Embed Size (px)
Citation preview

Childhood Accidents: an Emerging Concern
4 VOL. 45 NO. 3 2011ACTA MEDICA PHILIPPINA VOL. 43 N0. 4 200912 ACTA MEDICA PHILIPPINA
Heart Failure and Short Stature in a 43 year-old male
Katerina T. Leyritana1, Ma. Czarlota M. Acelajado-Valdenor1, Amado O. Tandoc III2 and Agnes D. Mejia1
1Department of Medicine, College of Medicine and Philippine General Hospital, University of the Philippines Manila
2Department of Pathology, College of Medicine, University of the Philippines Manila
CASE REPORT
Corresponding author: Ma. Czarlota Acelajado-Valdenor, M.D.Department of MedicinePhilippine General HospitalTaft Avenue, Manila, 1000 PhilippinesTelephone: +632 554-8488Email: [email protected]
Presentation of the caseThis is a case of a 43-year-old male presenting with short
stature and heart failure. The patient was admitted at the medicine ward of the Philippine General Hospital (PGH) for dyspnea. This paper will investigate several issues: differentiating congenital from acquired hypothyroidism, the relationship between hypothyroidism and the cardiomyopathies, and the therapeutic options in patients with cardiomyopathy secondary to hypothyroidism.
The patient had been born full term to a then 31-year-old Gravida 4 Para 3 (G4P3), the 4th of 9 siblings, with an apparently unremarkable delivery at home facilitated by a traditional birth attendant. He was noted to be normal at birth. The patient was allegedly at par with age both physically and mentally until eight years old when he was said to have stopped growing in height. He was brought to a private doctor, whose diagnosis was undisclosed, and he was given medications to increase height, which the patient took for only one month with no improvement. Through the years, the patient was apparently well, although still of short stature, with thick lips, coarse facial features and dry skin. He was notably slow in ambulation. He was said to have bronchial asthma at age 15 years, and since then he had been taking salbutamol tablets occasionally for bouts of dyspnea occurring one to two times annually.
The patient’s symptoms started in 2001 when he was reported to have sudden loss of consciousness. During this time, the patient did not have any symptoms of heart failure; no prior seizures, cyanotic episodes, chest pain, headache, or blurring of vision. He regained consciousness shortly after and was brought to a private physician, whose assessment was a “heart problem”. He was prescribed unrecalled medications taken for a few months and eventually discontinued when the syncopal episode did not recur.
In the next four years, the patient would develop intermittent, progressive exertional dyspnea and bipedal edema. Later on this would be accompanied by generalized body weakness, anorexia, and constipation, severe enough to
require regular laxative use. There was also a report of two more syncopal episodes. He was brought to another doctor in a private hospital where the assessment was still a “heart problem”. The patient was again prescribed unrecalled medications and again was lost to follow-up. This time, however, symptoms were persistent. He later consulted at another local hospital, where he was admitted and managed as a case of anemia and bronchial asthma. He was discharged slightly improved after four days, only to have recurrent heart failure symptoms, prompting admission at PGH.
Upon admission the patient was in mild respiratory distress, with stable vital signs and no note of fever. Pertinent physical exam findings included short stature, thick lips, non-pitting periorbital edema, dry skin, a displaced apical impulse, crackles on both lung fields, and bilateral non-pitting bipedal edema. There was also a 3 cm x 3 cm reducible umbilical hernia. However, there was no pallor, no neck vein distention, no apparent congenital malformations, no cardiac murmurs and no clubbing. There was also no note of an anterior neck mass.
Laboratory workup showed cardiomegaly with pulmonary congestion, thoracic dextroscoliosis, and atheromatous aorta by chest radiograph, and left ventricular hypertrophy by 12-lead electrocardiogram (12-L ECG) (Figures 1 and 2), normocytic normochromic anemia (Hgb 90 mg/dL), dyslipidemia, and pre-renal azotemia (serum creatinine 123 mmoL). Electrolytes on admission showed slight hyponatremia, hypokalemia, and hypochloremia (serum Na 136, K 3.35, Cl 86). Blood gases revealed partially compensated metabolic alkalosis with mild hypoxemia. The patient was noted to be hypothyroid based on elevated serum thyroid-stimulating hormone (TSH) and markedly decreased serum free thyroxine (FT4). The exact values are shown in Tables 1 and 2.
Upon admission to the wards, the patient was managed as having congestive heart failure from cardiomyopathy secondary to acquired hypothyroidism. Oral loop diuretics, angiotensin-converting enzyme (ACE) inhibitors, beta-blockers, statins, and levothyroxine were started. Electrolyte correction was instituted. The sections of Endocrinology and Cardiovascular Diseases were co-managing the patient together with the General Medicine service.
He soon developed respiratory failure, upon which the considerations were acute pulmonary congestion, nosocomial pneumonia, to rule out an acute coronary event. He was later
VOL. 43 N0. 4 2009 ACTA MEDICA PHILIPPINA 13
Heart Failure and Short Stature in a 43 year-old male
transferred to the intensive care unit (ICU) for ventilatory support and closer monitoring. On bedside cardiac ultrasound, there was a finding of eccentric left ventricular hypertrophy, global hypokinesia with depressed overall systolic function with concomitant spontaneous echo contrast on left ventricular (LV) cavity suggestive of rheologic stasis, the ejection fraction was 25%, with moderate mitral regurgitation, moderate aortic regurgitation with aortic sclerosis, severe tricuspid regurgitation with mild pulmonary hypertension, pulmonary regurgitation, and minimal pericardial effusion or pericardial
fat pad. Cardiac enzymes were not consistent with an acute coronary event (Table 3), however, intravenous (IV) heparin (overlapping with oral warfarin) was still given to cover for the presence of a possible LV thrombus as demonstrated by rheologic stasis on cardiac ultrasound. Medications were shifted to IV diuretics and inotropes; oral digoxin was started. IV antibiotics were given for possible pulmonary infection. The patient later on showed improvement, and was eventually weaned off from ventilatory support, extubated,
Table 1. Initial Laboratory Results
WBCRBCHGBHCTMCVMCHMCHCRDWPLTRETICSEGLYMPHMONOEOBASOBLAST
CBC
Reference Value5-104-6120-1500.38-0.4880-100 FL27-31 PG320-360 G/L11.5-15.5%200-4000.005-0.01550-70%20-44%2-9%0-4%0-2%0%
Result
4.5
900.27
Inc
48502000
RBSHGBA1CBUNCREAALBTAGHDLLDLTOTAL CHOLASTALTAlk po4NAKCLCA++PMG++
Reference Value3.9-6.14.27-6.072.6-6.453-11534-500.34-1.70.91-1.561.1-3.84.2-5.215-3730-65
140-1483.6-5.2100-1082.12-2.52
0.74-1
Result
6.36.45.0123320.820.674.215.259591184136.93.35862.372.270.83
Blood chem.
Color
TranspSp Gravity
pHSugar
ProteinRBCWBCCast
Epith cellBacteria
Mucus thCrystals
Am urates
straw
Clear1.0108.0
NEGNEG0-10-2
RareOcc’lRareRare
Urinalysis
pH
pCO2pO2
HCO3O2 satFiO2Temp
7.408
49.170
31.393.621%36.9
ABG
PBSSlight poikilocytosis, acanthocytes, ovalocytes, slight toxic granulation, slight anisocytosis
Table 2. Thyroid Function Tests
Free T4TSH
(0.8-2.0)(0.4-6.0)
0.02 ng/dL 24.75 Uiu/ml
Reference Value Result
Figure 1. Electrocardiogram upon admission
Table 3. Cardiac Enzymes
Qualitative Troponin ICK-MBCK-TOTAL
0-6.021-232
POSITIVE
1.14543
Reference Range (mmoL) Result
Figure 2. Chest radiograph on admission
VOL. 43 N0. 4 200912 ACTA MEDICA PHILIPPINA
Heart Failure and Short Stature in a 43 year-old male
Katerina T. Leyritana1, Ma. Czarlota M. Acelajado-Valdenor1, Amado O. Tandoc III2 and Agnes D. Mejia1
1Department of Medicine, College of Medicine and Philippine General Hospital, University of the Philippines Manila
2Department of Pathology, College of Medicine, University of the Philippines Manila
CASE REPORT
Corresponding author: Ma. Czarlota Acelajado-Valdenor, M.D.Department of MedicinePhilippine General HospitalTaft Avenue, Manila, 1000 PhilippinesTelephone: +632 554-8488Email: [email protected]
Presentation of the caseThis is a case of a 43-year-old male presenting with short
stature and heart failure. The patient was admitted at the medicine ward of the Philippine General Hospital (PGH) for dyspnea. This paper will investigate several issues: differentiating congenital from acquired hypothyroidism, the relationship between hypothyroidism and the cardiomyopathies, and the therapeutic options in patients with cardiomyopathy secondary to hypothyroidism.
The patient had been born full term to a then 31-year-old Gravida 4 Para 3 (G4P3), the 4th of 9 siblings, with an apparently unremarkable delivery at home facilitated by a traditional birth attendant. He was noted to be normal at birth. The patient was allegedly at par with age both physically and mentally until eight years old when he was said to have stopped growing in height. He was brought to a private doctor, whose diagnosis was undisclosed, and he was given medications to increase height, which the patient took for only one month with no improvement. Through the years, the patient was apparently well, although still of short stature, with thick lips, coarse facial features and dry skin. He was notably slow in ambulation. He was said to have bronchial asthma at age 15 years, and since then he had been taking salbutamol tablets occasionally for bouts of dyspnea occurring one to two times annually.
The patient’s symptoms started in 2001 when he was reported to have sudden loss of consciousness. During this time, the patient did not have any symptoms of heart failure; no prior seizures, cyanotic episodes, chest pain, headache, or blurring of vision. He regained consciousness shortly after and was brought to a private physician, whose assessment was a “heart problem”. He was prescribed unrecalled medications taken for a few months and eventually discontinued when the syncopal episode did not recur.
In the next four years, the patient would develop intermittent, progressive exertional dyspnea and bipedal edema. Later on this would be accompanied by generalized body weakness, anorexia, and constipation, severe enough to
require regular laxative use. There was also a report of two more syncopal episodes. He was brought to another doctor in a private hospital where the assessment was still a “heart problem”. The patient was again prescribed unrecalled medications and again was lost to follow-up. This time, however, symptoms were persistent. He later consulted at another local hospital, where he was admitted and managed as a case of anemia and bronchial asthma. He was discharged slightly improved after four days, only to have recurrent heart failure symptoms, prompting admission at PGH.
Upon admission the patient was in mild respiratory distress, with stable vital signs and no note of fever. Pertinent physical exam findings included short stature, thick lips, non-pitting periorbital edema, dry skin, a displaced apical impulse, crackles on both lung fields, and bilateral non-pitting bipedal edema. There was also a 3 cm x 3 cm reducible umbilical hernia. However, there was no pallor, no neck vein distention, no apparent congenital malformations, no cardiac murmurs and no clubbing. There was also no note of an anterior neck mass.
Laboratory workup showed cardiomegaly with pulmonary congestion, thoracic dextroscoliosis, and atheromatous aorta by chest radiograph, and left ventricular hypertrophy by 12-lead electrocardiogram (12-L ECG) (Figures 1 and 2), normocytic normochromic anemia (Hgb 90 mg/dL), dyslipidemia, and pre-renal azotemia (serum creatinine 123 mmoL). Electrolytes on admission showed slight hyponatremia, hypokalemia, and hypochloremia (serum Na 136, K 3.35, Cl 86). Blood gases revealed partially compensated metabolic alkalosis with mild hypoxemia. The patient was noted to be hypothyroid based on elevated serum thyroid-stimulating hormone (TSH) and markedly decreased serum free thyroxine (FT4). The exact values are shown in Tables 1 and 2.
Upon admission to the wards, the patient was managed as having congestive heart failure from cardiomyopathy secondary to acquired hypothyroidism. Oral loop diuretics, angiotensin-converting enzyme (ACE) inhibitors, beta-blockers, statins, and levothyroxine were started. Electrolyte correction was instituted. The sections of Endocrinology and Cardiovascular Diseases were co-managing the patient together with the General Medicine service.
He soon developed respiratory failure, upon which the considerations were acute pulmonary congestion, nosocomial pneumonia, to rule out an acute coronary event. He was later
FEATURE ARTICLE
________________
Lecture delivered during the University of the Philippines Manila Lecture Series, a pre-investiture activity in honor of Dr. Alfredo T. Ramirez, the 5th Chancellor of UP Manila last March 8-29, 2000 at the UP Manila College of Nursing Auditorium. Article reprinted with permission from UP Manila Journal, July-Sept 2000; 5(3):38-48. Corresponding Author: Ramon L. Arcadio, MD, MHPEd, DrHum Office of the Chancellor Philippine General Hospital University of the Philippines Manila Taft Avenue, Ermita, Manila 1000 Philippines Telephone: +632 5210184/+632 5268419/+632 3022215 Fax No:+632 5210184 Email: [email protected]
Childhood Accidents: an Emerging Concern
Ramon L. Arcadio
Department of Pediatrics, College of Medicine and Philippine General Hospital, University of the Philippines Manila
Introduction The study of childhood injuries and injury prevention is
merging as a legitimate field of clinical practice and research in pediatrics and community health. With the significant decrease in infant and child mortality due to communicable disease and malnutrition, deaths due to injuries are gaining prominence. In industrialized countries, injuries are the chief causes of death in children between ages of 1 and 15. In the Philippines, the number of fatal injuries is still high although deaths from injuries are lost among other causes, like infections, which are statistically more numerous. In terms of serious disability, medical costs, and morbidity, the total impact of childhood injuries, is enormous.
A number of definitions have been suggested to cover the concept of an accident or injury. The term “accident” has been abandoned in favor of the more accurate term “injury”. This represents a change of attitude from the idea of accidents as random, chance, uncontrollable events to the recognition of injuries as describable epidemiologic conditions that can be controlled and prevented. The use of the term “accident” implies unpredictability. However, the reality is that injuries are no more likely to occur by chance than are diseases. The nature of injury, just like a disease varies with age, sex, and a number of other factors. Not every child has the same probability of being injured therefore, injuries are not random events. As the experts succinctly state, “an injury is not accident.”
The World Health Organization (WHO) defines an accident as an event which is independent of human willpower, caused by an external force, acts rapidly, and results in bodily or mental damage.
Haddon defines injury as any damage caused by a transfer of energy (chemical, mechanical, thermal, electrical or radiation) from a hazardous agent to a susceptible host in a conducive environment (physical and social).
The use of the term “injury” allows separation of the event (accident) from its consequences (injuries) and advocates the application of a scientific approach to the injury epidemic; the most important aspect is PRIMARY PREVENTION. These are the programs and strategies to be implemented before any accident ever happens. SECONDARY PREVENTION are the strategies in order to minimize the severity of the resulting injuries.
The Philippine Health Statistics (PHS, 1992) ranks injuries as the fifth among the ten leading causes of morbidity and sixth among the ten leading causes of

VOL. 43 N0. 4 200912 ACTA MEDICA PHILIPPINA
Heart Failure and Short Stature in a 43 year-old male
Katerina T. Leyritana1, Ma. Czarlota M. Acelajado-Valdenor1, Amado O. Tandoc III2 and Agnes D. Mejia1
1Department of Medicine, College of Medicine and Philippine General Hospital, University of the Philippines Manila
2Department of Pathology, College of Medicine, University of the Philippines Manila
CASE REPORT
Corresponding author: Ma. Czarlota Acelajado-Valdenor, M.D.Department of MedicinePhilippine General HospitalTaft Avenue, Manila, 1000 PhilippinesTelephone: +632 554-8488Email: [email protected]
Presentation of the caseThis is a case of a 43-year-old male presenting with short
stature and heart failure. The patient was admitted at the medicine ward of the Philippine General Hospital (PGH) for dyspnea. This paper will investigate several issues: differentiating congenital from acquired hypothyroidism, the relationship between hypothyroidism and the cardiomyopathies, and the therapeutic options in patients with cardiomyopathy secondary to hypothyroidism.
The patient had been born full term to a then 31-year-old Gravida 4 Para 3 (G4P3), the 4th of 9 siblings, with an apparently unremarkable delivery at home facilitated by a traditional birth attendant. He was noted to be normal at birth. The patient was allegedly at par with age both physically and mentally until eight years old when he was said to have stopped growing in height. He was brought to a private doctor, whose diagnosis was undisclosed, and he was given medications to increase height, which the patient took for only one month with no improvement. Through the years, the patient was apparently well, although still of short stature, with thick lips, coarse facial features and dry skin. He was notably slow in ambulation. He was said to have bronchial asthma at age 15 years, and since then he had been taking salbutamol tablets occasionally for bouts of dyspnea occurring one to two times annually.
The patient’s symptoms started in 2001 when he was reported to have sudden loss of consciousness. During this time, the patient did not have any symptoms of heart failure; no prior seizures, cyanotic episodes, chest pain, headache, or blurring of vision. He regained consciousness shortly after and was brought to a private physician, whose assessment was a “heart problem”. He was prescribed unrecalled medications taken for a few months and eventually discontinued when the syncopal episode did not recur.
In the next four years, the patient would develop intermittent, progressive exertional dyspnea and bipedal edema. Later on this would be accompanied by generalized body weakness, anorexia, and constipation, severe enough to
require regular laxative use. There was also a report of two more syncopal episodes. He was brought to another doctor in a private hospital where the assessment was still a “heart problem”. The patient was again prescribed unrecalled medications and again was lost to follow-up. This time, however, symptoms were persistent. He later consulted at another local hospital, where he was admitted and managed as a case of anemia and bronchial asthma. He was discharged slightly improved after four days, only to have recurrent heart failure symptoms, prompting admission at PGH.
Upon admission the patient was in mild respiratory distress, with stable vital signs and no note of fever. Pertinent physical exam findings included short stature, thick lips, non-pitting periorbital edema, dry skin, a displaced apical impulse, crackles on both lung fields, and bilateral non-pitting bipedal edema. There was also a 3 cm x 3 cm reducible umbilical hernia. However, there was no pallor, no neck vein distention, no apparent congenital malformations, no cardiac murmurs and no clubbing. There was also no note of an anterior neck mass.
Laboratory workup showed cardiomegaly with pulmonary congestion, thoracic dextroscoliosis, and atheromatous aorta by chest radiograph, and left ventricular hypertrophy by 12-lead electrocardiogram (12-L ECG) (Figures 1 and 2), normocytic normochromic anemia (Hgb 90 mg/dL), dyslipidemia, and pre-renal azotemia (serum creatinine 123 mmoL). Electrolytes on admission showed slight hyponatremia, hypokalemia, and hypochloremia (serum Na 136, K 3.35, Cl 86). Blood gases revealed partially compensated metabolic alkalosis with mild hypoxemia. The patient was noted to be hypothyroid based on elevated serum thyroid-stimulating hormone (TSH) and markedly decreased serum free thyroxine (FT4). The exact values are shown in Tables 1 and 2.
Upon admission to the wards, the patient was managed as having congestive heart failure from cardiomyopathy secondary to acquired hypothyroidism. Oral loop diuretics, angiotensin-converting enzyme (ACE) inhibitors, beta-blockers, statins, and levothyroxine were started. Electrolyte correction was instituted. The sections of Endocrinology and Cardiovascular Diseases were co-managing the patient together with the General Medicine service.
He soon developed respiratory failure, upon which the considerations were acute pulmonary congestion, nosocomial pneumonia, to rule out an acute coronary event. He was later
Childhood Accidents: an Emerging Concern
5VOL. 45 NO. 3 2011 ACTA MEDICA PHILIPPINAVOL. 43 N0. 4 2009 ACTA MEDICA PHILIPPINA 13
Heart Failure and Short Stature in a 43 year-old male
transferred to the intensive care unit (ICU) for ventilatory support and closer monitoring. On bedside cardiac ultrasound, there was a finding of eccentric left ventricular hypertrophy, global hypokinesia with depressed overall systolic function with concomitant spontaneous echo contrast on left ventricular (LV) cavity suggestive of rheologic stasis, the ejection fraction was 25%, with moderate mitral regurgitation, moderate aortic regurgitation with aortic sclerosis, severe tricuspid regurgitation with mild pulmonary hypertension, pulmonary regurgitation, and minimal pericardial effusion or pericardial
fat pad. Cardiac enzymes were not consistent with an acute coronary event (Table 3), however, intravenous (IV) heparin (overlapping with oral warfarin) was still given to cover for the presence of a possible LV thrombus as demonstrated by rheologic stasis on cardiac ultrasound. Medications were shifted to IV diuretics and inotropes; oral digoxin was started. IV antibiotics were given for possible pulmonary infection. The patient later on showed improvement, and was eventually weaned off from ventilatory support, extubated,
Table 1. Initial Laboratory Results
WBCRBCHGBHCTMCVMCHMCHCRDWPLTRETICSEGLYMPHMONOEOBASOBLAST
CBC
Reference Value5-104-6120-1500.38-0.4880-100 FL27-31 PG320-360 G/L11.5-15.5%200-4000.005-0.01550-70%20-44%2-9%0-4%0-2%0%
Result
4.5
900.27
Inc
48502000
RBSHGBA1CBUNCREAALBTAGHDLLDLTOTAL CHOLASTALTAlk po4NAKCLCA++PMG++
Reference Value3.9-6.14.27-6.072.6-6.453-11534-500.34-1.70.91-1.561.1-3.84.2-5.215-3730-65
140-1483.6-5.2100-1082.12-2.52
0.74-1
Result
6.36.45.0123320.820.674.215.259591184136.93.35862.372.270.83
Blood chem.
Color
TranspSp Gravity
pHSugar
ProteinRBCWBCCast
Epith cellBacteria
Mucus thCrystals
Am urates
straw
Clear1.010
8.0NEGNEG0-10-2
RareOcc’lRareRare
Urinalysis
pH
pCO2pO2
HCO3O2 satFiO2Temp
7.408
49.170
31.393.621%36.9
ABG
PBSSlight poikilocytosis, acanthocytes, ovalocytes, slight toxic granulation, slight anisocytosis
Table 2. Thyroid Function Tests
Free T4TSH
(0.8-2.0)(0.4-6.0)
0.02 ng/dL 24.75 Uiu/ml
Reference Value Result
Figure 1. Electrocardiogram upon admission
Table 3. Cardiac Enzymes
Qualitative Troponin ICK-MBCK-TOTAL
0-6.021-232
POSITIVE
1.14543
Reference Range (mmoL) Result
Figure 2. Chest radiograph on admission
VOL. 43 N0. 4 200912 ACTA MEDICA PHILIPPINA
Heart Failure and Short Stature in a 43 year-old male
Katerina T. Leyritana1, Ma. Czarlota M. Acelajado-Valdenor1, Amado O. Tandoc III2 and Agnes D. Mejia1
1Department of Medicine, College of Medicine and Philippine General Hospital, University of the Philippines Manila
2Department of Pathology, College of Medicine, University of the Philippines Manila
CASE REPORT
Corresponding author: Ma. Czarlota Acelajado-Valdenor, M.D.Department of MedicinePhilippine General HospitalTaft Avenue, Manila, 1000 PhilippinesTelephone: +632 554-8488Email: [email protected]
Presentation of the caseThis is a case of a 43-year-old male presenting with short
stature and heart failure. The patient was admitted at the medicine ward of the Philippine General Hospital (PGH) for dyspnea. This paper will investigate several issues: differentiating congenital from acquired hypothyroidism, the relationship between hypothyroidism and the cardiomyopathies, and the therapeutic options in patients with cardiomyopathy secondary to hypothyroidism.
The patient had been born full term to a then 31-year-old Gravida 4 Para 3 (G4P3), the 4th of 9 siblings, with an apparently unremarkable delivery at home facilitated by a traditional birth attendant. He was noted to be normal at birth. The patient was allegedly at par with age both physically and mentally until eight years old when he was said to have stopped growing in height. He was brought to a private doctor, whose diagnosis was undisclosed, and he was given medications to increase height, which the patient took for only one month with no improvement. Through the years, the patient was apparently well, although still of short stature, with thick lips, coarse facial features and dry skin. He was notably slow in ambulation. He was said to have bronchial asthma at age 15 years, and since then he had been taking salbutamol tablets occasionally for bouts of dyspnea occurring one to two times annually.
The patient’s symptoms started in 2001 when he was reported to have sudden loss of consciousness. During this time, the patient did not have any symptoms of heart failure; no prior seizures, cyanotic episodes, chest pain, headache, or blurring of vision. He regained consciousness shortly after and was brought to a private physician, whose assessment was a “heart problem”. He was prescribed unrecalled medications taken for a few months and eventually discontinued when the syncopal episode did not recur.
In the next four years, the patient would develop intermittent, progressive exertional dyspnea and bipedal edema. Later on this would be accompanied by generalized body weakness, anorexia, and constipation, severe enough to
require regular laxative use. There was also a report of two more syncopal episodes. He was brought to another doctor in a private hospital where the assessment was still a “heart problem”. The patient was again prescribed unrecalled medications and again was lost to follow-up. This time, however, symptoms were persistent. He later consulted at another local hospital, where he was admitted and managed as a case of anemia and bronchial asthma. He was discharged slightly improved after four days, only to have recurrent heart failure symptoms, prompting admission at PGH.
Upon admission the patient was in mild respiratory distress, with stable vital signs and no note of fever. Pertinent physical exam findings included short stature, thick lips, non-pitting periorbital edema, dry skin, a displaced apical impulse, crackles on both lung fields, and bilateral non-pitting bipedal edema. There was also a 3 cm x 3 cm reducible umbilical hernia. However, there was no pallor, no neck vein distention, no apparent congenital malformations, no cardiac murmurs and no clubbing. There was also no note of an anterior neck mass.
Laboratory workup showed cardiomegaly with pulmonary congestion, thoracic dextroscoliosis, and atheromatous aorta by chest radiograph, and left ventricular hypertrophy by 12-lead electrocardiogram (12-L ECG) (Figures 1 and 2), normocytic normochromic anemia (Hgb 90 mg/dL), dyslipidemia, and pre-renal azotemia (serum creatinine 123 mmoL). Electrolytes on admission showed slight hyponatremia, hypokalemia, and hypochloremia (serum Na 136, K 3.35, Cl 86). Blood gases revealed partially compensated metabolic alkalosis with mild hypoxemia. The patient was noted to be hypothyroid based on elevated serum thyroid-stimulating hormone (TSH) and markedly decreased serum free thyroxine (FT4). The exact values are shown in Tables 1 and 2.
Upon admission to the wards, the patient was managed as having congestive heart failure from cardiomyopathy secondary to acquired hypothyroidism. Oral loop diuretics, angiotensin-converting enzyme (ACE) inhibitors, beta-blockers, statins, and levothyroxine were started. Electrolyte correction was instituted. The sections of Endocrinology and Cardiovascular Diseases were co-managing the patient together with the General Medicine service.
He soon developed respiratory failure, upon which the considerations were acute pulmonary congestion, nosocomial pneumonia, to rule out an acute coronary event. He was later
mortality in the general population (Figures 1 and 2). This rank represents a five-year average from 1987 to 1991. Of those who died, only about 35% (1990) were attended by a health worker.
Figure 1. Morbidity: Ten Leading Causes Rate per 100,000 Population, Philippines, 1993
Figure 2. Mortality: Ten Leading Causes Rate per 100,000 Population, Philippines, 1993
In our own survey, as well as, in the date of the Philippine Health Statistics (1992), the leading causes of injuries are traffic accidents, submersion injury or drowning and near drowning, falls, burns, poisoning. Most injuries with children occur at home and in school.
The patterns of injury vary in different cultures, economies, and climates. In most of Asia, just like the Philippines, the leading causes of injuries are vehicular or traffic accidents and drowning.
Mortality statistics are not the best measure of the grave consequences of childhood injuries. An alternate parameter is the number of working years of life lost, calculated on the basis of life expectancy. This parameter brings out more clearly the gravity of injuries which occur primarily in childhood and take a high toll of young and potentially productive lives. As shown in Figure 3, injury is the primary cause of the loss of more years of life than all forms of cancer and heart disease combined. Only AIDS is now beginning to compete with accident and violence as a cause of death in these age groups.
Morbidity statistics locally are less adequate than the mortality data. Not very much is known about the number
and the consequences of accidents that are not fatal. However, various epidemiological studies make it possible to state the following: for one fatal injury there are between 200 to 900 nonfatal injuries leading to about 10 hospitalizations: between one and four handicaps with permanent invalidity resulting from these accidents. Other studies have shown that every year between 6% and 10% of all children consult a doctor as a result of an injury. A study done a few years ago indicate that almost 40% of children suffer an injury each year that results in medical consultation or at least one restricted activity per day like absence from school or staying in bed.
Figure 3. Percentage years of potential life lost to injury, cancer, diseases, and other diseases before age 65. Table 1. Injury Priorities in Asia
COUNTRY MAJOR CAUSES HONG KONG Transport Homicide, other violence Suicide TAIWAN Traffic Burns Falls Foreign body in airway MALAYSIA Transport Burns Poisoning SINGAPORE Traffic Drowning Falls, Head Injuries Hanging, Strangulation Burns Poisoning INDONESIA Traffic Accident Falls Poisoning Drowning Work-related Injuries THAILAND Drowning Burns Transport Falls Intoxication Animal Bites (snakes, dogs)
(Source: 9th Asian Congress of Pediatrics, Hong Kong, March 1997)

Childhood Accidents: an Emerging Concern
6 VOL. 45 NO. 3 2011ACTA MEDICA PHILIPPINA VOL. 43 N0. 4 200912 ACTA MEDICA PHILIPPINA
Heart Failure and Short Stature in a 43 year-old male
Katerina T. Leyritana1, Ma. Czarlota M. Acelajado-Valdenor1, Amado O. Tandoc III2 and Agnes D. Mejia1
1Department of Medicine, College of Medicine and Philippine General Hospital, University of the Philippines Manila
2Department of Pathology, College of Medicine, University of the Philippines Manila
CASE REPORT
Corresponding author: Ma. Czarlota Acelajado-Valdenor, M.D.Department of MedicinePhilippine General HospitalTaft Avenue, Manila, 1000 PhilippinesTelephone: +632 554-8488Email: [email protected]
Presentation of the caseThis is a case of a 43-year-old male presenting with short
stature and heart failure. The patient was admitted at the medicine ward of the Philippine General Hospital (PGH) for dyspnea. This paper will investigate several issues: differentiating congenital from acquired hypothyroidism, the relationship between hypothyroidism and the cardiomyopathies, and the therapeutic options in patients with cardiomyopathy secondary to hypothyroidism.
The patient had been born full term to a then 31-year-old Gravida 4 Para 3 (G4P3), the 4th of 9 siblings, with an apparently unremarkable delivery at home facilitated by a traditional birth attendant. He was noted to be normal at birth. The patient was allegedly at par with age both physically and mentally until eight years old when he was said to have stopped growing in height. He was brought to a private doctor, whose diagnosis was undisclosed, and he was given medications to increase height, which the patient took for only one month with no improvement. Through the years, the patient was apparently well, although still of short stature, with thick lips, coarse facial features and dry skin. He was notably slow in ambulation. He was said to have bronchial asthma at age 15 years, and since then he had been taking salbutamol tablets occasionally for bouts of dyspnea occurring one to two times annually.
The patient’s symptoms started in 2001 when he was reported to have sudden loss of consciousness. During this time, the patient did not have any symptoms of heart failure; no prior seizures, cyanotic episodes, chest pain, headache, or blurring of vision. He regained consciousness shortly after and was brought to a private physician, whose assessment was a “heart problem”. He was prescribed unrecalled medications taken for a few months and eventually discontinued when the syncopal episode did not recur.
In the next four years, the patient would develop intermittent, progressive exertional dyspnea and bipedal edema. Later on this would be accompanied by generalized body weakness, anorexia, and constipation, severe enough to
require regular laxative use. There was also a report of two more syncopal episodes. He was brought to another doctor in a private hospital where the assessment was still a “heart problem”. The patient was again prescribed unrecalled medications and again was lost to follow-up. This time, however, symptoms were persistent. He later consulted at another local hospital, where he was admitted and managed as a case of anemia and bronchial asthma. He was discharged slightly improved after four days, only to have recurrent heart failure symptoms, prompting admission at PGH.
Upon admission the patient was in mild respiratory distress, with stable vital signs and no note of fever. Pertinent physical exam findings included short stature, thick lips, non-pitting periorbital edema, dry skin, a displaced apical impulse, crackles on both lung fields, and bilateral non-pitting bipedal edema. There was also a 3 cm x 3 cm reducible umbilical hernia. However, there was no pallor, no neck vein distention, no apparent congenital malformations, no cardiac murmurs and no clubbing. There was also no note of an anterior neck mass.
Laboratory workup showed cardiomegaly with pulmonary congestion, thoracic dextroscoliosis, and atheromatous aorta by chest radiograph, and left ventricular hypertrophy by 12-lead electrocardiogram (12-L ECG) (Figures 1 and 2), normocytic normochromic anemia (Hgb 90 mg/dL), dyslipidemia, and pre-renal azotemia (serum creatinine 123 mmoL). Electrolytes on admission showed slight hyponatremia, hypokalemia, and hypochloremia (serum Na 136, K 3.35, Cl 86). Blood gases revealed partially compensated metabolic alkalosis with mild hypoxemia. The patient was noted to be hypothyroid based on elevated serum thyroid-stimulating hormone (TSH) and markedly decreased serum free thyroxine (FT4). The exact values are shown in Tables 1 and 2.
Upon admission to the wards, the patient was managed as having congestive heart failure from cardiomyopathy secondary to acquired hypothyroidism. Oral loop diuretics, angiotensin-converting enzyme (ACE) inhibitors, beta-blockers, statins, and levothyroxine were started. Electrolyte correction was instituted. The sections of Endocrinology and Cardiovascular Diseases were co-managing the patient together with the General Medicine service.
He soon developed respiratory failure, upon which the considerations were acute pulmonary congestion, nosocomial pneumonia, to rule out an acute coronary event. He was later
VOL. 43 N0. 4 2009 ACTA MEDICA PHILIPPINA 13
Heart Failure and Short Stature in a 43 year-old male
transferred to the intensive care unit (ICU) for ventilatory support and closer monitoring. On bedside cardiac ultrasound, there was a finding of eccentric left ventricular hypertrophy, global hypokinesia with depressed overall systolic function with concomitant spontaneous echo contrast on left ventricular (LV) cavity suggestive of rheologic stasis, the ejection fraction was 25%, with moderate mitral regurgitation, moderate aortic regurgitation with aortic sclerosis, severe tricuspid regurgitation with mild pulmonary hypertension, pulmonary regurgitation, and minimal pericardial effusion or pericardial
fat pad. Cardiac enzymes were not consistent with an acute coronary event (Table 3), however, intravenous (IV) heparin (overlapping with oral warfarin) was still given to cover for the presence of a possible LV thrombus as demonstrated by rheologic stasis on cardiac ultrasound. Medications were shifted to IV diuretics and inotropes; oral digoxin was started. IV antibiotics were given for possible pulmonary infection. The patient later on showed improvement, and was eventually weaned off from ventilatory support, extubated,
Table 1. Initial Laboratory Results
WBCRBCHGBHCTMCVMCHMCHCRDWPLTRETICSEGLYMPHMONOEOBASOBLAST
CBC
Reference Value5-104-6120-1500.38-0.4880-100 FL27-31 PG320-360 G/L11.5-15.5%200-4000.005-0.01550-70%20-44%2-9%0-4%0-2%0%
Result
4.5
900.27
Inc
48502000
RBSHGBA1CBUNCREAALBTAGHDLLDLTOTAL CHOLASTALTAlk po4NAKCLCA++PMG++
Reference Value3.9-6.14.27-6.072.6-6.453-11534-500.34-1.70.91-1.561.1-3.84.2-5.215-3730-65
140-1483.6-5.2100-1082.12-2.52
0.74-1
Result
6.36.45.0123320.820.674.215.259591184136.93.35862.372.270.83
Blood chem.
Color
TranspSp Gravity
pHSugar
ProteinRBCWBCCast
Epith cellBacteria
Mucus thCrystals
Am urates
straw
Clear1.0108.0
NEGNEG0-10-2
RareOcc’lRareRare
Urinalysis
pH
pCO2pO2
HCO3O2 satFiO2Temp
7.408
49.170
31.393.621%36.9
ABG
PBSSlight poikilocytosis, acanthocytes, ovalocytes, slight toxic granulation, slight anisocytosis
Table 2. Thyroid Function Tests
Free T4TSH
(0.8-2.0)(0.4-6.0)
0.02 ng/dL 24.75 Uiu/ml
Reference Value Result
Figure 1. Electrocardiogram upon admission
Table 3. Cardiac Enzymes
Qualitative Troponin ICK-MBCK-TOTAL
0-6.021-232
POSITIVE
1.14543
Reference Range (mmoL) Result
Figure 2. Chest radiograph on admission
In the local studies that we did, the following were the epidemiological features noted:
The types of childhood injuries have a relationship with the child’s age and development. Younger children get injured at home, whereas children get injured outside the home – on the way to school or in the school campus.
The data shows a predominance of males over females in the number of childhood injuries.
More injuries occurred during the daytime (7:00a.m. to 6:00p.m.) when children are most active and at play either at home, in school, or even on the streets.
There were more injuries among children of families in the low income group and in those undergoing stress like parental separation or parental illness.
Increasing urbanization was associated with an increase in traffic injuries. Good roads lead to over speeding and vehicular injuries.
In most injuries at home and in schools, fall and burns were the most common types of accidents in these settings. The common resulting injuries were lacerations, contusions, and abrasions.
Kerosene and isoniazid were the leading causes of accidental poisoning.
Physical abuse was common among male adolescents who were usually involved in teen-age fights or rumbles. Female child abuse was usually family-related molestation.
Drowning usually involved a daring and curious male child, less than 10 years old. The high incidence of drowning cases is related to the long coastline of the country’s 7,100 islands.
Cases of bites were mostly caused by dogs. Filipino families love to keep dogs as their pets. There is no good local data on snake bites, a major problem in other Asian countries.
Prevention of accidents requires a good knowledge of
their “natural history.” The interactive model of agent-host-environment has long been used to described the epidemiology of communicable diseases and can be adopted for understanding childhood injuries as illustrated in Figure 4.
Any accident involves the following: the person who has the accident, in this case, a child or adolescent; the physical or human environment in which the person lives; and the agent of the accident itself.
Since a child is concerned, he or she has neither the experience nor the psychomotor and sensory capacity of an adult. He is thus more vulnerable.
Figure 4. Epidemiologic Framework: The Agent-Host Environmental Model
The human environment obviously plays an important
role. The fact that the child is under the supervision of an adult does not always prevent accidents. More than half of the accidents happen in the presence of an adult, perhaps in a moment of absent-mindedness, or simply because the adult did not imagine that the situation posed any danger for the child. The physical environment includes not only the physical situation, like vehicles, staircases, or scalding hot tap water, but also the psychosocial one. Serious stresses within the family, like a parent in the hospital, may create an environment in which a child is more likely to be injured.
The agent of the injury is the form of energy that damages body issues. For example, in a flame burn, the thermal energy damages cells, tissues, and blood vessels. In many poisonings, a chemical reaction interrupts the body’s ongoing metabolic processes.
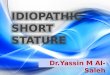
A developmental approach that emphasizes that children have different cognitive, perceptual, motor, and language competencies can provide a better understanding of the child’s contributions to the occurrence of injuries. This approach characterizes the child in terms of the “how”, “why”, and “what” of this behavior. The “how” of children’s behavior reflects the child’s behavioral style or temperament. The “why” reflects the child’s motivations to accomplish certain tasks. The “what” of behavior involves what children are capable of doing, their competencies at different ages.
Temperament is defined as the child’s behavioral style when interacting with the environment. It describes how a child behaves rather than what he/she can do or why he/she does it. Thus a child can be classified as a difficult child, easy child, or a slow to warm up child. Motivation reflects the child’s interest in accomplishing a task. The first aspect of motivation is the normal drive for autonomy. The children want to do things whether they are physically able to or not.

VOL. 43 N0. 4 200912 ACTA MEDICA PHILIPPINA
Heart Failure and Short Stature in a 43 year-old male
Katerina T. Leyritana1, Ma. Czarlota M. Acelajado-Valdenor1, Amado O. Tandoc III2 and Agnes D. Mejia1
1Department of Medicine, College of Medicine and Philippine General Hospital, University of the Philippines Manila
2Department of Pathology, College of Medicine, University of the Philippines Manila
CASE REPORT
Corresponding author: Ma. Czarlota Acelajado-Valdenor, M.D.Department of MedicinePhilippine General HospitalTaft Avenue, Manila, 1000 PhilippinesTelephone: +632 554-8488Email: [email protected]
Presentation of the caseThis is a case of a 43-year-old male presenting with short
stature and heart failure. The patient was admitted at the medicine ward of the Philippine General Hospital (PGH) for dyspnea. This paper will investigate several issues: differentiating congenital from acquired hypothyroidism, the relationship between hypothyroidism and the cardiomyopathies, and the therapeutic options in patients with cardiomyopathy secondary to hypothyroidism.
The patient had been born full term to a then 31-year-old Gravida 4 Para 3 (G4P3), the 4th of 9 siblings, with an apparently unremarkable delivery at home facilitated by a traditional birth attendant. He was noted to be normal at birth. The patient was allegedly at par with age both physically and mentally until eight years old when he was said to have stopped growing in height. He was brought to a private doctor, whose diagnosis was undisclosed, and he was given medications to increase height, which the patient took for only one month with no improvement. Through the years, the patient was apparently well, although still of short stature, with thick lips, coarse facial features and dry skin. He was notably slow in ambulation. He was said to have bronchial asthma at age 15 years, and since then he had been taking salbutamol tablets occasionally for bouts of dyspnea occurring one to two times annually.
The patient’s symptoms started in 2001 when he was reported to have sudden loss of consciousness. During this time, the patient did not have any symptoms of heart failure; no prior seizures, cyanotic episodes, chest pain, headache, or blurring of vision. He regained consciousness shortly after and was brought to a private physician, whose assessment was a “heart problem”. He was prescribed unrecalled medications taken for a few months and eventually discontinued when the syncopal episode did not recur.
In the next four years, the patient would develop intermittent, progressive exertional dyspnea and bipedal edema. Later on this would be accompanied by generalized body weakness, anorexia, and constipation, severe enough to
require regular laxative use. There was also a report of two more syncopal episodes. He was brought to another doctor in a private hospital where the assessment was still a “heart problem”. The patient was again prescribed unrecalled medications and again was lost to follow-up. This time, however, symptoms were persistent. He later consulted at another local hospital, where he was admitted and managed as a case of anemia and bronchial asthma. He was discharged slightly improved after four days, only to have recurrent heart failure symptoms, prompting admission at PGH.
Upon admission the patient was in mild respiratory distress, with stable vital signs and no note of fever. Pertinent physical exam findings included short stature, thick lips, non-pitting periorbital edema, dry skin, a displaced apical impulse, crackles on both lung fields, and bilateral non-pitting bipedal edema. There was also a 3 cm x 3 cm reducible umbilical hernia. However, there was no pallor, no neck vein distention, no apparent congenital malformations, no cardiac murmurs and no clubbing. There was also no note of an anterior neck mass.
Laboratory workup showed cardiomegaly with pulmonary congestion, thoracic dextroscoliosis, and atheromatous aorta by chest radiograph, and left ventricular hypertrophy by 12-lead electrocardiogram (12-L ECG) (Figures 1 and 2), normocytic normochromic anemia (Hgb 90 mg/dL), dyslipidemia, and pre-renal azotemia (serum creatinine 123 mmoL). Electrolytes on admission showed slight hyponatremia, hypokalemia, and hypochloremia (serum Na 136, K 3.35, Cl 86). Blood gases revealed partially compensated metabolic alkalosis with mild hypoxemia. The patient was noted to be hypothyroid based on elevated serum thyroid-stimulating hormone (TSH) and markedly decreased serum free thyroxine (FT4). The exact values are shown in Tables 1 and 2.
Upon admission to the wards, the patient was managed as having congestive heart failure from cardiomyopathy secondary to acquired hypothyroidism. Oral loop diuretics, angiotensin-converting enzyme (ACE) inhibitors, beta-blockers, statins, and levothyroxine were started. Electrolyte correction was instituted. The sections of Endocrinology and Cardiovascular Diseases were co-managing the patient together with the General Medicine service.
He soon developed respiratory failure, upon which the considerations were acute pulmonary congestion, nosocomial pneumonia, to rule out an acute coronary event. He was later
Childhood Accidents: an Emerging Concern
7VOL. 45 NO. 3 2011 ACTA MEDICA PHILIPPINAVOL. 43 N0. 4 2009 ACTA MEDICA PHILIPPINA 13
Heart Failure and Short Stature in a 43 year-old male
transferred to the intensive care unit (ICU) for ventilatory support and closer monitoring. On bedside cardiac ultrasound, there was a finding of eccentric left ventricular hypertrophy, global hypokinesia with depressed overall systolic function with concomitant spontaneous echo contrast on left ventricular (LV) cavity suggestive of rheologic stasis, the ejection fraction was 25%, with moderate mitral regurgitation, moderate aortic regurgitation with aortic sclerosis, severe tricuspid regurgitation with mild pulmonary hypertension, pulmonary regurgitation, and minimal pericardial effusion or pericardial
fat pad. Cardiac enzymes were not consistent with an acute coronary event (Table 3), however, intravenous (IV) heparin (overlapping with oral warfarin) was still given to cover for the presence of a possible LV thrombus as demonstrated by rheologic stasis on cardiac ultrasound. Medications were shifted to IV diuretics and inotropes; oral digoxin was started. IV antibiotics were given for possible pulmonary infection. The patient later on showed improvement, and was eventually weaned off from ventilatory support, extubated,
Table 1. Initial Laboratory Results
WBCRBCHGBHCTMCVMCHMCHCRDWPLTRETICSEGLYMPHMONOEOBASOBLAST
CBC
Reference Value5-104-6120-1500.38-0.4880-100 FL27-31 PG320-360 G/L11.5-15.5%200-4000.005-0.01550-70%20-44%2-9%0-4%0-2%0%
Result
4.5
900.27
Inc
48502000
RBSHGBA1CBUNCREAALBTAGHDLLDLTOTAL CHOLASTALTAlk po4NAKCLCA++PMG++
Reference Value3.9-6.14.27-6.072.6-6.453-11534-500.34-1.70.91-1.561.1-3.84.2-5.215-3730-65
140-1483.6-5.2100-1082.12-2.52
0.74-1
Result
6.36.45.0123320.820.674.215.259591184136.93.35862.372.270.83
Blood chem.
Color
TranspSp Gravity
pHSugar
ProteinRBCWBCCast
Epith cellBacteria
Mucus thCrystals
Am urates
straw
Clear1.010
8.0NEGNEG0-10-2
RareOcc’lRareRare
Urinalysis
pH
pCO2pO2
HCO3O2 satFiO2Temp
7.408
49.170
31.393.621%36.9
ABG
PBSSlight poikilocytosis, acanthocytes, ovalocytes, slight toxic granulation, slight anisocytosis
Table 2. Thyroid Function Tests
Free T4TSH
(0.8-2.0)(0.4-6.0)
0.02 ng/dL 24.75 Uiu/ml
Reference Value Result
Figure 1. Electrocardiogram upon admission
Table 3. Cardiac Enzymes
Qualitative Troponin ICK-MBCK-TOTAL
0-6.021-232
POSITIVE
1.14543
Reference Range (mmoL) Result
Figure 2. Chest radiograph on admission
For example, older children want to learn how to strike a match, ride bicycles further away from home or climb trees.
Child Development & Injuries TEMPERAMENT – the “how” behavior difficult child easy child slow to warm up child MOTIVATION – the “why” of behavior autonomy imitating behavior risk-taking or self-destructive behaviors COMPETENCIES – the “what” of behavior infants pre-school school age adolescent
A second motivational incentive is the child’s interest in
imitating behavior, especially that seen in the movies or television, and this may be a contributing factor to injuries. A third aspect of motivation includes risk-taking or self-destructive behaviors. The child may be motivated to injure himself as a consequence of family or peer stress. Children from emotionally impoverished homes demonstrate a general lack of bodily care, heedlessness, and lack of self-protective caution.
Epidemiologic data suggest a relationship between ages or developmental stages and types of injuries. By examining children’s functioning during certain developmental stages, we can propose theoretical and common sense reasons for risk to certain injuries.
The infant’s normal drive for autonomy, their relatively underdeveloped motor coordination, their inability to adequately perceive danger, control their impulses, or understand the consequences of their actions, explain why children at this development stage experience a high rate of injuries during childhood.
Preschool-age children have cognitive limitations. Parents need to continually remind children not to do certain things. The emphasis at this age should be that certain behaviors – hitting, throwing stones at people, and crossing the street are not acceptable. While they learn to accomplish certain motor tasks, the quality of their performance may be poor.
School-age children tend to be daring and adventurous. They are inclined to challenge rules. Road and traffic safety should be emphasized to them. These children do not understand many traffic terms and signs. They have a reduced ability to localize sounds and impaired perception of movement in their peripheral visual fields. They are still unable to appreciate speed and danger and this is aggravated by their physically being at a lower eye level. Their distractibility and impulsiveness increase the risk of traffic injury at this age.
The adolescent’s intellectual ability is better developed. They become overly involved in abstract matters and
sometimes lose touch with reality. They develop a feeling of immortality. This, combined with an innate need for experimentation, a tendency to imitate the behavior of older adolescents and adults, and the pressure of one’s peer group can lead to serious consequences in terms of injuries.
A knowledge of children’s developmental characteristics and behavior has at least two important implications. First, it will provide a framework for clinicians who want to individualize their injury prevention counseling to patients and their parents. Second, it will provide a framework for possible future research.
Compared to other major public health problems there has been little research in the field of injuries. This is due to insufficient funding, few scientists trained in epidemiology on injury control, and a negative perception that injury control is not a legitimate social and scientific pursuit. The reasons often cited by physicians are that:
Physicians are too busy with treatment Injury research: not of medical interest Injuries: not important medical problem Diseases, not “ACCIDENTS,” are the concern of
health professionals The number of years of life lost annually due to injuries
is much more compared to those of cancer and heart disease combined. However, the resources abroad allocate for cancer research alone are about 10 times greater than those devoted to accident research.
Figure 5. Pre-retirement years of life lost and research expenditures for major causes of death, USA, 1978
The three areas in injury control where research should be strengthened are: clinical, epidemiological and biotechnical (ergonomic) research. Clinical research will begin to answer a crucial question: is the reduction in accident mortality accompanied by an increase in persistent sequelae and long-lasting or permanent disability?

Childhood Accidents: an Emerging Concern
8 VOL. 45 NO. 3 2011ACTA MEDICA PHILIPPINA VOL. 43 N0. 4 200912 ACTA MEDICA PHILIPPINA
Heart Failure and Short Stature in a 43 year-old male
Katerina T. Leyritana1, Ma. Czarlota M. Acelajado-Valdenor1, Amado O. Tandoc III2 and Agnes D. Mejia1
1Department of Medicine, College of Medicine and Philippine General Hospital, University of the Philippines Manila
2Department of Pathology, College of Medicine, University of the Philippines Manila
CASE REPORT
Corresponding author: Ma. Czarlota Acelajado-Valdenor, M.D.Department of MedicinePhilippine General HospitalTaft Avenue, Manila, 1000 PhilippinesTelephone: +632 554-8488Email: [email protected]
Presentation of the caseThis is a case of a 43-year-old male presenting with short
stature and heart failure. The patient was admitted at the medicine ward of the Philippine General Hospital (PGH) for dyspnea. This paper will investigate several issues: differentiating congenital from acquired hypothyroidism, the relationship between hypothyroidism and the cardiomyopathies, and the therapeutic options in patients with cardiomyopathy secondary to hypothyroidism.
The patient had been born full term to a then 31-year-old Gravida 4 Para 3 (G4P3), the 4th of 9 siblings, with an apparently unremarkable delivery at home facilitated by a traditional birth attendant. He was noted to be normal at birth. The patient was allegedly at par with age both physically and mentally until eight years old when he was said to have stopped growing in height. He was brought to a private doctor, whose diagnosis was undisclosed, and he was given medications to increase height, which the patient took for only one month with no improvement. Through the years, the patient was apparently well, although still of short stature, with thick lips, coarse facial features and dry skin. He was notably slow in ambulation. He was said to have bronchial asthma at age 15 years, and since then he had been taking salbutamol tablets occasionally for bouts of dyspnea occurring one to two times annually.
The patient’s symptoms started in 2001 when he was reported to have sudden loss of consciousness. During this time, the patient did not have any symptoms of heart failure; no prior seizures, cyanotic episodes, chest pain, headache, or blurring of vision. He regained consciousness shortly after and was brought to a private physician, whose assessment was a “heart problem”. He was prescribed unrecalled medications taken for a few months and eventually discontinued when the syncopal episode did not recur.
In the next four years, the patient would develop intermittent, progressive exertional dyspnea and bipedal edema. Later on this would be accompanied by generalized body weakness, anorexia, and constipation, severe enough to
require regular laxative use. There was also a report of two more syncopal episodes. He was brought to another doctor in a private hospital where the assessment was still a “heart problem”. The patient was again prescribed unrecalled medications and again was lost to follow-up. This time, however, symptoms were persistent. He later consulted at another local hospital, where he was admitted and managed as a case of anemia and bronchial asthma. He was discharged slightly improved after four days, only to have recurrent heart failure symptoms, prompting admission at PGH.
Upon admission the patient was in mild respiratory distress, with stable vital signs and no note of fever. Pertinent physical exam findings included short stature, thick lips, non-pitting periorbital edema, dry skin, a displaced apical impulse, crackles on both lung fields, and bilateral non-pitting bipedal edema. There was also a 3 cm x 3 cm reducible umbilical hernia. However, there was no pallor, no neck vein distention, no apparent congenital malformations, no cardiac murmurs and no clubbing. There was also no note of an anterior neck mass.
Laboratory workup showed cardiomegaly with pulmonary congestion, thoracic dextroscoliosis, and atheromatous aorta by chest radiograph, and left ventricular hypertrophy by 12-lead electrocardiogram (12-L ECG) (Figures 1 and 2), normocytic normochromic anemia (Hgb 90 mg/dL), dyslipidemia, and pre-renal azotemia (serum creatinine 123 mmoL). Electrolytes on admission showed slight hyponatremia, hypokalemia, and hypochloremia (serum Na 136, K 3.35, Cl 86). Blood gases revealed partially compensated metabolic alkalosis with mild hypoxemia. The patient was noted to be hypothyroid based on elevated serum thyroid-stimulating hormone (TSH) and markedly decreased serum free thyroxine (FT4). The exact values are shown in Tables 1 and 2.
Upon admission to the wards, the patient was managed as having congestive heart failure from cardiomyopathy secondary to acquired hypothyroidism. Oral loop diuretics, angiotensin-converting enzyme (ACE) inhibitors, beta-blockers, statins, and levothyroxine were started. Electrolyte correction was instituted. The sections of Endocrinology and Cardiovascular Diseases were co-managing the patient together with the General Medicine service.
He soon developed respiratory failure, upon which the considerations were acute pulmonary congestion, nosocomial pneumonia, to rule out an acute coronary event. He was later
VOL. 43 N0. 4 2009 ACTA MEDICA PHILIPPINA 13
Heart Failure and Short Stature in a 43 year-old male
transferred to the intensive care unit (ICU) for ventilatory support and closer monitoring. On bedside cardiac ultrasound, there was a finding of eccentric left ventricular hypertrophy, global hypokinesia with depressed overall systolic function with concomitant spontaneous echo contrast on left ventricular (LV) cavity suggestive of rheologic stasis, the ejection fraction was 25%, with moderate mitral regurgitation, moderate aortic regurgitation with aortic sclerosis, severe tricuspid regurgitation with mild pulmonary hypertension, pulmonary regurgitation, and minimal pericardial effusion or pericardial
fat pad. Cardiac enzymes were not consistent with an acute coronary event (Table 3), however, intravenous (IV) heparin (overlapping with oral warfarin) was still given to cover for the presence of a possible LV thrombus as demonstrated by rheologic stasis on cardiac ultrasound. Medications were shifted to IV diuretics and inotropes; oral digoxin was started. IV antibiotics were given for possible pulmonary infection. The patient later on showed improvement, and was eventually weaned off from ventilatory support, extubated,
Table 1. Initial Laboratory Results
WBCRBCHGBHCTMCVMCHMCHCRDWPLTRETICSEGLYMPHMONOEOBASOBLAST
CBC
Reference Value5-104-6120-1500.38-0.4880-100 FL27-31 PG320-360 G/L11.5-15.5%200-4000.005-0.01550-70%20-44%2-9%0-4%0-2%0%
Result
4.5
900.27
Inc
48502000
RBSHGBA1CBUNCREAALBTAGHDLLDLTOTAL CHOLASTALTAlk po4NAKCLCA++PMG++
Reference Value3.9-6.14.27-6.072.6-6.453-11534-500.34-1.70.91-1.561.1-3.84.2-5.215-3730-65
140-1483.6-5.2100-1082.12-2.52
0.74-1
Result
6.36.45.0123320.820.674.215.259591184136.93.35862.372.270.83
Blood chem.
Color
TranspSp Gravity
pHSugar
ProteinRBCWBCCast
Epith cellBacteria
Mucus thCrystals
Am urates
straw
Clear1.0108.0
NEGNEG0-10-2
RareOcc’lRareRare
Urinalysis
pH
pCO2pO2
HCO3O2 satFiO2Temp
7.408
49.170
31.393.621%36.9
ABG
PBSSlight poikilocytosis, acanthocytes, ovalocytes, slight toxic granulation, slight anisocytosis
Table 2. Thyroid Function Tests
Free T4TSH
(0.8-2.0)(0.4-6.0)
0.02 ng/dL 24.75 Uiu/ml
Reference Value Result
Figure 1. Electrocardiogram upon admission
Table 3. Cardiac Enzymes
Qualitative Troponin ICK-MBCK-TOTAL
0-6.021-232
POSITIVE
1.14543
Reference Range (mmoL) Result
Figure 2. Chest radiograph on admission
Epidemiological surveys seem all the more important in that they can provide, in addition to simple scientific facts, a basis for rational prevention of accidents. Biotechnical or ergonomic research unites biology and engineering to provide a safer environment and considerably reduce the number of deaths and severe disabilities.
Data about the circumstances leading to injuries and which described the magnitude of the problem in terms of mortality and morbidity supports the scientific approach to injury prevention. Injury surveillance data which provides information about the pre-event phase of injury is important for primary and secondary prevention. Injury surveillance data from small geographical areas is particularly relevant for community-based intervention programs, but also has value at a national level. Minimum data, such as those enumerated below, are required as this will enable specific forms of intervention to take place.
Need For Injury Database Characteristics of the child Description of accident: circumstances, type, resulting injuries Care provided, initially and as follow-up Prognosis and final outcome Source and place of recording
Education, training and information are very crucial in
the prevention program for injuries. Educational or training packages should be prepared for professional groups and communicators, either to be used by them in educating target groups in the community, or to improve their own specialized knowledge and skills.
Professional groups and communicators are groups defined on the basis of their jobs or standing in the community who are potentially capable of educating target group in the community.
Target groups in the community are potential accident victims, people potentially causing accidents, close relatives or friends of these two groups.
The responsibility of teaching and preparing the educational packages directly concern medical schools, hospitals, medical and health organizations and other multidisciplinary and intersectoral groups.
As to what should be taught, a general framework can be developed as shown in Figure 6. For each type of accident, the content may include accident risks, preventive measures, management and resources.
Even if one considers injuries to be a health problem, vey often it remains difficult to think of all possible countermeasures because the problem appears too large and too wide. One useful approach is to consider each injury problem as resulting from an interaction between several discrete factors (host, vector, and environment), occurring over distinct phases in time (pre-event, event, post-event) which is illustrated in Figure 7. In developing a program of injury control measures for a particular injury problem we can go systematically through each cell of the matrix and
think up all possible countermeasures applicable to that cell. The usefulness is a tool for generating ideas. After all possible countermeasures have been listed, injury control experts and policymakers can select those which are most feasible, effective and politically acceptable.
Figure 6. General Framework
Figure 7. Injury Matrix
In conclusion, the author is enjoining everyone to be advocates for injury control. He encourages the government to coordinate with industry to enhance safety of products, building, vehicles, and roads. The ultimate goal of all advocacy efforts to get injury prevention is the national health agenda and to create national, regional, and local injury control committees. ___________ References Alpert, J.J. & Guyer, B. (Ed). (February, 1985). Symposium on injuries and
injury prevention.PCNA, 32 (1). Mclntire, M.S. (Ed.) (1987). Injury control for children and youth. American
Academy of Pediatrics. Committee on accident and Poison Prevention. Illinois: AAP.
Angel, C. et al. (November 1975). Locomotor skills and school accidents. Pediatrics, 56:819.
Arcadio, R.L., et al. (January-March, 1992). A hospital based epidemiological survey. The Philippine Journal of Pediatrics, vol. 41 no. 1

VOL. 43 N0. 4 200912 ACTA MEDICA PHILIPPINA
Heart Failure and Short Stature in a 43 year-old male
Katerina T. Leyritana1, Ma. Czarlota M. Acelajado-Valdenor1, Amado O. Tandoc III2 and Agnes D. Mejia1
1Department of Medicine, College of Medicine and Philippine General Hospital, University of the Philippines Manila
2Department of Pathology, College of Medicine, University of the Philippines Manila
CASE REPORT
Corresponding author: Ma. Czarlota Acelajado-Valdenor, M.D.Department of MedicinePhilippine General HospitalTaft Avenue, Manila, 1000 PhilippinesTelephone: +632 554-8488Email: [email protected]
Presentation of the caseThis is a case of a 43-year-old male presenting with short
stature and heart failure. The patient was admitted at the medicine ward of the Philippine General Hospital (PGH) for dyspnea. This paper will investigate several issues: differentiating congenital from acquired hypothyroidism, the relationship between hypothyroidism and the cardiomyopathies, and the therapeutic options in patients with cardiomyopathy secondary to hypothyroidism.
The patient had been born full term to a then 31-year-old Gravida 4 Para 3 (G4P3), the 4th of 9 siblings, with an apparently unremarkable delivery at home facilitated by a traditional birth attendant. He was noted to be normal at birth. The patient was allegedly at par with age both physically and mentally until eight years old when he was said to have stopped growing in height. He was brought to a private doctor, whose diagnosis was undisclosed, and he was given medications to increase height, which the patient took for only one month with no improvement. Through the years, the patient was apparently well, although still of short stature, with thick lips, coarse facial features and dry skin. He was notably slow in ambulation. He was said to have bronchial asthma at age 15 years, and since then he had been taking salbutamol tablets occasionally for bouts of dyspnea occurring one to two times annually.
The patient’s symptoms started in 2001 when he was reported to have sudden loss of consciousness. During this time, the patient did not have any symptoms of heart failure; no prior seizures, cyanotic episodes, chest pain, headache, or blurring of vision. He regained consciousness shortly after and was brought to a private physician, whose assessment was a “heart problem”. He was prescribed unrecalled medications taken for a few months and eventually discontinued when the syncopal episode did not recur.
In the next four years, the patient would develop intermittent, progressive exertional dyspnea and bipedal edema. Later on this would be accompanied by generalized body weakness, anorexia, and constipation, severe enough to
require regular laxative use. There was also a report of two more syncopal episodes. He was brought to another doctor in a private hospital where the assessment was still a “heart problem”. The patient was again prescribed unrecalled medications and again was lost to follow-up. This time, however, symptoms were persistent. He later consulted at another local hospital, where he was admitted and managed as a case of anemia and bronchial asthma. He was discharged slightly improved after four days, only to have recurrent heart failure symptoms, prompting admission at PGH.
Upon admission the patient was in mild respiratory distress, with stable vital signs and no note of fever. Pertinent physical exam findings included short stature, thick lips, non-pitting periorbital edema, dry skin, a displaced apical impulse, crackles on both lung fields, and bilateral non-pitting bipedal edema. There was also a 3 cm x 3 cm reducible umbilical hernia. However, there was no pallor, no neck vein distention, no apparent congenital malformations, no cardiac murmurs and no clubbing. There was also no note of an anterior neck mass.
Laboratory workup showed cardiomegaly with pulmonary congestion, thoracic dextroscoliosis, and atheromatous aorta by chest radiograph, and left ventricular hypertrophy by 12-lead electrocardiogram (12-L ECG) (Figures 1 and 2), normocytic normochromic anemia (Hgb 90 mg/dL), dyslipidemia, and pre-renal azotemia (serum creatinine 123 mmoL). Electrolytes on admission showed slight hyponatremia, hypokalemia, and hypochloremia (serum Na 136, K 3.35, Cl 86). Blood gases revealed partially compensated metabolic alkalosis with mild hypoxemia. The patient was noted to be hypothyroid based on elevated serum thyroid-stimulating hormone (TSH) and markedly decreased serum free thyroxine (FT4). The exact values are shown in Tables 1 and 2.
Upon admission to the wards, the patient was managed as having congestive heart failure from cardiomyopathy secondary to acquired hypothyroidism. Oral loop diuretics, angiotensin-converting enzyme (ACE) inhibitors, beta-blockers, statins, and levothyroxine were started. Electrolyte correction was instituted. The sections of Endocrinology and Cardiovascular Diseases were co-managing the patient together with the General Medicine service.
He soon developed respiratory failure, upon which the considerations were acute pulmonary congestion, nosocomial pneumonia, to rule out an acute coronary event. He was later
Childhood Accidents: an Emerging Concern
9VOL. 45 NO. 3 2011 ACTA MEDICA PHILIPPINAVOL. 43 N0. 4 2009 ACTA MEDICA PHILIPPINA 13
Heart Failure and Short Stature in a 43 year-old male
transferred to the intensive care unit (ICU) for ventilatory support and closer monitoring. On bedside cardiac ultrasound, there was a finding of eccentric left ventricular hypertrophy, global hypokinesia with depressed overall systolic function with concomitant spontaneous echo contrast on left ventricular (LV) cavity suggestive of rheologic stasis, the ejection fraction was 25%, with moderate mitral regurgitation, moderate aortic regurgitation with aortic sclerosis, severe tricuspid regurgitation with mild pulmonary hypertension, pulmonary regurgitation, and minimal pericardial effusion or pericardial
fat pad. Cardiac enzymes were not consistent with an acute coronary event (Table 3), however, intravenous (IV) heparin (overlapping with oral warfarin) was still given to cover for the presence of a possible LV thrombus as demonstrated by rheologic stasis on cardiac ultrasound. Medications were shifted to IV diuretics and inotropes; oral digoxin was started. IV antibiotics were given for possible pulmonary infection. The patient later on showed improvement, and was eventually weaned off from ventilatory support, extubated,
Table 1. Initial Laboratory Results
WBCRBCHGBHCTMCVMCHMCHCRDWPLTRETICSEGLYMPHMONOEOBASOBLAST
CBC
Reference Value5-104-6120-1500.38-0.4880-100 FL27-31 PG320-360 G/L11.5-15.5%200-4000.005-0.01550-70%20-44%2-9%0-4%0-2%0%
Result
4.5
900.27
Inc
48502000
RBSHGBA1CBUNCREAALBTAGHDLLDLTOTAL CHOLASTALTAlk po4NAKCLCA++PMG++
Reference Value3.9-6.14.27-6.072.6-6.453-11534-500.34-1.70.91-1.561.1-3.84.2-5.215-3730-65
140-1483.6-5.2100-1082.12-2.52
0.74-1
Result
6.36.45.0123320.820.674.215.259591184136.93.35862.372.270.83
Blood chem.
Color
TranspSp Gravity
pHSugar
ProteinRBCWBCCast
Epith cellBacteria
Mucus thCrystals
Am urates
straw
Clear1.010
8.0NEGNEG0-10-2
RareOcc’lRareRare
Urinalysis
pH
pCO2pO2
HCO3O2 satFiO2Temp
7.408
49.170
31.393.621%36.9
ABG
PBSSlight poikilocytosis, acanthocytes, ovalocytes, slight toxic granulation, slight anisocytosis
Table 2. Thyroid Function Tests
Free T4TSH
(0.8-2.0)(0.4-6.0)
0.02 ng/dL 24.75 Uiu/ml
Reference Value Result
Figure 1. Electrocardiogram upon admission
Table 3. Cardiac Enzymes
Qualitative Troponin ICK-MBCK-TOTAL
0-6.021-232
POSITIVE
1.14543
Reference Range (mmoL) Result
Figure 2. Chest radiograph on admission
Arcadio, R.L., et al. (January-March 1992). Childhood accidents: A community-based epidemiological survey (Part 11). The Philippine Journal of Pediatrics, vol. 41 no. 1
Arcadio, R.L., et al. (January-March 1992). Childhood Accidents: Part III. Survey of existing training programs on prevention of childhood accidents for medical students and pediatric residents in the Philippines. The Philippine Journal of Pediatrics, vol. 41 no. 1
Arcadio, R.L., et al. (January-March 1992). Home Accidents: The Philippine Experience. The Philippine Journal of Pediatrics, vol. 41 no. 1
Arcadio, R.L., et al. (January-March 1992). Childhood accidents in the Philippines: A country report. The Philippine Journal of Pediatrics, vol. 41 no. 1
Annual Report (1989). Armed Forces of the Philippines, Philippine Constabulary Highway Patrol Group.
Baker, D. et al. (December 1987). Human bites in children, a six year experience. American Journal of the Diseases of a Child, 141: 1285.
Bergner, L. et al. (19710. Falls from height: A childhood epidemic in an urban area. American Journal of Public Health, 61:90
Boyce, T. et al. (September 1984). Epidemiology of Injuries in a large urban school district. Pediatrics 74:342.
Canlas, et al. (July 1977). A descriptive study of fatal motor vehicle accidents in Quezon City from January-December, 1975. Anphi Papers, 12:2.
Cutiongco, E.C., & Arcadio, R.L. (January-March 1992). Attitudes toward home accidents prevention by care-providers of children at the UP-PGH Medical Center. The Philippine Journal of Pediatrics, vol. 41, no. 1.
Dauis-Lawas, D. et al. (July 1963). Poisoning in children. MD Journal, 12:503. Philippine Health Statistics (1986). Department of Health: Health Intelligence
Service. Philippine Health Statistics (1989). Department of Health: Health Intelligence
Service . Annual Report (1989). Department of Social Welfare and Development: Section of
Children and Youth Welfare. Deschamps, J.P. (1981). Prevention of traffic accidents in childhood. World
Health Organization: Copenhagen. Diets, P. et al. (April 1974). Drowning epidemiology and prevention. American
Journal of Public Health, 64:309. Evans, D. et al. (January 1989). Epidemiology of school injuries. A two years
experience in a municipal department. Pediatrics, 79:69. Fabella, S.F. (December 1971). Acute poisoning in children and the need for
poison control center in the Philippines. Philippine Journal of Pediatrics, 20:257.
Feldman, K. et al. (1980). Tap water scald burns in children. Pediatrics, 65:1070 The National Building Code of the Philippine and its Implementing Rules and
Regulations. (1990). Philippine Law Gazette. Manila Research on Accident and Injury Prevention. (1988). World Health Organization.
Advisory Committee on Health Research. Geneva Global Program on Accident Prevention: Eight General Program of Work for
1990-1995. (1988). World Health Organization: Geneva . Study Group on Assessment of Country Surveys on Accidents in Childhood.
Report on a WHO Meeting. World Health Organization: Ankara. Symposium on Accident Prevention in Childhood. (1984). World Health
Organization. Report on a WHO/ICC. IPA Meeting. Manila Zerrudo, E. & Dizon, J. (February 1967). The epidemiology of traffic accidents
in the Philippines. Journal of the Philippine Medical Association, 43:95. Gallagher, S. et al. (February 1985). A home injury prevention program for
children. PCNA 32:95 Hartigan-Go, K. et al. (1988). Five years retrospective study on poisoning cases
presenting at the poison control center of the Philippine General Hospital (1983-1987). Unpublished.
Lao, M.L. & De La Cruz, M.L. (October –January 1990). A study of the pattern of poisoning among patients seen at the Ospital ng Maynila, January 1986-December 1987. Journal of the Manila Medical Society, 15-8.
Lumicad, Z. & Fortaleza, V. (January 1979). Ecology of Home accidents. Anphi Papers, 14:12.
Mohan, D. (1983). Childhood accidents in India: extent of the problem and strategies for control. New Delhi: Indian Institute of Technology (Mimeograph).
National Bureau of Investigation (1989). Medico legal section: Statistics. National Census and Statistics. (1990). Annual paper, 1986-1989. Philippine Land Transportation Commission (1990). Annual Report, 1986-1989). Philippine Pediatric Society. (1990). Annual Report 1985-1989.
Ramirez, A.T., et al. (1969) Analysis of burn mortalities over Ten year period at Philippine General Hospital. Philippine Journal of Surgery.
Rivera, F. et al. (June 1982). Epidemiology of childhood injuries. American Journal of Dis Child, 136: 502

10 VOL. 45 NO. 3 2011ACTA MEDICA PHILIPPINA VOL. 43 N0. 4 200912 ACTA MEDICA PHILIPPINA
Heart Failure and Short Stature in a 43 year-old male
Katerina T. Leyritana1, Ma. Czarlota M. Acelajado-Valdenor1, Amado O. Tandoc III2 and Agnes D. Mejia1
1Department of Medicine, College of Medicine and Philippine General Hospital, University of the Philippines Manila
2Department of Pathology, College of Medicine, University of the Philippines Manila
CASE REPORT
Corresponding author: Ma. Czarlota Acelajado-Valdenor, M.D.Department of MedicinePhilippine General HospitalTaft Avenue, Manila, 1000 PhilippinesTelephone: +632 554-8488Email: [email protected]
Presentation of the caseThis is a case of a 43-year-old male presenting with short
stature and heart failure. The patient was admitted at the medicine ward of the Philippine General Hospital (PGH) for dyspnea. This paper will investigate several issues: differentiating congenital from acquired hypothyroidism, the relationship between hypothyroidism and the cardiomyopathies, and the therapeutic options in patients with cardiomyopathy secondary to hypothyroidism.
The patient had been born full term to a then 31-year-old Gravida 4 Para 3 (G4P3), the 4th of 9 siblings, with an apparently unremarkable delivery at home facilitated by a traditional birth attendant. He was noted to be normal at birth. The patient was allegedly at par with age both physically and mentally until eight years old when he was said to have stopped growing in height. He was brought to a private doctor, whose diagnosis was undisclosed, and he was given medications to increase height, which the patient took for only one month with no improvement. Through the years, the patient was apparently well, although still of short stature, with thick lips, coarse facial features and dry skin. He was notably slow in ambulation. He was said to have bronchial asthma at age 15 years, and since then he had been taking salbutamol tablets occasionally for bouts of dyspnea occurring one to two times annually.
The patient’s symptoms started in 2001 when he was reported to have sudden loss of consciousness. During this time, the patient did not have any symptoms of heart failure; no prior seizures, cyanotic episodes, chest pain, headache, or blurring of vision. He regained consciousness shortly after and was brought to a private physician, whose assessment was a “heart problem”. He was prescribed unrecalled medications taken for a few months and eventually discontinued when the syncopal episode did not recur.
In the next four years, the patient would develop intermittent, progressive exertional dyspnea and bipedal edema. Later on this would be accompanied by generalized body weakness, anorexia, and constipation, severe enough to
require regular laxative use. There was also a report of two more syncopal episodes. He was brought to another doctor in a private hospital where the assessment was still a “heart problem”. The patient was again prescribed unrecalled medications and again was lost to follow-up. This time, however, symptoms were persistent. He later consulted at another local hospital, where he was admitted and managed as a case of anemia and bronchial asthma. He was discharged slightly improved after four days, only to have recurrent heart failure symptoms, prompting admission at PGH.
Upon admission the patient was in mild respiratory distress, with stable vital signs and no note of fever. Pertinent physical exam findings included short stature, thick lips, non-pitting periorbital edema, dry skin, a displaced apical impulse, crackles on both lung fields, and bilateral non-pitting bipedal edema. There was also a 3 cm x 3 cm reducible umbilical hernia. However, there was no pallor, no neck vein distention, no apparent congenital malformations, no cardiac murmurs and no clubbing. There was also no note of an anterior neck mass.
Laboratory workup showed cardiomegaly with pulmonary congestion, thoracic dextroscoliosis, and atheromatous aorta by chest radiograph, and left ventricular hypertrophy by 12-lead electrocardiogram (12-L ECG) (Figures 1 and 2), normocytic normochromic anemia (Hgb 90 mg/dL), dyslipidemia, and pre-renal azotemia (serum creatinine 123 mmoL). Electrolytes on admission showed slight hyponatremia, hypokalemia, and hypochloremia (serum Na 136, K 3.35, Cl 86). Blood gases revealed partially compensated metabolic alkalosis with mild hypoxemia. The patient was noted to be hypothyroid based on elevated serum thyroid-stimulating hormone (TSH) and markedly decreased serum free thyroxine (FT4). The exact values are shown in Tables 1 and 2.
Upon admission to the wards, the patient was managed as having congestive heart failure from cardiomyopathy secondary to acquired hypothyroidism. Oral loop diuretics, angiotensin-converting enzyme (ACE) inhibitors, beta-blockers, statins, and levothyroxine were started. Electrolyte correction was instituted. The sections of Endocrinology and Cardiovascular Diseases were co-managing the patient together with the General Medicine service.
He soon developed respiratory failure, upon which the considerations were acute pulmonary congestion, nosocomial pneumonia, to rule out an acute coronary event. He was later
Ramon L. Arcadio: The Academic and Advocate for the Prevention of Childhood Injuries and Accidents in the Philippines
Rafael J. Consunji, MD, MPH1 and Jinky Leilanie D. Lu, MOH, PhD2
1Division of Surgical Critical Care and Trauma, Department of Surgery,
College of Medicine and Philippine General Hospital, University of the Philippines Manila 2National Institutes of Health, University of the Philippines Manila
This special issue on Injury Prevention and Control of the Acta Medica Philippina is dedicated to Chancellor Ramon L. Arcadio whose pioneering research work and advocacy for the prevention of childhood injuries/accidents which is the third leading cause of death in the Philippines has been unprecedented.
In 1992, Dr. Ramon L. Arcadio published the first extensive Philippine research data on childhood injuries (accidents), an important but underemphasized area in training and healthcare in the country. Five papers, as principal investigator, and one as co-investigator, were published in the Philippine Journal of Pediatrics. The pioneering researches were on hospital and community-based epidemiology, home accidents, and training programs on the prevention of childhood accidents. Before these publications, there were no data on childhood injuries in Philippine medical literature.
Even before being published, the research data were read by Dr. Arcadio in an international conference on childhood injuries in Kuala Lumpur, Malaysia in 1990. This was the first major sharing of data on childhood injuries among Asian countries held under the auspices of the 5th ASEAN Pediatric Federation. Dr. Arcadio also read his research data and spoke on the subject on various health fora, conventions, and scientific meetings.
Due to his scientific work and expertise on the subject, Dr. Arcadio was invited to write the chapter on Childhood Injuries in the 4th edition of the Textbook of Pediatrics and Child Health, edited by Dr. Fe del Mundo, et. al in 2000.
Dr. Arcadio is also the Convenor of the recently created National Institutes of Health Study Group on
Injury Prevention and Control.
Dr. Arcadio’s advocacy on the subject also resulted in the inclusion of childhood injuries in the curricula of the health sciences like Midwifery, Nursing and Medicine.
In 2003, Dr. Arcadio was elected Founding Chairman of the Board of Trustees of SAFEKIDS PHILIPPINES, a position he still currently holds. This organization is a SEC-registered non-government organization whose vision-mission is the prevention of
childhood injuries. It belongs to a network of about sixteen similar organizations in various countries, all affiliated with SAFEKIDS WORLDWIDE which is based in Washington D.C. USA. Safekids Philippines has prevention programs in Pasay, Parañaque, Olangapo, Cebu and Quezon City.
All throughout the chancellorship of Dr. Arcadio from 2006 to 2011, he has committed both administrative resources and his expertise in the prevention of injuries in general, and childhood injuries/accidents in particular.
Dr. Ramon L. Arcadio