Embed Size (px)
DESCRIPTION
Pediatric Bipolar Disorder. David Camenisch , MD/MPH PAL Conference Jackson, WY May 5, 2012. Cody (RR 2.5) - History. 6 year old mixed-race (NA/AA) boy new to your practice ADHD diagnosis at age 4. On and off stimulants for 2 years. - PowerPoint PPT Presentation
Citation preview
David Camenisch, MD/MPHPAL Conference
Jackson, WYMay 5, 2012
Pediatric Bipolar Disorder
May 5, 2012PAL Conference
Cody (RR 2.5) - History6 year old mixed-race (NA/AA) boy new to your
practiceADHD diagnosis at age 4. On and off stimulants for 2 years. Has been tried on both methylphenidate and
amphetamine preparations. They tend to work for a while but then things “go
back to normal.” He has always been “moody.” Struggling at school socially but “really smart.” Per
mom, “He reads real history books and remembers everything.”
May 5, 2012PAL Conference
Cody – Presentation Mom thinks he is bipolar. She just got
diagnosed and medications have really helped her.
Mom says she can’t control him at home. A little better with mom’s boyfriend of who has been in and out of the picture for 2 years.
Actually, mom just stopped stimulants because she heard they can make things worse if your kid has bipolar. She thinks he is doing better.
She asks you to prescribe “something” to treat his bipolar mood swings……
May 5, 2012PAL Conference
What To Do?What role should a primary care provider take
regarding the question of child bipolar disorder?Psychoeducation?Referral?Treatment?
How do you assess for childhood bipolar disorder?
When does it make sense to… WaitPrescribe a mood stabilizer?Refer to a therapist? Refer to a (child and adolescent) psychiatrist?
May 5, 2012PAL Conference
Bipolar Is A Hot TopicBipolar disorder in kids is much talked
about“Child Anxiety Disorder” on Google
26,600,000 hits (3,120,000)“Child Bipolar Disorder” on Google
33,100,000 hits (4,370,000)(Camenisch 2012, Camenisch 2011)
Child anxiety disorders are actually about 10 times more common than child bipolar disorder
40 fold increase in office visits for child bipolar disorder from 1994 to 2003 (Also 40-fold increase in diagnosis.)
National Center for Health Statistics May 5, 2012PAL Conference
Frequency of Childhood BipolarVery controversial Some assert a high frequency of all children
have bipolar disorder“The Bipolar Child” by Papolos and Papolos
Assert 1/3 of all children with ADHDStates about 6% of all children are bipolar
“Is Your Child Bipolar” by McDonnell and WozniakStates more than 3 million US kids have itBased on their estimates, incidence is 4%.
May 5, 2012PAL Conference
Quoted Child Rates Don’t Match Our Adult Knowledge
Adult Lifetime prevalence rates of bipolar disorder 1 to 2%
Greater diagnostic certainty with adultsBipolar disorder is a lifelong diagnosis – need
plausible explanation if pediatric bipolar is 3-6X > adult bipolar
Lessons from Great Smoky Mountain data set child bipolar NOS ≠ bipolar adult
Kids with bad mood swings cannot all have “true” bipolar disorder
May 5, 2012PAL Conference
Why is diagnosis so challenging?Symptom overlap + high rates of co-morbidityConfounding developmental issuesEnvironmental influences Limited ability of (many) children to verbalize
emotionsMany different “expert” opinionsInfluence of popular media/pharmaceutical
industryRequires extensive history – assessment of
both current symptoms and past episodes (subject to recall bias.)
May 5, 2012PAL Conference
DSM-IV TR (Hypo)Manic Episode
Manic Episode – 7 days + impairment, or hospitalization or psychosisDistinct period of abnormal and persistently
elevated*, expansive or irritable mood Plus 3 (4 if “irritable-only” mood) of the following:
DistractibleGrandiose/inflated self-esteem*Decrease need for sleep (< 3 hrs)More talkative/pressured speechIndiscretions/risk taking Flight of ideas/racing thoughts Increased goal directed activities/PMA
Hypomanic Episode – 4 days. No hospitalizations. No impairment.
May 5, 2012PAL Conference
Depressive Episode5 or more of following in same 2 week
period + depressed/irritable mood OR lost of interest/anhedonia
Sleep InterestGuilt Energy (fatigue)ConcentrationAttentionPMA/PMR (observable)Suicidal thoughts/feelings/behaviors
Functional ImpairmentNo Mixed Episode, R/O Substance, R/O
GMC, R/O BereavementMay 5, 2012PAL Conference
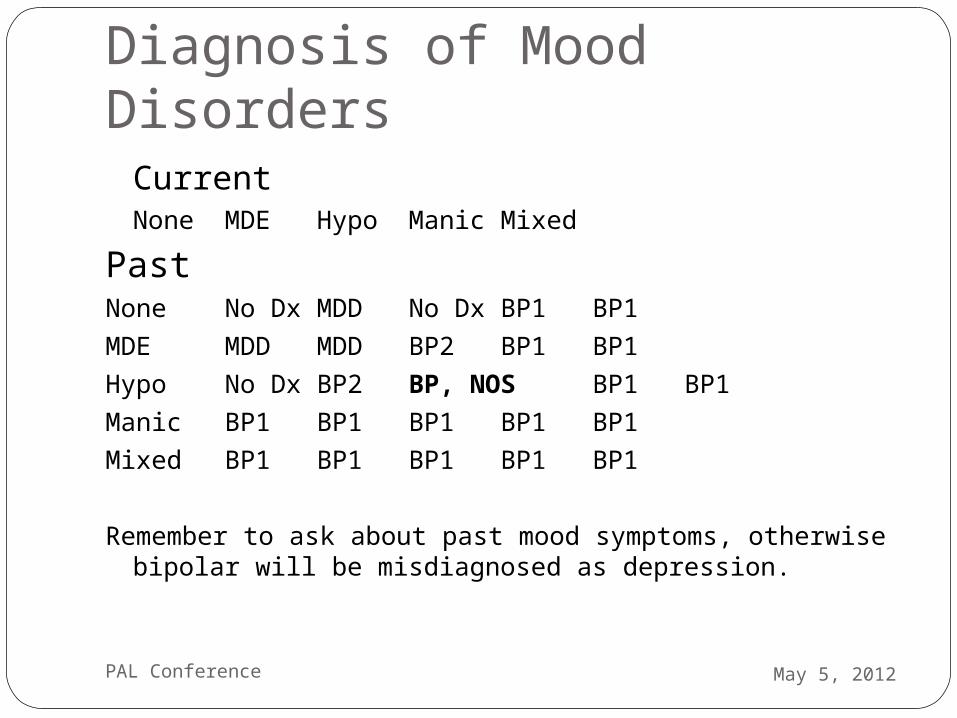
Diagnosis of Mood DisordersCurrent
None MDE Hypo Manic MixedPastNone No Dx MDD No Dx BP1 BP1MDE MDD MDD BP2 BP1 BP1Hypo No Dx BP2 BP, NOS BP1 BP1Manic BP1 BP1 BP1 BP1 BP1Mixed BP1 BP1 BP1 BP1 BP1
Remember to ask about past mood symptoms, otherwise bipolar will be misdiagnosed as depression.
May 5, 2012PAL Conference
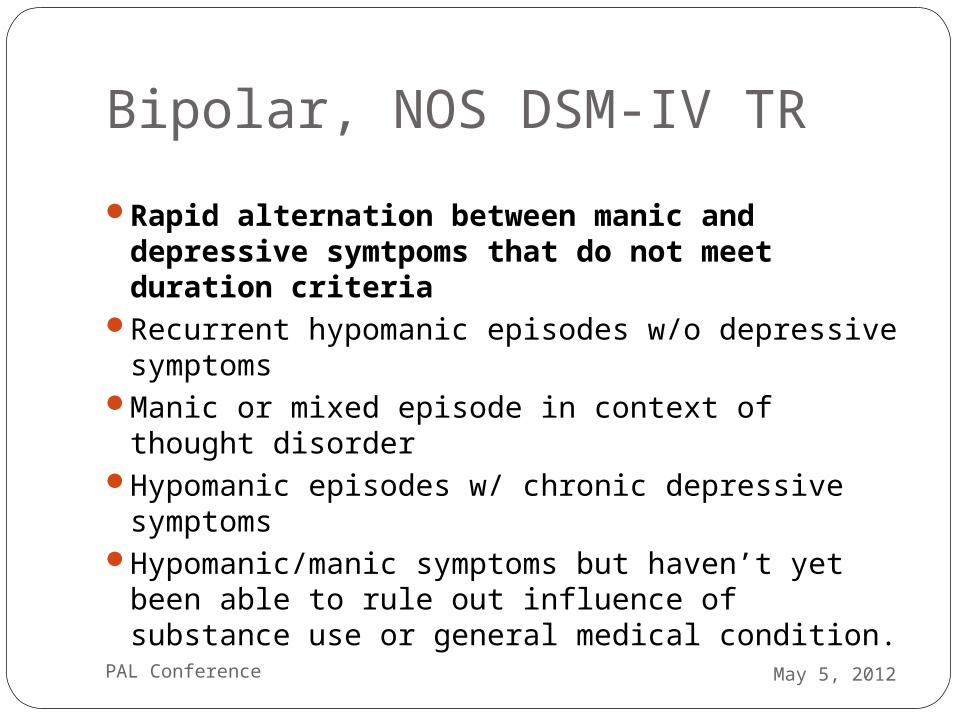
Bipolar, NOS DSM-IV TRRapid alternation between manic and
depressive symtpoms that do not meet duration criteria
Recurrent hypomanic episodes w/o depressive symptoms
Manic or mixed episode in context of thought disorder
Hypomanic episodes w/ chronic depressive symptoms
Hypomanic/manic symptoms but haven’t yet been able to rule out influence of substance use or general medical condition.
May 5, 2012PAL Conference
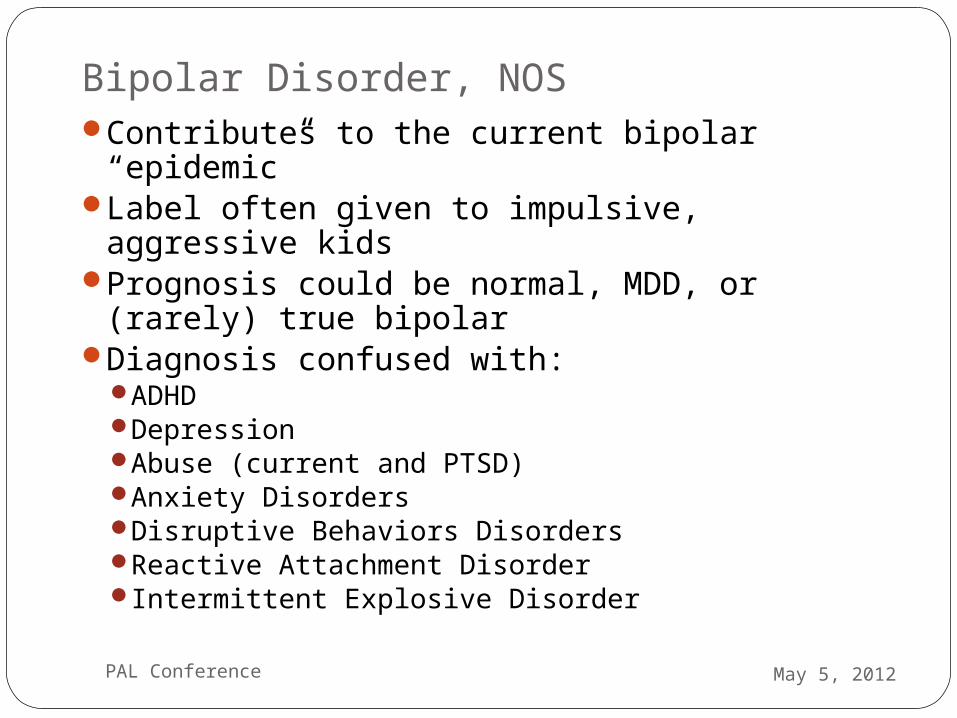
Bipolar Disorder, NOSContributes to the current bipolar “epidemic”Label often given to impulsive, aggressive
kidsPrognosis could be normal, MDD, or (rarely)
true bipolarDiagnosis confused with:
ADHDDepressionAbuse (current and PTSD)Anxiety DisordersDisruptive Behaviors Disorders Reactive Attachment Disorder Intermittent Explosive Disorder
May 5, 2012PAL Conference
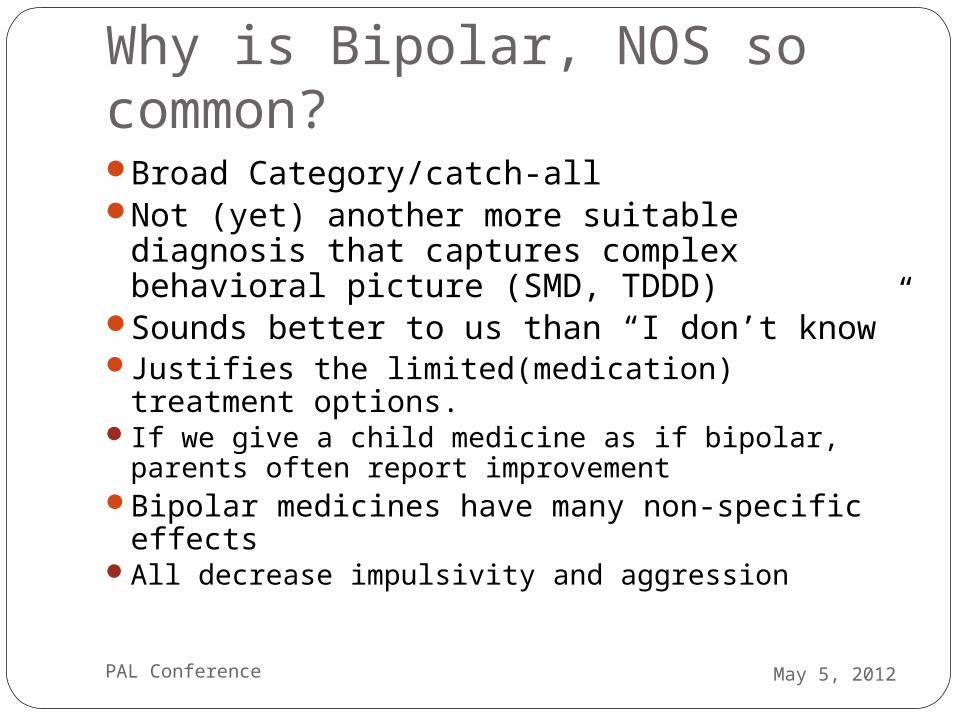
Why is Bipolar, NOS so common? Broad Category/catch-allNot (yet) another more suitable diagnosis
that captures complex behavioral picture (SMD, TDDD)
Sounds better to us than “I don’t know”Justifies the limited(medication) treatment
options.If we give a child medicine as if bipolar, parents
often report improvementBipolar medicines have many non-specific
effectsAll decrease impulsivity and aggression
May 5, 2012PAL Conference
If not bipolar, then what? DepressionOngoing abuse/neglect Post-trauma symptoms or syndrome Environmental Instability (frequent change in living
arrangement/primary care giver; parental mental illness)Disordered Attachment (RAD) Temperament Mismatch (Parent-Child Relational
Problem)Anxiety (especially brief, episodic, reactive “mood
swings” )Disruptive Behavior Disorders (ADHD,ODD) Affective lability in context of autism spectrum disorder
(co-morbidity versus core disorder attribution)May 5, 2012PAL Conference
Severe Mood Dysregulation (SMD)Clinical syndrome not a diagnosis (3.3%
lifetime prevalence ages 9-19)“chronically irritable children whose diagnosis
is in doubt.” (Often the “Bipolar, NOS crew) IS real and confers risk of psychopathology
down the line, but is NOT bipolar disorder (also not Axis II)
Presence of SMD increases risk of depressive disorder and GAD at 20 year follow-up. Stringaris et al, 2010
May 5, 2012PAL Conference
Bipolar Disorder Frequency Depends On Where You Look
Prevalence of “true” adolescent bipolar0.6% of high school students 1% in general outpatient practice 6 % of child psychiatry outpatients (CMHC)22% incarcerated adolescents 26-34% of child psychiatry inpatients manic
symptoms(1996-2004 CDC survey of discharge diagnosis)
Youngstrom et al, CAPC Vol 18
May 5, 2012PAL Conference
Cody – The QuestionsTest out whether un/under-treated ADHD (haven’t
found right medication, right dose; hasn’t had behavioral help, parenting support) or do you need to consider mood disorder?
Or co-morbidity (depression, anxiety, ODD) Ask for more detail than just “labile moods” (hyper-
arousal)and “won’t listen” (distractibility)How is his mood most of the day? What causes (if anything) his mood to change? When not upset, what does he look like? Can he “pull out of it”Does he “listen” when he is asked to do something he wants to
do?
May 5, 2012PAL Conference
Cody – The AnswersMom says he “never listens to me” especially
when asked to do chore/homework/go to bed. Goes into rages when doesn’t get his wayThrows things at mom, hits her. Says “I hate
you.” Tried “everything,” even spanking, taking
away the Xbox. With dad or other adults he behaves better.
Some talking back, but manageable. Knows he needs to cool it or he going to get in trouble.
May 5, 2012PAL Conference
Cody – At School In 2nd grade, teacher said he was not
listening well in beginning of year, is better now
In kindergarten he didn’t follow rules wellPerforming at grade level Not having rages at school Generally more of a problem at home
more than at school
May 5, 2012PAL Conference
Cody – Social History and Development Mom is primary caregiver.1 younger brother, mom thinks she might be
pregnant. No contact with dad. Left before Cody was born. Mom has few supports. Mom’s family and tribe
“disowned” her and Cody because his father is AA.
Developmental milestones were OK“Read early. Very verbal. Reads “anything
about history” and “remembers everything.” No in utero drug exposure identified.
May 5, 2012PAL Conference
How to answer Mom’s Question if this is Bipolar Disorder?Difficult diagnosis (no “tests”)Diagnosis best made “over time” ; usually not
point-in-time diagnosis --especially with chronic presentation
Many different opinions, even among specialistsDown side of labeling too early If you think NOT bipolar, continue with…
Psycho-education. (Non-specific nature of “mood swings” and “irritability” e.g. cough analogy)
Reasonable to consider treatment depending on potential consequences. (Sx-driven versus dx-driven treatment*)
May 5, 2012PAL Conference
Consider the large differential for each of these Mania symptoms in kids:
DistractibleIndiscretions/risk takingGrandioseFlight of ideas/racing thoughts Activity (goal directed) increaseSleep need decreasedTalkative (pressured speech)
Which can mimic ADHD symptoms? May 5, 2012PAL Conference
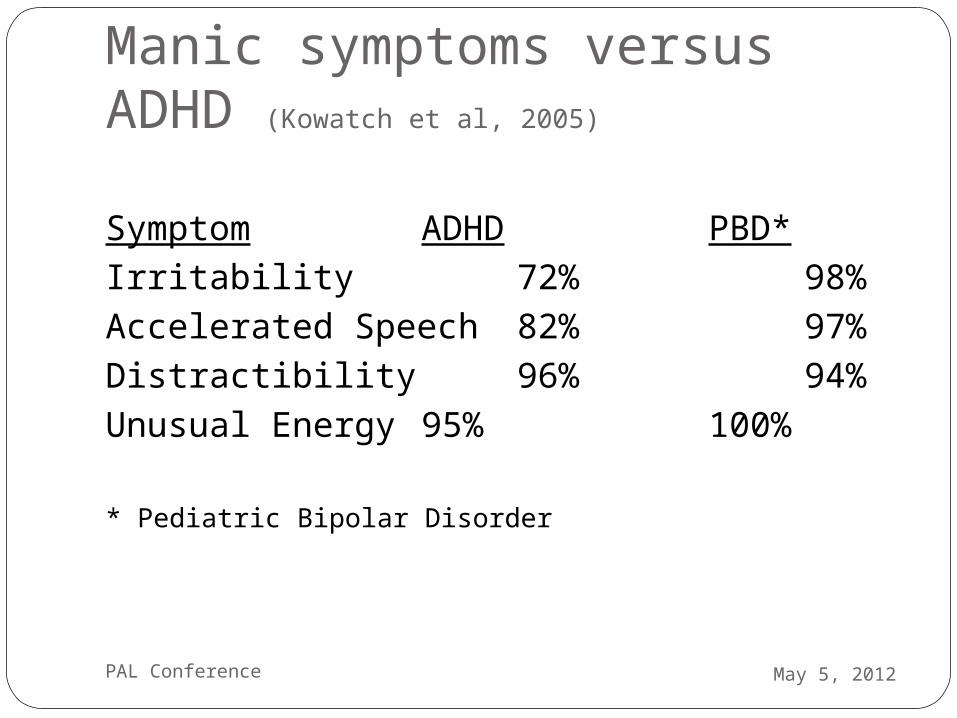
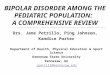
Manic symptoms versus ADHD (Kowatch et al, 2005)
Symptom ADHD PBD*Irritability 72% 98%Accelerated Speech 82% 97%Distractibility 96% 94%Unusual Energy 95% 100%
* Pediatric Bipolar Disorder
May 5, 2012PAL Conference
Diagnostic PerspectiveExperience with adult mania helps, but can
be challenging to translate to kids. (Different patterns of diagnosis between Adult and C&A psychiatrists?)
Compare child to a prototypic “manic” patientPressured speech -- not just talkativeHaving no doubt about their grandiose ideas --
impaired reality testing/lack of insight)Thought process is fast and jumping around Episodes that most commonly last days not minutes or
hoursLittle need for sleep (versus poor sleep.)
May 5, 2012PAL Conference
Look for Episodes and Patterns
Individual episodes represent a clear departure from baseline with some hallmark symptoms
Hopefully, the presence of hallmark symptoms will help distinguish irritable mania from irritable depression
The correct mood diagnosis (and treatment) requires establishing the pattern of mood episodes, not just presenting (current) episode.
May 5, 2012PAL Conference
Rapid Cycling Controversy Typical adult pattern is episodic. Rapid cycling is
rare in adult bipolar populations. Kids are more reactive and more common to get
story of “rapid cycling.” Consider “rapid cycling” in kids if there is no trigger
identifiable for the mood changesWhere many “episodes” become static, chronic
mood state is controversial.ADHD plus irritability should not generate a bipolar
diagnosisYouth with BP do spend more time cycling and have
more changes in mood polarity that adult populations. (Birmaher et al, 2006)
May 5, 2012PAL Conference
Chronic versus Episodic IrritabilityObjective: Test validity of distinction between chronic
and episodic irritability. (Central debate in pediatric bipolar)
Method: Community sample of 776 children and adolescents interviewed at 3 points in time (T0, T2y, T7y). Irritability rating scales used to tease out chronic versus episodic irritability. Association with age, gender and diagnosis were examined.
(Liebenluft et al, 2006)
May 5, 2012PAL Conference
Chronic vs Episodic Irritability Those with episodic irritability were more likely
than those with chronic irritability to have:A parent diagnosed with Bipolar Disorder Experienced elation and/or grandiosityMore symptoms of mania Psychotic symptomsHad a depressive episodeMade a suicide attempt
(Liebenluft et al, 2006)
May 5, 2012PAL Conference
Irritability and Later PsychopathologyChronic irritability at TI - associated with ADHD at T2 and depression at T3Episodic Irritability – associate with simple phobia at T2 and mania at T3
Conclusions: - Episodic and chronic irritability are distinct constructs. - Episodic irritability is associated with bipolar disorder and confers higher risk of future manic episodes than chronic irritability.
(Liebenluft et al, 2006)
May 5, 2012PAL Conference
Irritability Controversy Geller: Irritability is not diagnostic of PBD;
it is very common and shows high sensitivity, but poor specificity for PBD
Wozniak: irritability may be primary mood symptom; episodicity not relevant.
Leibenluft: In diagnosing PBD, episodic irritability is more suggestive of PBD than is chronic irritability
Hunt/Birmaher – episodic irritability alone can represent manic phase of illness; “irritable-only” mania exists but is rare; more common in younger children. (COBY).
May 5, 2012PAL Conference
Look for “Hallmark” SymptomsIncreased specificityMore likely bipolar…
Elation HyperactivityGrandiosityHypersexualityDecreased need for sleep
May 5, 2012PAL Conference
Bipolar Diagnostic AidesRating Scales
Young Mania Rating ScaleUseful for monitoring symptoms over timeNot a diagnostic tool (very low specificity)
DISC or KSADSUsed in research, have flawsImpractical for your office practice
Rating scales are too misleading to recommend for diagnostic use and are intentionally excluded from the PAL guide.
May 5, 2012PAL Conference
Cody Rage episodes seem directed mostly at
mom, and mom’s attempts to set limits at home
Mood changes occur mostly in response to frustrations
There are not any hallmark symptoms of grandiosity, euphoria, hypersexuality
No history of days-long episodesHe is very young to diagnose as bipolar
May 5, 2012PAL Conference
What about Family History?Mom says she has been diagnosed with bipolar
and his uncle is bipolar, “just like him”
Avoid overcalling a positive family historymany adults who call themselves bipolar may not
have that illnessfirst degree relative bipolar disorder, increases OR by
5second degree relative bipolar, increase OR by 2.5given a generous prevalence of 2% bipolar in the
population, most children of a bipolar parent (~90%) will not have bipolar disorder
Youngstrom E & Duax J, JAACAP 44:7, 2005
May 5, 2012PAL Conference
Looking back at adult bipolar….Several studies have asked adults with
bipolar about onset of their symptoms retrospectively
Bipolar adults look back and note symptoms became bipolar-like in their teen years (50-66%)
Many bipolar adults had major depression episodes as children
The younger the child’s first major depression, the more likely bipolar disorder is in the future
May 5, 2012PAL Conference
What if a “Bipolar” Child Really is Bipolar?Though rare in a PCP practice, becomes
more likely the older the child.Typical pattern is early onset
depression, and during teenage years getting first symptoms of mania.
Expect mood “episodes”. COBY study established validity of episodic course.
Assemble a team. Real deal bipolar disorder is a big problem.
May 5, 2012PAL Conference
Course Of True Bipolar DisorderSuicidalilty
up to 15% eventually complete suicideSubstance Abuse in up to 60%Anxiety disorders in up to 50%Psychotic features in up to 50%Relationship DisruptionsWork DisruptionsHospitalizations
Stern TA and Herman JB, 2004May 5, 2012PAL Conference
Bipolar TreatmentIf clear manic episodes, strongly
recommend get them to child psychiatristManagement difficult because:
High rate of substance abuseHigh rate of medication non-complianceEven with medication, recurrences happen
High rates of family disruption from the illness
Suicidal behavior is common
Brent et al, 1988, 1993
May 5, 2012PAL Conference
If No Child Psychiatrist Can Assume Care, Then What?Get collateral evaluations to help
establish correct diagnosisStrongly advise against rushing to offer diagnosis
of bipolar disorder.Seek consultant advice on medication
(when they are appropriate to consider)Preferred model of care:
MH specialist is primary prescriberPCP is a partner in the treatment team
Call the Provider Access Line. Sometimes PCP is left holding the bag
May 5, 2012PAL Conference
Bipolar Treatments (for when you are left holding the bag)
Atypical antipsychoticsMood StabilizersCombination therapyAntidepressants if used cautiouslyFamily therapy (support/education/adherence)Sleep hygeine Psychotherapy for:
depression treatmentcoping skillssupporting medication treatment adherence
May 5, 2012PAL Conference
Bipolar Medications
May 5, 2012PAL Conference
What Is A Mood Stabilizer?Includes both atypical anti-psychotics and anti-
epileptic drugs (AEDs)Generic term – clarify what they mean when
taking history and what you mean when proposing treatment.
FDA does not recognize this term As relates to treatment of bipolar disorder, ideally
treats both depressive and manic episodes as well as prevents recurrence of mood episodes.
Since no one compound does this well, multiple meds are often used together (but little evidence base to support it.)
May 5, 2012PAL Conference
Mood Stabilizers are Non-Specific to PBDMaladaptive aggression
Mental retardation (lithium, risperidone) Autism (risperidone, aripiprazole)Conduct Disorder (risperidone, valproic acid,
lithium) Seizure Disorders – kindling hypothesis;
neuroprotective effects in mood disorders (lithium)
Depression (risperidone, aripiprazole, quetiapine, lamotrigine)
Psychosis (primary, mood disorder, delirium) OCD (refractory) PTSD (intrusive thoughts)
May 5, 2012PAL Conference
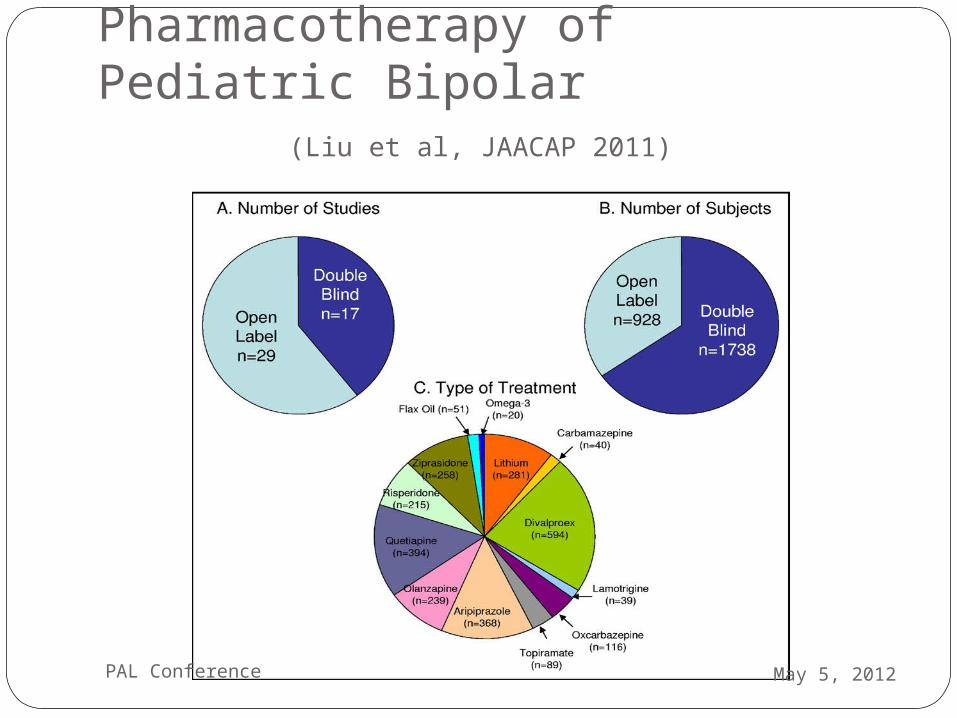
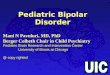
Pharmacotherapy of Pediatric Bipolar (Liu et al, JAACAP 2011)
May 5, 2012PAL Conference
Positive Randomized Trials Blinded RCT knowledge base in kids is lowAytpical anti-psychotics
OlanzapineAripiprazole (2) Quetiapine (3)Risperidone (1)
AEDsDivalproex sodium (Depakote) Li (maintenance)
May 5, 2012PAL Conference
Atypical Antipsychoticsrisperidone, quetiapine, olanzapine,
aripiprazole, ziprasidone11 OTs with 53% response rate8 DBRCTs with 66% response rate N = 1474
That DBRCTs showed greater efficacy than placebo is encouraging and noteworthy
Better tolerated than AEDs as a group.
May 5, 2012PAL Conference
Risks common to all Atypical Antipsychotics (Correll, JAACAP. 2008)
Sedation (olanzapine, quetiapine)Tardive Dyskinesia (0.4% annual incidence)Increased Cholesterol/ Triglycerides (olanzapine) Akathesia (aripiprazole) (youth<adults)Increase glucose (olanzapine, quetiapine)EPS (risperidone)Lower seizure threshold (mildly)QT interval change (~20ms for ziprasidone)Weight gain (olanzapine > quetiapine,
risperidone >the rest)Neuroleptic Malignant Syndrome
May 5, 2012PAL Conference
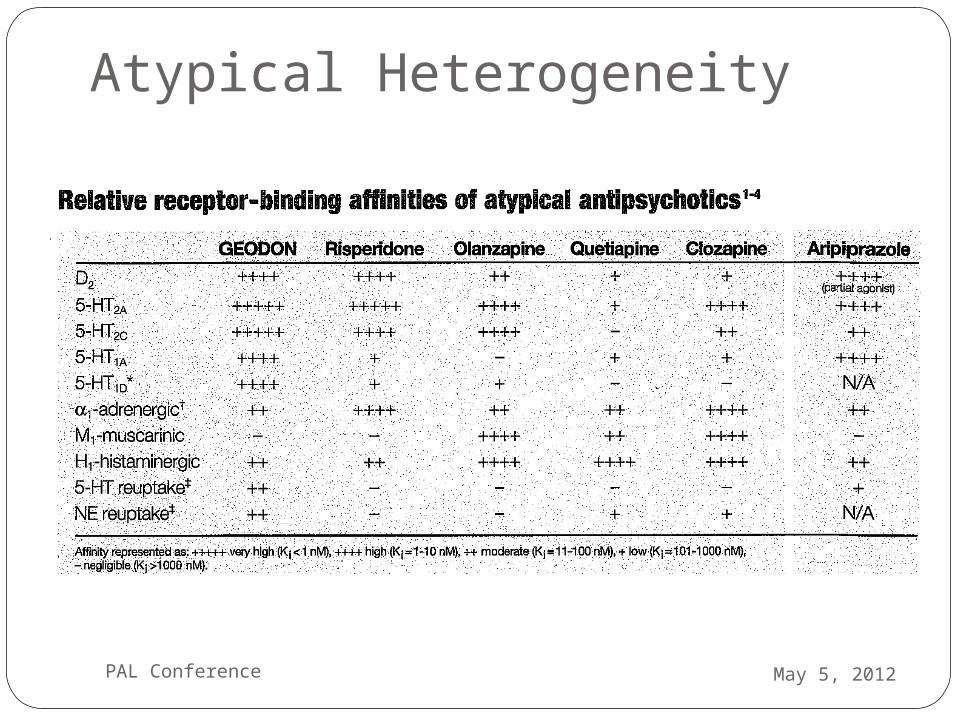
Atypical Heterogeneity
May 5, 2012PAL Conference
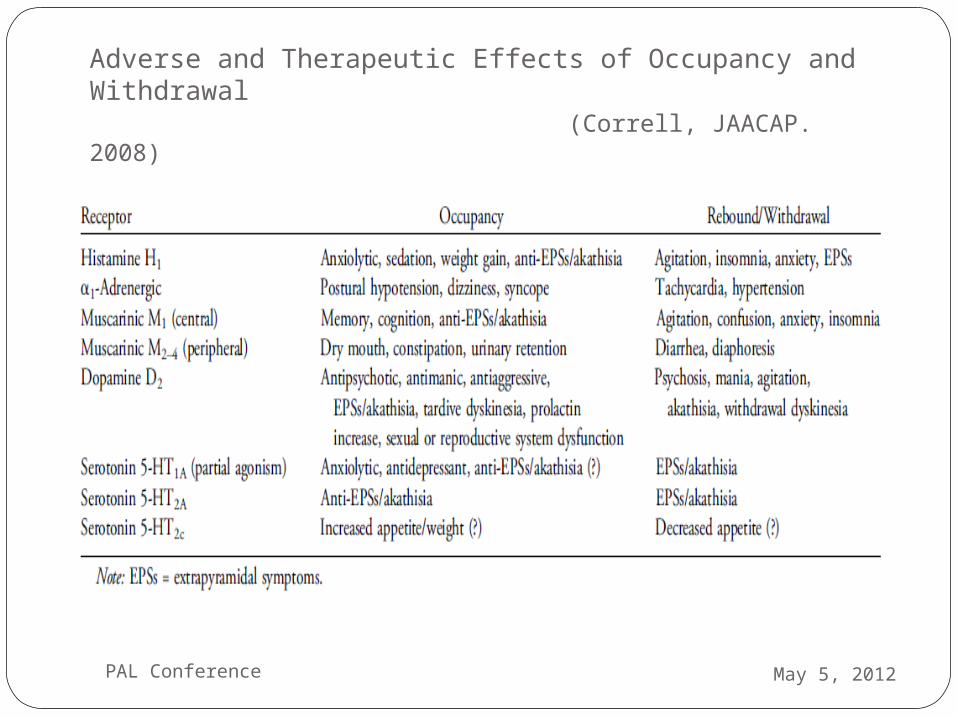
Adverse and Therapeutic Effects of Occupancy and Withdrawal
(Correll, JAACAP. 2008)
May 5, 2012PAL Conference
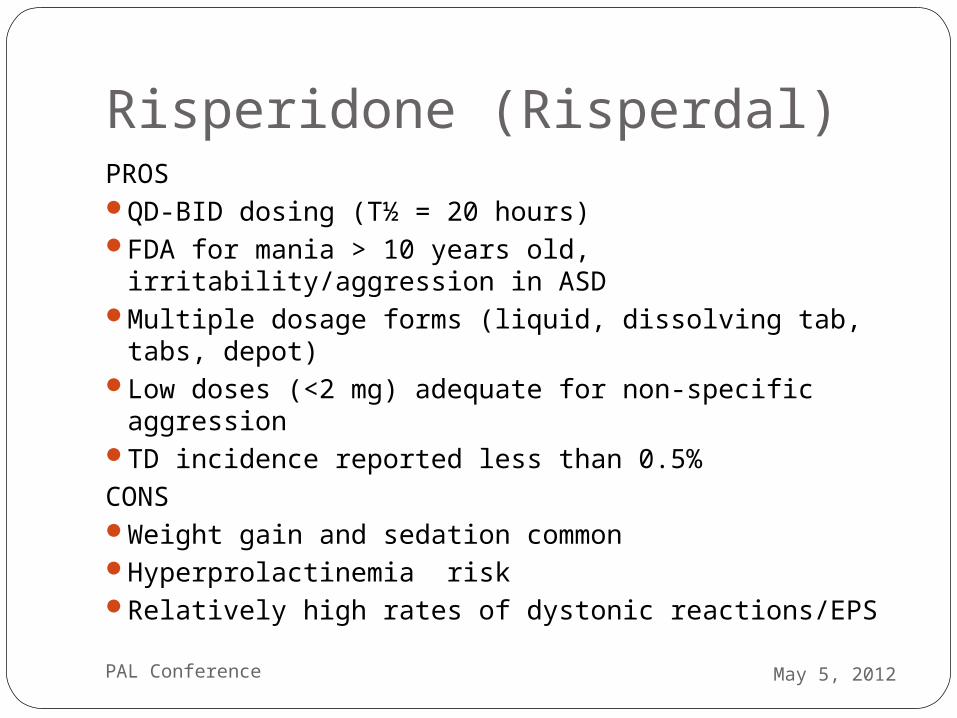
Risperidone (Risperdal)PROSQD-BID dosing (T½ = 20 hours)FDA for mania > 10 years old, irritability/aggression in
ASDMultiple dosage forms (liquid, dissolving tab, tabs,
depot) Low doses (<2 mg) adequate for non-specific aggressionTD incidence reported less than 0.5%CONS Weight gain and sedation commonHyperprolactinemia riskRelatively high rates of dystonic reactions/EPS
May 5, 2012PAL Conference
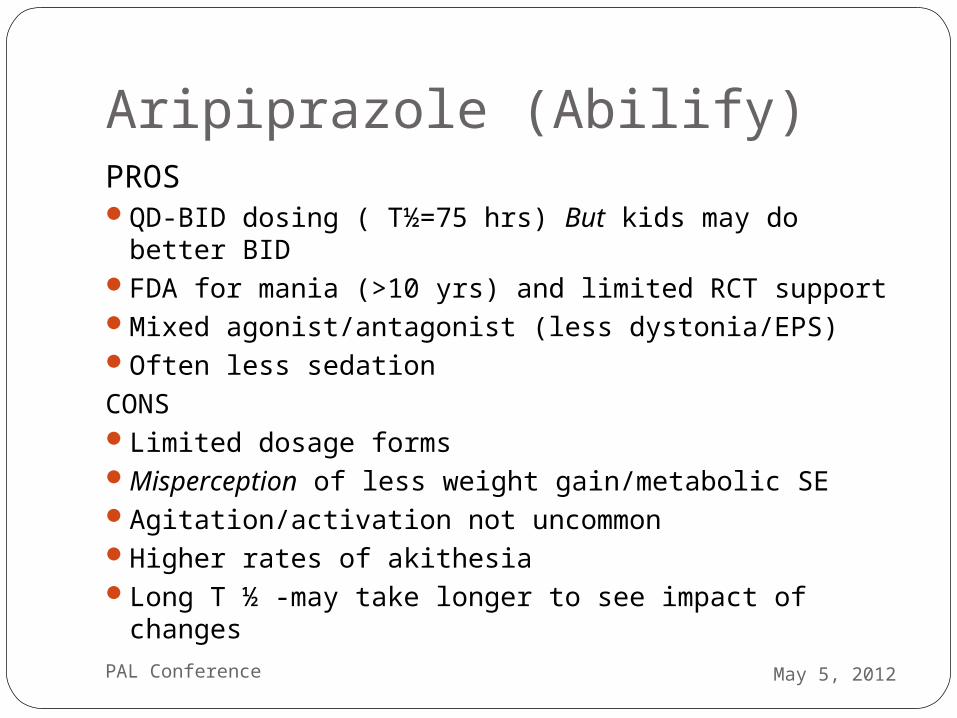
Aripiprazole (Abilify)PROSQD-BID dosing ( T½=75 hrs) But kids may do better
BIDFDA for mania (>10 yrs) and limited RCT supportMixed agonist/antagonist (less dystonia/EPS)Often less sedationCONSLimited dosage formsMisperception of less weight gain/metabolic SEAgitation/activation not uncommonHigher rates of akithesiaLong T ½ -may take longer to see impact of changes
May 5, 2012PAL Conference
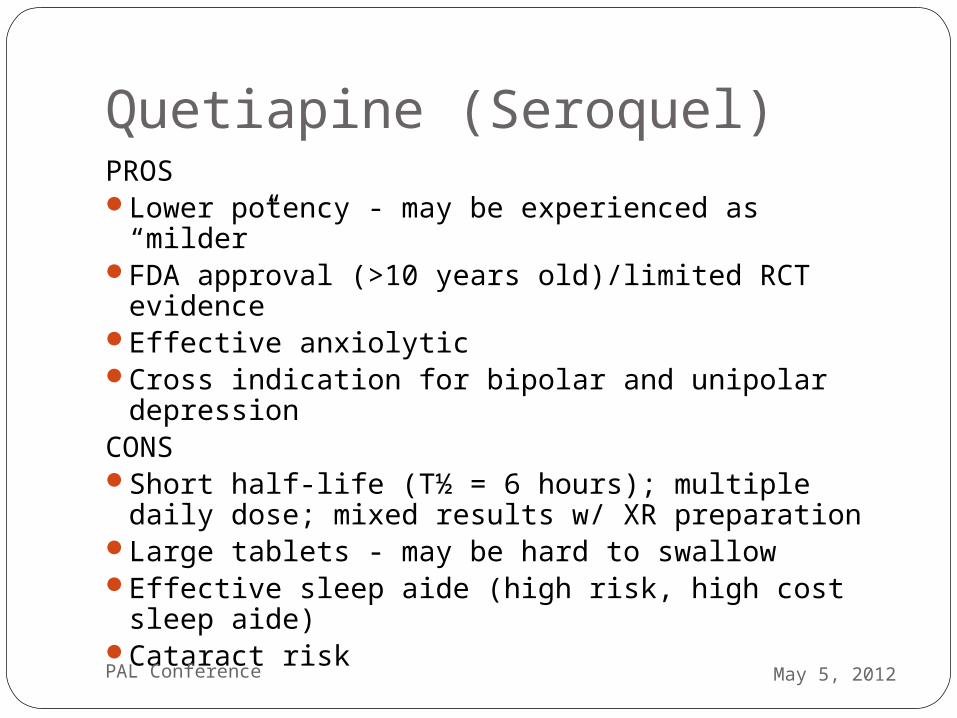
Quetiapine (Seroquel)PROS Lower potency - may be experienced as “milder”FDA approval (>10 years old)/limited RCT
evidenceEffective anxiolyticCross indication for bipolar and unipolar
depressionCONSShort half-life (T½ = 6 hours); multiple daily dose;
mixed results w/ XR preparationLarge tablets - may be hard to swallowEffective sleep aide (high risk, high cost sleep
aide) Cataract risk
May 5, 2012PAL Conference
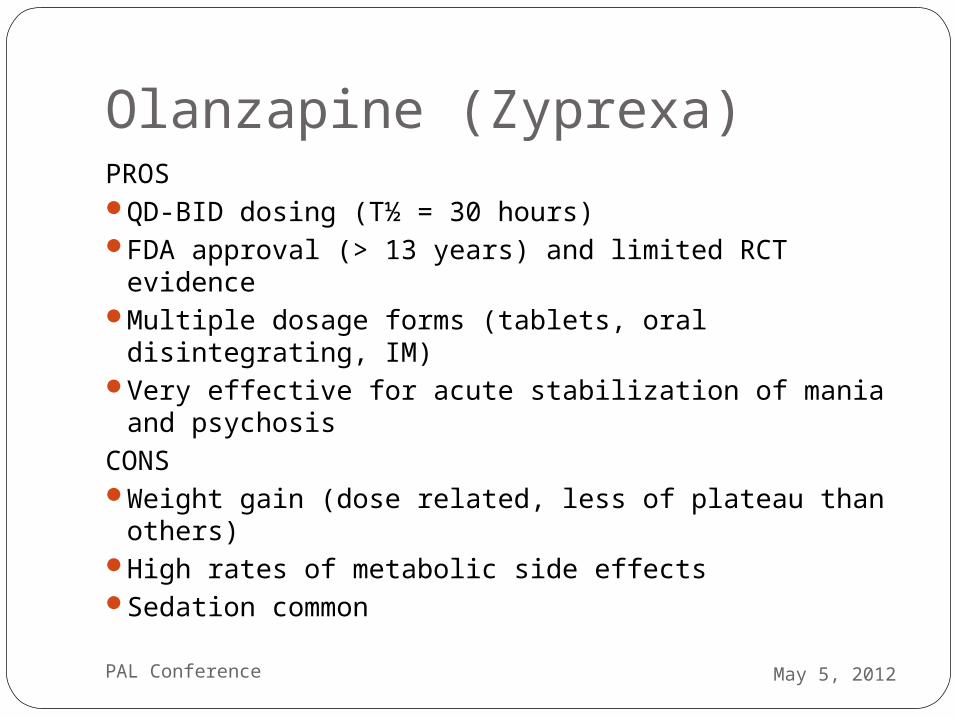
Olanzapine (Zyprexa)PROS QD-BID dosing (T½ = 30 hours)FDA approval (> 13 years) and limited RCT evidence Multiple dosage forms (tablets, oral disintegrating,
IM)Very effective for acute stabilization of mania and
psychosisCONSWeight gain (dose related, less of plateau than
others)High rates of metabolic side effectsSedation common
May 5, 2012PAL Conference
Ziprasidone (Geodon)PROSOften less sedatingMost weight neutralFewer metabolic side effects Unique receptor profile CONSBID-QID dosing (T ½ = 7 hrs)No FDA approval for pediatric maniaNo pediatric RCT support Concern for EKG changes has lowered its usage
May 5, 2012PAL Conference
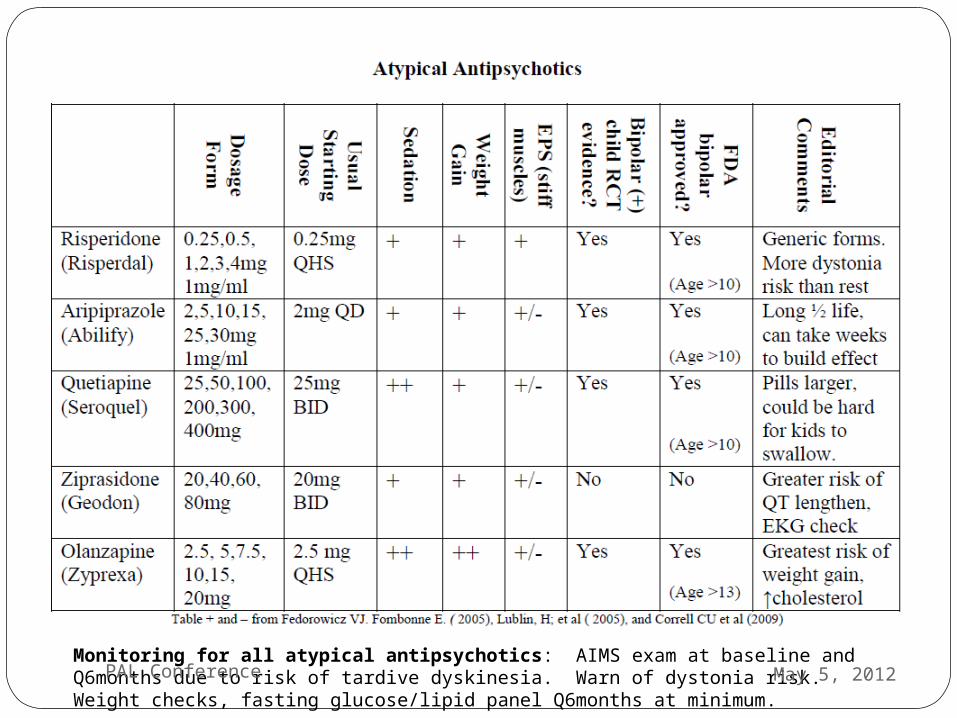
Monitoring for all atypical antipsychotics: AIMS exam at baseline and Q6months due to risk of tardive dyskinesia. Warn of dystonia risk. Weight checks, fasting glucose/lipid panel Q6months at minimum.
May 5, 2012PAL Conference
Anti-convulsantsLithium (Li), divalproex sodiumm(VPA),
carbamazepine (CBZ)14 OTs (41% response rate) 6 RCTs (40 % response rate) n = 915Only RCTs for divalproex sodiumNo RCTs for Li or CBZ
Lamotrigine, oxcarbazepine, topiramate3 OTs (43% response rate) 2 RCTs (39%)n = 244
May 5, 2012PAL Conference
LithiumPROSFDA approved for mania >12 years Some evidence in refractory depressionAnti-suicide propertiesSome EB dosing guidelines (adjust for age/GFR)CONSNarrow therapeutic index (close monitoring for toxicity w/
illness/dehydration; no NSAIDs) Usually best in combination, so committing to
polypharmacy if you start here (best w/ atypical or VPA) SE in therapeutic range similar to early toxicity (tremor,
diarrhea)SE often limit use (weight gain, acne, GI); HS dosing can
minimizeHard to predict who will respondNo evidence for maintenance treatment /slow anti-manic
effects May 5, 2012PAL Conference
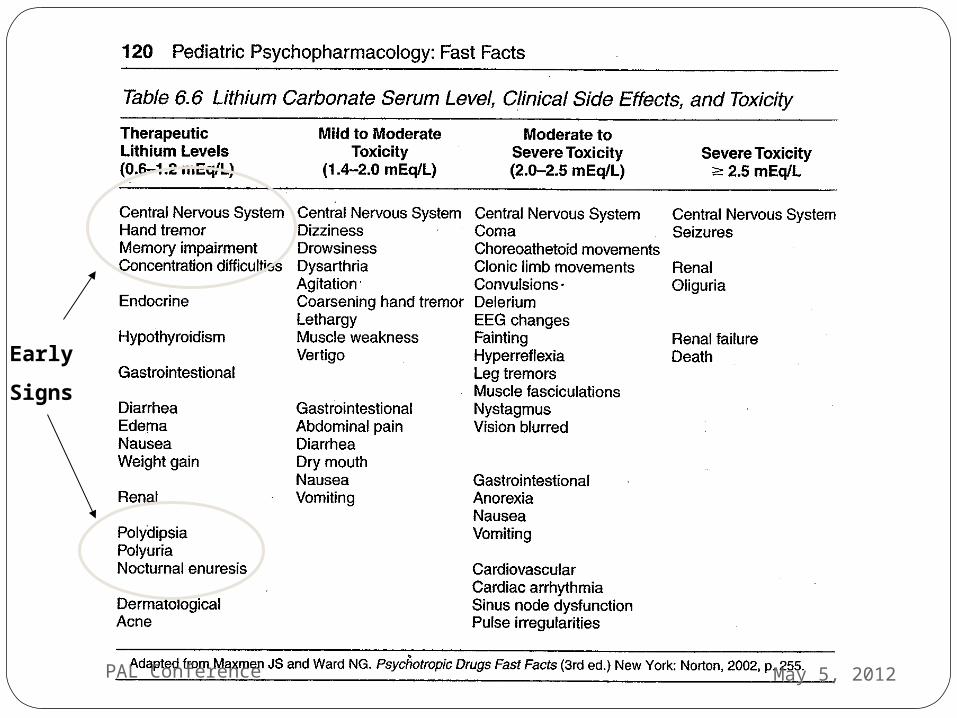
Early
Signs
May 5, 2012PAL Conference
Valproic Acid (Depakote)PROSSingle daily dosing can be effective (Depakote ER)Can be useful for maladaptive/non-specific
aggressionStudies suggest helpful, usually in combinationCONS Requires blood draws (levels, LFTs, amylase, CBC) Risk of hepatotoxicity (highest in first 6 months)High side-effect burden (weight gain, GI, tremor,
sedation, rash)Less ideal for females (risk of birth defects (NTD),
PCOS)
May 5, 2012PAL Conference
DepakoteHow well does it work?
Fair, usually works best in adolescents in combination with an antipsychotic (better than either one alone)
Some RCT’s have suggested that it works better than lithium on acute manic symptoms
Broad effects: also used for externalizing behavior disorders, conduct disorder
Lost in head-to-head trial with quetiapineSimilar long-term stabilizing effect to Lithium
after stabilization with both divalproex and lithium
DelBello MP et al, 2002, 2006Bowden C et al, 2004Rana M et al, 2005Findling, R et al 2005
May 5, 2012PAL Conference
Carbamazepine (Tegretol)PROSSome empirical supports for aggression2 OTs Similar response rates as Li and VPA (38%)
(Kowatch et al, 2005)
CONSDrug/drug interactions (OCPs, Lithium)Blood draws to check levels (auto-induced
metabolism) Weak evidence of benefit in bipolar (McClellan and
Werry, 1997)Risk of aplasia and liver failure
May 5, 2012PAL Conference
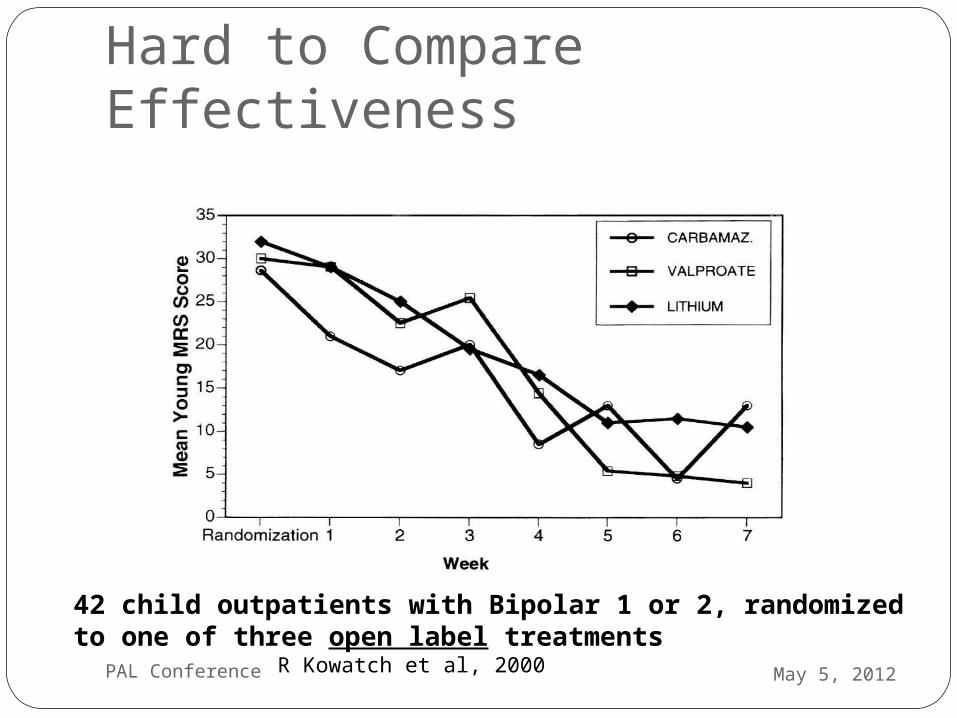
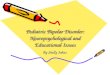
Hard to Compare Effectiveness
42 child outpatients with Bipolar 1 or 2, randomized to one of three open label treatments R Kowatch et al, 2000 May 5, 2012PAL Conference
Lamotrigine (Lamictal)PROSBipolar depression treatmentLess sedation and lower side effect profile in
general
CONSNot helpful for manic phaseRequires monitoring of CBC and liver
functionSignificant rash riskSlow titration (age >12)
May 5, 2012PAL Conference
Oxcarbazepine (Trileptal)PROSFDA approval for adults bipolar disorderWeight neutralLess risks/side effects than carbamazepineMonitoring of levels not required CONSLevels do not correlate well with efficacy or
toxicityNegative adolescent bipolar trial (Cochrane Review.
Vasudev et al. 2008)Hyponatremia not uncommon
May 5, 2012PAL Conference
Anticonvulsants Shown Not To Help In Adult Bipolar Disorder topiramate (Topamax) (1 negative
pediatric trial)gabapentin (Neurontin)levetiracetam (Keppra) - can cause
psychiatric symptomszonisamide (Zonegran)pregabalin (Lyrica)felbamate (Felbatol) - can cause
psychiatric symptomsMay 5, 2012PAL Conference
Bipolar Take-Home MessageDiagnosis of bipolar disorder made with relative
confidence in the presence of manic (Bipolar I) or hypomanic (Bipolar II) episodes. It gets tricky after that.
Mood episodes (all) involve distinct change from baseline with alternations in behavior and evidence of impairment.
Bipolar diagnosis is a serious diagnosis that has a life-long course and many management challenges.
True bipolar has high rates of morbidity and mortality. If suspected, strongly recommend involving a child
and adolescent psychiatrist .If you, as PCP, are playing central role in management,
check-in frequently to monitor side effects of medication(s) and surveillance of mood symptoms.
May 5, 2012PAL Conference
“Not-Bipolar” Take-Home MessageCurrently, there is no single diagnosis for chronically
dysregulated or irritable kids. Evidence is more suggestive of current and/or future depressive disorder.
Kids with severe, non-episodic irritability differ from those with bipolar in course, family history and performance in many cognitive tasks linked to more severe psychopathology.
Still a major role for parent support/training and mental health support. These kids can be draining and are high risk.
There can be a role for medications to decrease maladaptive aggression and affective instability.
May 5, 2012PAL Conference
At PCP level, recommend….…keeping in mind many possible causes of
mood swings and irritability. …resisting temptation to label impulsive,
difficult kids as “bipolar.”…reminding yourself and parents who are
struggling that most disruptive, irritable children do not have bipolar disorder but can still benefit from help.
…getting help with diagnostic and treatment questions as often as necessary.
May 5, 2012PAL Conference
Selected BibliographyPharmacologic Treatments for Pediatric
Bipolar Disorder: A Review and Meta-Analysis. Liu et al. JAACAP. August 2011.
Practitioner Review: The Assessment of Bipolar Disorder in Children and Adolescents. Baroni et al. JCPP. 2009.
Antipsychotic Use in Children and Adolescents:Minimizing Adverse Effects to Maximize Outcomes. Correll. JAACAP. January 2008.
May 5, 2012PAL Conference