Embed Size (px)
DESCRIPTION
This powerpoint presentation is about children's oncology.
Citation preview

Pediatric OncologyPediatric Oncology

Why are we discussing Why are we discussing pediatric oncology?pediatric oncology?
• Childhood cancer accounts for only 2% of all cancer cases
• Childhood cancer has an overall survival rate of 80%– Acute Lymphocytic Leukemia (ALL)
is over 90%

HOWEVER:HOWEVER:• Cancer is still the leading cause
of death in children from disease– Second to accidents
• Diagnosis is a life-changing one for the patient and all members of the family– Fear of the unknown difficult to
overcome and always in the background

CausesCauses• Cancer by itself needs to be viewed as an assortment
of “genetic” diseases– Not to be confused with hereditary
• Cause is usually not determined• Most view cancer etiology as multifactorial• Types of cell damage
– Conversion of proto-oncogenes (regulate cell growth) into oncogenes (abnormal growth)
– Inactivation of tumor suppressor genes– Bypass of DNA repair gene that tells cell to die after
damaged– Two-hit model

Acquired Capabilities of CancerAcquired Capabilities of Cancer
Essentials of Pediatric Oncology Nursing: A Core Curriculum, 2nd Ed. (2004) p. 16

Characteristics of Childhood Ca Vs. Cancer in AdultsCharacteristics of Childhood Ca Vs. Cancer in Adults
Childhood• Rare 1-2% of all cases• Tissues CNS, muscle, bone,
reticuloendothelial system• Brief latency• Genetic alterations a major
role• Minimal opportunity for
prevention• Small opportunity for
screening
Adults• 98-99% of all cases• Organs-breast, lungs, colon,
prostate• Latency may be 20+ years• Environmental & lifestyle
factors more than genetics• 80% estimated to be
preventable• Many can be detected by
screening methods
Essentials of Pediatric Oncology Nursing: A Core Curriculum, 2nd Ed. (2004) p. 12

Characteristics Characteristics (cont.)(cont.)
Childhood• Metastatic in 80% of cases• Pharmacokinetics
– Markedly different in children because of rapid developmental changes
– Many common tumor types responsive to chemo
– May tolerate higher doses & less difficulty with acute toxicity
– Vulnerable to long-term effects
• Genetic testing very rare• Treatment per research
protocols very common• Prognosis 70-90% cure
Adults• Local or regional disease• Pharmacokinetics
– Common tumor types less responsive to available chemo
– May have more difficulty with acute toxicity
– Less issues with long-term effects
• Genetic testing more common where available
• Treatment per research protocols less common
• Prognosis <60% cure Essentials of Pediatric Oncology Nursing: A Core Curriculum, 2nd Ed. (2004) p. 12

7 Cardinal Signs of Ca in Children7 Cardinal Signs of Ca in Children• These signs can also occur in nonmalignant
conditions– Presence of a mass– Purpura– Pallor– Weight loss– Whitish reflex in the eye– Vomiting in the early AM– Recurrent or persistent fever

5 More covert signs/symptoms5 More covert signs/symptoms• These also can easily occur in nonmalignant
conditions– Bone pain
• Increased concern if pain awakens child at night
– Headache• Especially in the morning upon awakening
– Persistent lymphadenopathy– Change in balance, gait, personality– Fatigue, malaise

Diagnostic TestsDiagnostic Tests• CBC with diff• CMP• LDH• Alkaline Phosphate• Uric acid• Alpha fetoprotein• Cathecholamines (urine)• Cytogenetic studies• Chest x-ray
• Bone marrow– Aspirate and biopsy
• CT Scans• MRI• PET Scan• Bone Scan• Lumbar Puncture• Biopsies
These tests are disease/symptom specific

Treatment for Childhood CancerTreatment for Childhood Cancer• Three major types of treatment
– Surgery• Can occur at different points of treatment plan• Biopsies• Staging• Debulking• Surgery due to complications of illness• Palliation• Placement of venous access devices

Treatment of Childhood Ca Treatment of Childhood Ca (cont.)(cont.)
– Chemotherapy• Can occur by itself or with surgery and/or radiation• Goals
– Reduce tumor volume & prevent tumor cell division & spread– Designed to kill tumor cells during different phases of cell cycle– Given as combination agents to thus attack cells during different
stages at the same time– Goals can be
• Cure, control, and/or palliation
• Roles– Multimodal, Neoadjuvant, Adjuvant, Sanctuary, Palliative
• Modes of delivery– IV, PO, IM, IT

Treatment of Childhood Ca Treatment of Childhood Ca (cont.)(cont.)
– Radiation Therapy (RT)• Goal is to target the tumor while sparing the surrounding
tissues• Causes single or double strand DNA breaks• Important to maintain Hgb >10
– Hypoxic cells are more resistant to RT
• Many different methods of delivery• Not used in all types of childhood ca

LeukemiaLeukemia• Is a neoplastic disease that involves the blood-
forming tissues of the bone marrow, spleen, and lymph nodes
• During blood cell production the white blood cell precursors proliferate in an abnormal, uncontrolled, and destructive manner– These immature cells crowd into all available
spaces– Production of normal cells is limited due to lack of
space and nutrients

Leukemia Leukemia (cont.)(cont.)
• The type of leukemia will depend on what cell line is affected and the level of cellular differentiation– ALL – Acute Lymphocytic leukemia
• 75-80%
– AML – Acute Myelogenous Leukemia• 2-25%
– CML – Chronic Myelocytic leukemia• Less than 5%
• Cytogenetic abnormalities are found in more than 90% of patients with ALL– Number of chromosomes and structure

Presenting Signs/SymptomsPresenting Signs/Symptoms• Fever• Anemia
– Malaise, fatigue, pallor
• Thrombocytopenia– Bruises, petechiae, bleeding
• Hepatosplenomegaly• Bone pain (23% of cases)• Lymphadenopathy• CNS disease (less than 10% of cases at diagnosis)
– Headache, vomiting, visual disturbances

TreatmentTreatment• Varies with diagnosis and risk group• AML receives induction chemotherapy to “clear”
marrow and put patient into remission (marrow clear of blasts cells)
• Frequently these patients will require an allogenic stem cell transplant if a matched related donor is available
• CNS prophylaxis is given to prevent CNS relapse– Treated even if CNS is “clean” at diagnosis

Treatment for ALLTreatment for ALL• Divided into 3 phases• Induction (first month of therapy)
– Goal is to eliminate as many leukemia cells in marrow as possible
– During beginning of this period patients are at risk for tumor lysis syndrome
– Includes CNS treatment along with combination chemotherapy (IV, PO, IM)
• Consolidation (usually for around 1 year)– Includes CNS treatment along with chemotherapy– Requires more hospital admissions for chemo

Treatment for ALL Treatment for ALL (cont.)(cont.)
• Maintenance (usually for 2-3 years)• Goals are:
– Maintain remission– Prevent drug resistance from developing– Minimize long-term side effects
• Includes CNS treatment along with combination chemotherapy (PO, IM, IV)
• Recurrent disease– Treatment will vary depending on when relapse
occurred

Leukemia Case StudyLeukemia Case Study• 4 year old male with one week history of low
grade fevers and fatigue• Parents brought child to primary MD this
morning due to bruises they noticed• CBC done in the office lab showed peripheral
blasts• Child and parents sent to tertiary hospital for
admission and consult with oncology• Over the next 24-72 hrs diagnosis is made,
bone marrow & LP performed, central line is placed and treatment is begun

Audience Participation TimeAudience Participation Time
• What types of issues would you the nurse have to address/deal with while caring for this patient/family?
• What important nursing routines need to occur?

Nursing CareNursing Care• Emotional support• Strict I & O’s• Monitor labs• Blood products as
needed• Assist with procedures• Monitor for side effects
Pain relief
• Education– Illness– Treatment– Care at home– Effects on other family
members
• Administer chemo & other medications
• HANDWASHING!!REMEMBER- Care involves more than just the patient, includes parents, siblings, and possibly extended family members. Life-changing diagnosis with possible fatal outcome. Fear constantly in the background, lots of new information to absorb and grasp.

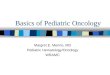
OsteosarcomaOsteosarcoma• Malignant tumor of the
bone• Occurs earlier in
females– Due to growth spurt
• More common in males
• Usually affects long bones
• Predominately during 2nd decade of life
Males
Females
0
10
20
30
40
50
60
10 20 30 40
%

Presenting Signs/SymptomsPresenting Signs/Symptoms• Pain
– Dull, aching, constant– Worse at night– Frequently attributed to trauma
• Swelling of soft tissue (possible)
• Altered gait (possible)
• 20% have visible metastatic disease (pulmonary) at initial diagnosis

TreatmentTreatment• Combination chemotherapy• Surgery
– Limb salvage or amputation
• Continued chemotherapy• Usually at least one year for entire course• Patients need to be cautioned to be careful with
the affected limb prior to surgery– Pathologic fracture always a possibility
• If pulmonary mets present may need thoracotomy performed in the future

Osteosarcoma Case StudyOsteosarcoma Case Study• 15 year old male has sports physical performed
and MD noted small amount of swelling on distal femur and pt c/o of increased pain while sleeping
• X-ray obtained and mass noted• Referred to orthopedic surgeon at tertiary
center– Biopsy performed and pt diagnosed with
osteosarcoma and referred to oncology– Diagnostic tests performed as an outpatient– Pt admitted 1 week later SDA s/p line placement
and will start chemotherapy this afternoon

Audience Participation Time Again!Audience Participation Time Again!
• What differences do you see in this case study compared to leukemia case study?
• Anything different in terms of nursing care?

Ewing’s SarcomaEwing’s Sarcoma
• Bone tumor– RADIOSENSITIVE
• May also develop in soft tissues
• Small, round, blue-cell tumor
• Translocation t (11;22)
• Caucasian (non-Hispanic) or Hispanic– Very rare in Asian or African descent

Presenting Signs/SymptomsPresenting Signs/Symptoms• Pain
– Intermittent, present for 3-9 months
• Palpable mass
• Pathological fractures more common
• Fever may be present

TreatmentTreatment
• Basically the same as osteosarcoma although the chemotherapy agents are different– Still chemo, surgery, more chemo
• Possible radiation therapy– Usually used if patient has reoccurrence

Brain TumorsBrain Tumors• Most common solid tumor in childhood ca
– Astrocytomas (also called Gliomas)• 50% of all pediatric brain tumors• Malignant or benign depending on histology• Can occur in a variety of areas of the brain and/or spine
– Medulloblastoma• 25% of all pediatric brain tumors• Most common malignant CNS tumor• Usually in cerebellum or 4th ventricle
– Hydrocephalus often occurs
– Ependymoma (10% of all cases)

Presenting Signs/SymptomsPresenting Signs/Symptoms• Symptoms vary depending on location of tumor• Sudden onset of symptoms more common in
aggressive tumors• Types of symptoms
– Headache (especially upon awakening in morning)– Vomiting– Ataxia– Nystagmus– Cranial nerve deficits– Visual changes– Seizures

TreatmentTreatment• Surgery
– Goal is maximum resection of tumor• Frequently seen by neurosurgeon before oncologist
• Radiation therapy – Delayed in children <3yrs of age
• Chemotherapy– Used to delay radiation in younger children
• High dose chemotherapy followed by autologous stem cell transplant– Highly malignant tumors with minimal residual
disease

NeuroblastomaNeuroblastoma• Most common extracranial solid tumor in
children (8-10%)
• Develops from neural crest cells– Anywhere along the sympathetic nervous system
• Chest, abdomen (may cross the midline), adrenal glands, head, pelvis
• Most common malignancy in infants– Diagnosis at < 1yr best prognosis– Phenomenon of spontaneous tumor regression &
maturation of the tumor can occur in this age group

Neuroblastoma Neuroblastoma (cont.)(cont.)
• Usually diagnosed between age 2-5
• “silent tumor” – Widespread metastatic disease in 70% of pts at
diagnosis• Sites include
– Lymph nodes– Bone– Bone marrow– Liver – Subcutaneous tissue
• Hardened bluish nodules
• Rarely spreads to lung and brain

Presenting Signs/SymptomsPresenting Signs/Symptoms• Pain
• Abdominal mass
• Malaise
• Cathecholamine secretion– HTN, flushing, excessive sweating, irritability
• Unique paraneoplastic syndrome (seen in 4% of pts)
– Opsomyoclonus• Myoclonic jerking and random eye movements
– Cerebellar ataxia

TreatmentTreatment• Treatment & prognosis depend on staging and
age of child
• Includes:– Surgery– Chemo– Radiation– Stem cell transplant

LymphomaLymphoma• Hodgkin’s & Non-Hodgkin’s Lymphoma (NHL)• NHL
– Malignant solid tumor of the immune system involving lymphoid cells
– Is a generalized disease at presentation– Disease spreads in a random, diffuse,
unpredictable, and aggressive manner• Quick diagnosis and rapid initiation of treatment is crucial
– Responds rapidly to chemo so need to be very watchful for tumor lysis syndrome
– Can involve T & B cell lines• Different subdivisions based on cell line involved

Presenting Signs/SymptomsPresenting Signs/Symptoms• Vary with site of disease
– Abdomen• Pain, N/V, change in bowel habits, distension
– Mediastinum• Dysphagia, cough, wheeze, strider, superior vena cava
syndrome
– Head and Neck• Cervical lymphadenopathy, jaw swelling, unilateral
tonsillar enlargement
– Bone marrow• Pallor, anemia, thrombocytopenia

Hodgkin’sHodgkin’s• A specific type of lymphoma that involves the
spleen and lymphatic system
• Characterized by binucleate or multinucleated giant cells
• 5% of all childhood cancers
• 3 distinct forms– Childhood (14 yr and younger)– Young adult (15-34)– Older adult (55-74)

Presenting Signs/SymptomsPresenting Signs/Symptoms• Painless supraclavicular or cervical adenopathy
• 2/3 of pts have mediastinal involvement– Coughing, s/s of airway obstruction
• Fatigue
• Anorexia
• 3 constitutional “B” symptoms – (correlate with prognosis)– Unexplained fever above 38 C– Unexplained weight loss (10% within 6 months)– Drenching night sweats

TreatmentTreatment
• Treatment – Either or both:
• Chemotherapy• Radiation therapy
• Children & adolescents in the favorable prognostic group have a 95% cure rate

RetinoblastomaRetinoblastoma• Intraocular tumor
– 80% pts are under age 4 yrs– Familial form in 40% of cases
• Predisposed affected patient to secondary neoplasms
• Presentation– Leukocoria (cat’s eye reflex)
• Lack of normal red reflex of the eye
– Strabismus– Esotropia or exotropia– Decreased vision in one eye

TreatmentTreatment
• Treatment (one or more of these therapies)– Enucleation– Radiation– Cryotherapy or thermotherapy– Chemotherapy– Laser photocoagulation

Wilm’s TumorWilm’s Tumor• Tumor of the kidney
• 6% of all childhood cancers
• Familial cases 1-2%
• Presentation– Asymptomatic abdominal mass– (20-30% of pts)
• pain• Malaise• Hematuria• HTN

TreatmentTreatment• Surgery
• Chemotherapy– Based on staging– Possibly prior to surgery
• Radiation therapy– Based on staging
• 80-more than 90% cure rate including stage IV disease

RhabdomyosarcomaRhabdomyosarcoma• Tumors that arise from cells of skeletal muscle
lineage– Can occur in tissues in which striated muscle cells
are not normally found
• Presentation– Mass or disturbance of normal body function
• Head and neck including orbits (35%)• Genitourinary tract (22%)• Extremities (18%)• Other sites (25%)
– Trunk, pelvis, retroperitoneal, biliary tract, liver, brain, trachea, heart, breast, ovary

General Nursing CareGeneral Nursing Care• Varies with what stage of illness is
occurring
• REMEMBER THIS IS A CHRONIC DISEASE WITH ACUTE PERIODS
• Teaching and reinforcement of teaching is common thread to all stages of illness

Newly DiagnosedNewly Diagnosed• Many questions
• Need for emotional support
• Lots of important decisions to be made– In a fairly short period of time
• May want second opinion
• Lots of teaching
• Nursing needs– I & O -Surgical post-op
needs– Blood products -Reverse isolation

TreatmentTreatment• Frequent admissions
– Weekly to q 3 weeks is norm
• I & O
• Large amount of hydration
• Chemo administration
• Monitor labs
• Supportive management– Nausea and vomiting
• Reinforce teaching

Neutropenia Neutropenia other non-scheduled admitsother non-scheduled admits
• Neutropenia is the #1 dose-limiting symptom for chemotherapy
• Emergency admission– Can occur 7-10 days after chemo txment
• High risk for sepsis
• Close monitoring of v/s and labs
• Antibiotics -I & O
• -Supportive management– Pain, mucositis, fatigue

End of TreatmentEnd of Treatment
• Happy to be over with treatments but fearful at same time to have them end– Support system from staff may be less– Fear of return of cancer– Change in routines
• Especially for younger patients

ReoccurrenceReoccurrence
• No longer naïve-fully aware of what is involved
• Body tired from previous chemotherapy cycle– May develop side effects quicker and/or more
severely
• Reality that cure is less of a possibility

End StageEnd Stage
• Acceptance of terminal stage may or may not have occurred
• Could be giving supportive care only
• May still be giving active treatment

Survivorship IssuesSurvivorship Issues• Long term effects to major organ systems
– Renal, cardiac– Can occur many years after therapy completed
• Genetic issues
• Hearing impairments
• Hepatitis C
• Infertility and sexuality issues
• Insurance

Survivorship Issues Survivorship Issues (cont.)(cont.)
• Learning disabilities
• Limb loss
• Secondary cancers
• Importance of yearly follow-ups with practitioners that are knowledgeable of survivorship issues!!

• Life-changing diagnosis that affects the entire family
• Patient may be medical or surgical at different times in their treatment course
• Treatment courses can last for 1-3 years of more if relapses occur
• Fear in the background even if not obvious
• Try to encourage families to maintain normalcy as much as possible– Home, school, friends
• Balance your involvement!