Embed Size (px)
Citation preview

PEDIATRIC HEART MURMURS
Manish Bansal, MD Clinical Assistant Professor
Division of Pediatric Cardiology University of Iowa
Murmur
murmur. (n.d.). Dictionary.com Unabridged. Retrieved March 9, 2018 from Dictionary.com website http://www.dictionary.com/browse/murmur

Murmur
• Sound or noises made by blood • Caused by abnormal flow patterns
– Abnormalities of the heart valves – Holes within the heart – Abnormal communications between blood vessels or
between blood vessels and the heart. • Often innocent and result from the normal patterns
of blood flow through the heart and vessels

Incidence and prevalence
• Revealed in over 50% of children and adolescents, with a peak incidence between 8 to 12 years
• CHD - 50-100/1000 live births • CHD may occur in presence of absence of heart
murmur • 6 cases per 1000 were moderate or severe
• Pediatr Cardiol. 1994 Nov-Dec; 15(6):282-7

History
History
• Feeding difficulties – appr 1/3 with CHD • Acute heart Failure
– Dyspnea (74%) – Nausea and vomiting (60%) – Fatigue (56%) – Cough (40%)
• Exercise intolerance – age appropriate history – Ability to play and the duration and vigor of feeding – Ability to participate in team sports with that of peers
History
• Chest pain is rarely a symptom of cardiac disease in children
• Chest pain or syncope prompted consultation in approximately 10 percent of children; only 11 percent of those with chest pain and 5 percent of those with syncope had cardiac disease.
• Pediatrics. 2004;114(4):e409-e417

History

Physical Examination
• Vitals compared with age appropriate norms. http://www.cc.nih.gov/ccc/pedweb/pedsstaff/age.html
• Focused examination of respiratory, cardiovascular and GI system.
• General appearance, activity level, color and respiratory effort
• Neck: prominent vessels, abnormal pulsations and bruits.
• Chest: abnormalities of sternum, abnormal cardiac impulse or thrills.

Physical examination
• Lungs – Abnormal breath sounds
• Abdomen – Liver location, enlargement or ascites
• Pulse: rate, rhythm, volume, character and capillary refill time

Examination of heart

Properties of a Murmur
• Timing - systolic vs diastolic • Duration-length in systole or diastole • Location—where in the heart they may originate • Quality or pitch—how they sound. This is important
in differentiating normal flow murmurs from the abnormal.
• Intensity or loudness—does not necessarily define the severity, but changes in intensity may help determine the type of murmur being heard.
• Presence of an extra sound called “a click”

Grading

My grading
• Grade 1: I can hear it (very faint) • Grade 2: resident can hear it easily (easily heard) • Grade 3: Medical student can hear it (can’t miss it!!) • Grade 4: Thrill • Grade 5: Stethoscope half of the chest • Grade 6: Stethoscope over the chest barely touching

Murmur (frequency or pitch)

Red flags (odds ratio OR) for pathologic murmur
• Holosystolic murmur (OR = 54) • Grade 3 or higher (OR = 4.8) • Harsh quality (OR = 2.4) • An abnormal S2 (OR = 4.1) • Maximal intensity at the upper left sternal border
(OR = 4.2) • Systolic click (OR = 8.3), • Diastolic murmur, or increased murmur intensity with
standing

Innocent murmurs
• May be heard in virtually anyone • Most often heard in childhood. • AKA
– Functional murmur – Flow murmur – Benign murmur – Normal murmur – Non pathologic murmur – In organic murmur

Innocent murmurs (seven S’s)
• Sensitive (changes with child’s position or with respiration)
• Short duration (not holosystolic) • Single (no associated clicks or gallops) • Small (murmur limited to a small area and non
radiating) • Soft (low amplitude) • Sweet (not harsh sounding) • Systolic (occurs during and is limited to systole)
Still murmur
• Still murmur – Grade 1 to 3 – Early systolic murmur – Low to medium pitch with a vibratory or musical quality – Best heard at lower left sternal border – Loudest when patient is supine and decreases when
patient stands – Infancy to adolescence, often 2 to 6 years – Can sound like Ventricular septal defect or hypertrophic
cardiomyopathy

Aortic Flow murmur
• Systolic ejection murmur best heard over the aortic valve
• Older childhood into adulthood • Usually result of increased flow velocity from the
larger stroke volume passing through relatively narrow LVOT and aortic valve annulus
• Pediatr Cardiol 27:19–24, 2006

Mammary artery soufflé
• High-pitched systolic murmur that can extend into diastole
• Best heard along the anterior chest wall over the breast
• Rare in adolescence • Arteriovenous anastomoses or patent ductus
arteriosus

Pulmonary flow murmur
• Grade 2 or 3 • Crescendo-decrescendo • Early- to mid-systolic murmur peaking in mid-systole • Best heard at the left sternal border between the second
and third intercostal spaces • Characterized by a rough, dissonant quality • Loudest when patient is supine and decreases when
patient is upright and holding breath • Heard in all ages • Can be confused with Atrial septal defect or pulmonary
valve stenosis

Supraclavicular/ brachiocephalic systolic murmur
• Brief, low-pitched, crescendo-decrescendo murmur heard in the first two-thirds of systole
• Best heard above clavicles • Radiates to neck • Diminishes when patient hyperextends shoulders • Childhood to young adulthood • D/D Bicuspid/stenotic aortic valve, pulmonary valve
stenosis, or coarctation of the aorta
Venous hum
• Grade 1 to 6 continuous murmur • Accentuated in diastole • Whining, roaring, or whirring quality • Best heard over low anterior neck, lateral to the
sternocleidomastoid • Louder on right • Resolves or changes when patient is supine • 3 to 8 years • D/D Cervical arteriovenous fistulas or patent ductus
arteriosus

Distribution of normal murmurs
Acta Informatica Medica. 2016;24(2):94-98
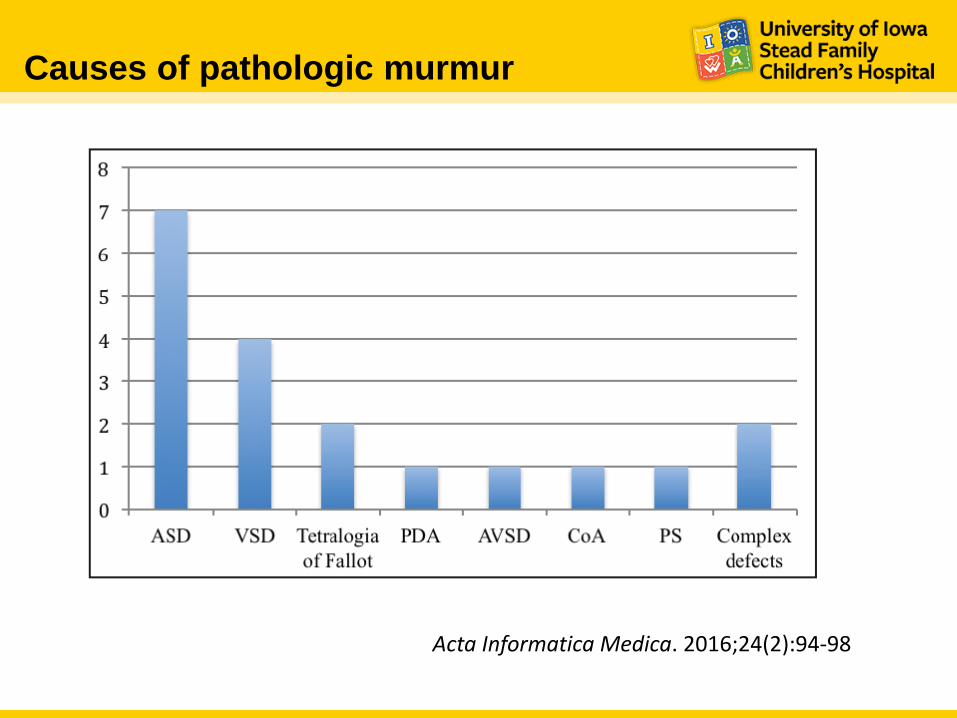
Causes of pathologic murmur
Acta Informatica Medica. 2016;24(2):94-98

Common Pathologic heart murmurs
Lesion Prevalence amongst children with CHD (%)
Clinical features Murmur characteristic
VSD 20-25 Small defects: usually asymptomatic Medium or large defects: CHF, symptoms of bronchial obstruction, frequent respiratory infections
Small: loud holosystolic murmur at LLSB Medium and large defects: prominent left ventricular impulses; thrill at LLSB; split or loud single S2; SEM to holosystolic murmur at LLSB without radiation; may also hear a grade 1 or 2 mid-diastolic rumble
ASD 8-13 Usually asymptomatic 2 or 3 SEM best heard at ULSB; wide split fixed S2; may have a grade 1 or 2 diastolic flow rumble at LLSB

Common Pathologic heart murmurs
Lesion Prevalence amongst children with CHD (%)
Clinical features Murmur characteristic
PDA 6-11 May be asymptomatic; can cause easy fatigue, CHF, and respiratory symptoms
Continuous murmur normal S1; S2 may be “buried” in the murmur; thrill or hyperdynamic left ventricular impulse may be present
Tetralogy of Fallot 10 Depends on the severity of PS
Central cyanosis; clubbing ; grade 3 or 4 long systolic ejection murmur heard at ULSB; increased S1; single S2
Pulmonary stenosis 7.5-9 Usually asymptomatic Systolic ejection murmur (grade 2 to 5); at ULSB radiating to infraclavicular regions, axillae, and back; normal or loud S1; variable S2; systolic ejection click

Common Pathologic heart murmurs
Lesion Prevalence amongst children with CHD (%)
Clinical features Murmur characteristic
Coarctation of Aorta 5.1-8.1 Newborns and infants: CHF Older children: hypertension, leg pain
SEM at back, decreased femoral pulses. BP lower in legs than arms
Aortic stenosis 5-6 Usually asymptomatic Moderate to severe: chest pain with exertion, dyspnea
SEM at RUSB radiating to carotids
TGA 5 Variable presentation Cyanosis. Murmur may be absent
TAPVR 2-3 Onset of CHF at 4-6 weeks Grade 2-3 systolic ejection murmur at ULSB; grade 1 or 2 mid-diastolic flow rumble at LLSB; wide split fixed S2
HLHS Rare May be asymptomatic at birth but cyanosis and CHG develop within first 2 weeks
Hyperdynamic precordium; single S2; nonspecific grade 1 or 2 systolic ejection murmur along left sternal border

Physiologic interventions
Auscultatory events Intervention and response
Valvar aortic stenosis Louder following a pause after a premature beat
HCM Louder on standing, Valsalva maneuver. Fainter with prompt squatting
Mitral regurgitation Louder on sudden squatting or with isometric handgrip
Mitral valve prolapse Midsystolic click moves toward S1 and late systolic murmur Starts earlier on standing; click may occur earlier on Inspiration; murmur starts later and click moves toward S2during squatting
Tricuspid regurgitation Louder with inspiration
VSD Louder with isometric grip

Physiologic interventions
Auscultatory events Intervention and response
Aortic regurgitation Louder with sitting upright and leaning forward, sudden squatting, and isometric handgrip
Mitral stenosis Louder with exercise, left lateral decubitus position, coughing
Continuous murmurs - Patent ductus arteriosus
Diastolic phase louder with isometric handgrip
Cervical venous hum Disappears with direct compression of Jugular vein

Role of diagnostic testing
• CXR rarely assist with diagnosis in an asymptomatic patient.
• ECG is useful depending on clinical examination and symptoms

Cost effectiveness and practical implications
J Pediatr 2002;141:504-11


Is echocardiogram necessary

Is Echocardiogram necessary

Indications for referral
• Innocent murmur – Absence of abnormal physical findings (except for
murmur) – Negative review of symptoms – Negative history – Murmur with seven features of innocent murmur
• Not appropriate for newborns and infants younger
than 1 year as there is higher rate of asymptomatic structural heart disease.

Neonatal Heart Murmurs
• Incidence 23.81 per 1000 live birth • Incidence of CHD 10.75 per 1000 live births
• Bansal M, Jain H. Cardiac Murmur in Neonates. Indian Pediatrics 2005; 42:397-398

Neonatal heart murmurs
• 1 percent of newborns have a heart murmur • 31 to 86 percent of these infants have structural
heart disease • Referral to a pediatric cardiologist is recommended • Sensitivity for detection of a pathologic heart murmur
in newborns ranges from 80.5 to 94.9% among pediatric cardiologists, with specificity ranging from 25 to 92 percent

Key recommendations
Clinical recommendation Evidence Rating
Structural heart disease is more likely when the murmur is holosystolic, diastolic, grade 3 or higher, or associated with a systolic click; when it increases in intensity with standing; or when it has a harsh quality.
C
Chest radiography and electrocardiography rarely assist in the diagnosis of heart murmurs in children.
B
Family physicians should consider referral to a pediatric cardiologist for newborns with a heart murmur, even if the child is asymptomatic, because of the higher prevalence of structural heart lesions in this population.
B
Am Fam Physician. 2011;84(7):793-800

References
1. Evaluation of heart murmurs in children: Cost-effectiveness and practical implications. Yi, Michael S. et al. The Journal of Pediatrics , Volume 141 , Issue 4 , 504 - 511
2. Phoon, Colin. (2001). Estimation of pressure gradients by auscultation: An innovative and accurate physical examination technique. American heart journal. 141. 500-6. 10.1067
3. Frank JE, Jacobe KM. Evaluation and Management of Heart Murmurs in Children. Am Fam Physician. 2011;84(7):793-800
4. Bansal M, Jain H. Cardiac Murmur in Neonates. Indian Pediatrics 2005; 42:397-398 5. Van Oort A, Le Blanc-Botden M, De Boo T, Van Der Werf T, Rohmer J, Daniëls O. The vibratory
innocent heart murmur in schoolchildren: difference in auscultatory findings between school medical officers and a pediatric cardiologist.Pediatr Cardiol. 1994 Nov-Dec; 15(6):282-7.
6. Begic Z, Dinarevic SM, Pesto S, Begic E, Dobraca A, Masic I. Evaluation of Diagnostic Methods in the Differentiation of Heart Murmurs in Children. Acta Informatica Medica. 2016;24(2):94-98. doi:10.5455/aim.2016.24.94-98.
7. Advani, N., Menahem, S., & Wilkinson, J. (2000). The diagnosis of innocent murmurs in childhood. Cardiology in the Young, 10(4), 340-342. doi:10.1017/S104795110000963X
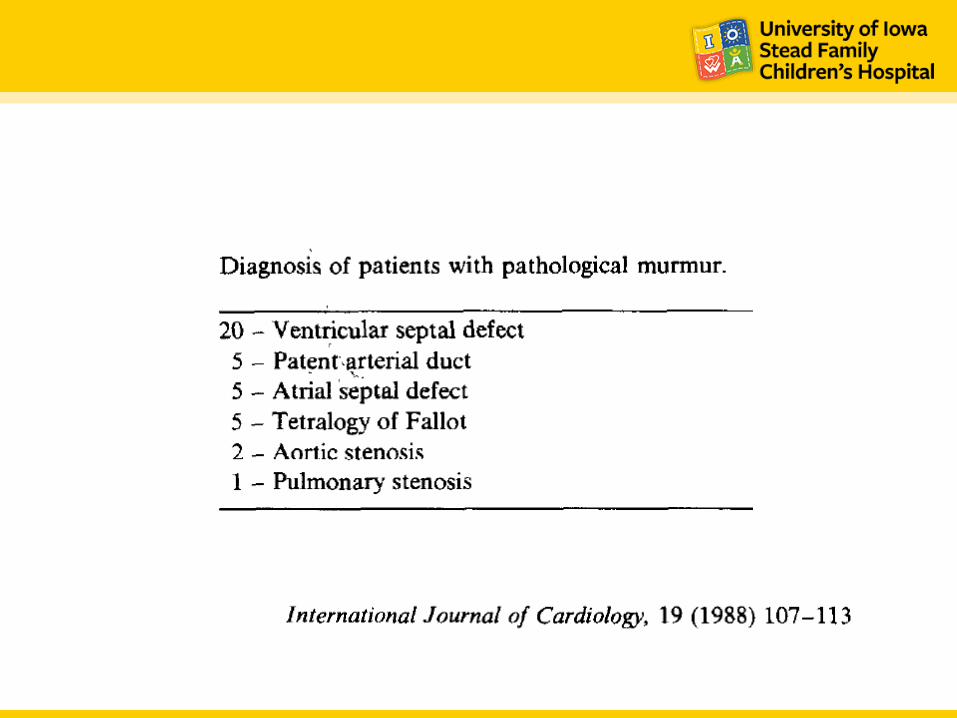
8. Geva, T, Hegash, J, Frand, M. Reappraisal of the approach to the child with heart murmur; is echocardiography mandatory? Int J Cardiol 1988. 107–113