Embed Size (px)
Citation preview

Kenneth J. Chang, MD, FACG
What To Do With Pancreatic Cysts?Pancreatic Cysts?
Kenneth J. Chang, MD, FACG
Pancreatic Cysts
• Incidence: A growing problem
•Previous diagnostic approaches
•Emerging data: the conundrum
•New problems need new psolutions
ACG Western Regional Postgraduate Course - Las Vegas, NV Copyright 2015 American College of Gastroenterology
1

Kenneth J. Chang, MD, FACG
Case scenario•• 65 65 yoyo female was found to have an female was found to have an
incidental 2.9 cm cyst in the head of the incidental 2.9 cm cyst in the head of the pancreaspancreas
Q 1: What would you do next?
1.1. Whipple resectionWhipple resectionpppp
2.2. Repeat CT in 12 monthsRepeat CT in 12 months
3.3. MRI/MRCPMRI/MRCP
4.4. ERCPERCP
5.5. EUS/FNAEUS/FNA
ACG Western Regional Postgraduate Course - Las Vegas, NV Copyright 2015 American College of Gastroenterology
2

Kenneth J. Chang, MD, FACG
Very common problem•• 300 300 consecutive autopsy casesconsecutive autopsy cases11
••186 cysts (at least 0.4 cm) in 73 cases (24.3%)186 cysts (at least 0.4 cm) in 73 cases (24.3%)186 cysts (at least 0.4 cm) in 73 cases (24.3%)186 cysts (at least 0.4 cm) in 73 cases (24.3%)
••Review of 24,039 CTs/MRIsReview of 24,039 CTs/MRIs22
•• 290 290 ptspts (1.2%) had pancreatic cysts(1.2%) had pancreatic cysts•• 168 (0.7%) w/o documentation of 168 (0.7%) w/o documentation of pancreatitispancreatitis
••Review ofReview of 2 832 MDCT2 832 MDCT33••Review of Review of 2,832 MDCT2,832 MDCT33
•• 73 73 ptspts (2.6%) had pancreatic cysts(2.6%) had pancreatic cysts•• 8.7% among elderly (age 808.7% among elderly (age 80--89)89)
1 Kimura W, et al. Int J Pancreatol 1995;18:197-206.2 Spinelli KS, et al. Ann of Surg 2004; 239: 651-6593 Laffan TA, et al. AJR 2008; 191: 802-807
Pathology ClassificationNonNon--MucinousMucinous
•• Serous NeoplasmsSerous Neoplasms~~ SerousSerous cystadenomacystadenoma
Mucinous• Mucinous cystic neoplasms
– LGD (adenoma)Serous Serous cystadenomacystadenoma•• MicrocysticMicrocystic•• MacrocysticMacrocystic•• SolidSolid•• VonVon--HippelHippel--
LandauLandau~~ Serous Serous
CystadenocarcinomaCystadenocarcinoma
( )– Moderate dysplasia (borderline)– HGD (carcinoma in situ)– Invasive carcinoma
• IPMNs– LGD (adenoma)– Moderate dysplasia (borderline)
Kloppel G SE, et al. World Health Organization classification of tumors of the digestive system. Lyon: IARC Press; 2000.
Hruban RH, et al. Tumors of the pancreas. AFIP Atlas of Tumor Pathology, 4th Series, Fascicle 6. Washington, DC: Armed Forces Institute of Pathology; 2007.
y p ( )– HGD (carcinoma in situ)– Invasive carcinoma
ACG Western Regional Postgraduate Course - Las Vegas, NV Copyright 2015 American College of Gastroenterology
3

Kenneth J. Chang, MD, FACG
Clinical Characteristics
Demographics Pseudo SCA MCN IPMN SPPT G dGender
(male:female) 1:1 1:3-4 1:9 2:1 1:10
Age (y), range 40-70 60-80 30-50 60-80 20-40
History Pancreatitis - - - -
Body/tail Body/tail HeadLocation Even Body/tail>Head
Body/tail>>Head
Head>Body/tail
Even
Katz 2008 J Am Coll Surg
Serous Cystadenoma/ Microcystic Adenoma
ACG Western Regional Postgraduate Course - Las Vegas, NV Copyright 2015 American College of Gastroenterology
4

Kenneth J. Chang, MD, FACG
Serous Cystadenoma / Oligocystic
Mucinous Cystic Neoplasm (MCN)
ACG Western Regional Postgraduate Course - Las Vegas, NV Copyright 2015 American College of Gastroenterology
5

Kenneth J. Chang, MD, FACG
MCN
Intraductal Papillary Mucinous Neoplasia (IPMN)
ACG Western Regional Postgraduate Course - Las Vegas, NV Copyright 2015 American College of Gastroenterology
6

Kenneth J. Chang, MD, FACG
IPMN – Main Duct Type
IPMN – Endoscopic View
ACG Western Regional Postgraduate Course - Las Vegas, NV Copyright 2015 American College of Gastroenterology
7

Kenneth J. Chang, MD, FACG
Tanaka et al. Pancreatology 2006
Solid Solid PseudopapillaryPseudopapillary Tumors (SPPT)Tumors (SPPT)
•• Rare neoplasms with Rare neoplasms with malignant potentialmalignant potential
•• Start as solid tumors, Start as solid tumors, undergo degeneration giving undergo degeneration giving rise to a cystic appearancerise to a cystic appearance
•• Growth rate can be dramatic Growth rate can be dramatic (>10cm)(>10cm)
•• Can arise from any part of the Can arise from any part of the pancreaspancreas
•• Predominantly young Predominantly young femalesfemales
ACG Western Regional Postgraduate Course - Las Vegas, NV Copyright 2015 American College of Gastroenterology
8

Kenneth J. Chang, MD, FACG
Solid Pseudopapillary Tumors (SPPT)•• Imaging: Imaging:
~~Range from solid to cystic, typically bothRange from solid to cystic, typically both~~WellWell marginatedmarginated~~Well Well marginatedmarginated~~Central calcificationCentral calcification~~Well vascularized with areas of hemorrhageWell vascularized with areas of hemorrhage
Solid Pseudopapillary Tumors (SPPT)•• EUSEUS--FNA:FNA:
~~Branching papillae with Branching papillae with myxoidmyxoid stromastroma~~The diagnostic accuracy of EUSThe diagnostic accuracy of EUS--FNA 75%FNA 75%**
•• Management: Management: ~~Considered low grade malignancyConsidered low grade malignancy~~Surgical resection to prevent local tumor Surgical resection to prevent local tumor
growth and distant metastases, to palliate growth and distant metastases, to palliate ttsymptomssymptoms
~~Favorable survival even in the face of Favorable survival even in the face of advanced disease (LN advanced disease (LN metsmets are rare)are rare)
*Dewitt et al. Endoscopy 2008 Mar;40(3):200-3.
ACG Western Regional Postgraduate Course - Las Vegas, NV Copyright 2015 American College of Gastroenterology
9

Kenneth J. Chang, MD, FACG
Pancreatic Cysts
• Incidence: A growing problem
•Previous diagnostic approaches
•Emerging data: the conundrum
•New problems need new psolutions
Sendai Consensus Guidelines 2004
1. Size 2. High risk features-Mural nodules-Dilated main PD (>10mm)-Positive cytology
Curr Gastroenterol Rep (2010)12:98-105
ACG Western Regional Postgraduate Course - Las Vegas, NV Copyright 2015 American College of Gastroenterology
10

Kenneth J. Chang, MD, FACG
MCN mural nodules
Updated “Sendai” Guidelines 2012
Pancreatology 2012
ACG Western Regional Postgraduate Course - Las Vegas, NV Copyright 2015 American College of Gastroenterology
11

Kenneth J. Chang, MD, FACG
EUS-FNA and Cyst Fluid Analysis of Cystic Pancreatic Lesions
LesionFluid Color
Viscosity CEA Amylase
PseudocystYellow/ brown
Thin Low High
SCN Colorless ThinLow/
UndetectedVariable
MCN ColorlessUsually
++ VariableMCN Colorlessy
thick++ Variable
MCAC Colorless Thick +++ Variable
IPMN ColorlessUsually
thick+ to +++ High
EUS-FNA of Pancreatic Cyst•• Cyst fluid CEA 192 Cyst fluid CEA 192 ngng/mL optimizes non/mL optimizes non--
MCN vs. MCNMCN vs. MCN11MCN vs. MCNMCN vs. MCN•• Cyst fluid cytology is insensitive but very Cyst fluid cytology is insensitive but very
specific for diagnosis, malignancy and specific for diagnosis, malignancy and MCN vs. nonMCN vs. non--MCNMCN22
•• Cyst fluid DNA may help differentiate Cyst fluid DNA may help differentiate li t/b i d ili t/b i d imalignant/benign and mucinous vs. nonmalignant/benign and mucinous vs. non--
mucinous cystsmucinous cysts33
1. Brugge WR. Gastroenterology 2004;126:1330-62. DeWitt J. Tech GI Endosc 2005;7:181-73. Khalid A, et al. GIE 2009;69:1095-1102
ACG Western Regional Postgraduate Course - Las Vegas, NV Copyright 2015 American College of Gastroenterology
12

Kenneth J. Chang, MD, FACG
National Coop. Panc Cyst Study
80
30
40
50
60
70
MorphologyCytologyMarker Analysis
0
10
20
% Accuracy
Brugge et al, Gastroenterology, 2004
Back to Clinical Scenario
6 months later a repeat EUS shows6 months later a repeat EUS shows6 months later, a repeat EUS shows 6 months later, a repeat EUS shows no change in size or morphology, but no change in size or morphology, but the CEA level went from 168 to 550the CEA level went from 168 to 550
ACG Western Regional Postgraduate Course - Las Vegas, NV Copyright 2015 American College of Gastroenterology
13

Kenneth J. Chang, MD, FACG
Q 2: Now what?
1. Whipple resection
2. Repeat CT in 12 months
3. MRI/MRCP in 3 months
4. ERCP
S/ 65. Repeat EUS/FNA in 6 months
Pancreatic Cysts
• Incidence: A growing problem
•Previous diagnostic approaches
•Emerging data: the conundrum
•New problems need new solutionsp
ACG Western Regional Postgraduate Course - Las Vegas, NV Copyright 2015 American College of Gastroenterology
14

Kenneth J. Chang, MD, FACG
CEA•Although may help distinguish mucinous
vs non-mucinous, does not distinguish gIPMN vs MCN.
•Not predictive of malignant progression1
•Not predictive of cyst size progression1
• Serial follow-up levels may be erattic2Serial follow up levels may be erattic
1. Othman MO. Dig Liver Dis 2012; 44:844-82. Nakai Y. ASGE abstract submission 2012
Serial CEA values in 87 patients
Nakai Y. Chang K. DDW 2012
14 pts with ≥ 3 FNA’s
ACG Western Regional Postgraduate Course - Las Vegas, NV Copyright 2015 American College of Gastroenterology
15

Kenneth J. Chang, MD, FACG
Cyst Size
•Not all small side-branch IPMN are benign, despite negative cytologydespite negative cytology
•Among 20 patients with < 3cm SB-IPMN, 6 (30%) had CIS (3) or invasive cancer (3) 1
• Cyst size > 3cm (Sendai Guideline) NOT a predictor of malignancy among 112
i l 2surgical cases2
1. Pitman MB. Pancreatology 2008:8;277-852. Genevay M. Ann Surg 2011;254:977–983
Morphology of Pancreatic Cysts by Surgical Diagnosis
Unilocular Microcystic MacrocysticCyst w/ solid componentcomponent
Pseudocyst SCA MCN MCN
Retention cyst IPMN IPMN IPMN
IPMN SCA SPT
MCNAcinar
CystadenomaPET
Pittman M. Cancer Cytopathology 2010; 118:1-13
Cystadenoma
SCA Lymphangioma Adenocarcinoma
Lymphoepithelial Metastasis
Acinar cell
ACG Western Regional Postgraduate Course - Las Vegas, NV Copyright 2015 American College of Gastroenterology
16

Kenneth J. Chang, MD, FACG
Pancreatic Cysts: Conundrum
CEA?
Imaging?
CEA?Amylase?
Cytology?
Biomarkers?SCAMCNIPMNSPPT
Size?
The answer is on the wall…
SCA
MCN
PAS+ cuboidal glycogen-staining cells
Frossard AJG 2003
MCN
ACG Western Regional Postgraduate Course - Las Vegas, NV Copyright 2015 American College of Gastroenterology
17

Kenneth J. Chang, MD, FACG
The answer is on the wall…
IPMN
Cytology
• Yield of cytology is lowU ll di i i h MCN IPMN•Usually cannot distinguish MCN vs IPMN
•May not distinguish grade of dysplasia, which also may require histology
• Cannot distinguish IPMN histologic subtype1,2
1. Furakawa T. Gut 2011; 60:509-162. Mino-Kenudson M. Gut 2011; 60:1712-1720
ACG Western Regional Postgraduate Course - Las Vegas, NV Copyright 2015 American College of Gastroenterology
18

Kenneth J. Chang, MD, FACG
Why low yield of cytology?• Cells don’t ready shed in cyst fluid; diluted
• Even for brush or biopsy – neoplastic epithelium can be heterogeneous (spotty); similar to Barrett’s
Back to Clinical Scenario
You are now fairly sure that theYou are now fairly sure that theYou are now fairly sure that the You are now fairly sure that the patient has IPMNpatient has IPMN
ACG Western Regional Postgraduate Course - Las Vegas, NV Copyright 2015 American College of Gastroenterology
19

Kenneth J. Chang, MD, FACG
Q 3: Which is most predictive of progression to cancer?
1 Male sex1. Male sex
2. Size of cyst
3. Main Duct type vs Side branch type
4. IPMN histologic subtypeg yp
5. CEA level
IPMN - 4 Histologic Types
Yamaguchi, H. Modern Pathology 2007;20, 552–561
ACG Western Regional Postgraduate Course - Las Vegas, NV Copyright 2015 American College of Gastroenterology
20

Kenneth J. Chang, MD, FACG
IPMN - 4 Histologic Types
Gastric
OncocyticOncocytic
Intestinal
Pancreatico-biliary
Furukawa Gut 2011
283 pts with IPMN
IPMN – disease specific death
Furukawa Gut 2011
ACG Western Regional Postgraduate Course - Las Vegas, NV Copyright 2015 American College of Gastroenterology
21

Kenneth J. Chang, MD, FACG
Pancreatic CystsPancreatic Cysts
• Incidence: A growing problem
•Previous diagnostic approaches
•Emerging data: the conundrum
•New problems need new solutions
EUS-nCLE(needle confocal laser endomicroscopy)
nCLE
19 G FNA
Mauna Kea Technologies AQ-Flex 19
ACG Western Regional Postgraduate Course - Las Vegas, NV Copyright 2015 American College of Gastroenterology
22

Kenneth J. Chang, MD, FACG
Pancreatic Cysts: nCLEATRAUMATICATRAUMATIC DIFFUSE SAMPLINGDIFFUSE SAMPLING
Pancreatic Cysts: nCLE
ACG Western Regional Postgraduate Course - Las Vegas, NV Copyright 2015 American College of Gastroenterology
23

Kenneth J. Chang, MD, FACG
nCLE - IPMN
nCLE - IPMN
ACG Western Regional Postgraduate Course - Las Vegas, NV Copyright 2015 American College of Gastroenterology
24

Kenneth J. Chang, MD, FACG
EUS nCLE IPMN
AGA #1204 An International, MultiAn International, Multi--Center Trial Center Trial on Needleon Needle--Based Confocal Laser Based Confocal Laser
EndomicroscopyEndomicroscopy ((nCLEnCLE): Results From the In ): Results From the In Vivo CLE Study in the Pancreas With Vivo CLE Study in the Pancreas With
EndosonographyEndosonography of Cystic Tumors of Cystic Tumors (INSPECT)(INSPECT)g p yg p y yy ( )( )VaniVani J. J. KondaKonda, , Alexander Alexander MeiningMeining, , LaithLaith H. H. JamilJamil, , Marc Marc GiovanniniGiovannini, ,
Kenneth J. Kenneth J. Chang, Chang, JooJoo Ha Ha Hwang, Hwang, Michael B. Michael B. Wallace, Wallace, UzmaUzma D. D. SiddiquiSiddiqui, , Harry R. Harry R. AslanianAslanian, , Simon K. Simon K. Lo, Lo, Michael D. Michael D. Saunders, Saunders,
John John Hart, Hart, Irving Irving WaxmanWaxman
ASGE #500 Diagnosis of Pancreatic Cysts: Diagnosis of Pancreatic Cysts: Endoscopic Ultrasound ThroughEndoscopic Ultrasound Through--thethe--NeedleNeedleEndoscopic Ultrasound, ThroughEndoscopic Ultrasound, Through thethe Needle Needle
Confocal LaserConfocal Laser--Induced Induced EndomicroscopyEndomicroscopy and and Cystoscopy Trial Cystoscopy Trial ((DETECT)DETECT)
YousukeYousuke NakaiNakai, , TakujiTakuji Iwashita, Do Hyun Park, Jason B. Iwashita, Do Hyun Park, Jason B. SamarasenaSamarasena, John G. Lee, Kenneth J. Chang , John G. Lee, Kenneth J. Chang
DDW 2012
ACG Western Regional Postgraduate Course - Las Vegas, NV Copyright 2015 American College of Gastroenterology
25

Kenneth J. Chang, MD, FACG
nCLE
• Presence of villous structures high specificity
for Mucinous Neoplasia
• But sensitivity only 59%
Konda VJ, et al. INSPECT study. Endoscopy. Dec 2013;45(12):1006-1013
Can we improve nCLE with “red flag” technology?
• EUS can only detect obvious noduleF B tt’ h d & NBI• For Barrett’s, we have endoscopy & NBI
• Why not do “cystoscopy” to guide nCLE?
ACG Western Regional Postgraduate Course - Las Vegas, NV Copyright 2015 American College of Gastroenterology
26

Kenneth J. Chang, MD, FACG
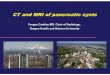
EUS-guided “through the needle” Cystoscopy
SCA MCN IPMNSmooth wallClear fluid
Smooth wallCloudy fluid
Papillary projectionsCloudy fluid
Cystoscopy
SCA
IPMNMCNNakai, Chang, et al DETECT study. GIE. 2015 (in press)
ACG Western Regional Postgraduate Course - Las Vegas, NV Copyright 2015 American College of Gastroenterology
27

Kenneth J. Chang, MD, FACG
Conclusions (1)
•• Pancreatic cysts are Pancreatic cysts are increasingly recognized increasingly recognized with routine use of crosswith routine use of cross sectional imagingsectional imagingwith routine use of crosswith routine use of cross--sectional imagingsectional imaging
•• WWide range of diagnosis: from benign to ide range of diagnosis: from benign to malignant (and everything in between)malignant (and everything in between)
•• Many have characteristic (but overMany have characteristic (but over--lapping) lapping) imagingimaging and demographicand demographic characteristicscharacteristicsimaging imaging and demographic and demographic characteristicscharacteristics
Conclusions (2)
•• Cyst fluid CEA does not appear to predict Cyst fluid CEA does not appear to predict malignant transformationmalignant transformationmalignant transformationmalignant transformation
•• Clinical decisionClinical decision--making based on cyst making based on cyst size alone is inadequatesize alone is inadequate
•• Histologic subtyping and degree of Histologic subtyping and degree of d l i i i t t f i kd l i i i t t f i k t tifi tit tifi tidysplasia is important for riskdysplasia is important for risk--stratification stratification and will require new techniques for tissue and will require new techniques for tissue sampling and/or intrasampling and/or intra--cystic imagingcystic imaging
ACG Western Regional Postgraduate Course - Las Vegas, NV Copyright 2015 American College of Gastroenterology
28

Kenneth J. Chang, MD, FACG
What To Do With Pancreatic Cysts?Pancreatic Cysts?
Kenneth J. Chang, MD, FACG
ACG Western Regional Postgraduate Course - Las Vegas, NV Copyright 2015 American College of Gastroenterology
29