Embed Size (px)
Citation preview
Ricardo A. Caicedo, MDPediatric Gastroenterology
University of Florida
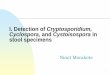
Diarrhea Increase in frequency and water content of stools
MECHANISM Examples
MALABSORPTION Celiac disease, Rotavirus
OSMOTIC Lactase deficiency
SECRETORY Cholera, C. difficile toxin
HYPERMOTILITY IBS
INFLAMMATORY IBD, Shigella
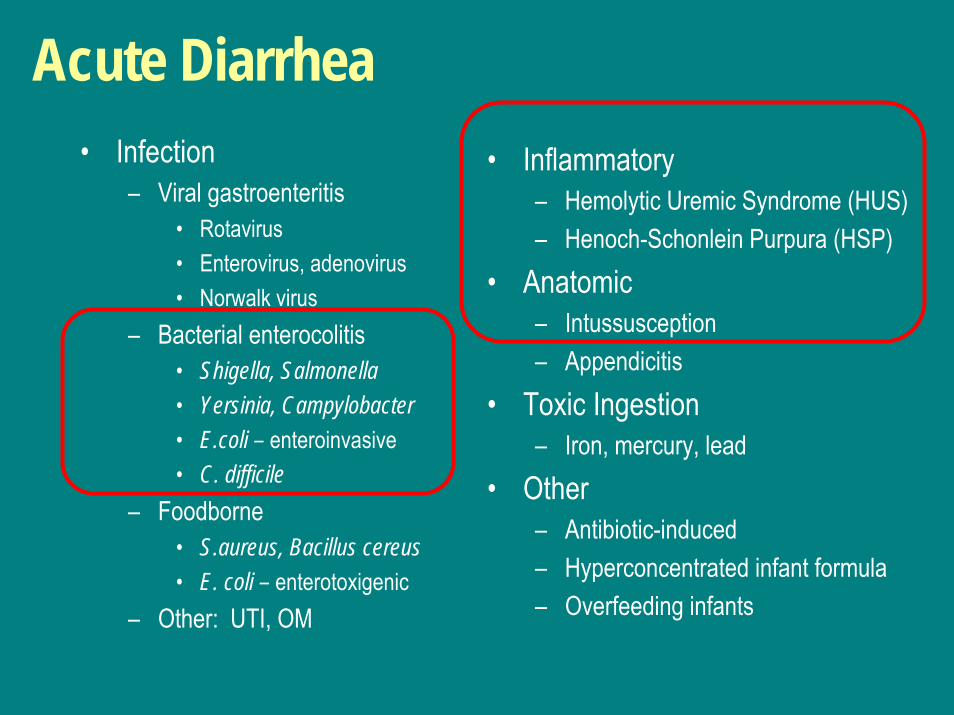
Acute Diarrhea• Infection
– Viral gastroenteritis• Rotavirus• Enterovirus, adenovirus• Norwalk virus
– Bacterial enterocolitis• Shigella, Salmonella• Yersinia, Campylobacter• E.coli – enteroinvasive• C. difficile
– Foodborne• S.aureus, Bacillus cereus• E. coli – enterotoxigenic
– Other: UTI, OM
• Inflammatory– Hemolytic Uremic Syndrome (HUS)– Henoch-Schonlein Purpura (HSP)
• Anatomic– Intussusception– Appendicitis
• Toxic Ingestion– Iron, mercury, lead
• Other– Antibiotic-induced– Hyperconcentrated infant formula– Overfeeding infants
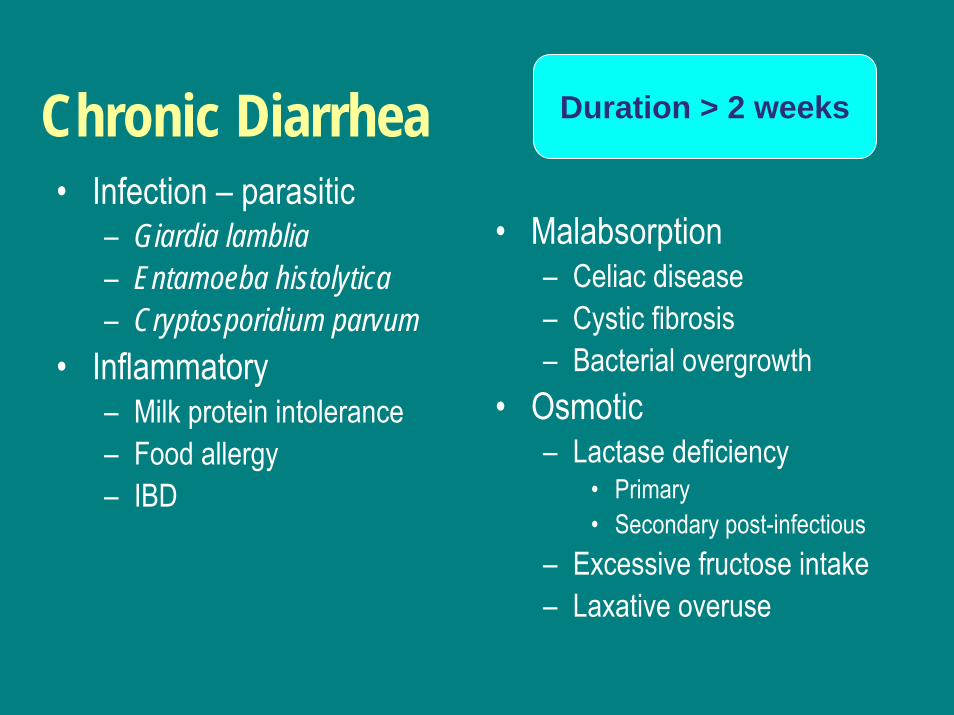
Duration > 2 weeksChronic Diarrhea• Infection – parasitic
– Giardia lamblia– Entamoeba histolytica– Cryptosporidium parvum
• Inflammatory– Milk protein intolerance– Food allergy– IBD
• Malabsorption– Celiac disease– Cystic fibrosis– Bacterial overgrowth
• Osmotic– Lactase deficiency
• Primary• Secondary post-infectious
– Excessive fructose intake– Laxative overuse
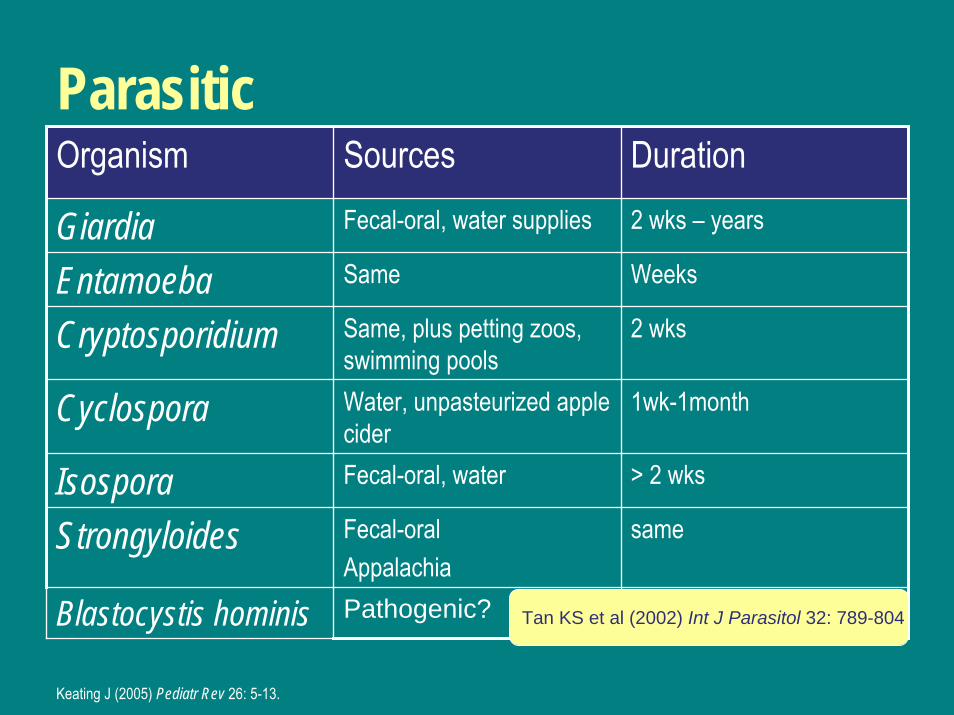
Parasitic Organism Sources Duration
Giardia Fecal-oral, water supplies 2 wks – years
Entamoeba Same Weeks
Cryptosporidium Same, plus petting zoos, swimming pools
2 wks
Cyclospora Water, unpasteurized apple cider
1wk-1month
Isospora Fecal-oral, water > 2 wks
Strongyloides Fecal-oralAppalachia
same
Blastocystis hominis Pathogenic? Tan KS et al (2002) Int J Parasitol 32: 789-804
Keating J (2005) Pediatr Rev 26: 5-13.
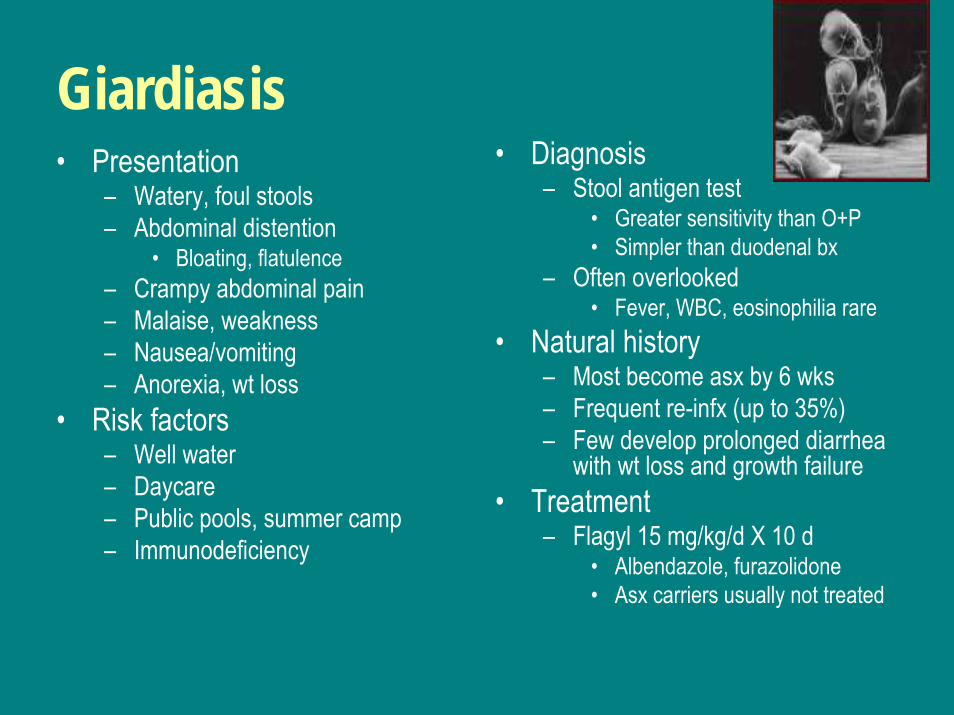
Giardiasis• Diagnosis
– Stool antigen test• Greater sensitivity than O+P • Simpler than duodenal bx
– Often overlooked• Fever, WBC, eosinophilia rare
• Natural history– Most become asx by 6 wks– Frequent re-infx (up to 35%)– Few develop prolonged diarrhea
with wt loss and growth failure• Treatment
– Flagyl 15 mg/kg/d X 10 d• Albendazole, furazolidone• Asx carriers usually not treated
• Presentation– Watery, foul stools– Abdominal distention
• Bloating, flatulence– Crampy abdominal pain– Malaise, weakness– Nausea/vomiting– Anorexia, wt loss
• Risk factors– Well water– Daycare– Public pools, summer camp– Immunodeficiency
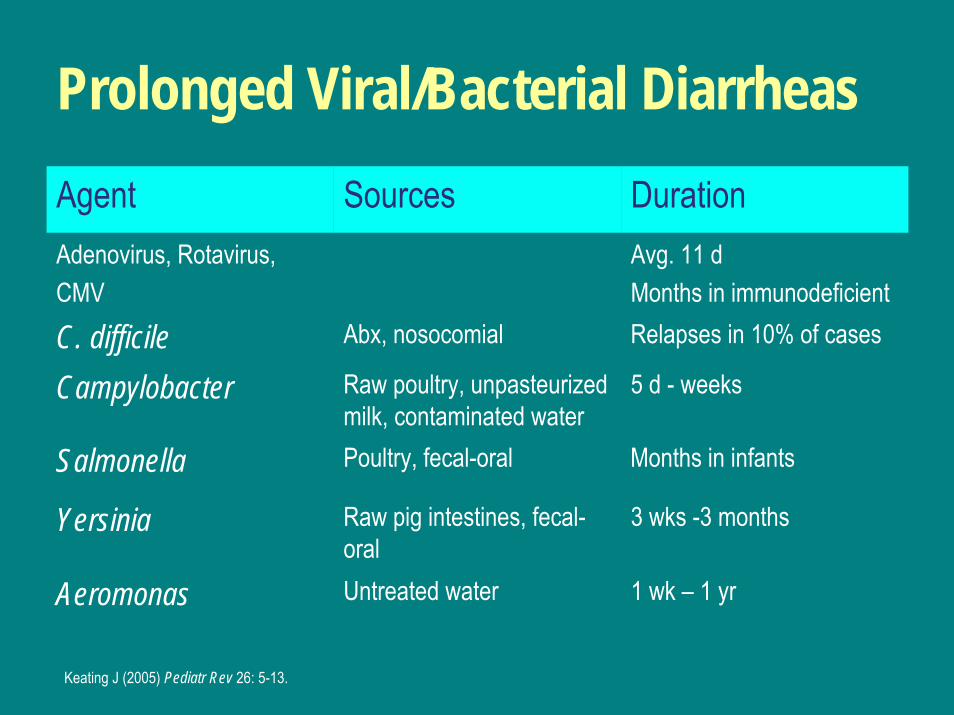
Prolonged Viral/Bacterial DiarrheasAgent Sources DurationAdenovirus, Rotavirus,CMV
Avg. 11 dMonths in immunodeficient
C. difficile Abx, nosocomial Relapses in 10% of cases
Campylobacter Raw poultry, unpasteurizedmilk, contaminated water
5 d - weeks
Salmonella Poultry, fecal-oral Months in infants
Yersinia Raw pig intestines, fecal-oral
3 wks -3 months
Aeromonas Untreated water 1 wk – 1 yr
Keating J (2005) Pediatr Rev 26: 5-13.
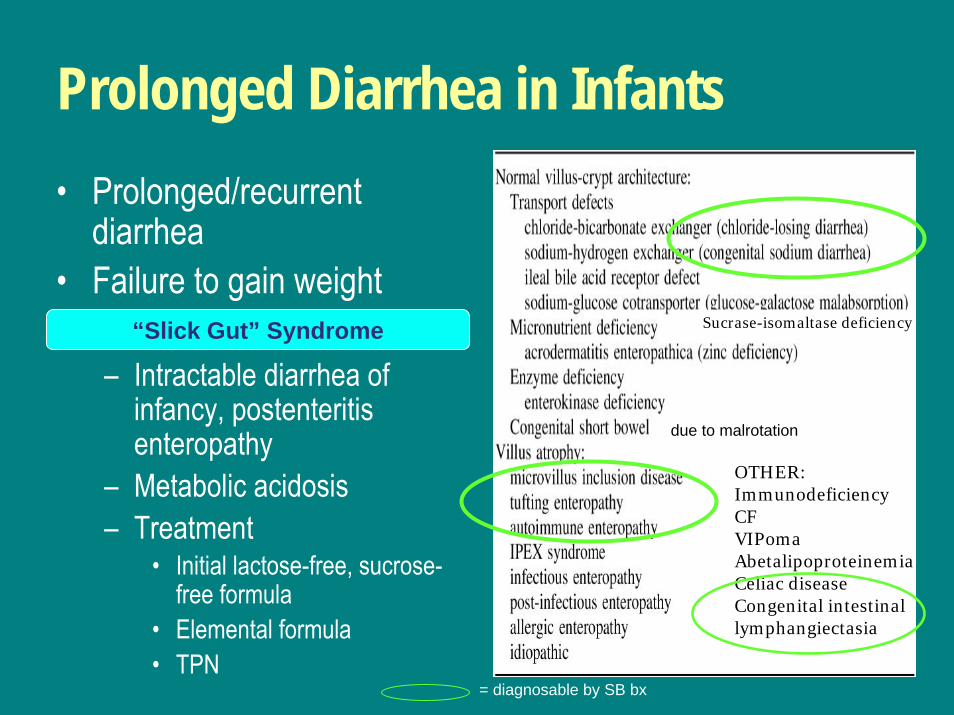
Prolonged Diarrhea in Infants• Prolonged/recurrent
diarrhea• Failure to gain weight
– Intractable diarrhea of infancy, postenteritisenteropathy
– Metabolic acidosis– Treatment
• Initial lactose-free, sucrose-free formula
• Elemental formula• TPN
“Slick Gut” Syndrome
OTHER:ImmunodeficiencyCFVIPomaAbetalipoproteinemiaCeliac diseaseCongenital intestinal lymphangiectasia
due to malrotation
Sucrase-isomaltase deficiency
= diagnosable by SB bx
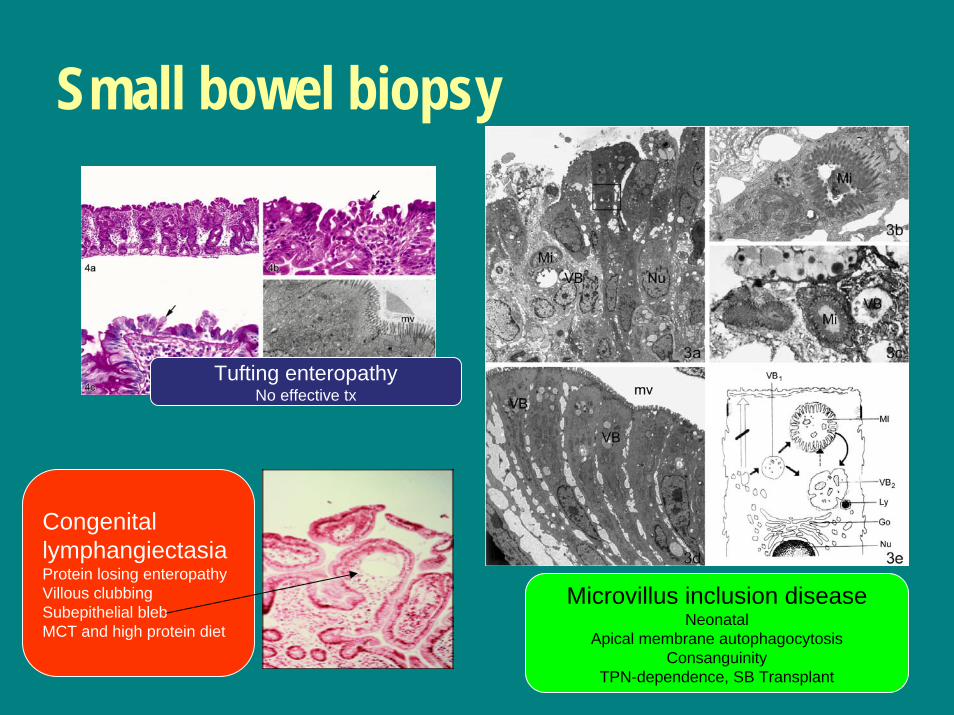
Small bowel biopsy
Microvillus inclusion diseaseNeonatal
Apical membrane autophagocytosisConsanguinity
TPN-dependence, SB Transplant
Tufting enteropathyNo effective tx
CongenitallymphangiectasiaProtein losing enteropathyVillous clubbingSubepithelial blebMCT and high protein diet
Toddler’s diarrhea• Chronic nonspecific diarrhea of childhood• Symptoms
– Explosive loose stools– Contain food particles– Frequent stools, decline as day goes on
• Management– Verify normal growth and absence of red flags
• Blood in stool, persistent fever, anemia– Exclude celiac disease (tTG) and Giardia– Trial of dietary modification
• Restrict fructose and/or lactose
Diarrhea in older children• OSMOTIC
– Lactase deficiency• Primary
– African, Asian, Hispanic • Secondary
– Postenteritis– Laxative overuse/Poisoning
• INFLAMMATORY– Infectious– IBD
• FUNCTIONAL/hypermotility– IBS– CNSD (Toddler’s)
• MALABSORPTIVE– Celiac disease– CF– Pancreatic insufficiency– Chronic cholestasis– Bacterial overgrowth– Zinc deficiency– Intestinal lymphangiectasia
• Cong. Heart Dz (Fontan physiol)• Tumor or radiation
• SECRETORY
steatorrhea
Secretory diarrheas• Voluminous watery• Persists despite bowel rest• Massive efflux of fluid/salt• Stool electrolyte content
similar to serum• WDHA syndrome
– Watery diarrhea– Hypokalemia– Alkalosis
• DIFFERENTIAL DX– Cholera– C. difficile– Severe mucosal injury– Short bowel syndrome– Secretory tumors
• Carcinoid• Gastrinoma• Ganglioneuroma• Neuroblastoma• Pheochromocytoma• VIPoma
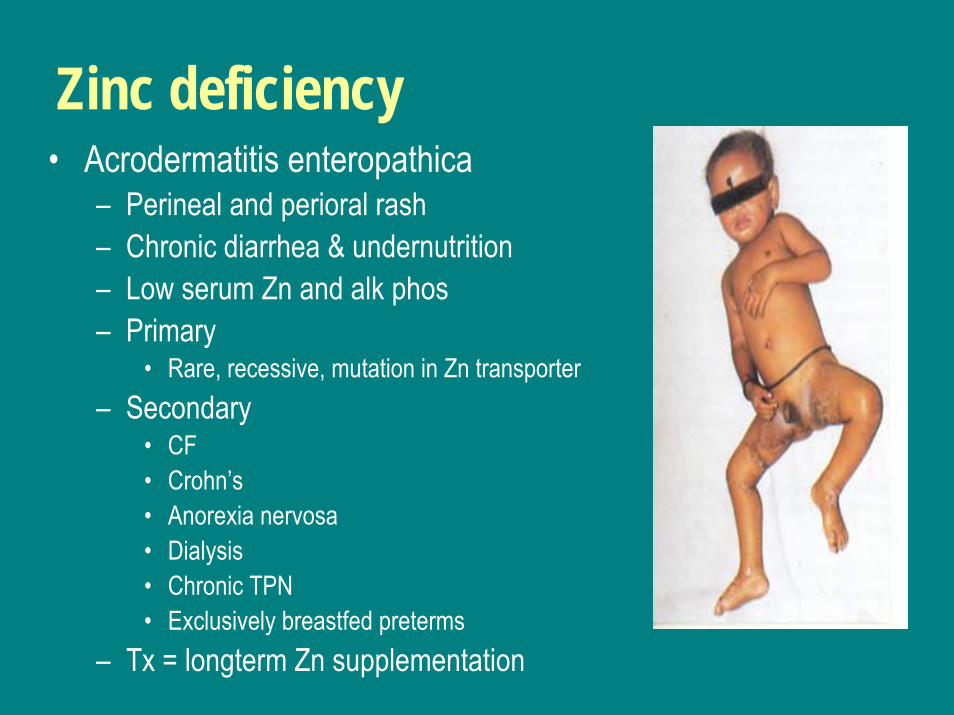
Zinc deficiency• Acrodermatitis enteropathica
– Perineal and perioral rash– Chronic diarrhea & undernutrition– Low serum Zn and alk phos– Primary
• Rare, recessive, mutation in Zn transporter– Secondary
• CF• Crohn’s• Anorexia nervosa• Dialysis• Chronic TPN• Exclusively breastfed preterms
– Tx = longterm Zn supplementation
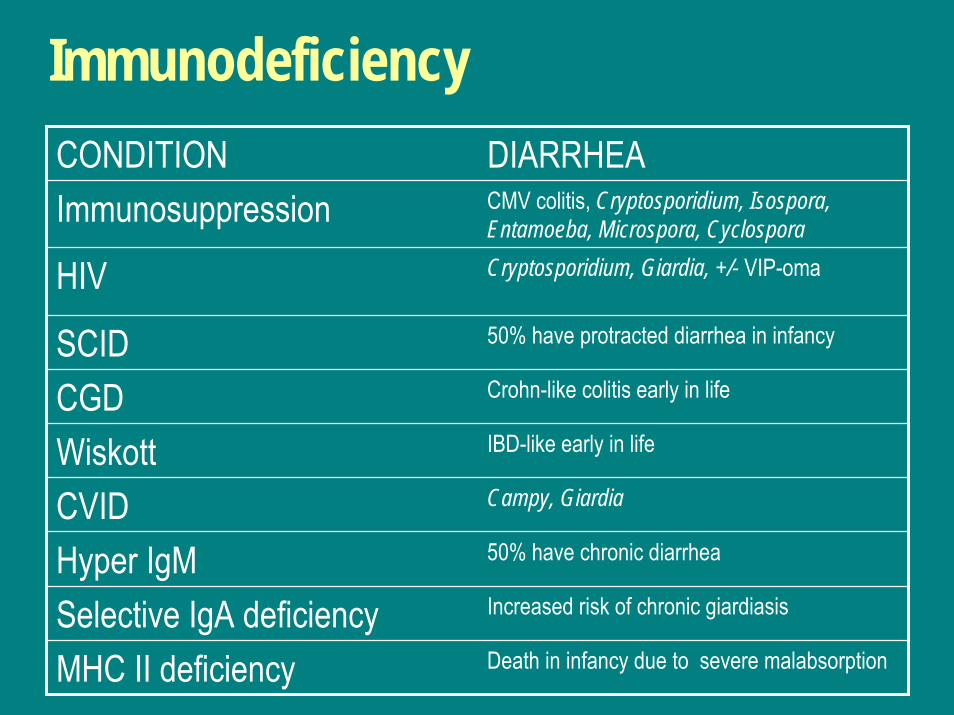
ImmunodeficiencyCONDITION DIARRHEAImmunosuppression CMV colitis, Cryptosporidium, Isospora,
Entamoeba, Microspora, Cyclospora
HIV Cryptosporidium, Giardia, +/- VIP-oma
SCID 50% have protracted diarrhea in infancy
CGD Crohn-like colitis early in life
Wiskott IBD-like early in life
CVID Campy, Giardia
Hyper IgM 50% have chronic diarrhea
Selective IgA deficiency Increased risk of chronic giardiasis
MHC II deficiency Death in infancy due to severe malabsorption
Approach• Impact of diarrhea
– How is the infant/child growing?– How is symptom affecting child’s life?
• Mechanism of diarrhea– Description of stool
• Blood? Oily? Food particles?• Frequency
– Diet and exposures• Complete physical exam
– Attention to skin, LN, spleen• Screening and diagnostic tests
Screening tests• BLOOD
– Electrolytes– Total protein/albumin– Liver tests– CBC– ESR– Celiac serology (tTG)– Vitamin levels
• B12, FA, Fe• A, D, E
• STOOL– Guaiac– pH and reducing substances– Spot fat stain– Gram stain/Culture– Giardia Ag– O+P– C. diff toxin– Osmolarity– Electrolytes
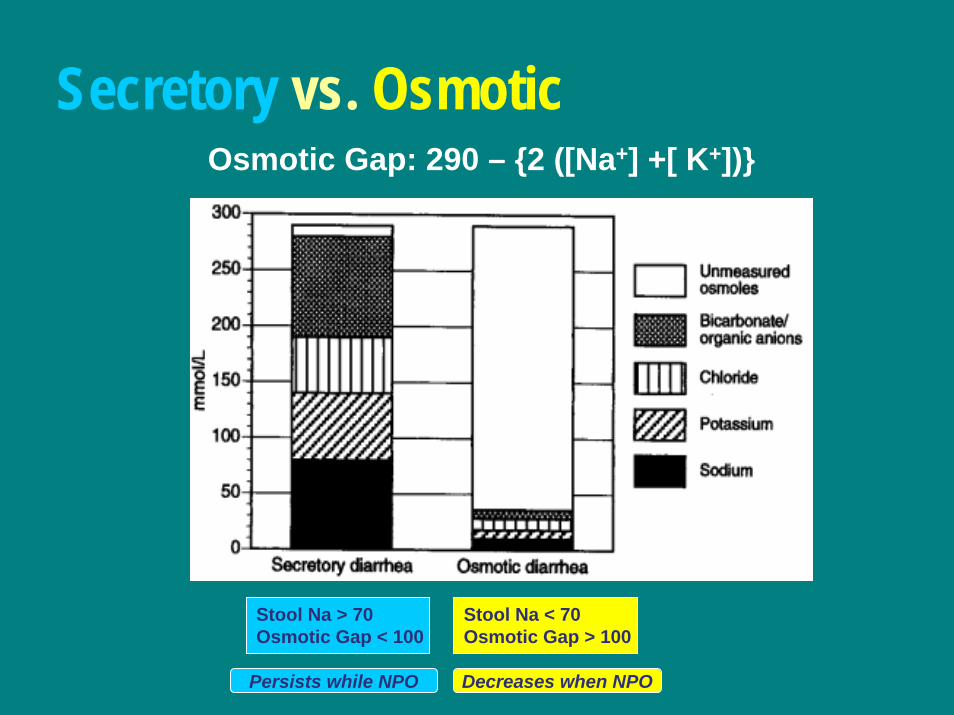
Secretory vs. OsmoticOsmotic Gap: 290 – {2 ([Na+] +[ K+])}
Stool Na > 70Osmotic Gap < 100
Stool Na < 70Osmotic Gap > 100
Persists while NPO Decreases when NPO
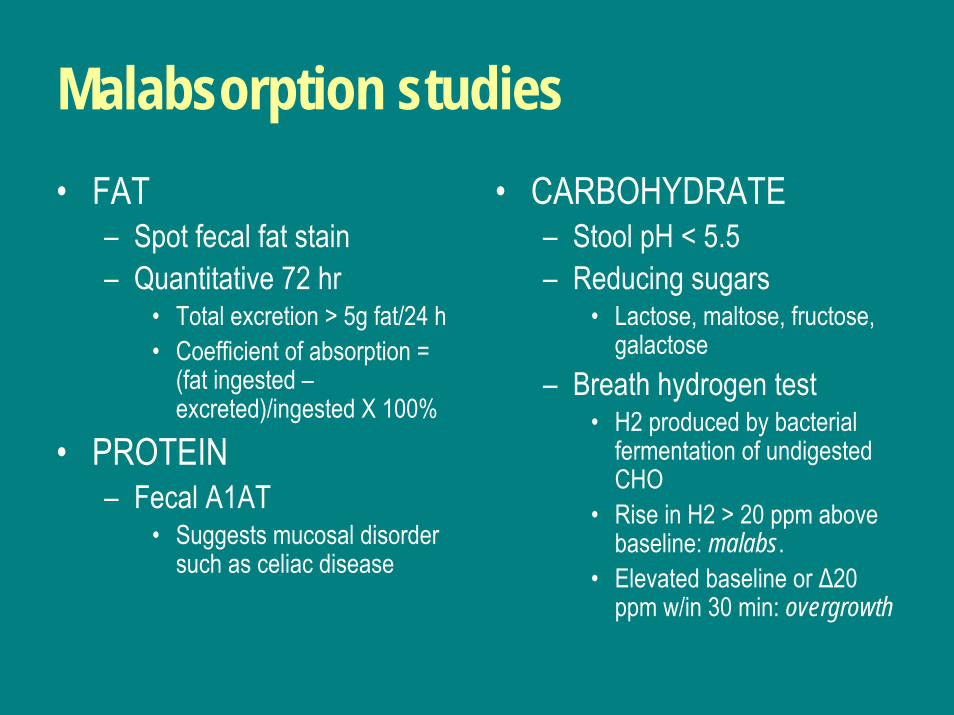
Malabsorption studies• FAT
– Spot fecal fat stain– Quantitative 72 hr
• Total excretion > 5g fat/24 h• Coefficient of absorption =
(fat ingested –excreted)/ingested X 100%
• PROTEIN– Fecal A1AT
• Suggests mucosal disorder such as celiac disease
• CARBOHYDRATE– Stool pH < 5.5– Reducing sugars
• Lactose, maltose, fructose, galactose
– Breath hydrogen test• H2 produced by bacterial
fermentation of undigested CHO
• Rise in H2 > 20 ppm above baseline: malabs.
• Elevated baseline or ∆20 ppm w/in 30 min: overgrowth
Barney Beagle
Thank You!