultivitamin (Tri-vi-sol, supplying 400IU of vitamin D3 per day) providinga total of 1400 IU of supplemental vi-tamin D daily. The mother continued tobreastfeed and was supplementedwith 400 IU/day of vitamin D2.
After 2 months of this regimen (1400 IUof vitamin D per day), serum calcium
(10.7 mg/dL) and 25-OHD (84 ng/mL)levels were elevated (Table 1). The1000 IU vitamin D3 supplement was dis-continued, although Tri-vi-sol was con-tinued, providing 400 IU of vitamin D3per day. The infant remained healthy,with length at the 50th centile, andweight at the 10th centile. At 5 months,serum calcium and 25-OHD levelsremained elevated and mild hyper-calciuria was evident (Table 1). Thus,themultivitamin was discontinued, andadditional oral hydration was begun.
By 6 months of age her biochemistryvalues had normalized. Radiographsdemonstrated improved cranial min-eralization. She has not required ad-ditional therapies and remains wellwithout vitamin D supplementation.
Case 2
This 4-month-old African American boypresented during the winter with a sei-zure. He was an otherwise healthy 7-kginfant, with no pre- or postnatalcomplications. He met developmentalmilestones appropriately, received nomedications, and had no known aller-gies. He was exclusively breastfed,without vitamin D supplementation. Hismother had received no supplementalvitaminsormineral supplements for theprevious 2 to 3 months. Physical exam-ination resultswere unremarkable,withno dysmorphic features or abnormalneurologic findings.
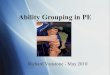
TABLE 1 Biochemical Values in Case 1 Before, During, and After Vitamin D Treatment
Before Vitamin D During and After Vitamin D
Age 1 d 3 d 12 d 2 mo 3 mo 5 mo 6 mo 7.5 mo 10 mo 24 moVitamin D (IU/day) — — 1400 1400 400 400 0a 0 0 0Calcium 8.2 9.3 — 10.7 10.2 11.0 10.2 11 10.5 9.9Phosphorous 5.0 7.6 — 6.5 7 5.9 5.6 5.8 4.7 4.2ALP (U/L) — — 265 429 393 — 265 — — 256iPTH — — — 11 — ,3 — — — —
25-OHD — — 21 84 69 78 65 55 58 331,25(OH)2D 74 — — 88 79 56 59 — 41 57Urine Ca/Cr ratio — — — — — 1.14 0.1 0.34 0.31 0.3
Reference values are as follows: calcium (8.8–10.2 mg/dL), phosphorous (2.2–4.2 mg/dL), iPTH (10–65 pg/mL), 25-OHD (.20ng/mL) 1,25(OH)2D (15–75 pg/mL), urine calcium to creatinine ratio (mg/mg) (normal for age,0.8). To convert from mg/dLto mmol/L: for calcium, multiply by 0.25; phosphorous, multiply by 0.323. To convert 25-OHD from ng/mL to nmol/L multiply by2.5. To convert 1,25(OH)2D from pg/mL to pmol/mL multiply by 2.6. ALP, alkaline phosphatase activity; iPTH, intact parathyroidhormone; Ca, calcium; Cr, creatinine.a Patient continued to receive ∼500 IU/day of vitamin D through dietary intake from 6 mo through follow-up.
CASE REPORT
PEDIATRICS Volume 129, Number 4, April 2012 e1061 at Indonesia:AAP Sponsored on January 13, 2013pediatrics.aappublications.orgDownloaded from

Initial biochemical evaluation revealedhypocalcemia (5.5mg/dL)andvitaminDdeficiency (Table 2). Electrocardiogramrevealed prolonged QT waves. Ricketsof the distal radius and ulna was evi-dent on radiographs. He was initiallytreated with intravenous calcium glu-conate, and subsequently with oralergocalciferol (4000 IU/day), calcitriol(0.5 mg/day), and calcium carbonate(100 mg/kg per day of elementalcalcium).
One week after hospital discharge, se-rum calcium (10.3 mg/dL) and 25-OHD(33 ng/mL) concentrations normalized.Thus, his ergocalciferol dose was de-creased to 2000 IU daily, calcitriol wasdiscontinued, and calcium supplemen-tationwas reduced to 50mg/kg per day.Six weeks later, a mild elevation in se-rumcalciumpersisted (10.4mg/dL), 25-OHDhad increased (79ng/mL), andmildhypercalciuria was evident (randomurine calcium/creatinine ratio, 0.9 mg/mg, normal ,0.8 mg/mg). All calciumand vitamin D supplementations were
discontinued. Six weeks later, serumcalcium normalized (10.1 mg/dL), andthere was a significant reduction in the25-OHD level (40 ng/mL).
Case 3
This 2 9/12-year-old African Americangirl was exclusively breastfed until 5months of age. Amultivitamin providing400 IU of vitamin D daily was prescribedduring the newborn period, but com-pliance with this regimen appearedlimited. At a 2-year well-child examina-tion, mild tibial bowing was observed.She remained primarily breastfed withsupplemental table foods. There hadbeen no previous hospitalizations ormajor illnesses, and no use of medi-cations. Biochemical evidence of vita-min D deficiency was documented(Table 2), and rickets was evident onlower extremity radiographs. She wasprovided 2000 IU of vitamin D daily withTri-vi-sol (containing 400 IU/day of vi-tamin D3) and ergocalciferol (1600 IU/day).
Threemonths later, hypercalcemia (10.9mg/dL) and hypervitaminosis D (25-OHD102 ng/mL) were evident, and vitamin Dsupplementation was discontinued. Af-ter3monthsoffvitaminDtherapy,serumcalcium (9.9 mg/dL) concentration nor-malized, and the 25-OHD level decreasedto 24 ng/mL. At this time, Tri-Vi-Sol wasresumed with the goal of providing 600IU of vitamin D per day, the Instituteof Medicine’s recently revised Recom-mended Dietary Allowance (RDA) forthis age group.3
DISCUSSION
Recent concerns regarding vitaminD deficiency in young children, witha high prevalence in African American,breastfed infants in northern latitudes4
has led to increased pharmacologicvitamin D therapy in this age group.Although vitamin D dosing schedules inthis setting are available,1,2 their safetymay depend on the severity of diseaseor deficiency, and duration of therapy.Because there are individual variationsin the calcemic response to vitamin D,there may well be a wide range ofresponses to a given dose.5 This vari-ance is likely due to differences in ab-sorption, metabolism, concentration ofvitamin D-binding protein in serum,and the capacity of storage sites.5
Furthermore, there is a lack of weight-based analyses of vitamin D dosing andkinetics; historically, RDAs have beenequivalent across much of childhoodand adult age ranges, despite largedifferences in body mass. Risk for tox-icity for many agents increases withhigher per body weight dosing, and theabsolute doses determined in adultsare likely unsafe for children. The casesdescribed herein suggest that the timeto resolution of hypervitaminosis D andhypercalcemia vary by age and peakserum calcium, but not by peak 25-OHDlevel (Table 2).
In addition to the aforementioned cases,we recently encountered a fourth child
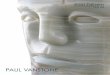
TABLE 2 Clinical Summary
Case 1 Case 2 Case 3
Age at initiation of treatment 2 wk 4 mo 2 and 9/12 yVitamin D dose, IU 1400/d 3 2 mo
400/d 3 3 mo4000/d 3 1 wk, 2000/d 3 6 wk 2000/d
Duration of treatment, wk 8 7 12Total vitamin D load, IU 120 000 112 000 168 000Clinician indication for treatment Craniotabes Hypocalcemic seizures Tibial bowingInitial biochemistry valuesCalcium, mg/dL 9.3 5.5 9.9Ionized calcium, mg/dL — 2.2 —
Phosphorus, mg/dL 7.6 6.4 4.9Alkaline phosphatase activity, U/L 265 1110 661Midmolecule PTH, nlEq/mLa — 58 —
Intact PTH, pg/mL — — 10225-OHD, ng/mL 21b ,5c 5d
1,25(OH)2D, pg/mL 74 7 156Peak calcium, mg/dL 11 10.4 10.9Peak 25-OHD, ng/dL 84 102 79Peak 1,25(OH)2D, pg/mL 88 Not obtained 165
Time to resolution of hypervitaminosis 6 mo 6 wk 3 mo
PTH, parathyroid hormone.a Reference ranges: Midmolecule PTH ,25; intact PTH10–69 pg/mL.b Measured at Esoterix Laboratories, Calabasas, California, by using high-performance liquid chromatography tandemmassspectrometry; reference range for all ages, 32–100 ng/mL.c Measured by using radioimmunoassay kit methodology (DiaSorin, Stillwater, Minnesota), reference range reported as.20 ng/mL.d Measured at Quest Diagnostics, by using liquid chromatography tandem mass spectrometry. Reference range reported as30–100 ng/mL.
e1062 VANSTONE et al at Indonesia:AAP Sponsored on January 13, 2013pediatrics.aappublications.orgDownloaded from

who was given high doses of vitamin Dfor an inappropriate indication, and notmonitoredby aphysician. This 3 and4/12-year-old girl presented with fatigue,abdominal pain, vomiting, constipation,headaches, polydipsia, nocturia, and ir-ritability.Duringtheprevious5weeks,shehad received a total 3 600 000 IU for ap-parent failure to thrive. Severe hyper-calcemia (17.4 mg/dL) was treated withintravenous saline, furosemide, andpamidronate. Twoweeks after discharge,serum calcium concentration had nor-malized (9.6 mg/dL). Similar cases ofhypervitaminosis D in children after high-dose supplementation for inappropriateindications are reported elsewhere.6 In 1recent series, seven children aged 7.5 to25 months were treated with 900 000 to4 000 000 IU of vitamin D for failure tothrive and developmental delay. All 7 hadhypercalcemia and hypercalciuria; neph-rocalcinosis was present in 5 patients.7
Upward modification of target thresh-olds for serum 25-hydroxyvitamin Dlevels in recent years has led to anincrease in the diagnosis of apparentvitamin D deficiency, and an increased
use of vitamin D supplements. Benefitsof this approach have yet to be demon-stratedby randomizedcontrolled trials.8
Recently, the Dietary Reference Intakesfor Calcium and Vitamin D (Institute ofMedicine, 2011)9 has provided evidence-based guidance for requirements, up-per tolerable limits of daily exposure,and target circulating 25-OHD levels forboth adults and children. The adequateintake of vitamin D for infants ,1 yearof age is 400 IU/day; the RDA is 600 IU forchildren aged 1 to 18 years, as well asthrough most of adulthood; the targetserum 25-OHD level is recommended as20 ng/mL (50 nmol/L).3
Because of the risk of toxicity, a conser-vative approach to therapy for vitamin Ddeficiency in infants and young chil-dren should be considered. Lower rangeof dosing, adjusted by appropriate bio-chemical monitoring is suggested, andshould include the measurement of se-rumcalciumwithinthefirst fewweeksoftherapy. Measurement of serum phos-phorus and alkaline phosphatase ac-tivity are helpful in the assessmentof expected biochemical and skeletal
response to therapy. Most notably, hy-percalcemia occurred in each of ourcases with the use of dosages withinwell-recognized recommendations fortreating vitamin D-deficient rickets,suggesting that treatment guidelinesfor vitamin D deficiency may requiremodification for this age group.
CONCLUSIONS
The incidence of hypervitaminosis Ddescribed in this series is far greaterthan we would expect on the basis onour own clinical observations duringthe previous 20 years. Vitamin D ther-apy, even when provided within estab-lished treatment guidelines, has thepotential to lead to toxicity in smallchildren when not monitored. We raisethe consideration that with heightenedawareness of vitamin D deficiency, andincreased prescribing of pharmaco-logic vitamin D to small children, anincreased risk of toxicity may also beemerging. Recommendations for vita-min D therapy require reexaminationfor safety in this age group.
REFERENCES
1. Pettifor JM. Rickets and vitamin D deficiencyin children and adolescents. EndocrinolMetab Clin North Am. 2005;34(3):537–553, vii
2. Misra M, Pacaud D, Petryk A, Collett-Solberg PF,Kappy M; Drug and Therapeutics Committee ofthe Lawson Wilkins Pediatric Endocrine Society.Vitamin D deficiency in children and its man-agement: review of current knowledge and rec-ommendations. Pediatrics. 2008;122(2):398–417
3. Ross AC, Manson JE, Abrams SA, et al. The2011 report on dietary reference intakes forcalcium and vitamin D from the Institute of
Medicine: what clinicians need to know.J Clin Endocrinol Metab. 2011;96(1):53–58
4. Ziegler EE, Hollis BW, Nelson SE, Jeter JM.Vitamin D deficiency in breastfed infants inIowa. Pediatrics. 2006;118(2):603–610
5. Plotkin H, Lifshitz F. Rickets and osteoporo-sis. In: Lifshitz F, ed. Pediatric Endocrinology.5th ed. New York, NY: Informa HealthcaseUSA; 2009:531–557
6. Barrueto F Jr, Wang-Flores HH, Howland MA,Hoffman RS, Nelson LS. Acute vitamin D in-toxication in a child. Pediatrics. 2005;116(3).
Available at: www.pediatrics.org/cgi/content/full/116/3/e453
7. Joshi R. Hypercalcemia due to hypervita-minosis D: report of seven patients. J TropPediatr. 2009;55(6):396–398
8. Reid IR, Avenell A. Evidence-based policy ondietary calcium and vitamin D. J Bone MinerRes. 2011;26(3):452–454
9. Institute of Medicine. 2011 Dietary Refer-ence Intakes for Calcium and Vitamin D.Washington, DC: The National AcademiesPress; 2011
CASE REPORT
PEDIATRICS Volume 129, Number 4, April 2012 e1063 at Indonesia:AAP Sponsored on January 13, 2013pediatrics.aappublications.orgDownloaded from

Wang et al. Morbidity and Mortality of Neonatal Respiratory Failure in China:Surfactant Treatment in Very Immature Infants. Pediatrics. 2012;129(3):e731–e740
Errors occurred in this article by Wang et al, titled “Morbidity and Mortality ofNeonatal Respiratory Failure in China: Surfactant Treatment in Very ImmatureInfants” published in the March 2012 issue of Pediatrics (2012;129[3]:e731–e740; originally published online February 13, 2012; doi:10.1542/peds.2011-0725).
1. On page e733, under Respiratory Support, on line 2 of the right column, itreads: “(range: 2.0–22.0 hours).” This should have read: “(IQR: 2.0–22.0hours).” (IQR is abbreviation of “interquartile range,” listed in Abbreviationson page e731.)
2. On page number e734, under Surfactant Therapy, on line 1 of the rightcolumn, it reads: “(range: 2.1–12.0 hours).” This should have read: “(IQR:2.1–12.0 hours).”
3. On page e735, left column, line 4: “.1500 g” should be “$1500 g.”
doi:10.1542/peds.2012-1481
Mohamed A, Shah PS. Transfusion Associated NecrotizingEnterocolitis: A Meta-analysis of Observational Data. Pediatrics. 2012;129(3):529–540
An error occurred in this article by Mohamed et al titled “TransfusionAssociated Necrotizing Enterocolitis: A Meta-analysis of Observational Data”published in the March 2012 issue of Pediatrics (2012;129[3]:529–540;originally published online February 20, 2012; doi:10.1542/peds.2011-2872).On page 538, under reference 39, “Gamma EL” should have read “LaGamma EF.”
doi:10.1542/peds.2012-1592
Vanstone et al. Hypercalcemia in Children Receiving Pharmacologic Doses ofVitamin D. Pediatrics. 2012;129(4):e1060–e1063
An error occurred in this article by Vanstone et al, titled “Hypercalcemia inChildren Receiving Pharmacologic Doses of Vitamin D” published in the April2012 issue of Pediatrics (2012;129[4]:e1060–1063; originally published onlineMarch 12, 2012; doi:10.1542/peds.2011-1663). On page e1061, under CaseReports (Case 1), line 80, this reads: “An older sibling was healthy, and thefamily had no history of musculoskeletal disorders.” This should have read:“The family had no history of musculoskeletal disorders.”
doi:10.1542/peds.2012-2194
ERRATA
PEDIATRICS Volume 130, Number 4, October 2012 763
ERRATA
at Indonesia:AAP Sponsored on January 13, 2013pediatrics.aappublications.orgDownloaded from

DOI: 10.1542/peds.2011-1663; originally published online March 12, 2012; 2012;129;e1060Pediatrics
Thomas O. CarpenterMichelle B. Vanstone, Sharon E. Oberfield, Laurel Shader, Laleh Ardeshirpour and
Hypercalcemia in Children Receiving Pharmacologic Doses of Vitamin D
ServicesUpdated Information &
htmlhttp://pediatrics.aappublications.org/content/129/4/e1060.full.including high resolution figures, can be found at:
References
html#ref-list-1http://pediatrics.aappublications.org/content/129/4/e1060.full.at:This article cites 6 articles, 3 of which can be accessed free
Citations
html#related-urlshttp://pediatrics.aappublications.org/content/129/4/e1060.full.This article has been cited by 1 HighWire-hosted articles:
Rs)3Peer Reviews (PPost-Publication
http://pediatrics.aappublications.org/cgi/eletters/129/4/e1060Rs have been posted to this article 32 P
Errata
htmlhttp://pediatrics.aappublications.org/content/130/4/763.3.full.see:An erratum has been published regarding this article. Please
Permissions & Licensing
tmlhttp://pediatrics.aappublications.org/site/misc/Permissions.xhtables) or in its entirety can be found online at: Information about reproducing this article in parts (figures,
Reprints http://pediatrics.aappublications.org/site/misc/reprints.xhtml
Information about ordering reprints can be found online:
rights reserved. Print ISSN: 0031-4005. Online ISSN: 1098-4275.Grove Village, Illinois, 60007. Copyright © 2012 by the American Academy of Pediatrics. All and trademarked by the American Academy of Pediatrics, 141 Northwest Point Boulevard, Elkpublication, it has been published continuously since 1948. PEDIATRICS is owned, published, PEDIATRICS is the official journal of the American Academy of Pediatrics. A monthly
at Indonesia:AAP Sponsored on January 13, 2013pediatrics.aappublications.orgDownloaded from