Embed Size (px)
Citation preview

DOI: 10.1542/pir.15-8-3111994;15;311Pediatrics in Review
Stephen ShustermanPediatric Dental Update
http://pedsinreview.aappublications.org/content/15/8/311the World Wide Web at:
The online version of this article, along with updated information and services, is located on
Print ISSN: 0191-9601. Village, Illinois, 60007. Copyright © 1994 by the American Academy of Pediatrics. All rights reserved.trademarked by the American Academy of Pediatrics, 141 Northwest Point Boulevard, Elk Grove
andpublication, it has been published continuously since 1979. Pediatrics in Review is owned, published, Pediatrics in Review is the official journal of the American Academy of Pediatrics. A monthly
at UNIV OF CHICAGO on April 26, 2013http://pedsinreview.aappublications.org/Downloaded from

FOCUS QUESTIONS
1. What are the major abnormalitiesof formation and eruption of theprimary and secondary dentitlon?
2. What are the most Important con-sequences of untreated dental car-ies?
3. What are the most cost-effectiveand acceptable approaches to car-ies prevention?
4. What Is the best approach to pre-vention, early recognition, andtimely treatment of gingivitis andperiodontitis?
5. What are the principles of manag-Ing oral trauma?
#{149}Dentist.in.Chief, Children’s Hospita4
Boston, MA.
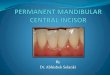
FIGURE 1. A newborn infant of several days
of age displays neonatal teeth and severelyulcerated dorsum of tongue.
Pediatrics in Review VoL 15 No. 8 August 1994 311
Pediatric Dental UpdateStephen Shusterman, DMD*
ARTICLE
IntroductionPediatricians are in an ideal positionto influence the oral health of theiryoung patients, from the first pre-natal interview with prospective par-ents and the initial newbornexamination through the duration oftheir general pediatric care. Teeth be-gin calcification between 14 and 16
weeks of embryonic life, and most ofthe crowns of the primary teeth, aswell as the occlusal edges of somepermanent teeth, are calcified bybirth. Early plaque removal from
gum pads and erupting teeth, the useof fluoride as a dietary supplement innonfluonidated communities, andtimely visits to the dentist all willhelp to assure a caries-free dentitionand healthy oral environment for thechild of the 21st century.
Dentistry has emerged from itsposition as a little understood andpoorly tolerated sideline of the itiner-ant surgeon to its status of partner insupporting total bodily health. Suchgains as local anesthesia and themeans to administer it painlessly,high-speed instrumentation to remove
caries comfortably (albeit mechani-cally), bonded resins (eg, pit and fis-sure sealants, composite resinrestorative materials) to prevent car-ies and esthetically restore broken ordeformed teeth, and implants to re-place missing teeth and to restorefunction and appearance have high-
lighted its recent evolution. Dentistryin the 1990s is confident of its ability
to control oral disease, but remainsdependent on pediatricians and fam-ily practitioners for support in influ-encing patients and their parentsabout the systemic importance of ahealthy and functional dentofacialcomplex.
Developmental and EruptionAnomaliesAt birth, infants usually are clinicallyedentubous, but within the jaws arethe immature forms of most of theprimary and many of the secondaryteeth. Several anomalies should berecognized in the newborn mouth. Inexamining a baby, the pediatricianmay find clear or bluish fluid-filledsacs, sometimes bilaterally or quadri-laterally, on the gum pads. These
dental bamina cysts generally are notpainful, are not surrounded by cry-thematous tissues, do not interferewith feeding, and disappear without
treatment after several weeks. Yel-bowish-white, slightly raised cysts onthe alveolar ridges are referred to asBohn nodules and those near themidpalatal raphe at the junction ofthe hard and soft palates as Epstein
pearls. They represent islands of epi-thebial cells left over from the embiy-onic formation of the dental bamina
or palatal fusion. These cysts arecommon, will disappear, and requireno treatment.
Teeth present at or shortly afterbirth are referred to as natal teeth. Ina 1984 study, Kates et al found natalteeth in 13 of 18 155 infants sur-veyed (1:1400), all in the mandibularincisor area. Natal teeth generally arepoorly formed, have thin hypoplasticenamel, and sometimes are at the endof a stalk of granubomatouslike un-calcified tissue, which is friable andextremely mobile. If natal teeth arepresent in the lower anterior gum,they may irritate and ulcerate thedorsum of the tongue, or they mayinterfere with nursing by irritating themother’s breast or disrupting suck-ing. If natal teeth are causing signifi-cant ulceration or if there is a cleardanger of aspiration, the teeth should
be removed (Figure 1). However,they generally represent primary teeththat may have formed superficiallyand erupted early and, therefore, willnot be replaced. Kates et al notedthat 95% of the natal teeth in theirsurvey were normal primary incisorsand only 5% were supernumerary(extra) teeth. If removed, space maybe lost for permanent successors, andyears later orthodontic treatment maybe necessary. Natal teeth are particu-larly common in children who have acleft lip and palate, where the patho-genesis of the anomaly may disruptthe dental lamina, resulting in super-ficial placement of primary toothbuds.
Primary teeth begin eruption at ap-proximately 6 months of age, but therange may vary between 3 and 16months. At this age, a child who hasno teeth but is developing normallyand meeting his or her other mile-stones should be examined by a den-tist. Dental radiographs are notnecessary unless there is reason tobelieve that there is a pathologicprocess and the child can be heldmotionless so that the film will be di-agnostic. Mandibular teeth generallyerupt first, and the sequence for theprimary teeth is the central incisor,lateral incisor, first molar, canine,and second molar.
All primary teeth usually haveerupted by age 3 years, and theprocess of root resorption then beginsfor their replacement by secondary(permanent) teeth. The first visit forroutine dental treatment should be at
this time, if the child has not beenseen earlier for preventive care or
at UNIV OF CHICAGO on April 26, 2013http://pedsinreview.aappublications.org/Downloaded from

Q
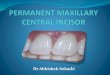
FIGURE 2. A patient who has ectoderrnal
dysplasia shows oligodontia and conically
shaped teeth.
I
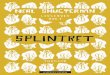
FIGURE 3. A 16-month-old child has early
nursing-type caries characterized by carioussmooth palatal and facial carious surfaces of
the maxil/aty incisors.
-�
312 Pediatrics in Review VoL 15 No. 8 August 1994
MOUTh AND TEETHDsntal Updats
management of traumatic injury tothe teeth. It is important to realizethat the space occupied by the pni-mary dentition (20 teeth), as mea-sured from the distal surface of onesecond molar around the arch to thedistal surface of the other second pni-mary molar, will be the space avail-abbe for the 20 succedaneouspermanent teeth. The face will growdownward and forward from the cna-nial base, but growth in the mouthwill occur behind the primary denti-tion to accommodate the 12 acces-sional teeth (permanent first, second,and third molars). Statistically, theperimeter of the primary dental archwill become slightly smaller due to
anterior vectors of force and medial
drift during tooth eruption. Any addi-tional space lost as a result of cariesor crowding may create the necessityfor orthodontic realignment.
At or about 6 years of age, thefirst permanent molars erupt distal tothe primary dentition, and the perma-nent incisors replace the primary in-
cisons. From that point until theexfoliation of the last primary teeth,
between 12 and 14 years of age, thedentition is referred to as “mixed”and after that as the “permanent”
dentition. Third molars, “wisdomteeth,” which may erupt in late ado-lescence, are blamed for many dentalproblems, including crowding andtemporomandibular joint pain. Many
people do not have adequate spacemedial to the mandibular namus or in
the retromolar pad area of the max-illa to accommodate these teeth. Thethird molar may erupt partially (par-tial impaction) or remain totally im-
pacted (unerupted). Removal may benecessary due to penicononal infectionon other degenerative changes, butusually not before late adolescence.Early attempts at third molar removal
in younger children are complicated,and morbidity is high.
Several conditions may alter on in-terfere with the eruption of teeth. Insome cases, there may be agenesis ofindividual teeth, commonly maxillarypermanent lateral incisors or mandi-bular second premolars, or multipleteeth may be missing (oligodontia).Oligodontia is found in Down syn-drome, incontinentia pigmenti, andectodermal dysplasia (Figure 2). Inthis latter condition, the teeth that arepresent are conically shaped, dys-
morphic, and may have short conicalroots. Missing primary teeth mayneed to be replaced prosthetically for
esthetic or functional reasons. Extra(supernumerary) teeth commonly arefound in the maxillary anterior mid-line and may interfere with eruptionof permanent incisors. Anterior andposterior multiple supernumerary
teeth are found in cleidocranial dy-sostosis and Gardner syndrome. Su-pernumerary teeth that interfere witheruption must be removed. If theyare not interfering, they may be leftuntil the adjacent permanent toothroots have completed formation, atwhich time they are removed sun-gically; in rare cases, they are left inplace. In some cases, supernumeraryteeth erupt and may be removedeasily.
Finally, systemic disease on endo-cnine malfunction may accelerate orretard eruption. Endocrine distur-bances of growth, such as hypothy-roidism or hypopituitanism, usuallyare reflected in a delayed eruption ofteeth, but endocrine disorders such as
functioning ovarian tumors maycause an acceleration in dental devel-opment. In both cases, teeth are nor-mal in size and morphology. Severemetabolic disturbances, such as ne-phrotic syndrome, which have theironset during the formation of perma-nent teeth, may result in a linear pat-tern of hypoplasia that affects thedentition in those areas forming dur-ing the acute metabolic disturbance.This phenomenon is similar to thestaining that occurs in teeth undergo-ing calcification during the adminis-tration of tetracycline drugs, whenthe drug is incorporated into the de-veloping tooth structure. Extrinsicstains such as iron (gray or green) orpostantibiotic stain (orange or brown)
usually can be removed; intrinsicstaining is permanent.
Dental Caries andPeriodontal Disease-Infectious Processes
According to a 1989 report by theNational Institute of Dental Research,
49.9% of children ages 5 to 7 werecaries-free compared with 36.6% in a1979 to 1980 survey. The trendshown in earlier studies continues
downward, with an increase of al-most 4 million caries-free childrensince 1980. However, the remaining
50% of children did have some can-ies, with almost 80% of 15- to 17-
year-olds having at least one de-cayed, missing, or filled tooth sun-face. Early loss of tooth structure not
only results in loss of space throughdrifting and tipping, but may resultin masticatory and nutritional prob-lems; psychological problems causedby the premature loss on disfigure-ment of teeth; pain, swelling, and in-fection; and speech problems. Inaddition, teeth that are aligned poorly
or crowded are more at risk for pen-odontal disease, another infectiousprocess that may have roots in child-hood.
NURSING-TYPE CARIES
One of the earliest manifestations ofa significant caries process is “nurs-ing-type caries” (Figure 3). Thisclassic pattern of caries begins on thesmooth surfaces of the maxillary in-cisors (facial or palatal surfaces),spreads posteriorly to involve thesmooth (cheek) surfaces of the maxil-lary primary molars, and then infeni-only and posteriorly to involve thesmooth (cheek) surfaces of the man-
at UNIV OF CHICAGO on April 26, 2013http://pedsinreview.aappublications.org/Downloaded from

FIGURE 4. Facial cellulitis (A) resulting from carious teeth (B).
Pediatrics in Review VoL 15 No. 8 August 1994 313
dibular primary molars. The mandi-bular incisors and canines becomeinvolved only after the process hasbeen long-standing, and the classicdescription is of gross caries involv-ing all teeth except the six mandibu-lan anterior teeth.
This nursing pattern of caries re-sults from prolonged and excessive
nursing, with nutrient materials suchas milk or juice being present in themouth frequently and when the child
falls asleep while nursing. It hasbeen theorized that the tongue comesupward and forward during nursing,
protecting the lower anterior teeth,which are also bathed in saliva fromthe sublingual salivary glands; then,during sleep, the salivary flow andswallowing frequency are decreased.It is important to note that I have Ia-beled this phenomenon “nursing-
type” rather than “baby bottle” can-ies to underscore the fact that a simi-bar caries pattern may result not onlyfrom bottle feeding, but also fromexcessive breastfeeding. The devel-opment of nursing-type caries frombreastfeeding is less common andmay take longer. The etiology is sim-
ilan; it is related to prolonged nursingon to the child sleeping with his orhen mother and nursing frequentlythrough the night. Because of thevery young ages of these patients, re-stonative treatment usually is possibleonly under general anesthesia andmay require the use of prefabricatedstainless steel crowns on the molarsas well as extraction of hopelessly in-volved teeth. Pediatric dentists arenot concerned by long-term use of
the bottle on bneastfeeding, but woulddiscourage “casual or frequentsnacking” during waking hours or
sleeping with a nursing bottle ormother.
DENTAL CARIES
In the more common caries process,decay begins in the deep occlusal pitsand fissures of the molars on inter-proximally, when posterior teeth con-
tact, just below the contact area. Theprocess is marked by an initial decal-cification on white spot, which, if leftuntreated, erodes as the cariesspreads through the enamel to thedentin. Unlike enamel, the dentin istubular in structure, enclosing an or-ganic projection from the odontoblast
that lines the pulpal chamber. Inva-sion of the dentin may provide thefirst sensitivity or pain, but it is notunusual for children to have exten-sive caries and never to complain ofpain.
Once caries has spread from thedentin to the pulp, which is corn-posed of nerve, blood supply, and fi-brous connective tissue, the classicinflammatory process spreads. Be-
cause this is a small, confined space,fluid collects rapidly, necrosis oc-curs, and pain may result. As infec-tion spreads into the peniradicular
space, the tooth becomes mobile, andpus may perforate the thin corticalplate of bone, resulting in a drainingfistula or “parulis.” In the mandible,if infection spreads from a molar tothe fascial spaces below the insertionof the rnylohyoid muscle, swellingmay spread below the tongue andacross the floor of the mouth, even-tually elevating the tongue and caus-ing respiratory embarrassment. Dueto the anatomic position of primarymolars, this condition, “Ludwig an-gina,” usually is not seen in childrenyounger than 7 years. In the rnaxilla,
infection may spread upward andbackward, involving the space belowthe infraonbital ridge, eventually in-volving the penionbital and supraorbi-tal spaces and closing the eye (Figure
4). Infection of a maxillary toothspreading in this manner may result
MOUTH AND TEEThDental Update
in sinus infection, cavernous sinusthrombosis, and brain abscess.
The antibiotic of choice in odonto-genic infection is penicillin V (250 to500 mg p0 every 6 hours, 50 mg/kgpen day); erythromycin (200 to 400mg p0 every 6 hours, 40 mg/kg perday) may be used for patients whoare allergic to penicillin. Respiratory
embarrassment on cavernous sinus in-fection is rare in children, but dehy-dration and sepsis may occur more
frequently. Because these complica-tions develop very rapidly, childrenwho have odontogenic infection andobvious facial cellulitis should be ad-mitted to the hospital for intravenousantibiotic coverage and close moni-toring when signs of toxicity and in-creasing dehydration are noted.
GINGIVITIS AND PERIODONTITIS
Gingivitis, an early and reversibleform of periodontal disease, is morecommon than previously believed inchildren and may precede the moreprogressive and irreversible form ofgum disease seen in later years. Gin-givitis refers to inflammation of that
portion of the gingiva (gum) just ad-jacent to the tooth, while peniodonti-tis refers to more widespread andextensive inflammation of the gingivaand supporting bone. The earliestform of gingivitis is associated withthe erupting tooth and disappears fol-
at UNIV OF CHICAGO on April 26, 2013http://pedsinreview.aappublications.org/Downloaded from

FIGURES. Tight attachment of the maxillarylabial frenum with wide diastema between
incisors. Surgery is not indicated prior to the
ernption of the permanent lateral and canine
teeth.
314 Pediatrics in Review VoL 15 No. 8 August 1994
F MOUTh AND TEETHDental Update
lowing emergence of the tooth. Justprior to eruption, it is not uncommon
to find a bluish, fluid-filled sac oven-lying the tooth (eruption “cyst”), anindication of minimal blood accumu-bation in the dental sac just prior toeruption. The eruption “cyst” or he-matoma (not a true cyst) usually dis-appears shortly after eruption andalmost never requires treatment.After eruption, however, the accumu-lation of “plaque” (a sticky combi-nation of food debris, bacteria, andsaliva) on the tooth surface just adja-cent to the gingiva may initiate amore serious form of gingivitis. In arecent survey conducted by the Na-
tional Institutes of Health, the mci-dence of mild-to-moderate gingivalinflammation was found to be 92%among schoolchildren; 3% of the
children surveyed had more seriousdisease that required treatment.
A more virulent form of peniodon-titis found in children is juvenilepeniodontitis (JP), which has beenshown to be responsible for rapidloss of supporting bone and deep in-flammation of the gingival tissues,particularly in the incisor and molarareas. Anaerobic microorganisms,primarily Actinobacillus actinomy-
cetem comitans and Capnocytophagasp have been associated with this dis-ease. Treatment includes surgical de-bnidement of the infected tissues,mechanical removal of calcified de-posits from the root surfaces of theaffected teeth, and tetracycline then-apy (these children usually are be-yond the tooth-forming ages whentetracyclines might result in perma-
nent dental staining). More com-monly, eruption of permanent teethin the mixed dentition stage may re-sult in crowding, rotation, and mal-position of some incisor teeth
(usually mandibular). Because ofmore labial placement in the alveolarbone and the difficulty in maintaining
adequate hygiene in these areas, gin-gival irritation is common and per-sistent and may result in severeinflammation, apical migration, andloss of bony support for these teeth.Treatment to prevent the loss of peri-odontal support is urgent and in-cludes removal of the local irritants,reduction of early crowding (perhapsby the selective removal of appropri-ate primary teeth), and replacementof lost gingival tissue by autologous
gingival grafting.Frenum attachments also have
been implicated in early mucogingi-val problems (Figure 5). Frena,which tightly bind the upper lip tothe gingiva labial to the maxillary in-cisors, on the tongue to the lingualtissues between the mandibular mci-sons, may exert intolerable tensionson these tissues. This causes gingivalstripping and loss of periodontal sup-port. In infancy, the labial, and lessfrequently the lingual, frenum are at-tached high on the alveolar ridges(gum pads), but they migrate apicallywith increasing age. Few actually ne-quire treatment. Frena should betreated surgically in infancy onlywhen the tongue is ve�y tightly at-tached to the gum and interferingwith feeding. The labial frenum usu-ally is not treated until early adoles-cence after the permanent canineteeth have erupted, when gingivaldegradation or a diastema betweenthe incisors is evident. Surgical man-agement in both cases must involvethe dissection and removal of themuscle insertion between the incisors(not a simple “snipping”) to relievethe gingival stripping and prevent re-currence. Frenectomy should be con-sidered carefully and performed onlywhen clearly indicated.
Preventive Dentistry
In recent years, dentistry has madegreat strides in preventing oral dis-
ease, but must do more to reachthose still affected by caries as wellas to focus on other areas such asperiodontal disease and malocclusion.Early infant oral health is a goal ofthe American Academy of PediatricDentistry, and although clear scien-
tific evidence to support “healthybaby” visits to the dentist may belacking, new parents must be madeaware of the rationale for good oral
hygiene, the possible effects of pro-longed on excessive nursing, the neg-ative effects of thumb and pacifiersucking, the use of mouthguards dun-ing athletic activities, and the bene-fits of appropriate fluoridesupplementation.
TEETh CLEANING
Infants collect plaque on their gumpads prior to the eruption of teeth
and will continue to accumulateplaque on the surfaces of newlyemergent teeth. Gingival irritationand caries are possible sequelae ofthis accumulation, and parents shouldbe counseled to clean the gum padsof their new infants, just as theybathe and clean other body parts. Aclean, moist washcloth or gauze pad,squeezed between the fingers and runtransversely across the gum pads toremove milk curd and food debris, isadequate for the predentate infant.
After the eruption of their child’sfirst teeth, parents gradually change
to a soft, multitufted toothbrush. Par-ents should assist their child inbrushing (through the first on secondgrade or until the child can demon-strate adequate dexterity and persist-ence) by standing or sitting behindhim on her and tipping the headbackward against them onto theirlaps. This stabilizes the head andprevents movement, gives access andviability, and allows cleaning of theteeth without trauma or gagging.Minimal quantities of dentifrice arenecessary, and it may be entirelyomitted at first. New parents alsoshould be counseled on factors in thediet that will contribute to dental car-ies, such as excessive nursing andadherent snack foods.
PACIFIERS AND ThUMB SUCKING
An important part of infant dentalcounseling is the issue of pacifierversus thumb sucking. Little evi-dence exists to support the use of theso-called orthodontic (Nuk�) pacifierover the conventional pacifier. Un-published data indicate more severemalocclusion as a result of dummy(pacifier) sucking. A recent paper inthe Journal of Pediatric Dentistry in-
at UNIV OF CHICAGO on April 26, 2013http://pedsinreview.aappublications.org/Downloaded from

�--�-�--- -�
FLUORIDECONTENT OFDRINKINGWATER (PPM)
BIRTh TO AGE2 Y (MG)
AGE2TO3 Y (MG)
AGE 3TO13 V (MG)
< 0.3* 0.25 0.50 1.00
0.3-0.7 0 025 0.50
� 0.7 Fluoride supplements not indicated
#{149}fnprocess of mod�flcation by the American Academy of Pediatrics to Ofor birth to age 6 ma,
0.25 mg for age6mo to3y, 0.50 mg for age3yto6y, and 1.0 mg for6yand older.
Mothfied from American Dental Association Council on Dental Therapeutics. Accepted DentalTherapeutics, ed 40. Chicago, Ill: The American Dental Association; 1984.
�rL�
‘��r %**IAI
FIGURE 6. Open bites as a result of
thumbsucking.
Pediatrics in Review VoL 15 No. 8 August 1994 315
MOUTh AND TEETHDsntal Update
dicated greaten overjet (protrusion)from the orthodontic pacifier and
more open-bite (anterior teeth not inocclusion) from the conventional pa-cifien. Certainly, the availability ofthe thumb and the sensation of dou-ble gratification (thumb and palate)help infants to satisfy their sucklinginstinct, but thumbsucking seems to
persist longer and is more difficult tostop. Pediatric dentists would preferneither habit, but when present, con-sider sucking habits relatively non-mal, even when they persist intoearly school grades. Open bites (Fig-une 6) and crossbites (malocclusionswhere teeth are reversed in their
usual labiolingual relationships) arenot unusual after prolonged suckinghabits, but are readily correctable, as
opposed to the lasting psychologicalimplications caused by deprivation or
forced cessation. If the sucking habitstops prior to the eruption of the per-manent incisors, the new teeth aremore likely to erupt into a normalposition. Gross maxillary protrusionon mandibular retnognathia probablyare rebated to genetic predispositionor growth imbalances rather than di-rectly to sucking habits.
FLUORIDE
Fluorides have been proven effectivein the reduction of dental caries. The
most economical method of fluorida-tion is through the public water sup-ply, and when that is not available,
the use of dietary supplementationaccording to the guidelines (Table)approved by the American Academyof Pediatrics. In recent years, ques-tions surrounding issues of safety inpublic water supplies have led to in-creased use of bottled water. In addi-tion, the benefits of breastfeedingover prepared or reconstituted infantformulas have raised concerns about“supplementing” infants and chil-dren who otherwise would be ingest-ing fluoridated water.
Fluorosis, a staining or mottling ofthe dental enamel due to excessive
fluoride ingestion, is being identifiedwith increasing frequency in newlyerupted teeth. Systemic fluorides areavailable from many sources, such astopical rinses and gels, dentifrices,and bottled waters containing naturalfluoride or bottled drinks prepared in
communities having fluoridated watersupplies. Several studies have identi-fled fluoridated dentifnices as asource of high doses of systemicfluorides, and the use of these tooth-pastes should be limited to verysmall amounts and carefully super-vised by parents. The appearance offluonotic enamel varies from a mini-mab pattern of white lacy lines toopaque white tooth surfaces with in-terspersed brown or deep yellowpatches (Figure 7). In many cases,children and their parents considerthese teeth unsightly and seek treat-ment alternatives to mask the disco-lored areas.
The apparent increase in the preva-lence of enamel opacities, in the ab-sence of dental caries activity, shouldinitiate a reconsideration of fluoride
dosages and availability for youngchildren. Dietary supplementation for
infants living in a fluoridated com-munity should be avoided, and dos-ages for supplemental fluoride incommunities having water fluoridelevels below 0.3 ppm may be reviseddownward to reduce the risk of fluo-rosis. The use of 0.25 mg of supple-mental fluoride from birth throughage 2 years, without regard toweight, is contrary to our usage ofmost other drugs and may be exces-sive for many. In addition, the sup-plementation of breastfeeding infantswhose mothers live in fluoridatedcommunities, based on the fact thatbreast milk may only contain traceamounts of fluoride, also may be un-necessary. Fluoride requirements atthese ages are very low (0.05 to0.07 mg/kg), and even the low fluo-ride concentration in breast milk maybe sufficient for early dental develop-ment. Later fluoride supplementationduring enamel maturation of the per-manent dentition (2 to 4 years) maybe more important. Pediatricians andpediatric dentists must emphasize theimportance of fluoride in the forma-tion of a healthy dentition, butshould be sensitive to its wide availa-bility and its relationship to the ap-parent increase in enamel opacities.
MOUTHGUARDS
Any discussion of prevention is notcomplete without mention of athleticmouthguards. When worn, mouth-guards may prevent injury to theteeth as well as concussion by cush-ioning the interface between upperand lower jaws. Mouthguards shouldbe considered mandatory equipmentin any organized sport where contactmight be anticipated, including foot-
at UNIV OF CHICAGO on April 26, 2013http://pedsinreview.aappublications.org/Downloaded from

FIGURE 7. Mild (A) and severe (B) fluorosis.
jk#{149}� LI
316 Pediatrics in Review VoL 15 No. 8 August 1994
MOUTH AND TEETHDental Update
ball, hockey, basketball, and la-
crosse. In children in the primary ormixed dentition phases, mouthguands
of the boilable or moldable type,which may be purchased off the shelfin sporting goods stores, are accepta-ble and economical and may be re-placed easily as the dentition
changes. It cannot be emphasizedenough that mouthguands are effec-tive only when they are worn; theirconstruction so as to allow rapidbreathing, shouted instructions, andcomfort is critical. Pediatric dentists
stand ready to advise and help par-ents and coaches, and pediatricianscan encourage the use of theseguards.
Trauma
Although many accidents to the den-tition are preventable, fractured, dis-placed, or avulsed teeth are commonin childhood, occurring at any timeafter the child first stands on walks.
Displaced teeth may be repositionedor may heal without treatment.Avulsed primary teeth should not bereimplanted because successful reat-tachment is very unlikely and thepermanent tooth will be at risk. Dis-
coloration of primary teeth as a se-quab to trauma is common, but
discoloration alone, in the absence ofother signs and symptoms of degen-eration, does not necessarily requiretreatment. Discoloration may be in-dicative of pulpal bleeding, but thetooth may remain asymptomatic andapparently vital until exfoliation.
Children who have traumatized teethshould be referred to the dentist forevaluation, and appropriate radio-graphs should be taken to identifyroot fractures, displacement, andproximity or changes in the perma-nent dentition.
Fractures of teeth are classified ac-
cording to the degree of involvementof tooth structure: enamel (class I);enamel and dentin (class II); enamel,dentin, and pulp (class III); and rootfractures. Because enamel, the outercovering of the tooth, has no directconnection to the pulp, no sensitivityis elicited in minimal fractures in-volving only the enamel. However,any trauma should be investigatedpromptly by the dentist, who willevaluate the extent of the injury. Itmay not be possible to determine thefull extent of the injury without aradiograph to determine root integrityand maturity.
A class II or III fracture involvingthe dentin or dental pulp requires im-mediate treatment to maintain the vi-tality of the pulp and to preserve thetooth. Exposed dentin is coveredwith calcium hydroxide (Ca(OH)2) to
stimulate healing, and the Ca(OH)2 iscovered by a bonded resin splint(“band-aid”). If the pulp is exposed,it must be treated promptly. In im-mature root formation, the exposedpulp may be partially amputated andtreated with Ca(OH)2 to promote vi-tal maturation; in mature and com-plete root formation, endodontics(root canal therapy) is the treatmentof choice.
When the root is fractured (a con-
dition that may not be obvious fromlooking at the tooth), the fracturemay be reduced manually, the toothsplinted (bonded) to adjacent teeth,and the splint left in position for sev-eral weeks until healing (an osteo-dentin bridge forms at the site of thefracture) takes place. Root canal ther-apy may be necessary on the moreproximal portion, although the distalsegment may remain vital.
Restoration of the immature oryoung tooth to a normal appearanceand function is possible using “bond-ing techniques” (Figure 8). In
bonded restorations, the surface ofthe tooth is prepared and etched with
mild phosphoric acid; an unfilledresin is applied to the surface; and afilled composite resin is added,shaped, and polished to appear as ifthe tooth is normal. In these restona-tions, the surface of the tooth ischanged only minimally, the treat-ment is accomplished at one session,the expenses and tooth preparationfor full crowns are avoided, the gin-gival contour and maturity of thetooth is not an issue, and the esthet-
ics and function are restored. Bondedrestorations lack edge (crushing)strength, particularly when exposedto nail-biting, but longevity and colonstability are excellent, and replace-ment should not become necessaryuntil many years later.
Avulsion of permanent teeth rep-resents a severe challenge for thedentist. Reimplantation is extremely
time-dependent, and after 30 mm-utes, the chances of success decreaserapidly. Avulsed teeth should not be-
come desiccated, non should they becleaned on debnided aggressively,which will make the periodontal biga-
ment (the soft tissue interface be-tween root and alveolar bone) lessvital. The tooth should be rinsed inplain water or saline solution andgently placed back into the socket.These patients should be instructed toclose their teeth into a gauze spongeand to see the dentist immediately. Ifthe situation prevents replacement ofthe tooth in the empty socket, plac-ing it in cold milk is an acceptableinterim solution for the trip to thedentist. The dentist will rinse and re-place the tooth, if it is not already inits socket, and splint the tooth to ad-
jacent teeth by using wire or bondedresins. After 1 week, the tooth isopened, pulpal contents are removed,and Ca(OH)2 is placed into the pulpcanal to maintain root integrity andstimulate root completion. Possible
complications include root resorptiondue to a reactive inflammation or re-placement by osteoid tissue with onwithout bony ankybosis. Successoften is short-lived and measured interms of normal eruption of adjacentteeth or maturation until an age whenprosthetic replacement is possible.Pediatricians and dentists should becertain that tetanus boosters are cur-rent and prescribe antibiotics (penicib-
at UNIV OF CHICAGO on April 26, 2013http://pedsinreview.aappublications.org/Downloaded from

�1
-� II fracture (enamel and dei of an incisor (A) and bonded restoration (B).
Pediatrics in Review VoL iS No. 8 August 1994 317
bin on erythromycin) to preventsecondary infection.
Special PatientsExtremely young, systemically ill,and immunosuppressed children andthose who have congenital anomalies
comprise a special group of patientswhose needs for treatment are uniqueand who benefit from the combined
treatment of physicians and dentists.Very young children who have se-vere dental caries may not toleraterestorative treatment in the usualchainside manner. Because of thecosts and risks, general anesthesia asan adjunct to restorative treatment isreserved for patients who require ex-
tensive treatment, who are unable totolerate chairside treatment, or whoby reason of physical, emotional, ormental handicap will not tolerate out-patient dental care. General anes-thesia and treatment in the mainoperating suite of a hospital is ac-
ceptable for restoring these children’sdentitions to relative dental health,
but it cannot be a crutch on which aparent may lean for ease of treat-ment. Parents must understand the
risks and be willing to assume theirown responsibility in assuring thatthis modality of treatment will not benecessary again. This treatment ap-pnoach must be reserved for truly in-dicated cases; a 10-year-old childbrought to the dentist to be “put tosleep” to have his teeth restored isnot an appropriate recipient for this
form of treatment. Sedation with ade-quate monitoring is a viable optionfor some of these patients and pro-vides a less expensive and less risky
alternative for limited restorativerequirements.
Patients who have systemic diseaseshould not be at increased risk ofdental infection. However, they mustbe educated to understand the neces-sity for maintaining good dentalhealth or be referred for treatment as
soon as that need is recognized. Pa-tients who have significant cardiacdisease, such as ventricular septal de-fects, tetralogy of Falbot, or valvulanprostheses, are at risk for bacterialendocarditis from dental infectionand should have restoration under
prophylactic antibiotic coverage priorto developing acute needs. In thesepatients, antibiotic SBE coverage is
necessary for all dental proceduresthat may produce a transient bactene-mia, including routine prophylaxis,according to the recommendations of
the American Heart Association.Similarly, patients who have renaldisease or indwelling shunts on cathe-tens also may be at risk for infectionand should be maintained in a stateof sound dental health and prescribedantibiotics prophylactically duringtreatment. Those who have hemo-philia and other bleeding diathesesmay be treated safely with factor ne-placements on plasma infusions, andclot breakdown after extraction maybe prevented further by use of epsi-lon aminocaproic acid 100 mg/kg forseveral days.
Patients undergoing chemotherapyor awaiting bone marrow transplantfrequently suffer from oral ulcena-tions, which are extremely painful.Oral rinses containing chlorhexidenereduce plaque accumulations and pro-mote healing; modified oral hygienetechniques further reduce inflamma-
tion. As in the case of those whohave cardiac disease, the overallhealth of these patients may be com-promised further by dental infection,and each patient should have a care-ful dental screening prior to the initi-
ation of treatment. Potential sourcesof dental infection should be elimi-nated. Similarly, pediatric patientswho have human immunodeficiencyvirus infection are subject to aggres-sive and painful episodes of gingivi-tis, and their overall condition isworsened by dental infection. Scru-pulous hygiene and restorative treat-ment before any condition reaches acritical stage may eliminate the denti-tion as a complication of treatment.
Finally, patients whose syndromesinclude craniofacial problems or pa-tients who have cleft lip and cleftpalate represent a unique opportunity
MOUTh AND TEETHDntaI Updat.
for the pediatrician and pediatric den-tist to provide care as members of amultidisciplinary, integrated healthcare team. Cleft lip and palate,which are separate (sometimes asso-ciated) entities, occur during thesame embryologic period as the initi-ation and development of the denti-tion. During development of theprimary palate and lip, the failure orbreakdown of the fusion of medialand lateral nasal processes with themaxillary process affects the dentalalveolus in the area of the lateral in-cisons. The insult to the dentitionmay involve the teeth and supportingalveolar bone from the central incisorto the canine tooth, and in the casesof bilateral cleft lip and palate, mayaffect both sides of the dentition.This congenital anomaly affects ap-proximately 1 in 800 live caucasianbirths, with a significantly higher in-cidence among Asians and lower in-cidence among African-Americans;males are affected more frequentlythan females, and in unilateral clefts,the left side is affected more fre-
quently than the right.At birth, immediate concerns focus
on nutrition and surgical correction,with a greater concern oven the pat-ency of the airway in Pierre Robinsyndrome (cleft palate, macroglossia,netrognathia with glossoptosis). Pe-diatric dentists may assist the feedingprocess on enhance the plastic sur-gical repair by constructing intnaoralappliances to obdurate the palate ordentofacial orthopedic appliances tomold the palatal segments and relievepressure on the lip prior to surgery.
Patients who have oral clefts pres-ent many dental challenges, includingthe absence of teeth (oligodontia);the presence of multiple supernumer-ary teeth in the area of the cleft al-veolus and palate; enamel hypoplasiaand gross deformities of teeth adja-
at UNIV OF CHICAGO on April 26, 2013http://pedsinreview.aappublications.org/Downloaded from

FIGURE 9. An 8 1/2-year-old male has a
repaired unilateral cleft lip and palate (A).
The greater palatal segment is ma/positioned
and the teeth are rotated and ma/positioned
prior to bone grafting and alignment of teeth
(B).
318 Pediatrics in Review VoL 15 No. 8 August 1994
MOUTH AND TEETHDental Update
cent to the cleft; mabocclusions, in-cluding anterior and posterior
crossbites (reversal of normal babio-lingual relationships of the maxillaryand mandibular dentitions); andgrowth discrepancies that reflect a
generalized maxillary hypoplasia re-sulting in a pnognathic malocclusionand soft tissue profile (Figure 9).Dental treatment requirements in-clude restorations, removal of extra
teeth, correction of mabocclusions viainterceptive and fully corrective or-thodontics, prosthetics to replace
missing teeth, and maxillofacial sun-gery to correct gross skeletal discrep-ancies of maxilla and mandible. The
pediatric dentist, along with the pe-diatnician, is key to informing theparents and supporting the earlygrowth and development of the pa-
tient who has a cleft lip/palate andfunctioning as a member of a teamthat includes the plastic surgeon, or-thodontist, speech pathologist, oto-rhinobaryngologist, audiologist,geneticist, nurse feeding specialist,and pediatrician.
Other congenital anomalies of thecraniofacial complex requiring theteam approach include Treacher-
Collins syndrome and hemifacial mi-crosomia, which affect the eyes,ears, vertebrae, and mandible. Thesepatients may exhibit a lack of devel-opment of one or both sides of themandible to varying degrees, result-ing in a canted plane of occlusion
and asymmetric facial development.Early dental treatment includes thesurgical lengthening of the affectedmandibular namus and the growth-assisted orthodontic correction of theresultant open bite. In Crouzon orApert syndrome (craniosynostoses),there is a maxillary hypoplasia, openbite, and significant dental crowding.Each patient who has anomalies af-fecting the craniofacial complex mustbe supported with effective dietarycounseling, fluoride supplementation,and home oral hygiene instructionbeginning in infancy to minimize thecomplicating effects of the dentalcaries process.
ConclusionIt is important that all pediatricianshave a thorough understanding oforal disease and its consequences tothe total health of the child. As the
director of health cane for the infant,the pediatrician usually is the first to
give dental advice to a parent andmay be the first to recognize theneed for the assistance of the oralhealth specialist, the dentist. Pedia-tnic dentists, trained in growth anddevelopment, behavioral sciences,and hospital services, stand ready aspartners to serve on the child’s healthcare team.
SUGGESTED READINGBaht M. Periodontal health of 14 to 17 year-
old United States school children. J Pub
Health Dent. 1991;51:5-11Committee on Nutrition. Fluoride supplemen-
tation. Pediatrics. 1986;77:758-761Fromm A. Epstein’s pearls, Bohn’s nodules,
and inclusion cysts of the oral cavity. JDent Child. 1967;34:275-287
Hughes iT, Rozier RG, Bawden JW. A surveyof periodontal disease in a state popu-lation-an emphasis on children. Ped Dent3. (Special Edition). 1981;l 14
Kaban LB. Pediatric Oral and Maxillofacial
Surgery. Philadelphia, Pa: WB Saunders;1990
Kates GA, Needleman HL, Holmes LB. Nataland neonatal teeth: a clinical study. JADA.1984;109:441-444
Lunt RC, Law DB. A review of thechronology of calcification of deciduousteeth. JADA. 1974 ;89:599
Macdonald RE, Avery DR. Dentistry for theChild and Adolescent, ed 5. St. Louis, Mo:cv Mosby; 1988
Milano M, Dushku JC. Evaluation of theeffects of orthodontic pacifiers on theprimary dentitions of 24-59-month-oldchildren: a preliminary study. Ped Dent.
1992;14: 14-18National Institute of Dental Research. The
Prevalence of Dental Caries in the UnitedStates in Children, Oral Health of U.S.
Children. NIH Pub No. 89-2247. Bethesda,MD; US Department of Health and HumanServices: 1989
Popovich F, Thompson OW. Thumb andfinger sucking: its relation to malocclusion.Am J Orthodont. 1973;63:148
Rosenblatt GM, Alongi JA, Deasy Mi.Periodontal disease in children. C/in Prey
Dent. 1983;5:1720
Shusterman 5, Needleman HL. In: Avery ME,First LR, eds. Dentistry in Pediatric
Medicine. Baltimore, Md: Williams andWilkins; 1989
at UNIV OF CHICAGO on April 26, 2013http://pedsinreview.aappublications.org/Downloaded from

DOI: 10.1542/pir.15-8-3111994;15;311Pediatrics in Review
Stephen ShustermanPediatric Dental Update
ServicesUpdated Information &
http://pedsinreview.aappublications.org/content/15/8/311including high resolution figures, can be found at:
Permissions & Licensing
/site/misc/Permissions.xhtmlits entirety can be found online at: Information about reproducing this article in parts (figures, tables) or in
Reprints/site/misc/reprints.xhtmlInformation about ordering reprints can be found online:
at UNIV OF CHICAGO on April 26, 2013http://pedsinreview.aappublications.org/Downloaded from