Embed Size (px)
Citation preview

Review ArticleDNA Damage as a Driver for Growth Delay ChromosomeInstability Syndromes with Intrauterine Growth Retardation
Benilde Garciacutea-de Teresa12 Mariana Hernaacutendez-Goacutemez34 and Sara Friacuteas15
1Laboratorio de Citogenetica Instituto Nacional de Pediatrıa Mexico City Mexico2Programa de Doctorado en Ciencias Biomedicas UNAM Mexico City Mexico3Universidad Anahuac Mexico City Mexico4Departamento de Genetica Instituto Nacional de Perinatologıa Mexico City Mexico5Instituto de Investigaciones Biomedicas UNAM Mexico City Mexico
Correspondence should be addressed to Sara Frıas sarafriasbiomedicasunammx
Received 4 February 2017 Revised 16 June 2017 Accepted 17 July 2017 Published 12 November 2017
Academic Editor Vassilios Fanos
Copyright copy 2017 Benilde Garcıa-de Teresa et al This is an open access article distributed under the Creative CommonsAttribution License which permits unrestricted use distribution and reproduction in any medium provided the original work isproperly cited
DNA is constantly exposed to endogenous and exogenous mutagenic stimuli that are capable of producing diverse lesions In orderto protect the integrity of the genetic material a wide array of DNA repair systems that can target each specific lesion has evolvedDespite the availability of several repair pathways a common general program known as the DNA damage response (DDR) isstimulated to promote lesion detection signaling and repair in order to maintain genetic integrity The genes that participate inthese pathways are subject to mutation a loss in their function would result in impaired DNA repair and genomic instabilityWhen the DDR is constitutionally altered every cell of the organism starting from development will show DNA damage andsubsequent genomic instability The cellular response to this is either uncontrolled proliferation and cell cycle deregulation thatensues overgrowth or apoptosis and senescence that result in tissue hypoplasiaThese diverging growth abnormalities can clinicallytranslate as cancer or growth retardation both features can be found in chromosome instability syndromes (CIS)The analysis of theclinical cellular and molecular phenotypes of CIS with intrauterine growth retardation allows inferring that replication alterationis their unifying feature
1 DNA and Genomic Integrity
DNA is our genetic heritage the genetic instructions that cellsuse to construct their components and function are encodedin their sequence DNA is also the molecule responsible fortransmitting information from generation to generation ona cell and organism scale This information is provided toeach human being in the nucleus of the fertilized egg in aset of 46 DNAmolecules forming chromosomes Subsequentdivisions generate millions of cells to form a fetus each oneof these cells has its own set of 46 chromosomes Amazinglyin spite of having been copied millions of times the DNAsequence of these chromosomes is remarkably similar to theoriginal molecule This is surprising since DNA is constantlyexposed to endogenous and exogenous mutagenic stimuliOn the one hand each replication round can result in
thousands of lesions while on the other hand environmentalgenotoxic agents are a constant and an inevitable source ofDNA damage [1 2] Every day the DNA of a fetus can thenaccumulate tens of thousands of lesions that could resultin mutations [2] However the DNA molecule is such animportant asset to the cell that a significant share of its geneticinformation and cellular energy are destined to the detectionand repair of DNA damage to preserve the organismrsquos geneticintegrity
2 DNA Damage and the DNADamage Response
The sources of induced lesions in DNA can be endogenousor exogenous The former originate from normal metabolicprocesses inside the cell such as DNA replication whichmay
HindawiBioMed Research InternationalVolume 2017 Article ID 8193892 14 pageshttpsdoiorg10115520178193892
2 BioMed Research International
Base excision repair (BER)
Mismatch repair (MMR)
Nucleotide excision repair (NER)
Homologous recombination repair (HR)
NonhomologousEnd Joining (NHEJ)
Source of damage Types of DNA lesions DNA repair pathway
Ionizing radiation
Bifunctional alkylatingagents
(i)
(ii)
Hydroxyurea(iii)
Single-strand break (direct lesion)
(i)
8-Oxo-G(ii)Abasic site(iii)Uracil in DNA(iv)
base mispairing(i)
Double-strand break (DSB) (direct and ICL product)Interstrand crosslink (ICL)Single-strand break (SSB) (ICL by-product or associated with DNA replication)
(i)
(ii)(iii)
64 photoproductTimidine dimerBulky adduct
(i)(ii)
(iii)
Replication Errors(i)
UV lightPolycyclic AromaticHydrocarbonsAlkylating agents
(i)(ii)
(iii)
UV lightOxigen radicalsAlkylating agentsSpontaneous Cytosine deamination
(i)(ii)
(iv)(iii)
Figure 1 DNA lesions are induced by endogenous and exogenous sources Every agent causes a particular lesion that will activate specificDNA repair pathways
incorporate noncomplementary WatsonndashCrick bases duringDNA synthesis It can also come from lesions caused byoxidative damage that occurs during normal metabolism inthe mitochondria and other cellular sites giving rise to theoxidation of several cellular components including DNAresulting in modified bases or breaking of the union betweenthem Besides spontaneous decay of the DNAmolecule maygenerate hydrolysis that creates abasic sites and deaminationcausing a change in the original bases Exogenous sourcesthat continually damage our DNA may be of four mainorigins (1) biological such as some virus (2) physicallike solar radiation or radiation therapy (3) chemical likepesticides and medical treatments (chemotherapy) and (4)personal habits such as smoking (Figure 1) All togetherthese mechanisms may generate more than ten thousandlesions per cell per day [3]
Two main factors the type of DNA lesions and thephase of the cell cycle where they are sensed affect thechoice of the DNA repair pathway to be used and thesubsequent outcome (Figure 1) Mispaired bases are repairedby mismatch repair (MMR) oxidative damage abasic sitesand uracil in DNA are corrected by removing the altered basethrough base excision repair (BER) UV radiation damageand bulky adducts that disrupt the structure of the double
helix are repaired by nucleotide excision repair (NER) inwhich an oligonucleotide of 30 bp containing the lesion isremoved [4] Most DNA lesions interfere with DNA repli-cation and transcription processes that are indispensablefor appropriate cell function However double-strand breaks(DSBs) in which both DNA strands lose continuity are themost dangerous type of DNA damage and have primarilycytotoxic or cytostatic consequences [2 3 5]
Interstrand crosslinks (ICLs) are detected and removedthrough the Fanconi anemia pathway [6 7] also knownas the FABRCA pathway The processing of ICLs occursduring the S phase resulting in the following intermediarylesions an adduct and a DSB which are further takencare of by known repair pathways The adduct is repairedby the NER pathway while the DSB is processed by oneof four independent pathways nonhomologous end joining(NHEJ) homologous recombination (HR) alternative-NHEJ(alt-NHEJ) and single-strand annealing (SSA)The selectionof the repair pathway that will take care of the DSB dependson the cell cycle phase and if the 31015840 ends of the DSBs areprocessed by an exonuclease or not [8] NHEJ operates in anyphase of the cell cycle and does not require any processingsince this repair pathway marks both blunt ends of the DSBwith a Ku70Ku80 heterodimer and joins them Meanwhile
BioMed Research International 3
p53
53BP1
Rif1
CtlP
BRCA1
KU80
KU70
+
+NBN
RAD50
MRE11gH2AX
gH2AXgH2AX
gH2AX
RPARPARPARPA
FAN
CM
G
G
Transducers ATMATR
Checkpoint
DNAPKcs
Chromatinreorganization
Effectors
Sensors and mediators
Senescence Celldeath
Reparable damage Irreparable damage
DNA repair Misrepair Genomicinstability
Normal cell growth Abnormal cell growth(cancerhypoplasia) Outcomes
or
Figure 2 DNA damage response can result in different outcomes following single strand breaks interstrand crosslinks and double strandbreaks Each DNA lesion is recognized by specific sensor proteins according to the cell cycle phase in which the cell is during S phase theprotein FANCM identifies a replication fork arrested by an ICL MRN + BRCA1 sense DSBs meanwhile Ku70Ku80 + 53BP1 can recognizeDSBs across the entire interphase RPA detects and covers ssDNA primarily during S phase The sensing process is then transduced andamplified on chromatin through a series of posttranslational histone modifications such as phosphorylation of H2AX (120574H2AX) on both sidesof the DSB These changes allow the recruitment of the specialized transducer kinase ATR that mainly responds to RPA-covered ssDNAoriginated by replication stress or DNA lesions such as ICLs concurrently ATM responds to DSBs Kinases activate several effector proteinsincluding the transcription factor p53 which acts downstream regulating diverse outcomes according to the type and quantity of remindinglesions in the cell
in order to repair a DSB using HR alt-NHEJ or SSA the 31015840blunt endsmust be processed to allow the loading of theMRNcomplex (a heterotrimer integrated by three proteins calledMRE11 RAD50 and NBN) to continue the repair processThis occurs primarily during the S and G2 phases of the cellcycle when sister chromatids are available and can be usedfor HR error-free repair [7 9]
3 DNA Damage Response
Even when each specific DNA lesion stimulates a particularDNA repair mechanism cells trigger a common generalprogram known as the DNA damage response (DDR) whichis charged with lesion detection signaling and repair pro-motion as well as cell cycle progression control It is nosurprise that the DDR is an extremely controlled process theexquisite balance between cell survival and cell death and
senescence relies on it [1 9 10] Tissue homeostasis or growthabnormalities such as cancer [11] or tissue hypoplasia dependamong other things on the amount and type of genomicdamage sensed and processed by the DDR
The DDR is composed of a network of regulatory non-coding RNAs and proteins that act as sensors transduc-ers and effectors [1 12] Sensor proteins recognize specificlesions (Figure 2) For example the FANCM protein detectsthe stalled replication fork caused by interstrand crosslinks(ICLs) theMRNcomplex is the typical sensor ofDSBs duringSG2 phase the Ku70Ku80 heterodimer is the primary DSBssensor duringG1while replication proteinA (RPA) overcoatssingle-strand DNA (ssDNA) found either at processed DSBoverhangs to be repaired by HR or at stalled replication forks[13]
Following recognition of the lesions by sensors andmediators the signal is amplified by transducer proteins
4 BioMed Research International
Table 1 Chromosomal instability syndromes with intrauterine growth deficiency
Syndrome Genes Function in DDR Repair pathway Cytogenetic alteration
Fanconi anemia 21 FANC genes
ICL detection andprocessing generation ofadducts and DSBs (sensorsmediators and effectors)
Homologous recombination Chromatid and chromosomal breaksRadial figures
Seckel Syndrome 1 ATRSSBs detection and signaltransduction(transducer)
Homologous recombinationNonhomologous recombination
Chromatid and chromosomal breaksandRearrangements
Nijmegen BreakageSyndrome NBN
DSBs detection andsignaling (sensor andmediator)
Homologous recombinationNonhomologous recombination
Chromatid and chromosomal breaksAneuploidiesRearrangements affectingchromosomes 7 and 14
Bloom Syndrome BLMHelicase process SSBs andHolliday Junctions(effector)
Homologous recombination QuadriradialsIncrease in sister chromatid exchange
The PIKK kinases (Phosphatidyl Inositol 3-Kinase-relatedKinases) family is the most important of this group it isintegrated by ataxia telangiectasia and Rad3-related (ATR)Ataxia telangiectasia-mutated (ATM) and DNA dependentprotein kinase (DNAPKcs) ATR is activated during the Sphase of the cell cycle in the presence of DNA damagesuch as base adducts crosslinks single-strand breaks (SSBs)replication stress andDSBs that originate during the S phasewhile ATM and DNAPKcs are activated by DSBs at anypoint of the cell cycle [13 14] The DDR kinases activatesignaling cascades through posttranslationalmodifications ofvarious proteins including phosphorylation ubiquitylationand PARylation which play a central role in regulation ofthe DDR [15] Specifically ATR and ATM can autoactivate ortransactivate each other through phosphorylation and thenphosphorylate the histone variant H2AX (120574H2AX) that actsas a platform to recruit DDR factors and prepare the cell torestore DNA integrity ATR and ATMrsquos main downstreamphosphorylation targets are proteins Chk1 and Chk2 andthe important effector p53 their activation allows regulating(a) the chromatin structure surrounding the lesion (b)checkpoints that stop the cell cycle (c) DNA repair proteins(d) proteins that induce senescence and (e) proteins that leadto cell death (Figure 2) [10 16]
Finally if DNA lesions are repaired the checkpoint that isresponsible for stopping the cell cycle is turned off and the cellcycle is allowed to restart through a process called checkpointrecovery This process is only turned on when the signalingfor theDNA lesions is silenced and the surviving cell recoversits normal homeostasis and growth When DNA damagecannot be properly repaired the cellrsquos destiny should beeither senescence or death Otherwise cellsmight dividewithunrepaired DNA damage through an erroneous activation ofthe checkpoint recovery process that allows cell survival withgenomic instability to promote cell dysfunction and cancer[17]
4 DNA Damage Response and Disease
Unrepaired or misrepaired lesions in DNAmay immediatelyimpair replication and transcription affecting the whole cell
function In an irreparable damage situation the amountand type of lesions as well as the cell cycle phase in whichthe cell is will influence the DDR response in order tofavor immediate cell death or the conversion of DNA lesionsinto durable mutations or stable chromosomal abnormalities[3]
Cell survival despite genomic damage can directly affectcell growth this can be evidenced by two opposite outcomesOn the one hand there can be an overgrowth effect sincemutations in critical genes such as oncogenes or tumorsuppressor genes can alter cell function and increase thelikelihood of cancer development [3 18 19] On the otherhand there can be cell hypoplasia or cell loss this happenswhen irreparable damage leads to either cell death or cellsenescence a cancer-protecting condition in which cellsare alive but unable to proliferate limiting the growth ofthe tissues and conducting to aging (Figure 2) This isevidenced by the phenotype of patients affected by diseasesthat alter the DDR and DNA repair in which growthalteration and increased cancer susceptibility are importantfeatures
5 Chromosome Instability Syndromes
Mutations in at least 114 genes involved in the DDR leadto disease some of the mutations are somatic resulting invarious types of spontaneous cancer and others are geneticdiseases with constitutionalmutations that lead to syndromesthat may or may not be related to the development ofcancer [10] Among the genetic diseases with mutations inDDR genes the chromosomal instability syndromes (CIS)are a group of rare Mendelian diseases characterized byincreased chromosome breakage resulting from unrepairedor misrepaired DNA strands breaks Other than chromoso-mal instability they also have clinical overlapping featureslike cancer proneness premature aging and growth abnor-malities even though each CIS has a particular phenotypethat distinguishes it from the others Only a subgroup of thesepatients has prenatal growth alterations this review focuseson those syndromes (Table 1)
BioMed Research International 5
6 DDR Alteration and Growth Failure
Historically disruption of the DDR has been associatedwith cell growth abnormalities in a unilateral way alwayspointing towards the increased cell number in the form ofderegulated cell proliferation in cancer [19] But there islittle information on how DDR alterations can also lead toderegulation of growth in the opposite direction resultingin lack of growth due to cell death and low cell repro-duction One of the first observations to partner growthdeficiency with an altered DDR was the finding that someSeckel syndrome patients (SS) a rare phenotype consistingof primordial dwarfism and microcephaly had mutationsin the ATR gene which encodes the ATR kinase a DDRtransducer Further analysis of SS patients revealed locusheterogeneity for this phenotype mutations in other genesrelated to DDR or DNA repair also led to this clinical pictureThis observation has reinforced the association betweenDDRfailure and severe intrauterine growth retardation Moreovergenes that participate in centrosomal biology are also relatedto the uncommon phenotype of microcephalic primordialdwarfism suggesting that centrosomes have a central rolefor the adequate differentiation of early neuroprogenitorsIt has then been proposed that failure in cell proliferationsecondary to abnormal mitosis is the cause of primordialdwarfism since the multipolar spindles result in the acti-vation of checkpoints reducing proliferation and activatingapoptosis [20]
For the phenotype of growth restriction to be evidentprenatally the mechanisms regulating growth must be com-promised from the beginning of the development in embry-onic stem cells (ESCs) which are pluripotent cells derivedfrom the three primary germ layers ectoderm endodermandmesoderm and that have the capacity to differentiate intomore than 200 cell typesThese cells have been proven to havean extremely efficient DDR and proficient DNA repair mech-anisms that allow for a rigorousmaintenance of their genomeintegrity otherwise unrepaired DNA damage in ESCs wouldbe amplified affecting normal human development
ESCs have an extremely active proliferation rate theircell cycle has a characteristically reduced G1 phase andrepair mechanisms are heightened When comparing ESCsto fibroblasts it stands out that MMR is enhanced BERand NER repair pathways are highly competent and therepair of DSBs is preferentially made through the reliableHR pathway [21] Moreover when HR is not available andDSBs accumulate apoptosis is the preferred route to removehighly damaged cells It is interesting that DSB repair inESCs requires signaling through ATR instead of ATM ESCshave a special mechanism to deal with DNA damaged cellswhen inefficient DNA repair or DDR affects the induction ofapoptosis or autophagy [22] This mechanism leads to ESCdifferentiation that is driven by damage-induced expressionof the p53 transcription factor damaged differentiated cellsare efficient in cell cycle arrest and apoptosis This strategyresults in the maintenance of genetic stability in a decreasednumber of ESCs and a portion of differentiated cells thatbecome senescent both resulting in growth deficiency[21]
Growth deficiency is at the center of many diseasesincluding extremely low body size In mammals overall sizeis determined by the number of cells body mass is then thesum of all the cells that have proliferated minus those thathave died A fetus that is growing harmonically has accuratebalance between these two processes failure of either one ofthese results in dramatic effects when they occur in the ESCpopulation a decrease in cell proliferation rate or an increasein apoptosis leads to intrauterine growth retardation (IUGR)[23]
7 Chromosome Instability Syndromes withIntrauterine Growth Retardation
71 Seckel Syndrome Seckel syndrome (SS) is an autosomalrecessive disorder clinically and genetically heterogeneousSo far at least six genes have been associated with the Seckelphenotype most of these genes participate in ATR-mediatedDDR and in centrosomal function Two clinical subgroupscan be identified on the one hand patients with mutationsin ATR NIN and ATRIP genes only present the Seckelphenotype while on the other hand those with mutationsin CENPJ CEP152 or RBBP8 show allelic heterogeneity andbesides the SS phenotype can also manifest as a spectrumof disorders known as Primary Autosomal Recessive Micro-cephalies [24ndash28] SS patients who bear mutations in ATRshow a classical Seckel phenotype the SS data presented herewill be limited to such patients
ATR is localized in 3q23 it is one of the serine threoninekinases that belong to the PIKK family They have a funda-mental role in the DDR since they participate as transducersin the signaling of DNA lesions especially when the DDRresponds to stalled replication forks and bulky lesions inDNA[24 25] ATR responds preferentially to ssDNA during the Sphase It also plays a crucial role in preventing DNA breakscaused by fork pausing when DNA replication machineryfinds DNA lesions or complex DNA structure and sequences[24] ATR stability depends on binding of ssDNA to theATR cofactor ATRIP (ATR interacting protein) and thesingle-stranded binding protein (RPA) ATRIP is required forATR localization to the ssDNA regions and hence for ATRactivation [25 27] Major functions of ATR are activation ofcell cycle check point arrest stabilization of stalled replicationforks and promotion of replication fork restart which isachieved through its ability to phosphorylate a wide range ofsubstrates that include p53 and H2AX [27 29]
Cellular phenotype of ATR deficient cells is characterizedby decreased phosphorylation of ATR-dependent substratesas well as an impaired G2M checkpoint arrest These cellsare characterized by markers that signal unrepaired DSBslike the presence of 120574H2AX chromosomal breakage [2629 30] and micronuclei formation This cellular phenotypemay be originated by a failure to recover from replicationstalling which generates DSBs that are normally repairedby HR when they occur during SG2 In SS cells theabsence of ATR is critical during embryonic developmentthis deficiency leads to genomic instability cell senescenceand cell death that leads to fetal growth and accelerated aging[31]
6 BioMed Research International
Figure 3 Seckel syndrome patient Note the severe microcephalyand the ldquobird-likerdquo appearance facies with micrognathia and reced-ing forehead The patient is severely disabled with no independentmarch
Moreover it appears that ATR and the other SS genes notonly participate in the DDR but also take part in the controlof centrosome maturation This engagement in centrosomebiology is also true for other DDR proteins like BRCA2biallelic mutations in its gene are responsible for a subgroupof Fanconi anemia patients [32]Theunifying feature betweenall Seckel patients irrespective of the molecular defect isthat their cells have an altered cell cycle progression thatis particularly evident during high rate cell division whenthere is hypersensitivity to replicative stress and centrosomaldysfunction This is especially important in cells with highdivision rates like the ones found in developmental stageswhere rapid replication is key [24 27]
SS is characterized by IUGR dwarfism microcephaly(below minus4 SD) mental retardation and some other anomalieslike luxation of the head of the radius scoliosis bone agedelay and seizures (Figure 3) The distinctive facial featuresinclude a prominent nose with micrognathia and a recedingforehead resulting in a ldquobird-like appearancerdquo [26 31 33]Since this syndrome has important clinical heterogeneityother anomalies have been reported including mandibularhypoplasia sternal abnormalities clinodactyly and low setears with hypoplastic lobules Although rare other reportedfeatures are moyamoya syndrome osteosarcoma and pol-yarteritis nodosa [26] Cerebral malformations like neuronalmigration abnormalities have been described but are notalways present [33] No glucose metabolism abnormalitieshave been reported
Dwarfism can be related to a reduction in the totalnumber of cells generated during development leading tohypoplastic tissue and reduced organism size [23] On theother handmicrocephalymay be related to an impairedDNAdamage response signal that could alter the cellular thresholdfor cell death resulting from DNA damage increasing thelevels of apoptosis during development developing neuronsare rapidly proliferating and potentially generate high levelsof oxidative damage which may lead to a higher level oflesions being faced at replication forks [23 25] Also analtered mitosis secondary to impaired spindle formationcould delay mitotic progression and increase the proportionof nonviable cell divisions Finally the stem cells may beaffected by abnormal centrosomal function Stems cells haveasymmetric divisions in order to preserve the characteristics
Figure 4 Fanconi anemia patient This six-year-old girl is 105 cmtall her height is just below the 5th percentile and her at-term birthweight is reported to be of 1900 gr Characteristic features of FA areevident skin hyperpigmentation bilateral radial defects consistingof bilateral thenar hypoplasia and absent fold of the right thumbwhich cannot be bent
of a stem cell and the centrosomes play an important role insuch divisions [23]
There is limited clinical information regarding age-related diseases in SS there is a void of prospective follow-up data from these patients that can only be obtained byfollowing a cohort of SS patients something that is apparentlynot being done at this time Nevertheless animal modelsbring some clues over the possibility of an aging phenotypein SS patients since ATR deficient adult mice show prematureage-related phenotypes as well as increased deterioration oftissue homeostasis [29 34]
72 Fanconi Anemia DNA interstrand crosslinks are ex-tremely noxious DNA lesions that affect central cellularprocesses like transcription and replication The FABRCApathway is responsible for the appropriate processing ofthese lesions protein products from at least 21 FANC genesparticipate in this pathway [35] The malfunction of any ofthose FANC proteins leads to the clinical phenotype knownas Fanconi anemia (FA) which is characterized by shortstature congenital malformations from the VACTERL-Hspectrum bone marrow failure and an increased suscepti-bility to cancer like acute myeloid leukemia epithelial headand neck cancer [36] (Figure 4) Most of the FA families bearbiallelic mutations in FANC genes that have an autosomicrecessive inheritance pattern only families with mutations inFANCB show an X-linked recessive pattern while those inwhich FANCR is the affected gene demonstrate an autosomicdominant one [35]
The FABRCA is an S-specific pathway that has 3 basicsteps it starts with the detection of the ICL by the proteinFANCM followed by the recruitment of the FA core com-plex that is responsible for the monoubiquitination of theFANCD2I heterodimer which in turn favors the recruit-ment of effector FANC-repair proteins that restore the DNAto its original form [35]
BioMed Research International 7
(a) (b)
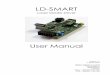
Figure 5 Chromosomal instability induced by 40 ngml mitomycin C (a) Lymphocytes from a healthy individual (b) lymphocytes from aFA patient Short arrows show chromosomal breaks the long arrow shows a quadriradial figure Note the exacerbated chromosome instabilityfound in the FA patient
The cellular phenotype of FA derived cells is extremelyconstant An aberrant FABRCA pathway can result inunrepaired DSBs that manifest as chromosomal breaks orabnormal repair by an error-prone repair pathway that resultsin radial figures These alterations are cytogenetic evidenceof chromosomal instability which is the hallmark of FA cellsand is exploited for clinical diagnostic purposes (Figure 5)The agents capable of inducing this chromosomal instabilityare from endogenous origin like aldehydes [37] and reactivespecies of oxygen (ROS) [38] as well as exogenous sourceslike bifunctional alkylating agents (diepoxybutane or mito-mycin C) In addition FA cells have accumulation of cells inG2 phase of the cell cycle resulting from a functional G2Mcheckpoint and a proapoptotic phenotype
In contrast with the cellular FA phenotype the clinicalpicture in FA patients is extremely variable not every patientwill have all the manifestations one-third of patients do nothave congenital malformations [39] while almost 90 willdevelop bone marrow failure [36] One of the more constantmanifestations in FApatients is growth parameters alterationAn analysis from the international Fanconi anemia registry(IFAR) data showed that over 60 of FA patients presentedshort stature (below the 5th percentile) while birth lengthandweight below the 5th percentile was respectively reportedin almost 30 and nearly half of FA patients [40]Moreover aprospective study of data from 54 IFAR participants showedthat the mean standard deviation score (SDS) for height inthese patients was significantly below normal for age and sexat minus235 plusmn 028 meanwhile mean SDS for weight was betteralthough below normal (minus126 plusmn 024) In this study perinatalgrowth data was not reported [41]
Other than the IFAR data on growth there are anothertwo studies that analyze growth parameters of FA patientsAnthropometric measurements from 45 patients with Fan-coni anemia from the National Cancer Institutersquos inher-ited bone marrow failure syndromes (IBMFS) cohort wereassessed This cohort had a mean SDS for height of minus21 plusmn
189 The height of over half of the participants (54) wascategorized as short (SDS gt 20 SD) in this subset of patientsthe mean SDS for height was minus38 plusmn 15 [42] Finally theevaluation of 120 FA patients from the FA ComprehensiveCare Clinic of Cincinnati Childrenrsquos Hospital Medical Centerrevealed that median height SDS was shorter than expectedin children and adults irrespective of gender Furthermorethis study presented birth information from 70 patients (59children and 11 adults) from the cohort 51 of the childrenand 3 adults were born small for gestational age their medianbirth weight at term was 202 kg (range 15ndash26 kg) [43] Theintrauterine growth restriction seen in FA patients has alsobeen documented in several case reports in which at-termbirth weight ranges from 1780 to 3200 gr [44ndash49] Eventhough growth abnormalities have been identified in FApatients with mutations in almost every FANC gene it hasbeen shown that patientswithmutations in certain genes havea more severe growth delay That is the case for patients withbiallelic mutations in FANCD1 [47 48] as well as those whobear mutations in FANCC for whom an SDS for height ofminus384 has been found [41]
Endocrine abnormalities have been proven to be aninherent part of the FA phenotype up to 80 of patientshave one or more endocrine abnormalities Besides growththyroid function and glucose homeostasis are frequentlyaffected [40ndash43] Considering the existing evidence for arelationship between low birth weight and an increased riskfor noncommunicable adult diseases like diabetes hyperten-sion heart disease dyslipidemia and osteoporosis [50] it isrelevant to revise these diseases in FA The FA cohorts inwhom growth was assessed were also evaluated for endocrinestatus Glucose homeostasis is affected in a large portion ofFA patients impaired glucose tolerance has been found in27ndash68 of them whereas diabetes has a prevalence of 8ndash10Dyslipidemia has been assessed in only a small portionof FA patients but it has been found in 17ndash55 of theevaluated subjects [51]There are conflicting results over bone
8 BioMed Research International
mineral density (BMD) status in FA the first time this wasevaluated 92 of the patients were found to have osteopeniaor osteoporosis [42] nevertheless a study that evaluated alarger FA cohort found that lowBMD is not a frequent finding[52] Further research on this topic has raised the questionof whether BMD deficit is intrinsic to the FA phenotype ora consequence of hematopoietic cell transplantation (HCT)an interrogation that is still awaiting to be answered [53]Cardiovascular adult diseases are not relevant in the FA phe-notype heart disease in these patients is from the congenitaltype as 13of patients have cardiacmalformations [40] whilehypertension has only been reported in two patients as theresult of renal malformations [54]
Findings from the different FA cohorts show that shortstature is an inherent feature of the FA phenotype thisfeature does not respond to a single explanation the apoptosisprone FA cellular phenotype is certainly a contributing factorfor this The fact that FA patients have a constitutionallydefective pathway since conception could explain the clinicalphenotype of RCIU Short stature may also be exacerbated byaccompanying endocrinopathies The cooccurrence of manyendocrine alterations has encouraged unifying explanationssome have proposed that endocrinopathies are secondaryto increased cytokine activity found in FA cells [41] whileothers favor the view that some endocrine secretory cellsmight be damaged by high levels of reactive oxygen specieswhich are known to be elevated in FA patients [43] In linewith the developmental origin of adult health and diseasetheory it could also be possible that the increased prevalenceof glucose homeostasis alterations and dyslipidemia reportedin FA patients is a consequence of intrauterine growthrestriction of these patients Nevertheless the attemptedgenotype-phenotype correlation of the endocrine phenotypein FA patients does not seem to support that Patients withmutations in FANCA show a mild endocrine phenotype inwhich height is not severely affected and insulin resistanceis mild whereas mutations in FANCC which are relatedto shorter stature have the least insulin resistance [41]Moreover no direct relationship between birth weight andglucose tolerance was identified when it was intentionallylooked for [43] although the number of patients in whichthese observations were made is limited
73 Nijmegen Breakage Syndrome Nijmegen breakage syn-drome (NBS) is an autosomal recessive disease caused bybiallelic mutations in NBN a gene that encodes nibrin aprotein involved in DNA repair and cell cycle checkpointregulation It participates in the former by sensing double-strand breaks as part of the trimeric complexMRN alongsideMRE11 andRAD50Meanwhile for the latter it contributes tothe appropriate activation of ATM andATRwhich are centraltransductors of the DNA damage response (DDR) [55] Themalfunction of nibrin translates in a cellular phenotypemarked by chromosomal instability radiosensitivity reducedphosphorylation of ATM substrates and S and G2M cellcycle defects [56] Chromosome instability is evidenced bycytogenetic methods in 10ndash60 of cells in the form of breaksand numeric and structural aberrations translocations andinversions affecting chromosomes 7 and 14 are found in the
147
Figure 6 Translocation between chromosomes 7 and 14 is typicalin NBS patientsrsquo cells
majority of NBS patients and are considered a cytogeneticcharacteristic of this syndrome (Figure 6) [57]
The clinical impact of these alterations is a phenotypecharacterized by microcephaly a distinctive facial appear-ance consisting of receding forehead and mandible and aprominent mid face with a long nose and philtrum aswell as immunodeficiency that leads to recurrent infectionsand an increased risk for the development of neoplasiaparticularly leukemia and lymphoma According to theinternational Nijmegen breakage syndrome study groupgrowth retardation is also a hallmark of this disease [58]although there is not many details about this feature in theliterature
Most of the information on the natural history of NBSavailable today comes from patients participating in reg-istries in which fairly large cohorts of NBS patients areincluded There is a large representation of Slavic patientsin these cohorts which correlates with the high carrierfrequency of a founder mutation of NBN in this populationFrom these studies it is evident that the most severelyaffected anthropometric measure in NBS patients is headcircumference since all participants display microcephalyeven though only 75 display this feature at birth Whenit comes to growth parameters the same study states thatall patients have growth retardation which is described asproportionate and early occurring [58] although the specifictemporality is not defined A posterior report points out thatthe growth retardation seen in most NBS patients locatesthem in the 10th percentile in growth charts and that birthheight and weight are usually within normal parameters [59]Nevertheless there are other authors who report prenataland postnatal growth retardation [55 60] and a tendency forshort stature that is more evident during the first year of life[61] Also several case reports of NBS patients in which birthweight is informed demonstrate prenatal growth restriction[62ndash67] although this could represent a report bias Themore comprehensive data analysis on growth that includesperinatal information of NBS patients is the one that analyzesdata from 67 patients followed for 15 years Eighty percentof these patients were born at term the girls were found tohave a mean birth weight of 27 kg and mean birth heightof 514 cm while boys were reported to have a mean birthweight of 28 kg and mean birth height of 523 cm Moreoverall patients irrespective of gender were found to have ameanheight reduced by over 2 SDS at one year old [57] These data
BioMed Research International 9
(a) (b)
Figure 7 Sister chromatid exchange in cells from a healthy individual (a) and from a BLM patient (b)
support the fact that growth retardation in NBS is a prenatalphenomenon
Nibrin has been found to have essential functions inthe regulation of the cell cycle which translates into anabsolute need for this protein for cell proliferation [68]It would seem logical that mutations of the NBN genethat compromise the appropriate function of nibrin wouldlead to abnormal growth when thought from an organismperspective Mechanistically speaking poor cellular growthcaused by mutations in a particular gene can be thought ofas the main explanation for the growth restricted phenotypebut it has been shown that mutations in other DDR genesthat share the cellular phenotype of poor growth like ATMdo not replicate the compromised growth phenotype atthe organism level growth retardation is absent in ataxiatelangiectasia (AT)This data suggests that there are certainlyother contributing factors to the abnormal growth phenotypeseen in NBS patients [58]
74 Bloom Syndrome Bloom syndrome (BS) is an autosomalrecessive disorder caused by homozygous or compoundheterozygous mutations in the BLM gene (15q261) thatencodes the RecQL3 helicase BLM has a critical role inthe maintenance of genome stability acting at the interfacebetweenDNAreplication recombination and repair [69 70]To date over sixty different mutations including nonsenseand missense have been identified all of them result inthe inactivation of BLM and the consequent loss of itshelicase activity The BLM gene encodes a 1417 amino acidnuclear protein its expression peaks during the S and G
2M
phases of the cell cycle which is consistent with its rolein DNA replication and recombination BLM specificallyunwinds structures like forked DNA duplexes RNA-DNAheteroduplexes and R-Loops which explains its importanceduring replication fork progression and transcription besidesit is central for Holliday Junctions (HJs) dissolution forHR The dissolution of HJs by the topoisomerase III120572-BLMcomplex cannot be replaced by any other RecQ helicase inthe family [69 70] It has also been found to have a role in
the annealing activity of the ssDNA the proper sister chro-matid segregation during mitosis and telomere maintenance[70]
BLM can have both pro- and antirecombinogenic func-tions that are regulated by posttranslational modificationsincluding phosphorylation sumoylation and ubiquitination[70]
BLM also enables sister chromatid segregation by pro-cessing unresolved replication intermediates that manifest inmitosis as ultrafine DNA bridges (UFBs) and together withtopoisomerase III120572 RMI1 and RMI2 localizes to UFBs inanaphase BML deficient cells exhibit and increase frequencyof UFBs suggesting a role of BLM in the resolution ofthese structures Failure to resolve these UFBs leads to DNAbreakage as mitosis proceeds [70]
Therefore BS cells are characterized by an increasein chromosomal aberrations including chromatid gapsand breaks telomere associations and quadriradial chro-mosomes resulting from unsolved recombination betweenhomologous chromosomes BS cells exhibit increased muta-tion rates and the genomic instability includes elevatedmitotic HR and unequal sister chromatid exchange (SCEs)(Figure 7) Perhaps the most characteristic feature is the overtenfold increase in SCEs which results from crossover eventsduring HR repair of damage replication forks [50 69 70]
Clinically the more striking BS feature is IUGR averagebirth weight at term is 1850 g and birth length is 44 cmFor both boys and girls weight and length in BS are morethan two standard deviations below normal indicating thatgrowth retardation has a prenatal origin At postnatal agesheight remains below the normal range and is accompaniedby a paucity of subcutaneous fat Average adult height inmales has been found to be 148 cm (130ndash162 cm) whilein females it has been reported to be 139 cm (122ndash151 cm)[50 70 71]
BS patients have overall proportionated short staturebut the head is reported to be small and narrow relativelyto the body size it is described as mild microcephalyand is accompanied by malar hypoplasia Patients have
10 BioMed Research International
Figure 8 Bloomsyndromepatient inwhom the characteristicmalarerythema is present
been described to have a high pitched voice [50 70] Theskin appears normal at birth but in the first or secondyear of life in response to sun exposure children developan erythematous rash with a butterfly distribution in themalar area and the back of hands and feet The rash caninclude telangiectasia The severity varies between patientssome can even lose their eyelashes and develop blisteringaround the mouth The presence of cafe-au-lait spots andhypopigmented areas of skin associated with contiguoushyperpigmented areas is common (Figure 8) Intellectualabilitiesmay be limited in some patients and normal in others[50 70]
Other clinical conditions reported in BS patients are gas-troesophageal reflux and diarrhea in infants mild immuno-logical deficiency with frequent episodes of otitis mediaazoospermia or severe oligospermia in males and prema-ture cessation of menstruation in females minor anatomicdefects and increased risk for neoplasia which is the maincause of dead in BS [70] Another common medical con-dition in BS is diabetes mellitus associated with impairedglucose tolerance and insulin resistance it has been reportedin up to 16 of patients [70] According to data fromthe Bloomrsquos Syndrome Registry diabetes in these patientstends to begin early with a mean age at diagnosis of 266years It is not associated with ketosis and it does nothave the classical hereditary pattern seen in type 2 diabetes[50 72]
Short stature in BS is not due to hormonal causes sincethe size of cells in persons with BS is normal it has beenhypothesized that there are fewer of them due to either adecrease in the cell division rate an increase in apoptosis oreven a combination of both BS cells have troublemeeting thedemands of fast cell divisions encountered in tissues duringembryonic development The leading hypothesis suggeststhat problems arising during DNA synthesis require a longerS phase to overcome the challenge which translates intoslowing of the cell division rate and an increase in apoptosis[70]
8 Concluding Remarks
This review has focused on discussing phenotypes of CISin which there is a prenatal alteration of growth The foursyndromes discussed here are rare diseases whose prevalenceis difficult to calculate since appropriate identification anddiagnosis of affected individuals among the general popula-tion are not straightforward It is important to note that theavailable information on the natural history of FA NBS andBS comes from the analysis of several patients that participatein registries This strategy results in detailed informationthat permits a better analysis of the clinical phenotype ofthese rare diseases Meanwhile available data of SS is moreanecdotic which results in a nonsystematic gathering ofinformation which is thus frequently incomplete
From the available clinical data of these CIS it is evidentthat growth is not affected in the same extent for all ofthese syndromes the phenotypes that exhibit a more severelystagnated perinatal growth are BS and SS The severe growthdelay reported in these patients has been described as apathognomonic sign of these diagnoses In patients withFA perinatal growth can also be severely affected but notevery FA patient shows this manifestation Finally NBShas been described to have growth retardation of prenatalorigin of mild severity almost within the lower normal range(Figure 9) The cephalic circumference can be affected in allof these syndromes severe microcephaly is pathognomonicin SS and NBS it is described as mild for BS patients and it isfound in less than half of FA patients (Table 2)
When trying to understand why a subset of CIS showsprenatal growth retardation it could be alleged that theintrinsic chromosomal instability is responsible for it Butthis would not explain why prenatal growth retardation isnot a universal CIS feature for example ataxia telangiectasiapatients who have biallelic mutations in the ATMkinase genedo not show prenatal growth delay It strikes that a molecularcommon feature shared by the prenatal growth retardationSIC phenotypes is that they are caused by mutations ingenes that are necessary for an appropriate response to DSBsduring the S phase of the cell cycle The molecular defectin SS affects the functioning of ATR the preferred DDRtransducing kinase used by highly replicating ESCs TheFABRCA pathway which is affected in patients with FAdetects ICLs upon replication fork arrest Nibrin the proteinaffected in patients with NBS is induced during S phasefor the detection of DSBs And the BS helicase forms aFANCM-BLM complex needed to sense ICLs during S phase[73] It could then be argued that altered DNA replicationis an important factor for the development of intrauterinegrowth restriction in these CIS Nevertheless it must be keptin mind that the inherent chromosome instability found inthese syndromes may also be affecting normal growth in thepatients [27 43 57 60 71]
Being small for gestational age has been associatedwith a higher risk of noncommunicable adult diseases likeglucose homeostasis disorders dyslipidemia hypertensionand others It has been proposed that fetal reprogrammingto enhance fetal survival despite the risk for adult onsetdiseases is an outcome that does not take into account
BioMed Research International 11
Table 2 Growth features of chromosomal instability syndromes
SyndromeldquoLocirdquo At-term birth weightheight Microcephaly Adult height Adult onset diseases
Seckel SyndromeldquoATR3q23rdquo
Birth weight below minus3 SD(2055 g)
Severeminus4 SD
Postnatal growth retardation(below minus5 SD) Not reported
Fanconi anemialdquo21 FANC genesrdquo
Median weight 202 kg(15ndash26 kg) In 20ndash50
50ndash60 of patients with medianheight lt minus18 SDSWomen minus34 SDSMen minus44 SDS
CancerDiabetes mellitusDyslipidemia
Altered bone mineral densityNijmegen BreakageSyndromeldquoNBN8q21rdquo
Mean weightheight girls27 kg514 cm
Mean weightheight boys28 kg523 cm
100 Mean height for women minus18 SDSMean height for men minus23 Cancer
Bloom SyndromeldquoBLM15q261rdquo
Mean weight 189 kg plusmn 035 kg forboys
Mean weight 187 kg plusmn 035 kg forgirls
Mean height 434 cm plusmn 44 cm forboys
Mean height 438 cm plusmn 28 cm forgirls
Mildmicrocephaly
Mean height 1455 cm plusmn 76 cmmales
Mean height 1415 cm plusmn 61 cm forfemales
CancerDiabetes mellitus
See [27 33 40 43 50 57 69]
45 53
43245
Height (cm)
Weight (kg)
Percentile 3 Percentile 97Percentile 50495
33
Normalindividual
Mean 2055
SeckelSyndrome
2615Median 202
FanconiAnemia
Mean 51
Mean 275
Nijmegen BreakageSyndrome
38 49
24513
Mean 436
Mean 188
BloomSyndrome
Figure 9 Anthropometric features at birth of chromosome instability syndromes with perinatal growth retardation Comparison of theavailable growth data from SS FA NBS and BS syndrome against birth data from the WHOrsquos growth standards for infants Although meanheight and weight values of NBS patients are found to be within normal percentiles according to WHO standards there are several authorswho refer to prenatal growth restriction [55 63 65 79]
the reason for the prenatal growth restraint [50 72 74] Itmust be kept in mind that noncommunicable diseases aremultifactorial entities in which genetic and environmentalfactors converge and their cause cannot be attributed to asingle explanation However when growth restriction is akey feature in syndromes with chromosome instability the
possibility that cell hypoplasia due to DNA repair malfunc-tion is contributing to the growth restriction phenotypemustbe contemplated Moreover since none of these adult onsetdiseases is reported as an inherent element of the SS and NBSphenotypes the direct connection between low birth weightand adult noncommunicable diseases is less of a straight
12 BioMed Research International
shot Furthermore there are other Mendelian syndromeswith mutations in DNA repair genes that characteristicallyshow adult noncommunicable diseases but do not haveIUGR such is the case for Werner syndrome a progeroiddisease caused by biallelic mutations in another RecQ heli-case (RecQ4) that clinically presents with postnatal shortstature and a prevalence of type 2 diabetes mellitus of 70[50 70 74]
Natural history of FA NBS and BS documented throughthe existing patient registries has allowed the identificationof noncommunicable diseases to be a part of the clinicalspectrum of these syndromes (Table 2) Meanwhile from theinformation available through SS case reports no adult onsetdisease has been found to be part of this phenotype To thebest of our knowledge the direct investigation of nonevidentendocrinologic alterations like glucose homeostasis or dys-lipidemia has not been directlymade in SS patients For a raredisease like SS such a study can only be done if a fairly largegroup of patients like the one found in registries is availableIf such a study was to be performed hidden features in SSpatients could be unraveled
Oxidative stress sensibility is a cellular feature sharedby all the SIC syndromes with IUGR that could contributeto the explanation of the premature development of non-communicable adult diseases in these patients Reports haveshown that BS and NBS cells have endogenous reactiveoxygen species (ROS) overproduction and an impairedmitochondrial homeostasis [75] it is also well known thatFA cells show increased levels of oxidative damage [3876] and there is evidence that oxidative stress can activateATR-mediated checkpoint signaling [77] Since this kind ofdamage has soundly been related to age-associated diseasesthat result from tissue degeneration exacerbated oxidativedamage found in these syndromes could result in cellu-lar aging that manifests as overall premature aging withparticular symptoms like glucose homeostasis alterations[76 77]
Fetal growth restriction is a multifactorial conditionwhere wide arrays of factors converge Fetal aspects inparticular those affecting the genetic constitution of thefetus have been recognized to play an important role Ithas been demonstrated that chromosomal abnormalities andmonogenic syndromes caused by mutations in genes thatparticipate in growth or metabolic pathways directly affectfetal growth [78] Even though they are rare entities CISappear as another group of monogenic pathologies thatbroaden the list of genetic fetal factors of fetal growthrestriction
Consent
The necessary consent for the publication of the photographswas obtained
Conflicts of Interest
The authors declare that there are no conflicts of interestregarding the publication of this paper
Authorsrsquo Contributions
The three authors contributed equally andwrote the first draftof the paper The final version was approved by everyone
Acknowledgments
This paper is supported by SEP-CONACYT Project 243102Benilde Garcıa-de Teresa received the 574025 scholarshipfrom CONACYT The paper is also supported by PAPIIT-UNAM Project IA202615 and Fondos Federales INP Project41-2014
References
[1] K W J Derks J H J Hoeijmakers and J Pothof ldquoThe DNAdamage response The omics era and its impactrdquo DNA Repairvol 19 pp 214ndash220 2014
[2] S P Jackson and J Bartek ldquoThe DNA-damage response inhuman biology and diseaserdquoNature vol 461 no 7267 pp 1071ndash1078 2009
[3] J H J Hoeijmakers ldquoDNA damage aging and cancerrdquo TheNew England Journal of Medicine vol 361 no 15 pp 1475ndash14852009
[4] G Spivak ldquoNucleotide excision repair in humansrdquoDNARepairvol 36 pp 13ndash18 2015
[5] J Vijg XDong BMilholland andL Zhang ldquoGenome instabil-ity a conserved mechanism of ageingrdquo Essays in Biochemistryvol 61 no 3 pp 305ndash315 2017
[6] J I Garaycoechea and K J Patel ldquoWhy does the bone marrowfail in Fanconi anemiardquo Blood vol 123 no 1 pp 26ndash34 2014
[7] R Ceccaldi B Rondinelli andAD DrsquoAndrea ldquoRepair PathwayChoices andConsequences at theDouble-Strand BreakrdquoTrendsin Cell Biology vol 26 no 1 pp 52ndash64 2016
[8] R Biehs M Steinlage O Barton et al ldquoDNA Double-StrandBreak Resection Occurs during Non-homologous End Joiningin G1 but Is Distinct from Resection during HomologousRecombinationrdquo Molecular Cell vol 65 no 4 pp 671ndash684e52017
[9] A Ciccia and S J Elledge ldquoTheDNAdamage response makingit safe to play with knivesrdquoMolecular Cell vol 40 no 2 pp 179ndash204 2010
[10] L H Pearl A C Schierz S E Ward B Al-Lazikani and F MG Pearl ldquoTherapeutic opportunities within the DNA damageresponserdquo Nature Reviews Cancer vol 15 no 3 pp 166ndash1802015
[11] S-F Yang C-W Chang R-J Wei Y-L Shiue S-N Wang andY-T Yeh ldquoInvolvement of DNA damage response pathways inhepatocellular carcinomardquo BioMed Research International vol2014 Article ID 153867 2014
[12] M He W Zhou C Li and M Guo ldquoMicroRNAs DNAdamage response and cancer treatmentrdquo International Journalof Molecular Sciences vol 17 no 12 article no 2087 2016
[13] K A Cimprich and D Cortez ldquoATR an essential regulator ofgenome integrityrdquo Nature Reviews Molecular Cell Biology vol9 no 8 pp 616ndash627 2008
[14] B M Sirbu and D Cortez ldquoDNA damage response three levelsof DNA repair regulationrdquo Cold Spring Harbor Perspectives inBiology vol 5 article a012724 no 8 2013
BioMed Research International 13
[15] C Beck I Robert B Reina-San-Martin V Schreiber andF Dantzer ldquoPoly(ADP-ribose) polymerases in double-strandbreak repair focus on PARP1 PARP2 and PARP3rdquo Experimen-tal Cell Research vol 329 no 1 pp 18ndash25 2014
[16] D W Meek ldquoTumour suppression by p53 a role for the DNAdamage responserdquo Nature Reviews Cancer vol 9 no 10 pp714ndash723 2009
[17] A Rodrıguez L Torres U Juarez et al ldquoFanconi anemiacells with unrepaired DNA damage activate components of thecheckpoint recovery processrdquo Theoretical Biology and MedicalModelling vol 12 no 1 article 11 2015
[18] H Wang X Zhang L Teng and R J Legerski ldquoDNA damagecheckpoint recovery and cancer developmentrdquo ExperimentalCell Research vol 334 no 2 pp 350ndash358 2015
[19] P A Jeggo L H Pearl and A M Carr ldquoDNA repair genomestability and cancer A historical perspectiverdquo Nature ReviewsCancer vol 16 no 1 pp 35ndash42 2016
[20] F S Alkuraya ldquoPrimordial dwarfism An updaterdquo CurrentOpinion in Endocrinology Diabetes and Obesity vol 22 no 1pp 55ndash64 2015
[21] P Fortini C Ferretti and E Dogliotti ldquoThe response to DNAdamage during differentiation pathways and consequencesrdquoMutation ResearchmdashFundamental and Molecular Mechanismsof Mutagenesis vol 743-744 pp 160ndash168 2013
[22] B R Adams S E Golding R R Rao and K Valerie ldquoDynamicdependence on ATR and ATM for double-Strand break repairin human embryonic stem cells and neural descendantsrdquo PLoSONE vol 5 article e10001 no 4 2010
[23] A Klingseisen and A P Jackson ldquoMechanisms and pathways ofgrowth failure in primordial dwarfismrdquo Genes amp Developmentvol 25 no 19 pp 2011ndash2024 2011
[24] H Mokrani-Benhelli L Gaillard P Biasutto et al ldquoPrimaryMicrocephaly Impaired DNA Replication and Genomic Insta-bility Caused by Compound Heterozygous ATR MutationsrdquoHuman Mutation vol 34 no 2 pp 374ndash384 2013
[25] M OrsquoDriscoll A R Gennery J Seidel P Concannon and PA Jeggo ldquoAn overview of three new disorders associated withgenetic instability LIG4 syndrome RS-SCID and ATR-Seckelsyndromerdquo DNA Repair vol 3 no 8-9 pp 1227ndash1235 2004
[26] P Khetarpal S Das I Panigrahi and A Munshi ldquoPrimordialdwarfism overview of clinical and genetic aspectsrdquo MolecularGenetics and Genomics vol 291 no 1 pp 1ndash15 2016
[27] TOgi SWalker T Stiff et al ldquoIdentification of the First ATRIP-Deficient Patient and Novel Mutations in ATRDefine a ClinicalSpectrum for ATR-ATRIP Seckel Syndromerdquo PLoS Geneticsvol 8 no 11 Article ID e1002945 2012
[28] A Verloes S Drunat and P Gressens Primary autosomalrecessive microcephalies and Seckel syndrome spectrum disor-ders 2013
[29] A D Brown B W Sager A Gorthi S S Tonapi E J Brownand A J R Bishop ldquoATR suppresses endogenous DNA damageand allows completion of homologous recombination repairrdquoPLoS ONE vol 9 article e91222 no 3 2014
[30] E J Brown and D Baltimore ldquoEssential and dispensable rolesof ATR in cell cycle arrest and genome maintenancerdquo Genes ampDevelopment vol 17 no 5 pp 615ndash628 2003
[31] B Fitzgerald M OrsquoDriscoll K Chong S Keating and PShannon ldquoNeuropathology of fetal stage Seckel syndromeA case report providing a morphological correlate for theemerging molecular mechanismsrdquo Brain amp Development vol34 no 3 pp 238ndash243 2012
[32] L I Mullee and C G Morrison ldquoCentrosomes in the DNAdamage responsemdashthe hub outside the centrerdquo ChromosomeResearch vol 24 no 1 pp 35ndash51 2016
[33] K M Takikawa A Kikuchi A Yokoyama et al ldquoPerinatalfindings of Seckel syndrome A case report of a fetus showingprimordial dwarfism and severe microcephalyrdquo Fetal Diagnosisand Therapy vol 24 no 4 pp 405ndash408 2009
[34] Y Ruzankina C Pinzon-Guzman A Asare et al ldquoDeletion ofthe Developmentally Essential Gene ATR in Adult Mice Leadsto Age-Related Phenotypes and Stem Cell Lossrdquo Cell Stem Cellvol 1 no 1 pp 113ndash126 2007
[35] N E Mamrak A Shimamura and N G Howlett ldquoRecentdiscoveries in the molecular pathogenesis of the inherited bonemarrow failure syndrome Fanconi anemiardquo Blood Reviews vol31 no 3 pp 93ndash99 2017
[36] B P Alter ldquoDiagnosis Genetics and Management of InheritedBone Marrow Failure Syndromesrdquo International Journal ofHematology vol 2007 no 1 pp 29ndash39 2007
[37] L B Pontel I V Rosado G Burgos-Barragan et al ldquoEndoge-nous Formaldehyde Is a Hematopoietic Stem Cell Genotoxinand Metabolic Carcinogenrdquo Molecular Cell vol 60 no 1 pp177ndash188 2015
[38] G Pagano P Degan M DrsquoIschia et al ldquoOxidative stress asa multiple effector in Fanconi anaemia clinical phenotyperdquoEuropean Journal of Haematology vol 75 no 2 pp 93ndash1002005
[39] P FGiampietro P CVerlander J GDavis andADAuerbachldquoDiagnosis of Fanconi anemia in patients without congenitalmalformations An International Fanconi Anemia Registrystudyrdquo American Journal of Medical Genetics vol 68 no 1 pp58ndash61 1997
[40] P F Giampietro B Adler-Brecher P C Verlander S GPavlakis J G Davis and A D Auerbach ldquoThe need for moreaccurate and timely diagnosis in Fanconi anemia A report fromthe International Fanconi Anemia Registryrdquo Pediatrics vol 91no 6 pp 1116ndash1120 1993
[41] M P Wajnrajch J M Gertner Z Huma et al ldquoEvaluationof growth and hormonal status in patients referred to theinternational fanconi anemia registryrdquo Pediatrics vol 107 no4 I pp 744ndash754 2001
[42] N Giri D L Batista B P Alter and C A Stratakis ldquoEndocrineabnormalities in patients with fanconi anemiardquo The Journal ofClinical Endocrinology amp Metabolism vol 92 no 7 pp 2624ndash2631 2007
[43] S R Rose K C Myers M M Rutter et al ldquoEndocrine phe-notype of children and adults with Fanconi anemiardquo PediatricBlood amp Cancer vol 59 no 4 pp 690ndash696 2012
[44] A D Auerbach B Adler and R S K Chaganti ldquoPrenatal andpostnatal diagnosis and carrier detection of Fanconi anemia bya cytogeneticmethodrdquoPediatrics vol 67 no 1 pp 128ndash135 1981
[45] A D Auerbach M Sagi and B Adler ldquoFanconi anemiaPrenatal diagnosis in 30 fetuses at riskrdquo Pediatrics vol 76 no5 pp 794ndash800 1985
[46] L Faivre M F Portnoı G Pals et al ldquoShould chromosomebreakage studies be performed in patients with VACTERLassociationrdquo American Journal of Medical Genetics vol 137 no1 pp 55ndash58 2005
[47] B P Alter P S Rosenberg and L C Brody ldquoClinicaland molecular features associated with biallelic mutations inFANCD1BRCA2rdquo Journal ofMedical Genetics vol 44 no 1 pp1ndash9 2007
14 BioMed Research International
[48] K Myers S M Davies R E Harris et al ldquoThe clinicalphenotype of children with Fanconi anemia caused by biallelicFANCD1BRCA2mutationsrdquo Pediatric Blood amp Cancer vol 58no 3 pp 462ndash465 2012
[49] B G Yoon H N Kim U J Han et al ldquoLong-term follow-up of Fanconi anemia Clinical manifestation and treatmentoutcomerdquo Korean Journal of Pediatrics vol 57 no 3 pp 125ndash134 2014
[50] J G Hall ldquoReview and hypothesis Syndromes with severeintrauterine growth restriction and very short stature - Are theyrelated to the epigeneticmechanism(s) of fetal survival involvedin the developmental origins of adult health and diseaserdquoAmerican Journal of Medical Genetics Part A vol 152 no 2 pp512ndash527 2010
[51] A Petryk R K Shankar N Giri et al ldquoEndocrine disordersin Fanconi anemia Recommendations for screening and treat-mentrdquoThe Journal of Clinical Endocrinology ampMetabolism vol100 no 3 pp 803ndash811 2015
[52] S R RoseMM Rutter RMueller et al ldquoBonemineral densityis normal in children with Fanconi anemiardquo Pediatric Blood ampCancer vol 57 no 6 pp 1034ndash1038 2011
[53] A Petryk L E Polgreen J L Barnum et al ldquoBone mineraldensity in childrenwith fanconi anemia after hematopoietic celltransplantationrdquo Biology of Blood and Marrow Transplantationvol 21 no 5 pp 894ndash899 2015
[54] R Purkait A Mukherji S Datta and R Bhadra ldquoRenal arterystenosis An unusual etiology of hypertensive encephalopathyin a childwith fanconi anemiardquo Saudi Journal of KidneyDiseasesand Transplantation vol 26 no 4 pp 778ndash782 2015
[55] K H Chrzanowska H Gregorek B Dembowska-BaginskaM A Kalina and M Digweed ldquoNijmegen breakage syndrome(NBS)rdquoOrphanet Journal of Rare Diseases vol 7 article 13 2012
[56] L C Riches A M Lynch and N J Gooderham ldquoEarly eventsin the mammalian response to DNA double-strand breaksrdquoMutagenesis vol 23 no 5 pp 331ndash339 2008
[57] K Chrzanowska M Kalina H Rysiewski et al ldquoGrowthpattern in patients withNijmegen breakage syndrome evidencefroma longitudinal studyrdquoHormoneResearch in Paediatrics vol74 article S38 2010
[58] Group TINBSS ldquoNijmegen breakage syndromerdquo Archives ofDisease in Childhood vol 82 pp 400ndash406 2000
[59] M Digweed and K Sperling ldquoNijmegen breakage syndromeClinical manifestation of defective response to DNA double-strand breaksrdquo DNA Repair vol 3 no 8-9 pp 1207ndash1217 2004
[60] E Seemanova ldquoAn increased risk for malignant neoplasmsin heterozygotes for a syndrome of microcephaly normalintelligence growth retardation remarkable facies immun-odeficiency and chromosomal instabilityrdquo Mutation ResearchReviews in Genetic Toxicology vol 238 no 3 pp 321ndash324 1990
[61] K H Chrzanowska M Szarras-Czapnik M Gajdulewicz et alldquoHigh prevalence of primary ovarian insufficiency in girls andyoung women with Nijmegen breakage syndrome Evidencefrom a longitudinal studyrdquoThe Journal of Clinical Endocrinologyamp Metabolism vol 95 no 7 pp 3133ndash3140 2010
[62] C M R Weemaes T W J Hustinx J M J C Scheres P J JV Munster J A J M Bakkeren and R D F M Taalman ldquoAnew chromosomal instability disorder The nijmegen breakagesyndromerdquo Acta Paediatrica Scandinavica vol 70 no 4 pp557ndash564 1981
[63] A J Green J R W Yates A M R Taylor et al ldquoSevere micro-cephaly with normal intellectual development The Nijmegen
breakage syndromerdquo Archives of Disease in Childhood vol 73no 5 pp 431ndash434 1995
[64] D Gupta and A Nagarkar ldquoSpeech impairment in Nijmegenbreakage syndrome A rare anomalyrdquo International Journal ofPediatric Otorhinolaryngology vol 73 no 6 pp 873ndash875 2009
[65] P Muschke H Gola R Varon et al ldquoRetrospective diagnosisand subsequent prenatal diagnosis of Nijmegen breakage syn-dromerdquo Prenatal Diagnosis vol 24 no 2 pp 111ndash113 2004
[66] S Pasic M Cupic T Jovanovic S Djukic M Kavaric andI Lazarevic ldquoNijmegen breakage syndrome and chronic pol-yarthritisrdquo Italian Journal of Pediatrics vol 39 no 1 article no59 2013
[67] J P Patel J M Puck R Srinivasan et al ldquoNijmegen BreakageSyndrome Detected by Newborn Screening for T Cell ReceptorExcision Circles (TRECs)rdquo Journal of Clinical Immunology vol35 no 2 pp 227ndash233 2015
[68] I Demuth and M Digweed ldquoThe clinical manifestation of adefective response to DNA double-strand breaks as exemplifiedby Nijmegen breakage syndromerdquoOncogene vol 26 no 56 pp7792ndash7798 2007
[69] H Arora A H Chacon S Choudhary et al ldquoBloom syn-dromerdquo International Journal of Dermatology vol 53 no 7 pp798ndash802 2014
[70] C de Renty and N A Ellis ldquoBloomrsquos syndrome Why not pre-mature aging A comparison of the BLM andWRN helicasesrdquoAgeing Research Reviews vol 33 pp 36ndash51 2017
[71] C Keller K R Keller S B Shew and S E Plon ldquoGrowthdeficiency and malnutrition in Bloom syndromerdquo Journal ofPediatrics vol 134 no 4 pp 472ndash479 1999
[72] A Diaz M G Vogiatzi M M Sanz and J German ldquoEval-uation of short stature carbohydrate metabolism and otherendocrinopathies in Bloomrsquos syndromerdquo Hormone Researchvol 66 no 3 pp 111ndash117 2006
[73] C Ling J Huang Z Yan et al ldquoBloom syndrome complexpromotes FANCM recruitment to stalled replication forksand facilitates both repair and traverse of DNA interstrandcrosslinksrdquo Cell Discovery vol 2 article 16047 2016
[74] J S Renes R H Willemsen A Wagner M J J Finken and AC SHokken-Koelega ldquoBloom syndrome in short children bornsmall for gestational age A challenging diagnosisrdquoThe Journalof Clinical EndocrinologyampMetabolism vol 98 no 10 pp 3932ndash3938 2013
[75] M Maciejczyk B Mikoluc B Pietrucha et al ldquoOxidativestress mitochondrial abnormalities and antioxidant defense inAtaxia-telangiectasia Bloom syndrome andNijmegen breakagesyndromerdquo Redox Biology vol 11 pp 375ndash383 2017
[76] R M Brosh M Bellani Y Liu and M M Seidman ldquoFanconiAnemia A DNA repair disorder characterized by accelerateddecline of the hematopoietic stem cell compartment and otherfeatures of agingrdquo Ageing Research Reviews vol 33 pp 67ndash752017
[77] S Yan M Sorrell and Z Berman ldquoFunctional interplay be-tween ATMATR-mediated DNA damage response and DNArepair pathways in oxidative stressrdquo Cellular and Molecular LifeSciences vol 71 no 20 pp 3951ndash3967 2014
[78] L M M Nardozza A C R Caetano A C P Zamarian etal ldquoFetal growth restriction current knowledgerdquo Archives ofGynecology and Obstetrics vol 295 no 5 pp 1061ndash1077 2017
[79] M Tomas Vila J P Verdu M R Piera and C O AlonsoldquoNijmegen breakage syndrome phenotype a disorder to con-sider in the diagnosis ofmicrocephalyrdquoAnales De Pediatria vol74 pp 58ndash60 2011
Submit your manuscripts athttpswwwhindawicom
Stem CellsInternational
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
MEDIATORSINFLAMMATION
of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Behavioural Neurology
EndocrinologyInternational Journal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Disease Markers
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
BioMed Research International
OncologyJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Oxidative Medicine and Cellular Longevity
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
PPAR Research
The Scientific World JournalHindawi Publishing Corporation httpwwwhindawicom Volume 2014
Immunology ResearchHindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Journal of
ObesityJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Computational and Mathematical Methods in Medicine
OphthalmologyJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Diabetes ResearchJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Research and TreatmentAIDS
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Gastroenterology Research and Practice
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Parkinsonrsquos Disease
Evidence-Based Complementary and Alternative Medicine
Volume 2014Hindawi Publishing Corporationhttpwwwhindawicom

2 BioMed Research International
Base excision repair (BER)
Mismatch repair (MMR)
Nucleotide excision repair (NER)
Homologous recombination repair (HR)
NonhomologousEnd Joining (NHEJ)
Source of damage Types of DNA lesions DNA repair pathway
Ionizing radiation
Bifunctional alkylatingagents
(i)
(ii)
Hydroxyurea(iii)
Single-strand break (direct lesion)
(i)
8-Oxo-G(ii)Abasic site(iii)Uracil in DNA(iv)
base mispairing(i)
Double-strand break (DSB) (direct and ICL product)Interstrand crosslink (ICL)Single-strand break (SSB) (ICL by-product or associated with DNA replication)
(i)
(ii)(iii)
64 photoproductTimidine dimerBulky adduct
(i)(ii)
(iii)
Replication Errors(i)
UV lightPolycyclic AromaticHydrocarbonsAlkylating agents
(i)(ii)
(iii)
UV lightOxigen radicalsAlkylating agentsSpontaneous Cytosine deamination
(i)(ii)
(iv)(iii)
Figure 1 DNA lesions are induced by endogenous and exogenous sources Every agent causes a particular lesion that will activate specificDNA repair pathways
incorporate noncomplementary WatsonndashCrick bases duringDNA synthesis It can also come from lesions caused byoxidative damage that occurs during normal metabolism inthe mitochondria and other cellular sites giving rise to theoxidation of several cellular components including DNAresulting in modified bases or breaking of the union betweenthem Besides spontaneous decay of the DNAmolecule maygenerate hydrolysis that creates abasic sites and deaminationcausing a change in the original bases Exogenous sourcesthat continually damage our DNA may be of four mainorigins (1) biological such as some virus (2) physicallike solar radiation or radiation therapy (3) chemical likepesticides and medical treatments (chemotherapy) and (4)personal habits such as smoking (Figure 1) All togetherthese mechanisms may generate more than ten thousandlesions per cell per day [3]
Two main factors the type of DNA lesions and thephase of the cell cycle where they are sensed affect thechoice of the DNA repair pathway to be used and thesubsequent outcome (Figure 1) Mispaired bases are repairedby mismatch repair (MMR) oxidative damage abasic sitesand uracil in DNA are corrected by removing the altered basethrough base excision repair (BER) UV radiation damageand bulky adducts that disrupt the structure of the double
helix are repaired by nucleotide excision repair (NER) inwhich an oligonucleotide of 30 bp containing the lesion isremoved [4] Most DNA lesions interfere with DNA repli-cation and transcription processes that are indispensablefor appropriate cell function However double-strand breaks(DSBs) in which both DNA strands lose continuity are themost dangerous type of DNA damage and have primarilycytotoxic or cytostatic consequences [2 3 5]
Interstrand crosslinks (ICLs) are detected and removedthrough the Fanconi anemia pathway [6 7] also knownas the FABRCA pathway The processing of ICLs occursduring the S phase resulting in the following intermediarylesions an adduct and a DSB which are further takencare of by known repair pathways The adduct is repairedby the NER pathway while the DSB is processed by oneof four independent pathways nonhomologous end joining(NHEJ) homologous recombination (HR) alternative-NHEJ(alt-NHEJ) and single-strand annealing (SSA)The selectionof the repair pathway that will take care of the DSB dependson the cell cycle phase and if the 31015840 ends of the DSBs areprocessed by an exonuclease or not [8] NHEJ operates in anyphase of the cell cycle and does not require any processingsince this repair pathway marks both blunt ends of the DSBwith a Ku70Ku80 heterodimer and joins them Meanwhile
BioMed Research International 3
p53
53BP1
Rif1
CtlP
BRCA1
KU80
KU70
+
+NBN
RAD50
MRE11gH2AX
gH2AXgH2AX
gH2AX
RPARPARPARPA
FAN
CM
G
G
Transducers ATMATR
Checkpoint
DNAPKcs
Chromatinreorganization
Effectors
Sensors and mediators
Senescence Celldeath
Reparable damage Irreparable damage
DNA repair Misrepair Genomicinstability
Normal cell growth Abnormal cell growth(cancerhypoplasia) Outcomes
or
Figure 2 DNA damage response can result in different outcomes following single strand breaks interstrand crosslinks and double strandbreaks Each DNA lesion is recognized by specific sensor proteins according to the cell cycle phase in which the cell is during S phase theprotein FANCM identifies a replication fork arrested by an ICL MRN + BRCA1 sense DSBs meanwhile Ku70Ku80 + 53BP1 can recognizeDSBs across the entire interphase RPA detects and covers ssDNA primarily during S phase The sensing process is then transduced andamplified on chromatin through a series of posttranslational histone modifications such as phosphorylation of H2AX (120574H2AX) on both sidesof the DSB These changes allow the recruitment of the specialized transducer kinase ATR that mainly responds to RPA-covered ssDNAoriginated by replication stress or DNA lesions such as ICLs concurrently ATM responds to DSBs Kinases activate several effector proteinsincluding the transcription factor p53 which acts downstream regulating diverse outcomes according to the type and quantity of remindinglesions in the cell
in order to repair a DSB using HR alt-NHEJ or SSA the 31015840blunt endsmust be processed to allow the loading of theMRNcomplex (a heterotrimer integrated by three proteins calledMRE11 RAD50 and NBN) to continue the repair processThis occurs primarily during the S and G2 phases of the cellcycle when sister chromatids are available and can be usedfor HR error-free repair [7 9]
3 DNA Damage Response
Even when each specific DNA lesion stimulates a particularDNA repair mechanism cells trigger a common generalprogram known as the DNA damage response (DDR) whichis charged with lesion detection signaling and repair pro-motion as well as cell cycle progression control It is nosurprise that the DDR is an extremely controlled process theexquisite balance between cell survival and cell death and
senescence relies on it [1 9 10] Tissue homeostasis or growthabnormalities such as cancer [11] or tissue hypoplasia dependamong other things on the amount and type of genomicdamage sensed and processed by the DDR
The DDR is composed of a network of regulatory non-coding RNAs and proteins that act as sensors transduc-ers and effectors [1 12] Sensor proteins recognize specificlesions (Figure 2) For example the FANCM protein detectsthe stalled replication fork caused by interstrand crosslinks(ICLs) theMRNcomplex is the typical sensor ofDSBs duringSG2 phase the Ku70Ku80 heterodimer is the primary DSBssensor duringG1while replication proteinA (RPA) overcoatssingle-strand DNA (ssDNA) found either at processed DSBoverhangs to be repaired by HR or at stalled replication forks[13]
Following recognition of the lesions by sensors andmediators the signal is amplified by transducer proteins
4 BioMed Research International
Table 1 Chromosomal instability syndromes with intrauterine growth deficiency
Syndrome Genes Function in DDR Repair pathway Cytogenetic alteration
Fanconi anemia 21 FANC genes
ICL detection andprocessing generation ofadducts and DSBs (sensorsmediators and effectors)
Homologous recombination Chromatid and chromosomal breaksRadial figures
Seckel Syndrome 1 ATRSSBs detection and signaltransduction(transducer)
Homologous recombinationNonhomologous recombination
Chromatid and chromosomal breaksandRearrangements
Nijmegen BreakageSyndrome NBN
DSBs detection andsignaling (sensor andmediator)
Homologous recombinationNonhomologous recombination
Chromatid and chromosomal breaksAneuploidiesRearrangements affectingchromosomes 7 and 14
Bloom Syndrome BLMHelicase process SSBs andHolliday Junctions(effector)
Homologous recombination QuadriradialsIncrease in sister chromatid exchange
The PIKK kinases (Phosphatidyl Inositol 3-Kinase-relatedKinases) family is the most important of this group it isintegrated by ataxia telangiectasia and Rad3-related (ATR)Ataxia telangiectasia-mutated (ATM) and DNA dependentprotein kinase (DNAPKcs) ATR is activated during the Sphase of the cell cycle in the presence of DNA damagesuch as base adducts crosslinks single-strand breaks (SSBs)replication stress andDSBs that originate during the S phasewhile ATM and DNAPKcs are activated by DSBs at anypoint of the cell cycle [13 14] The DDR kinases activatesignaling cascades through posttranslationalmodifications ofvarious proteins including phosphorylation ubiquitylationand PARylation which play a central role in regulation ofthe DDR [15] Specifically ATR and ATM can autoactivate ortransactivate each other through phosphorylation and thenphosphorylate the histone variant H2AX (120574H2AX) that actsas a platform to recruit DDR factors and prepare the cell torestore DNA integrity ATR and ATMrsquos main downstreamphosphorylation targets are proteins Chk1 and Chk2 andthe important effector p53 their activation allows regulating(a) the chromatin structure surrounding the lesion (b)checkpoints that stop the cell cycle (c) DNA repair proteins(d) proteins that induce senescence and (e) proteins that leadto cell death (Figure 2) [10 16]
Finally if DNA lesions are repaired the checkpoint that isresponsible for stopping the cell cycle is turned off and the cellcycle is allowed to restart through a process called checkpointrecovery This process is only turned on when the signalingfor theDNA lesions is silenced and the surviving cell recoversits normal homeostasis and growth When DNA damagecannot be properly repaired the cellrsquos destiny should beeither senescence or death Otherwise cellsmight dividewithunrepaired DNA damage through an erroneous activation ofthe checkpoint recovery process that allows cell survival withgenomic instability to promote cell dysfunction and cancer[17]
4 DNA Damage Response and Disease
Unrepaired or misrepaired lesions in DNAmay immediatelyimpair replication and transcription affecting the whole cell
function In an irreparable damage situation the amountand type of lesions as well as the cell cycle phase in whichthe cell is will influence the DDR response in order tofavor immediate cell death or the conversion of DNA lesionsinto durable mutations or stable chromosomal abnormalities[3]
Cell survival despite genomic damage can directly affectcell growth this can be evidenced by two opposite outcomesOn the one hand there can be an overgrowth effect sincemutations in critical genes such as oncogenes or tumorsuppressor genes can alter cell function and increase thelikelihood of cancer development [3 18 19] On the otherhand there can be cell hypoplasia or cell loss this happenswhen irreparable damage leads to either cell death or cellsenescence a cancer-protecting condition in which cellsare alive but unable to proliferate limiting the growth ofthe tissues and conducting to aging (Figure 2) This isevidenced by the phenotype of patients affected by diseasesthat alter the DDR and DNA repair in which growthalteration and increased cancer susceptibility are importantfeatures
5 Chromosome Instability Syndromes
Mutations in at least 114 genes involved in the DDR leadto disease some of the mutations are somatic resulting invarious types of spontaneous cancer and others are geneticdiseases with constitutionalmutations that lead to syndromesthat may or may not be related to the development ofcancer [10] Among the genetic diseases with mutations inDDR genes the chromosomal instability syndromes (CIS)are a group of rare Mendelian diseases characterized byincreased chromosome breakage resulting from unrepairedor misrepaired DNA strands breaks Other than chromoso-mal instability they also have clinical overlapping featureslike cancer proneness premature aging and growth abnor-malities even though each CIS has a particular phenotypethat distinguishes it from the others Only a subgroup of thesepatients has prenatal growth alterations this review focuseson those syndromes (Table 1)
BioMed Research International 5
6 DDR Alteration and Growth Failure
Historically disruption of the DDR has been associatedwith cell growth abnormalities in a unilateral way alwayspointing towards the increased cell number in the form ofderegulated cell proliferation in cancer [19] But there islittle information on how DDR alterations can also lead toderegulation of growth in the opposite direction resultingin lack of growth due to cell death and low cell repro-duction One of the first observations to partner growthdeficiency with an altered DDR was the finding that someSeckel syndrome patients (SS) a rare phenotype consistingof primordial dwarfism and microcephaly had mutationsin the ATR gene which encodes the ATR kinase a DDRtransducer Further analysis of SS patients revealed locusheterogeneity for this phenotype mutations in other genesrelated to DDR or DNA repair also led to this clinical pictureThis observation has reinforced the association betweenDDRfailure and severe intrauterine growth retardation Moreovergenes that participate in centrosomal biology are also relatedto the uncommon phenotype of microcephalic primordialdwarfism suggesting that centrosomes have a central rolefor the adequate differentiation of early neuroprogenitorsIt has then been proposed that failure in cell proliferationsecondary to abnormal mitosis is the cause of primordialdwarfism since the multipolar spindles result in the acti-vation of checkpoints reducing proliferation and activatingapoptosis [20]
For the phenotype of growth restriction to be evidentprenatally the mechanisms regulating growth must be com-promised from the beginning of the development in embry-onic stem cells (ESCs) which are pluripotent cells derivedfrom the three primary germ layers ectoderm endodermandmesoderm and that have the capacity to differentiate intomore than 200 cell typesThese cells have been proven to havean extremely efficient DDR and proficient DNA repair mech-anisms that allow for a rigorousmaintenance of their genomeintegrity otherwise unrepaired DNA damage in ESCs wouldbe amplified affecting normal human development
ESCs have an extremely active proliferation rate theircell cycle has a characteristically reduced G1 phase andrepair mechanisms are heightened When comparing ESCsto fibroblasts it stands out that MMR is enhanced BERand NER repair pathways are highly competent and therepair of DSBs is preferentially made through the reliableHR pathway [21] Moreover when HR is not available andDSBs accumulate apoptosis is the preferred route to removehighly damaged cells It is interesting that DSB repair inESCs requires signaling through ATR instead of ATM ESCshave a special mechanism to deal with DNA damaged cellswhen inefficient DNA repair or DDR affects the induction ofapoptosis or autophagy [22] This mechanism leads to ESCdifferentiation that is driven by damage-induced expressionof the p53 transcription factor damaged differentiated cellsare efficient in cell cycle arrest and apoptosis This strategyresults in the maintenance of genetic stability in a decreasednumber of ESCs and a portion of differentiated cells thatbecome senescent both resulting in growth deficiency[21]
Growth deficiency is at the center of many diseasesincluding extremely low body size In mammals overall sizeis determined by the number of cells body mass is then thesum of all the cells that have proliferated minus those thathave died A fetus that is growing harmonically has accuratebalance between these two processes failure of either one ofthese results in dramatic effects when they occur in the ESCpopulation a decrease in cell proliferation rate or an increasein apoptosis leads to intrauterine growth retardation (IUGR)[23]
7 Chromosome Instability Syndromes withIntrauterine Growth Retardation
71 Seckel Syndrome Seckel syndrome (SS) is an autosomalrecessive disorder clinically and genetically heterogeneousSo far at least six genes have been associated with the Seckelphenotype most of these genes participate in ATR-mediatedDDR and in centrosomal function Two clinical subgroupscan be identified on the one hand patients with mutationsin ATR NIN and ATRIP genes only present the Seckelphenotype while on the other hand those with mutationsin CENPJ CEP152 or RBBP8 show allelic heterogeneity andbesides the SS phenotype can also manifest as a spectrumof disorders known as Primary Autosomal Recessive Micro-cephalies [24ndash28] SS patients who bear mutations in ATRshow a classical Seckel phenotype the SS data presented herewill be limited to such patients
ATR is localized in 3q23 it is one of the serine threoninekinases that belong to the PIKK family They have a funda-mental role in the DDR since they participate as transducersin the signaling of DNA lesions especially when the DDRresponds to stalled replication forks and bulky lesions inDNA[24 25] ATR responds preferentially to ssDNA during the Sphase It also plays a crucial role in preventing DNA breakscaused by fork pausing when DNA replication machineryfinds DNA lesions or complex DNA structure and sequences[24] ATR stability depends on binding of ssDNA to theATR cofactor ATRIP (ATR interacting protein) and thesingle-stranded binding protein (RPA) ATRIP is required forATR localization to the ssDNA regions and hence for ATRactivation [25 27] Major functions of ATR are activation ofcell cycle check point arrest stabilization of stalled replicationforks and promotion of replication fork restart which isachieved through its ability to phosphorylate a wide range ofsubstrates that include p53 and H2AX [27 29]
Cellular phenotype of ATR deficient cells is characterizedby decreased phosphorylation of ATR-dependent substratesas well as an impaired G2M checkpoint arrest These cellsare characterized by markers that signal unrepaired DSBslike the presence of 120574H2AX chromosomal breakage [2629 30] and micronuclei formation This cellular phenotypemay be originated by a failure to recover from replicationstalling which generates DSBs that are normally repairedby HR when they occur during SG2 In SS cells theabsence of ATR is critical during embryonic developmentthis deficiency leads to genomic instability cell senescenceand cell death that leads to fetal growth and accelerated aging[31]
6 BioMed Research International
Figure 3 Seckel syndrome patient Note the severe microcephalyand the ldquobird-likerdquo appearance facies with micrognathia and reced-ing forehead The patient is severely disabled with no independentmarch
Moreover it appears that ATR and the other SS genes notonly participate in the DDR but also take part in the controlof centrosome maturation This engagement in centrosomebiology is also true for other DDR proteins like BRCA2biallelic mutations in its gene are responsible for a subgroupof Fanconi anemia patients [32]Theunifying feature betweenall Seckel patients irrespective of the molecular defect isthat their cells have an altered cell cycle progression thatis particularly evident during high rate cell division whenthere is hypersensitivity to replicative stress and centrosomaldysfunction This is especially important in cells with highdivision rates like the ones found in developmental stageswhere rapid replication is key [24 27]
SS is characterized by IUGR dwarfism microcephaly(below minus4 SD) mental retardation and some other anomalieslike luxation of the head of the radius scoliosis bone agedelay and seizures (Figure 3) The distinctive facial featuresinclude a prominent nose with micrognathia and a recedingforehead resulting in a ldquobird-like appearancerdquo [26 31 33]Since this syndrome has important clinical heterogeneityother anomalies have been reported including mandibularhypoplasia sternal abnormalities clinodactyly and low setears with hypoplastic lobules Although rare other reportedfeatures are moyamoya syndrome osteosarcoma and pol-yarteritis nodosa [26] Cerebral malformations like neuronalmigration abnormalities have been described but are notalways present [33] No glucose metabolism abnormalitieshave been reported
Dwarfism can be related to a reduction in the totalnumber of cells generated during development leading tohypoplastic tissue and reduced organism size [23] On theother handmicrocephalymay be related to an impairedDNAdamage response signal that could alter the cellular thresholdfor cell death resulting from DNA damage increasing thelevels of apoptosis during development developing neuronsare rapidly proliferating and potentially generate high levelsof oxidative damage which may lead to a higher level oflesions being faced at replication forks [23 25] Also analtered mitosis secondary to impaired spindle formationcould delay mitotic progression and increase the proportionof nonviable cell divisions Finally the stem cells may beaffected by abnormal centrosomal function Stems cells haveasymmetric divisions in order to preserve the characteristics
Figure 4 Fanconi anemia patient This six-year-old girl is 105 cmtall her height is just below the 5th percentile and her at-term birthweight is reported to be of 1900 gr Characteristic features of FA areevident skin hyperpigmentation bilateral radial defects consistingof bilateral thenar hypoplasia and absent fold of the right thumbwhich cannot be bent
of a stem cell and the centrosomes play an important role insuch divisions [23]
There is limited clinical information regarding age-related diseases in SS there is a void of prospective follow-up data from these patients that can only be obtained byfollowing a cohort of SS patients something that is apparentlynot being done at this time Nevertheless animal modelsbring some clues over the possibility of an aging phenotypein SS patients since ATR deficient adult mice show prematureage-related phenotypes as well as increased deterioration oftissue homeostasis [29 34]
72 Fanconi Anemia DNA interstrand crosslinks are ex-tremely noxious DNA lesions that affect central cellularprocesses like transcription and replication The FABRCApathway is responsible for the appropriate processing ofthese lesions protein products from at least 21 FANC genesparticipate in this pathway [35] The malfunction of any ofthose FANC proteins leads to the clinical phenotype knownas Fanconi anemia (FA) which is characterized by shortstature congenital malformations from the VACTERL-Hspectrum bone marrow failure and an increased suscepti-bility to cancer like acute myeloid leukemia epithelial headand neck cancer [36] (Figure 4) Most of the FA families bearbiallelic mutations in FANC genes that have an autosomicrecessive inheritance pattern only families with mutations inFANCB show an X-linked recessive pattern while those inwhich FANCR is the affected gene demonstrate an autosomicdominant one [35]
The FABRCA is an S-specific pathway that has 3 basicsteps it starts with the detection of the ICL by the proteinFANCM followed by the recruitment of the FA core com-plex that is responsible for the monoubiquitination of theFANCD2I heterodimer which in turn favors the recruit-ment of effector FANC-repair proteins that restore the DNAto its original form [35]
BioMed Research International 7
(a) (b)
Figure 5 Chromosomal instability induced by 40 ngml mitomycin C (a) Lymphocytes from a healthy individual (b) lymphocytes from aFA patient Short arrows show chromosomal breaks the long arrow shows a quadriradial figure Note the exacerbated chromosome instabilityfound in the FA patient
The cellular phenotype of FA derived cells is extremelyconstant An aberrant FABRCA pathway can result inunrepaired DSBs that manifest as chromosomal breaks orabnormal repair by an error-prone repair pathway that resultsin radial figures These alterations are cytogenetic evidenceof chromosomal instability which is the hallmark of FA cellsand is exploited for clinical diagnostic purposes (Figure 5)The agents capable of inducing this chromosomal instabilityare from endogenous origin like aldehydes [37] and reactivespecies of oxygen (ROS) [38] as well as exogenous sourceslike bifunctional alkylating agents (diepoxybutane or mito-mycin C) In addition FA cells have accumulation of cells inG2 phase of the cell cycle resulting from a functional G2Mcheckpoint and a proapoptotic phenotype
In contrast with the cellular FA phenotype the clinicalpicture in FA patients is extremely variable not every patientwill have all the manifestations one-third of patients do nothave congenital malformations [39] while almost 90 willdevelop bone marrow failure [36] One of the more constantmanifestations in FApatients is growth parameters alterationAn analysis from the international Fanconi anemia registry(IFAR) data showed that over 60 of FA patients presentedshort stature (below the 5th percentile) while birth lengthandweight below the 5th percentile was respectively reportedin almost 30 and nearly half of FA patients [40]Moreover aprospective study of data from 54 IFAR participants showedthat the mean standard deviation score (SDS) for height inthese patients was significantly below normal for age and sexat minus235 plusmn 028 meanwhile mean SDS for weight was betteralthough below normal (minus126 plusmn 024) In this study perinatalgrowth data was not reported [41]
Other than the IFAR data on growth there are anothertwo studies that analyze growth parameters of FA patientsAnthropometric measurements from 45 patients with Fan-coni anemia from the National Cancer Institutersquos inher-ited bone marrow failure syndromes (IBMFS) cohort wereassessed This cohort had a mean SDS for height of minus21 plusmn
189 The height of over half of the participants (54) wascategorized as short (SDS gt 20 SD) in this subset of patientsthe mean SDS for height was minus38 plusmn 15 [42] Finally theevaluation of 120 FA patients from the FA ComprehensiveCare Clinic of Cincinnati Childrenrsquos Hospital Medical Centerrevealed that median height SDS was shorter than expectedin children and adults irrespective of gender Furthermorethis study presented birth information from 70 patients (59children and 11 adults) from the cohort 51 of the childrenand 3 adults were born small for gestational age their medianbirth weight at term was 202 kg (range 15ndash26 kg) [43] Theintrauterine growth restriction seen in FA patients has alsobeen documented in several case reports in which at-termbirth weight ranges from 1780 to 3200 gr [44ndash49] Eventhough growth abnormalities have been identified in FApatients with mutations in almost every FANC gene it hasbeen shown that patientswithmutations in certain genes havea more severe growth delay That is the case for patients withbiallelic mutations in FANCD1 [47 48] as well as those whobear mutations in FANCC for whom an SDS for height ofminus384 has been found [41]
Endocrine abnormalities have been proven to be aninherent part of the FA phenotype up to 80 of patientshave one or more endocrine abnormalities Besides growththyroid function and glucose homeostasis are frequentlyaffected [40ndash43] Considering the existing evidence for arelationship between low birth weight and an increased riskfor noncommunicable adult diseases like diabetes hyperten-sion heart disease dyslipidemia and osteoporosis [50] it isrelevant to revise these diseases in FA The FA cohorts inwhom growth was assessed were also evaluated for endocrinestatus Glucose homeostasis is affected in a large portion ofFA patients impaired glucose tolerance has been found in27ndash68 of them whereas diabetes has a prevalence of 8ndash10Dyslipidemia has been assessed in only a small portionof FA patients but it has been found in 17ndash55 of theevaluated subjects [51]There are conflicting results over bone
8 BioMed Research International
mineral density (BMD) status in FA the first time this wasevaluated 92 of the patients were found to have osteopeniaor osteoporosis [42] nevertheless a study that evaluated alarger FA cohort found that lowBMD is not a frequent finding[52] Further research on this topic has raised the questionof whether BMD deficit is intrinsic to the FA phenotype ora consequence of hematopoietic cell transplantation (HCT)an interrogation that is still awaiting to be answered [53]Cardiovascular adult diseases are not relevant in the FA phe-notype heart disease in these patients is from the congenitaltype as 13of patients have cardiacmalformations [40] whilehypertension has only been reported in two patients as theresult of renal malformations [54]
Findings from the different FA cohorts show that shortstature is an inherent feature of the FA phenotype thisfeature does not respond to a single explanation the apoptosisprone FA cellular phenotype is certainly a contributing factorfor this The fact that FA patients have a constitutionallydefective pathway since conception could explain the clinicalphenotype of RCIU Short stature may also be exacerbated byaccompanying endocrinopathies The cooccurrence of manyendocrine alterations has encouraged unifying explanationssome have proposed that endocrinopathies are secondaryto increased cytokine activity found in FA cells [41] whileothers favor the view that some endocrine secretory cellsmight be damaged by high levels of reactive oxygen specieswhich are known to be elevated in FA patients [43] In linewith the developmental origin of adult health and diseasetheory it could also be possible that the increased prevalenceof glucose homeostasis alterations and dyslipidemia reportedin FA patients is a consequence of intrauterine growthrestriction of these patients Nevertheless the attemptedgenotype-phenotype correlation of the endocrine phenotypein FA patients does not seem to support that Patients withmutations in FANCA show a mild endocrine phenotype inwhich height is not severely affected and insulin resistanceis mild whereas mutations in FANCC which are relatedto shorter stature have the least insulin resistance [41]Moreover no direct relationship between birth weight andglucose tolerance was identified when it was intentionallylooked for [43] although the number of patients in whichthese observations were made is limited
73 Nijmegen Breakage Syndrome Nijmegen breakage syn-drome (NBS) is an autosomal recessive disease caused bybiallelic mutations in NBN a gene that encodes nibrin aprotein involved in DNA repair and cell cycle checkpointregulation It participates in the former by sensing double-strand breaks as part of the trimeric complexMRN alongsideMRE11 andRAD50Meanwhile for the latter it contributes tothe appropriate activation of ATM andATRwhich are centraltransductors of the DNA damage response (DDR) [55] Themalfunction of nibrin translates in a cellular phenotypemarked by chromosomal instability radiosensitivity reducedphosphorylation of ATM substrates and S and G2M cellcycle defects [56] Chromosome instability is evidenced bycytogenetic methods in 10ndash60 of cells in the form of breaksand numeric and structural aberrations translocations andinversions affecting chromosomes 7 and 14 are found in the
147
Figure 6 Translocation between chromosomes 7 and 14 is typicalin NBS patientsrsquo cells
majority of NBS patients and are considered a cytogeneticcharacteristic of this syndrome (Figure 6) [57]
The clinical impact of these alterations is a phenotypecharacterized by microcephaly a distinctive facial appear-ance consisting of receding forehead and mandible and aprominent mid face with a long nose and philtrum aswell as immunodeficiency that leads to recurrent infectionsand an increased risk for the development of neoplasiaparticularly leukemia and lymphoma According to theinternational Nijmegen breakage syndrome study groupgrowth retardation is also a hallmark of this disease [58]although there is not many details about this feature in theliterature
Most of the information on the natural history of NBSavailable today comes from patients participating in reg-istries in which fairly large cohorts of NBS patients areincluded There is a large representation of Slavic patientsin these cohorts which correlates with the high carrierfrequency of a founder mutation of NBN in this populationFrom these studies it is evident that the most severelyaffected anthropometric measure in NBS patients is headcircumference since all participants display microcephalyeven though only 75 display this feature at birth Whenit comes to growth parameters the same study states thatall patients have growth retardation which is described asproportionate and early occurring [58] although the specifictemporality is not defined A posterior report points out thatthe growth retardation seen in most NBS patients locatesthem in the 10th percentile in growth charts and that birthheight and weight are usually within normal parameters [59]Nevertheless there are other authors who report prenataland postnatal growth retardation [55 60] and a tendency forshort stature that is more evident during the first year of life[61] Also several case reports of NBS patients in which birthweight is informed demonstrate prenatal growth restriction[62ndash67] although this could represent a report bias Themore comprehensive data analysis on growth that includesperinatal information of NBS patients is the one that analyzesdata from 67 patients followed for 15 years Eighty percentof these patients were born at term the girls were found tohave a mean birth weight of 27 kg and mean birth heightof 514 cm while boys were reported to have a mean birthweight of 28 kg and mean birth height of 523 cm Moreoverall patients irrespective of gender were found to have ameanheight reduced by over 2 SDS at one year old [57] These data
BioMed Research International 9
(a) (b)
Figure 7 Sister chromatid exchange in cells from a healthy individual (a) and from a BLM patient (b)
support the fact that growth retardation in NBS is a prenatalphenomenon
Nibrin has been found to have essential functions inthe regulation of the cell cycle which translates into anabsolute need for this protein for cell proliferation [68]It would seem logical that mutations of the NBN genethat compromise the appropriate function of nibrin wouldlead to abnormal growth when thought from an organismperspective Mechanistically speaking poor cellular growthcaused by mutations in a particular gene can be thought ofas the main explanation for the growth restricted phenotypebut it has been shown that mutations in other DDR genesthat share the cellular phenotype of poor growth like ATMdo not replicate the compromised growth phenotype atthe organism level growth retardation is absent in ataxiatelangiectasia (AT)This data suggests that there are certainlyother contributing factors to the abnormal growth phenotypeseen in NBS patients [58]
74 Bloom Syndrome Bloom syndrome (BS) is an autosomalrecessive disorder caused by homozygous or compoundheterozygous mutations in the BLM gene (15q261) thatencodes the RecQL3 helicase BLM has a critical role inthe maintenance of genome stability acting at the interfacebetweenDNAreplication recombination and repair [69 70]To date over sixty different mutations including nonsenseand missense have been identified all of them result inthe inactivation of BLM and the consequent loss of itshelicase activity The BLM gene encodes a 1417 amino acidnuclear protein its expression peaks during the S and G
2M
phases of the cell cycle which is consistent with its rolein DNA replication and recombination BLM specificallyunwinds structures like forked DNA duplexes RNA-DNAheteroduplexes and R-Loops which explains its importanceduring replication fork progression and transcription besidesit is central for Holliday Junctions (HJs) dissolution forHR The dissolution of HJs by the topoisomerase III120572-BLMcomplex cannot be replaced by any other RecQ helicase inthe family [69 70] It has also been found to have a role in
the annealing activity of the ssDNA the proper sister chro-matid segregation during mitosis and telomere maintenance[70]
BLM can have both pro- and antirecombinogenic func-tions that are regulated by posttranslational modificationsincluding phosphorylation sumoylation and ubiquitination[70]
BLM also enables sister chromatid segregation by pro-cessing unresolved replication intermediates that manifest inmitosis as ultrafine DNA bridges (UFBs) and together withtopoisomerase III120572 RMI1 and RMI2 localizes to UFBs inanaphase BML deficient cells exhibit and increase frequencyof UFBs suggesting a role of BLM in the resolution ofthese structures Failure to resolve these UFBs leads to DNAbreakage as mitosis proceeds [70]
Therefore BS cells are characterized by an increasein chromosomal aberrations including chromatid gapsand breaks telomere associations and quadriradial chro-mosomes resulting from unsolved recombination betweenhomologous chromosomes BS cells exhibit increased muta-tion rates and the genomic instability includes elevatedmitotic HR and unequal sister chromatid exchange (SCEs)(Figure 7) Perhaps the most characteristic feature is the overtenfold increase in SCEs which results from crossover eventsduring HR repair of damage replication forks [50 69 70]
Clinically the more striking BS feature is IUGR averagebirth weight at term is 1850 g and birth length is 44 cmFor both boys and girls weight and length in BS are morethan two standard deviations below normal indicating thatgrowth retardation has a prenatal origin At postnatal agesheight remains below the normal range and is accompaniedby a paucity of subcutaneous fat Average adult height inmales has been found to be 148 cm (130ndash162 cm) whilein females it has been reported to be 139 cm (122ndash151 cm)[50 70 71]
BS patients have overall proportionated short staturebut the head is reported to be small and narrow relativelyto the body size it is described as mild microcephalyand is accompanied by malar hypoplasia Patients have
10 BioMed Research International
Figure 8 Bloomsyndromepatient inwhom the characteristicmalarerythema is present
been described to have a high pitched voice [50 70] Theskin appears normal at birth but in the first or secondyear of life in response to sun exposure children developan erythematous rash with a butterfly distribution in themalar area and the back of hands and feet The rash caninclude telangiectasia The severity varies between patientssome can even lose their eyelashes and develop blisteringaround the mouth The presence of cafe-au-lait spots andhypopigmented areas of skin associated with contiguoushyperpigmented areas is common (Figure 8) Intellectualabilitiesmay be limited in some patients and normal in others[50 70]
Other clinical conditions reported in BS patients are gas-troesophageal reflux and diarrhea in infants mild immuno-logical deficiency with frequent episodes of otitis mediaazoospermia or severe oligospermia in males and prema-ture cessation of menstruation in females minor anatomicdefects and increased risk for neoplasia which is the maincause of dead in BS [70] Another common medical con-dition in BS is diabetes mellitus associated with impairedglucose tolerance and insulin resistance it has been reportedin up to 16 of patients [70] According to data fromthe Bloomrsquos Syndrome Registry diabetes in these patientstends to begin early with a mean age at diagnosis of 266years It is not associated with ketosis and it does nothave the classical hereditary pattern seen in type 2 diabetes[50 72]
Short stature in BS is not due to hormonal causes sincethe size of cells in persons with BS is normal it has beenhypothesized that there are fewer of them due to either adecrease in the cell division rate an increase in apoptosis oreven a combination of both BS cells have troublemeeting thedemands of fast cell divisions encountered in tissues duringembryonic development The leading hypothesis suggeststhat problems arising during DNA synthesis require a longerS phase to overcome the challenge which translates intoslowing of the cell division rate and an increase in apoptosis[70]
8 Concluding Remarks
This review has focused on discussing phenotypes of CISin which there is a prenatal alteration of growth The foursyndromes discussed here are rare diseases whose prevalenceis difficult to calculate since appropriate identification anddiagnosis of affected individuals among the general popula-tion are not straightforward It is important to note that theavailable information on the natural history of FA NBS andBS comes from the analysis of several patients that participatein registries This strategy results in detailed informationthat permits a better analysis of the clinical phenotype ofthese rare diseases Meanwhile available data of SS is moreanecdotic which results in a nonsystematic gathering ofinformation which is thus frequently incomplete
From the available clinical data of these CIS it is evidentthat growth is not affected in the same extent for all ofthese syndromes the phenotypes that exhibit a more severelystagnated perinatal growth are BS and SS The severe growthdelay reported in these patients has been described as apathognomonic sign of these diagnoses In patients withFA perinatal growth can also be severely affected but notevery FA patient shows this manifestation Finally NBShas been described to have growth retardation of prenatalorigin of mild severity almost within the lower normal range(Figure 9) The cephalic circumference can be affected in allof these syndromes severe microcephaly is pathognomonicin SS and NBS it is described as mild for BS patients and it isfound in less than half of FA patients (Table 2)
When trying to understand why a subset of CIS showsprenatal growth retardation it could be alleged that theintrinsic chromosomal instability is responsible for it Butthis would not explain why prenatal growth retardation isnot a universal CIS feature for example ataxia telangiectasiapatients who have biallelic mutations in the ATMkinase genedo not show prenatal growth delay It strikes that a molecularcommon feature shared by the prenatal growth retardationSIC phenotypes is that they are caused by mutations ingenes that are necessary for an appropriate response to DSBsduring the S phase of the cell cycle The molecular defectin SS affects the functioning of ATR the preferred DDRtransducing kinase used by highly replicating ESCs TheFABRCA pathway which is affected in patients with FAdetects ICLs upon replication fork arrest Nibrin the proteinaffected in patients with NBS is induced during S phasefor the detection of DSBs And the BS helicase forms aFANCM-BLM complex needed to sense ICLs during S phase[73] It could then be argued that altered DNA replicationis an important factor for the development of intrauterinegrowth restriction in these CIS Nevertheless it must be keptin mind that the inherent chromosome instability found inthese syndromes may also be affecting normal growth in thepatients [27 43 57 60 71]
Being small for gestational age has been associatedwith a higher risk of noncommunicable adult diseases likeglucose homeostasis disorders dyslipidemia hypertensionand others It has been proposed that fetal reprogrammingto enhance fetal survival despite the risk for adult onsetdiseases is an outcome that does not take into account
BioMed Research International 11
Table 2 Growth features of chromosomal instability syndromes
SyndromeldquoLocirdquo At-term birth weightheight Microcephaly Adult height Adult onset diseases
Seckel SyndromeldquoATR3q23rdquo
Birth weight below minus3 SD(2055 g)
Severeminus4 SD
Postnatal growth retardation(below minus5 SD) Not reported
Fanconi anemialdquo21 FANC genesrdquo
Median weight 202 kg(15ndash26 kg) In 20ndash50
50ndash60 of patients with medianheight lt minus18 SDSWomen minus34 SDSMen minus44 SDS
CancerDiabetes mellitusDyslipidemia
Altered bone mineral densityNijmegen BreakageSyndromeldquoNBN8q21rdquo
Mean weightheight girls27 kg514 cm
Mean weightheight boys28 kg523 cm
100 Mean height for women minus18 SDSMean height for men minus23 Cancer
Bloom SyndromeldquoBLM15q261rdquo
Mean weight 189 kg plusmn 035 kg forboys
Mean weight 187 kg plusmn 035 kg forgirls
Mean height 434 cm plusmn 44 cm forboys
Mean height 438 cm plusmn 28 cm forgirls
Mildmicrocephaly
Mean height 1455 cm plusmn 76 cmmales
Mean height 1415 cm plusmn 61 cm forfemales
CancerDiabetes mellitus
See [27 33 40 43 50 57 69]
45 53
43245
Height (cm)
Weight (kg)
Percentile 3 Percentile 97Percentile 50495
33
Normalindividual
Mean 2055
SeckelSyndrome
2615Median 202
FanconiAnemia
Mean 51
Mean 275
Nijmegen BreakageSyndrome
38 49
24513
Mean 436
Mean 188
BloomSyndrome
Figure 9 Anthropometric features at birth of chromosome instability syndromes with perinatal growth retardation Comparison of theavailable growth data from SS FA NBS and BS syndrome against birth data from the WHOrsquos growth standards for infants Although meanheight and weight values of NBS patients are found to be within normal percentiles according to WHO standards there are several authorswho refer to prenatal growth restriction [55 63 65 79]
the reason for the prenatal growth restraint [50 72 74] Itmust be kept in mind that noncommunicable diseases aremultifactorial entities in which genetic and environmentalfactors converge and their cause cannot be attributed to asingle explanation However when growth restriction is akey feature in syndromes with chromosome instability the
possibility that cell hypoplasia due to DNA repair malfunc-tion is contributing to the growth restriction phenotypemustbe contemplated Moreover since none of these adult onsetdiseases is reported as an inherent element of the SS and NBSphenotypes the direct connection between low birth weightand adult noncommunicable diseases is less of a straight
12 BioMed Research International
shot Furthermore there are other Mendelian syndromeswith mutations in DNA repair genes that characteristicallyshow adult noncommunicable diseases but do not haveIUGR such is the case for Werner syndrome a progeroiddisease caused by biallelic mutations in another RecQ heli-case (RecQ4) that clinically presents with postnatal shortstature and a prevalence of type 2 diabetes mellitus of 70[50 70 74]
Natural history of FA NBS and BS documented throughthe existing patient registries has allowed the identificationof noncommunicable diseases to be a part of the clinicalspectrum of these syndromes (Table 2) Meanwhile from theinformation available through SS case reports no adult onsetdisease has been found to be part of this phenotype To thebest of our knowledge the direct investigation of nonevidentendocrinologic alterations like glucose homeostasis or dys-lipidemia has not been directlymade in SS patients For a raredisease like SS such a study can only be done if a fairly largegroup of patients like the one found in registries is availableIf such a study was to be performed hidden features in SSpatients could be unraveled
Oxidative stress sensibility is a cellular feature sharedby all the SIC syndromes with IUGR that could contributeto the explanation of the premature development of non-communicable adult diseases in these patients Reports haveshown that BS and NBS cells have endogenous reactiveoxygen species (ROS) overproduction and an impairedmitochondrial homeostasis [75] it is also well known thatFA cells show increased levels of oxidative damage [3876] and there is evidence that oxidative stress can activateATR-mediated checkpoint signaling [77] Since this kind ofdamage has soundly been related to age-associated diseasesthat result from tissue degeneration exacerbated oxidativedamage found in these syndromes could result in cellu-lar aging that manifests as overall premature aging withparticular symptoms like glucose homeostasis alterations[76 77]
Fetal growth restriction is a multifactorial conditionwhere wide arrays of factors converge Fetal aspects inparticular those affecting the genetic constitution of thefetus have been recognized to play an important role Ithas been demonstrated that chromosomal abnormalities andmonogenic syndromes caused by mutations in genes thatparticipate in growth or metabolic pathways directly affectfetal growth [78] Even though they are rare entities CISappear as another group of monogenic pathologies thatbroaden the list of genetic fetal factors of fetal growthrestriction
Consent
The necessary consent for the publication of the photographswas obtained
Conflicts of Interest
The authors declare that there are no conflicts of interestregarding the publication of this paper
Authorsrsquo Contributions
The three authors contributed equally andwrote the first draftof the paper The final version was approved by everyone
Acknowledgments
This paper is supported by SEP-CONACYT Project 243102Benilde Garcıa-de Teresa received the 574025 scholarshipfrom CONACYT The paper is also supported by PAPIIT-UNAM Project IA202615 and Fondos Federales INP Project41-2014
References
[1] K W J Derks J H J Hoeijmakers and J Pothof ldquoThe DNAdamage response The omics era and its impactrdquo DNA Repairvol 19 pp 214ndash220 2014
[2] S P Jackson and J Bartek ldquoThe DNA-damage response inhuman biology and diseaserdquoNature vol 461 no 7267 pp 1071ndash1078 2009
[3] J H J Hoeijmakers ldquoDNA damage aging and cancerrdquo TheNew England Journal of Medicine vol 361 no 15 pp 1475ndash14852009
[4] G Spivak ldquoNucleotide excision repair in humansrdquoDNARepairvol 36 pp 13ndash18 2015
[5] J Vijg XDong BMilholland andL Zhang ldquoGenome instabil-ity a conserved mechanism of ageingrdquo Essays in Biochemistryvol 61 no 3 pp 305ndash315 2017
[6] J I Garaycoechea and K J Patel ldquoWhy does the bone marrowfail in Fanconi anemiardquo Blood vol 123 no 1 pp 26ndash34 2014
[7] R Ceccaldi B Rondinelli andAD DrsquoAndrea ldquoRepair PathwayChoices andConsequences at theDouble-Strand BreakrdquoTrendsin Cell Biology vol 26 no 1 pp 52ndash64 2016
[8] R Biehs M Steinlage O Barton et al ldquoDNA Double-StrandBreak Resection Occurs during Non-homologous End Joiningin G1 but Is Distinct from Resection during HomologousRecombinationrdquo Molecular Cell vol 65 no 4 pp 671ndash684e52017
[9] A Ciccia and S J Elledge ldquoTheDNAdamage response makingit safe to play with knivesrdquoMolecular Cell vol 40 no 2 pp 179ndash204 2010
[10] L H Pearl A C Schierz S E Ward B Al-Lazikani and F MG Pearl ldquoTherapeutic opportunities within the DNA damageresponserdquo Nature Reviews Cancer vol 15 no 3 pp 166ndash1802015
[11] S-F Yang C-W Chang R-J Wei Y-L Shiue S-N Wang andY-T Yeh ldquoInvolvement of DNA damage response pathways inhepatocellular carcinomardquo BioMed Research International vol2014 Article ID 153867 2014
[12] M He W Zhou C Li and M Guo ldquoMicroRNAs DNAdamage response and cancer treatmentrdquo International Journalof Molecular Sciences vol 17 no 12 article no 2087 2016
[13] K A Cimprich and D Cortez ldquoATR an essential regulator ofgenome integrityrdquo Nature Reviews Molecular Cell Biology vol9 no 8 pp 616ndash627 2008
[14] B M Sirbu and D Cortez ldquoDNA damage response three levelsof DNA repair regulationrdquo Cold Spring Harbor Perspectives inBiology vol 5 article a012724 no 8 2013
BioMed Research International 13
[15] C Beck I Robert B Reina-San-Martin V Schreiber andF Dantzer ldquoPoly(ADP-ribose) polymerases in double-strandbreak repair focus on PARP1 PARP2 and PARP3rdquo Experimen-tal Cell Research vol 329 no 1 pp 18ndash25 2014
[16] D W Meek ldquoTumour suppression by p53 a role for the DNAdamage responserdquo Nature Reviews Cancer vol 9 no 10 pp714ndash723 2009
[17] A Rodrıguez L Torres U Juarez et al ldquoFanconi anemiacells with unrepaired DNA damage activate components of thecheckpoint recovery processrdquo Theoretical Biology and MedicalModelling vol 12 no 1 article 11 2015
[18] H Wang X Zhang L Teng and R J Legerski ldquoDNA damagecheckpoint recovery and cancer developmentrdquo ExperimentalCell Research vol 334 no 2 pp 350ndash358 2015
[19] P A Jeggo L H Pearl and A M Carr ldquoDNA repair genomestability and cancer A historical perspectiverdquo Nature ReviewsCancer vol 16 no 1 pp 35ndash42 2016
[20] F S Alkuraya ldquoPrimordial dwarfism An updaterdquo CurrentOpinion in Endocrinology Diabetes and Obesity vol 22 no 1pp 55ndash64 2015
[21] P Fortini C Ferretti and E Dogliotti ldquoThe response to DNAdamage during differentiation pathways and consequencesrdquoMutation ResearchmdashFundamental and Molecular Mechanismsof Mutagenesis vol 743-744 pp 160ndash168 2013
[22] B R Adams S E Golding R R Rao and K Valerie ldquoDynamicdependence on ATR and ATM for double-Strand break repairin human embryonic stem cells and neural descendantsrdquo PLoSONE vol 5 article e10001 no 4 2010
[23] A Klingseisen and A P Jackson ldquoMechanisms and pathways ofgrowth failure in primordial dwarfismrdquo Genes amp Developmentvol 25 no 19 pp 2011ndash2024 2011
[24] H Mokrani-Benhelli L Gaillard P Biasutto et al ldquoPrimaryMicrocephaly Impaired DNA Replication and Genomic Insta-bility Caused by Compound Heterozygous ATR MutationsrdquoHuman Mutation vol 34 no 2 pp 374ndash384 2013
[25] M OrsquoDriscoll A R Gennery J Seidel P Concannon and PA Jeggo ldquoAn overview of three new disorders associated withgenetic instability LIG4 syndrome RS-SCID and ATR-Seckelsyndromerdquo DNA Repair vol 3 no 8-9 pp 1227ndash1235 2004
[26] P Khetarpal S Das I Panigrahi and A Munshi ldquoPrimordialdwarfism overview of clinical and genetic aspectsrdquo MolecularGenetics and Genomics vol 291 no 1 pp 1ndash15 2016
[27] TOgi SWalker T Stiff et al ldquoIdentification of the First ATRIP-Deficient Patient and Novel Mutations in ATRDefine a ClinicalSpectrum for ATR-ATRIP Seckel Syndromerdquo PLoS Geneticsvol 8 no 11 Article ID e1002945 2012
[28] A Verloes S Drunat and P Gressens Primary autosomalrecessive microcephalies and Seckel syndrome spectrum disor-ders 2013
[29] A D Brown B W Sager A Gorthi S S Tonapi E J Brownand A J R Bishop ldquoATR suppresses endogenous DNA damageand allows completion of homologous recombination repairrdquoPLoS ONE vol 9 article e91222 no 3 2014
[30] E J Brown and D Baltimore ldquoEssential and dispensable rolesof ATR in cell cycle arrest and genome maintenancerdquo Genes ampDevelopment vol 17 no 5 pp 615ndash628 2003
[31] B Fitzgerald M OrsquoDriscoll K Chong S Keating and PShannon ldquoNeuropathology of fetal stage Seckel syndromeA case report providing a morphological correlate for theemerging molecular mechanismsrdquo Brain amp Development vol34 no 3 pp 238ndash243 2012
[32] L I Mullee and C G Morrison ldquoCentrosomes in the DNAdamage responsemdashthe hub outside the centrerdquo ChromosomeResearch vol 24 no 1 pp 35ndash51 2016
[33] K M Takikawa A Kikuchi A Yokoyama et al ldquoPerinatalfindings of Seckel syndrome A case report of a fetus showingprimordial dwarfism and severe microcephalyrdquo Fetal Diagnosisand Therapy vol 24 no 4 pp 405ndash408 2009
[34] Y Ruzankina C Pinzon-Guzman A Asare et al ldquoDeletion ofthe Developmentally Essential Gene ATR in Adult Mice Leadsto Age-Related Phenotypes and Stem Cell Lossrdquo Cell Stem Cellvol 1 no 1 pp 113ndash126 2007
[35] N E Mamrak A Shimamura and N G Howlett ldquoRecentdiscoveries in the molecular pathogenesis of the inherited bonemarrow failure syndrome Fanconi anemiardquo Blood Reviews vol31 no 3 pp 93ndash99 2017
[36] B P Alter ldquoDiagnosis Genetics and Management of InheritedBone Marrow Failure Syndromesrdquo International Journal ofHematology vol 2007 no 1 pp 29ndash39 2007
[37] L B Pontel I V Rosado G Burgos-Barragan et al ldquoEndoge-nous Formaldehyde Is a Hematopoietic Stem Cell Genotoxinand Metabolic Carcinogenrdquo Molecular Cell vol 60 no 1 pp177ndash188 2015
[38] G Pagano P Degan M DrsquoIschia et al ldquoOxidative stress asa multiple effector in Fanconi anaemia clinical phenotyperdquoEuropean Journal of Haematology vol 75 no 2 pp 93ndash1002005
[39] P FGiampietro P CVerlander J GDavis andADAuerbachldquoDiagnosis of Fanconi anemia in patients without congenitalmalformations An International Fanconi Anemia Registrystudyrdquo American Journal of Medical Genetics vol 68 no 1 pp58ndash61 1997
[40] P F Giampietro B Adler-Brecher P C Verlander S GPavlakis J G Davis and A D Auerbach ldquoThe need for moreaccurate and timely diagnosis in Fanconi anemia A report fromthe International Fanconi Anemia Registryrdquo Pediatrics vol 91no 6 pp 1116ndash1120 1993
[41] M P Wajnrajch J M Gertner Z Huma et al ldquoEvaluationof growth and hormonal status in patients referred to theinternational fanconi anemia registryrdquo Pediatrics vol 107 no4 I pp 744ndash754 2001
[42] N Giri D L Batista B P Alter and C A Stratakis ldquoEndocrineabnormalities in patients with fanconi anemiardquo The Journal ofClinical Endocrinology amp Metabolism vol 92 no 7 pp 2624ndash2631 2007
[43] S R Rose K C Myers M M Rutter et al ldquoEndocrine phe-notype of children and adults with Fanconi anemiardquo PediatricBlood amp Cancer vol 59 no 4 pp 690ndash696 2012
[44] A D Auerbach B Adler and R S K Chaganti ldquoPrenatal andpostnatal diagnosis and carrier detection of Fanconi anemia bya cytogeneticmethodrdquoPediatrics vol 67 no 1 pp 128ndash135 1981
[45] A D Auerbach M Sagi and B Adler ldquoFanconi anemiaPrenatal diagnosis in 30 fetuses at riskrdquo Pediatrics vol 76 no5 pp 794ndash800 1985
[46] L Faivre M F Portnoı G Pals et al ldquoShould chromosomebreakage studies be performed in patients with VACTERLassociationrdquo American Journal of Medical Genetics vol 137 no1 pp 55ndash58 2005
[47] B P Alter P S Rosenberg and L C Brody ldquoClinicaland molecular features associated with biallelic mutations inFANCD1BRCA2rdquo Journal ofMedical Genetics vol 44 no 1 pp1ndash9 2007
14 BioMed Research International
[48] K Myers S M Davies R E Harris et al ldquoThe clinicalphenotype of children with Fanconi anemia caused by biallelicFANCD1BRCA2mutationsrdquo Pediatric Blood amp Cancer vol 58no 3 pp 462ndash465 2012
[49] B G Yoon H N Kim U J Han et al ldquoLong-term follow-up of Fanconi anemia Clinical manifestation and treatmentoutcomerdquo Korean Journal of Pediatrics vol 57 no 3 pp 125ndash134 2014
[50] J G Hall ldquoReview and hypothesis Syndromes with severeintrauterine growth restriction and very short stature - Are theyrelated to the epigeneticmechanism(s) of fetal survival involvedin the developmental origins of adult health and diseaserdquoAmerican Journal of Medical Genetics Part A vol 152 no 2 pp512ndash527 2010
[51] A Petryk R K Shankar N Giri et al ldquoEndocrine disordersin Fanconi anemia Recommendations for screening and treat-mentrdquoThe Journal of Clinical Endocrinology ampMetabolism vol100 no 3 pp 803ndash811 2015
[52] S R RoseMM Rutter RMueller et al ldquoBonemineral densityis normal in children with Fanconi anemiardquo Pediatric Blood ampCancer vol 57 no 6 pp 1034ndash1038 2011
[53] A Petryk L E Polgreen J L Barnum et al ldquoBone mineraldensity in childrenwith fanconi anemia after hematopoietic celltransplantationrdquo Biology of Blood and Marrow Transplantationvol 21 no 5 pp 894ndash899 2015
[54] R Purkait A Mukherji S Datta and R Bhadra ldquoRenal arterystenosis An unusual etiology of hypertensive encephalopathyin a childwith fanconi anemiardquo Saudi Journal of KidneyDiseasesand Transplantation vol 26 no 4 pp 778ndash782 2015
[55] K H Chrzanowska H Gregorek B Dembowska-BaginskaM A Kalina and M Digweed ldquoNijmegen breakage syndrome(NBS)rdquoOrphanet Journal of Rare Diseases vol 7 article 13 2012
[56] L C Riches A M Lynch and N J Gooderham ldquoEarly eventsin the mammalian response to DNA double-strand breaksrdquoMutagenesis vol 23 no 5 pp 331ndash339 2008
[57] K Chrzanowska M Kalina H Rysiewski et al ldquoGrowthpattern in patients withNijmegen breakage syndrome evidencefroma longitudinal studyrdquoHormoneResearch in Paediatrics vol74 article S38 2010
[58] Group TINBSS ldquoNijmegen breakage syndromerdquo Archives ofDisease in Childhood vol 82 pp 400ndash406 2000
[59] M Digweed and K Sperling ldquoNijmegen breakage syndromeClinical manifestation of defective response to DNA double-strand breaksrdquo DNA Repair vol 3 no 8-9 pp 1207ndash1217 2004
[60] E Seemanova ldquoAn increased risk for malignant neoplasmsin heterozygotes for a syndrome of microcephaly normalintelligence growth retardation remarkable facies immun-odeficiency and chromosomal instabilityrdquo Mutation ResearchReviews in Genetic Toxicology vol 238 no 3 pp 321ndash324 1990
[61] K H Chrzanowska M Szarras-Czapnik M Gajdulewicz et alldquoHigh prevalence of primary ovarian insufficiency in girls andyoung women with Nijmegen breakage syndrome Evidencefrom a longitudinal studyrdquoThe Journal of Clinical Endocrinologyamp Metabolism vol 95 no 7 pp 3133ndash3140 2010
[62] C M R Weemaes T W J Hustinx J M J C Scheres P J JV Munster J A J M Bakkeren and R D F M Taalman ldquoAnew chromosomal instability disorder The nijmegen breakagesyndromerdquo Acta Paediatrica Scandinavica vol 70 no 4 pp557ndash564 1981
[63] A J Green J R W Yates A M R Taylor et al ldquoSevere micro-cephaly with normal intellectual development The Nijmegen
breakage syndromerdquo Archives of Disease in Childhood vol 73no 5 pp 431ndash434 1995
[64] D Gupta and A Nagarkar ldquoSpeech impairment in Nijmegenbreakage syndrome A rare anomalyrdquo International Journal ofPediatric Otorhinolaryngology vol 73 no 6 pp 873ndash875 2009
[65] P Muschke H Gola R Varon et al ldquoRetrospective diagnosisand subsequent prenatal diagnosis of Nijmegen breakage syn-dromerdquo Prenatal Diagnosis vol 24 no 2 pp 111ndash113 2004
[66] S Pasic M Cupic T Jovanovic S Djukic M Kavaric andI Lazarevic ldquoNijmegen breakage syndrome and chronic pol-yarthritisrdquo Italian Journal of Pediatrics vol 39 no 1 article no59 2013
[67] J P Patel J M Puck R Srinivasan et al ldquoNijmegen BreakageSyndrome Detected by Newborn Screening for T Cell ReceptorExcision Circles (TRECs)rdquo Journal of Clinical Immunology vol35 no 2 pp 227ndash233 2015
[68] I Demuth and M Digweed ldquoThe clinical manifestation of adefective response to DNA double-strand breaks as exemplifiedby Nijmegen breakage syndromerdquoOncogene vol 26 no 56 pp7792ndash7798 2007
[69] H Arora A H Chacon S Choudhary et al ldquoBloom syn-dromerdquo International Journal of Dermatology vol 53 no 7 pp798ndash802 2014
[70] C de Renty and N A Ellis ldquoBloomrsquos syndrome Why not pre-mature aging A comparison of the BLM andWRN helicasesrdquoAgeing Research Reviews vol 33 pp 36ndash51 2017
[71] C Keller K R Keller S B Shew and S E Plon ldquoGrowthdeficiency and malnutrition in Bloom syndromerdquo Journal ofPediatrics vol 134 no 4 pp 472ndash479 1999
[72] A Diaz M G Vogiatzi M M Sanz and J German ldquoEval-uation of short stature carbohydrate metabolism and otherendocrinopathies in Bloomrsquos syndromerdquo Hormone Researchvol 66 no 3 pp 111ndash117 2006
[73] C Ling J Huang Z Yan et al ldquoBloom syndrome complexpromotes FANCM recruitment to stalled replication forksand facilitates both repair and traverse of DNA interstrandcrosslinksrdquo Cell Discovery vol 2 article 16047 2016
[74] J S Renes R H Willemsen A Wagner M J J Finken and AC SHokken-Koelega ldquoBloom syndrome in short children bornsmall for gestational age A challenging diagnosisrdquoThe Journalof Clinical EndocrinologyampMetabolism vol 98 no 10 pp 3932ndash3938 2013
[75] M Maciejczyk B Mikoluc B Pietrucha et al ldquoOxidativestress mitochondrial abnormalities and antioxidant defense inAtaxia-telangiectasia Bloom syndrome andNijmegen breakagesyndromerdquo Redox Biology vol 11 pp 375ndash383 2017
[76] R M Brosh M Bellani Y Liu and M M Seidman ldquoFanconiAnemia A DNA repair disorder characterized by accelerateddecline of the hematopoietic stem cell compartment and otherfeatures of agingrdquo Ageing Research Reviews vol 33 pp 67ndash752017
[77] S Yan M Sorrell and Z Berman ldquoFunctional interplay be-tween ATMATR-mediated DNA damage response and DNArepair pathways in oxidative stressrdquo Cellular and Molecular LifeSciences vol 71 no 20 pp 3951ndash3967 2014
[78] L M M Nardozza A C R Caetano A C P Zamarian etal ldquoFetal growth restriction current knowledgerdquo Archives ofGynecology and Obstetrics vol 295 no 5 pp 1061ndash1077 2017
[79] M Tomas Vila J P Verdu M R Piera and C O AlonsoldquoNijmegen breakage syndrome phenotype a disorder to con-sider in the diagnosis ofmicrocephalyrdquoAnales De Pediatria vol74 pp 58ndash60 2011
Submit your manuscripts athttpswwwhindawicom
Stem CellsInternational
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
MEDIATORSINFLAMMATION
of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Behavioural Neurology
EndocrinologyInternational Journal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Disease Markers
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
BioMed Research International
OncologyJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Oxidative Medicine and Cellular Longevity
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
PPAR Research
The Scientific World JournalHindawi Publishing Corporation httpwwwhindawicom Volume 2014
Immunology ResearchHindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Journal of
ObesityJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Computational and Mathematical Methods in Medicine
OphthalmologyJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Diabetes ResearchJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Research and TreatmentAIDS
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Gastroenterology Research and Practice
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Parkinsonrsquos Disease
Evidence-Based Complementary and Alternative Medicine
Volume 2014Hindawi Publishing Corporationhttpwwwhindawicom

BioMed Research International 3
p53
53BP1
Rif1
CtlP
BRCA1
KU80
KU70
+
+NBN
RAD50
MRE11gH2AX
gH2AXgH2AX
gH2AX
RPARPARPARPA
FAN
CM
G
G
Transducers ATMATR
Checkpoint
DNAPKcs
Chromatinreorganization
Effectors
Sensors and mediators
Senescence Celldeath
Reparable damage Irreparable damage
DNA repair Misrepair Genomicinstability
Normal cell growth Abnormal cell growth(cancerhypoplasia) Outcomes
or
Figure 2 DNA damage response can result in different outcomes following single strand breaks interstrand crosslinks and double strandbreaks Each DNA lesion is recognized by specific sensor proteins according to the cell cycle phase in which the cell is during S phase theprotein FANCM identifies a replication fork arrested by an ICL MRN + BRCA1 sense DSBs meanwhile Ku70Ku80 + 53BP1 can recognizeDSBs across the entire interphase RPA detects and covers ssDNA primarily during S phase The sensing process is then transduced andamplified on chromatin through a series of posttranslational histone modifications such as phosphorylation of H2AX (120574H2AX) on both sidesof the DSB These changes allow the recruitment of the specialized transducer kinase ATR that mainly responds to RPA-covered ssDNAoriginated by replication stress or DNA lesions such as ICLs concurrently ATM responds to DSBs Kinases activate several effector proteinsincluding the transcription factor p53 which acts downstream regulating diverse outcomes according to the type and quantity of remindinglesions in the cell
in order to repair a DSB using HR alt-NHEJ or SSA the 31015840blunt endsmust be processed to allow the loading of theMRNcomplex (a heterotrimer integrated by three proteins calledMRE11 RAD50 and NBN) to continue the repair processThis occurs primarily during the S and G2 phases of the cellcycle when sister chromatids are available and can be usedfor HR error-free repair [7 9]
3 DNA Damage Response
Even when each specific DNA lesion stimulates a particularDNA repair mechanism cells trigger a common generalprogram known as the DNA damage response (DDR) whichis charged with lesion detection signaling and repair pro-motion as well as cell cycle progression control It is nosurprise that the DDR is an extremely controlled process theexquisite balance between cell survival and cell death and
senescence relies on it [1 9 10] Tissue homeostasis or growthabnormalities such as cancer [11] or tissue hypoplasia dependamong other things on the amount and type of genomicdamage sensed and processed by the DDR
The DDR is composed of a network of regulatory non-coding RNAs and proteins that act as sensors transduc-ers and effectors [1 12] Sensor proteins recognize specificlesions (Figure 2) For example the FANCM protein detectsthe stalled replication fork caused by interstrand crosslinks(ICLs) theMRNcomplex is the typical sensor ofDSBs duringSG2 phase the Ku70Ku80 heterodimer is the primary DSBssensor duringG1while replication proteinA (RPA) overcoatssingle-strand DNA (ssDNA) found either at processed DSBoverhangs to be repaired by HR or at stalled replication forks[13]
Following recognition of the lesions by sensors andmediators the signal is amplified by transducer proteins
4 BioMed Research International
Table 1 Chromosomal instability syndromes with intrauterine growth deficiency
Syndrome Genes Function in DDR Repair pathway Cytogenetic alteration
Fanconi anemia 21 FANC genes
ICL detection andprocessing generation ofadducts and DSBs (sensorsmediators and effectors)
Homologous recombination Chromatid and chromosomal breaksRadial figures
Seckel Syndrome 1 ATRSSBs detection and signaltransduction(transducer)
Homologous recombinationNonhomologous recombination
Chromatid and chromosomal breaksandRearrangements
Nijmegen BreakageSyndrome NBN
DSBs detection andsignaling (sensor andmediator)
Homologous recombinationNonhomologous recombination
Chromatid and chromosomal breaksAneuploidiesRearrangements affectingchromosomes 7 and 14
Bloom Syndrome BLMHelicase process SSBs andHolliday Junctions(effector)
Homologous recombination QuadriradialsIncrease in sister chromatid exchange
The PIKK kinases (Phosphatidyl Inositol 3-Kinase-relatedKinases) family is the most important of this group it isintegrated by ataxia telangiectasia and Rad3-related (ATR)Ataxia telangiectasia-mutated (ATM) and DNA dependentprotein kinase (DNAPKcs) ATR is activated during the Sphase of the cell cycle in the presence of DNA damagesuch as base adducts crosslinks single-strand breaks (SSBs)replication stress andDSBs that originate during the S phasewhile ATM and DNAPKcs are activated by DSBs at anypoint of the cell cycle [13 14] The DDR kinases activatesignaling cascades through posttranslationalmodifications ofvarious proteins including phosphorylation ubiquitylationand PARylation which play a central role in regulation ofthe DDR [15] Specifically ATR and ATM can autoactivate ortransactivate each other through phosphorylation and thenphosphorylate the histone variant H2AX (120574H2AX) that actsas a platform to recruit DDR factors and prepare the cell torestore DNA integrity ATR and ATMrsquos main downstreamphosphorylation targets are proteins Chk1 and Chk2 andthe important effector p53 their activation allows regulating(a) the chromatin structure surrounding the lesion (b)checkpoints that stop the cell cycle (c) DNA repair proteins(d) proteins that induce senescence and (e) proteins that leadto cell death (Figure 2) [10 16]
Finally if DNA lesions are repaired the checkpoint that isresponsible for stopping the cell cycle is turned off and the cellcycle is allowed to restart through a process called checkpointrecovery This process is only turned on when the signalingfor theDNA lesions is silenced and the surviving cell recoversits normal homeostasis and growth When DNA damagecannot be properly repaired the cellrsquos destiny should beeither senescence or death Otherwise cellsmight dividewithunrepaired DNA damage through an erroneous activation ofthe checkpoint recovery process that allows cell survival withgenomic instability to promote cell dysfunction and cancer[17]
4 DNA Damage Response and Disease
Unrepaired or misrepaired lesions in DNAmay immediatelyimpair replication and transcription affecting the whole cell
function In an irreparable damage situation the amountand type of lesions as well as the cell cycle phase in whichthe cell is will influence the DDR response in order tofavor immediate cell death or the conversion of DNA lesionsinto durable mutations or stable chromosomal abnormalities[3]
Cell survival despite genomic damage can directly affectcell growth this can be evidenced by two opposite outcomesOn the one hand there can be an overgrowth effect sincemutations in critical genes such as oncogenes or tumorsuppressor genes can alter cell function and increase thelikelihood of cancer development [3 18 19] On the otherhand there can be cell hypoplasia or cell loss this happenswhen irreparable damage leads to either cell death or cellsenescence a cancer-protecting condition in which cellsare alive but unable to proliferate limiting the growth ofthe tissues and conducting to aging (Figure 2) This isevidenced by the phenotype of patients affected by diseasesthat alter the DDR and DNA repair in which growthalteration and increased cancer susceptibility are importantfeatures
5 Chromosome Instability Syndromes
Mutations in at least 114 genes involved in the DDR leadto disease some of the mutations are somatic resulting invarious types of spontaneous cancer and others are geneticdiseases with constitutionalmutations that lead to syndromesthat may or may not be related to the development ofcancer [10] Among the genetic diseases with mutations inDDR genes the chromosomal instability syndromes (CIS)are a group of rare Mendelian diseases characterized byincreased chromosome breakage resulting from unrepairedor misrepaired DNA strands breaks Other than chromoso-mal instability they also have clinical overlapping featureslike cancer proneness premature aging and growth abnor-malities even though each CIS has a particular phenotypethat distinguishes it from the others Only a subgroup of thesepatients has prenatal growth alterations this review focuseson those syndromes (Table 1)
BioMed Research International 5
6 DDR Alteration and Growth Failure
Historically disruption of the DDR has been associatedwith cell growth abnormalities in a unilateral way alwayspointing towards the increased cell number in the form ofderegulated cell proliferation in cancer [19] But there islittle information on how DDR alterations can also lead toderegulation of growth in the opposite direction resultingin lack of growth due to cell death and low cell repro-duction One of the first observations to partner growthdeficiency with an altered DDR was the finding that someSeckel syndrome patients (SS) a rare phenotype consistingof primordial dwarfism and microcephaly had mutationsin the ATR gene which encodes the ATR kinase a DDRtransducer Further analysis of SS patients revealed locusheterogeneity for this phenotype mutations in other genesrelated to DDR or DNA repair also led to this clinical pictureThis observation has reinforced the association betweenDDRfailure and severe intrauterine growth retardation Moreovergenes that participate in centrosomal biology are also relatedto the uncommon phenotype of microcephalic primordialdwarfism suggesting that centrosomes have a central rolefor the adequate differentiation of early neuroprogenitorsIt has then been proposed that failure in cell proliferationsecondary to abnormal mitosis is the cause of primordialdwarfism since the multipolar spindles result in the acti-vation of checkpoints reducing proliferation and activatingapoptosis [20]
For the phenotype of growth restriction to be evidentprenatally the mechanisms regulating growth must be com-promised from the beginning of the development in embry-onic stem cells (ESCs) which are pluripotent cells derivedfrom the three primary germ layers ectoderm endodermandmesoderm and that have the capacity to differentiate intomore than 200 cell typesThese cells have been proven to havean extremely efficient DDR and proficient DNA repair mech-anisms that allow for a rigorousmaintenance of their genomeintegrity otherwise unrepaired DNA damage in ESCs wouldbe amplified affecting normal human development
ESCs have an extremely active proliferation rate theircell cycle has a characteristically reduced G1 phase andrepair mechanisms are heightened When comparing ESCsto fibroblasts it stands out that MMR is enhanced BERand NER repair pathways are highly competent and therepair of DSBs is preferentially made through the reliableHR pathway [21] Moreover when HR is not available andDSBs accumulate apoptosis is the preferred route to removehighly damaged cells It is interesting that DSB repair inESCs requires signaling through ATR instead of ATM ESCshave a special mechanism to deal with DNA damaged cellswhen inefficient DNA repair or DDR affects the induction ofapoptosis or autophagy [22] This mechanism leads to ESCdifferentiation that is driven by damage-induced expressionof the p53 transcription factor damaged differentiated cellsare efficient in cell cycle arrest and apoptosis This strategyresults in the maintenance of genetic stability in a decreasednumber of ESCs and a portion of differentiated cells thatbecome senescent both resulting in growth deficiency[21]
Growth deficiency is at the center of many diseasesincluding extremely low body size In mammals overall sizeis determined by the number of cells body mass is then thesum of all the cells that have proliferated minus those thathave died A fetus that is growing harmonically has accuratebalance between these two processes failure of either one ofthese results in dramatic effects when they occur in the ESCpopulation a decrease in cell proliferation rate or an increasein apoptosis leads to intrauterine growth retardation (IUGR)[23]
7 Chromosome Instability Syndromes withIntrauterine Growth Retardation
71 Seckel Syndrome Seckel syndrome (SS) is an autosomalrecessive disorder clinically and genetically heterogeneousSo far at least six genes have been associated with the Seckelphenotype most of these genes participate in ATR-mediatedDDR and in centrosomal function Two clinical subgroupscan be identified on the one hand patients with mutationsin ATR NIN and ATRIP genes only present the Seckelphenotype while on the other hand those with mutationsin CENPJ CEP152 or RBBP8 show allelic heterogeneity andbesides the SS phenotype can also manifest as a spectrumof disorders known as Primary Autosomal Recessive Micro-cephalies [24ndash28] SS patients who bear mutations in ATRshow a classical Seckel phenotype the SS data presented herewill be limited to such patients
ATR is localized in 3q23 it is one of the serine threoninekinases that belong to the PIKK family They have a funda-mental role in the DDR since they participate as transducersin the signaling of DNA lesions especially when the DDRresponds to stalled replication forks and bulky lesions inDNA[24 25] ATR responds preferentially to ssDNA during the Sphase It also plays a crucial role in preventing DNA breakscaused by fork pausing when DNA replication machineryfinds DNA lesions or complex DNA structure and sequences[24] ATR stability depends on binding of ssDNA to theATR cofactor ATRIP (ATR interacting protein) and thesingle-stranded binding protein (RPA) ATRIP is required forATR localization to the ssDNA regions and hence for ATRactivation [25 27] Major functions of ATR are activation ofcell cycle check point arrest stabilization of stalled replicationforks and promotion of replication fork restart which isachieved through its ability to phosphorylate a wide range ofsubstrates that include p53 and H2AX [27 29]
Cellular phenotype of ATR deficient cells is characterizedby decreased phosphorylation of ATR-dependent substratesas well as an impaired G2M checkpoint arrest These cellsare characterized by markers that signal unrepaired DSBslike the presence of 120574H2AX chromosomal breakage [2629 30] and micronuclei formation This cellular phenotypemay be originated by a failure to recover from replicationstalling which generates DSBs that are normally repairedby HR when they occur during SG2 In SS cells theabsence of ATR is critical during embryonic developmentthis deficiency leads to genomic instability cell senescenceand cell death that leads to fetal growth and accelerated aging[31]
6 BioMed Research International
Figure 3 Seckel syndrome patient Note the severe microcephalyand the ldquobird-likerdquo appearance facies with micrognathia and reced-ing forehead The patient is severely disabled with no independentmarch
Moreover it appears that ATR and the other SS genes notonly participate in the DDR but also take part in the controlof centrosome maturation This engagement in centrosomebiology is also true for other DDR proteins like BRCA2biallelic mutations in its gene are responsible for a subgroupof Fanconi anemia patients [32]Theunifying feature betweenall Seckel patients irrespective of the molecular defect isthat their cells have an altered cell cycle progression thatis particularly evident during high rate cell division whenthere is hypersensitivity to replicative stress and centrosomaldysfunction This is especially important in cells with highdivision rates like the ones found in developmental stageswhere rapid replication is key [24 27]
SS is characterized by IUGR dwarfism microcephaly(below minus4 SD) mental retardation and some other anomalieslike luxation of the head of the radius scoliosis bone agedelay and seizures (Figure 3) The distinctive facial featuresinclude a prominent nose with micrognathia and a recedingforehead resulting in a ldquobird-like appearancerdquo [26 31 33]Since this syndrome has important clinical heterogeneityother anomalies have been reported including mandibularhypoplasia sternal abnormalities clinodactyly and low setears with hypoplastic lobules Although rare other reportedfeatures are moyamoya syndrome osteosarcoma and pol-yarteritis nodosa [26] Cerebral malformations like neuronalmigration abnormalities have been described but are notalways present [33] No glucose metabolism abnormalitieshave been reported
Dwarfism can be related to a reduction in the totalnumber of cells generated during development leading tohypoplastic tissue and reduced organism size [23] On theother handmicrocephalymay be related to an impairedDNAdamage response signal that could alter the cellular thresholdfor cell death resulting from DNA damage increasing thelevels of apoptosis during development developing neuronsare rapidly proliferating and potentially generate high levelsof oxidative damage which may lead to a higher level oflesions being faced at replication forks [23 25] Also analtered mitosis secondary to impaired spindle formationcould delay mitotic progression and increase the proportionof nonviable cell divisions Finally the stem cells may beaffected by abnormal centrosomal function Stems cells haveasymmetric divisions in order to preserve the characteristics
Figure 4 Fanconi anemia patient This six-year-old girl is 105 cmtall her height is just below the 5th percentile and her at-term birthweight is reported to be of 1900 gr Characteristic features of FA areevident skin hyperpigmentation bilateral radial defects consistingof bilateral thenar hypoplasia and absent fold of the right thumbwhich cannot be bent
of a stem cell and the centrosomes play an important role insuch divisions [23]
There is limited clinical information regarding age-related diseases in SS there is a void of prospective follow-up data from these patients that can only be obtained byfollowing a cohort of SS patients something that is apparentlynot being done at this time Nevertheless animal modelsbring some clues over the possibility of an aging phenotypein SS patients since ATR deficient adult mice show prematureage-related phenotypes as well as increased deterioration oftissue homeostasis [29 34]
72 Fanconi Anemia DNA interstrand crosslinks are ex-tremely noxious DNA lesions that affect central cellularprocesses like transcription and replication The FABRCApathway is responsible for the appropriate processing ofthese lesions protein products from at least 21 FANC genesparticipate in this pathway [35] The malfunction of any ofthose FANC proteins leads to the clinical phenotype knownas Fanconi anemia (FA) which is characterized by shortstature congenital malformations from the VACTERL-Hspectrum bone marrow failure and an increased suscepti-bility to cancer like acute myeloid leukemia epithelial headand neck cancer [36] (Figure 4) Most of the FA families bearbiallelic mutations in FANC genes that have an autosomicrecessive inheritance pattern only families with mutations inFANCB show an X-linked recessive pattern while those inwhich FANCR is the affected gene demonstrate an autosomicdominant one [35]
The FABRCA is an S-specific pathway that has 3 basicsteps it starts with the detection of the ICL by the proteinFANCM followed by the recruitment of the FA core com-plex that is responsible for the monoubiquitination of theFANCD2I heterodimer which in turn favors the recruit-ment of effector FANC-repair proteins that restore the DNAto its original form [35]
BioMed Research International 7
(a) (b)
Figure 5 Chromosomal instability induced by 40 ngml mitomycin C (a) Lymphocytes from a healthy individual (b) lymphocytes from aFA patient Short arrows show chromosomal breaks the long arrow shows a quadriradial figure Note the exacerbated chromosome instabilityfound in the FA patient
The cellular phenotype of FA derived cells is extremelyconstant An aberrant FABRCA pathway can result inunrepaired DSBs that manifest as chromosomal breaks orabnormal repair by an error-prone repair pathway that resultsin radial figures These alterations are cytogenetic evidenceof chromosomal instability which is the hallmark of FA cellsand is exploited for clinical diagnostic purposes (Figure 5)The agents capable of inducing this chromosomal instabilityare from endogenous origin like aldehydes [37] and reactivespecies of oxygen (ROS) [38] as well as exogenous sourceslike bifunctional alkylating agents (diepoxybutane or mito-mycin C) In addition FA cells have accumulation of cells inG2 phase of the cell cycle resulting from a functional G2Mcheckpoint and a proapoptotic phenotype
In contrast with the cellular FA phenotype the clinicalpicture in FA patients is extremely variable not every patientwill have all the manifestations one-third of patients do nothave congenital malformations [39] while almost 90 willdevelop bone marrow failure [36] One of the more constantmanifestations in FApatients is growth parameters alterationAn analysis from the international Fanconi anemia registry(IFAR) data showed that over 60 of FA patients presentedshort stature (below the 5th percentile) while birth lengthandweight below the 5th percentile was respectively reportedin almost 30 and nearly half of FA patients [40]Moreover aprospective study of data from 54 IFAR participants showedthat the mean standard deviation score (SDS) for height inthese patients was significantly below normal for age and sexat minus235 plusmn 028 meanwhile mean SDS for weight was betteralthough below normal (minus126 plusmn 024) In this study perinatalgrowth data was not reported [41]
Other than the IFAR data on growth there are anothertwo studies that analyze growth parameters of FA patientsAnthropometric measurements from 45 patients with Fan-coni anemia from the National Cancer Institutersquos inher-ited bone marrow failure syndromes (IBMFS) cohort wereassessed This cohort had a mean SDS for height of minus21 plusmn
189 The height of over half of the participants (54) wascategorized as short (SDS gt 20 SD) in this subset of patientsthe mean SDS for height was minus38 plusmn 15 [42] Finally theevaluation of 120 FA patients from the FA ComprehensiveCare Clinic of Cincinnati Childrenrsquos Hospital Medical Centerrevealed that median height SDS was shorter than expectedin children and adults irrespective of gender Furthermorethis study presented birth information from 70 patients (59children and 11 adults) from the cohort 51 of the childrenand 3 adults were born small for gestational age their medianbirth weight at term was 202 kg (range 15ndash26 kg) [43] Theintrauterine growth restriction seen in FA patients has alsobeen documented in several case reports in which at-termbirth weight ranges from 1780 to 3200 gr [44ndash49] Eventhough growth abnormalities have been identified in FApatients with mutations in almost every FANC gene it hasbeen shown that patientswithmutations in certain genes havea more severe growth delay That is the case for patients withbiallelic mutations in FANCD1 [47 48] as well as those whobear mutations in FANCC for whom an SDS for height ofminus384 has been found [41]
Endocrine abnormalities have been proven to be aninherent part of the FA phenotype up to 80 of patientshave one or more endocrine abnormalities Besides growththyroid function and glucose homeostasis are frequentlyaffected [40ndash43] Considering the existing evidence for arelationship between low birth weight and an increased riskfor noncommunicable adult diseases like diabetes hyperten-sion heart disease dyslipidemia and osteoporosis [50] it isrelevant to revise these diseases in FA The FA cohorts inwhom growth was assessed were also evaluated for endocrinestatus Glucose homeostasis is affected in a large portion ofFA patients impaired glucose tolerance has been found in27ndash68 of them whereas diabetes has a prevalence of 8ndash10Dyslipidemia has been assessed in only a small portionof FA patients but it has been found in 17ndash55 of theevaluated subjects [51]There are conflicting results over bone
8 BioMed Research International
mineral density (BMD) status in FA the first time this wasevaluated 92 of the patients were found to have osteopeniaor osteoporosis [42] nevertheless a study that evaluated alarger FA cohort found that lowBMD is not a frequent finding[52] Further research on this topic has raised the questionof whether BMD deficit is intrinsic to the FA phenotype ora consequence of hematopoietic cell transplantation (HCT)an interrogation that is still awaiting to be answered [53]Cardiovascular adult diseases are not relevant in the FA phe-notype heart disease in these patients is from the congenitaltype as 13of patients have cardiacmalformations [40] whilehypertension has only been reported in two patients as theresult of renal malformations [54]
Findings from the different FA cohorts show that shortstature is an inherent feature of the FA phenotype thisfeature does not respond to a single explanation the apoptosisprone FA cellular phenotype is certainly a contributing factorfor this The fact that FA patients have a constitutionallydefective pathway since conception could explain the clinicalphenotype of RCIU Short stature may also be exacerbated byaccompanying endocrinopathies The cooccurrence of manyendocrine alterations has encouraged unifying explanationssome have proposed that endocrinopathies are secondaryto increased cytokine activity found in FA cells [41] whileothers favor the view that some endocrine secretory cellsmight be damaged by high levels of reactive oxygen specieswhich are known to be elevated in FA patients [43] In linewith the developmental origin of adult health and diseasetheory it could also be possible that the increased prevalenceof glucose homeostasis alterations and dyslipidemia reportedin FA patients is a consequence of intrauterine growthrestriction of these patients Nevertheless the attemptedgenotype-phenotype correlation of the endocrine phenotypein FA patients does not seem to support that Patients withmutations in FANCA show a mild endocrine phenotype inwhich height is not severely affected and insulin resistanceis mild whereas mutations in FANCC which are relatedto shorter stature have the least insulin resistance [41]Moreover no direct relationship between birth weight andglucose tolerance was identified when it was intentionallylooked for [43] although the number of patients in whichthese observations were made is limited
73 Nijmegen Breakage Syndrome Nijmegen breakage syn-drome (NBS) is an autosomal recessive disease caused bybiallelic mutations in NBN a gene that encodes nibrin aprotein involved in DNA repair and cell cycle checkpointregulation It participates in the former by sensing double-strand breaks as part of the trimeric complexMRN alongsideMRE11 andRAD50Meanwhile for the latter it contributes tothe appropriate activation of ATM andATRwhich are centraltransductors of the DNA damage response (DDR) [55] Themalfunction of nibrin translates in a cellular phenotypemarked by chromosomal instability radiosensitivity reducedphosphorylation of ATM substrates and S and G2M cellcycle defects [56] Chromosome instability is evidenced bycytogenetic methods in 10ndash60 of cells in the form of breaksand numeric and structural aberrations translocations andinversions affecting chromosomes 7 and 14 are found in the
147
Figure 6 Translocation between chromosomes 7 and 14 is typicalin NBS patientsrsquo cells
majority of NBS patients and are considered a cytogeneticcharacteristic of this syndrome (Figure 6) [57]
The clinical impact of these alterations is a phenotypecharacterized by microcephaly a distinctive facial appear-ance consisting of receding forehead and mandible and aprominent mid face with a long nose and philtrum aswell as immunodeficiency that leads to recurrent infectionsand an increased risk for the development of neoplasiaparticularly leukemia and lymphoma According to theinternational Nijmegen breakage syndrome study groupgrowth retardation is also a hallmark of this disease [58]although there is not many details about this feature in theliterature
Most of the information on the natural history of NBSavailable today comes from patients participating in reg-istries in which fairly large cohorts of NBS patients areincluded There is a large representation of Slavic patientsin these cohorts which correlates with the high carrierfrequency of a founder mutation of NBN in this populationFrom these studies it is evident that the most severelyaffected anthropometric measure in NBS patients is headcircumference since all participants display microcephalyeven though only 75 display this feature at birth Whenit comes to growth parameters the same study states thatall patients have growth retardation which is described asproportionate and early occurring [58] although the specifictemporality is not defined A posterior report points out thatthe growth retardation seen in most NBS patients locatesthem in the 10th percentile in growth charts and that birthheight and weight are usually within normal parameters [59]Nevertheless there are other authors who report prenataland postnatal growth retardation [55 60] and a tendency forshort stature that is more evident during the first year of life[61] Also several case reports of NBS patients in which birthweight is informed demonstrate prenatal growth restriction[62ndash67] although this could represent a report bias Themore comprehensive data analysis on growth that includesperinatal information of NBS patients is the one that analyzesdata from 67 patients followed for 15 years Eighty percentof these patients were born at term the girls were found tohave a mean birth weight of 27 kg and mean birth heightof 514 cm while boys were reported to have a mean birthweight of 28 kg and mean birth height of 523 cm Moreoverall patients irrespective of gender were found to have ameanheight reduced by over 2 SDS at one year old [57] These data
BioMed Research International 9
(a) (b)
Figure 7 Sister chromatid exchange in cells from a healthy individual (a) and from a BLM patient (b)
support the fact that growth retardation in NBS is a prenatalphenomenon
Nibrin has been found to have essential functions inthe regulation of the cell cycle which translates into anabsolute need for this protein for cell proliferation [68]It would seem logical that mutations of the NBN genethat compromise the appropriate function of nibrin wouldlead to abnormal growth when thought from an organismperspective Mechanistically speaking poor cellular growthcaused by mutations in a particular gene can be thought ofas the main explanation for the growth restricted phenotypebut it has been shown that mutations in other DDR genesthat share the cellular phenotype of poor growth like ATMdo not replicate the compromised growth phenotype atthe organism level growth retardation is absent in ataxiatelangiectasia (AT)This data suggests that there are certainlyother contributing factors to the abnormal growth phenotypeseen in NBS patients [58]
74 Bloom Syndrome Bloom syndrome (BS) is an autosomalrecessive disorder caused by homozygous or compoundheterozygous mutations in the BLM gene (15q261) thatencodes the RecQL3 helicase BLM has a critical role inthe maintenance of genome stability acting at the interfacebetweenDNAreplication recombination and repair [69 70]To date over sixty different mutations including nonsenseand missense have been identified all of them result inthe inactivation of BLM and the consequent loss of itshelicase activity The BLM gene encodes a 1417 amino acidnuclear protein its expression peaks during the S and G
2M
phases of the cell cycle which is consistent with its rolein DNA replication and recombination BLM specificallyunwinds structures like forked DNA duplexes RNA-DNAheteroduplexes and R-Loops which explains its importanceduring replication fork progression and transcription besidesit is central for Holliday Junctions (HJs) dissolution forHR The dissolution of HJs by the topoisomerase III120572-BLMcomplex cannot be replaced by any other RecQ helicase inthe family [69 70] It has also been found to have a role in
the annealing activity of the ssDNA the proper sister chro-matid segregation during mitosis and telomere maintenance[70]
BLM can have both pro- and antirecombinogenic func-tions that are regulated by posttranslational modificationsincluding phosphorylation sumoylation and ubiquitination[70]
BLM also enables sister chromatid segregation by pro-cessing unresolved replication intermediates that manifest inmitosis as ultrafine DNA bridges (UFBs) and together withtopoisomerase III120572 RMI1 and RMI2 localizes to UFBs inanaphase BML deficient cells exhibit and increase frequencyof UFBs suggesting a role of BLM in the resolution ofthese structures Failure to resolve these UFBs leads to DNAbreakage as mitosis proceeds [70]
Therefore BS cells are characterized by an increasein chromosomal aberrations including chromatid gapsand breaks telomere associations and quadriradial chro-mosomes resulting from unsolved recombination betweenhomologous chromosomes BS cells exhibit increased muta-tion rates and the genomic instability includes elevatedmitotic HR and unequal sister chromatid exchange (SCEs)(Figure 7) Perhaps the most characteristic feature is the overtenfold increase in SCEs which results from crossover eventsduring HR repair of damage replication forks [50 69 70]
Clinically the more striking BS feature is IUGR averagebirth weight at term is 1850 g and birth length is 44 cmFor both boys and girls weight and length in BS are morethan two standard deviations below normal indicating thatgrowth retardation has a prenatal origin At postnatal agesheight remains below the normal range and is accompaniedby a paucity of subcutaneous fat Average adult height inmales has been found to be 148 cm (130ndash162 cm) whilein females it has been reported to be 139 cm (122ndash151 cm)[50 70 71]
BS patients have overall proportionated short staturebut the head is reported to be small and narrow relativelyto the body size it is described as mild microcephalyand is accompanied by malar hypoplasia Patients have
10 BioMed Research International
Figure 8 Bloomsyndromepatient inwhom the characteristicmalarerythema is present
been described to have a high pitched voice [50 70] Theskin appears normal at birth but in the first or secondyear of life in response to sun exposure children developan erythematous rash with a butterfly distribution in themalar area and the back of hands and feet The rash caninclude telangiectasia The severity varies between patientssome can even lose their eyelashes and develop blisteringaround the mouth The presence of cafe-au-lait spots andhypopigmented areas of skin associated with contiguoushyperpigmented areas is common (Figure 8) Intellectualabilitiesmay be limited in some patients and normal in others[50 70]
Other clinical conditions reported in BS patients are gas-troesophageal reflux and diarrhea in infants mild immuno-logical deficiency with frequent episodes of otitis mediaazoospermia or severe oligospermia in males and prema-ture cessation of menstruation in females minor anatomicdefects and increased risk for neoplasia which is the maincause of dead in BS [70] Another common medical con-dition in BS is diabetes mellitus associated with impairedglucose tolerance and insulin resistance it has been reportedin up to 16 of patients [70] According to data fromthe Bloomrsquos Syndrome Registry diabetes in these patientstends to begin early with a mean age at diagnosis of 266years It is not associated with ketosis and it does nothave the classical hereditary pattern seen in type 2 diabetes[50 72]
Short stature in BS is not due to hormonal causes sincethe size of cells in persons with BS is normal it has beenhypothesized that there are fewer of them due to either adecrease in the cell division rate an increase in apoptosis oreven a combination of both BS cells have troublemeeting thedemands of fast cell divisions encountered in tissues duringembryonic development The leading hypothesis suggeststhat problems arising during DNA synthesis require a longerS phase to overcome the challenge which translates intoslowing of the cell division rate and an increase in apoptosis[70]
8 Concluding Remarks
This review has focused on discussing phenotypes of CISin which there is a prenatal alteration of growth The foursyndromes discussed here are rare diseases whose prevalenceis difficult to calculate since appropriate identification anddiagnosis of affected individuals among the general popula-tion are not straightforward It is important to note that theavailable information on the natural history of FA NBS andBS comes from the analysis of several patients that participatein registries This strategy results in detailed informationthat permits a better analysis of the clinical phenotype ofthese rare diseases Meanwhile available data of SS is moreanecdotic which results in a nonsystematic gathering ofinformation which is thus frequently incomplete
From the available clinical data of these CIS it is evidentthat growth is not affected in the same extent for all ofthese syndromes the phenotypes that exhibit a more severelystagnated perinatal growth are BS and SS The severe growthdelay reported in these patients has been described as apathognomonic sign of these diagnoses In patients withFA perinatal growth can also be severely affected but notevery FA patient shows this manifestation Finally NBShas been described to have growth retardation of prenatalorigin of mild severity almost within the lower normal range(Figure 9) The cephalic circumference can be affected in allof these syndromes severe microcephaly is pathognomonicin SS and NBS it is described as mild for BS patients and it isfound in less than half of FA patients (Table 2)
When trying to understand why a subset of CIS showsprenatal growth retardation it could be alleged that theintrinsic chromosomal instability is responsible for it Butthis would not explain why prenatal growth retardation isnot a universal CIS feature for example ataxia telangiectasiapatients who have biallelic mutations in the ATMkinase genedo not show prenatal growth delay It strikes that a molecularcommon feature shared by the prenatal growth retardationSIC phenotypes is that they are caused by mutations ingenes that are necessary for an appropriate response to DSBsduring the S phase of the cell cycle The molecular defectin SS affects the functioning of ATR the preferred DDRtransducing kinase used by highly replicating ESCs TheFABRCA pathway which is affected in patients with FAdetects ICLs upon replication fork arrest Nibrin the proteinaffected in patients with NBS is induced during S phasefor the detection of DSBs And the BS helicase forms aFANCM-BLM complex needed to sense ICLs during S phase[73] It could then be argued that altered DNA replicationis an important factor for the development of intrauterinegrowth restriction in these CIS Nevertheless it must be keptin mind that the inherent chromosome instability found inthese syndromes may also be affecting normal growth in thepatients [27 43 57 60 71]
Being small for gestational age has been associatedwith a higher risk of noncommunicable adult diseases likeglucose homeostasis disorders dyslipidemia hypertensionand others It has been proposed that fetal reprogrammingto enhance fetal survival despite the risk for adult onsetdiseases is an outcome that does not take into account
BioMed Research International 11
Table 2 Growth features of chromosomal instability syndromes
SyndromeldquoLocirdquo At-term birth weightheight Microcephaly Adult height Adult onset diseases
Seckel SyndromeldquoATR3q23rdquo
Birth weight below minus3 SD(2055 g)
Severeminus4 SD
Postnatal growth retardation(below minus5 SD) Not reported
Fanconi anemialdquo21 FANC genesrdquo
Median weight 202 kg(15ndash26 kg) In 20ndash50
50ndash60 of patients with medianheight lt minus18 SDSWomen minus34 SDSMen minus44 SDS
CancerDiabetes mellitusDyslipidemia
Altered bone mineral densityNijmegen BreakageSyndromeldquoNBN8q21rdquo
Mean weightheight girls27 kg514 cm
Mean weightheight boys28 kg523 cm
100 Mean height for women minus18 SDSMean height for men minus23 Cancer
Bloom SyndromeldquoBLM15q261rdquo
Mean weight 189 kg plusmn 035 kg forboys
Mean weight 187 kg plusmn 035 kg forgirls
Mean height 434 cm plusmn 44 cm forboys
Mean height 438 cm plusmn 28 cm forgirls
Mildmicrocephaly
Mean height 1455 cm plusmn 76 cmmales
Mean height 1415 cm plusmn 61 cm forfemales
CancerDiabetes mellitus
See [27 33 40 43 50 57 69]
45 53
43245
Height (cm)
Weight (kg)
Percentile 3 Percentile 97Percentile 50495
33
Normalindividual
Mean 2055
SeckelSyndrome
2615Median 202
FanconiAnemia
Mean 51
Mean 275
Nijmegen BreakageSyndrome
38 49
24513
Mean 436
Mean 188
BloomSyndrome
Figure 9 Anthropometric features at birth of chromosome instability syndromes with perinatal growth retardation Comparison of theavailable growth data from SS FA NBS and BS syndrome against birth data from the WHOrsquos growth standards for infants Although meanheight and weight values of NBS patients are found to be within normal percentiles according to WHO standards there are several authorswho refer to prenatal growth restriction [55 63 65 79]
the reason for the prenatal growth restraint [50 72 74] Itmust be kept in mind that noncommunicable diseases aremultifactorial entities in which genetic and environmentalfactors converge and their cause cannot be attributed to asingle explanation However when growth restriction is akey feature in syndromes with chromosome instability the
possibility that cell hypoplasia due to DNA repair malfunc-tion is contributing to the growth restriction phenotypemustbe contemplated Moreover since none of these adult onsetdiseases is reported as an inherent element of the SS and NBSphenotypes the direct connection between low birth weightand adult noncommunicable diseases is less of a straight
12 BioMed Research International
shot Furthermore there are other Mendelian syndromeswith mutations in DNA repair genes that characteristicallyshow adult noncommunicable diseases but do not haveIUGR such is the case for Werner syndrome a progeroiddisease caused by biallelic mutations in another RecQ heli-case (RecQ4) that clinically presents with postnatal shortstature and a prevalence of type 2 diabetes mellitus of 70[50 70 74]
Natural history of FA NBS and BS documented throughthe existing patient registries has allowed the identificationof noncommunicable diseases to be a part of the clinicalspectrum of these syndromes (Table 2) Meanwhile from theinformation available through SS case reports no adult onsetdisease has been found to be part of this phenotype To thebest of our knowledge the direct investigation of nonevidentendocrinologic alterations like glucose homeostasis or dys-lipidemia has not been directlymade in SS patients For a raredisease like SS such a study can only be done if a fairly largegroup of patients like the one found in registries is availableIf such a study was to be performed hidden features in SSpatients could be unraveled
Oxidative stress sensibility is a cellular feature sharedby all the SIC syndromes with IUGR that could contributeto the explanation of the premature development of non-communicable adult diseases in these patients Reports haveshown that BS and NBS cells have endogenous reactiveoxygen species (ROS) overproduction and an impairedmitochondrial homeostasis [75] it is also well known thatFA cells show increased levels of oxidative damage [3876] and there is evidence that oxidative stress can activateATR-mediated checkpoint signaling [77] Since this kind ofdamage has soundly been related to age-associated diseasesthat result from tissue degeneration exacerbated oxidativedamage found in these syndromes could result in cellu-lar aging that manifests as overall premature aging withparticular symptoms like glucose homeostasis alterations[76 77]
Fetal growth restriction is a multifactorial conditionwhere wide arrays of factors converge Fetal aspects inparticular those affecting the genetic constitution of thefetus have been recognized to play an important role Ithas been demonstrated that chromosomal abnormalities andmonogenic syndromes caused by mutations in genes thatparticipate in growth or metabolic pathways directly affectfetal growth [78] Even though they are rare entities CISappear as another group of monogenic pathologies thatbroaden the list of genetic fetal factors of fetal growthrestriction
Consent
The necessary consent for the publication of the photographswas obtained
Conflicts of Interest
The authors declare that there are no conflicts of interestregarding the publication of this paper
Authorsrsquo Contributions
The three authors contributed equally andwrote the first draftof the paper The final version was approved by everyone
Acknowledgments
This paper is supported by SEP-CONACYT Project 243102Benilde Garcıa-de Teresa received the 574025 scholarshipfrom CONACYT The paper is also supported by PAPIIT-UNAM Project IA202615 and Fondos Federales INP Project41-2014
References
[1] K W J Derks J H J Hoeijmakers and J Pothof ldquoThe DNAdamage response The omics era and its impactrdquo DNA Repairvol 19 pp 214ndash220 2014
[2] S P Jackson and J Bartek ldquoThe DNA-damage response inhuman biology and diseaserdquoNature vol 461 no 7267 pp 1071ndash1078 2009
[3] J H J Hoeijmakers ldquoDNA damage aging and cancerrdquo TheNew England Journal of Medicine vol 361 no 15 pp 1475ndash14852009
[4] G Spivak ldquoNucleotide excision repair in humansrdquoDNARepairvol 36 pp 13ndash18 2015
[5] J Vijg XDong BMilholland andL Zhang ldquoGenome instabil-ity a conserved mechanism of ageingrdquo Essays in Biochemistryvol 61 no 3 pp 305ndash315 2017
[6] J I Garaycoechea and K J Patel ldquoWhy does the bone marrowfail in Fanconi anemiardquo Blood vol 123 no 1 pp 26ndash34 2014
[7] R Ceccaldi B Rondinelli andAD DrsquoAndrea ldquoRepair PathwayChoices andConsequences at theDouble-Strand BreakrdquoTrendsin Cell Biology vol 26 no 1 pp 52ndash64 2016
[8] R Biehs M Steinlage O Barton et al ldquoDNA Double-StrandBreak Resection Occurs during Non-homologous End Joiningin G1 but Is Distinct from Resection during HomologousRecombinationrdquo Molecular Cell vol 65 no 4 pp 671ndash684e52017
[9] A Ciccia and S J Elledge ldquoTheDNAdamage response makingit safe to play with knivesrdquoMolecular Cell vol 40 no 2 pp 179ndash204 2010
[10] L H Pearl A C Schierz S E Ward B Al-Lazikani and F MG Pearl ldquoTherapeutic opportunities within the DNA damageresponserdquo Nature Reviews Cancer vol 15 no 3 pp 166ndash1802015
[11] S-F Yang C-W Chang R-J Wei Y-L Shiue S-N Wang andY-T Yeh ldquoInvolvement of DNA damage response pathways inhepatocellular carcinomardquo BioMed Research International vol2014 Article ID 153867 2014
[12] M He W Zhou C Li and M Guo ldquoMicroRNAs DNAdamage response and cancer treatmentrdquo International Journalof Molecular Sciences vol 17 no 12 article no 2087 2016
[13] K A Cimprich and D Cortez ldquoATR an essential regulator ofgenome integrityrdquo Nature Reviews Molecular Cell Biology vol9 no 8 pp 616ndash627 2008
[14] B M Sirbu and D Cortez ldquoDNA damage response three levelsof DNA repair regulationrdquo Cold Spring Harbor Perspectives inBiology vol 5 article a012724 no 8 2013
BioMed Research International 13
[15] C Beck I Robert B Reina-San-Martin V Schreiber andF Dantzer ldquoPoly(ADP-ribose) polymerases in double-strandbreak repair focus on PARP1 PARP2 and PARP3rdquo Experimen-tal Cell Research vol 329 no 1 pp 18ndash25 2014
[16] D W Meek ldquoTumour suppression by p53 a role for the DNAdamage responserdquo Nature Reviews Cancer vol 9 no 10 pp714ndash723 2009
[17] A Rodrıguez L Torres U Juarez et al ldquoFanconi anemiacells with unrepaired DNA damage activate components of thecheckpoint recovery processrdquo Theoretical Biology and MedicalModelling vol 12 no 1 article 11 2015
[18] H Wang X Zhang L Teng and R J Legerski ldquoDNA damagecheckpoint recovery and cancer developmentrdquo ExperimentalCell Research vol 334 no 2 pp 350ndash358 2015
[19] P A Jeggo L H Pearl and A M Carr ldquoDNA repair genomestability and cancer A historical perspectiverdquo Nature ReviewsCancer vol 16 no 1 pp 35ndash42 2016
[20] F S Alkuraya ldquoPrimordial dwarfism An updaterdquo CurrentOpinion in Endocrinology Diabetes and Obesity vol 22 no 1pp 55ndash64 2015
[21] P Fortini C Ferretti and E Dogliotti ldquoThe response to DNAdamage during differentiation pathways and consequencesrdquoMutation ResearchmdashFundamental and Molecular Mechanismsof Mutagenesis vol 743-744 pp 160ndash168 2013
[22] B R Adams S E Golding R R Rao and K Valerie ldquoDynamicdependence on ATR and ATM for double-Strand break repairin human embryonic stem cells and neural descendantsrdquo PLoSONE vol 5 article e10001 no 4 2010
[23] A Klingseisen and A P Jackson ldquoMechanisms and pathways ofgrowth failure in primordial dwarfismrdquo Genes amp Developmentvol 25 no 19 pp 2011ndash2024 2011
[24] H Mokrani-Benhelli L Gaillard P Biasutto et al ldquoPrimaryMicrocephaly Impaired DNA Replication and Genomic Insta-bility Caused by Compound Heterozygous ATR MutationsrdquoHuman Mutation vol 34 no 2 pp 374ndash384 2013
[25] M OrsquoDriscoll A R Gennery J Seidel P Concannon and PA Jeggo ldquoAn overview of three new disorders associated withgenetic instability LIG4 syndrome RS-SCID and ATR-Seckelsyndromerdquo DNA Repair vol 3 no 8-9 pp 1227ndash1235 2004
[26] P Khetarpal S Das I Panigrahi and A Munshi ldquoPrimordialdwarfism overview of clinical and genetic aspectsrdquo MolecularGenetics and Genomics vol 291 no 1 pp 1ndash15 2016
[27] TOgi SWalker T Stiff et al ldquoIdentification of the First ATRIP-Deficient Patient and Novel Mutations in ATRDefine a ClinicalSpectrum for ATR-ATRIP Seckel Syndromerdquo PLoS Geneticsvol 8 no 11 Article ID e1002945 2012
[28] A Verloes S Drunat and P Gressens Primary autosomalrecessive microcephalies and Seckel syndrome spectrum disor-ders 2013
[29] A D Brown B W Sager A Gorthi S S Tonapi E J Brownand A J R Bishop ldquoATR suppresses endogenous DNA damageand allows completion of homologous recombination repairrdquoPLoS ONE vol 9 article e91222 no 3 2014
[30] E J Brown and D Baltimore ldquoEssential and dispensable rolesof ATR in cell cycle arrest and genome maintenancerdquo Genes ampDevelopment vol 17 no 5 pp 615ndash628 2003
[31] B Fitzgerald M OrsquoDriscoll K Chong S Keating and PShannon ldquoNeuropathology of fetal stage Seckel syndromeA case report providing a morphological correlate for theemerging molecular mechanismsrdquo Brain amp Development vol34 no 3 pp 238ndash243 2012
[32] L I Mullee and C G Morrison ldquoCentrosomes in the DNAdamage responsemdashthe hub outside the centrerdquo ChromosomeResearch vol 24 no 1 pp 35ndash51 2016
[33] K M Takikawa A Kikuchi A Yokoyama et al ldquoPerinatalfindings of Seckel syndrome A case report of a fetus showingprimordial dwarfism and severe microcephalyrdquo Fetal Diagnosisand Therapy vol 24 no 4 pp 405ndash408 2009
[34] Y Ruzankina C Pinzon-Guzman A Asare et al ldquoDeletion ofthe Developmentally Essential Gene ATR in Adult Mice Leadsto Age-Related Phenotypes and Stem Cell Lossrdquo Cell Stem Cellvol 1 no 1 pp 113ndash126 2007
[35] N E Mamrak A Shimamura and N G Howlett ldquoRecentdiscoveries in the molecular pathogenesis of the inherited bonemarrow failure syndrome Fanconi anemiardquo Blood Reviews vol31 no 3 pp 93ndash99 2017
[36] B P Alter ldquoDiagnosis Genetics and Management of InheritedBone Marrow Failure Syndromesrdquo International Journal ofHematology vol 2007 no 1 pp 29ndash39 2007
[37] L B Pontel I V Rosado G Burgos-Barragan et al ldquoEndoge-nous Formaldehyde Is a Hematopoietic Stem Cell Genotoxinand Metabolic Carcinogenrdquo Molecular Cell vol 60 no 1 pp177ndash188 2015
[38] G Pagano P Degan M DrsquoIschia et al ldquoOxidative stress asa multiple effector in Fanconi anaemia clinical phenotyperdquoEuropean Journal of Haematology vol 75 no 2 pp 93ndash1002005
[39] P FGiampietro P CVerlander J GDavis andADAuerbachldquoDiagnosis of Fanconi anemia in patients without congenitalmalformations An International Fanconi Anemia Registrystudyrdquo American Journal of Medical Genetics vol 68 no 1 pp58ndash61 1997
[40] P F Giampietro B Adler-Brecher P C Verlander S GPavlakis J G Davis and A D Auerbach ldquoThe need for moreaccurate and timely diagnosis in Fanconi anemia A report fromthe International Fanconi Anemia Registryrdquo Pediatrics vol 91no 6 pp 1116ndash1120 1993
[41] M P Wajnrajch J M Gertner Z Huma et al ldquoEvaluationof growth and hormonal status in patients referred to theinternational fanconi anemia registryrdquo Pediatrics vol 107 no4 I pp 744ndash754 2001
[42] N Giri D L Batista B P Alter and C A Stratakis ldquoEndocrineabnormalities in patients with fanconi anemiardquo The Journal ofClinical Endocrinology amp Metabolism vol 92 no 7 pp 2624ndash2631 2007
[43] S R Rose K C Myers M M Rutter et al ldquoEndocrine phe-notype of children and adults with Fanconi anemiardquo PediatricBlood amp Cancer vol 59 no 4 pp 690ndash696 2012
[44] A D Auerbach B Adler and R S K Chaganti ldquoPrenatal andpostnatal diagnosis and carrier detection of Fanconi anemia bya cytogeneticmethodrdquoPediatrics vol 67 no 1 pp 128ndash135 1981
[45] A D Auerbach M Sagi and B Adler ldquoFanconi anemiaPrenatal diagnosis in 30 fetuses at riskrdquo Pediatrics vol 76 no5 pp 794ndash800 1985
[46] L Faivre M F Portnoı G Pals et al ldquoShould chromosomebreakage studies be performed in patients with VACTERLassociationrdquo American Journal of Medical Genetics vol 137 no1 pp 55ndash58 2005
[47] B P Alter P S Rosenberg and L C Brody ldquoClinicaland molecular features associated with biallelic mutations inFANCD1BRCA2rdquo Journal ofMedical Genetics vol 44 no 1 pp1ndash9 2007
14 BioMed Research International
[48] K Myers S M Davies R E Harris et al ldquoThe clinicalphenotype of children with Fanconi anemia caused by biallelicFANCD1BRCA2mutationsrdquo Pediatric Blood amp Cancer vol 58no 3 pp 462ndash465 2012
[49] B G Yoon H N Kim U J Han et al ldquoLong-term follow-up of Fanconi anemia Clinical manifestation and treatmentoutcomerdquo Korean Journal of Pediatrics vol 57 no 3 pp 125ndash134 2014
[50] J G Hall ldquoReview and hypothesis Syndromes with severeintrauterine growth restriction and very short stature - Are theyrelated to the epigeneticmechanism(s) of fetal survival involvedin the developmental origins of adult health and diseaserdquoAmerican Journal of Medical Genetics Part A vol 152 no 2 pp512ndash527 2010
[51] A Petryk R K Shankar N Giri et al ldquoEndocrine disordersin Fanconi anemia Recommendations for screening and treat-mentrdquoThe Journal of Clinical Endocrinology ampMetabolism vol100 no 3 pp 803ndash811 2015
[52] S R RoseMM Rutter RMueller et al ldquoBonemineral densityis normal in children with Fanconi anemiardquo Pediatric Blood ampCancer vol 57 no 6 pp 1034ndash1038 2011
[53] A Petryk L E Polgreen J L Barnum et al ldquoBone mineraldensity in childrenwith fanconi anemia after hematopoietic celltransplantationrdquo Biology of Blood and Marrow Transplantationvol 21 no 5 pp 894ndash899 2015
[54] R Purkait A Mukherji S Datta and R Bhadra ldquoRenal arterystenosis An unusual etiology of hypertensive encephalopathyin a childwith fanconi anemiardquo Saudi Journal of KidneyDiseasesand Transplantation vol 26 no 4 pp 778ndash782 2015
[55] K H Chrzanowska H Gregorek B Dembowska-BaginskaM A Kalina and M Digweed ldquoNijmegen breakage syndrome(NBS)rdquoOrphanet Journal of Rare Diseases vol 7 article 13 2012
[56] L C Riches A M Lynch and N J Gooderham ldquoEarly eventsin the mammalian response to DNA double-strand breaksrdquoMutagenesis vol 23 no 5 pp 331ndash339 2008
[57] K Chrzanowska M Kalina H Rysiewski et al ldquoGrowthpattern in patients withNijmegen breakage syndrome evidencefroma longitudinal studyrdquoHormoneResearch in Paediatrics vol74 article S38 2010
[58] Group TINBSS ldquoNijmegen breakage syndromerdquo Archives ofDisease in Childhood vol 82 pp 400ndash406 2000
[59] M Digweed and K Sperling ldquoNijmegen breakage syndromeClinical manifestation of defective response to DNA double-strand breaksrdquo DNA Repair vol 3 no 8-9 pp 1207ndash1217 2004
[60] E Seemanova ldquoAn increased risk for malignant neoplasmsin heterozygotes for a syndrome of microcephaly normalintelligence growth retardation remarkable facies immun-odeficiency and chromosomal instabilityrdquo Mutation ResearchReviews in Genetic Toxicology vol 238 no 3 pp 321ndash324 1990
[61] K H Chrzanowska M Szarras-Czapnik M Gajdulewicz et alldquoHigh prevalence of primary ovarian insufficiency in girls andyoung women with Nijmegen breakage syndrome Evidencefrom a longitudinal studyrdquoThe Journal of Clinical Endocrinologyamp Metabolism vol 95 no 7 pp 3133ndash3140 2010
[62] C M R Weemaes T W J Hustinx J M J C Scheres P J JV Munster J A J M Bakkeren and R D F M Taalman ldquoAnew chromosomal instability disorder The nijmegen breakagesyndromerdquo Acta Paediatrica Scandinavica vol 70 no 4 pp557ndash564 1981
[63] A J Green J R W Yates A M R Taylor et al ldquoSevere micro-cephaly with normal intellectual development The Nijmegen
breakage syndromerdquo Archives of Disease in Childhood vol 73no 5 pp 431ndash434 1995
[64] D Gupta and A Nagarkar ldquoSpeech impairment in Nijmegenbreakage syndrome A rare anomalyrdquo International Journal ofPediatric Otorhinolaryngology vol 73 no 6 pp 873ndash875 2009
[65] P Muschke H Gola R Varon et al ldquoRetrospective diagnosisand subsequent prenatal diagnosis of Nijmegen breakage syn-dromerdquo Prenatal Diagnosis vol 24 no 2 pp 111ndash113 2004
[66] S Pasic M Cupic T Jovanovic S Djukic M Kavaric andI Lazarevic ldquoNijmegen breakage syndrome and chronic pol-yarthritisrdquo Italian Journal of Pediatrics vol 39 no 1 article no59 2013
[67] J P Patel J M Puck R Srinivasan et al ldquoNijmegen BreakageSyndrome Detected by Newborn Screening for T Cell ReceptorExcision Circles (TRECs)rdquo Journal of Clinical Immunology vol35 no 2 pp 227ndash233 2015
[68] I Demuth and M Digweed ldquoThe clinical manifestation of adefective response to DNA double-strand breaks as exemplifiedby Nijmegen breakage syndromerdquoOncogene vol 26 no 56 pp7792ndash7798 2007
[69] H Arora A H Chacon S Choudhary et al ldquoBloom syn-dromerdquo International Journal of Dermatology vol 53 no 7 pp798ndash802 2014
[70] C de Renty and N A Ellis ldquoBloomrsquos syndrome Why not pre-mature aging A comparison of the BLM andWRN helicasesrdquoAgeing Research Reviews vol 33 pp 36ndash51 2017
[71] C Keller K R Keller S B Shew and S E Plon ldquoGrowthdeficiency and malnutrition in Bloom syndromerdquo Journal ofPediatrics vol 134 no 4 pp 472ndash479 1999
[72] A Diaz M G Vogiatzi M M Sanz and J German ldquoEval-uation of short stature carbohydrate metabolism and otherendocrinopathies in Bloomrsquos syndromerdquo Hormone Researchvol 66 no 3 pp 111ndash117 2006
[73] C Ling J Huang Z Yan et al ldquoBloom syndrome complexpromotes FANCM recruitment to stalled replication forksand facilitates both repair and traverse of DNA interstrandcrosslinksrdquo Cell Discovery vol 2 article 16047 2016
[74] J S Renes R H Willemsen A Wagner M J J Finken and AC SHokken-Koelega ldquoBloom syndrome in short children bornsmall for gestational age A challenging diagnosisrdquoThe Journalof Clinical EndocrinologyampMetabolism vol 98 no 10 pp 3932ndash3938 2013
[75] M Maciejczyk B Mikoluc B Pietrucha et al ldquoOxidativestress mitochondrial abnormalities and antioxidant defense inAtaxia-telangiectasia Bloom syndrome andNijmegen breakagesyndromerdquo Redox Biology vol 11 pp 375ndash383 2017
[76] R M Brosh M Bellani Y Liu and M M Seidman ldquoFanconiAnemia A DNA repair disorder characterized by accelerateddecline of the hematopoietic stem cell compartment and otherfeatures of agingrdquo Ageing Research Reviews vol 33 pp 67ndash752017
[77] S Yan M Sorrell and Z Berman ldquoFunctional interplay be-tween ATMATR-mediated DNA damage response and DNArepair pathways in oxidative stressrdquo Cellular and Molecular LifeSciences vol 71 no 20 pp 3951ndash3967 2014
[78] L M M Nardozza A C R Caetano A C P Zamarian etal ldquoFetal growth restriction current knowledgerdquo Archives ofGynecology and Obstetrics vol 295 no 5 pp 1061ndash1077 2017
[79] M Tomas Vila J P Verdu M R Piera and C O AlonsoldquoNijmegen breakage syndrome phenotype a disorder to con-sider in the diagnosis ofmicrocephalyrdquoAnales De Pediatria vol74 pp 58ndash60 2011
Submit your manuscripts athttpswwwhindawicom
Stem CellsInternational
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
MEDIATORSINFLAMMATION
of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Behavioural Neurology
EndocrinologyInternational Journal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Disease Markers
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
BioMed Research International
OncologyJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Oxidative Medicine and Cellular Longevity
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
PPAR Research
The Scientific World JournalHindawi Publishing Corporation httpwwwhindawicom Volume 2014
Immunology ResearchHindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Journal of
ObesityJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Computational and Mathematical Methods in Medicine
OphthalmologyJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Diabetes ResearchJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Research and TreatmentAIDS
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Gastroenterology Research and Practice
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Parkinsonrsquos Disease
Evidence-Based Complementary and Alternative Medicine
Volume 2014Hindawi Publishing Corporationhttpwwwhindawicom

4 BioMed Research International
Table 1 Chromosomal instability syndromes with intrauterine growth deficiency
Syndrome Genes Function in DDR Repair pathway Cytogenetic alteration
Fanconi anemia 21 FANC genes
ICL detection andprocessing generation ofadducts and DSBs (sensorsmediators and effectors)
Homologous recombination Chromatid and chromosomal breaksRadial figures
Seckel Syndrome 1 ATRSSBs detection and signaltransduction(transducer)
Homologous recombinationNonhomologous recombination
Chromatid and chromosomal breaksandRearrangements
Nijmegen BreakageSyndrome NBN
DSBs detection andsignaling (sensor andmediator)
Homologous recombinationNonhomologous recombination
Chromatid and chromosomal breaksAneuploidiesRearrangements affectingchromosomes 7 and 14
Bloom Syndrome BLMHelicase process SSBs andHolliday Junctions(effector)
Homologous recombination QuadriradialsIncrease in sister chromatid exchange
The PIKK kinases (Phosphatidyl Inositol 3-Kinase-relatedKinases) family is the most important of this group it isintegrated by ataxia telangiectasia and Rad3-related (ATR)Ataxia telangiectasia-mutated (ATM) and DNA dependentprotein kinase (DNAPKcs) ATR is activated during the Sphase of the cell cycle in the presence of DNA damagesuch as base adducts crosslinks single-strand breaks (SSBs)replication stress andDSBs that originate during the S phasewhile ATM and DNAPKcs are activated by DSBs at anypoint of the cell cycle [13 14] The DDR kinases activatesignaling cascades through posttranslationalmodifications ofvarious proteins including phosphorylation ubiquitylationand PARylation which play a central role in regulation ofthe DDR [15] Specifically ATR and ATM can autoactivate ortransactivate each other through phosphorylation and thenphosphorylate the histone variant H2AX (120574H2AX) that actsas a platform to recruit DDR factors and prepare the cell torestore DNA integrity ATR and ATMrsquos main downstreamphosphorylation targets are proteins Chk1 and Chk2 andthe important effector p53 their activation allows regulating(a) the chromatin structure surrounding the lesion (b)checkpoints that stop the cell cycle (c) DNA repair proteins(d) proteins that induce senescence and (e) proteins that leadto cell death (Figure 2) [10 16]
Finally if DNA lesions are repaired the checkpoint that isresponsible for stopping the cell cycle is turned off and the cellcycle is allowed to restart through a process called checkpointrecovery This process is only turned on when the signalingfor theDNA lesions is silenced and the surviving cell recoversits normal homeostasis and growth When DNA damagecannot be properly repaired the cellrsquos destiny should beeither senescence or death Otherwise cellsmight dividewithunrepaired DNA damage through an erroneous activation ofthe checkpoint recovery process that allows cell survival withgenomic instability to promote cell dysfunction and cancer[17]
4 DNA Damage Response and Disease
Unrepaired or misrepaired lesions in DNAmay immediatelyimpair replication and transcription affecting the whole cell
function In an irreparable damage situation the amountand type of lesions as well as the cell cycle phase in whichthe cell is will influence the DDR response in order tofavor immediate cell death or the conversion of DNA lesionsinto durable mutations or stable chromosomal abnormalities[3]
Cell survival despite genomic damage can directly affectcell growth this can be evidenced by two opposite outcomesOn the one hand there can be an overgrowth effect sincemutations in critical genes such as oncogenes or tumorsuppressor genes can alter cell function and increase thelikelihood of cancer development [3 18 19] On the otherhand there can be cell hypoplasia or cell loss this happenswhen irreparable damage leads to either cell death or cellsenescence a cancer-protecting condition in which cellsare alive but unable to proliferate limiting the growth ofthe tissues and conducting to aging (Figure 2) This isevidenced by the phenotype of patients affected by diseasesthat alter the DDR and DNA repair in which growthalteration and increased cancer susceptibility are importantfeatures
5 Chromosome Instability Syndromes
Mutations in at least 114 genes involved in the DDR leadto disease some of the mutations are somatic resulting invarious types of spontaneous cancer and others are geneticdiseases with constitutionalmutations that lead to syndromesthat may or may not be related to the development ofcancer [10] Among the genetic diseases with mutations inDDR genes the chromosomal instability syndromes (CIS)are a group of rare Mendelian diseases characterized byincreased chromosome breakage resulting from unrepairedor misrepaired DNA strands breaks Other than chromoso-mal instability they also have clinical overlapping featureslike cancer proneness premature aging and growth abnor-malities even though each CIS has a particular phenotypethat distinguishes it from the others Only a subgroup of thesepatients has prenatal growth alterations this review focuseson those syndromes (Table 1)
BioMed Research International 5
6 DDR Alteration and Growth Failure
Historically disruption of the DDR has been associatedwith cell growth abnormalities in a unilateral way alwayspointing towards the increased cell number in the form ofderegulated cell proliferation in cancer [19] But there islittle information on how DDR alterations can also lead toderegulation of growth in the opposite direction resultingin lack of growth due to cell death and low cell repro-duction One of the first observations to partner growthdeficiency with an altered DDR was the finding that someSeckel syndrome patients (SS) a rare phenotype consistingof primordial dwarfism and microcephaly had mutationsin the ATR gene which encodes the ATR kinase a DDRtransducer Further analysis of SS patients revealed locusheterogeneity for this phenotype mutations in other genesrelated to DDR or DNA repair also led to this clinical pictureThis observation has reinforced the association betweenDDRfailure and severe intrauterine growth retardation Moreovergenes that participate in centrosomal biology are also relatedto the uncommon phenotype of microcephalic primordialdwarfism suggesting that centrosomes have a central rolefor the adequate differentiation of early neuroprogenitorsIt has then been proposed that failure in cell proliferationsecondary to abnormal mitosis is the cause of primordialdwarfism since the multipolar spindles result in the acti-vation of checkpoints reducing proliferation and activatingapoptosis [20]
For the phenotype of growth restriction to be evidentprenatally the mechanisms regulating growth must be com-promised from the beginning of the development in embry-onic stem cells (ESCs) which are pluripotent cells derivedfrom the three primary germ layers ectoderm endodermandmesoderm and that have the capacity to differentiate intomore than 200 cell typesThese cells have been proven to havean extremely efficient DDR and proficient DNA repair mech-anisms that allow for a rigorousmaintenance of their genomeintegrity otherwise unrepaired DNA damage in ESCs wouldbe amplified affecting normal human development
ESCs have an extremely active proliferation rate theircell cycle has a characteristically reduced G1 phase andrepair mechanisms are heightened When comparing ESCsto fibroblasts it stands out that MMR is enhanced BERand NER repair pathways are highly competent and therepair of DSBs is preferentially made through the reliableHR pathway [21] Moreover when HR is not available andDSBs accumulate apoptosis is the preferred route to removehighly damaged cells It is interesting that DSB repair inESCs requires signaling through ATR instead of ATM ESCshave a special mechanism to deal with DNA damaged cellswhen inefficient DNA repair or DDR affects the induction ofapoptosis or autophagy [22] This mechanism leads to ESCdifferentiation that is driven by damage-induced expressionof the p53 transcription factor damaged differentiated cellsare efficient in cell cycle arrest and apoptosis This strategyresults in the maintenance of genetic stability in a decreasednumber of ESCs and a portion of differentiated cells thatbecome senescent both resulting in growth deficiency[21]
Growth deficiency is at the center of many diseasesincluding extremely low body size In mammals overall sizeis determined by the number of cells body mass is then thesum of all the cells that have proliferated minus those thathave died A fetus that is growing harmonically has accuratebalance between these two processes failure of either one ofthese results in dramatic effects when they occur in the ESCpopulation a decrease in cell proliferation rate or an increasein apoptosis leads to intrauterine growth retardation (IUGR)[23]
7 Chromosome Instability Syndromes withIntrauterine Growth Retardation
71 Seckel Syndrome Seckel syndrome (SS) is an autosomalrecessive disorder clinically and genetically heterogeneousSo far at least six genes have been associated with the Seckelphenotype most of these genes participate in ATR-mediatedDDR and in centrosomal function Two clinical subgroupscan be identified on the one hand patients with mutationsin ATR NIN and ATRIP genes only present the Seckelphenotype while on the other hand those with mutationsin CENPJ CEP152 or RBBP8 show allelic heterogeneity andbesides the SS phenotype can also manifest as a spectrumof disorders known as Primary Autosomal Recessive Micro-cephalies [24ndash28] SS patients who bear mutations in ATRshow a classical Seckel phenotype the SS data presented herewill be limited to such patients
ATR is localized in 3q23 it is one of the serine threoninekinases that belong to the PIKK family They have a funda-mental role in the DDR since they participate as transducersin the signaling of DNA lesions especially when the DDRresponds to stalled replication forks and bulky lesions inDNA[24 25] ATR responds preferentially to ssDNA during the Sphase It also plays a crucial role in preventing DNA breakscaused by fork pausing when DNA replication machineryfinds DNA lesions or complex DNA structure and sequences[24] ATR stability depends on binding of ssDNA to theATR cofactor ATRIP (ATR interacting protein) and thesingle-stranded binding protein (RPA) ATRIP is required forATR localization to the ssDNA regions and hence for ATRactivation [25 27] Major functions of ATR are activation ofcell cycle check point arrest stabilization of stalled replicationforks and promotion of replication fork restart which isachieved through its ability to phosphorylate a wide range ofsubstrates that include p53 and H2AX [27 29]
Cellular phenotype of ATR deficient cells is characterizedby decreased phosphorylation of ATR-dependent substratesas well as an impaired G2M checkpoint arrest These cellsare characterized by markers that signal unrepaired DSBslike the presence of 120574H2AX chromosomal breakage [2629 30] and micronuclei formation This cellular phenotypemay be originated by a failure to recover from replicationstalling which generates DSBs that are normally repairedby HR when they occur during SG2 In SS cells theabsence of ATR is critical during embryonic developmentthis deficiency leads to genomic instability cell senescenceand cell death that leads to fetal growth and accelerated aging[31]
6 BioMed Research International
Figure 3 Seckel syndrome patient Note the severe microcephalyand the ldquobird-likerdquo appearance facies with micrognathia and reced-ing forehead The patient is severely disabled with no independentmarch
Moreover it appears that ATR and the other SS genes notonly participate in the DDR but also take part in the controlof centrosome maturation This engagement in centrosomebiology is also true for other DDR proteins like BRCA2biallelic mutations in its gene are responsible for a subgroupof Fanconi anemia patients [32]Theunifying feature betweenall Seckel patients irrespective of the molecular defect isthat their cells have an altered cell cycle progression thatis particularly evident during high rate cell division whenthere is hypersensitivity to replicative stress and centrosomaldysfunction This is especially important in cells with highdivision rates like the ones found in developmental stageswhere rapid replication is key [24 27]
SS is characterized by IUGR dwarfism microcephaly(below minus4 SD) mental retardation and some other anomalieslike luxation of the head of the radius scoliosis bone agedelay and seizures (Figure 3) The distinctive facial featuresinclude a prominent nose with micrognathia and a recedingforehead resulting in a ldquobird-like appearancerdquo [26 31 33]Since this syndrome has important clinical heterogeneityother anomalies have been reported including mandibularhypoplasia sternal abnormalities clinodactyly and low setears with hypoplastic lobules Although rare other reportedfeatures are moyamoya syndrome osteosarcoma and pol-yarteritis nodosa [26] Cerebral malformations like neuronalmigration abnormalities have been described but are notalways present [33] No glucose metabolism abnormalitieshave been reported
Dwarfism can be related to a reduction in the totalnumber of cells generated during development leading tohypoplastic tissue and reduced organism size [23] On theother handmicrocephalymay be related to an impairedDNAdamage response signal that could alter the cellular thresholdfor cell death resulting from DNA damage increasing thelevels of apoptosis during development developing neuronsare rapidly proliferating and potentially generate high levelsof oxidative damage which may lead to a higher level oflesions being faced at replication forks [23 25] Also analtered mitosis secondary to impaired spindle formationcould delay mitotic progression and increase the proportionof nonviable cell divisions Finally the stem cells may beaffected by abnormal centrosomal function Stems cells haveasymmetric divisions in order to preserve the characteristics
Figure 4 Fanconi anemia patient This six-year-old girl is 105 cmtall her height is just below the 5th percentile and her at-term birthweight is reported to be of 1900 gr Characteristic features of FA areevident skin hyperpigmentation bilateral radial defects consistingof bilateral thenar hypoplasia and absent fold of the right thumbwhich cannot be bent
of a stem cell and the centrosomes play an important role insuch divisions [23]
There is limited clinical information regarding age-related diseases in SS there is a void of prospective follow-up data from these patients that can only be obtained byfollowing a cohort of SS patients something that is apparentlynot being done at this time Nevertheless animal modelsbring some clues over the possibility of an aging phenotypein SS patients since ATR deficient adult mice show prematureage-related phenotypes as well as increased deterioration oftissue homeostasis [29 34]
72 Fanconi Anemia DNA interstrand crosslinks are ex-tremely noxious DNA lesions that affect central cellularprocesses like transcription and replication The FABRCApathway is responsible for the appropriate processing ofthese lesions protein products from at least 21 FANC genesparticipate in this pathway [35] The malfunction of any ofthose FANC proteins leads to the clinical phenotype knownas Fanconi anemia (FA) which is characterized by shortstature congenital malformations from the VACTERL-Hspectrum bone marrow failure and an increased suscepti-bility to cancer like acute myeloid leukemia epithelial headand neck cancer [36] (Figure 4) Most of the FA families bearbiallelic mutations in FANC genes that have an autosomicrecessive inheritance pattern only families with mutations inFANCB show an X-linked recessive pattern while those inwhich FANCR is the affected gene demonstrate an autosomicdominant one [35]
The FABRCA is an S-specific pathway that has 3 basicsteps it starts with the detection of the ICL by the proteinFANCM followed by the recruitment of the FA core com-plex that is responsible for the monoubiquitination of theFANCD2I heterodimer which in turn favors the recruit-ment of effector FANC-repair proteins that restore the DNAto its original form [35]
BioMed Research International 7
(a) (b)
Figure 5 Chromosomal instability induced by 40 ngml mitomycin C (a) Lymphocytes from a healthy individual (b) lymphocytes from aFA patient Short arrows show chromosomal breaks the long arrow shows a quadriradial figure Note the exacerbated chromosome instabilityfound in the FA patient
The cellular phenotype of FA derived cells is extremelyconstant An aberrant FABRCA pathway can result inunrepaired DSBs that manifest as chromosomal breaks orabnormal repair by an error-prone repair pathway that resultsin radial figures These alterations are cytogenetic evidenceof chromosomal instability which is the hallmark of FA cellsand is exploited for clinical diagnostic purposes (Figure 5)The agents capable of inducing this chromosomal instabilityare from endogenous origin like aldehydes [37] and reactivespecies of oxygen (ROS) [38] as well as exogenous sourceslike bifunctional alkylating agents (diepoxybutane or mito-mycin C) In addition FA cells have accumulation of cells inG2 phase of the cell cycle resulting from a functional G2Mcheckpoint and a proapoptotic phenotype
In contrast with the cellular FA phenotype the clinicalpicture in FA patients is extremely variable not every patientwill have all the manifestations one-third of patients do nothave congenital malformations [39] while almost 90 willdevelop bone marrow failure [36] One of the more constantmanifestations in FApatients is growth parameters alterationAn analysis from the international Fanconi anemia registry(IFAR) data showed that over 60 of FA patients presentedshort stature (below the 5th percentile) while birth lengthandweight below the 5th percentile was respectively reportedin almost 30 and nearly half of FA patients [40]Moreover aprospective study of data from 54 IFAR participants showedthat the mean standard deviation score (SDS) for height inthese patients was significantly below normal for age and sexat minus235 plusmn 028 meanwhile mean SDS for weight was betteralthough below normal (minus126 plusmn 024) In this study perinatalgrowth data was not reported [41]
Other than the IFAR data on growth there are anothertwo studies that analyze growth parameters of FA patientsAnthropometric measurements from 45 patients with Fan-coni anemia from the National Cancer Institutersquos inher-ited bone marrow failure syndromes (IBMFS) cohort wereassessed This cohort had a mean SDS for height of minus21 plusmn
189 The height of over half of the participants (54) wascategorized as short (SDS gt 20 SD) in this subset of patientsthe mean SDS for height was minus38 plusmn 15 [42] Finally theevaluation of 120 FA patients from the FA ComprehensiveCare Clinic of Cincinnati Childrenrsquos Hospital Medical Centerrevealed that median height SDS was shorter than expectedin children and adults irrespective of gender Furthermorethis study presented birth information from 70 patients (59children and 11 adults) from the cohort 51 of the childrenand 3 adults were born small for gestational age their medianbirth weight at term was 202 kg (range 15ndash26 kg) [43] Theintrauterine growth restriction seen in FA patients has alsobeen documented in several case reports in which at-termbirth weight ranges from 1780 to 3200 gr [44ndash49] Eventhough growth abnormalities have been identified in FApatients with mutations in almost every FANC gene it hasbeen shown that patientswithmutations in certain genes havea more severe growth delay That is the case for patients withbiallelic mutations in FANCD1 [47 48] as well as those whobear mutations in FANCC for whom an SDS for height ofminus384 has been found [41]
Endocrine abnormalities have been proven to be aninherent part of the FA phenotype up to 80 of patientshave one or more endocrine abnormalities Besides growththyroid function and glucose homeostasis are frequentlyaffected [40ndash43] Considering the existing evidence for arelationship between low birth weight and an increased riskfor noncommunicable adult diseases like diabetes hyperten-sion heart disease dyslipidemia and osteoporosis [50] it isrelevant to revise these diseases in FA The FA cohorts inwhom growth was assessed were also evaluated for endocrinestatus Glucose homeostasis is affected in a large portion ofFA patients impaired glucose tolerance has been found in27ndash68 of them whereas diabetes has a prevalence of 8ndash10Dyslipidemia has been assessed in only a small portionof FA patients but it has been found in 17ndash55 of theevaluated subjects [51]There are conflicting results over bone
8 BioMed Research International
mineral density (BMD) status in FA the first time this wasevaluated 92 of the patients were found to have osteopeniaor osteoporosis [42] nevertheless a study that evaluated alarger FA cohort found that lowBMD is not a frequent finding[52] Further research on this topic has raised the questionof whether BMD deficit is intrinsic to the FA phenotype ora consequence of hematopoietic cell transplantation (HCT)an interrogation that is still awaiting to be answered [53]Cardiovascular adult diseases are not relevant in the FA phe-notype heart disease in these patients is from the congenitaltype as 13of patients have cardiacmalformations [40] whilehypertension has only been reported in two patients as theresult of renal malformations [54]
Findings from the different FA cohorts show that shortstature is an inherent feature of the FA phenotype thisfeature does not respond to a single explanation the apoptosisprone FA cellular phenotype is certainly a contributing factorfor this The fact that FA patients have a constitutionallydefective pathway since conception could explain the clinicalphenotype of RCIU Short stature may also be exacerbated byaccompanying endocrinopathies The cooccurrence of manyendocrine alterations has encouraged unifying explanationssome have proposed that endocrinopathies are secondaryto increased cytokine activity found in FA cells [41] whileothers favor the view that some endocrine secretory cellsmight be damaged by high levels of reactive oxygen specieswhich are known to be elevated in FA patients [43] In linewith the developmental origin of adult health and diseasetheory it could also be possible that the increased prevalenceof glucose homeostasis alterations and dyslipidemia reportedin FA patients is a consequence of intrauterine growthrestriction of these patients Nevertheless the attemptedgenotype-phenotype correlation of the endocrine phenotypein FA patients does not seem to support that Patients withmutations in FANCA show a mild endocrine phenotype inwhich height is not severely affected and insulin resistanceis mild whereas mutations in FANCC which are relatedto shorter stature have the least insulin resistance [41]Moreover no direct relationship between birth weight andglucose tolerance was identified when it was intentionallylooked for [43] although the number of patients in whichthese observations were made is limited
73 Nijmegen Breakage Syndrome Nijmegen breakage syn-drome (NBS) is an autosomal recessive disease caused bybiallelic mutations in NBN a gene that encodes nibrin aprotein involved in DNA repair and cell cycle checkpointregulation It participates in the former by sensing double-strand breaks as part of the trimeric complexMRN alongsideMRE11 andRAD50Meanwhile for the latter it contributes tothe appropriate activation of ATM andATRwhich are centraltransductors of the DNA damage response (DDR) [55] Themalfunction of nibrin translates in a cellular phenotypemarked by chromosomal instability radiosensitivity reducedphosphorylation of ATM substrates and S and G2M cellcycle defects [56] Chromosome instability is evidenced bycytogenetic methods in 10ndash60 of cells in the form of breaksand numeric and structural aberrations translocations andinversions affecting chromosomes 7 and 14 are found in the
147
Figure 6 Translocation between chromosomes 7 and 14 is typicalin NBS patientsrsquo cells
majority of NBS patients and are considered a cytogeneticcharacteristic of this syndrome (Figure 6) [57]
The clinical impact of these alterations is a phenotypecharacterized by microcephaly a distinctive facial appear-ance consisting of receding forehead and mandible and aprominent mid face with a long nose and philtrum aswell as immunodeficiency that leads to recurrent infectionsand an increased risk for the development of neoplasiaparticularly leukemia and lymphoma According to theinternational Nijmegen breakage syndrome study groupgrowth retardation is also a hallmark of this disease [58]although there is not many details about this feature in theliterature
Most of the information on the natural history of NBSavailable today comes from patients participating in reg-istries in which fairly large cohorts of NBS patients areincluded There is a large representation of Slavic patientsin these cohorts which correlates with the high carrierfrequency of a founder mutation of NBN in this populationFrom these studies it is evident that the most severelyaffected anthropometric measure in NBS patients is headcircumference since all participants display microcephalyeven though only 75 display this feature at birth Whenit comes to growth parameters the same study states thatall patients have growth retardation which is described asproportionate and early occurring [58] although the specifictemporality is not defined A posterior report points out thatthe growth retardation seen in most NBS patients locatesthem in the 10th percentile in growth charts and that birthheight and weight are usually within normal parameters [59]Nevertheless there are other authors who report prenataland postnatal growth retardation [55 60] and a tendency forshort stature that is more evident during the first year of life[61] Also several case reports of NBS patients in which birthweight is informed demonstrate prenatal growth restriction[62ndash67] although this could represent a report bias Themore comprehensive data analysis on growth that includesperinatal information of NBS patients is the one that analyzesdata from 67 patients followed for 15 years Eighty percentof these patients were born at term the girls were found tohave a mean birth weight of 27 kg and mean birth heightof 514 cm while boys were reported to have a mean birthweight of 28 kg and mean birth height of 523 cm Moreoverall patients irrespective of gender were found to have ameanheight reduced by over 2 SDS at one year old [57] These data
BioMed Research International 9
(a) (b)
Figure 7 Sister chromatid exchange in cells from a healthy individual (a) and from a BLM patient (b)
support the fact that growth retardation in NBS is a prenatalphenomenon
Nibrin has been found to have essential functions inthe regulation of the cell cycle which translates into anabsolute need for this protein for cell proliferation [68]It would seem logical that mutations of the NBN genethat compromise the appropriate function of nibrin wouldlead to abnormal growth when thought from an organismperspective Mechanistically speaking poor cellular growthcaused by mutations in a particular gene can be thought ofas the main explanation for the growth restricted phenotypebut it has been shown that mutations in other DDR genesthat share the cellular phenotype of poor growth like ATMdo not replicate the compromised growth phenotype atthe organism level growth retardation is absent in ataxiatelangiectasia (AT)This data suggests that there are certainlyother contributing factors to the abnormal growth phenotypeseen in NBS patients [58]
74 Bloom Syndrome Bloom syndrome (BS) is an autosomalrecessive disorder caused by homozygous or compoundheterozygous mutations in the BLM gene (15q261) thatencodes the RecQL3 helicase BLM has a critical role inthe maintenance of genome stability acting at the interfacebetweenDNAreplication recombination and repair [69 70]To date over sixty different mutations including nonsenseand missense have been identified all of them result inthe inactivation of BLM and the consequent loss of itshelicase activity The BLM gene encodes a 1417 amino acidnuclear protein its expression peaks during the S and G
2M
phases of the cell cycle which is consistent with its rolein DNA replication and recombination BLM specificallyunwinds structures like forked DNA duplexes RNA-DNAheteroduplexes and R-Loops which explains its importanceduring replication fork progression and transcription besidesit is central for Holliday Junctions (HJs) dissolution forHR The dissolution of HJs by the topoisomerase III120572-BLMcomplex cannot be replaced by any other RecQ helicase inthe family [69 70] It has also been found to have a role in
the annealing activity of the ssDNA the proper sister chro-matid segregation during mitosis and telomere maintenance[70]
BLM can have both pro- and antirecombinogenic func-tions that are regulated by posttranslational modificationsincluding phosphorylation sumoylation and ubiquitination[70]
BLM also enables sister chromatid segregation by pro-cessing unresolved replication intermediates that manifest inmitosis as ultrafine DNA bridges (UFBs) and together withtopoisomerase III120572 RMI1 and RMI2 localizes to UFBs inanaphase BML deficient cells exhibit and increase frequencyof UFBs suggesting a role of BLM in the resolution ofthese structures Failure to resolve these UFBs leads to DNAbreakage as mitosis proceeds [70]
Therefore BS cells are characterized by an increasein chromosomal aberrations including chromatid gapsand breaks telomere associations and quadriradial chro-mosomes resulting from unsolved recombination betweenhomologous chromosomes BS cells exhibit increased muta-tion rates and the genomic instability includes elevatedmitotic HR and unequal sister chromatid exchange (SCEs)(Figure 7) Perhaps the most characteristic feature is the overtenfold increase in SCEs which results from crossover eventsduring HR repair of damage replication forks [50 69 70]
Clinically the more striking BS feature is IUGR averagebirth weight at term is 1850 g and birth length is 44 cmFor both boys and girls weight and length in BS are morethan two standard deviations below normal indicating thatgrowth retardation has a prenatal origin At postnatal agesheight remains below the normal range and is accompaniedby a paucity of subcutaneous fat Average adult height inmales has been found to be 148 cm (130ndash162 cm) whilein females it has been reported to be 139 cm (122ndash151 cm)[50 70 71]
BS patients have overall proportionated short staturebut the head is reported to be small and narrow relativelyto the body size it is described as mild microcephalyand is accompanied by malar hypoplasia Patients have
10 BioMed Research International
Figure 8 Bloomsyndromepatient inwhom the characteristicmalarerythema is present
been described to have a high pitched voice [50 70] Theskin appears normal at birth but in the first or secondyear of life in response to sun exposure children developan erythematous rash with a butterfly distribution in themalar area and the back of hands and feet The rash caninclude telangiectasia The severity varies between patientssome can even lose their eyelashes and develop blisteringaround the mouth The presence of cafe-au-lait spots andhypopigmented areas of skin associated with contiguoushyperpigmented areas is common (Figure 8) Intellectualabilitiesmay be limited in some patients and normal in others[50 70]
Other clinical conditions reported in BS patients are gas-troesophageal reflux and diarrhea in infants mild immuno-logical deficiency with frequent episodes of otitis mediaazoospermia or severe oligospermia in males and prema-ture cessation of menstruation in females minor anatomicdefects and increased risk for neoplasia which is the maincause of dead in BS [70] Another common medical con-dition in BS is diabetes mellitus associated with impairedglucose tolerance and insulin resistance it has been reportedin up to 16 of patients [70] According to data fromthe Bloomrsquos Syndrome Registry diabetes in these patientstends to begin early with a mean age at diagnosis of 266years It is not associated with ketosis and it does nothave the classical hereditary pattern seen in type 2 diabetes[50 72]
Short stature in BS is not due to hormonal causes sincethe size of cells in persons with BS is normal it has beenhypothesized that there are fewer of them due to either adecrease in the cell division rate an increase in apoptosis oreven a combination of both BS cells have troublemeeting thedemands of fast cell divisions encountered in tissues duringembryonic development The leading hypothesis suggeststhat problems arising during DNA synthesis require a longerS phase to overcome the challenge which translates intoslowing of the cell division rate and an increase in apoptosis[70]
8 Concluding Remarks
This review has focused on discussing phenotypes of CISin which there is a prenatal alteration of growth The foursyndromes discussed here are rare diseases whose prevalenceis difficult to calculate since appropriate identification anddiagnosis of affected individuals among the general popula-tion are not straightforward It is important to note that theavailable information on the natural history of FA NBS andBS comes from the analysis of several patients that participatein registries This strategy results in detailed informationthat permits a better analysis of the clinical phenotype ofthese rare diseases Meanwhile available data of SS is moreanecdotic which results in a nonsystematic gathering ofinformation which is thus frequently incomplete
From the available clinical data of these CIS it is evidentthat growth is not affected in the same extent for all ofthese syndromes the phenotypes that exhibit a more severelystagnated perinatal growth are BS and SS The severe growthdelay reported in these patients has been described as apathognomonic sign of these diagnoses In patients withFA perinatal growth can also be severely affected but notevery FA patient shows this manifestation Finally NBShas been described to have growth retardation of prenatalorigin of mild severity almost within the lower normal range(Figure 9) The cephalic circumference can be affected in allof these syndromes severe microcephaly is pathognomonicin SS and NBS it is described as mild for BS patients and it isfound in less than half of FA patients (Table 2)
When trying to understand why a subset of CIS showsprenatal growth retardation it could be alleged that theintrinsic chromosomal instability is responsible for it Butthis would not explain why prenatal growth retardation isnot a universal CIS feature for example ataxia telangiectasiapatients who have biallelic mutations in the ATMkinase genedo not show prenatal growth delay It strikes that a molecularcommon feature shared by the prenatal growth retardationSIC phenotypes is that they are caused by mutations ingenes that are necessary for an appropriate response to DSBsduring the S phase of the cell cycle The molecular defectin SS affects the functioning of ATR the preferred DDRtransducing kinase used by highly replicating ESCs TheFABRCA pathway which is affected in patients with FAdetects ICLs upon replication fork arrest Nibrin the proteinaffected in patients with NBS is induced during S phasefor the detection of DSBs And the BS helicase forms aFANCM-BLM complex needed to sense ICLs during S phase[73] It could then be argued that altered DNA replicationis an important factor for the development of intrauterinegrowth restriction in these CIS Nevertheless it must be keptin mind that the inherent chromosome instability found inthese syndromes may also be affecting normal growth in thepatients [27 43 57 60 71]
Being small for gestational age has been associatedwith a higher risk of noncommunicable adult diseases likeglucose homeostasis disorders dyslipidemia hypertensionand others It has been proposed that fetal reprogrammingto enhance fetal survival despite the risk for adult onsetdiseases is an outcome that does not take into account
BioMed Research International 11
Table 2 Growth features of chromosomal instability syndromes
SyndromeldquoLocirdquo At-term birth weightheight Microcephaly Adult height Adult onset diseases
Seckel SyndromeldquoATR3q23rdquo
Birth weight below minus3 SD(2055 g)
Severeminus4 SD
Postnatal growth retardation(below minus5 SD) Not reported
Fanconi anemialdquo21 FANC genesrdquo
Median weight 202 kg(15ndash26 kg) In 20ndash50
50ndash60 of patients with medianheight lt minus18 SDSWomen minus34 SDSMen minus44 SDS
CancerDiabetes mellitusDyslipidemia
Altered bone mineral densityNijmegen BreakageSyndromeldquoNBN8q21rdquo
Mean weightheight girls27 kg514 cm
Mean weightheight boys28 kg523 cm
100 Mean height for women minus18 SDSMean height for men minus23 Cancer
Bloom SyndromeldquoBLM15q261rdquo
Mean weight 189 kg plusmn 035 kg forboys
Mean weight 187 kg plusmn 035 kg forgirls
Mean height 434 cm plusmn 44 cm forboys
Mean height 438 cm plusmn 28 cm forgirls
Mildmicrocephaly
Mean height 1455 cm plusmn 76 cmmales
Mean height 1415 cm plusmn 61 cm forfemales
CancerDiabetes mellitus
See [27 33 40 43 50 57 69]
45 53
43245
Height (cm)
Weight (kg)
Percentile 3 Percentile 97Percentile 50495
33
Normalindividual
Mean 2055
SeckelSyndrome
2615Median 202
FanconiAnemia
Mean 51
Mean 275
Nijmegen BreakageSyndrome
38 49
24513
Mean 436
Mean 188
BloomSyndrome
Figure 9 Anthropometric features at birth of chromosome instability syndromes with perinatal growth retardation Comparison of theavailable growth data from SS FA NBS and BS syndrome against birth data from the WHOrsquos growth standards for infants Although meanheight and weight values of NBS patients are found to be within normal percentiles according to WHO standards there are several authorswho refer to prenatal growth restriction [55 63 65 79]
the reason for the prenatal growth restraint [50 72 74] Itmust be kept in mind that noncommunicable diseases aremultifactorial entities in which genetic and environmentalfactors converge and their cause cannot be attributed to asingle explanation However when growth restriction is akey feature in syndromes with chromosome instability the
possibility that cell hypoplasia due to DNA repair malfunc-tion is contributing to the growth restriction phenotypemustbe contemplated Moreover since none of these adult onsetdiseases is reported as an inherent element of the SS and NBSphenotypes the direct connection between low birth weightand adult noncommunicable diseases is less of a straight
12 BioMed Research International
shot Furthermore there are other Mendelian syndromeswith mutations in DNA repair genes that characteristicallyshow adult noncommunicable diseases but do not haveIUGR such is the case for Werner syndrome a progeroiddisease caused by biallelic mutations in another RecQ heli-case (RecQ4) that clinically presents with postnatal shortstature and a prevalence of type 2 diabetes mellitus of 70[50 70 74]
Natural history of FA NBS and BS documented throughthe existing patient registries has allowed the identificationof noncommunicable diseases to be a part of the clinicalspectrum of these syndromes (Table 2) Meanwhile from theinformation available through SS case reports no adult onsetdisease has been found to be part of this phenotype To thebest of our knowledge the direct investigation of nonevidentendocrinologic alterations like glucose homeostasis or dys-lipidemia has not been directlymade in SS patients For a raredisease like SS such a study can only be done if a fairly largegroup of patients like the one found in registries is availableIf such a study was to be performed hidden features in SSpatients could be unraveled
Oxidative stress sensibility is a cellular feature sharedby all the SIC syndromes with IUGR that could contributeto the explanation of the premature development of non-communicable adult diseases in these patients Reports haveshown that BS and NBS cells have endogenous reactiveoxygen species (ROS) overproduction and an impairedmitochondrial homeostasis [75] it is also well known thatFA cells show increased levels of oxidative damage [3876] and there is evidence that oxidative stress can activateATR-mediated checkpoint signaling [77] Since this kind ofdamage has soundly been related to age-associated diseasesthat result from tissue degeneration exacerbated oxidativedamage found in these syndromes could result in cellu-lar aging that manifests as overall premature aging withparticular symptoms like glucose homeostasis alterations[76 77]
Fetal growth restriction is a multifactorial conditionwhere wide arrays of factors converge Fetal aspects inparticular those affecting the genetic constitution of thefetus have been recognized to play an important role Ithas been demonstrated that chromosomal abnormalities andmonogenic syndromes caused by mutations in genes thatparticipate in growth or metabolic pathways directly affectfetal growth [78] Even though they are rare entities CISappear as another group of monogenic pathologies thatbroaden the list of genetic fetal factors of fetal growthrestriction
Consent
The necessary consent for the publication of the photographswas obtained
Conflicts of Interest
The authors declare that there are no conflicts of interestregarding the publication of this paper
Authorsrsquo Contributions
The three authors contributed equally andwrote the first draftof the paper The final version was approved by everyone
Acknowledgments
This paper is supported by SEP-CONACYT Project 243102Benilde Garcıa-de Teresa received the 574025 scholarshipfrom CONACYT The paper is also supported by PAPIIT-UNAM Project IA202615 and Fondos Federales INP Project41-2014
References
[1] K W J Derks J H J Hoeijmakers and J Pothof ldquoThe DNAdamage response The omics era and its impactrdquo DNA Repairvol 19 pp 214ndash220 2014
[2] S P Jackson and J Bartek ldquoThe DNA-damage response inhuman biology and diseaserdquoNature vol 461 no 7267 pp 1071ndash1078 2009
[3] J H J Hoeijmakers ldquoDNA damage aging and cancerrdquo TheNew England Journal of Medicine vol 361 no 15 pp 1475ndash14852009
[4] G Spivak ldquoNucleotide excision repair in humansrdquoDNARepairvol 36 pp 13ndash18 2015
[5] J Vijg XDong BMilholland andL Zhang ldquoGenome instabil-ity a conserved mechanism of ageingrdquo Essays in Biochemistryvol 61 no 3 pp 305ndash315 2017
[6] J I Garaycoechea and K J Patel ldquoWhy does the bone marrowfail in Fanconi anemiardquo Blood vol 123 no 1 pp 26ndash34 2014
[7] R Ceccaldi B Rondinelli andAD DrsquoAndrea ldquoRepair PathwayChoices andConsequences at theDouble-Strand BreakrdquoTrendsin Cell Biology vol 26 no 1 pp 52ndash64 2016
[8] R Biehs M Steinlage O Barton et al ldquoDNA Double-StrandBreak Resection Occurs during Non-homologous End Joiningin G1 but Is Distinct from Resection during HomologousRecombinationrdquo Molecular Cell vol 65 no 4 pp 671ndash684e52017
[9] A Ciccia and S J Elledge ldquoTheDNAdamage response makingit safe to play with knivesrdquoMolecular Cell vol 40 no 2 pp 179ndash204 2010
[10] L H Pearl A C Schierz S E Ward B Al-Lazikani and F MG Pearl ldquoTherapeutic opportunities within the DNA damageresponserdquo Nature Reviews Cancer vol 15 no 3 pp 166ndash1802015
[11] S-F Yang C-W Chang R-J Wei Y-L Shiue S-N Wang andY-T Yeh ldquoInvolvement of DNA damage response pathways inhepatocellular carcinomardquo BioMed Research International vol2014 Article ID 153867 2014
[12] M He W Zhou C Li and M Guo ldquoMicroRNAs DNAdamage response and cancer treatmentrdquo International Journalof Molecular Sciences vol 17 no 12 article no 2087 2016
[13] K A Cimprich and D Cortez ldquoATR an essential regulator ofgenome integrityrdquo Nature Reviews Molecular Cell Biology vol9 no 8 pp 616ndash627 2008
[14] B M Sirbu and D Cortez ldquoDNA damage response three levelsof DNA repair regulationrdquo Cold Spring Harbor Perspectives inBiology vol 5 article a012724 no 8 2013
BioMed Research International 13
[15] C Beck I Robert B Reina-San-Martin V Schreiber andF Dantzer ldquoPoly(ADP-ribose) polymerases in double-strandbreak repair focus on PARP1 PARP2 and PARP3rdquo Experimen-tal Cell Research vol 329 no 1 pp 18ndash25 2014
[16] D W Meek ldquoTumour suppression by p53 a role for the DNAdamage responserdquo Nature Reviews Cancer vol 9 no 10 pp714ndash723 2009
[17] A Rodrıguez L Torres U Juarez et al ldquoFanconi anemiacells with unrepaired DNA damage activate components of thecheckpoint recovery processrdquo Theoretical Biology and MedicalModelling vol 12 no 1 article 11 2015
[18] H Wang X Zhang L Teng and R J Legerski ldquoDNA damagecheckpoint recovery and cancer developmentrdquo ExperimentalCell Research vol 334 no 2 pp 350ndash358 2015
[19] P A Jeggo L H Pearl and A M Carr ldquoDNA repair genomestability and cancer A historical perspectiverdquo Nature ReviewsCancer vol 16 no 1 pp 35ndash42 2016
[20] F S Alkuraya ldquoPrimordial dwarfism An updaterdquo CurrentOpinion in Endocrinology Diabetes and Obesity vol 22 no 1pp 55ndash64 2015
[21] P Fortini C Ferretti and E Dogliotti ldquoThe response to DNAdamage during differentiation pathways and consequencesrdquoMutation ResearchmdashFundamental and Molecular Mechanismsof Mutagenesis vol 743-744 pp 160ndash168 2013
[22] B R Adams S E Golding R R Rao and K Valerie ldquoDynamicdependence on ATR and ATM for double-Strand break repairin human embryonic stem cells and neural descendantsrdquo PLoSONE vol 5 article e10001 no 4 2010
[23] A Klingseisen and A P Jackson ldquoMechanisms and pathways ofgrowth failure in primordial dwarfismrdquo Genes amp Developmentvol 25 no 19 pp 2011ndash2024 2011
[24] H Mokrani-Benhelli L Gaillard P Biasutto et al ldquoPrimaryMicrocephaly Impaired DNA Replication and Genomic Insta-bility Caused by Compound Heterozygous ATR MutationsrdquoHuman Mutation vol 34 no 2 pp 374ndash384 2013
[25] M OrsquoDriscoll A R Gennery J Seidel P Concannon and PA Jeggo ldquoAn overview of three new disorders associated withgenetic instability LIG4 syndrome RS-SCID and ATR-Seckelsyndromerdquo DNA Repair vol 3 no 8-9 pp 1227ndash1235 2004
[26] P Khetarpal S Das I Panigrahi and A Munshi ldquoPrimordialdwarfism overview of clinical and genetic aspectsrdquo MolecularGenetics and Genomics vol 291 no 1 pp 1ndash15 2016
[27] TOgi SWalker T Stiff et al ldquoIdentification of the First ATRIP-Deficient Patient and Novel Mutations in ATRDefine a ClinicalSpectrum for ATR-ATRIP Seckel Syndromerdquo PLoS Geneticsvol 8 no 11 Article ID e1002945 2012
[28] A Verloes S Drunat and P Gressens Primary autosomalrecessive microcephalies and Seckel syndrome spectrum disor-ders 2013
[29] A D Brown B W Sager A Gorthi S S Tonapi E J Brownand A J R Bishop ldquoATR suppresses endogenous DNA damageand allows completion of homologous recombination repairrdquoPLoS ONE vol 9 article e91222 no 3 2014
[30] E J Brown and D Baltimore ldquoEssential and dispensable rolesof ATR in cell cycle arrest and genome maintenancerdquo Genes ampDevelopment vol 17 no 5 pp 615ndash628 2003
[31] B Fitzgerald M OrsquoDriscoll K Chong S Keating and PShannon ldquoNeuropathology of fetal stage Seckel syndromeA case report providing a morphological correlate for theemerging molecular mechanismsrdquo Brain amp Development vol34 no 3 pp 238ndash243 2012
[32] L I Mullee and C G Morrison ldquoCentrosomes in the DNAdamage responsemdashthe hub outside the centrerdquo ChromosomeResearch vol 24 no 1 pp 35ndash51 2016
[33] K M Takikawa A Kikuchi A Yokoyama et al ldquoPerinatalfindings of Seckel syndrome A case report of a fetus showingprimordial dwarfism and severe microcephalyrdquo Fetal Diagnosisand Therapy vol 24 no 4 pp 405ndash408 2009
[34] Y Ruzankina C Pinzon-Guzman A Asare et al ldquoDeletion ofthe Developmentally Essential Gene ATR in Adult Mice Leadsto Age-Related Phenotypes and Stem Cell Lossrdquo Cell Stem Cellvol 1 no 1 pp 113ndash126 2007
[35] N E Mamrak A Shimamura and N G Howlett ldquoRecentdiscoveries in the molecular pathogenesis of the inherited bonemarrow failure syndrome Fanconi anemiardquo Blood Reviews vol31 no 3 pp 93ndash99 2017
[36] B P Alter ldquoDiagnosis Genetics and Management of InheritedBone Marrow Failure Syndromesrdquo International Journal ofHematology vol 2007 no 1 pp 29ndash39 2007
[37] L B Pontel I V Rosado G Burgos-Barragan et al ldquoEndoge-nous Formaldehyde Is a Hematopoietic Stem Cell Genotoxinand Metabolic Carcinogenrdquo Molecular Cell vol 60 no 1 pp177ndash188 2015
[38] G Pagano P Degan M DrsquoIschia et al ldquoOxidative stress asa multiple effector in Fanconi anaemia clinical phenotyperdquoEuropean Journal of Haematology vol 75 no 2 pp 93ndash1002005
[39] P FGiampietro P CVerlander J GDavis andADAuerbachldquoDiagnosis of Fanconi anemia in patients without congenitalmalformations An International Fanconi Anemia Registrystudyrdquo American Journal of Medical Genetics vol 68 no 1 pp58ndash61 1997
[40] P F Giampietro B Adler-Brecher P C Verlander S GPavlakis J G Davis and A D Auerbach ldquoThe need for moreaccurate and timely diagnosis in Fanconi anemia A report fromthe International Fanconi Anemia Registryrdquo Pediatrics vol 91no 6 pp 1116ndash1120 1993
[41] M P Wajnrajch J M Gertner Z Huma et al ldquoEvaluationof growth and hormonal status in patients referred to theinternational fanconi anemia registryrdquo Pediatrics vol 107 no4 I pp 744ndash754 2001
[42] N Giri D L Batista B P Alter and C A Stratakis ldquoEndocrineabnormalities in patients with fanconi anemiardquo The Journal ofClinical Endocrinology amp Metabolism vol 92 no 7 pp 2624ndash2631 2007
[43] S R Rose K C Myers M M Rutter et al ldquoEndocrine phe-notype of children and adults with Fanconi anemiardquo PediatricBlood amp Cancer vol 59 no 4 pp 690ndash696 2012
[44] A D Auerbach B Adler and R S K Chaganti ldquoPrenatal andpostnatal diagnosis and carrier detection of Fanconi anemia bya cytogeneticmethodrdquoPediatrics vol 67 no 1 pp 128ndash135 1981
[45] A D Auerbach M Sagi and B Adler ldquoFanconi anemiaPrenatal diagnosis in 30 fetuses at riskrdquo Pediatrics vol 76 no5 pp 794ndash800 1985
[46] L Faivre M F Portnoı G Pals et al ldquoShould chromosomebreakage studies be performed in patients with VACTERLassociationrdquo American Journal of Medical Genetics vol 137 no1 pp 55ndash58 2005
[47] B P Alter P S Rosenberg and L C Brody ldquoClinicaland molecular features associated with biallelic mutations inFANCD1BRCA2rdquo Journal ofMedical Genetics vol 44 no 1 pp1ndash9 2007
14 BioMed Research International
[48] K Myers S M Davies R E Harris et al ldquoThe clinicalphenotype of children with Fanconi anemia caused by biallelicFANCD1BRCA2mutationsrdquo Pediatric Blood amp Cancer vol 58no 3 pp 462ndash465 2012
[49] B G Yoon H N Kim U J Han et al ldquoLong-term follow-up of Fanconi anemia Clinical manifestation and treatmentoutcomerdquo Korean Journal of Pediatrics vol 57 no 3 pp 125ndash134 2014
[50] J G Hall ldquoReview and hypothesis Syndromes with severeintrauterine growth restriction and very short stature - Are theyrelated to the epigeneticmechanism(s) of fetal survival involvedin the developmental origins of adult health and diseaserdquoAmerican Journal of Medical Genetics Part A vol 152 no 2 pp512ndash527 2010
[51] A Petryk R K Shankar N Giri et al ldquoEndocrine disordersin Fanconi anemia Recommendations for screening and treat-mentrdquoThe Journal of Clinical Endocrinology ampMetabolism vol100 no 3 pp 803ndash811 2015
[52] S R RoseMM Rutter RMueller et al ldquoBonemineral densityis normal in children with Fanconi anemiardquo Pediatric Blood ampCancer vol 57 no 6 pp 1034ndash1038 2011
[53] A Petryk L E Polgreen J L Barnum et al ldquoBone mineraldensity in childrenwith fanconi anemia after hematopoietic celltransplantationrdquo Biology of Blood and Marrow Transplantationvol 21 no 5 pp 894ndash899 2015
[54] R Purkait A Mukherji S Datta and R Bhadra ldquoRenal arterystenosis An unusual etiology of hypertensive encephalopathyin a childwith fanconi anemiardquo Saudi Journal of KidneyDiseasesand Transplantation vol 26 no 4 pp 778ndash782 2015
[55] K H Chrzanowska H Gregorek B Dembowska-BaginskaM A Kalina and M Digweed ldquoNijmegen breakage syndrome(NBS)rdquoOrphanet Journal of Rare Diseases vol 7 article 13 2012
[56] L C Riches A M Lynch and N J Gooderham ldquoEarly eventsin the mammalian response to DNA double-strand breaksrdquoMutagenesis vol 23 no 5 pp 331ndash339 2008
[57] K Chrzanowska M Kalina H Rysiewski et al ldquoGrowthpattern in patients withNijmegen breakage syndrome evidencefroma longitudinal studyrdquoHormoneResearch in Paediatrics vol74 article S38 2010
[58] Group TINBSS ldquoNijmegen breakage syndromerdquo Archives ofDisease in Childhood vol 82 pp 400ndash406 2000
[59] M Digweed and K Sperling ldquoNijmegen breakage syndromeClinical manifestation of defective response to DNA double-strand breaksrdquo DNA Repair vol 3 no 8-9 pp 1207ndash1217 2004
[60] E Seemanova ldquoAn increased risk for malignant neoplasmsin heterozygotes for a syndrome of microcephaly normalintelligence growth retardation remarkable facies immun-odeficiency and chromosomal instabilityrdquo Mutation ResearchReviews in Genetic Toxicology vol 238 no 3 pp 321ndash324 1990
[61] K H Chrzanowska M Szarras-Czapnik M Gajdulewicz et alldquoHigh prevalence of primary ovarian insufficiency in girls andyoung women with Nijmegen breakage syndrome Evidencefrom a longitudinal studyrdquoThe Journal of Clinical Endocrinologyamp Metabolism vol 95 no 7 pp 3133ndash3140 2010
[62] C M R Weemaes T W J Hustinx J M J C Scheres P J JV Munster J A J M Bakkeren and R D F M Taalman ldquoAnew chromosomal instability disorder The nijmegen breakagesyndromerdquo Acta Paediatrica Scandinavica vol 70 no 4 pp557ndash564 1981
[63] A J Green J R W Yates A M R Taylor et al ldquoSevere micro-cephaly with normal intellectual development The Nijmegen
breakage syndromerdquo Archives of Disease in Childhood vol 73no 5 pp 431ndash434 1995
[64] D Gupta and A Nagarkar ldquoSpeech impairment in Nijmegenbreakage syndrome A rare anomalyrdquo International Journal ofPediatric Otorhinolaryngology vol 73 no 6 pp 873ndash875 2009
[65] P Muschke H Gola R Varon et al ldquoRetrospective diagnosisand subsequent prenatal diagnosis of Nijmegen breakage syn-dromerdquo Prenatal Diagnosis vol 24 no 2 pp 111ndash113 2004
[66] S Pasic M Cupic T Jovanovic S Djukic M Kavaric andI Lazarevic ldquoNijmegen breakage syndrome and chronic pol-yarthritisrdquo Italian Journal of Pediatrics vol 39 no 1 article no59 2013
[67] J P Patel J M Puck R Srinivasan et al ldquoNijmegen BreakageSyndrome Detected by Newborn Screening for T Cell ReceptorExcision Circles (TRECs)rdquo Journal of Clinical Immunology vol35 no 2 pp 227ndash233 2015
[68] I Demuth and M Digweed ldquoThe clinical manifestation of adefective response to DNA double-strand breaks as exemplifiedby Nijmegen breakage syndromerdquoOncogene vol 26 no 56 pp7792ndash7798 2007
[69] H Arora A H Chacon S Choudhary et al ldquoBloom syn-dromerdquo International Journal of Dermatology vol 53 no 7 pp798ndash802 2014
[70] C de Renty and N A Ellis ldquoBloomrsquos syndrome Why not pre-mature aging A comparison of the BLM andWRN helicasesrdquoAgeing Research Reviews vol 33 pp 36ndash51 2017
[71] C Keller K R Keller S B Shew and S E Plon ldquoGrowthdeficiency and malnutrition in Bloom syndromerdquo Journal ofPediatrics vol 134 no 4 pp 472ndash479 1999
[72] A Diaz M G Vogiatzi M M Sanz and J German ldquoEval-uation of short stature carbohydrate metabolism and otherendocrinopathies in Bloomrsquos syndromerdquo Hormone Researchvol 66 no 3 pp 111ndash117 2006
[73] C Ling J Huang Z Yan et al ldquoBloom syndrome complexpromotes FANCM recruitment to stalled replication forksand facilitates both repair and traverse of DNA interstrandcrosslinksrdquo Cell Discovery vol 2 article 16047 2016
[74] J S Renes R H Willemsen A Wagner M J J Finken and AC SHokken-Koelega ldquoBloom syndrome in short children bornsmall for gestational age A challenging diagnosisrdquoThe Journalof Clinical EndocrinologyampMetabolism vol 98 no 10 pp 3932ndash3938 2013
[75] M Maciejczyk B Mikoluc B Pietrucha et al ldquoOxidativestress mitochondrial abnormalities and antioxidant defense inAtaxia-telangiectasia Bloom syndrome andNijmegen breakagesyndromerdquo Redox Biology vol 11 pp 375ndash383 2017
[76] R M Brosh M Bellani Y Liu and M M Seidman ldquoFanconiAnemia A DNA repair disorder characterized by accelerateddecline of the hematopoietic stem cell compartment and otherfeatures of agingrdquo Ageing Research Reviews vol 33 pp 67ndash752017
[77] S Yan M Sorrell and Z Berman ldquoFunctional interplay be-tween ATMATR-mediated DNA damage response and DNArepair pathways in oxidative stressrdquo Cellular and Molecular LifeSciences vol 71 no 20 pp 3951ndash3967 2014
[78] L M M Nardozza A C R Caetano A C P Zamarian etal ldquoFetal growth restriction current knowledgerdquo Archives ofGynecology and Obstetrics vol 295 no 5 pp 1061ndash1077 2017
[79] M Tomas Vila J P Verdu M R Piera and C O AlonsoldquoNijmegen breakage syndrome phenotype a disorder to con-sider in the diagnosis ofmicrocephalyrdquoAnales De Pediatria vol74 pp 58ndash60 2011
Submit your manuscripts athttpswwwhindawicom
Stem CellsInternational
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
MEDIATORSINFLAMMATION
of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Behavioural Neurology
EndocrinologyInternational Journal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Disease Markers
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
BioMed Research International
OncologyJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Oxidative Medicine and Cellular Longevity
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
PPAR Research
The Scientific World JournalHindawi Publishing Corporation httpwwwhindawicom Volume 2014
Immunology ResearchHindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Journal of
ObesityJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Computational and Mathematical Methods in Medicine
OphthalmologyJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Diabetes ResearchJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Research and TreatmentAIDS
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Gastroenterology Research and Practice
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Parkinsonrsquos Disease
Evidence-Based Complementary and Alternative Medicine
Volume 2014Hindawi Publishing Corporationhttpwwwhindawicom

BioMed Research International 5
6 DDR Alteration and Growth Failure
Historically disruption of the DDR has been associatedwith cell growth abnormalities in a unilateral way alwayspointing towards the increased cell number in the form ofderegulated cell proliferation in cancer [19] But there islittle information on how DDR alterations can also lead toderegulation of growth in the opposite direction resultingin lack of growth due to cell death and low cell repro-duction One of the first observations to partner growthdeficiency with an altered DDR was the finding that someSeckel syndrome patients (SS) a rare phenotype consistingof primordial dwarfism and microcephaly had mutationsin the ATR gene which encodes the ATR kinase a DDRtransducer Further analysis of SS patients revealed locusheterogeneity for this phenotype mutations in other genesrelated to DDR or DNA repair also led to this clinical pictureThis observation has reinforced the association betweenDDRfailure and severe intrauterine growth retardation Moreovergenes that participate in centrosomal biology are also relatedto the uncommon phenotype of microcephalic primordialdwarfism suggesting that centrosomes have a central rolefor the adequate differentiation of early neuroprogenitorsIt has then been proposed that failure in cell proliferationsecondary to abnormal mitosis is the cause of primordialdwarfism since the multipolar spindles result in the acti-vation of checkpoints reducing proliferation and activatingapoptosis [20]
For the phenotype of growth restriction to be evidentprenatally the mechanisms regulating growth must be com-promised from the beginning of the development in embry-onic stem cells (ESCs) which are pluripotent cells derivedfrom the three primary germ layers ectoderm endodermandmesoderm and that have the capacity to differentiate intomore than 200 cell typesThese cells have been proven to havean extremely efficient DDR and proficient DNA repair mech-anisms that allow for a rigorousmaintenance of their genomeintegrity otherwise unrepaired DNA damage in ESCs wouldbe amplified affecting normal human development
ESCs have an extremely active proliferation rate theircell cycle has a characteristically reduced G1 phase andrepair mechanisms are heightened When comparing ESCsto fibroblasts it stands out that MMR is enhanced BERand NER repair pathways are highly competent and therepair of DSBs is preferentially made through the reliableHR pathway [21] Moreover when HR is not available andDSBs accumulate apoptosis is the preferred route to removehighly damaged cells It is interesting that DSB repair inESCs requires signaling through ATR instead of ATM ESCshave a special mechanism to deal with DNA damaged cellswhen inefficient DNA repair or DDR affects the induction ofapoptosis or autophagy [22] This mechanism leads to ESCdifferentiation that is driven by damage-induced expressionof the p53 transcription factor damaged differentiated cellsare efficient in cell cycle arrest and apoptosis This strategyresults in the maintenance of genetic stability in a decreasednumber of ESCs and a portion of differentiated cells thatbecome senescent both resulting in growth deficiency[21]
Growth deficiency is at the center of many diseasesincluding extremely low body size In mammals overall sizeis determined by the number of cells body mass is then thesum of all the cells that have proliferated minus those thathave died A fetus that is growing harmonically has accuratebalance between these two processes failure of either one ofthese results in dramatic effects when they occur in the ESCpopulation a decrease in cell proliferation rate or an increasein apoptosis leads to intrauterine growth retardation (IUGR)[23]
7 Chromosome Instability Syndromes withIntrauterine Growth Retardation
71 Seckel Syndrome Seckel syndrome (SS) is an autosomalrecessive disorder clinically and genetically heterogeneousSo far at least six genes have been associated with the Seckelphenotype most of these genes participate in ATR-mediatedDDR and in centrosomal function Two clinical subgroupscan be identified on the one hand patients with mutationsin ATR NIN and ATRIP genes only present the Seckelphenotype while on the other hand those with mutationsin CENPJ CEP152 or RBBP8 show allelic heterogeneity andbesides the SS phenotype can also manifest as a spectrumof disorders known as Primary Autosomal Recessive Micro-cephalies [24ndash28] SS patients who bear mutations in ATRshow a classical Seckel phenotype the SS data presented herewill be limited to such patients
ATR is localized in 3q23 it is one of the serine threoninekinases that belong to the PIKK family They have a funda-mental role in the DDR since they participate as transducersin the signaling of DNA lesions especially when the DDRresponds to stalled replication forks and bulky lesions inDNA[24 25] ATR responds preferentially to ssDNA during the Sphase It also plays a crucial role in preventing DNA breakscaused by fork pausing when DNA replication machineryfinds DNA lesions or complex DNA structure and sequences[24] ATR stability depends on binding of ssDNA to theATR cofactor ATRIP (ATR interacting protein) and thesingle-stranded binding protein (RPA) ATRIP is required forATR localization to the ssDNA regions and hence for ATRactivation [25 27] Major functions of ATR are activation ofcell cycle check point arrest stabilization of stalled replicationforks and promotion of replication fork restart which isachieved through its ability to phosphorylate a wide range ofsubstrates that include p53 and H2AX [27 29]
Cellular phenotype of ATR deficient cells is characterizedby decreased phosphorylation of ATR-dependent substratesas well as an impaired G2M checkpoint arrest These cellsare characterized by markers that signal unrepaired DSBslike the presence of 120574H2AX chromosomal breakage [2629 30] and micronuclei formation This cellular phenotypemay be originated by a failure to recover from replicationstalling which generates DSBs that are normally repairedby HR when they occur during SG2 In SS cells theabsence of ATR is critical during embryonic developmentthis deficiency leads to genomic instability cell senescenceand cell death that leads to fetal growth and accelerated aging[31]
6 BioMed Research International
Figure 3 Seckel syndrome patient Note the severe microcephalyand the ldquobird-likerdquo appearance facies with micrognathia and reced-ing forehead The patient is severely disabled with no independentmarch
Moreover it appears that ATR and the other SS genes notonly participate in the DDR but also take part in the controlof centrosome maturation This engagement in centrosomebiology is also true for other DDR proteins like BRCA2biallelic mutations in its gene are responsible for a subgroupof Fanconi anemia patients [32]Theunifying feature betweenall Seckel patients irrespective of the molecular defect isthat their cells have an altered cell cycle progression thatis particularly evident during high rate cell division whenthere is hypersensitivity to replicative stress and centrosomaldysfunction This is especially important in cells with highdivision rates like the ones found in developmental stageswhere rapid replication is key [24 27]
SS is characterized by IUGR dwarfism microcephaly(below minus4 SD) mental retardation and some other anomalieslike luxation of the head of the radius scoliosis bone agedelay and seizures (Figure 3) The distinctive facial featuresinclude a prominent nose with micrognathia and a recedingforehead resulting in a ldquobird-like appearancerdquo [26 31 33]Since this syndrome has important clinical heterogeneityother anomalies have been reported including mandibularhypoplasia sternal abnormalities clinodactyly and low setears with hypoplastic lobules Although rare other reportedfeatures are moyamoya syndrome osteosarcoma and pol-yarteritis nodosa [26] Cerebral malformations like neuronalmigration abnormalities have been described but are notalways present [33] No glucose metabolism abnormalitieshave been reported
Dwarfism can be related to a reduction in the totalnumber of cells generated during development leading tohypoplastic tissue and reduced organism size [23] On theother handmicrocephalymay be related to an impairedDNAdamage response signal that could alter the cellular thresholdfor cell death resulting from DNA damage increasing thelevels of apoptosis during development developing neuronsare rapidly proliferating and potentially generate high levelsof oxidative damage which may lead to a higher level oflesions being faced at replication forks [23 25] Also analtered mitosis secondary to impaired spindle formationcould delay mitotic progression and increase the proportionof nonviable cell divisions Finally the stem cells may beaffected by abnormal centrosomal function Stems cells haveasymmetric divisions in order to preserve the characteristics
Figure 4 Fanconi anemia patient This six-year-old girl is 105 cmtall her height is just below the 5th percentile and her at-term birthweight is reported to be of 1900 gr Characteristic features of FA areevident skin hyperpigmentation bilateral radial defects consistingof bilateral thenar hypoplasia and absent fold of the right thumbwhich cannot be bent
of a stem cell and the centrosomes play an important role insuch divisions [23]
There is limited clinical information regarding age-related diseases in SS there is a void of prospective follow-up data from these patients that can only be obtained byfollowing a cohort of SS patients something that is apparentlynot being done at this time Nevertheless animal modelsbring some clues over the possibility of an aging phenotypein SS patients since ATR deficient adult mice show prematureage-related phenotypes as well as increased deterioration oftissue homeostasis [29 34]
72 Fanconi Anemia DNA interstrand crosslinks are ex-tremely noxious DNA lesions that affect central cellularprocesses like transcription and replication The FABRCApathway is responsible for the appropriate processing ofthese lesions protein products from at least 21 FANC genesparticipate in this pathway [35] The malfunction of any ofthose FANC proteins leads to the clinical phenotype knownas Fanconi anemia (FA) which is characterized by shortstature congenital malformations from the VACTERL-Hspectrum bone marrow failure and an increased suscepti-bility to cancer like acute myeloid leukemia epithelial headand neck cancer [36] (Figure 4) Most of the FA families bearbiallelic mutations in FANC genes that have an autosomicrecessive inheritance pattern only families with mutations inFANCB show an X-linked recessive pattern while those inwhich FANCR is the affected gene demonstrate an autosomicdominant one [35]
The FABRCA is an S-specific pathway that has 3 basicsteps it starts with the detection of the ICL by the proteinFANCM followed by the recruitment of the FA core com-plex that is responsible for the monoubiquitination of theFANCD2I heterodimer which in turn favors the recruit-ment of effector FANC-repair proteins that restore the DNAto its original form [35]
BioMed Research International 7
(a) (b)
Figure 5 Chromosomal instability induced by 40 ngml mitomycin C (a) Lymphocytes from a healthy individual (b) lymphocytes from aFA patient Short arrows show chromosomal breaks the long arrow shows a quadriradial figure Note the exacerbated chromosome instabilityfound in the FA patient
The cellular phenotype of FA derived cells is extremelyconstant An aberrant FABRCA pathway can result inunrepaired DSBs that manifest as chromosomal breaks orabnormal repair by an error-prone repair pathway that resultsin radial figures These alterations are cytogenetic evidenceof chromosomal instability which is the hallmark of FA cellsand is exploited for clinical diagnostic purposes (Figure 5)The agents capable of inducing this chromosomal instabilityare from endogenous origin like aldehydes [37] and reactivespecies of oxygen (ROS) [38] as well as exogenous sourceslike bifunctional alkylating agents (diepoxybutane or mito-mycin C) In addition FA cells have accumulation of cells inG2 phase of the cell cycle resulting from a functional G2Mcheckpoint and a proapoptotic phenotype
In contrast with the cellular FA phenotype the clinicalpicture in FA patients is extremely variable not every patientwill have all the manifestations one-third of patients do nothave congenital malformations [39] while almost 90 willdevelop bone marrow failure [36] One of the more constantmanifestations in FApatients is growth parameters alterationAn analysis from the international Fanconi anemia registry(IFAR) data showed that over 60 of FA patients presentedshort stature (below the 5th percentile) while birth lengthandweight below the 5th percentile was respectively reportedin almost 30 and nearly half of FA patients [40]Moreover aprospective study of data from 54 IFAR participants showedthat the mean standard deviation score (SDS) for height inthese patients was significantly below normal for age and sexat minus235 plusmn 028 meanwhile mean SDS for weight was betteralthough below normal (minus126 plusmn 024) In this study perinatalgrowth data was not reported [41]
Other than the IFAR data on growth there are anothertwo studies that analyze growth parameters of FA patientsAnthropometric measurements from 45 patients with Fan-coni anemia from the National Cancer Institutersquos inher-ited bone marrow failure syndromes (IBMFS) cohort wereassessed This cohort had a mean SDS for height of minus21 plusmn
189 The height of over half of the participants (54) wascategorized as short (SDS gt 20 SD) in this subset of patientsthe mean SDS for height was minus38 plusmn 15 [42] Finally theevaluation of 120 FA patients from the FA ComprehensiveCare Clinic of Cincinnati Childrenrsquos Hospital Medical Centerrevealed that median height SDS was shorter than expectedin children and adults irrespective of gender Furthermorethis study presented birth information from 70 patients (59children and 11 adults) from the cohort 51 of the childrenand 3 adults were born small for gestational age their medianbirth weight at term was 202 kg (range 15ndash26 kg) [43] Theintrauterine growth restriction seen in FA patients has alsobeen documented in several case reports in which at-termbirth weight ranges from 1780 to 3200 gr [44ndash49] Eventhough growth abnormalities have been identified in FApatients with mutations in almost every FANC gene it hasbeen shown that patientswithmutations in certain genes havea more severe growth delay That is the case for patients withbiallelic mutations in FANCD1 [47 48] as well as those whobear mutations in FANCC for whom an SDS for height ofminus384 has been found [41]
Endocrine abnormalities have been proven to be aninherent part of the FA phenotype up to 80 of patientshave one or more endocrine abnormalities Besides growththyroid function and glucose homeostasis are frequentlyaffected [40ndash43] Considering the existing evidence for arelationship between low birth weight and an increased riskfor noncommunicable adult diseases like diabetes hyperten-sion heart disease dyslipidemia and osteoporosis [50] it isrelevant to revise these diseases in FA The FA cohorts inwhom growth was assessed were also evaluated for endocrinestatus Glucose homeostasis is affected in a large portion ofFA patients impaired glucose tolerance has been found in27ndash68 of them whereas diabetes has a prevalence of 8ndash10Dyslipidemia has been assessed in only a small portionof FA patients but it has been found in 17ndash55 of theevaluated subjects [51]There are conflicting results over bone
8 BioMed Research International
mineral density (BMD) status in FA the first time this wasevaluated 92 of the patients were found to have osteopeniaor osteoporosis [42] nevertheless a study that evaluated alarger FA cohort found that lowBMD is not a frequent finding[52] Further research on this topic has raised the questionof whether BMD deficit is intrinsic to the FA phenotype ora consequence of hematopoietic cell transplantation (HCT)an interrogation that is still awaiting to be answered [53]Cardiovascular adult diseases are not relevant in the FA phe-notype heart disease in these patients is from the congenitaltype as 13of patients have cardiacmalformations [40] whilehypertension has only been reported in two patients as theresult of renal malformations [54]
Findings from the different FA cohorts show that shortstature is an inherent feature of the FA phenotype thisfeature does not respond to a single explanation the apoptosisprone FA cellular phenotype is certainly a contributing factorfor this The fact that FA patients have a constitutionallydefective pathway since conception could explain the clinicalphenotype of RCIU Short stature may also be exacerbated byaccompanying endocrinopathies The cooccurrence of manyendocrine alterations has encouraged unifying explanationssome have proposed that endocrinopathies are secondaryto increased cytokine activity found in FA cells [41] whileothers favor the view that some endocrine secretory cellsmight be damaged by high levels of reactive oxygen specieswhich are known to be elevated in FA patients [43] In linewith the developmental origin of adult health and diseasetheory it could also be possible that the increased prevalenceof glucose homeostasis alterations and dyslipidemia reportedin FA patients is a consequence of intrauterine growthrestriction of these patients Nevertheless the attemptedgenotype-phenotype correlation of the endocrine phenotypein FA patients does not seem to support that Patients withmutations in FANCA show a mild endocrine phenotype inwhich height is not severely affected and insulin resistanceis mild whereas mutations in FANCC which are relatedto shorter stature have the least insulin resistance [41]Moreover no direct relationship between birth weight andglucose tolerance was identified when it was intentionallylooked for [43] although the number of patients in whichthese observations were made is limited
73 Nijmegen Breakage Syndrome Nijmegen breakage syn-drome (NBS) is an autosomal recessive disease caused bybiallelic mutations in NBN a gene that encodes nibrin aprotein involved in DNA repair and cell cycle checkpointregulation It participates in the former by sensing double-strand breaks as part of the trimeric complexMRN alongsideMRE11 andRAD50Meanwhile for the latter it contributes tothe appropriate activation of ATM andATRwhich are centraltransductors of the DNA damage response (DDR) [55] Themalfunction of nibrin translates in a cellular phenotypemarked by chromosomal instability radiosensitivity reducedphosphorylation of ATM substrates and S and G2M cellcycle defects [56] Chromosome instability is evidenced bycytogenetic methods in 10ndash60 of cells in the form of breaksand numeric and structural aberrations translocations andinversions affecting chromosomes 7 and 14 are found in the
147
Figure 6 Translocation between chromosomes 7 and 14 is typicalin NBS patientsrsquo cells
majority of NBS patients and are considered a cytogeneticcharacteristic of this syndrome (Figure 6) [57]
The clinical impact of these alterations is a phenotypecharacterized by microcephaly a distinctive facial appear-ance consisting of receding forehead and mandible and aprominent mid face with a long nose and philtrum aswell as immunodeficiency that leads to recurrent infectionsand an increased risk for the development of neoplasiaparticularly leukemia and lymphoma According to theinternational Nijmegen breakage syndrome study groupgrowth retardation is also a hallmark of this disease [58]although there is not many details about this feature in theliterature
Most of the information on the natural history of NBSavailable today comes from patients participating in reg-istries in which fairly large cohorts of NBS patients areincluded There is a large representation of Slavic patientsin these cohorts which correlates with the high carrierfrequency of a founder mutation of NBN in this populationFrom these studies it is evident that the most severelyaffected anthropometric measure in NBS patients is headcircumference since all participants display microcephalyeven though only 75 display this feature at birth Whenit comes to growth parameters the same study states thatall patients have growth retardation which is described asproportionate and early occurring [58] although the specifictemporality is not defined A posterior report points out thatthe growth retardation seen in most NBS patients locatesthem in the 10th percentile in growth charts and that birthheight and weight are usually within normal parameters [59]Nevertheless there are other authors who report prenataland postnatal growth retardation [55 60] and a tendency forshort stature that is more evident during the first year of life[61] Also several case reports of NBS patients in which birthweight is informed demonstrate prenatal growth restriction[62ndash67] although this could represent a report bias Themore comprehensive data analysis on growth that includesperinatal information of NBS patients is the one that analyzesdata from 67 patients followed for 15 years Eighty percentof these patients were born at term the girls were found tohave a mean birth weight of 27 kg and mean birth heightof 514 cm while boys were reported to have a mean birthweight of 28 kg and mean birth height of 523 cm Moreoverall patients irrespective of gender were found to have ameanheight reduced by over 2 SDS at one year old [57] These data
BioMed Research International 9
(a) (b)
Figure 7 Sister chromatid exchange in cells from a healthy individual (a) and from a BLM patient (b)
support the fact that growth retardation in NBS is a prenatalphenomenon
Nibrin has been found to have essential functions inthe regulation of the cell cycle which translates into anabsolute need for this protein for cell proliferation [68]It would seem logical that mutations of the NBN genethat compromise the appropriate function of nibrin wouldlead to abnormal growth when thought from an organismperspective Mechanistically speaking poor cellular growthcaused by mutations in a particular gene can be thought ofas the main explanation for the growth restricted phenotypebut it has been shown that mutations in other DDR genesthat share the cellular phenotype of poor growth like ATMdo not replicate the compromised growth phenotype atthe organism level growth retardation is absent in ataxiatelangiectasia (AT)This data suggests that there are certainlyother contributing factors to the abnormal growth phenotypeseen in NBS patients [58]
74 Bloom Syndrome Bloom syndrome (BS) is an autosomalrecessive disorder caused by homozygous or compoundheterozygous mutations in the BLM gene (15q261) thatencodes the RecQL3 helicase BLM has a critical role inthe maintenance of genome stability acting at the interfacebetweenDNAreplication recombination and repair [69 70]To date over sixty different mutations including nonsenseand missense have been identified all of them result inthe inactivation of BLM and the consequent loss of itshelicase activity The BLM gene encodes a 1417 amino acidnuclear protein its expression peaks during the S and G
2M
phases of the cell cycle which is consistent with its rolein DNA replication and recombination BLM specificallyunwinds structures like forked DNA duplexes RNA-DNAheteroduplexes and R-Loops which explains its importanceduring replication fork progression and transcription besidesit is central for Holliday Junctions (HJs) dissolution forHR The dissolution of HJs by the topoisomerase III120572-BLMcomplex cannot be replaced by any other RecQ helicase inthe family [69 70] It has also been found to have a role in
the annealing activity of the ssDNA the proper sister chro-matid segregation during mitosis and telomere maintenance[70]
BLM can have both pro- and antirecombinogenic func-tions that are regulated by posttranslational modificationsincluding phosphorylation sumoylation and ubiquitination[70]
BLM also enables sister chromatid segregation by pro-cessing unresolved replication intermediates that manifest inmitosis as ultrafine DNA bridges (UFBs) and together withtopoisomerase III120572 RMI1 and RMI2 localizes to UFBs inanaphase BML deficient cells exhibit and increase frequencyof UFBs suggesting a role of BLM in the resolution ofthese structures Failure to resolve these UFBs leads to DNAbreakage as mitosis proceeds [70]
Therefore BS cells are characterized by an increasein chromosomal aberrations including chromatid gapsand breaks telomere associations and quadriradial chro-mosomes resulting from unsolved recombination betweenhomologous chromosomes BS cells exhibit increased muta-tion rates and the genomic instability includes elevatedmitotic HR and unequal sister chromatid exchange (SCEs)(Figure 7) Perhaps the most characteristic feature is the overtenfold increase in SCEs which results from crossover eventsduring HR repair of damage replication forks [50 69 70]
Clinically the more striking BS feature is IUGR averagebirth weight at term is 1850 g and birth length is 44 cmFor both boys and girls weight and length in BS are morethan two standard deviations below normal indicating thatgrowth retardation has a prenatal origin At postnatal agesheight remains below the normal range and is accompaniedby a paucity of subcutaneous fat Average adult height inmales has been found to be 148 cm (130ndash162 cm) whilein females it has been reported to be 139 cm (122ndash151 cm)[50 70 71]
BS patients have overall proportionated short staturebut the head is reported to be small and narrow relativelyto the body size it is described as mild microcephalyand is accompanied by malar hypoplasia Patients have
10 BioMed Research International
Figure 8 Bloomsyndromepatient inwhom the characteristicmalarerythema is present
been described to have a high pitched voice [50 70] Theskin appears normal at birth but in the first or secondyear of life in response to sun exposure children developan erythematous rash with a butterfly distribution in themalar area and the back of hands and feet The rash caninclude telangiectasia The severity varies between patientssome can even lose their eyelashes and develop blisteringaround the mouth The presence of cafe-au-lait spots andhypopigmented areas of skin associated with contiguoushyperpigmented areas is common (Figure 8) Intellectualabilitiesmay be limited in some patients and normal in others[50 70]
Other clinical conditions reported in BS patients are gas-troesophageal reflux and diarrhea in infants mild immuno-logical deficiency with frequent episodes of otitis mediaazoospermia or severe oligospermia in males and prema-ture cessation of menstruation in females minor anatomicdefects and increased risk for neoplasia which is the maincause of dead in BS [70] Another common medical con-dition in BS is diabetes mellitus associated with impairedglucose tolerance and insulin resistance it has been reportedin up to 16 of patients [70] According to data fromthe Bloomrsquos Syndrome Registry diabetes in these patientstends to begin early with a mean age at diagnosis of 266years It is not associated with ketosis and it does nothave the classical hereditary pattern seen in type 2 diabetes[50 72]
Short stature in BS is not due to hormonal causes sincethe size of cells in persons with BS is normal it has beenhypothesized that there are fewer of them due to either adecrease in the cell division rate an increase in apoptosis oreven a combination of both BS cells have troublemeeting thedemands of fast cell divisions encountered in tissues duringembryonic development The leading hypothesis suggeststhat problems arising during DNA synthesis require a longerS phase to overcome the challenge which translates intoslowing of the cell division rate and an increase in apoptosis[70]
8 Concluding Remarks
This review has focused on discussing phenotypes of CISin which there is a prenatal alteration of growth The foursyndromes discussed here are rare diseases whose prevalenceis difficult to calculate since appropriate identification anddiagnosis of affected individuals among the general popula-tion are not straightforward It is important to note that theavailable information on the natural history of FA NBS andBS comes from the analysis of several patients that participatein registries This strategy results in detailed informationthat permits a better analysis of the clinical phenotype ofthese rare diseases Meanwhile available data of SS is moreanecdotic which results in a nonsystematic gathering ofinformation which is thus frequently incomplete
From the available clinical data of these CIS it is evidentthat growth is not affected in the same extent for all ofthese syndromes the phenotypes that exhibit a more severelystagnated perinatal growth are BS and SS The severe growthdelay reported in these patients has been described as apathognomonic sign of these diagnoses In patients withFA perinatal growth can also be severely affected but notevery FA patient shows this manifestation Finally NBShas been described to have growth retardation of prenatalorigin of mild severity almost within the lower normal range(Figure 9) The cephalic circumference can be affected in allof these syndromes severe microcephaly is pathognomonicin SS and NBS it is described as mild for BS patients and it isfound in less than half of FA patients (Table 2)
When trying to understand why a subset of CIS showsprenatal growth retardation it could be alleged that theintrinsic chromosomal instability is responsible for it Butthis would not explain why prenatal growth retardation isnot a universal CIS feature for example ataxia telangiectasiapatients who have biallelic mutations in the ATMkinase genedo not show prenatal growth delay It strikes that a molecularcommon feature shared by the prenatal growth retardationSIC phenotypes is that they are caused by mutations ingenes that are necessary for an appropriate response to DSBsduring the S phase of the cell cycle The molecular defectin SS affects the functioning of ATR the preferred DDRtransducing kinase used by highly replicating ESCs TheFABRCA pathway which is affected in patients with FAdetects ICLs upon replication fork arrest Nibrin the proteinaffected in patients with NBS is induced during S phasefor the detection of DSBs And the BS helicase forms aFANCM-BLM complex needed to sense ICLs during S phase[73] It could then be argued that altered DNA replicationis an important factor for the development of intrauterinegrowth restriction in these CIS Nevertheless it must be keptin mind that the inherent chromosome instability found inthese syndromes may also be affecting normal growth in thepatients [27 43 57 60 71]
Being small for gestational age has been associatedwith a higher risk of noncommunicable adult diseases likeglucose homeostasis disorders dyslipidemia hypertensionand others It has been proposed that fetal reprogrammingto enhance fetal survival despite the risk for adult onsetdiseases is an outcome that does not take into account
BioMed Research International 11
Table 2 Growth features of chromosomal instability syndromes
SyndromeldquoLocirdquo At-term birth weightheight Microcephaly Adult height Adult onset diseases
Seckel SyndromeldquoATR3q23rdquo
Birth weight below minus3 SD(2055 g)
Severeminus4 SD
Postnatal growth retardation(below minus5 SD) Not reported
Fanconi anemialdquo21 FANC genesrdquo
Median weight 202 kg(15ndash26 kg) In 20ndash50
50ndash60 of patients with medianheight lt minus18 SDSWomen minus34 SDSMen minus44 SDS
CancerDiabetes mellitusDyslipidemia
Altered bone mineral densityNijmegen BreakageSyndromeldquoNBN8q21rdquo
Mean weightheight girls27 kg514 cm
Mean weightheight boys28 kg523 cm
100 Mean height for women minus18 SDSMean height for men minus23 Cancer
Bloom SyndromeldquoBLM15q261rdquo
Mean weight 189 kg plusmn 035 kg forboys
Mean weight 187 kg plusmn 035 kg forgirls
Mean height 434 cm plusmn 44 cm forboys
Mean height 438 cm plusmn 28 cm forgirls
Mildmicrocephaly
Mean height 1455 cm plusmn 76 cmmales
Mean height 1415 cm plusmn 61 cm forfemales
CancerDiabetes mellitus
See [27 33 40 43 50 57 69]
45 53
43245
Height (cm)
Weight (kg)
Percentile 3 Percentile 97Percentile 50495
33
Normalindividual
Mean 2055
SeckelSyndrome
2615Median 202
FanconiAnemia
Mean 51
Mean 275
Nijmegen BreakageSyndrome
38 49
24513
Mean 436
Mean 188
BloomSyndrome
Figure 9 Anthropometric features at birth of chromosome instability syndromes with perinatal growth retardation Comparison of theavailable growth data from SS FA NBS and BS syndrome against birth data from the WHOrsquos growth standards for infants Although meanheight and weight values of NBS patients are found to be within normal percentiles according to WHO standards there are several authorswho refer to prenatal growth restriction [55 63 65 79]
the reason for the prenatal growth restraint [50 72 74] Itmust be kept in mind that noncommunicable diseases aremultifactorial entities in which genetic and environmentalfactors converge and their cause cannot be attributed to asingle explanation However when growth restriction is akey feature in syndromes with chromosome instability the
possibility that cell hypoplasia due to DNA repair malfunc-tion is contributing to the growth restriction phenotypemustbe contemplated Moreover since none of these adult onsetdiseases is reported as an inherent element of the SS and NBSphenotypes the direct connection between low birth weightand adult noncommunicable diseases is less of a straight
12 BioMed Research International
shot Furthermore there are other Mendelian syndromeswith mutations in DNA repair genes that characteristicallyshow adult noncommunicable diseases but do not haveIUGR such is the case for Werner syndrome a progeroiddisease caused by biallelic mutations in another RecQ heli-case (RecQ4) that clinically presents with postnatal shortstature and a prevalence of type 2 diabetes mellitus of 70[50 70 74]
Natural history of FA NBS and BS documented throughthe existing patient registries has allowed the identificationof noncommunicable diseases to be a part of the clinicalspectrum of these syndromes (Table 2) Meanwhile from theinformation available through SS case reports no adult onsetdisease has been found to be part of this phenotype To thebest of our knowledge the direct investigation of nonevidentendocrinologic alterations like glucose homeostasis or dys-lipidemia has not been directlymade in SS patients For a raredisease like SS such a study can only be done if a fairly largegroup of patients like the one found in registries is availableIf such a study was to be performed hidden features in SSpatients could be unraveled
Oxidative stress sensibility is a cellular feature sharedby all the SIC syndromes with IUGR that could contributeto the explanation of the premature development of non-communicable adult diseases in these patients Reports haveshown that BS and NBS cells have endogenous reactiveoxygen species (ROS) overproduction and an impairedmitochondrial homeostasis [75] it is also well known thatFA cells show increased levels of oxidative damage [3876] and there is evidence that oxidative stress can activateATR-mediated checkpoint signaling [77] Since this kind ofdamage has soundly been related to age-associated diseasesthat result from tissue degeneration exacerbated oxidativedamage found in these syndromes could result in cellu-lar aging that manifests as overall premature aging withparticular symptoms like glucose homeostasis alterations[76 77]
Fetal growth restriction is a multifactorial conditionwhere wide arrays of factors converge Fetal aspects inparticular those affecting the genetic constitution of thefetus have been recognized to play an important role Ithas been demonstrated that chromosomal abnormalities andmonogenic syndromes caused by mutations in genes thatparticipate in growth or metabolic pathways directly affectfetal growth [78] Even though they are rare entities CISappear as another group of monogenic pathologies thatbroaden the list of genetic fetal factors of fetal growthrestriction
Consent
The necessary consent for the publication of the photographswas obtained
Conflicts of Interest
The authors declare that there are no conflicts of interestregarding the publication of this paper
Authorsrsquo Contributions
The three authors contributed equally andwrote the first draftof the paper The final version was approved by everyone
Acknowledgments
This paper is supported by SEP-CONACYT Project 243102Benilde Garcıa-de Teresa received the 574025 scholarshipfrom CONACYT The paper is also supported by PAPIIT-UNAM Project IA202615 and Fondos Federales INP Project41-2014
References
[1] K W J Derks J H J Hoeijmakers and J Pothof ldquoThe DNAdamage response The omics era and its impactrdquo DNA Repairvol 19 pp 214ndash220 2014
[2] S P Jackson and J Bartek ldquoThe DNA-damage response inhuman biology and diseaserdquoNature vol 461 no 7267 pp 1071ndash1078 2009
[3] J H J Hoeijmakers ldquoDNA damage aging and cancerrdquo TheNew England Journal of Medicine vol 361 no 15 pp 1475ndash14852009
[4] G Spivak ldquoNucleotide excision repair in humansrdquoDNARepairvol 36 pp 13ndash18 2015
[5] J Vijg XDong BMilholland andL Zhang ldquoGenome instabil-ity a conserved mechanism of ageingrdquo Essays in Biochemistryvol 61 no 3 pp 305ndash315 2017
[6] J I Garaycoechea and K J Patel ldquoWhy does the bone marrowfail in Fanconi anemiardquo Blood vol 123 no 1 pp 26ndash34 2014
[7] R Ceccaldi B Rondinelli andAD DrsquoAndrea ldquoRepair PathwayChoices andConsequences at theDouble-Strand BreakrdquoTrendsin Cell Biology vol 26 no 1 pp 52ndash64 2016
[8] R Biehs M Steinlage O Barton et al ldquoDNA Double-StrandBreak Resection Occurs during Non-homologous End Joiningin G1 but Is Distinct from Resection during HomologousRecombinationrdquo Molecular Cell vol 65 no 4 pp 671ndash684e52017
[9] A Ciccia and S J Elledge ldquoTheDNAdamage response makingit safe to play with knivesrdquoMolecular Cell vol 40 no 2 pp 179ndash204 2010
[10] L H Pearl A C Schierz S E Ward B Al-Lazikani and F MG Pearl ldquoTherapeutic opportunities within the DNA damageresponserdquo Nature Reviews Cancer vol 15 no 3 pp 166ndash1802015
[11] S-F Yang C-W Chang R-J Wei Y-L Shiue S-N Wang andY-T Yeh ldquoInvolvement of DNA damage response pathways inhepatocellular carcinomardquo BioMed Research International vol2014 Article ID 153867 2014
[12] M He W Zhou C Li and M Guo ldquoMicroRNAs DNAdamage response and cancer treatmentrdquo International Journalof Molecular Sciences vol 17 no 12 article no 2087 2016
[13] K A Cimprich and D Cortez ldquoATR an essential regulator ofgenome integrityrdquo Nature Reviews Molecular Cell Biology vol9 no 8 pp 616ndash627 2008
[14] B M Sirbu and D Cortez ldquoDNA damage response three levelsof DNA repair regulationrdquo Cold Spring Harbor Perspectives inBiology vol 5 article a012724 no 8 2013
BioMed Research International 13
[15] C Beck I Robert B Reina-San-Martin V Schreiber andF Dantzer ldquoPoly(ADP-ribose) polymerases in double-strandbreak repair focus on PARP1 PARP2 and PARP3rdquo Experimen-tal Cell Research vol 329 no 1 pp 18ndash25 2014
[16] D W Meek ldquoTumour suppression by p53 a role for the DNAdamage responserdquo Nature Reviews Cancer vol 9 no 10 pp714ndash723 2009
[17] A Rodrıguez L Torres U Juarez et al ldquoFanconi anemiacells with unrepaired DNA damage activate components of thecheckpoint recovery processrdquo Theoretical Biology and MedicalModelling vol 12 no 1 article 11 2015
[18] H Wang X Zhang L Teng and R J Legerski ldquoDNA damagecheckpoint recovery and cancer developmentrdquo ExperimentalCell Research vol 334 no 2 pp 350ndash358 2015
[19] P A Jeggo L H Pearl and A M Carr ldquoDNA repair genomestability and cancer A historical perspectiverdquo Nature ReviewsCancer vol 16 no 1 pp 35ndash42 2016
[20] F S Alkuraya ldquoPrimordial dwarfism An updaterdquo CurrentOpinion in Endocrinology Diabetes and Obesity vol 22 no 1pp 55ndash64 2015
[21] P Fortini C Ferretti and E Dogliotti ldquoThe response to DNAdamage during differentiation pathways and consequencesrdquoMutation ResearchmdashFundamental and Molecular Mechanismsof Mutagenesis vol 743-744 pp 160ndash168 2013
[22] B R Adams S E Golding R R Rao and K Valerie ldquoDynamicdependence on ATR and ATM for double-Strand break repairin human embryonic stem cells and neural descendantsrdquo PLoSONE vol 5 article e10001 no 4 2010
[23] A Klingseisen and A P Jackson ldquoMechanisms and pathways ofgrowth failure in primordial dwarfismrdquo Genes amp Developmentvol 25 no 19 pp 2011ndash2024 2011
[24] H Mokrani-Benhelli L Gaillard P Biasutto et al ldquoPrimaryMicrocephaly Impaired DNA Replication and Genomic Insta-bility Caused by Compound Heterozygous ATR MutationsrdquoHuman Mutation vol 34 no 2 pp 374ndash384 2013
[25] M OrsquoDriscoll A R Gennery J Seidel P Concannon and PA Jeggo ldquoAn overview of three new disorders associated withgenetic instability LIG4 syndrome RS-SCID and ATR-Seckelsyndromerdquo DNA Repair vol 3 no 8-9 pp 1227ndash1235 2004
[26] P Khetarpal S Das I Panigrahi and A Munshi ldquoPrimordialdwarfism overview of clinical and genetic aspectsrdquo MolecularGenetics and Genomics vol 291 no 1 pp 1ndash15 2016
[27] TOgi SWalker T Stiff et al ldquoIdentification of the First ATRIP-Deficient Patient and Novel Mutations in ATRDefine a ClinicalSpectrum for ATR-ATRIP Seckel Syndromerdquo PLoS Geneticsvol 8 no 11 Article ID e1002945 2012
[28] A Verloes S Drunat and P Gressens Primary autosomalrecessive microcephalies and Seckel syndrome spectrum disor-ders 2013
[29] A D Brown B W Sager A Gorthi S S Tonapi E J Brownand A J R Bishop ldquoATR suppresses endogenous DNA damageand allows completion of homologous recombination repairrdquoPLoS ONE vol 9 article e91222 no 3 2014
[30] E J Brown and D Baltimore ldquoEssential and dispensable rolesof ATR in cell cycle arrest and genome maintenancerdquo Genes ampDevelopment vol 17 no 5 pp 615ndash628 2003
[31] B Fitzgerald M OrsquoDriscoll K Chong S Keating and PShannon ldquoNeuropathology of fetal stage Seckel syndromeA case report providing a morphological correlate for theemerging molecular mechanismsrdquo Brain amp Development vol34 no 3 pp 238ndash243 2012
[32] L I Mullee and C G Morrison ldquoCentrosomes in the DNAdamage responsemdashthe hub outside the centrerdquo ChromosomeResearch vol 24 no 1 pp 35ndash51 2016
[33] K M Takikawa A Kikuchi A Yokoyama et al ldquoPerinatalfindings of Seckel syndrome A case report of a fetus showingprimordial dwarfism and severe microcephalyrdquo Fetal Diagnosisand Therapy vol 24 no 4 pp 405ndash408 2009
[34] Y Ruzankina C Pinzon-Guzman A Asare et al ldquoDeletion ofthe Developmentally Essential Gene ATR in Adult Mice Leadsto Age-Related Phenotypes and Stem Cell Lossrdquo Cell Stem Cellvol 1 no 1 pp 113ndash126 2007
[35] N E Mamrak A Shimamura and N G Howlett ldquoRecentdiscoveries in the molecular pathogenesis of the inherited bonemarrow failure syndrome Fanconi anemiardquo Blood Reviews vol31 no 3 pp 93ndash99 2017
[36] B P Alter ldquoDiagnosis Genetics and Management of InheritedBone Marrow Failure Syndromesrdquo International Journal ofHematology vol 2007 no 1 pp 29ndash39 2007
[37] L B Pontel I V Rosado G Burgos-Barragan et al ldquoEndoge-nous Formaldehyde Is a Hematopoietic Stem Cell Genotoxinand Metabolic Carcinogenrdquo Molecular Cell vol 60 no 1 pp177ndash188 2015
[38] G Pagano P Degan M DrsquoIschia et al ldquoOxidative stress asa multiple effector in Fanconi anaemia clinical phenotyperdquoEuropean Journal of Haematology vol 75 no 2 pp 93ndash1002005
[39] P FGiampietro P CVerlander J GDavis andADAuerbachldquoDiagnosis of Fanconi anemia in patients without congenitalmalformations An International Fanconi Anemia Registrystudyrdquo American Journal of Medical Genetics vol 68 no 1 pp58ndash61 1997
[40] P F Giampietro B Adler-Brecher P C Verlander S GPavlakis J G Davis and A D Auerbach ldquoThe need for moreaccurate and timely diagnosis in Fanconi anemia A report fromthe International Fanconi Anemia Registryrdquo Pediatrics vol 91no 6 pp 1116ndash1120 1993
[41] M P Wajnrajch J M Gertner Z Huma et al ldquoEvaluationof growth and hormonal status in patients referred to theinternational fanconi anemia registryrdquo Pediatrics vol 107 no4 I pp 744ndash754 2001
[42] N Giri D L Batista B P Alter and C A Stratakis ldquoEndocrineabnormalities in patients with fanconi anemiardquo The Journal ofClinical Endocrinology amp Metabolism vol 92 no 7 pp 2624ndash2631 2007
[43] S R Rose K C Myers M M Rutter et al ldquoEndocrine phe-notype of children and adults with Fanconi anemiardquo PediatricBlood amp Cancer vol 59 no 4 pp 690ndash696 2012
[44] A D Auerbach B Adler and R S K Chaganti ldquoPrenatal andpostnatal diagnosis and carrier detection of Fanconi anemia bya cytogeneticmethodrdquoPediatrics vol 67 no 1 pp 128ndash135 1981
[45] A D Auerbach M Sagi and B Adler ldquoFanconi anemiaPrenatal diagnosis in 30 fetuses at riskrdquo Pediatrics vol 76 no5 pp 794ndash800 1985
[46] L Faivre M F Portnoı G Pals et al ldquoShould chromosomebreakage studies be performed in patients with VACTERLassociationrdquo American Journal of Medical Genetics vol 137 no1 pp 55ndash58 2005
[47] B P Alter P S Rosenberg and L C Brody ldquoClinicaland molecular features associated with biallelic mutations inFANCD1BRCA2rdquo Journal ofMedical Genetics vol 44 no 1 pp1ndash9 2007
14 BioMed Research International
[48] K Myers S M Davies R E Harris et al ldquoThe clinicalphenotype of children with Fanconi anemia caused by biallelicFANCD1BRCA2mutationsrdquo Pediatric Blood amp Cancer vol 58no 3 pp 462ndash465 2012
[49] B G Yoon H N Kim U J Han et al ldquoLong-term follow-up of Fanconi anemia Clinical manifestation and treatmentoutcomerdquo Korean Journal of Pediatrics vol 57 no 3 pp 125ndash134 2014
[50] J G Hall ldquoReview and hypothesis Syndromes with severeintrauterine growth restriction and very short stature - Are theyrelated to the epigeneticmechanism(s) of fetal survival involvedin the developmental origins of adult health and diseaserdquoAmerican Journal of Medical Genetics Part A vol 152 no 2 pp512ndash527 2010
[51] A Petryk R K Shankar N Giri et al ldquoEndocrine disordersin Fanconi anemia Recommendations for screening and treat-mentrdquoThe Journal of Clinical Endocrinology ampMetabolism vol100 no 3 pp 803ndash811 2015
[52] S R RoseMM Rutter RMueller et al ldquoBonemineral densityis normal in children with Fanconi anemiardquo Pediatric Blood ampCancer vol 57 no 6 pp 1034ndash1038 2011
[53] A Petryk L E Polgreen J L Barnum et al ldquoBone mineraldensity in childrenwith fanconi anemia after hematopoietic celltransplantationrdquo Biology of Blood and Marrow Transplantationvol 21 no 5 pp 894ndash899 2015
[54] R Purkait A Mukherji S Datta and R Bhadra ldquoRenal arterystenosis An unusual etiology of hypertensive encephalopathyin a childwith fanconi anemiardquo Saudi Journal of KidneyDiseasesand Transplantation vol 26 no 4 pp 778ndash782 2015
[55] K H Chrzanowska H Gregorek B Dembowska-BaginskaM A Kalina and M Digweed ldquoNijmegen breakage syndrome(NBS)rdquoOrphanet Journal of Rare Diseases vol 7 article 13 2012
[56] L C Riches A M Lynch and N J Gooderham ldquoEarly eventsin the mammalian response to DNA double-strand breaksrdquoMutagenesis vol 23 no 5 pp 331ndash339 2008
[57] K Chrzanowska M Kalina H Rysiewski et al ldquoGrowthpattern in patients withNijmegen breakage syndrome evidencefroma longitudinal studyrdquoHormoneResearch in Paediatrics vol74 article S38 2010
[58] Group TINBSS ldquoNijmegen breakage syndromerdquo Archives ofDisease in Childhood vol 82 pp 400ndash406 2000
[59] M Digweed and K Sperling ldquoNijmegen breakage syndromeClinical manifestation of defective response to DNA double-strand breaksrdquo DNA Repair vol 3 no 8-9 pp 1207ndash1217 2004
[60] E Seemanova ldquoAn increased risk for malignant neoplasmsin heterozygotes for a syndrome of microcephaly normalintelligence growth retardation remarkable facies immun-odeficiency and chromosomal instabilityrdquo Mutation ResearchReviews in Genetic Toxicology vol 238 no 3 pp 321ndash324 1990
[61] K H Chrzanowska M Szarras-Czapnik M Gajdulewicz et alldquoHigh prevalence of primary ovarian insufficiency in girls andyoung women with Nijmegen breakage syndrome Evidencefrom a longitudinal studyrdquoThe Journal of Clinical Endocrinologyamp Metabolism vol 95 no 7 pp 3133ndash3140 2010
[62] C M R Weemaes T W J Hustinx J M J C Scheres P J JV Munster J A J M Bakkeren and R D F M Taalman ldquoAnew chromosomal instability disorder The nijmegen breakagesyndromerdquo Acta Paediatrica Scandinavica vol 70 no 4 pp557ndash564 1981
[63] A J Green J R W Yates A M R Taylor et al ldquoSevere micro-cephaly with normal intellectual development The Nijmegen
breakage syndromerdquo Archives of Disease in Childhood vol 73no 5 pp 431ndash434 1995
[64] D Gupta and A Nagarkar ldquoSpeech impairment in Nijmegenbreakage syndrome A rare anomalyrdquo International Journal ofPediatric Otorhinolaryngology vol 73 no 6 pp 873ndash875 2009
[65] P Muschke H Gola R Varon et al ldquoRetrospective diagnosisand subsequent prenatal diagnosis of Nijmegen breakage syn-dromerdquo Prenatal Diagnosis vol 24 no 2 pp 111ndash113 2004
[66] S Pasic M Cupic T Jovanovic S Djukic M Kavaric andI Lazarevic ldquoNijmegen breakage syndrome and chronic pol-yarthritisrdquo Italian Journal of Pediatrics vol 39 no 1 article no59 2013
[67] J P Patel J M Puck R Srinivasan et al ldquoNijmegen BreakageSyndrome Detected by Newborn Screening for T Cell ReceptorExcision Circles (TRECs)rdquo Journal of Clinical Immunology vol35 no 2 pp 227ndash233 2015
[68] I Demuth and M Digweed ldquoThe clinical manifestation of adefective response to DNA double-strand breaks as exemplifiedby Nijmegen breakage syndromerdquoOncogene vol 26 no 56 pp7792ndash7798 2007
[69] H Arora A H Chacon S Choudhary et al ldquoBloom syn-dromerdquo International Journal of Dermatology vol 53 no 7 pp798ndash802 2014
[70] C de Renty and N A Ellis ldquoBloomrsquos syndrome Why not pre-mature aging A comparison of the BLM andWRN helicasesrdquoAgeing Research Reviews vol 33 pp 36ndash51 2017
[71] C Keller K R Keller S B Shew and S E Plon ldquoGrowthdeficiency and malnutrition in Bloom syndromerdquo Journal ofPediatrics vol 134 no 4 pp 472ndash479 1999
[72] A Diaz M G Vogiatzi M M Sanz and J German ldquoEval-uation of short stature carbohydrate metabolism and otherendocrinopathies in Bloomrsquos syndromerdquo Hormone Researchvol 66 no 3 pp 111ndash117 2006
[73] C Ling J Huang Z Yan et al ldquoBloom syndrome complexpromotes FANCM recruitment to stalled replication forksand facilitates both repair and traverse of DNA interstrandcrosslinksrdquo Cell Discovery vol 2 article 16047 2016
[74] J S Renes R H Willemsen A Wagner M J J Finken and AC SHokken-Koelega ldquoBloom syndrome in short children bornsmall for gestational age A challenging diagnosisrdquoThe Journalof Clinical EndocrinologyampMetabolism vol 98 no 10 pp 3932ndash3938 2013
[75] M Maciejczyk B Mikoluc B Pietrucha et al ldquoOxidativestress mitochondrial abnormalities and antioxidant defense inAtaxia-telangiectasia Bloom syndrome andNijmegen breakagesyndromerdquo Redox Biology vol 11 pp 375ndash383 2017
[76] R M Brosh M Bellani Y Liu and M M Seidman ldquoFanconiAnemia A DNA repair disorder characterized by accelerateddecline of the hematopoietic stem cell compartment and otherfeatures of agingrdquo Ageing Research Reviews vol 33 pp 67ndash752017
[77] S Yan M Sorrell and Z Berman ldquoFunctional interplay be-tween ATMATR-mediated DNA damage response and DNArepair pathways in oxidative stressrdquo Cellular and Molecular LifeSciences vol 71 no 20 pp 3951ndash3967 2014
[78] L M M Nardozza A C R Caetano A C P Zamarian etal ldquoFetal growth restriction current knowledgerdquo Archives ofGynecology and Obstetrics vol 295 no 5 pp 1061ndash1077 2017
[79] M Tomas Vila J P Verdu M R Piera and C O AlonsoldquoNijmegen breakage syndrome phenotype a disorder to con-sider in the diagnosis ofmicrocephalyrdquoAnales De Pediatria vol74 pp 58ndash60 2011
Submit your manuscripts athttpswwwhindawicom
Stem CellsInternational
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
MEDIATORSINFLAMMATION
of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Behavioural Neurology
EndocrinologyInternational Journal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Disease Markers
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
BioMed Research International
OncologyJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Oxidative Medicine and Cellular Longevity
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
PPAR Research
The Scientific World JournalHindawi Publishing Corporation httpwwwhindawicom Volume 2014
Immunology ResearchHindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Journal of
ObesityJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Computational and Mathematical Methods in Medicine
OphthalmologyJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Diabetes ResearchJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Research and TreatmentAIDS
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Gastroenterology Research and Practice
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Parkinsonrsquos Disease
Evidence-Based Complementary and Alternative Medicine
Volume 2014Hindawi Publishing Corporationhttpwwwhindawicom

6 BioMed Research International
Figure 3 Seckel syndrome patient Note the severe microcephalyand the ldquobird-likerdquo appearance facies with micrognathia and reced-ing forehead The patient is severely disabled with no independentmarch
Moreover it appears that ATR and the other SS genes notonly participate in the DDR but also take part in the controlof centrosome maturation This engagement in centrosomebiology is also true for other DDR proteins like BRCA2biallelic mutations in its gene are responsible for a subgroupof Fanconi anemia patients [32]Theunifying feature betweenall Seckel patients irrespective of the molecular defect isthat their cells have an altered cell cycle progression thatis particularly evident during high rate cell division whenthere is hypersensitivity to replicative stress and centrosomaldysfunction This is especially important in cells with highdivision rates like the ones found in developmental stageswhere rapid replication is key [24 27]
SS is characterized by IUGR dwarfism microcephaly(below minus4 SD) mental retardation and some other anomalieslike luxation of the head of the radius scoliosis bone agedelay and seizures (Figure 3) The distinctive facial featuresinclude a prominent nose with micrognathia and a recedingforehead resulting in a ldquobird-like appearancerdquo [26 31 33]Since this syndrome has important clinical heterogeneityother anomalies have been reported including mandibularhypoplasia sternal abnormalities clinodactyly and low setears with hypoplastic lobules Although rare other reportedfeatures are moyamoya syndrome osteosarcoma and pol-yarteritis nodosa [26] Cerebral malformations like neuronalmigration abnormalities have been described but are notalways present [33] No glucose metabolism abnormalitieshave been reported
Dwarfism can be related to a reduction in the totalnumber of cells generated during development leading tohypoplastic tissue and reduced organism size [23] On theother handmicrocephalymay be related to an impairedDNAdamage response signal that could alter the cellular thresholdfor cell death resulting from DNA damage increasing thelevels of apoptosis during development developing neuronsare rapidly proliferating and potentially generate high levelsof oxidative damage which may lead to a higher level oflesions being faced at replication forks [23 25] Also analtered mitosis secondary to impaired spindle formationcould delay mitotic progression and increase the proportionof nonviable cell divisions Finally the stem cells may beaffected by abnormal centrosomal function Stems cells haveasymmetric divisions in order to preserve the characteristics
Figure 4 Fanconi anemia patient This six-year-old girl is 105 cmtall her height is just below the 5th percentile and her at-term birthweight is reported to be of 1900 gr Characteristic features of FA areevident skin hyperpigmentation bilateral radial defects consistingof bilateral thenar hypoplasia and absent fold of the right thumbwhich cannot be bent
of a stem cell and the centrosomes play an important role insuch divisions [23]
There is limited clinical information regarding age-related diseases in SS there is a void of prospective follow-up data from these patients that can only be obtained byfollowing a cohort of SS patients something that is apparentlynot being done at this time Nevertheless animal modelsbring some clues over the possibility of an aging phenotypein SS patients since ATR deficient adult mice show prematureage-related phenotypes as well as increased deterioration oftissue homeostasis [29 34]
72 Fanconi Anemia DNA interstrand crosslinks are ex-tremely noxious DNA lesions that affect central cellularprocesses like transcription and replication The FABRCApathway is responsible for the appropriate processing ofthese lesions protein products from at least 21 FANC genesparticipate in this pathway [35] The malfunction of any ofthose FANC proteins leads to the clinical phenotype knownas Fanconi anemia (FA) which is characterized by shortstature congenital malformations from the VACTERL-Hspectrum bone marrow failure and an increased suscepti-bility to cancer like acute myeloid leukemia epithelial headand neck cancer [36] (Figure 4) Most of the FA families bearbiallelic mutations in FANC genes that have an autosomicrecessive inheritance pattern only families with mutations inFANCB show an X-linked recessive pattern while those inwhich FANCR is the affected gene demonstrate an autosomicdominant one [35]
The FABRCA is an S-specific pathway that has 3 basicsteps it starts with the detection of the ICL by the proteinFANCM followed by the recruitment of the FA core com-plex that is responsible for the monoubiquitination of theFANCD2I heterodimer which in turn favors the recruit-ment of effector FANC-repair proteins that restore the DNAto its original form [35]
BioMed Research International 7
(a) (b)
Figure 5 Chromosomal instability induced by 40 ngml mitomycin C (a) Lymphocytes from a healthy individual (b) lymphocytes from aFA patient Short arrows show chromosomal breaks the long arrow shows a quadriradial figure Note the exacerbated chromosome instabilityfound in the FA patient
The cellular phenotype of FA derived cells is extremelyconstant An aberrant FABRCA pathway can result inunrepaired DSBs that manifest as chromosomal breaks orabnormal repair by an error-prone repair pathway that resultsin radial figures These alterations are cytogenetic evidenceof chromosomal instability which is the hallmark of FA cellsand is exploited for clinical diagnostic purposes (Figure 5)The agents capable of inducing this chromosomal instabilityare from endogenous origin like aldehydes [37] and reactivespecies of oxygen (ROS) [38] as well as exogenous sourceslike bifunctional alkylating agents (diepoxybutane or mito-mycin C) In addition FA cells have accumulation of cells inG2 phase of the cell cycle resulting from a functional G2Mcheckpoint and a proapoptotic phenotype
In contrast with the cellular FA phenotype the clinicalpicture in FA patients is extremely variable not every patientwill have all the manifestations one-third of patients do nothave congenital malformations [39] while almost 90 willdevelop bone marrow failure [36] One of the more constantmanifestations in FApatients is growth parameters alterationAn analysis from the international Fanconi anemia registry(IFAR) data showed that over 60 of FA patients presentedshort stature (below the 5th percentile) while birth lengthandweight below the 5th percentile was respectively reportedin almost 30 and nearly half of FA patients [40]Moreover aprospective study of data from 54 IFAR participants showedthat the mean standard deviation score (SDS) for height inthese patients was significantly below normal for age and sexat minus235 plusmn 028 meanwhile mean SDS for weight was betteralthough below normal (minus126 plusmn 024) In this study perinatalgrowth data was not reported [41]
Other than the IFAR data on growth there are anothertwo studies that analyze growth parameters of FA patientsAnthropometric measurements from 45 patients with Fan-coni anemia from the National Cancer Institutersquos inher-ited bone marrow failure syndromes (IBMFS) cohort wereassessed This cohort had a mean SDS for height of minus21 plusmn
189 The height of over half of the participants (54) wascategorized as short (SDS gt 20 SD) in this subset of patientsthe mean SDS for height was minus38 plusmn 15 [42] Finally theevaluation of 120 FA patients from the FA ComprehensiveCare Clinic of Cincinnati Childrenrsquos Hospital Medical Centerrevealed that median height SDS was shorter than expectedin children and adults irrespective of gender Furthermorethis study presented birth information from 70 patients (59children and 11 adults) from the cohort 51 of the childrenand 3 adults were born small for gestational age their medianbirth weight at term was 202 kg (range 15ndash26 kg) [43] Theintrauterine growth restriction seen in FA patients has alsobeen documented in several case reports in which at-termbirth weight ranges from 1780 to 3200 gr [44ndash49] Eventhough growth abnormalities have been identified in FApatients with mutations in almost every FANC gene it hasbeen shown that patientswithmutations in certain genes havea more severe growth delay That is the case for patients withbiallelic mutations in FANCD1 [47 48] as well as those whobear mutations in FANCC for whom an SDS for height ofminus384 has been found [41]
Endocrine abnormalities have been proven to be aninherent part of the FA phenotype up to 80 of patientshave one or more endocrine abnormalities Besides growththyroid function and glucose homeostasis are frequentlyaffected [40ndash43] Considering the existing evidence for arelationship between low birth weight and an increased riskfor noncommunicable adult diseases like diabetes hyperten-sion heart disease dyslipidemia and osteoporosis [50] it isrelevant to revise these diseases in FA The FA cohorts inwhom growth was assessed were also evaluated for endocrinestatus Glucose homeostasis is affected in a large portion ofFA patients impaired glucose tolerance has been found in27ndash68 of them whereas diabetes has a prevalence of 8ndash10Dyslipidemia has been assessed in only a small portionof FA patients but it has been found in 17ndash55 of theevaluated subjects [51]There are conflicting results over bone
8 BioMed Research International
mineral density (BMD) status in FA the first time this wasevaluated 92 of the patients were found to have osteopeniaor osteoporosis [42] nevertheless a study that evaluated alarger FA cohort found that lowBMD is not a frequent finding[52] Further research on this topic has raised the questionof whether BMD deficit is intrinsic to the FA phenotype ora consequence of hematopoietic cell transplantation (HCT)an interrogation that is still awaiting to be answered [53]Cardiovascular adult diseases are not relevant in the FA phe-notype heart disease in these patients is from the congenitaltype as 13of patients have cardiacmalformations [40] whilehypertension has only been reported in two patients as theresult of renal malformations [54]
Findings from the different FA cohorts show that shortstature is an inherent feature of the FA phenotype thisfeature does not respond to a single explanation the apoptosisprone FA cellular phenotype is certainly a contributing factorfor this The fact that FA patients have a constitutionallydefective pathway since conception could explain the clinicalphenotype of RCIU Short stature may also be exacerbated byaccompanying endocrinopathies The cooccurrence of manyendocrine alterations has encouraged unifying explanationssome have proposed that endocrinopathies are secondaryto increased cytokine activity found in FA cells [41] whileothers favor the view that some endocrine secretory cellsmight be damaged by high levels of reactive oxygen specieswhich are known to be elevated in FA patients [43] In linewith the developmental origin of adult health and diseasetheory it could also be possible that the increased prevalenceof glucose homeostasis alterations and dyslipidemia reportedin FA patients is a consequence of intrauterine growthrestriction of these patients Nevertheless the attemptedgenotype-phenotype correlation of the endocrine phenotypein FA patients does not seem to support that Patients withmutations in FANCA show a mild endocrine phenotype inwhich height is not severely affected and insulin resistanceis mild whereas mutations in FANCC which are relatedto shorter stature have the least insulin resistance [41]Moreover no direct relationship between birth weight andglucose tolerance was identified when it was intentionallylooked for [43] although the number of patients in whichthese observations were made is limited
73 Nijmegen Breakage Syndrome Nijmegen breakage syn-drome (NBS) is an autosomal recessive disease caused bybiallelic mutations in NBN a gene that encodes nibrin aprotein involved in DNA repair and cell cycle checkpointregulation It participates in the former by sensing double-strand breaks as part of the trimeric complexMRN alongsideMRE11 andRAD50Meanwhile for the latter it contributes tothe appropriate activation of ATM andATRwhich are centraltransductors of the DNA damage response (DDR) [55] Themalfunction of nibrin translates in a cellular phenotypemarked by chromosomal instability radiosensitivity reducedphosphorylation of ATM substrates and S and G2M cellcycle defects [56] Chromosome instability is evidenced bycytogenetic methods in 10ndash60 of cells in the form of breaksand numeric and structural aberrations translocations andinversions affecting chromosomes 7 and 14 are found in the
147
Figure 6 Translocation between chromosomes 7 and 14 is typicalin NBS patientsrsquo cells
majority of NBS patients and are considered a cytogeneticcharacteristic of this syndrome (Figure 6) [57]
The clinical impact of these alterations is a phenotypecharacterized by microcephaly a distinctive facial appear-ance consisting of receding forehead and mandible and aprominent mid face with a long nose and philtrum aswell as immunodeficiency that leads to recurrent infectionsand an increased risk for the development of neoplasiaparticularly leukemia and lymphoma According to theinternational Nijmegen breakage syndrome study groupgrowth retardation is also a hallmark of this disease [58]although there is not many details about this feature in theliterature
Most of the information on the natural history of NBSavailable today comes from patients participating in reg-istries in which fairly large cohorts of NBS patients areincluded There is a large representation of Slavic patientsin these cohorts which correlates with the high carrierfrequency of a founder mutation of NBN in this populationFrom these studies it is evident that the most severelyaffected anthropometric measure in NBS patients is headcircumference since all participants display microcephalyeven though only 75 display this feature at birth Whenit comes to growth parameters the same study states thatall patients have growth retardation which is described asproportionate and early occurring [58] although the specifictemporality is not defined A posterior report points out thatthe growth retardation seen in most NBS patients locatesthem in the 10th percentile in growth charts and that birthheight and weight are usually within normal parameters [59]Nevertheless there are other authors who report prenataland postnatal growth retardation [55 60] and a tendency forshort stature that is more evident during the first year of life[61] Also several case reports of NBS patients in which birthweight is informed demonstrate prenatal growth restriction[62ndash67] although this could represent a report bias Themore comprehensive data analysis on growth that includesperinatal information of NBS patients is the one that analyzesdata from 67 patients followed for 15 years Eighty percentof these patients were born at term the girls were found tohave a mean birth weight of 27 kg and mean birth heightof 514 cm while boys were reported to have a mean birthweight of 28 kg and mean birth height of 523 cm Moreoverall patients irrespective of gender were found to have ameanheight reduced by over 2 SDS at one year old [57] These data
BioMed Research International 9
(a) (b)
Figure 7 Sister chromatid exchange in cells from a healthy individual (a) and from a BLM patient (b)
support the fact that growth retardation in NBS is a prenatalphenomenon
Nibrin has been found to have essential functions inthe regulation of the cell cycle which translates into anabsolute need for this protein for cell proliferation [68]It would seem logical that mutations of the NBN genethat compromise the appropriate function of nibrin wouldlead to abnormal growth when thought from an organismperspective Mechanistically speaking poor cellular growthcaused by mutations in a particular gene can be thought ofas the main explanation for the growth restricted phenotypebut it has been shown that mutations in other DDR genesthat share the cellular phenotype of poor growth like ATMdo not replicate the compromised growth phenotype atthe organism level growth retardation is absent in ataxiatelangiectasia (AT)This data suggests that there are certainlyother contributing factors to the abnormal growth phenotypeseen in NBS patients [58]
74 Bloom Syndrome Bloom syndrome (BS) is an autosomalrecessive disorder caused by homozygous or compoundheterozygous mutations in the BLM gene (15q261) thatencodes the RecQL3 helicase BLM has a critical role inthe maintenance of genome stability acting at the interfacebetweenDNAreplication recombination and repair [69 70]To date over sixty different mutations including nonsenseand missense have been identified all of them result inthe inactivation of BLM and the consequent loss of itshelicase activity The BLM gene encodes a 1417 amino acidnuclear protein its expression peaks during the S and G
2M
phases of the cell cycle which is consistent with its rolein DNA replication and recombination BLM specificallyunwinds structures like forked DNA duplexes RNA-DNAheteroduplexes and R-Loops which explains its importanceduring replication fork progression and transcription besidesit is central for Holliday Junctions (HJs) dissolution forHR The dissolution of HJs by the topoisomerase III120572-BLMcomplex cannot be replaced by any other RecQ helicase inthe family [69 70] It has also been found to have a role in
the annealing activity of the ssDNA the proper sister chro-matid segregation during mitosis and telomere maintenance[70]
BLM can have both pro- and antirecombinogenic func-tions that are regulated by posttranslational modificationsincluding phosphorylation sumoylation and ubiquitination[70]
BLM also enables sister chromatid segregation by pro-cessing unresolved replication intermediates that manifest inmitosis as ultrafine DNA bridges (UFBs) and together withtopoisomerase III120572 RMI1 and RMI2 localizes to UFBs inanaphase BML deficient cells exhibit and increase frequencyof UFBs suggesting a role of BLM in the resolution ofthese structures Failure to resolve these UFBs leads to DNAbreakage as mitosis proceeds [70]
Therefore BS cells are characterized by an increasein chromosomal aberrations including chromatid gapsand breaks telomere associations and quadriradial chro-mosomes resulting from unsolved recombination betweenhomologous chromosomes BS cells exhibit increased muta-tion rates and the genomic instability includes elevatedmitotic HR and unequal sister chromatid exchange (SCEs)(Figure 7) Perhaps the most characteristic feature is the overtenfold increase in SCEs which results from crossover eventsduring HR repair of damage replication forks [50 69 70]
Clinically the more striking BS feature is IUGR averagebirth weight at term is 1850 g and birth length is 44 cmFor both boys and girls weight and length in BS are morethan two standard deviations below normal indicating thatgrowth retardation has a prenatal origin At postnatal agesheight remains below the normal range and is accompaniedby a paucity of subcutaneous fat Average adult height inmales has been found to be 148 cm (130ndash162 cm) whilein females it has been reported to be 139 cm (122ndash151 cm)[50 70 71]
BS patients have overall proportionated short staturebut the head is reported to be small and narrow relativelyto the body size it is described as mild microcephalyand is accompanied by malar hypoplasia Patients have
10 BioMed Research International
Figure 8 Bloomsyndromepatient inwhom the characteristicmalarerythema is present
been described to have a high pitched voice [50 70] Theskin appears normal at birth but in the first or secondyear of life in response to sun exposure children developan erythematous rash with a butterfly distribution in themalar area and the back of hands and feet The rash caninclude telangiectasia The severity varies between patientssome can even lose their eyelashes and develop blisteringaround the mouth The presence of cafe-au-lait spots andhypopigmented areas of skin associated with contiguoushyperpigmented areas is common (Figure 8) Intellectualabilitiesmay be limited in some patients and normal in others[50 70]
Other clinical conditions reported in BS patients are gas-troesophageal reflux and diarrhea in infants mild immuno-logical deficiency with frequent episodes of otitis mediaazoospermia or severe oligospermia in males and prema-ture cessation of menstruation in females minor anatomicdefects and increased risk for neoplasia which is the maincause of dead in BS [70] Another common medical con-dition in BS is diabetes mellitus associated with impairedglucose tolerance and insulin resistance it has been reportedin up to 16 of patients [70] According to data fromthe Bloomrsquos Syndrome Registry diabetes in these patientstends to begin early with a mean age at diagnosis of 266years It is not associated with ketosis and it does nothave the classical hereditary pattern seen in type 2 diabetes[50 72]
Short stature in BS is not due to hormonal causes sincethe size of cells in persons with BS is normal it has beenhypothesized that there are fewer of them due to either adecrease in the cell division rate an increase in apoptosis oreven a combination of both BS cells have troublemeeting thedemands of fast cell divisions encountered in tissues duringembryonic development The leading hypothesis suggeststhat problems arising during DNA synthesis require a longerS phase to overcome the challenge which translates intoslowing of the cell division rate and an increase in apoptosis[70]
8 Concluding Remarks
This review has focused on discussing phenotypes of CISin which there is a prenatal alteration of growth The foursyndromes discussed here are rare diseases whose prevalenceis difficult to calculate since appropriate identification anddiagnosis of affected individuals among the general popula-tion are not straightforward It is important to note that theavailable information on the natural history of FA NBS andBS comes from the analysis of several patients that participatein registries This strategy results in detailed informationthat permits a better analysis of the clinical phenotype ofthese rare diseases Meanwhile available data of SS is moreanecdotic which results in a nonsystematic gathering ofinformation which is thus frequently incomplete
From the available clinical data of these CIS it is evidentthat growth is not affected in the same extent for all ofthese syndromes the phenotypes that exhibit a more severelystagnated perinatal growth are BS and SS The severe growthdelay reported in these patients has been described as apathognomonic sign of these diagnoses In patients withFA perinatal growth can also be severely affected but notevery FA patient shows this manifestation Finally NBShas been described to have growth retardation of prenatalorigin of mild severity almost within the lower normal range(Figure 9) The cephalic circumference can be affected in allof these syndromes severe microcephaly is pathognomonicin SS and NBS it is described as mild for BS patients and it isfound in less than half of FA patients (Table 2)
When trying to understand why a subset of CIS showsprenatal growth retardation it could be alleged that theintrinsic chromosomal instability is responsible for it Butthis would not explain why prenatal growth retardation isnot a universal CIS feature for example ataxia telangiectasiapatients who have biallelic mutations in the ATMkinase genedo not show prenatal growth delay It strikes that a molecularcommon feature shared by the prenatal growth retardationSIC phenotypes is that they are caused by mutations ingenes that are necessary for an appropriate response to DSBsduring the S phase of the cell cycle The molecular defectin SS affects the functioning of ATR the preferred DDRtransducing kinase used by highly replicating ESCs TheFABRCA pathway which is affected in patients with FAdetects ICLs upon replication fork arrest Nibrin the proteinaffected in patients with NBS is induced during S phasefor the detection of DSBs And the BS helicase forms aFANCM-BLM complex needed to sense ICLs during S phase[73] It could then be argued that altered DNA replicationis an important factor for the development of intrauterinegrowth restriction in these CIS Nevertheless it must be keptin mind that the inherent chromosome instability found inthese syndromes may also be affecting normal growth in thepatients [27 43 57 60 71]
Being small for gestational age has been associatedwith a higher risk of noncommunicable adult diseases likeglucose homeostasis disorders dyslipidemia hypertensionand others It has been proposed that fetal reprogrammingto enhance fetal survival despite the risk for adult onsetdiseases is an outcome that does not take into account
BioMed Research International 11
Table 2 Growth features of chromosomal instability syndromes
SyndromeldquoLocirdquo At-term birth weightheight Microcephaly Adult height Adult onset diseases
Seckel SyndromeldquoATR3q23rdquo
Birth weight below minus3 SD(2055 g)
Severeminus4 SD
Postnatal growth retardation(below minus5 SD) Not reported
Fanconi anemialdquo21 FANC genesrdquo
Median weight 202 kg(15ndash26 kg) In 20ndash50
50ndash60 of patients with medianheight lt minus18 SDSWomen minus34 SDSMen minus44 SDS
CancerDiabetes mellitusDyslipidemia
Altered bone mineral densityNijmegen BreakageSyndromeldquoNBN8q21rdquo
Mean weightheight girls27 kg514 cm
Mean weightheight boys28 kg523 cm
100 Mean height for women minus18 SDSMean height for men minus23 Cancer
Bloom SyndromeldquoBLM15q261rdquo
Mean weight 189 kg plusmn 035 kg forboys
Mean weight 187 kg plusmn 035 kg forgirls
Mean height 434 cm plusmn 44 cm forboys
Mean height 438 cm plusmn 28 cm forgirls
Mildmicrocephaly
Mean height 1455 cm plusmn 76 cmmales
Mean height 1415 cm plusmn 61 cm forfemales
CancerDiabetes mellitus
See [27 33 40 43 50 57 69]
45 53
43245
Height (cm)
Weight (kg)
Percentile 3 Percentile 97Percentile 50495
33
Normalindividual
Mean 2055
SeckelSyndrome
2615Median 202
FanconiAnemia
Mean 51
Mean 275
Nijmegen BreakageSyndrome
38 49
24513
Mean 436
Mean 188
BloomSyndrome
Figure 9 Anthropometric features at birth of chromosome instability syndromes with perinatal growth retardation Comparison of theavailable growth data from SS FA NBS and BS syndrome against birth data from the WHOrsquos growth standards for infants Although meanheight and weight values of NBS patients are found to be within normal percentiles according to WHO standards there are several authorswho refer to prenatal growth restriction [55 63 65 79]
the reason for the prenatal growth restraint [50 72 74] Itmust be kept in mind that noncommunicable diseases aremultifactorial entities in which genetic and environmentalfactors converge and their cause cannot be attributed to asingle explanation However when growth restriction is akey feature in syndromes with chromosome instability the
possibility that cell hypoplasia due to DNA repair malfunc-tion is contributing to the growth restriction phenotypemustbe contemplated Moreover since none of these adult onsetdiseases is reported as an inherent element of the SS and NBSphenotypes the direct connection between low birth weightand adult noncommunicable diseases is less of a straight
12 BioMed Research International
shot Furthermore there are other Mendelian syndromeswith mutations in DNA repair genes that characteristicallyshow adult noncommunicable diseases but do not haveIUGR such is the case for Werner syndrome a progeroiddisease caused by biallelic mutations in another RecQ heli-case (RecQ4) that clinically presents with postnatal shortstature and a prevalence of type 2 diabetes mellitus of 70[50 70 74]
Natural history of FA NBS and BS documented throughthe existing patient registries has allowed the identificationof noncommunicable diseases to be a part of the clinicalspectrum of these syndromes (Table 2) Meanwhile from theinformation available through SS case reports no adult onsetdisease has been found to be part of this phenotype To thebest of our knowledge the direct investigation of nonevidentendocrinologic alterations like glucose homeostasis or dys-lipidemia has not been directlymade in SS patients For a raredisease like SS such a study can only be done if a fairly largegroup of patients like the one found in registries is availableIf such a study was to be performed hidden features in SSpatients could be unraveled
Oxidative stress sensibility is a cellular feature sharedby all the SIC syndromes with IUGR that could contributeto the explanation of the premature development of non-communicable adult diseases in these patients Reports haveshown that BS and NBS cells have endogenous reactiveoxygen species (ROS) overproduction and an impairedmitochondrial homeostasis [75] it is also well known thatFA cells show increased levels of oxidative damage [3876] and there is evidence that oxidative stress can activateATR-mediated checkpoint signaling [77] Since this kind ofdamage has soundly been related to age-associated diseasesthat result from tissue degeneration exacerbated oxidativedamage found in these syndromes could result in cellu-lar aging that manifests as overall premature aging withparticular symptoms like glucose homeostasis alterations[76 77]
Fetal growth restriction is a multifactorial conditionwhere wide arrays of factors converge Fetal aspects inparticular those affecting the genetic constitution of thefetus have been recognized to play an important role Ithas been demonstrated that chromosomal abnormalities andmonogenic syndromes caused by mutations in genes thatparticipate in growth or metabolic pathways directly affectfetal growth [78] Even though they are rare entities CISappear as another group of monogenic pathologies thatbroaden the list of genetic fetal factors of fetal growthrestriction
Consent
The necessary consent for the publication of the photographswas obtained
Conflicts of Interest
The authors declare that there are no conflicts of interestregarding the publication of this paper
Authorsrsquo Contributions
The three authors contributed equally andwrote the first draftof the paper The final version was approved by everyone
Acknowledgments
This paper is supported by SEP-CONACYT Project 243102Benilde Garcıa-de Teresa received the 574025 scholarshipfrom CONACYT The paper is also supported by PAPIIT-UNAM Project IA202615 and Fondos Federales INP Project41-2014
References
[1] K W J Derks J H J Hoeijmakers and J Pothof ldquoThe DNAdamage response The omics era and its impactrdquo DNA Repairvol 19 pp 214ndash220 2014
[2] S P Jackson and J Bartek ldquoThe DNA-damage response inhuman biology and diseaserdquoNature vol 461 no 7267 pp 1071ndash1078 2009
[3] J H J Hoeijmakers ldquoDNA damage aging and cancerrdquo TheNew England Journal of Medicine vol 361 no 15 pp 1475ndash14852009
[4] G Spivak ldquoNucleotide excision repair in humansrdquoDNARepairvol 36 pp 13ndash18 2015
[5] J Vijg XDong BMilholland andL Zhang ldquoGenome instabil-ity a conserved mechanism of ageingrdquo Essays in Biochemistryvol 61 no 3 pp 305ndash315 2017
[6] J I Garaycoechea and K J Patel ldquoWhy does the bone marrowfail in Fanconi anemiardquo Blood vol 123 no 1 pp 26ndash34 2014
[7] R Ceccaldi B Rondinelli andAD DrsquoAndrea ldquoRepair PathwayChoices andConsequences at theDouble-Strand BreakrdquoTrendsin Cell Biology vol 26 no 1 pp 52ndash64 2016
[8] R Biehs M Steinlage O Barton et al ldquoDNA Double-StrandBreak Resection Occurs during Non-homologous End Joiningin G1 but Is Distinct from Resection during HomologousRecombinationrdquo Molecular Cell vol 65 no 4 pp 671ndash684e52017
[9] A Ciccia and S J Elledge ldquoTheDNAdamage response makingit safe to play with knivesrdquoMolecular Cell vol 40 no 2 pp 179ndash204 2010
[10] L H Pearl A C Schierz S E Ward B Al-Lazikani and F MG Pearl ldquoTherapeutic opportunities within the DNA damageresponserdquo Nature Reviews Cancer vol 15 no 3 pp 166ndash1802015
[11] S-F Yang C-W Chang R-J Wei Y-L Shiue S-N Wang andY-T Yeh ldquoInvolvement of DNA damage response pathways inhepatocellular carcinomardquo BioMed Research International vol2014 Article ID 153867 2014
[12] M He W Zhou C Li and M Guo ldquoMicroRNAs DNAdamage response and cancer treatmentrdquo International Journalof Molecular Sciences vol 17 no 12 article no 2087 2016
[13] K A Cimprich and D Cortez ldquoATR an essential regulator ofgenome integrityrdquo Nature Reviews Molecular Cell Biology vol9 no 8 pp 616ndash627 2008
[14] B M Sirbu and D Cortez ldquoDNA damage response three levelsof DNA repair regulationrdquo Cold Spring Harbor Perspectives inBiology vol 5 article a012724 no 8 2013
BioMed Research International 13
[15] C Beck I Robert B Reina-San-Martin V Schreiber andF Dantzer ldquoPoly(ADP-ribose) polymerases in double-strandbreak repair focus on PARP1 PARP2 and PARP3rdquo Experimen-tal Cell Research vol 329 no 1 pp 18ndash25 2014
[16] D W Meek ldquoTumour suppression by p53 a role for the DNAdamage responserdquo Nature Reviews Cancer vol 9 no 10 pp714ndash723 2009
[17] A Rodrıguez L Torres U Juarez et al ldquoFanconi anemiacells with unrepaired DNA damage activate components of thecheckpoint recovery processrdquo Theoretical Biology and MedicalModelling vol 12 no 1 article 11 2015
[18] H Wang X Zhang L Teng and R J Legerski ldquoDNA damagecheckpoint recovery and cancer developmentrdquo ExperimentalCell Research vol 334 no 2 pp 350ndash358 2015
[19] P A Jeggo L H Pearl and A M Carr ldquoDNA repair genomestability and cancer A historical perspectiverdquo Nature ReviewsCancer vol 16 no 1 pp 35ndash42 2016
[20] F S Alkuraya ldquoPrimordial dwarfism An updaterdquo CurrentOpinion in Endocrinology Diabetes and Obesity vol 22 no 1pp 55ndash64 2015
[21] P Fortini C Ferretti and E Dogliotti ldquoThe response to DNAdamage during differentiation pathways and consequencesrdquoMutation ResearchmdashFundamental and Molecular Mechanismsof Mutagenesis vol 743-744 pp 160ndash168 2013
[22] B R Adams S E Golding R R Rao and K Valerie ldquoDynamicdependence on ATR and ATM for double-Strand break repairin human embryonic stem cells and neural descendantsrdquo PLoSONE vol 5 article e10001 no 4 2010
[23] A Klingseisen and A P Jackson ldquoMechanisms and pathways ofgrowth failure in primordial dwarfismrdquo Genes amp Developmentvol 25 no 19 pp 2011ndash2024 2011
[24] H Mokrani-Benhelli L Gaillard P Biasutto et al ldquoPrimaryMicrocephaly Impaired DNA Replication and Genomic Insta-bility Caused by Compound Heterozygous ATR MutationsrdquoHuman Mutation vol 34 no 2 pp 374ndash384 2013
[25] M OrsquoDriscoll A R Gennery J Seidel P Concannon and PA Jeggo ldquoAn overview of three new disorders associated withgenetic instability LIG4 syndrome RS-SCID and ATR-Seckelsyndromerdquo DNA Repair vol 3 no 8-9 pp 1227ndash1235 2004
[26] P Khetarpal S Das I Panigrahi and A Munshi ldquoPrimordialdwarfism overview of clinical and genetic aspectsrdquo MolecularGenetics and Genomics vol 291 no 1 pp 1ndash15 2016
[27] TOgi SWalker T Stiff et al ldquoIdentification of the First ATRIP-Deficient Patient and Novel Mutations in ATRDefine a ClinicalSpectrum for ATR-ATRIP Seckel Syndromerdquo PLoS Geneticsvol 8 no 11 Article ID e1002945 2012
[28] A Verloes S Drunat and P Gressens Primary autosomalrecessive microcephalies and Seckel syndrome spectrum disor-ders 2013
[29] A D Brown B W Sager A Gorthi S S Tonapi E J Brownand A J R Bishop ldquoATR suppresses endogenous DNA damageand allows completion of homologous recombination repairrdquoPLoS ONE vol 9 article e91222 no 3 2014
[30] E J Brown and D Baltimore ldquoEssential and dispensable rolesof ATR in cell cycle arrest and genome maintenancerdquo Genes ampDevelopment vol 17 no 5 pp 615ndash628 2003
[31] B Fitzgerald M OrsquoDriscoll K Chong S Keating and PShannon ldquoNeuropathology of fetal stage Seckel syndromeA case report providing a morphological correlate for theemerging molecular mechanismsrdquo Brain amp Development vol34 no 3 pp 238ndash243 2012
[32] L I Mullee and C G Morrison ldquoCentrosomes in the DNAdamage responsemdashthe hub outside the centrerdquo ChromosomeResearch vol 24 no 1 pp 35ndash51 2016
[33] K M Takikawa A Kikuchi A Yokoyama et al ldquoPerinatalfindings of Seckel syndrome A case report of a fetus showingprimordial dwarfism and severe microcephalyrdquo Fetal Diagnosisand Therapy vol 24 no 4 pp 405ndash408 2009
[34] Y Ruzankina C Pinzon-Guzman A Asare et al ldquoDeletion ofthe Developmentally Essential Gene ATR in Adult Mice Leadsto Age-Related Phenotypes and Stem Cell Lossrdquo Cell Stem Cellvol 1 no 1 pp 113ndash126 2007
[35] N E Mamrak A Shimamura and N G Howlett ldquoRecentdiscoveries in the molecular pathogenesis of the inherited bonemarrow failure syndrome Fanconi anemiardquo Blood Reviews vol31 no 3 pp 93ndash99 2017
[36] B P Alter ldquoDiagnosis Genetics and Management of InheritedBone Marrow Failure Syndromesrdquo International Journal ofHematology vol 2007 no 1 pp 29ndash39 2007
[37] L B Pontel I V Rosado G Burgos-Barragan et al ldquoEndoge-nous Formaldehyde Is a Hematopoietic Stem Cell Genotoxinand Metabolic Carcinogenrdquo Molecular Cell vol 60 no 1 pp177ndash188 2015
[38] G Pagano P Degan M DrsquoIschia et al ldquoOxidative stress asa multiple effector in Fanconi anaemia clinical phenotyperdquoEuropean Journal of Haematology vol 75 no 2 pp 93ndash1002005
[39] P FGiampietro P CVerlander J GDavis andADAuerbachldquoDiagnosis of Fanconi anemia in patients without congenitalmalformations An International Fanconi Anemia Registrystudyrdquo American Journal of Medical Genetics vol 68 no 1 pp58ndash61 1997
[40] P F Giampietro B Adler-Brecher P C Verlander S GPavlakis J G Davis and A D Auerbach ldquoThe need for moreaccurate and timely diagnosis in Fanconi anemia A report fromthe International Fanconi Anemia Registryrdquo Pediatrics vol 91no 6 pp 1116ndash1120 1993
[41] M P Wajnrajch J M Gertner Z Huma et al ldquoEvaluationof growth and hormonal status in patients referred to theinternational fanconi anemia registryrdquo Pediatrics vol 107 no4 I pp 744ndash754 2001
[42] N Giri D L Batista B P Alter and C A Stratakis ldquoEndocrineabnormalities in patients with fanconi anemiardquo The Journal ofClinical Endocrinology amp Metabolism vol 92 no 7 pp 2624ndash2631 2007
[43] S R Rose K C Myers M M Rutter et al ldquoEndocrine phe-notype of children and adults with Fanconi anemiardquo PediatricBlood amp Cancer vol 59 no 4 pp 690ndash696 2012
[44] A D Auerbach B Adler and R S K Chaganti ldquoPrenatal andpostnatal diagnosis and carrier detection of Fanconi anemia bya cytogeneticmethodrdquoPediatrics vol 67 no 1 pp 128ndash135 1981
[45] A D Auerbach M Sagi and B Adler ldquoFanconi anemiaPrenatal diagnosis in 30 fetuses at riskrdquo Pediatrics vol 76 no5 pp 794ndash800 1985
[46] L Faivre M F Portnoı G Pals et al ldquoShould chromosomebreakage studies be performed in patients with VACTERLassociationrdquo American Journal of Medical Genetics vol 137 no1 pp 55ndash58 2005
[47] B P Alter P S Rosenberg and L C Brody ldquoClinicaland molecular features associated with biallelic mutations inFANCD1BRCA2rdquo Journal ofMedical Genetics vol 44 no 1 pp1ndash9 2007
14 BioMed Research International
[48] K Myers S M Davies R E Harris et al ldquoThe clinicalphenotype of children with Fanconi anemia caused by biallelicFANCD1BRCA2mutationsrdquo Pediatric Blood amp Cancer vol 58no 3 pp 462ndash465 2012
[49] B G Yoon H N Kim U J Han et al ldquoLong-term follow-up of Fanconi anemia Clinical manifestation and treatmentoutcomerdquo Korean Journal of Pediatrics vol 57 no 3 pp 125ndash134 2014
[50] J G Hall ldquoReview and hypothesis Syndromes with severeintrauterine growth restriction and very short stature - Are theyrelated to the epigeneticmechanism(s) of fetal survival involvedin the developmental origins of adult health and diseaserdquoAmerican Journal of Medical Genetics Part A vol 152 no 2 pp512ndash527 2010
[51] A Petryk R K Shankar N Giri et al ldquoEndocrine disordersin Fanconi anemia Recommendations for screening and treat-mentrdquoThe Journal of Clinical Endocrinology ampMetabolism vol100 no 3 pp 803ndash811 2015
[52] S R RoseMM Rutter RMueller et al ldquoBonemineral densityis normal in children with Fanconi anemiardquo Pediatric Blood ampCancer vol 57 no 6 pp 1034ndash1038 2011
[53] A Petryk L E Polgreen J L Barnum et al ldquoBone mineraldensity in childrenwith fanconi anemia after hematopoietic celltransplantationrdquo Biology of Blood and Marrow Transplantationvol 21 no 5 pp 894ndash899 2015
[54] R Purkait A Mukherji S Datta and R Bhadra ldquoRenal arterystenosis An unusual etiology of hypertensive encephalopathyin a childwith fanconi anemiardquo Saudi Journal of KidneyDiseasesand Transplantation vol 26 no 4 pp 778ndash782 2015
[55] K H Chrzanowska H Gregorek B Dembowska-BaginskaM A Kalina and M Digweed ldquoNijmegen breakage syndrome(NBS)rdquoOrphanet Journal of Rare Diseases vol 7 article 13 2012
[56] L C Riches A M Lynch and N J Gooderham ldquoEarly eventsin the mammalian response to DNA double-strand breaksrdquoMutagenesis vol 23 no 5 pp 331ndash339 2008
[57] K Chrzanowska M Kalina H Rysiewski et al ldquoGrowthpattern in patients withNijmegen breakage syndrome evidencefroma longitudinal studyrdquoHormoneResearch in Paediatrics vol74 article S38 2010
[58] Group TINBSS ldquoNijmegen breakage syndromerdquo Archives ofDisease in Childhood vol 82 pp 400ndash406 2000
[59] M Digweed and K Sperling ldquoNijmegen breakage syndromeClinical manifestation of defective response to DNA double-strand breaksrdquo DNA Repair vol 3 no 8-9 pp 1207ndash1217 2004
[60] E Seemanova ldquoAn increased risk for malignant neoplasmsin heterozygotes for a syndrome of microcephaly normalintelligence growth retardation remarkable facies immun-odeficiency and chromosomal instabilityrdquo Mutation ResearchReviews in Genetic Toxicology vol 238 no 3 pp 321ndash324 1990
[61] K H Chrzanowska M Szarras-Czapnik M Gajdulewicz et alldquoHigh prevalence of primary ovarian insufficiency in girls andyoung women with Nijmegen breakage syndrome Evidencefrom a longitudinal studyrdquoThe Journal of Clinical Endocrinologyamp Metabolism vol 95 no 7 pp 3133ndash3140 2010
[62] C M R Weemaes T W J Hustinx J M J C Scheres P J JV Munster J A J M Bakkeren and R D F M Taalman ldquoAnew chromosomal instability disorder The nijmegen breakagesyndromerdquo Acta Paediatrica Scandinavica vol 70 no 4 pp557ndash564 1981
[63] A J Green J R W Yates A M R Taylor et al ldquoSevere micro-cephaly with normal intellectual development The Nijmegen
breakage syndromerdquo Archives of Disease in Childhood vol 73no 5 pp 431ndash434 1995
[64] D Gupta and A Nagarkar ldquoSpeech impairment in Nijmegenbreakage syndrome A rare anomalyrdquo International Journal ofPediatric Otorhinolaryngology vol 73 no 6 pp 873ndash875 2009
[65] P Muschke H Gola R Varon et al ldquoRetrospective diagnosisand subsequent prenatal diagnosis of Nijmegen breakage syn-dromerdquo Prenatal Diagnosis vol 24 no 2 pp 111ndash113 2004
[66] S Pasic M Cupic T Jovanovic S Djukic M Kavaric andI Lazarevic ldquoNijmegen breakage syndrome and chronic pol-yarthritisrdquo Italian Journal of Pediatrics vol 39 no 1 article no59 2013
[67] J P Patel J M Puck R Srinivasan et al ldquoNijmegen BreakageSyndrome Detected by Newborn Screening for T Cell ReceptorExcision Circles (TRECs)rdquo Journal of Clinical Immunology vol35 no 2 pp 227ndash233 2015
[68] I Demuth and M Digweed ldquoThe clinical manifestation of adefective response to DNA double-strand breaks as exemplifiedby Nijmegen breakage syndromerdquoOncogene vol 26 no 56 pp7792ndash7798 2007
[69] H Arora A H Chacon S Choudhary et al ldquoBloom syn-dromerdquo International Journal of Dermatology vol 53 no 7 pp798ndash802 2014
[70] C de Renty and N A Ellis ldquoBloomrsquos syndrome Why not pre-mature aging A comparison of the BLM andWRN helicasesrdquoAgeing Research Reviews vol 33 pp 36ndash51 2017
[71] C Keller K R Keller S B Shew and S E Plon ldquoGrowthdeficiency and malnutrition in Bloom syndromerdquo Journal ofPediatrics vol 134 no 4 pp 472ndash479 1999
[72] A Diaz M G Vogiatzi M M Sanz and J German ldquoEval-uation of short stature carbohydrate metabolism and otherendocrinopathies in Bloomrsquos syndromerdquo Hormone Researchvol 66 no 3 pp 111ndash117 2006
[73] C Ling J Huang Z Yan et al ldquoBloom syndrome complexpromotes FANCM recruitment to stalled replication forksand facilitates both repair and traverse of DNA interstrandcrosslinksrdquo Cell Discovery vol 2 article 16047 2016
[74] J S Renes R H Willemsen A Wagner M J J Finken and AC SHokken-Koelega ldquoBloom syndrome in short children bornsmall for gestational age A challenging diagnosisrdquoThe Journalof Clinical EndocrinologyampMetabolism vol 98 no 10 pp 3932ndash3938 2013
[75] M Maciejczyk B Mikoluc B Pietrucha et al ldquoOxidativestress mitochondrial abnormalities and antioxidant defense inAtaxia-telangiectasia Bloom syndrome andNijmegen breakagesyndromerdquo Redox Biology vol 11 pp 375ndash383 2017
[76] R M Brosh M Bellani Y Liu and M M Seidman ldquoFanconiAnemia A DNA repair disorder characterized by accelerateddecline of the hematopoietic stem cell compartment and otherfeatures of agingrdquo Ageing Research Reviews vol 33 pp 67ndash752017
[77] S Yan M Sorrell and Z Berman ldquoFunctional interplay be-tween ATMATR-mediated DNA damage response and DNArepair pathways in oxidative stressrdquo Cellular and Molecular LifeSciences vol 71 no 20 pp 3951ndash3967 2014
[78] L M M Nardozza A C R Caetano A C P Zamarian etal ldquoFetal growth restriction current knowledgerdquo Archives ofGynecology and Obstetrics vol 295 no 5 pp 1061ndash1077 2017
[79] M Tomas Vila J P Verdu M R Piera and C O AlonsoldquoNijmegen breakage syndrome phenotype a disorder to con-sider in the diagnosis ofmicrocephalyrdquoAnales De Pediatria vol74 pp 58ndash60 2011
Submit your manuscripts athttpswwwhindawicom
Stem CellsInternational
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
MEDIATORSINFLAMMATION
of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Behavioural Neurology
EndocrinologyInternational Journal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Disease Markers
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
BioMed Research International
OncologyJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Oxidative Medicine and Cellular Longevity
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
PPAR Research
The Scientific World JournalHindawi Publishing Corporation httpwwwhindawicom Volume 2014
Immunology ResearchHindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Journal of
ObesityJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Computational and Mathematical Methods in Medicine
OphthalmologyJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Diabetes ResearchJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Research and TreatmentAIDS
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Gastroenterology Research and Practice
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Parkinsonrsquos Disease
Evidence-Based Complementary and Alternative Medicine
Volume 2014Hindawi Publishing Corporationhttpwwwhindawicom

BioMed Research International 7
(a) (b)
Figure 5 Chromosomal instability induced by 40 ngml mitomycin C (a) Lymphocytes from a healthy individual (b) lymphocytes from aFA patient Short arrows show chromosomal breaks the long arrow shows a quadriradial figure Note the exacerbated chromosome instabilityfound in the FA patient
The cellular phenotype of FA derived cells is extremelyconstant An aberrant FABRCA pathway can result inunrepaired DSBs that manifest as chromosomal breaks orabnormal repair by an error-prone repair pathway that resultsin radial figures These alterations are cytogenetic evidenceof chromosomal instability which is the hallmark of FA cellsand is exploited for clinical diagnostic purposes (Figure 5)The agents capable of inducing this chromosomal instabilityare from endogenous origin like aldehydes [37] and reactivespecies of oxygen (ROS) [38] as well as exogenous sourceslike bifunctional alkylating agents (diepoxybutane or mito-mycin C) In addition FA cells have accumulation of cells inG2 phase of the cell cycle resulting from a functional G2Mcheckpoint and a proapoptotic phenotype
In contrast with the cellular FA phenotype the clinicalpicture in FA patients is extremely variable not every patientwill have all the manifestations one-third of patients do nothave congenital malformations [39] while almost 90 willdevelop bone marrow failure [36] One of the more constantmanifestations in FApatients is growth parameters alterationAn analysis from the international Fanconi anemia registry(IFAR) data showed that over 60 of FA patients presentedshort stature (below the 5th percentile) while birth lengthandweight below the 5th percentile was respectively reportedin almost 30 and nearly half of FA patients [40]Moreover aprospective study of data from 54 IFAR participants showedthat the mean standard deviation score (SDS) for height inthese patients was significantly below normal for age and sexat minus235 plusmn 028 meanwhile mean SDS for weight was betteralthough below normal (minus126 plusmn 024) In this study perinatalgrowth data was not reported [41]
Other than the IFAR data on growth there are anothertwo studies that analyze growth parameters of FA patientsAnthropometric measurements from 45 patients with Fan-coni anemia from the National Cancer Institutersquos inher-ited bone marrow failure syndromes (IBMFS) cohort wereassessed This cohort had a mean SDS for height of minus21 plusmn
189 The height of over half of the participants (54) wascategorized as short (SDS gt 20 SD) in this subset of patientsthe mean SDS for height was minus38 plusmn 15 [42] Finally theevaluation of 120 FA patients from the FA ComprehensiveCare Clinic of Cincinnati Childrenrsquos Hospital Medical Centerrevealed that median height SDS was shorter than expectedin children and adults irrespective of gender Furthermorethis study presented birth information from 70 patients (59children and 11 adults) from the cohort 51 of the childrenand 3 adults were born small for gestational age their medianbirth weight at term was 202 kg (range 15ndash26 kg) [43] Theintrauterine growth restriction seen in FA patients has alsobeen documented in several case reports in which at-termbirth weight ranges from 1780 to 3200 gr [44ndash49] Eventhough growth abnormalities have been identified in FApatients with mutations in almost every FANC gene it hasbeen shown that patientswithmutations in certain genes havea more severe growth delay That is the case for patients withbiallelic mutations in FANCD1 [47 48] as well as those whobear mutations in FANCC for whom an SDS for height ofminus384 has been found [41]
Endocrine abnormalities have been proven to be aninherent part of the FA phenotype up to 80 of patientshave one or more endocrine abnormalities Besides growththyroid function and glucose homeostasis are frequentlyaffected [40ndash43] Considering the existing evidence for arelationship between low birth weight and an increased riskfor noncommunicable adult diseases like diabetes hyperten-sion heart disease dyslipidemia and osteoporosis [50] it isrelevant to revise these diseases in FA The FA cohorts inwhom growth was assessed were also evaluated for endocrinestatus Glucose homeostasis is affected in a large portion ofFA patients impaired glucose tolerance has been found in27ndash68 of them whereas diabetes has a prevalence of 8ndash10Dyslipidemia has been assessed in only a small portionof FA patients but it has been found in 17ndash55 of theevaluated subjects [51]There are conflicting results over bone
8 BioMed Research International
mineral density (BMD) status in FA the first time this wasevaluated 92 of the patients were found to have osteopeniaor osteoporosis [42] nevertheless a study that evaluated alarger FA cohort found that lowBMD is not a frequent finding[52] Further research on this topic has raised the questionof whether BMD deficit is intrinsic to the FA phenotype ora consequence of hematopoietic cell transplantation (HCT)an interrogation that is still awaiting to be answered [53]Cardiovascular adult diseases are not relevant in the FA phe-notype heart disease in these patients is from the congenitaltype as 13of patients have cardiacmalformations [40] whilehypertension has only been reported in two patients as theresult of renal malformations [54]
Findings from the different FA cohorts show that shortstature is an inherent feature of the FA phenotype thisfeature does not respond to a single explanation the apoptosisprone FA cellular phenotype is certainly a contributing factorfor this The fact that FA patients have a constitutionallydefective pathway since conception could explain the clinicalphenotype of RCIU Short stature may also be exacerbated byaccompanying endocrinopathies The cooccurrence of manyendocrine alterations has encouraged unifying explanationssome have proposed that endocrinopathies are secondaryto increased cytokine activity found in FA cells [41] whileothers favor the view that some endocrine secretory cellsmight be damaged by high levels of reactive oxygen specieswhich are known to be elevated in FA patients [43] In linewith the developmental origin of adult health and diseasetheory it could also be possible that the increased prevalenceof glucose homeostasis alterations and dyslipidemia reportedin FA patients is a consequence of intrauterine growthrestriction of these patients Nevertheless the attemptedgenotype-phenotype correlation of the endocrine phenotypein FA patients does not seem to support that Patients withmutations in FANCA show a mild endocrine phenotype inwhich height is not severely affected and insulin resistanceis mild whereas mutations in FANCC which are relatedto shorter stature have the least insulin resistance [41]Moreover no direct relationship between birth weight andglucose tolerance was identified when it was intentionallylooked for [43] although the number of patients in whichthese observations were made is limited
73 Nijmegen Breakage Syndrome Nijmegen breakage syn-drome (NBS) is an autosomal recessive disease caused bybiallelic mutations in NBN a gene that encodes nibrin aprotein involved in DNA repair and cell cycle checkpointregulation It participates in the former by sensing double-strand breaks as part of the trimeric complexMRN alongsideMRE11 andRAD50Meanwhile for the latter it contributes tothe appropriate activation of ATM andATRwhich are centraltransductors of the DNA damage response (DDR) [55] Themalfunction of nibrin translates in a cellular phenotypemarked by chromosomal instability radiosensitivity reducedphosphorylation of ATM substrates and S and G2M cellcycle defects [56] Chromosome instability is evidenced bycytogenetic methods in 10ndash60 of cells in the form of breaksand numeric and structural aberrations translocations andinversions affecting chromosomes 7 and 14 are found in the
147
Figure 6 Translocation between chromosomes 7 and 14 is typicalin NBS patientsrsquo cells
majority of NBS patients and are considered a cytogeneticcharacteristic of this syndrome (Figure 6) [57]
The clinical impact of these alterations is a phenotypecharacterized by microcephaly a distinctive facial appear-ance consisting of receding forehead and mandible and aprominent mid face with a long nose and philtrum aswell as immunodeficiency that leads to recurrent infectionsand an increased risk for the development of neoplasiaparticularly leukemia and lymphoma According to theinternational Nijmegen breakage syndrome study groupgrowth retardation is also a hallmark of this disease [58]although there is not many details about this feature in theliterature
Most of the information on the natural history of NBSavailable today comes from patients participating in reg-istries in which fairly large cohorts of NBS patients areincluded There is a large representation of Slavic patientsin these cohorts which correlates with the high carrierfrequency of a founder mutation of NBN in this populationFrom these studies it is evident that the most severelyaffected anthropometric measure in NBS patients is headcircumference since all participants display microcephalyeven though only 75 display this feature at birth Whenit comes to growth parameters the same study states thatall patients have growth retardation which is described asproportionate and early occurring [58] although the specifictemporality is not defined A posterior report points out thatthe growth retardation seen in most NBS patients locatesthem in the 10th percentile in growth charts and that birthheight and weight are usually within normal parameters [59]Nevertheless there are other authors who report prenataland postnatal growth retardation [55 60] and a tendency forshort stature that is more evident during the first year of life[61] Also several case reports of NBS patients in which birthweight is informed demonstrate prenatal growth restriction[62ndash67] although this could represent a report bias Themore comprehensive data analysis on growth that includesperinatal information of NBS patients is the one that analyzesdata from 67 patients followed for 15 years Eighty percentof these patients were born at term the girls were found tohave a mean birth weight of 27 kg and mean birth heightof 514 cm while boys were reported to have a mean birthweight of 28 kg and mean birth height of 523 cm Moreoverall patients irrespective of gender were found to have ameanheight reduced by over 2 SDS at one year old [57] These data
BioMed Research International 9
(a) (b)
Figure 7 Sister chromatid exchange in cells from a healthy individual (a) and from a BLM patient (b)
support the fact that growth retardation in NBS is a prenatalphenomenon
Nibrin has been found to have essential functions inthe regulation of the cell cycle which translates into anabsolute need for this protein for cell proliferation [68]It would seem logical that mutations of the NBN genethat compromise the appropriate function of nibrin wouldlead to abnormal growth when thought from an organismperspective Mechanistically speaking poor cellular growthcaused by mutations in a particular gene can be thought ofas the main explanation for the growth restricted phenotypebut it has been shown that mutations in other DDR genesthat share the cellular phenotype of poor growth like ATMdo not replicate the compromised growth phenotype atthe organism level growth retardation is absent in ataxiatelangiectasia (AT)This data suggests that there are certainlyother contributing factors to the abnormal growth phenotypeseen in NBS patients [58]
74 Bloom Syndrome Bloom syndrome (BS) is an autosomalrecessive disorder caused by homozygous or compoundheterozygous mutations in the BLM gene (15q261) thatencodes the RecQL3 helicase BLM has a critical role inthe maintenance of genome stability acting at the interfacebetweenDNAreplication recombination and repair [69 70]To date over sixty different mutations including nonsenseand missense have been identified all of them result inthe inactivation of BLM and the consequent loss of itshelicase activity The BLM gene encodes a 1417 amino acidnuclear protein its expression peaks during the S and G
2M
phases of the cell cycle which is consistent with its rolein DNA replication and recombination BLM specificallyunwinds structures like forked DNA duplexes RNA-DNAheteroduplexes and R-Loops which explains its importanceduring replication fork progression and transcription besidesit is central for Holliday Junctions (HJs) dissolution forHR The dissolution of HJs by the topoisomerase III120572-BLMcomplex cannot be replaced by any other RecQ helicase inthe family [69 70] It has also been found to have a role in
the annealing activity of the ssDNA the proper sister chro-matid segregation during mitosis and telomere maintenance[70]
BLM can have both pro- and antirecombinogenic func-tions that are regulated by posttranslational modificationsincluding phosphorylation sumoylation and ubiquitination[70]
BLM also enables sister chromatid segregation by pro-cessing unresolved replication intermediates that manifest inmitosis as ultrafine DNA bridges (UFBs) and together withtopoisomerase III120572 RMI1 and RMI2 localizes to UFBs inanaphase BML deficient cells exhibit and increase frequencyof UFBs suggesting a role of BLM in the resolution ofthese structures Failure to resolve these UFBs leads to DNAbreakage as mitosis proceeds [70]
Therefore BS cells are characterized by an increasein chromosomal aberrations including chromatid gapsand breaks telomere associations and quadriradial chro-mosomes resulting from unsolved recombination betweenhomologous chromosomes BS cells exhibit increased muta-tion rates and the genomic instability includes elevatedmitotic HR and unequal sister chromatid exchange (SCEs)(Figure 7) Perhaps the most characteristic feature is the overtenfold increase in SCEs which results from crossover eventsduring HR repair of damage replication forks [50 69 70]
Clinically the more striking BS feature is IUGR averagebirth weight at term is 1850 g and birth length is 44 cmFor both boys and girls weight and length in BS are morethan two standard deviations below normal indicating thatgrowth retardation has a prenatal origin At postnatal agesheight remains below the normal range and is accompaniedby a paucity of subcutaneous fat Average adult height inmales has been found to be 148 cm (130ndash162 cm) whilein females it has been reported to be 139 cm (122ndash151 cm)[50 70 71]
BS patients have overall proportionated short staturebut the head is reported to be small and narrow relativelyto the body size it is described as mild microcephalyand is accompanied by malar hypoplasia Patients have
10 BioMed Research International
Figure 8 Bloomsyndromepatient inwhom the characteristicmalarerythema is present
been described to have a high pitched voice [50 70] Theskin appears normal at birth but in the first or secondyear of life in response to sun exposure children developan erythematous rash with a butterfly distribution in themalar area and the back of hands and feet The rash caninclude telangiectasia The severity varies between patientssome can even lose their eyelashes and develop blisteringaround the mouth The presence of cafe-au-lait spots andhypopigmented areas of skin associated with contiguoushyperpigmented areas is common (Figure 8) Intellectualabilitiesmay be limited in some patients and normal in others[50 70]
Other clinical conditions reported in BS patients are gas-troesophageal reflux and diarrhea in infants mild immuno-logical deficiency with frequent episodes of otitis mediaazoospermia or severe oligospermia in males and prema-ture cessation of menstruation in females minor anatomicdefects and increased risk for neoplasia which is the maincause of dead in BS [70] Another common medical con-dition in BS is diabetes mellitus associated with impairedglucose tolerance and insulin resistance it has been reportedin up to 16 of patients [70] According to data fromthe Bloomrsquos Syndrome Registry diabetes in these patientstends to begin early with a mean age at diagnosis of 266years It is not associated with ketosis and it does nothave the classical hereditary pattern seen in type 2 diabetes[50 72]
Short stature in BS is not due to hormonal causes sincethe size of cells in persons with BS is normal it has beenhypothesized that there are fewer of them due to either adecrease in the cell division rate an increase in apoptosis oreven a combination of both BS cells have troublemeeting thedemands of fast cell divisions encountered in tissues duringembryonic development The leading hypothesis suggeststhat problems arising during DNA synthesis require a longerS phase to overcome the challenge which translates intoslowing of the cell division rate and an increase in apoptosis[70]
8 Concluding Remarks
This review has focused on discussing phenotypes of CISin which there is a prenatal alteration of growth The foursyndromes discussed here are rare diseases whose prevalenceis difficult to calculate since appropriate identification anddiagnosis of affected individuals among the general popula-tion are not straightforward It is important to note that theavailable information on the natural history of FA NBS andBS comes from the analysis of several patients that participatein registries This strategy results in detailed informationthat permits a better analysis of the clinical phenotype ofthese rare diseases Meanwhile available data of SS is moreanecdotic which results in a nonsystematic gathering ofinformation which is thus frequently incomplete
From the available clinical data of these CIS it is evidentthat growth is not affected in the same extent for all ofthese syndromes the phenotypes that exhibit a more severelystagnated perinatal growth are BS and SS The severe growthdelay reported in these patients has been described as apathognomonic sign of these diagnoses In patients withFA perinatal growth can also be severely affected but notevery FA patient shows this manifestation Finally NBShas been described to have growth retardation of prenatalorigin of mild severity almost within the lower normal range(Figure 9) The cephalic circumference can be affected in allof these syndromes severe microcephaly is pathognomonicin SS and NBS it is described as mild for BS patients and it isfound in less than half of FA patients (Table 2)
When trying to understand why a subset of CIS showsprenatal growth retardation it could be alleged that theintrinsic chromosomal instability is responsible for it Butthis would not explain why prenatal growth retardation isnot a universal CIS feature for example ataxia telangiectasiapatients who have biallelic mutations in the ATMkinase genedo not show prenatal growth delay It strikes that a molecularcommon feature shared by the prenatal growth retardationSIC phenotypes is that they are caused by mutations ingenes that are necessary for an appropriate response to DSBsduring the S phase of the cell cycle The molecular defectin SS affects the functioning of ATR the preferred DDRtransducing kinase used by highly replicating ESCs TheFABRCA pathway which is affected in patients with FAdetects ICLs upon replication fork arrest Nibrin the proteinaffected in patients with NBS is induced during S phasefor the detection of DSBs And the BS helicase forms aFANCM-BLM complex needed to sense ICLs during S phase[73] It could then be argued that altered DNA replicationis an important factor for the development of intrauterinegrowth restriction in these CIS Nevertheless it must be keptin mind that the inherent chromosome instability found inthese syndromes may also be affecting normal growth in thepatients [27 43 57 60 71]
Being small for gestational age has been associatedwith a higher risk of noncommunicable adult diseases likeglucose homeostasis disorders dyslipidemia hypertensionand others It has been proposed that fetal reprogrammingto enhance fetal survival despite the risk for adult onsetdiseases is an outcome that does not take into account
BioMed Research International 11
Table 2 Growth features of chromosomal instability syndromes
SyndromeldquoLocirdquo At-term birth weightheight Microcephaly Adult height Adult onset diseases
Seckel SyndromeldquoATR3q23rdquo
Birth weight below minus3 SD(2055 g)
Severeminus4 SD
Postnatal growth retardation(below minus5 SD) Not reported
Fanconi anemialdquo21 FANC genesrdquo
Median weight 202 kg(15ndash26 kg) In 20ndash50
50ndash60 of patients with medianheight lt minus18 SDSWomen minus34 SDSMen minus44 SDS
CancerDiabetes mellitusDyslipidemia
Altered bone mineral densityNijmegen BreakageSyndromeldquoNBN8q21rdquo
Mean weightheight girls27 kg514 cm
Mean weightheight boys28 kg523 cm
100 Mean height for women minus18 SDSMean height for men minus23 Cancer
Bloom SyndromeldquoBLM15q261rdquo
Mean weight 189 kg plusmn 035 kg forboys
Mean weight 187 kg plusmn 035 kg forgirls
Mean height 434 cm plusmn 44 cm forboys
Mean height 438 cm plusmn 28 cm forgirls
Mildmicrocephaly
Mean height 1455 cm plusmn 76 cmmales
Mean height 1415 cm plusmn 61 cm forfemales
CancerDiabetes mellitus
See [27 33 40 43 50 57 69]
45 53
43245
Height (cm)
Weight (kg)
Percentile 3 Percentile 97Percentile 50495
33
Normalindividual
Mean 2055
SeckelSyndrome
2615Median 202
FanconiAnemia
Mean 51
Mean 275
Nijmegen BreakageSyndrome
38 49
24513
Mean 436
Mean 188
BloomSyndrome
Figure 9 Anthropometric features at birth of chromosome instability syndromes with perinatal growth retardation Comparison of theavailable growth data from SS FA NBS and BS syndrome against birth data from the WHOrsquos growth standards for infants Although meanheight and weight values of NBS patients are found to be within normal percentiles according to WHO standards there are several authorswho refer to prenatal growth restriction [55 63 65 79]
the reason for the prenatal growth restraint [50 72 74] Itmust be kept in mind that noncommunicable diseases aremultifactorial entities in which genetic and environmentalfactors converge and their cause cannot be attributed to asingle explanation However when growth restriction is akey feature in syndromes with chromosome instability the
possibility that cell hypoplasia due to DNA repair malfunc-tion is contributing to the growth restriction phenotypemustbe contemplated Moreover since none of these adult onsetdiseases is reported as an inherent element of the SS and NBSphenotypes the direct connection between low birth weightand adult noncommunicable diseases is less of a straight
12 BioMed Research International
shot Furthermore there are other Mendelian syndromeswith mutations in DNA repair genes that characteristicallyshow adult noncommunicable diseases but do not haveIUGR such is the case for Werner syndrome a progeroiddisease caused by biallelic mutations in another RecQ heli-case (RecQ4) that clinically presents with postnatal shortstature and a prevalence of type 2 diabetes mellitus of 70[50 70 74]
Natural history of FA NBS and BS documented throughthe existing patient registries has allowed the identificationof noncommunicable diseases to be a part of the clinicalspectrum of these syndromes (Table 2) Meanwhile from theinformation available through SS case reports no adult onsetdisease has been found to be part of this phenotype To thebest of our knowledge the direct investigation of nonevidentendocrinologic alterations like glucose homeostasis or dys-lipidemia has not been directlymade in SS patients For a raredisease like SS such a study can only be done if a fairly largegroup of patients like the one found in registries is availableIf such a study was to be performed hidden features in SSpatients could be unraveled
Oxidative stress sensibility is a cellular feature sharedby all the SIC syndromes with IUGR that could contributeto the explanation of the premature development of non-communicable adult diseases in these patients Reports haveshown that BS and NBS cells have endogenous reactiveoxygen species (ROS) overproduction and an impairedmitochondrial homeostasis [75] it is also well known thatFA cells show increased levels of oxidative damage [3876] and there is evidence that oxidative stress can activateATR-mediated checkpoint signaling [77] Since this kind ofdamage has soundly been related to age-associated diseasesthat result from tissue degeneration exacerbated oxidativedamage found in these syndromes could result in cellu-lar aging that manifests as overall premature aging withparticular symptoms like glucose homeostasis alterations[76 77]
Fetal growth restriction is a multifactorial conditionwhere wide arrays of factors converge Fetal aspects inparticular those affecting the genetic constitution of thefetus have been recognized to play an important role Ithas been demonstrated that chromosomal abnormalities andmonogenic syndromes caused by mutations in genes thatparticipate in growth or metabolic pathways directly affectfetal growth [78] Even though they are rare entities CISappear as another group of monogenic pathologies thatbroaden the list of genetic fetal factors of fetal growthrestriction
Consent
The necessary consent for the publication of the photographswas obtained
Conflicts of Interest
The authors declare that there are no conflicts of interestregarding the publication of this paper
Authorsrsquo Contributions
The three authors contributed equally andwrote the first draftof the paper The final version was approved by everyone
Acknowledgments
This paper is supported by SEP-CONACYT Project 243102Benilde Garcıa-de Teresa received the 574025 scholarshipfrom CONACYT The paper is also supported by PAPIIT-UNAM Project IA202615 and Fondos Federales INP Project41-2014
References
[1] K W J Derks J H J Hoeijmakers and J Pothof ldquoThe DNAdamage response The omics era and its impactrdquo DNA Repairvol 19 pp 214ndash220 2014
[2] S P Jackson and J Bartek ldquoThe DNA-damage response inhuman biology and diseaserdquoNature vol 461 no 7267 pp 1071ndash1078 2009
[3] J H J Hoeijmakers ldquoDNA damage aging and cancerrdquo TheNew England Journal of Medicine vol 361 no 15 pp 1475ndash14852009
[4] G Spivak ldquoNucleotide excision repair in humansrdquoDNARepairvol 36 pp 13ndash18 2015
[5] J Vijg XDong BMilholland andL Zhang ldquoGenome instabil-ity a conserved mechanism of ageingrdquo Essays in Biochemistryvol 61 no 3 pp 305ndash315 2017
[6] J I Garaycoechea and K J Patel ldquoWhy does the bone marrowfail in Fanconi anemiardquo Blood vol 123 no 1 pp 26ndash34 2014
[7] R Ceccaldi B Rondinelli andAD DrsquoAndrea ldquoRepair PathwayChoices andConsequences at theDouble-Strand BreakrdquoTrendsin Cell Biology vol 26 no 1 pp 52ndash64 2016
[8] R Biehs M Steinlage O Barton et al ldquoDNA Double-StrandBreak Resection Occurs during Non-homologous End Joiningin G1 but Is Distinct from Resection during HomologousRecombinationrdquo Molecular Cell vol 65 no 4 pp 671ndash684e52017
[9] A Ciccia and S J Elledge ldquoTheDNAdamage response makingit safe to play with knivesrdquoMolecular Cell vol 40 no 2 pp 179ndash204 2010
[10] L H Pearl A C Schierz S E Ward B Al-Lazikani and F MG Pearl ldquoTherapeutic opportunities within the DNA damageresponserdquo Nature Reviews Cancer vol 15 no 3 pp 166ndash1802015
[11] S-F Yang C-W Chang R-J Wei Y-L Shiue S-N Wang andY-T Yeh ldquoInvolvement of DNA damage response pathways inhepatocellular carcinomardquo BioMed Research International vol2014 Article ID 153867 2014
[12] M He W Zhou C Li and M Guo ldquoMicroRNAs DNAdamage response and cancer treatmentrdquo International Journalof Molecular Sciences vol 17 no 12 article no 2087 2016
[13] K A Cimprich and D Cortez ldquoATR an essential regulator ofgenome integrityrdquo Nature Reviews Molecular Cell Biology vol9 no 8 pp 616ndash627 2008
[14] B M Sirbu and D Cortez ldquoDNA damage response three levelsof DNA repair regulationrdquo Cold Spring Harbor Perspectives inBiology vol 5 article a012724 no 8 2013
BioMed Research International 13
[15] C Beck I Robert B Reina-San-Martin V Schreiber andF Dantzer ldquoPoly(ADP-ribose) polymerases in double-strandbreak repair focus on PARP1 PARP2 and PARP3rdquo Experimen-tal Cell Research vol 329 no 1 pp 18ndash25 2014
[16] D W Meek ldquoTumour suppression by p53 a role for the DNAdamage responserdquo Nature Reviews Cancer vol 9 no 10 pp714ndash723 2009
[17] A Rodrıguez L Torres U Juarez et al ldquoFanconi anemiacells with unrepaired DNA damage activate components of thecheckpoint recovery processrdquo Theoretical Biology and MedicalModelling vol 12 no 1 article 11 2015
[18] H Wang X Zhang L Teng and R J Legerski ldquoDNA damagecheckpoint recovery and cancer developmentrdquo ExperimentalCell Research vol 334 no 2 pp 350ndash358 2015
[19] P A Jeggo L H Pearl and A M Carr ldquoDNA repair genomestability and cancer A historical perspectiverdquo Nature ReviewsCancer vol 16 no 1 pp 35ndash42 2016
[20] F S Alkuraya ldquoPrimordial dwarfism An updaterdquo CurrentOpinion in Endocrinology Diabetes and Obesity vol 22 no 1pp 55ndash64 2015
[21] P Fortini C Ferretti and E Dogliotti ldquoThe response to DNAdamage during differentiation pathways and consequencesrdquoMutation ResearchmdashFundamental and Molecular Mechanismsof Mutagenesis vol 743-744 pp 160ndash168 2013
[22] B R Adams S E Golding R R Rao and K Valerie ldquoDynamicdependence on ATR and ATM for double-Strand break repairin human embryonic stem cells and neural descendantsrdquo PLoSONE vol 5 article e10001 no 4 2010
[23] A Klingseisen and A P Jackson ldquoMechanisms and pathways ofgrowth failure in primordial dwarfismrdquo Genes amp Developmentvol 25 no 19 pp 2011ndash2024 2011
[24] H Mokrani-Benhelli L Gaillard P Biasutto et al ldquoPrimaryMicrocephaly Impaired DNA Replication and Genomic Insta-bility Caused by Compound Heterozygous ATR MutationsrdquoHuman Mutation vol 34 no 2 pp 374ndash384 2013
[25] M OrsquoDriscoll A R Gennery J Seidel P Concannon and PA Jeggo ldquoAn overview of three new disorders associated withgenetic instability LIG4 syndrome RS-SCID and ATR-Seckelsyndromerdquo DNA Repair vol 3 no 8-9 pp 1227ndash1235 2004
[26] P Khetarpal S Das I Panigrahi and A Munshi ldquoPrimordialdwarfism overview of clinical and genetic aspectsrdquo MolecularGenetics and Genomics vol 291 no 1 pp 1ndash15 2016
[27] TOgi SWalker T Stiff et al ldquoIdentification of the First ATRIP-Deficient Patient and Novel Mutations in ATRDefine a ClinicalSpectrum for ATR-ATRIP Seckel Syndromerdquo PLoS Geneticsvol 8 no 11 Article ID e1002945 2012
[28] A Verloes S Drunat and P Gressens Primary autosomalrecessive microcephalies and Seckel syndrome spectrum disor-ders 2013
[29] A D Brown B W Sager A Gorthi S S Tonapi E J Brownand A J R Bishop ldquoATR suppresses endogenous DNA damageand allows completion of homologous recombination repairrdquoPLoS ONE vol 9 article e91222 no 3 2014
[30] E J Brown and D Baltimore ldquoEssential and dispensable rolesof ATR in cell cycle arrest and genome maintenancerdquo Genes ampDevelopment vol 17 no 5 pp 615ndash628 2003
[31] B Fitzgerald M OrsquoDriscoll K Chong S Keating and PShannon ldquoNeuropathology of fetal stage Seckel syndromeA case report providing a morphological correlate for theemerging molecular mechanismsrdquo Brain amp Development vol34 no 3 pp 238ndash243 2012
[32] L I Mullee and C G Morrison ldquoCentrosomes in the DNAdamage responsemdashthe hub outside the centrerdquo ChromosomeResearch vol 24 no 1 pp 35ndash51 2016
[33] K M Takikawa A Kikuchi A Yokoyama et al ldquoPerinatalfindings of Seckel syndrome A case report of a fetus showingprimordial dwarfism and severe microcephalyrdquo Fetal Diagnosisand Therapy vol 24 no 4 pp 405ndash408 2009
[34] Y Ruzankina C Pinzon-Guzman A Asare et al ldquoDeletion ofthe Developmentally Essential Gene ATR in Adult Mice Leadsto Age-Related Phenotypes and Stem Cell Lossrdquo Cell Stem Cellvol 1 no 1 pp 113ndash126 2007
[35] N E Mamrak A Shimamura and N G Howlett ldquoRecentdiscoveries in the molecular pathogenesis of the inherited bonemarrow failure syndrome Fanconi anemiardquo Blood Reviews vol31 no 3 pp 93ndash99 2017
[36] B P Alter ldquoDiagnosis Genetics and Management of InheritedBone Marrow Failure Syndromesrdquo International Journal ofHematology vol 2007 no 1 pp 29ndash39 2007
[37] L B Pontel I V Rosado G Burgos-Barragan et al ldquoEndoge-nous Formaldehyde Is a Hematopoietic Stem Cell Genotoxinand Metabolic Carcinogenrdquo Molecular Cell vol 60 no 1 pp177ndash188 2015
[38] G Pagano P Degan M DrsquoIschia et al ldquoOxidative stress asa multiple effector in Fanconi anaemia clinical phenotyperdquoEuropean Journal of Haematology vol 75 no 2 pp 93ndash1002005
[39] P FGiampietro P CVerlander J GDavis andADAuerbachldquoDiagnosis of Fanconi anemia in patients without congenitalmalformations An International Fanconi Anemia Registrystudyrdquo American Journal of Medical Genetics vol 68 no 1 pp58ndash61 1997
[40] P F Giampietro B Adler-Brecher P C Verlander S GPavlakis J G Davis and A D Auerbach ldquoThe need for moreaccurate and timely diagnosis in Fanconi anemia A report fromthe International Fanconi Anemia Registryrdquo Pediatrics vol 91no 6 pp 1116ndash1120 1993
[41] M P Wajnrajch J M Gertner Z Huma et al ldquoEvaluationof growth and hormonal status in patients referred to theinternational fanconi anemia registryrdquo Pediatrics vol 107 no4 I pp 744ndash754 2001
[42] N Giri D L Batista B P Alter and C A Stratakis ldquoEndocrineabnormalities in patients with fanconi anemiardquo The Journal ofClinical Endocrinology amp Metabolism vol 92 no 7 pp 2624ndash2631 2007
[43] S R Rose K C Myers M M Rutter et al ldquoEndocrine phe-notype of children and adults with Fanconi anemiardquo PediatricBlood amp Cancer vol 59 no 4 pp 690ndash696 2012
[44] A D Auerbach B Adler and R S K Chaganti ldquoPrenatal andpostnatal diagnosis and carrier detection of Fanconi anemia bya cytogeneticmethodrdquoPediatrics vol 67 no 1 pp 128ndash135 1981
[45] A D Auerbach M Sagi and B Adler ldquoFanconi anemiaPrenatal diagnosis in 30 fetuses at riskrdquo Pediatrics vol 76 no5 pp 794ndash800 1985
[46] L Faivre M F Portnoı G Pals et al ldquoShould chromosomebreakage studies be performed in patients with VACTERLassociationrdquo American Journal of Medical Genetics vol 137 no1 pp 55ndash58 2005
[47] B P Alter P S Rosenberg and L C Brody ldquoClinicaland molecular features associated with biallelic mutations inFANCD1BRCA2rdquo Journal ofMedical Genetics vol 44 no 1 pp1ndash9 2007
14 BioMed Research International
[48] K Myers S M Davies R E Harris et al ldquoThe clinicalphenotype of children with Fanconi anemia caused by biallelicFANCD1BRCA2mutationsrdquo Pediatric Blood amp Cancer vol 58no 3 pp 462ndash465 2012
[49] B G Yoon H N Kim U J Han et al ldquoLong-term follow-up of Fanconi anemia Clinical manifestation and treatmentoutcomerdquo Korean Journal of Pediatrics vol 57 no 3 pp 125ndash134 2014
[50] J G Hall ldquoReview and hypothesis Syndromes with severeintrauterine growth restriction and very short stature - Are theyrelated to the epigeneticmechanism(s) of fetal survival involvedin the developmental origins of adult health and diseaserdquoAmerican Journal of Medical Genetics Part A vol 152 no 2 pp512ndash527 2010
[51] A Petryk R K Shankar N Giri et al ldquoEndocrine disordersin Fanconi anemia Recommendations for screening and treat-mentrdquoThe Journal of Clinical Endocrinology ampMetabolism vol100 no 3 pp 803ndash811 2015
[52] S R RoseMM Rutter RMueller et al ldquoBonemineral densityis normal in children with Fanconi anemiardquo Pediatric Blood ampCancer vol 57 no 6 pp 1034ndash1038 2011
[53] A Petryk L E Polgreen J L Barnum et al ldquoBone mineraldensity in childrenwith fanconi anemia after hematopoietic celltransplantationrdquo Biology of Blood and Marrow Transplantationvol 21 no 5 pp 894ndash899 2015
[54] R Purkait A Mukherji S Datta and R Bhadra ldquoRenal arterystenosis An unusual etiology of hypertensive encephalopathyin a childwith fanconi anemiardquo Saudi Journal of KidneyDiseasesand Transplantation vol 26 no 4 pp 778ndash782 2015
[55] K H Chrzanowska H Gregorek B Dembowska-BaginskaM A Kalina and M Digweed ldquoNijmegen breakage syndrome(NBS)rdquoOrphanet Journal of Rare Diseases vol 7 article 13 2012
[56] L C Riches A M Lynch and N J Gooderham ldquoEarly eventsin the mammalian response to DNA double-strand breaksrdquoMutagenesis vol 23 no 5 pp 331ndash339 2008
[57] K Chrzanowska M Kalina H Rysiewski et al ldquoGrowthpattern in patients withNijmegen breakage syndrome evidencefroma longitudinal studyrdquoHormoneResearch in Paediatrics vol74 article S38 2010
[58] Group TINBSS ldquoNijmegen breakage syndromerdquo Archives ofDisease in Childhood vol 82 pp 400ndash406 2000
[59] M Digweed and K Sperling ldquoNijmegen breakage syndromeClinical manifestation of defective response to DNA double-strand breaksrdquo DNA Repair vol 3 no 8-9 pp 1207ndash1217 2004
[60] E Seemanova ldquoAn increased risk for malignant neoplasmsin heterozygotes for a syndrome of microcephaly normalintelligence growth retardation remarkable facies immun-odeficiency and chromosomal instabilityrdquo Mutation ResearchReviews in Genetic Toxicology vol 238 no 3 pp 321ndash324 1990
[61] K H Chrzanowska M Szarras-Czapnik M Gajdulewicz et alldquoHigh prevalence of primary ovarian insufficiency in girls andyoung women with Nijmegen breakage syndrome Evidencefrom a longitudinal studyrdquoThe Journal of Clinical Endocrinologyamp Metabolism vol 95 no 7 pp 3133ndash3140 2010
[62] C M R Weemaes T W J Hustinx J M J C Scheres P J JV Munster J A J M Bakkeren and R D F M Taalman ldquoAnew chromosomal instability disorder The nijmegen breakagesyndromerdquo Acta Paediatrica Scandinavica vol 70 no 4 pp557ndash564 1981
[63] A J Green J R W Yates A M R Taylor et al ldquoSevere micro-cephaly with normal intellectual development The Nijmegen
breakage syndromerdquo Archives of Disease in Childhood vol 73no 5 pp 431ndash434 1995
[64] D Gupta and A Nagarkar ldquoSpeech impairment in Nijmegenbreakage syndrome A rare anomalyrdquo International Journal ofPediatric Otorhinolaryngology vol 73 no 6 pp 873ndash875 2009
[65] P Muschke H Gola R Varon et al ldquoRetrospective diagnosisand subsequent prenatal diagnosis of Nijmegen breakage syn-dromerdquo Prenatal Diagnosis vol 24 no 2 pp 111ndash113 2004
[66] S Pasic M Cupic T Jovanovic S Djukic M Kavaric andI Lazarevic ldquoNijmegen breakage syndrome and chronic pol-yarthritisrdquo Italian Journal of Pediatrics vol 39 no 1 article no59 2013
[67] J P Patel J M Puck R Srinivasan et al ldquoNijmegen BreakageSyndrome Detected by Newborn Screening for T Cell ReceptorExcision Circles (TRECs)rdquo Journal of Clinical Immunology vol35 no 2 pp 227ndash233 2015
[68] I Demuth and M Digweed ldquoThe clinical manifestation of adefective response to DNA double-strand breaks as exemplifiedby Nijmegen breakage syndromerdquoOncogene vol 26 no 56 pp7792ndash7798 2007
[69] H Arora A H Chacon S Choudhary et al ldquoBloom syn-dromerdquo International Journal of Dermatology vol 53 no 7 pp798ndash802 2014
[70] C de Renty and N A Ellis ldquoBloomrsquos syndrome Why not pre-mature aging A comparison of the BLM andWRN helicasesrdquoAgeing Research Reviews vol 33 pp 36ndash51 2017
[71] C Keller K R Keller S B Shew and S E Plon ldquoGrowthdeficiency and malnutrition in Bloom syndromerdquo Journal ofPediatrics vol 134 no 4 pp 472ndash479 1999
[72] A Diaz M G Vogiatzi M M Sanz and J German ldquoEval-uation of short stature carbohydrate metabolism and otherendocrinopathies in Bloomrsquos syndromerdquo Hormone Researchvol 66 no 3 pp 111ndash117 2006
[73] C Ling J Huang Z Yan et al ldquoBloom syndrome complexpromotes FANCM recruitment to stalled replication forksand facilitates both repair and traverse of DNA interstrandcrosslinksrdquo Cell Discovery vol 2 article 16047 2016
[74] J S Renes R H Willemsen A Wagner M J J Finken and AC SHokken-Koelega ldquoBloom syndrome in short children bornsmall for gestational age A challenging diagnosisrdquoThe Journalof Clinical EndocrinologyampMetabolism vol 98 no 10 pp 3932ndash3938 2013
[75] M Maciejczyk B Mikoluc B Pietrucha et al ldquoOxidativestress mitochondrial abnormalities and antioxidant defense inAtaxia-telangiectasia Bloom syndrome andNijmegen breakagesyndromerdquo Redox Biology vol 11 pp 375ndash383 2017
[76] R M Brosh M Bellani Y Liu and M M Seidman ldquoFanconiAnemia A DNA repair disorder characterized by accelerateddecline of the hematopoietic stem cell compartment and otherfeatures of agingrdquo Ageing Research Reviews vol 33 pp 67ndash752017
[77] S Yan M Sorrell and Z Berman ldquoFunctional interplay be-tween ATMATR-mediated DNA damage response and DNArepair pathways in oxidative stressrdquo Cellular and Molecular LifeSciences vol 71 no 20 pp 3951ndash3967 2014
[78] L M M Nardozza A C R Caetano A C P Zamarian etal ldquoFetal growth restriction current knowledgerdquo Archives ofGynecology and Obstetrics vol 295 no 5 pp 1061ndash1077 2017
[79] M Tomas Vila J P Verdu M R Piera and C O AlonsoldquoNijmegen breakage syndrome phenotype a disorder to con-sider in the diagnosis ofmicrocephalyrdquoAnales De Pediatria vol74 pp 58ndash60 2011
Submit your manuscripts athttpswwwhindawicom
Stem CellsInternational
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
MEDIATORSINFLAMMATION
of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Behavioural Neurology
EndocrinologyInternational Journal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Disease Markers
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
BioMed Research International
OncologyJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Oxidative Medicine and Cellular Longevity
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
PPAR Research
The Scientific World JournalHindawi Publishing Corporation httpwwwhindawicom Volume 2014
Immunology ResearchHindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Journal of
ObesityJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Computational and Mathematical Methods in Medicine
OphthalmologyJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Diabetes ResearchJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Research and TreatmentAIDS
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Gastroenterology Research and Practice
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Parkinsonrsquos Disease
Evidence-Based Complementary and Alternative Medicine
Volume 2014Hindawi Publishing Corporationhttpwwwhindawicom

8 BioMed Research International
mineral density (BMD) status in FA the first time this wasevaluated 92 of the patients were found to have osteopeniaor osteoporosis [42] nevertheless a study that evaluated alarger FA cohort found that lowBMD is not a frequent finding[52] Further research on this topic has raised the questionof whether BMD deficit is intrinsic to the FA phenotype ora consequence of hematopoietic cell transplantation (HCT)an interrogation that is still awaiting to be answered [53]Cardiovascular adult diseases are not relevant in the FA phe-notype heart disease in these patients is from the congenitaltype as 13of patients have cardiacmalformations [40] whilehypertension has only been reported in two patients as theresult of renal malformations [54]
Findings from the different FA cohorts show that shortstature is an inherent feature of the FA phenotype thisfeature does not respond to a single explanation the apoptosisprone FA cellular phenotype is certainly a contributing factorfor this The fact that FA patients have a constitutionallydefective pathway since conception could explain the clinicalphenotype of RCIU Short stature may also be exacerbated byaccompanying endocrinopathies The cooccurrence of manyendocrine alterations has encouraged unifying explanationssome have proposed that endocrinopathies are secondaryto increased cytokine activity found in FA cells [41] whileothers favor the view that some endocrine secretory cellsmight be damaged by high levels of reactive oxygen specieswhich are known to be elevated in FA patients [43] In linewith the developmental origin of adult health and diseasetheory it could also be possible that the increased prevalenceof glucose homeostasis alterations and dyslipidemia reportedin FA patients is a consequence of intrauterine growthrestriction of these patients Nevertheless the attemptedgenotype-phenotype correlation of the endocrine phenotypein FA patients does not seem to support that Patients withmutations in FANCA show a mild endocrine phenotype inwhich height is not severely affected and insulin resistanceis mild whereas mutations in FANCC which are relatedto shorter stature have the least insulin resistance [41]Moreover no direct relationship between birth weight andglucose tolerance was identified when it was intentionallylooked for [43] although the number of patients in whichthese observations were made is limited
73 Nijmegen Breakage Syndrome Nijmegen breakage syn-drome (NBS) is an autosomal recessive disease caused bybiallelic mutations in NBN a gene that encodes nibrin aprotein involved in DNA repair and cell cycle checkpointregulation It participates in the former by sensing double-strand breaks as part of the trimeric complexMRN alongsideMRE11 andRAD50Meanwhile for the latter it contributes tothe appropriate activation of ATM andATRwhich are centraltransductors of the DNA damage response (DDR) [55] Themalfunction of nibrin translates in a cellular phenotypemarked by chromosomal instability radiosensitivity reducedphosphorylation of ATM substrates and S and G2M cellcycle defects [56] Chromosome instability is evidenced bycytogenetic methods in 10ndash60 of cells in the form of breaksand numeric and structural aberrations translocations andinversions affecting chromosomes 7 and 14 are found in the
147
Figure 6 Translocation between chromosomes 7 and 14 is typicalin NBS patientsrsquo cells
majority of NBS patients and are considered a cytogeneticcharacteristic of this syndrome (Figure 6) [57]
The clinical impact of these alterations is a phenotypecharacterized by microcephaly a distinctive facial appear-ance consisting of receding forehead and mandible and aprominent mid face with a long nose and philtrum aswell as immunodeficiency that leads to recurrent infectionsand an increased risk for the development of neoplasiaparticularly leukemia and lymphoma According to theinternational Nijmegen breakage syndrome study groupgrowth retardation is also a hallmark of this disease [58]although there is not many details about this feature in theliterature
Most of the information on the natural history of NBSavailable today comes from patients participating in reg-istries in which fairly large cohorts of NBS patients areincluded There is a large representation of Slavic patientsin these cohorts which correlates with the high carrierfrequency of a founder mutation of NBN in this populationFrom these studies it is evident that the most severelyaffected anthropometric measure in NBS patients is headcircumference since all participants display microcephalyeven though only 75 display this feature at birth Whenit comes to growth parameters the same study states thatall patients have growth retardation which is described asproportionate and early occurring [58] although the specifictemporality is not defined A posterior report points out thatthe growth retardation seen in most NBS patients locatesthem in the 10th percentile in growth charts and that birthheight and weight are usually within normal parameters [59]Nevertheless there are other authors who report prenataland postnatal growth retardation [55 60] and a tendency forshort stature that is more evident during the first year of life[61] Also several case reports of NBS patients in which birthweight is informed demonstrate prenatal growth restriction[62ndash67] although this could represent a report bias Themore comprehensive data analysis on growth that includesperinatal information of NBS patients is the one that analyzesdata from 67 patients followed for 15 years Eighty percentof these patients were born at term the girls were found tohave a mean birth weight of 27 kg and mean birth heightof 514 cm while boys were reported to have a mean birthweight of 28 kg and mean birth height of 523 cm Moreoverall patients irrespective of gender were found to have ameanheight reduced by over 2 SDS at one year old [57] These data
BioMed Research International 9
(a) (b)
Figure 7 Sister chromatid exchange in cells from a healthy individual (a) and from a BLM patient (b)
support the fact that growth retardation in NBS is a prenatalphenomenon
Nibrin has been found to have essential functions inthe regulation of the cell cycle which translates into anabsolute need for this protein for cell proliferation [68]It would seem logical that mutations of the NBN genethat compromise the appropriate function of nibrin wouldlead to abnormal growth when thought from an organismperspective Mechanistically speaking poor cellular growthcaused by mutations in a particular gene can be thought ofas the main explanation for the growth restricted phenotypebut it has been shown that mutations in other DDR genesthat share the cellular phenotype of poor growth like ATMdo not replicate the compromised growth phenotype atthe organism level growth retardation is absent in ataxiatelangiectasia (AT)This data suggests that there are certainlyother contributing factors to the abnormal growth phenotypeseen in NBS patients [58]
74 Bloom Syndrome Bloom syndrome (BS) is an autosomalrecessive disorder caused by homozygous or compoundheterozygous mutations in the BLM gene (15q261) thatencodes the RecQL3 helicase BLM has a critical role inthe maintenance of genome stability acting at the interfacebetweenDNAreplication recombination and repair [69 70]To date over sixty different mutations including nonsenseand missense have been identified all of them result inthe inactivation of BLM and the consequent loss of itshelicase activity The BLM gene encodes a 1417 amino acidnuclear protein its expression peaks during the S and G
2M
phases of the cell cycle which is consistent with its rolein DNA replication and recombination BLM specificallyunwinds structures like forked DNA duplexes RNA-DNAheteroduplexes and R-Loops which explains its importanceduring replication fork progression and transcription besidesit is central for Holliday Junctions (HJs) dissolution forHR The dissolution of HJs by the topoisomerase III120572-BLMcomplex cannot be replaced by any other RecQ helicase inthe family [69 70] It has also been found to have a role in
the annealing activity of the ssDNA the proper sister chro-matid segregation during mitosis and telomere maintenance[70]
BLM can have both pro- and antirecombinogenic func-tions that are regulated by posttranslational modificationsincluding phosphorylation sumoylation and ubiquitination[70]
BLM also enables sister chromatid segregation by pro-cessing unresolved replication intermediates that manifest inmitosis as ultrafine DNA bridges (UFBs) and together withtopoisomerase III120572 RMI1 and RMI2 localizes to UFBs inanaphase BML deficient cells exhibit and increase frequencyof UFBs suggesting a role of BLM in the resolution ofthese structures Failure to resolve these UFBs leads to DNAbreakage as mitosis proceeds [70]
Therefore BS cells are characterized by an increasein chromosomal aberrations including chromatid gapsand breaks telomere associations and quadriradial chro-mosomes resulting from unsolved recombination betweenhomologous chromosomes BS cells exhibit increased muta-tion rates and the genomic instability includes elevatedmitotic HR and unequal sister chromatid exchange (SCEs)(Figure 7) Perhaps the most characteristic feature is the overtenfold increase in SCEs which results from crossover eventsduring HR repair of damage replication forks [50 69 70]
Clinically the more striking BS feature is IUGR averagebirth weight at term is 1850 g and birth length is 44 cmFor both boys and girls weight and length in BS are morethan two standard deviations below normal indicating thatgrowth retardation has a prenatal origin At postnatal agesheight remains below the normal range and is accompaniedby a paucity of subcutaneous fat Average adult height inmales has been found to be 148 cm (130ndash162 cm) whilein females it has been reported to be 139 cm (122ndash151 cm)[50 70 71]
BS patients have overall proportionated short staturebut the head is reported to be small and narrow relativelyto the body size it is described as mild microcephalyand is accompanied by malar hypoplasia Patients have
10 BioMed Research International
Figure 8 Bloomsyndromepatient inwhom the characteristicmalarerythema is present
been described to have a high pitched voice [50 70] Theskin appears normal at birth but in the first or secondyear of life in response to sun exposure children developan erythematous rash with a butterfly distribution in themalar area and the back of hands and feet The rash caninclude telangiectasia The severity varies between patientssome can even lose their eyelashes and develop blisteringaround the mouth The presence of cafe-au-lait spots andhypopigmented areas of skin associated with contiguoushyperpigmented areas is common (Figure 8) Intellectualabilitiesmay be limited in some patients and normal in others[50 70]
Other clinical conditions reported in BS patients are gas-troesophageal reflux and diarrhea in infants mild immuno-logical deficiency with frequent episodes of otitis mediaazoospermia or severe oligospermia in males and prema-ture cessation of menstruation in females minor anatomicdefects and increased risk for neoplasia which is the maincause of dead in BS [70] Another common medical con-dition in BS is diabetes mellitus associated with impairedglucose tolerance and insulin resistance it has been reportedin up to 16 of patients [70] According to data fromthe Bloomrsquos Syndrome Registry diabetes in these patientstends to begin early with a mean age at diagnosis of 266years It is not associated with ketosis and it does nothave the classical hereditary pattern seen in type 2 diabetes[50 72]
Short stature in BS is not due to hormonal causes sincethe size of cells in persons with BS is normal it has beenhypothesized that there are fewer of them due to either adecrease in the cell division rate an increase in apoptosis oreven a combination of both BS cells have troublemeeting thedemands of fast cell divisions encountered in tissues duringembryonic development The leading hypothesis suggeststhat problems arising during DNA synthesis require a longerS phase to overcome the challenge which translates intoslowing of the cell division rate and an increase in apoptosis[70]
8 Concluding Remarks
This review has focused on discussing phenotypes of CISin which there is a prenatal alteration of growth The foursyndromes discussed here are rare diseases whose prevalenceis difficult to calculate since appropriate identification anddiagnosis of affected individuals among the general popula-tion are not straightforward It is important to note that theavailable information on the natural history of FA NBS andBS comes from the analysis of several patients that participatein registries This strategy results in detailed informationthat permits a better analysis of the clinical phenotype ofthese rare diseases Meanwhile available data of SS is moreanecdotic which results in a nonsystematic gathering ofinformation which is thus frequently incomplete
From the available clinical data of these CIS it is evidentthat growth is not affected in the same extent for all ofthese syndromes the phenotypes that exhibit a more severelystagnated perinatal growth are BS and SS The severe growthdelay reported in these patients has been described as apathognomonic sign of these diagnoses In patients withFA perinatal growth can also be severely affected but notevery FA patient shows this manifestation Finally NBShas been described to have growth retardation of prenatalorigin of mild severity almost within the lower normal range(Figure 9) The cephalic circumference can be affected in allof these syndromes severe microcephaly is pathognomonicin SS and NBS it is described as mild for BS patients and it isfound in less than half of FA patients (Table 2)
When trying to understand why a subset of CIS showsprenatal growth retardation it could be alleged that theintrinsic chromosomal instability is responsible for it Butthis would not explain why prenatal growth retardation isnot a universal CIS feature for example ataxia telangiectasiapatients who have biallelic mutations in the ATMkinase genedo not show prenatal growth delay It strikes that a molecularcommon feature shared by the prenatal growth retardationSIC phenotypes is that they are caused by mutations ingenes that are necessary for an appropriate response to DSBsduring the S phase of the cell cycle The molecular defectin SS affects the functioning of ATR the preferred DDRtransducing kinase used by highly replicating ESCs TheFABRCA pathway which is affected in patients with FAdetects ICLs upon replication fork arrest Nibrin the proteinaffected in patients with NBS is induced during S phasefor the detection of DSBs And the BS helicase forms aFANCM-BLM complex needed to sense ICLs during S phase[73] It could then be argued that altered DNA replicationis an important factor for the development of intrauterinegrowth restriction in these CIS Nevertheless it must be keptin mind that the inherent chromosome instability found inthese syndromes may also be affecting normal growth in thepatients [27 43 57 60 71]
Being small for gestational age has been associatedwith a higher risk of noncommunicable adult diseases likeglucose homeostasis disorders dyslipidemia hypertensionand others It has been proposed that fetal reprogrammingto enhance fetal survival despite the risk for adult onsetdiseases is an outcome that does not take into account
BioMed Research International 11
Table 2 Growth features of chromosomal instability syndromes
SyndromeldquoLocirdquo At-term birth weightheight Microcephaly Adult height Adult onset diseases
Seckel SyndromeldquoATR3q23rdquo
Birth weight below minus3 SD(2055 g)
Severeminus4 SD
Postnatal growth retardation(below minus5 SD) Not reported
Fanconi anemialdquo21 FANC genesrdquo
Median weight 202 kg(15ndash26 kg) In 20ndash50
50ndash60 of patients with medianheight lt minus18 SDSWomen minus34 SDSMen minus44 SDS
CancerDiabetes mellitusDyslipidemia
Altered bone mineral densityNijmegen BreakageSyndromeldquoNBN8q21rdquo
Mean weightheight girls27 kg514 cm
Mean weightheight boys28 kg523 cm
100 Mean height for women minus18 SDSMean height for men minus23 Cancer
Bloom SyndromeldquoBLM15q261rdquo
Mean weight 189 kg plusmn 035 kg forboys
Mean weight 187 kg plusmn 035 kg forgirls
Mean height 434 cm plusmn 44 cm forboys
Mean height 438 cm plusmn 28 cm forgirls
Mildmicrocephaly
Mean height 1455 cm plusmn 76 cmmales
Mean height 1415 cm plusmn 61 cm forfemales
CancerDiabetes mellitus
See [27 33 40 43 50 57 69]
45 53
43245
Height (cm)
Weight (kg)
Percentile 3 Percentile 97Percentile 50495
33
Normalindividual
Mean 2055
SeckelSyndrome
2615Median 202
FanconiAnemia
Mean 51
Mean 275
Nijmegen BreakageSyndrome
38 49
24513
Mean 436
Mean 188
BloomSyndrome
Figure 9 Anthropometric features at birth of chromosome instability syndromes with perinatal growth retardation Comparison of theavailable growth data from SS FA NBS and BS syndrome against birth data from the WHOrsquos growth standards for infants Although meanheight and weight values of NBS patients are found to be within normal percentiles according to WHO standards there are several authorswho refer to prenatal growth restriction [55 63 65 79]
the reason for the prenatal growth restraint [50 72 74] Itmust be kept in mind that noncommunicable diseases aremultifactorial entities in which genetic and environmentalfactors converge and their cause cannot be attributed to asingle explanation However when growth restriction is akey feature in syndromes with chromosome instability the
possibility that cell hypoplasia due to DNA repair malfunc-tion is contributing to the growth restriction phenotypemustbe contemplated Moreover since none of these adult onsetdiseases is reported as an inherent element of the SS and NBSphenotypes the direct connection between low birth weightand adult noncommunicable diseases is less of a straight
12 BioMed Research International
shot Furthermore there are other Mendelian syndromeswith mutations in DNA repair genes that characteristicallyshow adult noncommunicable diseases but do not haveIUGR such is the case for Werner syndrome a progeroiddisease caused by biallelic mutations in another RecQ heli-case (RecQ4) that clinically presents with postnatal shortstature and a prevalence of type 2 diabetes mellitus of 70[50 70 74]
Natural history of FA NBS and BS documented throughthe existing patient registries has allowed the identificationof noncommunicable diseases to be a part of the clinicalspectrum of these syndromes (Table 2) Meanwhile from theinformation available through SS case reports no adult onsetdisease has been found to be part of this phenotype To thebest of our knowledge the direct investigation of nonevidentendocrinologic alterations like glucose homeostasis or dys-lipidemia has not been directlymade in SS patients For a raredisease like SS such a study can only be done if a fairly largegroup of patients like the one found in registries is availableIf such a study was to be performed hidden features in SSpatients could be unraveled
Oxidative stress sensibility is a cellular feature sharedby all the SIC syndromes with IUGR that could contributeto the explanation of the premature development of non-communicable adult diseases in these patients Reports haveshown that BS and NBS cells have endogenous reactiveoxygen species (ROS) overproduction and an impairedmitochondrial homeostasis [75] it is also well known thatFA cells show increased levels of oxidative damage [3876] and there is evidence that oxidative stress can activateATR-mediated checkpoint signaling [77] Since this kind ofdamage has soundly been related to age-associated diseasesthat result from tissue degeneration exacerbated oxidativedamage found in these syndromes could result in cellu-lar aging that manifests as overall premature aging withparticular symptoms like glucose homeostasis alterations[76 77]
Fetal growth restriction is a multifactorial conditionwhere wide arrays of factors converge Fetal aspects inparticular those affecting the genetic constitution of thefetus have been recognized to play an important role Ithas been demonstrated that chromosomal abnormalities andmonogenic syndromes caused by mutations in genes thatparticipate in growth or metabolic pathways directly affectfetal growth [78] Even though they are rare entities CISappear as another group of monogenic pathologies thatbroaden the list of genetic fetal factors of fetal growthrestriction
Consent
The necessary consent for the publication of the photographswas obtained
Conflicts of Interest
The authors declare that there are no conflicts of interestregarding the publication of this paper
Authorsrsquo Contributions
The three authors contributed equally andwrote the first draftof the paper The final version was approved by everyone
Acknowledgments
This paper is supported by SEP-CONACYT Project 243102Benilde Garcıa-de Teresa received the 574025 scholarshipfrom CONACYT The paper is also supported by PAPIIT-UNAM Project IA202615 and Fondos Federales INP Project41-2014
References
[1] K W J Derks J H J Hoeijmakers and J Pothof ldquoThe DNAdamage response The omics era and its impactrdquo DNA Repairvol 19 pp 214ndash220 2014
[2] S P Jackson and J Bartek ldquoThe DNA-damage response inhuman biology and diseaserdquoNature vol 461 no 7267 pp 1071ndash1078 2009
[3] J H J Hoeijmakers ldquoDNA damage aging and cancerrdquo TheNew England Journal of Medicine vol 361 no 15 pp 1475ndash14852009
[4] G Spivak ldquoNucleotide excision repair in humansrdquoDNARepairvol 36 pp 13ndash18 2015
[5] J Vijg XDong BMilholland andL Zhang ldquoGenome instabil-ity a conserved mechanism of ageingrdquo Essays in Biochemistryvol 61 no 3 pp 305ndash315 2017
[6] J I Garaycoechea and K J Patel ldquoWhy does the bone marrowfail in Fanconi anemiardquo Blood vol 123 no 1 pp 26ndash34 2014
[7] R Ceccaldi B Rondinelli andAD DrsquoAndrea ldquoRepair PathwayChoices andConsequences at theDouble-Strand BreakrdquoTrendsin Cell Biology vol 26 no 1 pp 52ndash64 2016
[8] R Biehs M Steinlage O Barton et al ldquoDNA Double-StrandBreak Resection Occurs during Non-homologous End Joiningin G1 but Is Distinct from Resection during HomologousRecombinationrdquo Molecular Cell vol 65 no 4 pp 671ndash684e52017
[9] A Ciccia and S J Elledge ldquoTheDNAdamage response makingit safe to play with knivesrdquoMolecular Cell vol 40 no 2 pp 179ndash204 2010
[10] L H Pearl A C Schierz S E Ward B Al-Lazikani and F MG Pearl ldquoTherapeutic opportunities within the DNA damageresponserdquo Nature Reviews Cancer vol 15 no 3 pp 166ndash1802015
[11] S-F Yang C-W Chang R-J Wei Y-L Shiue S-N Wang andY-T Yeh ldquoInvolvement of DNA damage response pathways inhepatocellular carcinomardquo BioMed Research International vol2014 Article ID 153867 2014
[12] M He W Zhou C Li and M Guo ldquoMicroRNAs DNAdamage response and cancer treatmentrdquo International Journalof Molecular Sciences vol 17 no 12 article no 2087 2016
[13] K A Cimprich and D Cortez ldquoATR an essential regulator ofgenome integrityrdquo Nature Reviews Molecular Cell Biology vol9 no 8 pp 616ndash627 2008
[14] B M Sirbu and D Cortez ldquoDNA damage response three levelsof DNA repair regulationrdquo Cold Spring Harbor Perspectives inBiology vol 5 article a012724 no 8 2013
BioMed Research International 13
[15] C Beck I Robert B Reina-San-Martin V Schreiber andF Dantzer ldquoPoly(ADP-ribose) polymerases in double-strandbreak repair focus on PARP1 PARP2 and PARP3rdquo Experimen-tal Cell Research vol 329 no 1 pp 18ndash25 2014
[16] D W Meek ldquoTumour suppression by p53 a role for the DNAdamage responserdquo Nature Reviews Cancer vol 9 no 10 pp714ndash723 2009
[17] A Rodrıguez L Torres U Juarez et al ldquoFanconi anemiacells with unrepaired DNA damage activate components of thecheckpoint recovery processrdquo Theoretical Biology and MedicalModelling vol 12 no 1 article 11 2015
[18] H Wang X Zhang L Teng and R J Legerski ldquoDNA damagecheckpoint recovery and cancer developmentrdquo ExperimentalCell Research vol 334 no 2 pp 350ndash358 2015
[19] P A Jeggo L H Pearl and A M Carr ldquoDNA repair genomestability and cancer A historical perspectiverdquo Nature ReviewsCancer vol 16 no 1 pp 35ndash42 2016
[20] F S Alkuraya ldquoPrimordial dwarfism An updaterdquo CurrentOpinion in Endocrinology Diabetes and Obesity vol 22 no 1pp 55ndash64 2015
[21] P Fortini C Ferretti and E Dogliotti ldquoThe response to DNAdamage during differentiation pathways and consequencesrdquoMutation ResearchmdashFundamental and Molecular Mechanismsof Mutagenesis vol 743-744 pp 160ndash168 2013
[22] B R Adams S E Golding R R Rao and K Valerie ldquoDynamicdependence on ATR and ATM for double-Strand break repairin human embryonic stem cells and neural descendantsrdquo PLoSONE vol 5 article e10001 no 4 2010
[23] A Klingseisen and A P Jackson ldquoMechanisms and pathways ofgrowth failure in primordial dwarfismrdquo Genes amp Developmentvol 25 no 19 pp 2011ndash2024 2011
[24] H Mokrani-Benhelli L Gaillard P Biasutto et al ldquoPrimaryMicrocephaly Impaired DNA Replication and Genomic Insta-bility Caused by Compound Heterozygous ATR MutationsrdquoHuman Mutation vol 34 no 2 pp 374ndash384 2013
[25] M OrsquoDriscoll A R Gennery J Seidel P Concannon and PA Jeggo ldquoAn overview of three new disorders associated withgenetic instability LIG4 syndrome RS-SCID and ATR-Seckelsyndromerdquo DNA Repair vol 3 no 8-9 pp 1227ndash1235 2004
[26] P Khetarpal S Das I Panigrahi and A Munshi ldquoPrimordialdwarfism overview of clinical and genetic aspectsrdquo MolecularGenetics and Genomics vol 291 no 1 pp 1ndash15 2016
[27] TOgi SWalker T Stiff et al ldquoIdentification of the First ATRIP-Deficient Patient and Novel Mutations in ATRDefine a ClinicalSpectrum for ATR-ATRIP Seckel Syndromerdquo PLoS Geneticsvol 8 no 11 Article ID e1002945 2012
[28] A Verloes S Drunat and P Gressens Primary autosomalrecessive microcephalies and Seckel syndrome spectrum disor-ders 2013
[29] A D Brown B W Sager A Gorthi S S Tonapi E J Brownand A J R Bishop ldquoATR suppresses endogenous DNA damageand allows completion of homologous recombination repairrdquoPLoS ONE vol 9 article e91222 no 3 2014
[30] E J Brown and D Baltimore ldquoEssential and dispensable rolesof ATR in cell cycle arrest and genome maintenancerdquo Genes ampDevelopment vol 17 no 5 pp 615ndash628 2003
[31] B Fitzgerald M OrsquoDriscoll K Chong S Keating and PShannon ldquoNeuropathology of fetal stage Seckel syndromeA case report providing a morphological correlate for theemerging molecular mechanismsrdquo Brain amp Development vol34 no 3 pp 238ndash243 2012
[32] L I Mullee and C G Morrison ldquoCentrosomes in the DNAdamage responsemdashthe hub outside the centrerdquo ChromosomeResearch vol 24 no 1 pp 35ndash51 2016
[33] K M Takikawa A Kikuchi A Yokoyama et al ldquoPerinatalfindings of Seckel syndrome A case report of a fetus showingprimordial dwarfism and severe microcephalyrdquo Fetal Diagnosisand Therapy vol 24 no 4 pp 405ndash408 2009
[34] Y Ruzankina C Pinzon-Guzman A Asare et al ldquoDeletion ofthe Developmentally Essential Gene ATR in Adult Mice Leadsto Age-Related Phenotypes and Stem Cell Lossrdquo Cell Stem Cellvol 1 no 1 pp 113ndash126 2007
[35] N E Mamrak A Shimamura and N G Howlett ldquoRecentdiscoveries in the molecular pathogenesis of the inherited bonemarrow failure syndrome Fanconi anemiardquo Blood Reviews vol31 no 3 pp 93ndash99 2017
[36] B P Alter ldquoDiagnosis Genetics and Management of InheritedBone Marrow Failure Syndromesrdquo International Journal ofHematology vol 2007 no 1 pp 29ndash39 2007
[37] L B Pontel I V Rosado G Burgos-Barragan et al ldquoEndoge-nous Formaldehyde Is a Hematopoietic Stem Cell Genotoxinand Metabolic Carcinogenrdquo Molecular Cell vol 60 no 1 pp177ndash188 2015
[38] G Pagano P Degan M DrsquoIschia et al ldquoOxidative stress asa multiple effector in Fanconi anaemia clinical phenotyperdquoEuropean Journal of Haematology vol 75 no 2 pp 93ndash1002005
[39] P FGiampietro P CVerlander J GDavis andADAuerbachldquoDiagnosis of Fanconi anemia in patients without congenitalmalformations An International Fanconi Anemia Registrystudyrdquo American Journal of Medical Genetics vol 68 no 1 pp58ndash61 1997
[40] P F Giampietro B Adler-Brecher P C Verlander S GPavlakis J G Davis and A D Auerbach ldquoThe need for moreaccurate and timely diagnosis in Fanconi anemia A report fromthe International Fanconi Anemia Registryrdquo Pediatrics vol 91no 6 pp 1116ndash1120 1993
[41] M P Wajnrajch J M Gertner Z Huma et al ldquoEvaluationof growth and hormonal status in patients referred to theinternational fanconi anemia registryrdquo Pediatrics vol 107 no4 I pp 744ndash754 2001
[42] N Giri D L Batista B P Alter and C A Stratakis ldquoEndocrineabnormalities in patients with fanconi anemiardquo The Journal ofClinical Endocrinology amp Metabolism vol 92 no 7 pp 2624ndash2631 2007
[43] S R Rose K C Myers M M Rutter et al ldquoEndocrine phe-notype of children and adults with Fanconi anemiardquo PediatricBlood amp Cancer vol 59 no 4 pp 690ndash696 2012
[44] A D Auerbach B Adler and R S K Chaganti ldquoPrenatal andpostnatal diagnosis and carrier detection of Fanconi anemia bya cytogeneticmethodrdquoPediatrics vol 67 no 1 pp 128ndash135 1981
[45] A D Auerbach M Sagi and B Adler ldquoFanconi anemiaPrenatal diagnosis in 30 fetuses at riskrdquo Pediatrics vol 76 no5 pp 794ndash800 1985
[46] L Faivre M F Portnoı G Pals et al ldquoShould chromosomebreakage studies be performed in patients with VACTERLassociationrdquo American Journal of Medical Genetics vol 137 no1 pp 55ndash58 2005
[47] B P Alter P S Rosenberg and L C Brody ldquoClinicaland molecular features associated with biallelic mutations inFANCD1BRCA2rdquo Journal ofMedical Genetics vol 44 no 1 pp1ndash9 2007
14 BioMed Research International
[48] K Myers S M Davies R E Harris et al ldquoThe clinicalphenotype of children with Fanconi anemia caused by biallelicFANCD1BRCA2mutationsrdquo Pediatric Blood amp Cancer vol 58no 3 pp 462ndash465 2012
[49] B G Yoon H N Kim U J Han et al ldquoLong-term follow-up of Fanconi anemia Clinical manifestation and treatmentoutcomerdquo Korean Journal of Pediatrics vol 57 no 3 pp 125ndash134 2014
[50] J G Hall ldquoReview and hypothesis Syndromes with severeintrauterine growth restriction and very short stature - Are theyrelated to the epigeneticmechanism(s) of fetal survival involvedin the developmental origins of adult health and diseaserdquoAmerican Journal of Medical Genetics Part A vol 152 no 2 pp512ndash527 2010
[51] A Petryk R K Shankar N Giri et al ldquoEndocrine disordersin Fanconi anemia Recommendations for screening and treat-mentrdquoThe Journal of Clinical Endocrinology ampMetabolism vol100 no 3 pp 803ndash811 2015
[52] S R RoseMM Rutter RMueller et al ldquoBonemineral densityis normal in children with Fanconi anemiardquo Pediatric Blood ampCancer vol 57 no 6 pp 1034ndash1038 2011
[53] A Petryk L E Polgreen J L Barnum et al ldquoBone mineraldensity in childrenwith fanconi anemia after hematopoietic celltransplantationrdquo Biology of Blood and Marrow Transplantationvol 21 no 5 pp 894ndash899 2015
[54] R Purkait A Mukherji S Datta and R Bhadra ldquoRenal arterystenosis An unusual etiology of hypertensive encephalopathyin a childwith fanconi anemiardquo Saudi Journal of KidneyDiseasesand Transplantation vol 26 no 4 pp 778ndash782 2015
[55] K H Chrzanowska H Gregorek B Dembowska-BaginskaM A Kalina and M Digweed ldquoNijmegen breakage syndrome(NBS)rdquoOrphanet Journal of Rare Diseases vol 7 article 13 2012
[56] L C Riches A M Lynch and N J Gooderham ldquoEarly eventsin the mammalian response to DNA double-strand breaksrdquoMutagenesis vol 23 no 5 pp 331ndash339 2008
[57] K Chrzanowska M Kalina H Rysiewski et al ldquoGrowthpattern in patients withNijmegen breakage syndrome evidencefroma longitudinal studyrdquoHormoneResearch in Paediatrics vol74 article S38 2010
[58] Group TINBSS ldquoNijmegen breakage syndromerdquo Archives ofDisease in Childhood vol 82 pp 400ndash406 2000
[59] M Digweed and K Sperling ldquoNijmegen breakage syndromeClinical manifestation of defective response to DNA double-strand breaksrdquo DNA Repair vol 3 no 8-9 pp 1207ndash1217 2004
[60] E Seemanova ldquoAn increased risk for malignant neoplasmsin heterozygotes for a syndrome of microcephaly normalintelligence growth retardation remarkable facies immun-odeficiency and chromosomal instabilityrdquo Mutation ResearchReviews in Genetic Toxicology vol 238 no 3 pp 321ndash324 1990
[61] K H Chrzanowska M Szarras-Czapnik M Gajdulewicz et alldquoHigh prevalence of primary ovarian insufficiency in girls andyoung women with Nijmegen breakage syndrome Evidencefrom a longitudinal studyrdquoThe Journal of Clinical Endocrinologyamp Metabolism vol 95 no 7 pp 3133ndash3140 2010
[62] C M R Weemaes T W J Hustinx J M J C Scheres P J JV Munster J A J M Bakkeren and R D F M Taalman ldquoAnew chromosomal instability disorder The nijmegen breakagesyndromerdquo Acta Paediatrica Scandinavica vol 70 no 4 pp557ndash564 1981
[63] A J Green J R W Yates A M R Taylor et al ldquoSevere micro-cephaly with normal intellectual development The Nijmegen
breakage syndromerdquo Archives of Disease in Childhood vol 73no 5 pp 431ndash434 1995
[64] D Gupta and A Nagarkar ldquoSpeech impairment in Nijmegenbreakage syndrome A rare anomalyrdquo International Journal ofPediatric Otorhinolaryngology vol 73 no 6 pp 873ndash875 2009
[65] P Muschke H Gola R Varon et al ldquoRetrospective diagnosisand subsequent prenatal diagnosis of Nijmegen breakage syn-dromerdquo Prenatal Diagnosis vol 24 no 2 pp 111ndash113 2004
[66] S Pasic M Cupic T Jovanovic S Djukic M Kavaric andI Lazarevic ldquoNijmegen breakage syndrome and chronic pol-yarthritisrdquo Italian Journal of Pediatrics vol 39 no 1 article no59 2013
[67] J P Patel J M Puck R Srinivasan et al ldquoNijmegen BreakageSyndrome Detected by Newborn Screening for T Cell ReceptorExcision Circles (TRECs)rdquo Journal of Clinical Immunology vol35 no 2 pp 227ndash233 2015
[68] I Demuth and M Digweed ldquoThe clinical manifestation of adefective response to DNA double-strand breaks as exemplifiedby Nijmegen breakage syndromerdquoOncogene vol 26 no 56 pp7792ndash7798 2007
[69] H Arora A H Chacon S Choudhary et al ldquoBloom syn-dromerdquo International Journal of Dermatology vol 53 no 7 pp798ndash802 2014
[70] C de Renty and N A Ellis ldquoBloomrsquos syndrome Why not pre-mature aging A comparison of the BLM andWRN helicasesrdquoAgeing Research Reviews vol 33 pp 36ndash51 2017
[71] C Keller K R Keller S B Shew and S E Plon ldquoGrowthdeficiency and malnutrition in Bloom syndromerdquo Journal ofPediatrics vol 134 no 4 pp 472ndash479 1999
[72] A Diaz M G Vogiatzi M M Sanz and J German ldquoEval-uation of short stature carbohydrate metabolism and otherendocrinopathies in Bloomrsquos syndromerdquo Hormone Researchvol 66 no 3 pp 111ndash117 2006
[73] C Ling J Huang Z Yan et al ldquoBloom syndrome complexpromotes FANCM recruitment to stalled replication forksand facilitates both repair and traverse of DNA interstrandcrosslinksrdquo Cell Discovery vol 2 article 16047 2016
[74] J S Renes R H Willemsen A Wagner M J J Finken and AC SHokken-Koelega ldquoBloom syndrome in short children bornsmall for gestational age A challenging diagnosisrdquoThe Journalof Clinical EndocrinologyampMetabolism vol 98 no 10 pp 3932ndash3938 2013
[75] M Maciejczyk B Mikoluc B Pietrucha et al ldquoOxidativestress mitochondrial abnormalities and antioxidant defense inAtaxia-telangiectasia Bloom syndrome andNijmegen breakagesyndromerdquo Redox Biology vol 11 pp 375ndash383 2017
[76] R M Brosh M Bellani Y Liu and M M Seidman ldquoFanconiAnemia A DNA repair disorder characterized by accelerateddecline of the hematopoietic stem cell compartment and otherfeatures of agingrdquo Ageing Research Reviews vol 33 pp 67ndash752017
[77] S Yan M Sorrell and Z Berman ldquoFunctional interplay be-tween ATMATR-mediated DNA damage response and DNArepair pathways in oxidative stressrdquo Cellular and Molecular LifeSciences vol 71 no 20 pp 3951ndash3967 2014
[78] L M M Nardozza A C R Caetano A C P Zamarian etal ldquoFetal growth restriction current knowledgerdquo Archives ofGynecology and Obstetrics vol 295 no 5 pp 1061ndash1077 2017
[79] M Tomas Vila J P Verdu M R Piera and C O AlonsoldquoNijmegen breakage syndrome phenotype a disorder to con-sider in the diagnosis ofmicrocephalyrdquoAnales De Pediatria vol74 pp 58ndash60 2011
Submit your manuscripts athttpswwwhindawicom
Stem CellsInternational
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
MEDIATORSINFLAMMATION
of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Behavioural Neurology
EndocrinologyInternational Journal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Disease Markers
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
BioMed Research International
OncologyJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Oxidative Medicine and Cellular Longevity
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
PPAR Research
The Scientific World JournalHindawi Publishing Corporation httpwwwhindawicom Volume 2014
Immunology ResearchHindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Journal of
ObesityJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Computational and Mathematical Methods in Medicine
OphthalmologyJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Diabetes ResearchJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Research and TreatmentAIDS
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Gastroenterology Research and Practice
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Parkinsonrsquos Disease
Evidence-Based Complementary and Alternative Medicine
Volume 2014Hindawi Publishing Corporationhttpwwwhindawicom

BioMed Research International 9
(a) (b)
Figure 7 Sister chromatid exchange in cells from a healthy individual (a) and from a BLM patient (b)
support the fact that growth retardation in NBS is a prenatalphenomenon
Nibrin has been found to have essential functions inthe regulation of the cell cycle which translates into anabsolute need for this protein for cell proliferation [68]It would seem logical that mutations of the NBN genethat compromise the appropriate function of nibrin wouldlead to abnormal growth when thought from an organismperspective Mechanistically speaking poor cellular growthcaused by mutations in a particular gene can be thought ofas the main explanation for the growth restricted phenotypebut it has been shown that mutations in other DDR genesthat share the cellular phenotype of poor growth like ATMdo not replicate the compromised growth phenotype atthe organism level growth retardation is absent in ataxiatelangiectasia (AT)This data suggests that there are certainlyother contributing factors to the abnormal growth phenotypeseen in NBS patients [58]
74 Bloom Syndrome Bloom syndrome (BS) is an autosomalrecessive disorder caused by homozygous or compoundheterozygous mutations in the BLM gene (15q261) thatencodes the RecQL3 helicase BLM has a critical role inthe maintenance of genome stability acting at the interfacebetweenDNAreplication recombination and repair [69 70]To date over sixty different mutations including nonsenseand missense have been identified all of them result inthe inactivation of BLM and the consequent loss of itshelicase activity The BLM gene encodes a 1417 amino acidnuclear protein its expression peaks during the S and G
2M
phases of the cell cycle which is consistent with its rolein DNA replication and recombination BLM specificallyunwinds structures like forked DNA duplexes RNA-DNAheteroduplexes and R-Loops which explains its importanceduring replication fork progression and transcription besidesit is central for Holliday Junctions (HJs) dissolution forHR The dissolution of HJs by the topoisomerase III120572-BLMcomplex cannot be replaced by any other RecQ helicase inthe family [69 70] It has also been found to have a role in
the annealing activity of the ssDNA the proper sister chro-matid segregation during mitosis and telomere maintenance[70]
BLM can have both pro- and antirecombinogenic func-tions that are regulated by posttranslational modificationsincluding phosphorylation sumoylation and ubiquitination[70]
BLM also enables sister chromatid segregation by pro-cessing unresolved replication intermediates that manifest inmitosis as ultrafine DNA bridges (UFBs) and together withtopoisomerase III120572 RMI1 and RMI2 localizes to UFBs inanaphase BML deficient cells exhibit and increase frequencyof UFBs suggesting a role of BLM in the resolution ofthese structures Failure to resolve these UFBs leads to DNAbreakage as mitosis proceeds [70]
Therefore BS cells are characterized by an increasein chromosomal aberrations including chromatid gapsand breaks telomere associations and quadriradial chro-mosomes resulting from unsolved recombination betweenhomologous chromosomes BS cells exhibit increased muta-tion rates and the genomic instability includes elevatedmitotic HR and unequal sister chromatid exchange (SCEs)(Figure 7) Perhaps the most characteristic feature is the overtenfold increase in SCEs which results from crossover eventsduring HR repair of damage replication forks [50 69 70]
Clinically the more striking BS feature is IUGR averagebirth weight at term is 1850 g and birth length is 44 cmFor both boys and girls weight and length in BS are morethan two standard deviations below normal indicating thatgrowth retardation has a prenatal origin At postnatal agesheight remains below the normal range and is accompaniedby a paucity of subcutaneous fat Average adult height inmales has been found to be 148 cm (130ndash162 cm) whilein females it has been reported to be 139 cm (122ndash151 cm)[50 70 71]
BS patients have overall proportionated short staturebut the head is reported to be small and narrow relativelyto the body size it is described as mild microcephalyand is accompanied by malar hypoplasia Patients have
10 BioMed Research International
Figure 8 Bloomsyndromepatient inwhom the characteristicmalarerythema is present
been described to have a high pitched voice [50 70] Theskin appears normal at birth but in the first or secondyear of life in response to sun exposure children developan erythematous rash with a butterfly distribution in themalar area and the back of hands and feet The rash caninclude telangiectasia The severity varies between patientssome can even lose their eyelashes and develop blisteringaround the mouth The presence of cafe-au-lait spots andhypopigmented areas of skin associated with contiguoushyperpigmented areas is common (Figure 8) Intellectualabilitiesmay be limited in some patients and normal in others[50 70]
Other clinical conditions reported in BS patients are gas-troesophageal reflux and diarrhea in infants mild immuno-logical deficiency with frequent episodes of otitis mediaazoospermia or severe oligospermia in males and prema-ture cessation of menstruation in females minor anatomicdefects and increased risk for neoplasia which is the maincause of dead in BS [70] Another common medical con-dition in BS is diabetes mellitus associated with impairedglucose tolerance and insulin resistance it has been reportedin up to 16 of patients [70] According to data fromthe Bloomrsquos Syndrome Registry diabetes in these patientstends to begin early with a mean age at diagnosis of 266years It is not associated with ketosis and it does nothave the classical hereditary pattern seen in type 2 diabetes[50 72]
Short stature in BS is not due to hormonal causes sincethe size of cells in persons with BS is normal it has beenhypothesized that there are fewer of them due to either adecrease in the cell division rate an increase in apoptosis oreven a combination of both BS cells have troublemeeting thedemands of fast cell divisions encountered in tissues duringembryonic development The leading hypothesis suggeststhat problems arising during DNA synthesis require a longerS phase to overcome the challenge which translates intoslowing of the cell division rate and an increase in apoptosis[70]
8 Concluding Remarks
This review has focused on discussing phenotypes of CISin which there is a prenatal alteration of growth The foursyndromes discussed here are rare diseases whose prevalenceis difficult to calculate since appropriate identification anddiagnosis of affected individuals among the general popula-tion are not straightforward It is important to note that theavailable information on the natural history of FA NBS andBS comes from the analysis of several patients that participatein registries This strategy results in detailed informationthat permits a better analysis of the clinical phenotype ofthese rare diseases Meanwhile available data of SS is moreanecdotic which results in a nonsystematic gathering ofinformation which is thus frequently incomplete
From the available clinical data of these CIS it is evidentthat growth is not affected in the same extent for all ofthese syndromes the phenotypes that exhibit a more severelystagnated perinatal growth are BS and SS The severe growthdelay reported in these patients has been described as apathognomonic sign of these diagnoses In patients withFA perinatal growth can also be severely affected but notevery FA patient shows this manifestation Finally NBShas been described to have growth retardation of prenatalorigin of mild severity almost within the lower normal range(Figure 9) The cephalic circumference can be affected in allof these syndromes severe microcephaly is pathognomonicin SS and NBS it is described as mild for BS patients and it isfound in less than half of FA patients (Table 2)
When trying to understand why a subset of CIS showsprenatal growth retardation it could be alleged that theintrinsic chromosomal instability is responsible for it Butthis would not explain why prenatal growth retardation isnot a universal CIS feature for example ataxia telangiectasiapatients who have biallelic mutations in the ATMkinase genedo not show prenatal growth delay It strikes that a molecularcommon feature shared by the prenatal growth retardationSIC phenotypes is that they are caused by mutations ingenes that are necessary for an appropriate response to DSBsduring the S phase of the cell cycle The molecular defectin SS affects the functioning of ATR the preferred DDRtransducing kinase used by highly replicating ESCs TheFABRCA pathway which is affected in patients with FAdetects ICLs upon replication fork arrest Nibrin the proteinaffected in patients with NBS is induced during S phasefor the detection of DSBs And the BS helicase forms aFANCM-BLM complex needed to sense ICLs during S phase[73] It could then be argued that altered DNA replicationis an important factor for the development of intrauterinegrowth restriction in these CIS Nevertheless it must be keptin mind that the inherent chromosome instability found inthese syndromes may also be affecting normal growth in thepatients [27 43 57 60 71]
Being small for gestational age has been associatedwith a higher risk of noncommunicable adult diseases likeglucose homeostasis disorders dyslipidemia hypertensionand others It has been proposed that fetal reprogrammingto enhance fetal survival despite the risk for adult onsetdiseases is an outcome that does not take into account
BioMed Research International 11
Table 2 Growth features of chromosomal instability syndromes
SyndromeldquoLocirdquo At-term birth weightheight Microcephaly Adult height Adult onset diseases
Seckel SyndromeldquoATR3q23rdquo
Birth weight below minus3 SD(2055 g)
Severeminus4 SD
Postnatal growth retardation(below minus5 SD) Not reported
Fanconi anemialdquo21 FANC genesrdquo
Median weight 202 kg(15ndash26 kg) In 20ndash50
50ndash60 of patients with medianheight lt minus18 SDSWomen minus34 SDSMen minus44 SDS
CancerDiabetes mellitusDyslipidemia
Altered bone mineral densityNijmegen BreakageSyndromeldquoNBN8q21rdquo
Mean weightheight girls27 kg514 cm
Mean weightheight boys28 kg523 cm
100 Mean height for women minus18 SDSMean height for men minus23 Cancer
Bloom SyndromeldquoBLM15q261rdquo
Mean weight 189 kg plusmn 035 kg forboys
Mean weight 187 kg plusmn 035 kg forgirls
Mean height 434 cm plusmn 44 cm forboys
Mean height 438 cm plusmn 28 cm forgirls
Mildmicrocephaly
Mean height 1455 cm plusmn 76 cmmales
Mean height 1415 cm plusmn 61 cm forfemales
CancerDiabetes mellitus
See [27 33 40 43 50 57 69]
45 53
43245
Height (cm)
Weight (kg)
Percentile 3 Percentile 97Percentile 50495
33
Normalindividual
Mean 2055
SeckelSyndrome
2615Median 202
FanconiAnemia
Mean 51
Mean 275
Nijmegen BreakageSyndrome
38 49
24513
Mean 436
Mean 188
BloomSyndrome
Figure 9 Anthropometric features at birth of chromosome instability syndromes with perinatal growth retardation Comparison of theavailable growth data from SS FA NBS and BS syndrome against birth data from the WHOrsquos growth standards for infants Although meanheight and weight values of NBS patients are found to be within normal percentiles according to WHO standards there are several authorswho refer to prenatal growth restriction [55 63 65 79]
the reason for the prenatal growth restraint [50 72 74] Itmust be kept in mind that noncommunicable diseases aremultifactorial entities in which genetic and environmentalfactors converge and their cause cannot be attributed to asingle explanation However when growth restriction is akey feature in syndromes with chromosome instability the
possibility that cell hypoplasia due to DNA repair malfunc-tion is contributing to the growth restriction phenotypemustbe contemplated Moreover since none of these adult onsetdiseases is reported as an inherent element of the SS and NBSphenotypes the direct connection between low birth weightand adult noncommunicable diseases is less of a straight
12 BioMed Research International
shot Furthermore there are other Mendelian syndromeswith mutations in DNA repair genes that characteristicallyshow adult noncommunicable diseases but do not haveIUGR such is the case for Werner syndrome a progeroiddisease caused by biallelic mutations in another RecQ heli-case (RecQ4) that clinically presents with postnatal shortstature and a prevalence of type 2 diabetes mellitus of 70[50 70 74]
Natural history of FA NBS and BS documented throughthe existing patient registries has allowed the identificationof noncommunicable diseases to be a part of the clinicalspectrum of these syndromes (Table 2) Meanwhile from theinformation available through SS case reports no adult onsetdisease has been found to be part of this phenotype To thebest of our knowledge the direct investigation of nonevidentendocrinologic alterations like glucose homeostasis or dys-lipidemia has not been directlymade in SS patients For a raredisease like SS such a study can only be done if a fairly largegroup of patients like the one found in registries is availableIf such a study was to be performed hidden features in SSpatients could be unraveled
Oxidative stress sensibility is a cellular feature sharedby all the SIC syndromes with IUGR that could contributeto the explanation of the premature development of non-communicable adult diseases in these patients Reports haveshown that BS and NBS cells have endogenous reactiveoxygen species (ROS) overproduction and an impairedmitochondrial homeostasis [75] it is also well known thatFA cells show increased levels of oxidative damage [3876] and there is evidence that oxidative stress can activateATR-mediated checkpoint signaling [77] Since this kind ofdamage has soundly been related to age-associated diseasesthat result from tissue degeneration exacerbated oxidativedamage found in these syndromes could result in cellu-lar aging that manifests as overall premature aging withparticular symptoms like glucose homeostasis alterations[76 77]
Fetal growth restriction is a multifactorial conditionwhere wide arrays of factors converge Fetal aspects inparticular those affecting the genetic constitution of thefetus have been recognized to play an important role Ithas been demonstrated that chromosomal abnormalities andmonogenic syndromes caused by mutations in genes thatparticipate in growth or metabolic pathways directly affectfetal growth [78] Even though they are rare entities CISappear as another group of monogenic pathologies thatbroaden the list of genetic fetal factors of fetal growthrestriction
Consent
The necessary consent for the publication of the photographswas obtained
Conflicts of Interest
The authors declare that there are no conflicts of interestregarding the publication of this paper
Authorsrsquo Contributions
The three authors contributed equally andwrote the first draftof the paper The final version was approved by everyone
Acknowledgments
This paper is supported by SEP-CONACYT Project 243102Benilde Garcıa-de Teresa received the 574025 scholarshipfrom CONACYT The paper is also supported by PAPIIT-UNAM Project IA202615 and Fondos Federales INP Project41-2014
References
[1] K W J Derks J H J Hoeijmakers and J Pothof ldquoThe DNAdamage response The omics era and its impactrdquo DNA Repairvol 19 pp 214ndash220 2014
[2] S P Jackson and J Bartek ldquoThe DNA-damage response inhuman biology and diseaserdquoNature vol 461 no 7267 pp 1071ndash1078 2009
[3] J H J Hoeijmakers ldquoDNA damage aging and cancerrdquo TheNew England Journal of Medicine vol 361 no 15 pp 1475ndash14852009
[4] G Spivak ldquoNucleotide excision repair in humansrdquoDNARepairvol 36 pp 13ndash18 2015
[5] J Vijg XDong BMilholland andL Zhang ldquoGenome instabil-ity a conserved mechanism of ageingrdquo Essays in Biochemistryvol 61 no 3 pp 305ndash315 2017
[6] J I Garaycoechea and K J Patel ldquoWhy does the bone marrowfail in Fanconi anemiardquo Blood vol 123 no 1 pp 26ndash34 2014
[7] R Ceccaldi B Rondinelli andAD DrsquoAndrea ldquoRepair PathwayChoices andConsequences at theDouble-Strand BreakrdquoTrendsin Cell Biology vol 26 no 1 pp 52ndash64 2016
[8] R Biehs M Steinlage O Barton et al ldquoDNA Double-StrandBreak Resection Occurs during Non-homologous End Joiningin G1 but Is Distinct from Resection during HomologousRecombinationrdquo Molecular Cell vol 65 no 4 pp 671ndash684e52017
[9] A Ciccia and S J Elledge ldquoTheDNAdamage response makingit safe to play with knivesrdquoMolecular Cell vol 40 no 2 pp 179ndash204 2010
[10] L H Pearl A C Schierz S E Ward B Al-Lazikani and F MG Pearl ldquoTherapeutic opportunities within the DNA damageresponserdquo Nature Reviews Cancer vol 15 no 3 pp 166ndash1802015
[11] S-F Yang C-W Chang R-J Wei Y-L Shiue S-N Wang andY-T Yeh ldquoInvolvement of DNA damage response pathways inhepatocellular carcinomardquo BioMed Research International vol2014 Article ID 153867 2014
[12] M He W Zhou C Li and M Guo ldquoMicroRNAs DNAdamage response and cancer treatmentrdquo International Journalof Molecular Sciences vol 17 no 12 article no 2087 2016
[13] K A Cimprich and D Cortez ldquoATR an essential regulator ofgenome integrityrdquo Nature Reviews Molecular Cell Biology vol9 no 8 pp 616ndash627 2008
[14] B M Sirbu and D Cortez ldquoDNA damage response three levelsof DNA repair regulationrdquo Cold Spring Harbor Perspectives inBiology vol 5 article a012724 no 8 2013
BioMed Research International 13
[15] C Beck I Robert B Reina-San-Martin V Schreiber andF Dantzer ldquoPoly(ADP-ribose) polymerases in double-strandbreak repair focus on PARP1 PARP2 and PARP3rdquo Experimen-tal Cell Research vol 329 no 1 pp 18ndash25 2014
[16] D W Meek ldquoTumour suppression by p53 a role for the DNAdamage responserdquo Nature Reviews Cancer vol 9 no 10 pp714ndash723 2009
[17] A Rodrıguez L Torres U Juarez et al ldquoFanconi anemiacells with unrepaired DNA damage activate components of thecheckpoint recovery processrdquo Theoretical Biology and MedicalModelling vol 12 no 1 article 11 2015
[18] H Wang X Zhang L Teng and R J Legerski ldquoDNA damagecheckpoint recovery and cancer developmentrdquo ExperimentalCell Research vol 334 no 2 pp 350ndash358 2015
[19] P A Jeggo L H Pearl and A M Carr ldquoDNA repair genomestability and cancer A historical perspectiverdquo Nature ReviewsCancer vol 16 no 1 pp 35ndash42 2016
[20] F S Alkuraya ldquoPrimordial dwarfism An updaterdquo CurrentOpinion in Endocrinology Diabetes and Obesity vol 22 no 1pp 55ndash64 2015
[21] P Fortini C Ferretti and E Dogliotti ldquoThe response to DNAdamage during differentiation pathways and consequencesrdquoMutation ResearchmdashFundamental and Molecular Mechanismsof Mutagenesis vol 743-744 pp 160ndash168 2013
[22] B R Adams S E Golding R R Rao and K Valerie ldquoDynamicdependence on ATR and ATM for double-Strand break repairin human embryonic stem cells and neural descendantsrdquo PLoSONE vol 5 article e10001 no 4 2010
[23] A Klingseisen and A P Jackson ldquoMechanisms and pathways ofgrowth failure in primordial dwarfismrdquo Genes amp Developmentvol 25 no 19 pp 2011ndash2024 2011
[24] H Mokrani-Benhelli L Gaillard P Biasutto et al ldquoPrimaryMicrocephaly Impaired DNA Replication and Genomic Insta-bility Caused by Compound Heterozygous ATR MutationsrdquoHuman Mutation vol 34 no 2 pp 374ndash384 2013
[25] M OrsquoDriscoll A R Gennery J Seidel P Concannon and PA Jeggo ldquoAn overview of three new disorders associated withgenetic instability LIG4 syndrome RS-SCID and ATR-Seckelsyndromerdquo DNA Repair vol 3 no 8-9 pp 1227ndash1235 2004
[26] P Khetarpal S Das I Panigrahi and A Munshi ldquoPrimordialdwarfism overview of clinical and genetic aspectsrdquo MolecularGenetics and Genomics vol 291 no 1 pp 1ndash15 2016
[27] TOgi SWalker T Stiff et al ldquoIdentification of the First ATRIP-Deficient Patient and Novel Mutations in ATRDefine a ClinicalSpectrum for ATR-ATRIP Seckel Syndromerdquo PLoS Geneticsvol 8 no 11 Article ID e1002945 2012
[28] A Verloes S Drunat and P Gressens Primary autosomalrecessive microcephalies and Seckel syndrome spectrum disor-ders 2013
[29] A D Brown B W Sager A Gorthi S S Tonapi E J Brownand A J R Bishop ldquoATR suppresses endogenous DNA damageand allows completion of homologous recombination repairrdquoPLoS ONE vol 9 article e91222 no 3 2014
[30] E J Brown and D Baltimore ldquoEssential and dispensable rolesof ATR in cell cycle arrest and genome maintenancerdquo Genes ampDevelopment vol 17 no 5 pp 615ndash628 2003
[31] B Fitzgerald M OrsquoDriscoll K Chong S Keating and PShannon ldquoNeuropathology of fetal stage Seckel syndromeA case report providing a morphological correlate for theemerging molecular mechanismsrdquo Brain amp Development vol34 no 3 pp 238ndash243 2012
[32] L I Mullee and C G Morrison ldquoCentrosomes in the DNAdamage responsemdashthe hub outside the centrerdquo ChromosomeResearch vol 24 no 1 pp 35ndash51 2016
[33] K M Takikawa A Kikuchi A Yokoyama et al ldquoPerinatalfindings of Seckel syndrome A case report of a fetus showingprimordial dwarfism and severe microcephalyrdquo Fetal Diagnosisand Therapy vol 24 no 4 pp 405ndash408 2009
[34] Y Ruzankina C Pinzon-Guzman A Asare et al ldquoDeletion ofthe Developmentally Essential Gene ATR in Adult Mice Leadsto Age-Related Phenotypes and Stem Cell Lossrdquo Cell Stem Cellvol 1 no 1 pp 113ndash126 2007
[35] N E Mamrak A Shimamura and N G Howlett ldquoRecentdiscoveries in the molecular pathogenesis of the inherited bonemarrow failure syndrome Fanconi anemiardquo Blood Reviews vol31 no 3 pp 93ndash99 2017
[36] B P Alter ldquoDiagnosis Genetics and Management of InheritedBone Marrow Failure Syndromesrdquo International Journal ofHematology vol 2007 no 1 pp 29ndash39 2007
[37] L B Pontel I V Rosado G Burgos-Barragan et al ldquoEndoge-nous Formaldehyde Is a Hematopoietic Stem Cell Genotoxinand Metabolic Carcinogenrdquo Molecular Cell vol 60 no 1 pp177ndash188 2015
[38] G Pagano P Degan M DrsquoIschia et al ldquoOxidative stress asa multiple effector in Fanconi anaemia clinical phenotyperdquoEuropean Journal of Haematology vol 75 no 2 pp 93ndash1002005
[39] P FGiampietro P CVerlander J GDavis andADAuerbachldquoDiagnosis of Fanconi anemia in patients without congenitalmalformations An International Fanconi Anemia Registrystudyrdquo American Journal of Medical Genetics vol 68 no 1 pp58ndash61 1997
[40] P F Giampietro B Adler-Brecher P C Verlander S GPavlakis J G Davis and A D Auerbach ldquoThe need for moreaccurate and timely diagnosis in Fanconi anemia A report fromthe International Fanconi Anemia Registryrdquo Pediatrics vol 91no 6 pp 1116ndash1120 1993
[41] M P Wajnrajch J M Gertner Z Huma et al ldquoEvaluationof growth and hormonal status in patients referred to theinternational fanconi anemia registryrdquo Pediatrics vol 107 no4 I pp 744ndash754 2001
[42] N Giri D L Batista B P Alter and C A Stratakis ldquoEndocrineabnormalities in patients with fanconi anemiardquo The Journal ofClinical Endocrinology amp Metabolism vol 92 no 7 pp 2624ndash2631 2007
[43] S R Rose K C Myers M M Rutter et al ldquoEndocrine phe-notype of children and adults with Fanconi anemiardquo PediatricBlood amp Cancer vol 59 no 4 pp 690ndash696 2012
[44] A D Auerbach B Adler and R S K Chaganti ldquoPrenatal andpostnatal diagnosis and carrier detection of Fanconi anemia bya cytogeneticmethodrdquoPediatrics vol 67 no 1 pp 128ndash135 1981
[45] A D Auerbach M Sagi and B Adler ldquoFanconi anemiaPrenatal diagnosis in 30 fetuses at riskrdquo Pediatrics vol 76 no5 pp 794ndash800 1985
[46] L Faivre M F Portnoı G Pals et al ldquoShould chromosomebreakage studies be performed in patients with VACTERLassociationrdquo American Journal of Medical Genetics vol 137 no1 pp 55ndash58 2005
[47] B P Alter P S Rosenberg and L C Brody ldquoClinicaland molecular features associated with biallelic mutations inFANCD1BRCA2rdquo Journal ofMedical Genetics vol 44 no 1 pp1ndash9 2007
14 BioMed Research International
[48] K Myers S M Davies R E Harris et al ldquoThe clinicalphenotype of children with Fanconi anemia caused by biallelicFANCD1BRCA2mutationsrdquo Pediatric Blood amp Cancer vol 58no 3 pp 462ndash465 2012
[49] B G Yoon H N Kim U J Han et al ldquoLong-term follow-up of Fanconi anemia Clinical manifestation and treatmentoutcomerdquo Korean Journal of Pediatrics vol 57 no 3 pp 125ndash134 2014
[50] J G Hall ldquoReview and hypothesis Syndromes with severeintrauterine growth restriction and very short stature - Are theyrelated to the epigeneticmechanism(s) of fetal survival involvedin the developmental origins of adult health and diseaserdquoAmerican Journal of Medical Genetics Part A vol 152 no 2 pp512ndash527 2010
[51] A Petryk R K Shankar N Giri et al ldquoEndocrine disordersin Fanconi anemia Recommendations for screening and treat-mentrdquoThe Journal of Clinical Endocrinology ampMetabolism vol100 no 3 pp 803ndash811 2015
[52] S R RoseMM Rutter RMueller et al ldquoBonemineral densityis normal in children with Fanconi anemiardquo Pediatric Blood ampCancer vol 57 no 6 pp 1034ndash1038 2011
[53] A Petryk L E Polgreen J L Barnum et al ldquoBone mineraldensity in childrenwith fanconi anemia after hematopoietic celltransplantationrdquo Biology of Blood and Marrow Transplantationvol 21 no 5 pp 894ndash899 2015
[54] R Purkait A Mukherji S Datta and R Bhadra ldquoRenal arterystenosis An unusual etiology of hypertensive encephalopathyin a childwith fanconi anemiardquo Saudi Journal of KidneyDiseasesand Transplantation vol 26 no 4 pp 778ndash782 2015
[55] K H Chrzanowska H Gregorek B Dembowska-BaginskaM A Kalina and M Digweed ldquoNijmegen breakage syndrome(NBS)rdquoOrphanet Journal of Rare Diseases vol 7 article 13 2012
[56] L C Riches A M Lynch and N J Gooderham ldquoEarly eventsin the mammalian response to DNA double-strand breaksrdquoMutagenesis vol 23 no 5 pp 331ndash339 2008
[57] K Chrzanowska M Kalina H Rysiewski et al ldquoGrowthpattern in patients withNijmegen breakage syndrome evidencefroma longitudinal studyrdquoHormoneResearch in Paediatrics vol74 article S38 2010
[58] Group TINBSS ldquoNijmegen breakage syndromerdquo Archives ofDisease in Childhood vol 82 pp 400ndash406 2000
[59] M Digweed and K Sperling ldquoNijmegen breakage syndromeClinical manifestation of defective response to DNA double-strand breaksrdquo DNA Repair vol 3 no 8-9 pp 1207ndash1217 2004
[60] E Seemanova ldquoAn increased risk for malignant neoplasmsin heterozygotes for a syndrome of microcephaly normalintelligence growth retardation remarkable facies immun-odeficiency and chromosomal instabilityrdquo Mutation ResearchReviews in Genetic Toxicology vol 238 no 3 pp 321ndash324 1990
[61] K H Chrzanowska M Szarras-Czapnik M Gajdulewicz et alldquoHigh prevalence of primary ovarian insufficiency in girls andyoung women with Nijmegen breakage syndrome Evidencefrom a longitudinal studyrdquoThe Journal of Clinical Endocrinologyamp Metabolism vol 95 no 7 pp 3133ndash3140 2010
[62] C M R Weemaes T W J Hustinx J M J C Scheres P J JV Munster J A J M Bakkeren and R D F M Taalman ldquoAnew chromosomal instability disorder The nijmegen breakagesyndromerdquo Acta Paediatrica Scandinavica vol 70 no 4 pp557ndash564 1981
[63] A J Green J R W Yates A M R Taylor et al ldquoSevere micro-cephaly with normal intellectual development The Nijmegen
breakage syndromerdquo Archives of Disease in Childhood vol 73no 5 pp 431ndash434 1995
[64] D Gupta and A Nagarkar ldquoSpeech impairment in Nijmegenbreakage syndrome A rare anomalyrdquo International Journal ofPediatric Otorhinolaryngology vol 73 no 6 pp 873ndash875 2009
[65] P Muschke H Gola R Varon et al ldquoRetrospective diagnosisand subsequent prenatal diagnosis of Nijmegen breakage syn-dromerdquo Prenatal Diagnosis vol 24 no 2 pp 111ndash113 2004
[66] S Pasic M Cupic T Jovanovic S Djukic M Kavaric andI Lazarevic ldquoNijmegen breakage syndrome and chronic pol-yarthritisrdquo Italian Journal of Pediatrics vol 39 no 1 article no59 2013
[67] J P Patel J M Puck R Srinivasan et al ldquoNijmegen BreakageSyndrome Detected by Newborn Screening for T Cell ReceptorExcision Circles (TRECs)rdquo Journal of Clinical Immunology vol35 no 2 pp 227ndash233 2015
[68] I Demuth and M Digweed ldquoThe clinical manifestation of adefective response to DNA double-strand breaks as exemplifiedby Nijmegen breakage syndromerdquoOncogene vol 26 no 56 pp7792ndash7798 2007
[69] H Arora A H Chacon S Choudhary et al ldquoBloom syn-dromerdquo International Journal of Dermatology vol 53 no 7 pp798ndash802 2014
[70] C de Renty and N A Ellis ldquoBloomrsquos syndrome Why not pre-mature aging A comparison of the BLM andWRN helicasesrdquoAgeing Research Reviews vol 33 pp 36ndash51 2017
[71] C Keller K R Keller S B Shew and S E Plon ldquoGrowthdeficiency and malnutrition in Bloom syndromerdquo Journal ofPediatrics vol 134 no 4 pp 472ndash479 1999
[72] A Diaz M G Vogiatzi M M Sanz and J German ldquoEval-uation of short stature carbohydrate metabolism and otherendocrinopathies in Bloomrsquos syndromerdquo Hormone Researchvol 66 no 3 pp 111ndash117 2006
[73] C Ling J Huang Z Yan et al ldquoBloom syndrome complexpromotes FANCM recruitment to stalled replication forksand facilitates both repair and traverse of DNA interstrandcrosslinksrdquo Cell Discovery vol 2 article 16047 2016
[74] J S Renes R H Willemsen A Wagner M J J Finken and AC SHokken-Koelega ldquoBloom syndrome in short children bornsmall for gestational age A challenging diagnosisrdquoThe Journalof Clinical EndocrinologyampMetabolism vol 98 no 10 pp 3932ndash3938 2013
[75] M Maciejczyk B Mikoluc B Pietrucha et al ldquoOxidativestress mitochondrial abnormalities and antioxidant defense inAtaxia-telangiectasia Bloom syndrome andNijmegen breakagesyndromerdquo Redox Biology vol 11 pp 375ndash383 2017
[76] R M Brosh M Bellani Y Liu and M M Seidman ldquoFanconiAnemia A DNA repair disorder characterized by accelerateddecline of the hematopoietic stem cell compartment and otherfeatures of agingrdquo Ageing Research Reviews vol 33 pp 67ndash752017
[77] S Yan M Sorrell and Z Berman ldquoFunctional interplay be-tween ATMATR-mediated DNA damage response and DNArepair pathways in oxidative stressrdquo Cellular and Molecular LifeSciences vol 71 no 20 pp 3951ndash3967 2014
[78] L M M Nardozza A C R Caetano A C P Zamarian etal ldquoFetal growth restriction current knowledgerdquo Archives ofGynecology and Obstetrics vol 295 no 5 pp 1061ndash1077 2017
[79] M Tomas Vila J P Verdu M R Piera and C O AlonsoldquoNijmegen breakage syndrome phenotype a disorder to con-sider in the diagnosis ofmicrocephalyrdquoAnales De Pediatria vol74 pp 58ndash60 2011
Submit your manuscripts athttpswwwhindawicom
Stem CellsInternational
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
MEDIATORSINFLAMMATION
of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Behavioural Neurology
EndocrinologyInternational Journal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Disease Markers
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
BioMed Research International
OncologyJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Oxidative Medicine and Cellular Longevity
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
PPAR Research
The Scientific World JournalHindawi Publishing Corporation httpwwwhindawicom Volume 2014
Immunology ResearchHindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Journal of
ObesityJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Computational and Mathematical Methods in Medicine
OphthalmologyJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Diabetes ResearchJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Research and TreatmentAIDS
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Gastroenterology Research and Practice
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Parkinsonrsquos Disease
Evidence-Based Complementary and Alternative Medicine
Volume 2014Hindawi Publishing Corporationhttpwwwhindawicom

10 BioMed Research International
Figure 8 Bloomsyndromepatient inwhom the characteristicmalarerythema is present
been described to have a high pitched voice [50 70] Theskin appears normal at birth but in the first or secondyear of life in response to sun exposure children developan erythematous rash with a butterfly distribution in themalar area and the back of hands and feet The rash caninclude telangiectasia The severity varies between patientssome can even lose their eyelashes and develop blisteringaround the mouth The presence of cafe-au-lait spots andhypopigmented areas of skin associated with contiguoushyperpigmented areas is common (Figure 8) Intellectualabilitiesmay be limited in some patients and normal in others[50 70]
Other clinical conditions reported in BS patients are gas-troesophageal reflux and diarrhea in infants mild immuno-logical deficiency with frequent episodes of otitis mediaazoospermia or severe oligospermia in males and prema-ture cessation of menstruation in females minor anatomicdefects and increased risk for neoplasia which is the maincause of dead in BS [70] Another common medical con-dition in BS is diabetes mellitus associated with impairedglucose tolerance and insulin resistance it has been reportedin up to 16 of patients [70] According to data fromthe Bloomrsquos Syndrome Registry diabetes in these patientstends to begin early with a mean age at diagnosis of 266years It is not associated with ketosis and it does nothave the classical hereditary pattern seen in type 2 diabetes[50 72]
Short stature in BS is not due to hormonal causes sincethe size of cells in persons with BS is normal it has beenhypothesized that there are fewer of them due to either adecrease in the cell division rate an increase in apoptosis oreven a combination of both BS cells have troublemeeting thedemands of fast cell divisions encountered in tissues duringembryonic development The leading hypothesis suggeststhat problems arising during DNA synthesis require a longerS phase to overcome the challenge which translates intoslowing of the cell division rate and an increase in apoptosis[70]
8 Concluding Remarks
This review has focused on discussing phenotypes of CISin which there is a prenatal alteration of growth The foursyndromes discussed here are rare diseases whose prevalenceis difficult to calculate since appropriate identification anddiagnosis of affected individuals among the general popula-tion are not straightforward It is important to note that theavailable information on the natural history of FA NBS andBS comes from the analysis of several patients that participatein registries This strategy results in detailed informationthat permits a better analysis of the clinical phenotype ofthese rare diseases Meanwhile available data of SS is moreanecdotic which results in a nonsystematic gathering ofinformation which is thus frequently incomplete
From the available clinical data of these CIS it is evidentthat growth is not affected in the same extent for all ofthese syndromes the phenotypes that exhibit a more severelystagnated perinatal growth are BS and SS The severe growthdelay reported in these patients has been described as apathognomonic sign of these diagnoses In patients withFA perinatal growth can also be severely affected but notevery FA patient shows this manifestation Finally NBShas been described to have growth retardation of prenatalorigin of mild severity almost within the lower normal range(Figure 9) The cephalic circumference can be affected in allof these syndromes severe microcephaly is pathognomonicin SS and NBS it is described as mild for BS patients and it isfound in less than half of FA patients (Table 2)
When trying to understand why a subset of CIS showsprenatal growth retardation it could be alleged that theintrinsic chromosomal instability is responsible for it Butthis would not explain why prenatal growth retardation isnot a universal CIS feature for example ataxia telangiectasiapatients who have biallelic mutations in the ATMkinase genedo not show prenatal growth delay It strikes that a molecularcommon feature shared by the prenatal growth retardationSIC phenotypes is that they are caused by mutations ingenes that are necessary for an appropriate response to DSBsduring the S phase of the cell cycle The molecular defectin SS affects the functioning of ATR the preferred DDRtransducing kinase used by highly replicating ESCs TheFABRCA pathway which is affected in patients with FAdetects ICLs upon replication fork arrest Nibrin the proteinaffected in patients with NBS is induced during S phasefor the detection of DSBs And the BS helicase forms aFANCM-BLM complex needed to sense ICLs during S phase[73] It could then be argued that altered DNA replicationis an important factor for the development of intrauterinegrowth restriction in these CIS Nevertheless it must be keptin mind that the inherent chromosome instability found inthese syndromes may also be affecting normal growth in thepatients [27 43 57 60 71]
Being small for gestational age has been associatedwith a higher risk of noncommunicable adult diseases likeglucose homeostasis disorders dyslipidemia hypertensionand others It has been proposed that fetal reprogrammingto enhance fetal survival despite the risk for adult onsetdiseases is an outcome that does not take into account
BioMed Research International 11
Table 2 Growth features of chromosomal instability syndromes
SyndromeldquoLocirdquo At-term birth weightheight Microcephaly Adult height Adult onset diseases
Seckel SyndromeldquoATR3q23rdquo
Birth weight below minus3 SD(2055 g)
Severeminus4 SD
Postnatal growth retardation(below minus5 SD) Not reported
Fanconi anemialdquo21 FANC genesrdquo
Median weight 202 kg(15ndash26 kg) In 20ndash50
50ndash60 of patients with medianheight lt minus18 SDSWomen minus34 SDSMen minus44 SDS
CancerDiabetes mellitusDyslipidemia
Altered bone mineral densityNijmegen BreakageSyndromeldquoNBN8q21rdquo
Mean weightheight girls27 kg514 cm
Mean weightheight boys28 kg523 cm
100 Mean height for women minus18 SDSMean height for men minus23 Cancer
Bloom SyndromeldquoBLM15q261rdquo
Mean weight 189 kg plusmn 035 kg forboys
Mean weight 187 kg plusmn 035 kg forgirls
Mean height 434 cm plusmn 44 cm forboys
Mean height 438 cm plusmn 28 cm forgirls
Mildmicrocephaly
Mean height 1455 cm plusmn 76 cmmales
Mean height 1415 cm plusmn 61 cm forfemales
CancerDiabetes mellitus
See [27 33 40 43 50 57 69]
45 53
43245
Height (cm)
Weight (kg)
Percentile 3 Percentile 97Percentile 50495
33
Normalindividual
Mean 2055
SeckelSyndrome
2615Median 202
FanconiAnemia
Mean 51
Mean 275
Nijmegen BreakageSyndrome
38 49
24513
Mean 436
Mean 188
BloomSyndrome
Figure 9 Anthropometric features at birth of chromosome instability syndromes with perinatal growth retardation Comparison of theavailable growth data from SS FA NBS and BS syndrome against birth data from the WHOrsquos growth standards for infants Although meanheight and weight values of NBS patients are found to be within normal percentiles according to WHO standards there are several authorswho refer to prenatal growth restriction [55 63 65 79]
the reason for the prenatal growth restraint [50 72 74] Itmust be kept in mind that noncommunicable diseases aremultifactorial entities in which genetic and environmentalfactors converge and their cause cannot be attributed to asingle explanation However when growth restriction is akey feature in syndromes with chromosome instability the
possibility that cell hypoplasia due to DNA repair malfunc-tion is contributing to the growth restriction phenotypemustbe contemplated Moreover since none of these adult onsetdiseases is reported as an inherent element of the SS and NBSphenotypes the direct connection between low birth weightand adult noncommunicable diseases is less of a straight
12 BioMed Research International
shot Furthermore there are other Mendelian syndromeswith mutations in DNA repair genes that characteristicallyshow adult noncommunicable diseases but do not haveIUGR such is the case for Werner syndrome a progeroiddisease caused by biallelic mutations in another RecQ heli-case (RecQ4) that clinically presents with postnatal shortstature and a prevalence of type 2 diabetes mellitus of 70[50 70 74]
Natural history of FA NBS and BS documented throughthe existing patient registries has allowed the identificationof noncommunicable diseases to be a part of the clinicalspectrum of these syndromes (Table 2) Meanwhile from theinformation available through SS case reports no adult onsetdisease has been found to be part of this phenotype To thebest of our knowledge the direct investigation of nonevidentendocrinologic alterations like glucose homeostasis or dys-lipidemia has not been directlymade in SS patients For a raredisease like SS such a study can only be done if a fairly largegroup of patients like the one found in registries is availableIf such a study was to be performed hidden features in SSpatients could be unraveled
Oxidative stress sensibility is a cellular feature sharedby all the SIC syndromes with IUGR that could contributeto the explanation of the premature development of non-communicable adult diseases in these patients Reports haveshown that BS and NBS cells have endogenous reactiveoxygen species (ROS) overproduction and an impairedmitochondrial homeostasis [75] it is also well known thatFA cells show increased levels of oxidative damage [3876] and there is evidence that oxidative stress can activateATR-mediated checkpoint signaling [77] Since this kind ofdamage has soundly been related to age-associated diseasesthat result from tissue degeneration exacerbated oxidativedamage found in these syndromes could result in cellu-lar aging that manifests as overall premature aging withparticular symptoms like glucose homeostasis alterations[76 77]
Fetal growth restriction is a multifactorial conditionwhere wide arrays of factors converge Fetal aspects inparticular those affecting the genetic constitution of thefetus have been recognized to play an important role Ithas been demonstrated that chromosomal abnormalities andmonogenic syndromes caused by mutations in genes thatparticipate in growth or metabolic pathways directly affectfetal growth [78] Even though they are rare entities CISappear as another group of monogenic pathologies thatbroaden the list of genetic fetal factors of fetal growthrestriction
Consent
The necessary consent for the publication of the photographswas obtained
Conflicts of Interest
The authors declare that there are no conflicts of interestregarding the publication of this paper
Authorsrsquo Contributions
The three authors contributed equally andwrote the first draftof the paper The final version was approved by everyone
Acknowledgments
This paper is supported by SEP-CONACYT Project 243102Benilde Garcıa-de Teresa received the 574025 scholarshipfrom CONACYT The paper is also supported by PAPIIT-UNAM Project IA202615 and Fondos Federales INP Project41-2014
References
[1] K W J Derks J H J Hoeijmakers and J Pothof ldquoThe DNAdamage response The omics era and its impactrdquo DNA Repairvol 19 pp 214ndash220 2014
[2] S P Jackson and J Bartek ldquoThe DNA-damage response inhuman biology and diseaserdquoNature vol 461 no 7267 pp 1071ndash1078 2009
[3] J H J Hoeijmakers ldquoDNA damage aging and cancerrdquo TheNew England Journal of Medicine vol 361 no 15 pp 1475ndash14852009
[4] G Spivak ldquoNucleotide excision repair in humansrdquoDNARepairvol 36 pp 13ndash18 2015
[5] J Vijg XDong BMilholland andL Zhang ldquoGenome instabil-ity a conserved mechanism of ageingrdquo Essays in Biochemistryvol 61 no 3 pp 305ndash315 2017
[6] J I Garaycoechea and K J Patel ldquoWhy does the bone marrowfail in Fanconi anemiardquo Blood vol 123 no 1 pp 26ndash34 2014
[7] R Ceccaldi B Rondinelli andAD DrsquoAndrea ldquoRepair PathwayChoices andConsequences at theDouble-Strand BreakrdquoTrendsin Cell Biology vol 26 no 1 pp 52ndash64 2016
[8] R Biehs M Steinlage O Barton et al ldquoDNA Double-StrandBreak Resection Occurs during Non-homologous End Joiningin G1 but Is Distinct from Resection during HomologousRecombinationrdquo Molecular Cell vol 65 no 4 pp 671ndash684e52017
[9] A Ciccia and S J Elledge ldquoTheDNAdamage response makingit safe to play with knivesrdquoMolecular Cell vol 40 no 2 pp 179ndash204 2010
[10] L H Pearl A C Schierz S E Ward B Al-Lazikani and F MG Pearl ldquoTherapeutic opportunities within the DNA damageresponserdquo Nature Reviews Cancer vol 15 no 3 pp 166ndash1802015
[11] S-F Yang C-W Chang R-J Wei Y-L Shiue S-N Wang andY-T Yeh ldquoInvolvement of DNA damage response pathways inhepatocellular carcinomardquo BioMed Research International vol2014 Article ID 153867 2014
[12] M He W Zhou C Li and M Guo ldquoMicroRNAs DNAdamage response and cancer treatmentrdquo International Journalof Molecular Sciences vol 17 no 12 article no 2087 2016
[13] K A Cimprich and D Cortez ldquoATR an essential regulator ofgenome integrityrdquo Nature Reviews Molecular Cell Biology vol9 no 8 pp 616ndash627 2008
[14] B M Sirbu and D Cortez ldquoDNA damage response three levelsof DNA repair regulationrdquo Cold Spring Harbor Perspectives inBiology vol 5 article a012724 no 8 2013
BioMed Research International 13
[15] C Beck I Robert B Reina-San-Martin V Schreiber andF Dantzer ldquoPoly(ADP-ribose) polymerases in double-strandbreak repair focus on PARP1 PARP2 and PARP3rdquo Experimen-tal Cell Research vol 329 no 1 pp 18ndash25 2014
[16] D W Meek ldquoTumour suppression by p53 a role for the DNAdamage responserdquo Nature Reviews Cancer vol 9 no 10 pp714ndash723 2009
[17] A Rodrıguez L Torres U Juarez et al ldquoFanconi anemiacells with unrepaired DNA damage activate components of thecheckpoint recovery processrdquo Theoretical Biology and MedicalModelling vol 12 no 1 article 11 2015
[18] H Wang X Zhang L Teng and R J Legerski ldquoDNA damagecheckpoint recovery and cancer developmentrdquo ExperimentalCell Research vol 334 no 2 pp 350ndash358 2015
[19] P A Jeggo L H Pearl and A M Carr ldquoDNA repair genomestability and cancer A historical perspectiverdquo Nature ReviewsCancer vol 16 no 1 pp 35ndash42 2016
[20] F S Alkuraya ldquoPrimordial dwarfism An updaterdquo CurrentOpinion in Endocrinology Diabetes and Obesity vol 22 no 1pp 55ndash64 2015
[21] P Fortini C Ferretti and E Dogliotti ldquoThe response to DNAdamage during differentiation pathways and consequencesrdquoMutation ResearchmdashFundamental and Molecular Mechanismsof Mutagenesis vol 743-744 pp 160ndash168 2013
[22] B R Adams S E Golding R R Rao and K Valerie ldquoDynamicdependence on ATR and ATM for double-Strand break repairin human embryonic stem cells and neural descendantsrdquo PLoSONE vol 5 article e10001 no 4 2010
[23] A Klingseisen and A P Jackson ldquoMechanisms and pathways ofgrowth failure in primordial dwarfismrdquo Genes amp Developmentvol 25 no 19 pp 2011ndash2024 2011
[24] H Mokrani-Benhelli L Gaillard P Biasutto et al ldquoPrimaryMicrocephaly Impaired DNA Replication and Genomic Insta-bility Caused by Compound Heterozygous ATR MutationsrdquoHuman Mutation vol 34 no 2 pp 374ndash384 2013
[25] M OrsquoDriscoll A R Gennery J Seidel P Concannon and PA Jeggo ldquoAn overview of three new disorders associated withgenetic instability LIG4 syndrome RS-SCID and ATR-Seckelsyndromerdquo DNA Repair vol 3 no 8-9 pp 1227ndash1235 2004
[26] P Khetarpal S Das I Panigrahi and A Munshi ldquoPrimordialdwarfism overview of clinical and genetic aspectsrdquo MolecularGenetics and Genomics vol 291 no 1 pp 1ndash15 2016
[27] TOgi SWalker T Stiff et al ldquoIdentification of the First ATRIP-Deficient Patient and Novel Mutations in ATRDefine a ClinicalSpectrum for ATR-ATRIP Seckel Syndromerdquo PLoS Geneticsvol 8 no 11 Article ID e1002945 2012
[28] A Verloes S Drunat and P Gressens Primary autosomalrecessive microcephalies and Seckel syndrome spectrum disor-ders 2013
[29] A D Brown B W Sager A Gorthi S S Tonapi E J Brownand A J R Bishop ldquoATR suppresses endogenous DNA damageand allows completion of homologous recombination repairrdquoPLoS ONE vol 9 article e91222 no 3 2014
[30] E J Brown and D Baltimore ldquoEssential and dispensable rolesof ATR in cell cycle arrest and genome maintenancerdquo Genes ampDevelopment vol 17 no 5 pp 615ndash628 2003
[31] B Fitzgerald M OrsquoDriscoll K Chong S Keating and PShannon ldquoNeuropathology of fetal stage Seckel syndromeA case report providing a morphological correlate for theemerging molecular mechanismsrdquo Brain amp Development vol34 no 3 pp 238ndash243 2012
[32] L I Mullee and C G Morrison ldquoCentrosomes in the DNAdamage responsemdashthe hub outside the centrerdquo ChromosomeResearch vol 24 no 1 pp 35ndash51 2016
[33] K M Takikawa A Kikuchi A Yokoyama et al ldquoPerinatalfindings of Seckel syndrome A case report of a fetus showingprimordial dwarfism and severe microcephalyrdquo Fetal Diagnosisand Therapy vol 24 no 4 pp 405ndash408 2009
[34] Y Ruzankina C Pinzon-Guzman A Asare et al ldquoDeletion ofthe Developmentally Essential Gene ATR in Adult Mice Leadsto Age-Related Phenotypes and Stem Cell Lossrdquo Cell Stem Cellvol 1 no 1 pp 113ndash126 2007
[35] N E Mamrak A Shimamura and N G Howlett ldquoRecentdiscoveries in the molecular pathogenesis of the inherited bonemarrow failure syndrome Fanconi anemiardquo Blood Reviews vol31 no 3 pp 93ndash99 2017
[36] B P Alter ldquoDiagnosis Genetics and Management of InheritedBone Marrow Failure Syndromesrdquo International Journal ofHematology vol 2007 no 1 pp 29ndash39 2007
[37] L B Pontel I V Rosado G Burgos-Barragan et al ldquoEndoge-nous Formaldehyde Is a Hematopoietic Stem Cell Genotoxinand Metabolic Carcinogenrdquo Molecular Cell vol 60 no 1 pp177ndash188 2015
[38] G Pagano P Degan M DrsquoIschia et al ldquoOxidative stress asa multiple effector in Fanconi anaemia clinical phenotyperdquoEuropean Journal of Haematology vol 75 no 2 pp 93ndash1002005
[39] P FGiampietro P CVerlander J GDavis andADAuerbachldquoDiagnosis of Fanconi anemia in patients without congenitalmalformations An International Fanconi Anemia Registrystudyrdquo American Journal of Medical Genetics vol 68 no 1 pp58ndash61 1997
[40] P F Giampietro B Adler-Brecher P C Verlander S GPavlakis J G Davis and A D Auerbach ldquoThe need for moreaccurate and timely diagnosis in Fanconi anemia A report fromthe International Fanconi Anemia Registryrdquo Pediatrics vol 91no 6 pp 1116ndash1120 1993
[41] M P Wajnrajch J M Gertner Z Huma et al ldquoEvaluationof growth and hormonal status in patients referred to theinternational fanconi anemia registryrdquo Pediatrics vol 107 no4 I pp 744ndash754 2001
[42] N Giri D L Batista B P Alter and C A Stratakis ldquoEndocrineabnormalities in patients with fanconi anemiardquo The Journal ofClinical Endocrinology amp Metabolism vol 92 no 7 pp 2624ndash2631 2007
[43] S R Rose K C Myers M M Rutter et al ldquoEndocrine phe-notype of children and adults with Fanconi anemiardquo PediatricBlood amp Cancer vol 59 no 4 pp 690ndash696 2012
[44] A D Auerbach B Adler and R S K Chaganti ldquoPrenatal andpostnatal diagnosis and carrier detection of Fanconi anemia bya cytogeneticmethodrdquoPediatrics vol 67 no 1 pp 128ndash135 1981
[45] A D Auerbach M Sagi and B Adler ldquoFanconi anemiaPrenatal diagnosis in 30 fetuses at riskrdquo Pediatrics vol 76 no5 pp 794ndash800 1985
[46] L Faivre M F Portnoı G Pals et al ldquoShould chromosomebreakage studies be performed in patients with VACTERLassociationrdquo American Journal of Medical Genetics vol 137 no1 pp 55ndash58 2005
[47] B P Alter P S Rosenberg and L C Brody ldquoClinicaland molecular features associated with biallelic mutations inFANCD1BRCA2rdquo Journal ofMedical Genetics vol 44 no 1 pp1ndash9 2007
14 BioMed Research International
[48] K Myers S M Davies R E Harris et al ldquoThe clinicalphenotype of children with Fanconi anemia caused by biallelicFANCD1BRCA2mutationsrdquo Pediatric Blood amp Cancer vol 58no 3 pp 462ndash465 2012
[49] B G Yoon H N Kim U J Han et al ldquoLong-term follow-up of Fanconi anemia Clinical manifestation and treatmentoutcomerdquo Korean Journal of Pediatrics vol 57 no 3 pp 125ndash134 2014
[50] J G Hall ldquoReview and hypothesis Syndromes with severeintrauterine growth restriction and very short stature - Are theyrelated to the epigeneticmechanism(s) of fetal survival involvedin the developmental origins of adult health and diseaserdquoAmerican Journal of Medical Genetics Part A vol 152 no 2 pp512ndash527 2010
[51] A Petryk R K Shankar N Giri et al ldquoEndocrine disordersin Fanconi anemia Recommendations for screening and treat-mentrdquoThe Journal of Clinical Endocrinology ampMetabolism vol100 no 3 pp 803ndash811 2015
[52] S R RoseMM Rutter RMueller et al ldquoBonemineral densityis normal in children with Fanconi anemiardquo Pediatric Blood ampCancer vol 57 no 6 pp 1034ndash1038 2011
[53] A Petryk L E Polgreen J L Barnum et al ldquoBone mineraldensity in childrenwith fanconi anemia after hematopoietic celltransplantationrdquo Biology of Blood and Marrow Transplantationvol 21 no 5 pp 894ndash899 2015
[54] R Purkait A Mukherji S Datta and R Bhadra ldquoRenal arterystenosis An unusual etiology of hypertensive encephalopathyin a childwith fanconi anemiardquo Saudi Journal of KidneyDiseasesand Transplantation vol 26 no 4 pp 778ndash782 2015
[55] K H Chrzanowska H Gregorek B Dembowska-BaginskaM A Kalina and M Digweed ldquoNijmegen breakage syndrome(NBS)rdquoOrphanet Journal of Rare Diseases vol 7 article 13 2012
[56] L C Riches A M Lynch and N J Gooderham ldquoEarly eventsin the mammalian response to DNA double-strand breaksrdquoMutagenesis vol 23 no 5 pp 331ndash339 2008
[57] K Chrzanowska M Kalina H Rysiewski et al ldquoGrowthpattern in patients withNijmegen breakage syndrome evidencefroma longitudinal studyrdquoHormoneResearch in Paediatrics vol74 article S38 2010
[58] Group TINBSS ldquoNijmegen breakage syndromerdquo Archives ofDisease in Childhood vol 82 pp 400ndash406 2000
[59] M Digweed and K Sperling ldquoNijmegen breakage syndromeClinical manifestation of defective response to DNA double-strand breaksrdquo DNA Repair vol 3 no 8-9 pp 1207ndash1217 2004
[60] E Seemanova ldquoAn increased risk for malignant neoplasmsin heterozygotes for a syndrome of microcephaly normalintelligence growth retardation remarkable facies immun-odeficiency and chromosomal instabilityrdquo Mutation ResearchReviews in Genetic Toxicology vol 238 no 3 pp 321ndash324 1990
[61] K H Chrzanowska M Szarras-Czapnik M Gajdulewicz et alldquoHigh prevalence of primary ovarian insufficiency in girls andyoung women with Nijmegen breakage syndrome Evidencefrom a longitudinal studyrdquoThe Journal of Clinical Endocrinologyamp Metabolism vol 95 no 7 pp 3133ndash3140 2010
[62] C M R Weemaes T W J Hustinx J M J C Scheres P J JV Munster J A J M Bakkeren and R D F M Taalman ldquoAnew chromosomal instability disorder The nijmegen breakagesyndromerdquo Acta Paediatrica Scandinavica vol 70 no 4 pp557ndash564 1981
[63] A J Green J R W Yates A M R Taylor et al ldquoSevere micro-cephaly with normal intellectual development The Nijmegen
breakage syndromerdquo Archives of Disease in Childhood vol 73no 5 pp 431ndash434 1995
[64] D Gupta and A Nagarkar ldquoSpeech impairment in Nijmegenbreakage syndrome A rare anomalyrdquo International Journal ofPediatric Otorhinolaryngology vol 73 no 6 pp 873ndash875 2009
[65] P Muschke H Gola R Varon et al ldquoRetrospective diagnosisand subsequent prenatal diagnosis of Nijmegen breakage syn-dromerdquo Prenatal Diagnosis vol 24 no 2 pp 111ndash113 2004
[66] S Pasic M Cupic T Jovanovic S Djukic M Kavaric andI Lazarevic ldquoNijmegen breakage syndrome and chronic pol-yarthritisrdquo Italian Journal of Pediatrics vol 39 no 1 article no59 2013
[67] J P Patel J M Puck R Srinivasan et al ldquoNijmegen BreakageSyndrome Detected by Newborn Screening for T Cell ReceptorExcision Circles (TRECs)rdquo Journal of Clinical Immunology vol35 no 2 pp 227ndash233 2015
[68] I Demuth and M Digweed ldquoThe clinical manifestation of adefective response to DNA double-strand breaks as exemplifiedby Nijmegen breakage syndromerdquoOncogene vol 26 no 56 pp7792ndash7798 2007
[69] H Arora A H Chacon S Choudhary et al ldquoBloom syn-dromerdquo International Journal of Dermatology vol 53 no 7 pp798ndash802 2014
[70] C de Renty and N A Ellis ldquoBloomrsquos syndrome Why not pre-mature aging A comparison of the BLM andWRN helicasesrdquoAgeing Research Reviews vol 33 pp 36ndash51 2017
[71] C Keller K R Keller S B Shew and S E Plon ldquoGrowthdeficiency and malnutrition in Bloom syndromerdquo Journal ofPediatrics vol 134 no 4 pp 472ndash479 1999
[72] A Diaz M G Vogiatzi M M Sanz and J German ldquoEval-uation of short stature carbohydrate metabolism and otherendocrinopathies in Bloomrsquos syndromerdquo Hormone Researchvol 66 no 3 pp 111ndash117 2006
[73] C Ling J Huang Z Yan et al ldquoBloom syndrome complexpromotes FANCM recruitment to stalled replication forksand facilitates both repair and traverse of DNA interstrandcrosslinksrdquo Cell Discovery vol 2 article 16047 2016
[74] J S Renes R H Willemsen A Wagner M J J Finken and AC SHokken-Koelega ldquoBloom syndrome in short children bornsmall for gestational age A challenging diagnosisrdquoThe Journalof Clinical EndocrinologyampMetabolism vol 98 no 10 pp 3932ndash3938 2013
[75] M Maciejczyk B Mikoluc B Pietrucha et al ldquoOxidativestress mitochondrial abnormalities and antioxidant defense inAtaxia-telangiectasia Bloom syndrome andNijmegen breakagesyndromerdquo Redox Biology vol 11 pp 375ndash383 2017
[76] R M Brosh M Bellani Y Liu and M M Seidman ldquoFanconiAnemia A DNA repair disorder characterized by accelerateddecline of the hematopoietic stem cell compartment and otherfeatures of agingrdquo Ageing Research Reviews vol 33 pp 67ndash752017
[77] S Yan M Sorrell and Z Berman ldquoFunctional interplay be-tween ATMATR-mediated DNA damage response and DNArepair pathways in oxidative stressrdquo Cellular and Molecular LifeSciences vol 71 no 20 pp 3951ndash3967 2014
[78] L M M Nardozza A C R Caetano A C P Zamarian etal ldquoFetal growth restriction current knowledgerdquo Archives ofGynecology and Obstetrics vol 295 no 5 pp 1061ndash1077 2017
[79] M Tomas Vila J P Verdu M R Piera and C O AlonsoldquoNijmegen breakage syndrome phenotype a disorder to con-sider in the diagnosis ofmicrocephalyrdquoAnales De Pediatria vol74 pp 58ndash60 2011
Submit your manuscripts athttpswwwhindawicom
Stem CellsInternational
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
MEDIATORSINFLAMMATION
of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Behavioural Neurology
EndocrinologyInternational Journal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Disease Markers
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
BioMed Research International
OncologyJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Oxidative Medicine and Cellular Longevity
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
PPAR Research
The Scientific World JournalHindawi Publishing Corporation httpwwwhindawicom Volume 2014
Immunology ResearchHindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Journal of
ObesityJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Computational and Mathematical Methods in Medicine
OphthalmologyJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Diabetes ResearchJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Research and TreatmentAIDS
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Gastroenterology Research and Practice
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Parkinsonrsquos Disease
Evidence-Based Complementary and Alternative Medicine
Volume 2014Hindawi Publishing Corporationhttpwwwhindawicom

BioMed Research International 11
Table 2 Growth features of chromosomal instability syndromes
SyndromeldquoLocirdquo At-term birth weightheight Microcephaly Adult height Adult onset diseases
Seckel SyndromeldquoATR3q23rdquo
Birth weight below minus3 SD(2055 g)
Severeminus4 SD
Postnatal growth retardation(below minus5 SD) Not reported
Fanconi anemialdquo21 FANC genesrdquo
Median weight 202 kg(15ndash26 kg) In 20ndash50
50ndash60 of patients with medianheight lt minus18 SDSWomen minus34 SDSMen minus44 SDS
CancerDiabetes mellitusDyslipidemia
Altered bone mineral densityNijmegen BreakageSyndromeldquoNBN8q21rdquo
Mean weightheight girls27 kg514 cm
Mean weightheight boys28 kg523 cm
100 Mean height for women minus18 SDSMean height for men minus23 Cancer
Bloom SyndromeldquoBLM15q261rdquo
Mean weight 189 kg plusmn 035 kg forboys
Mean weight 187 kg plusmn 035 kg forgirls
Mean height 434 cm plusmn 44 cm forboys
Mean height 438 cm plusmn 28 cm forgirls
Mildmicrocephaly
Mean height 1455 cm plusmn 76 cmmales
Mean height 1415 cm plusmn 61 cm forfemales
CancerDiabetes mellitus
See [27 33 40 43 50 57 69]
45 53
43245
Height (cm)
Weight (kg)
Percentile 3 Percentile 97Percentile 50495
33
Normalindividual
Mean 2055
SeckelSyndrome
2615Median 202
FanconiAnemia
Mean 51
Mean 275
Nijmegen BreakageSyndrome
38 49
24513
Mean 436
Mean 188
BloomSyndrome
Figure 9 Anthropometric features at birth of chromosome instability syndromes with perinatal growth retardation Comparison of theavailable growth data from SS FA NBS and BS syndrome against birth data from the WHOrsquos growth standards for infants Although meanheight and weight values of NBS patients are found to be within normal percentiles according to WHO standards there are several authorswho refer to prenatal growth restriction [55 63 65 79]
the reason for the prenatal growth restraint [50 72 74] Itmust be kept in mind that noncommunicable diseases aremultifactorial entities in which genetic and environmentalfactors converge and their cause cannot be attributed to asingle explanation However when growth restriction is akey feature in syndromes with chromosome instability the
possibility that cell hypoplasia due to DNA repair malfunc-tion is contributing to the growth restriction phenotypemustbe contemplated Moreover since none of these adult onsetdiseases is reported as an inherent element of the SS and NBSphenotypes the direct connection between low birth weightand adult noncommunicable diseases is less of a straight
12 BioMed Research International
shot Furthermore there are other Mendelian syndromeswith mutations in DNA repair genes that characteristicallyshow adult noncommunicable diseases but do not haveIUGR such is the case for Werner syndrome a progeroiddisease caused by biallelic mutations in another RecQ heli-case (RecQ4) that clinically presents with postnatal shortstature and a prevalence of type 2 diabetes mellitus of 70[50 70 74]
Natural history of FA NBS and BS documented throughthe existing patient registries has allowed the identificationof noncommunicable diseases to be a part of the clinicalspectrum of these syndromes (Table 2) Meanwhile from theinformation available through SS case reports no adult onsetdisease has been found to be part of this phenotype To thebest of our knowledge the direct investigation of nonevidentendocrinologic alterations like glucose homeostasis or dys-lipidemia has not been directlymade in SS patients For a raredisease like SS such a study can only be done if a fairly largegroup of patients like the one found in registries is availableIf such a study was to be performed hidden features in SSpatients could be unraveled
Oxidative stress sensibility is a cellular feature sharedby all the SIC syndromes with IUGR that could contributeto the explanation of the premature development of non-communicable adult diseases in these patients Reports haveshown that BS and NBS cells have endogenous reactiveoxygen species (ROS) overproduction and an impairedmitochondrial homeostasis [75] it is also well known thatFA cells show increased levels of oxidative damage [3876] and there is evidence that oxidative stress can activateATR-mediated checkpoint signaling [77] Since this kind ofdamage has soundly been related to age-associated diseasesthat result from tissue degeneration exacerbated oxidativedamage found in these syndromes could result in cellu-lar aging that manifests as overall premature aging withparticular symptoms like glucose homeostasis alterations[76 77]
Fetal growth restriction is a multifactorial conditionwhere wide arrays of factors converge Fetal aspects inparticular those affecting the genetic constitution of thefetus have been recognized to play an important role Ithas been demonstrated that chromosomal abnormalities andmonogenic syndromes caused by mutations in genes thatparticipate in growth or metabolic pathways directly affectfetal growth [78] Even though they are rare entities CISappear as another group of monogenic pathologies thatbroaden the list of genetic fetal factors of fetal growthrestriction
Consent
The necessary consent for the publication of the photographswas obtained
Conflicts of Interest
The authors declare that there are no conflicts of interestregarding the publication of this paper
Authorsrsquo Contributions
The three authors contributed equally andwrote the first draftof the paper The final version was approved by everyone
Acknowledgments
This paper is supported by SEP-CONACYT Project 243102Benilde Garcıa-de Teresa received the 574025 scholarshipfrom CONACYT The paper is also supported by PAPIIT-UNAM Project IA202615 and Fondos Federales INP Project41-2014
References
[1] K W J Derks J H J Hoeijmakers and J Pothof ldquoThe DNAdamage response The omics era and its impactrdquo DNA Repairvol 19 pp 214ndash220 2014
[2] S P Jackson and J Bartek ldquoThe DNA-damage response inhuman biology and diseaserdquoNature vol 461 no 7267 pp 1071ndash1078 2009
[3] J H J Hoeijmakers ldquoDNA damage aging and cancerrdquo TheNew England Journal of Medicine vol 361 no 15 pp 1475ndash14852009
[4] G Spivak ldquoNucleotide excision repair in humansrdquoDNARepairvol 36 pp 13ndash18 2015
[5] J Vijg XDong BMilholland andL Zhang ldquoGenome instabil-ity a conserved mechanism of ageingrdquo Essays in Biochemistryvol 61 no 3 pp 305ndash315 2017
[6] J I Garaycoechea and K J Patel ldquoWhy does the bone marrowfail in Fanconi anemiardquo Blood vol 123 no 1 pp 26ndash34 2014
[7] R Ceccaldi B Rondinelli andAD DrsquoAndrea ldquoRepair PathwayChoices andConsequences at theDouble-Strand BreakrdquoTrendsin Cell Biology vol 26 no 1 pp 52ndash64 2016
[8] R Biehs M Steinlage O Barton et al ldquoDNA Double-StrandBreak Resection Occurs during Non-homologous End Joiningin G1 but Is Distinct from Resection during HomologousRecombinationrdquo Molecular Cell vol 65 no 4 pp 671ndash684e52017
[9] A Ciccia and S J Elledge ldquoTheDNAdamage response makingit safe to play with knivesrdquoMolecular Cell vol 40 no 2 pp 179ndash204 2010
[10] L H Pearl A C Schierz S E Ward B Al-Lazikani and F MG Pearl ldquoTherapeutic opportunities within the DNA damageresponserdquo Nature Reviews Cancer vol 15 no 3 pp 166ndash1802015
[11] S-F Yang C-W Chang R-J Wei Y-L Shiue S-N Wang andY-T Yeh ldquoInvolvement of DNA damage response pathways inhepatocellular carcinomardquo BioMed Research International vol2014 Article ID 153867 2014
[12] M He W Zhou C Li and M Guo ldquoMicroRNAs DNAdamage response and cancer treatmentrdquo International Journalof Molecular Sciences vol 17 no 12 article no 2087 2016
[13] K A Cimprich and D Cortez ldquoATR an essential regulator ofgenome integrityrdquo Nature Reviews Molecular Cell Biology vol9 no 8 pp 616ndash627 2008
[14] B M Sirbu and D Cortez ldquoDNA damage response three levelsof DNA repair regulationrdquo Cold Spring Harbor Perspectives inBiology vol 5 article a012724 no 8 2013
BioMed Research International 13
[15] C Beck I Robert B Reina-San-Martin V Schreiber andF Dantzer ldquoPoly(ADP-ribose) polymerases in double-strandbreak repair focus on PARP1 PARP2 and PARP3rdquo Experimen-tal Cell Research vol 329 no 1 pp 18ndash25 2014
[16] D W Meek ldquoTumour suppression by p53 a role for the DNAdamage responserdquo Nature Reviews Cancer vol 9 no 10 pp714ndash723 2009
[17] A Rodrıguez L Torres U Juarez et al ldquoFanconi anemiacells with unrepaired DNA damage activate components of thecheckpoint recovery processrdquo Theoretical Biology and MedicalModelling vol 12 no 1 article 11 2015
[18] H Wang X Zhang L Teng and R J Legerski ldquoDNA damagecheckpoint recovery and cancer developmentrdquo ExperimentalCell Research vol 334 no 2 pp 350ndash358 2015
[19] P A Jeggo L H Pearl and A M Carr ldquoDNA repair genomestability and cancer A historical perspectiverdquo Nature ReviewsCancer vol 16 no 1 pp 35ndash42 2016
[20] F S Alkuraya ldquoPrimordial dwarfism An updaterdquo CurrentOpinion in Endocrinology Diabetes and Obesity vol 22 no 1pp 55ndash64 2015
[21] P Fortini C Ferretti and E Dogliotti ldquoThe response to DNAdamage during differentiation pathways and consequencesrdquoMutation ResearchmdashFundamental and Molecular Mechanismsof Mutagenesis vol 743-744 pp 160ndash168 2013
[22] B R Adams S E Golding R R Rao and K Valerie ldquoDynamicdependence on ATR and ATM for double-Strand break repairin human embryonic stem cells and neural descendantsrdquo PLoSONE vol 5 article e10001 no 4 2010
[23] A Klingseisen and A P Jackson ldquoMechanisms and pathways ofgrowth failure in primordial dwarfismrdquo Genes amp Developmentvol 25 no 19 pp 2011ndash2024 2011
[24] H Mokrani-Benhelli L Gaillard P Biasutto et al ldquoPrimaryMicrocephaly Impaired DNA Replication and Genomic Insta-bility Caused by Compound Heterozygous ATR MutationsrdquoHuman Mutation vol 34 no 2 pp 374ndash384 2013
[25] M OrsquoDriscoll A R Gennery J Seidel P Concannon and PA Jeggo ldquoAn overview of three new disorders associated withgenetic instability LIG4 syndrome RS-SCID and ATR-Seckelsyndromerdquo DNA Repair vol 3 no 8-9 pp 1227ndash1235 2004
[26] P Khetarpal S Das I Panigrahi and A Munshi ldquoPrimordialdwarfism overview of clinical and genetic aspectsrdquo MolecularGenetics and Genomics vol 291 no 1 pp 1ndash15 2016
[27] TOgi SWalker T Stiff et al ldquoIdentification of the First ATRIP-Deficient Patient and Novel Mutations in ATRDefine a ClinicalSpectrum for ATR-ATRIP Seckel Syndromerdquo PLoS Geneticsvol 8 no 11 Article ID e1002945 2012
[28] A Verloes S Drunat and P Gressens Primary autosomalrecessive microcephalies and Seckel syndrome spectrum disor-ders 2013
[29] A D Brown B W Sager A Gorthi S S Tonapi E J Brownand A J R Bishop ldquoATR suppresses endogenous DNA damageand allows completion of homologous recombination repairrdquoPLoS ONE vol 9 article e91222 no 3 2014
[30] E J Brown and D Baltimore ldquoEssential and dispensable rolesof ATR in cell cycle arrest and genome maintenancerdquo Genes ampDevelopment vol 17 no 5 pp 615ndash628 2003
[31] B Fitzgerald M OrsquoDriscoll K Chong S Keating and PShannon ldquoNeuropathology of fetal stage Seckel syndromeA case report providing a morphological correlate for theemerging molecular mechanismsrdquo Brain amp Development vol34 no 3 pp 238ndash243 2012
[32] L I Mullee and C G Morrison ldquoCentrosomes in the DNAdamage responsemdashthe hub outside the centrerdquo ChromosomeResearch vol 24 no 1 pp 35ndash51 2016
[33] K M Takikawa A Kikuchi A Yokoyama et al ldquoPerinatalfindings of Seckel syndrome A case report of a fetus showingprimordial dwarfism and severe microcephalyrdquo Fetal Diagnosisand Therapy vol 24 no 4 pp 405ndash408 2009
[34] Y Ruzankina C Pinzon-Guzman A Asare et al ldquoDeletion ofthe Developmentally Essential Gene ATR in Adult Mice Leadsto Age-Related Phenotypes and Stem Cell Lossrdquo Cell Stem Cellvol 1 no 1 pp 113ndash126 2007
[35] N E Mamrak A Shimamura and N G Howlett ldquoRecentdiscoveries in the molecular pathogenesis of the inherited bonemarrow failure syndrome Fanconi anemiardquo Blood Reviews vol31 no 3 pp 93ndash99 2017
[36] B P Alter ldquoDiagnosis Genetics and Management of InheritedBone Marrow Failure Syndromesrdquo International Journal ofHematology vol 2007 no 1 pp 29ndash39 2007
[37] L B Pontel I V Rosado G Burgos-Barragan et al ldquoEndoge-nous Formaldehyde Is a Hematopoietic Stem Cell Genotoxinand Metabolic Carcinogenrdquo Molecular Cell vol 60 no 1 pp177ndash188 2015
[38] G Pagano P Degan M DrsquoIschia et al ldquoOxidative stress asa multiple effector in Fanconi anaemia clinical phenotyperdquoEuropean Journal of Haematology vol 75 no 2 pp 93ndash1002005
[39] P FGiampietro P CVerlander J GDavis andADAuerbachldquoDiagnosis of Fanconi anemia in patients without congenitalmalformations An International Fanconi Anemia Registrystudyrdquo American Journal of Medical Genetics vol 68 no 1 pp58ndash61 1997
[40] P F Giampietro B Adler-Brecher P C Verlander S GPavlakis J G Davis and A D Auerbach ldquoThe need for moreaccurate and timely diagnosis in Fanconi anemia A report fromthe International Fanconi Anemia Registryrdquo Pediatrics vol 91no 6 pp 1116ndash1120 1993
[41] M P Wajnrajch J M Gertner Z Huma et al ldquoEvaluationof growth and hormonal status in patients referred to theinternational fanconi anemia registryrdquo Pediatrics vol 107 no4 I pp 744ndash754 2001
[42] N Giri D L Batista B P Alter and C A Stratakis ldquoEndocrineabnormalities in patients with fanconi anemiardquo The Journal ofClinical Endocrinology amp Metabolism vol 92 no 7 pp 2624ndash2631 2007
[43] S R Rose K C Myers M M Rutter et al ldquoEndocrine phe-notype of children and adults with Fanconi anemiardquo PediatricBlood amp Cancer vol 59 no 4 pp 690ndash696 2012
[44] A D Auerbach B Adler and R S K Chaganti ldquoPrenatal andpostnatal diagnosis and carrier detection of Fanconi anemia bya cytogeneticmethodrdquoPediatrics vol 67 no 1 pp 128ndash135 1981
[45] A D Auerbach M Sagi and B Adler ldquoFanconi anemiaPrenatal diagnosis in 30 fetuses at riskrdquo Pediatrics vol 76 no5 pp 794ndash800 1985
[46] L Faivre M F Portnoı G Pals et al ldquoShould chromosomebreakage studies be performed in patients with VACTERLassociationrdquo American Journal of Medical Genetics vol 137 no1 pp 55ndash58 2005
[47] B P Alter P S Rosenberg and L C Brody ldquoClinicaland molecular features associated with biallelic mutations inFANCD1BRCA2rdquo Journal ofMedical Genetics vol 44 no 1 pp1ndash9 2007
14 BioMed Research International
[48] K Myers S M Davies R E Harris et al ldquoThe clinicalphenotype of children with Fanconi anemia caused by biallelicFANCD1BRCA2mutationsrdquo Pediatric Blood amp Cancer vol 58no 3 pp 462ndash465 2012
[49] B G Yoon H N Kim U J Han et al ldquoLong-term follow-up of Fanconi anemia Clinical manifestation and treatmentoutcomerdquo Korean Journal of Pediatrics vol 57 no 3 pp 125ndash134 2014
[50] J G Hall ldquoReview and hypothesis Syndromes with severeintrauterine growth restriction and very short stature - Are theyrelated to the epigeneticmechanism(s) of fetal survival involvedin the developmental origins of adult health and diseaserdquoAmerican Journal of Medical Genetics Part A vol 152 no 2 pp512ndash527 2010
[51] A Petryk R K Shankar N Giri et al ldquoEndocrine disordersin Fanconi anemia Recommendations for screening and treat-mentrdquoThe Journal of Clinical Endocrinology ampMetabolism vol100 no 3 pp 803ndash811 2015
[52] S R RoseMM Rutter RMueller et al ldquoBonemineral densityis normal in children with Fanconi anemiardquo Pediatric Blood ampCancer vol 57 no 6 pp 1034ndash1038 2011
[53] A Petryk L E Polgreen J L Barnum et al ldquoBone mineraldensity in childrenwith fanconi anemia after hematopoietic celltransplantationrdquo Biology of Blood and Marrow Transplantationvol 21 no 5 pp 894ndash899 2015
[54] R Purkait A Mukherji S Datta and R Bhadra ldquoRenal arterystenosis An unusual etiology of hypertensive encephalopathyin a childwith fanconi anemiardquo Saudi Journal of KidneyDiseasesand Transplantation vol 26 no 4 pp 778ndash782 2015
[55] K H Chrzanowska H Gregorek B Dembowska-BaginskaM A Kalina and M Digweed ldquoNijmegen breakage syndrome(NBS)rdquoOrphanet Journal of Rare Diseases vol 7 article 13 2012
[56] L C Riches A M Lynch and N J Gooderham ldquoEarly eventsin the mammalian response to DNA double-strand breaksrdquoMutagenesis vol 23 no 5 pp 331ndash339 2008
[57] K Chrzanowska M Kalina H Rysiewski et al ldquoGrowthpattern in patients withNijmegen breakage syndrome evidencefroma longitudinal studyrdquoHormoneResearch in Paediatrics vol74 article S38 2010
[58] Group TINBSS ldquoNijmegen breakage syndromerdquo Archives ofDisease in Childhood vol 82 pp 400ndash406 2000
[59] M Digweed and K Sperling ldquoNijmegen breakage syndromeClinical manifestation of defective response to DNA double-strand breaksrdquo DNA Repair vol 3 no 8-9 pp 1207ndash1217 2004
[60] E Seemanova ldquoAn increased risk for malignant neoplasmsin heterozygotes for a syndrome of microcephaly normalintelligence growth retardation remarkable facies immun-odeficiency and chromosomal instabilityrdquo Mutation ResearchReviews in Genetic Toxicology vol 238 no 3 pp 321ndash324 1990
[61] K H Chrzanowska M Szarras-Czapnik M Gajdulewicz et alldquoHigh prevalence of primary ovarian insufficiency in girls andyoung women with Nijmegen breakage syndrome Evidencefrom a longitudinal studyrdquoThe Journal of Clinical Endocrinologyamp Metabolism vol 95 no 7 pp 3133ndash3140 2010
[62] C M R Weemaes T W J Hustinx J M J C Scheres P J JV Munster J A J M Bakkeren and R D F M Taalman ldquoAnew chromosomal instability disorder The nijmegen breakagesyndromerdquo Acta Paediatrica Scandinavica vol 70 no 4 pp557ndash564 1981
[63] A J Green J R W Yates A M R Taylor et al ldquoSevere micro-cephaly with normal intellectual development The Nijmegen
breakage syndromerdquo Archives of Disease in Childhood vol 73no 5 pp 431ndash434 1995
[64] D Gupta and A Nagarkar ldquoSpeech impairment in Nijmegenbreakage syndrome A rare anomalyrdquo International Journal ofPediatric Otorhinolaryngology vol 73 no 6 pp 873ndash875 2009
[65] P Muschke H Gola R Varon et al ldquoRetrospective diagnosisand subsequent prenatal diagnosis of Nijmegen breakage syn-dromerdquo Prenatal Diagnosis vol 24 no 2 pp 111ndash113 2004
[66] S Pasic M Cupic T Jovanovic S Djukic M Kavaric andI Lazarevic ldquoNijmegen breakage syndrome and chronic pol-yarthritisrdquo Italian Journal of Pediatrics vol 39 no 1 article no59 2013
[67] J P Patel J M Puck R Srinivasan et al ldquoNijmegen BreakageSyndrome Detected by Newborn Screening for T Cell ReceptorExcision Circles (TRECs)rdquo Journal of Clinical Immunology vol35 no 2 pp 227ndash233 2015
[68] I Demuth and M Digweed ldquoThe clinical manifestation of adefective response to DNA double-strand breaks as exemplifiedby Nijmegen breakage syndromerdquoOncogene vol 26 no 56 pp7792ndash7798 2007
[69] H Arora A H Chacon S Choudhary et al ldquoBloom syn-dromerdquo International Journal of Dermatology vol 53 no 7 pp798ndash802 2014
[70] C de Renty and N A Ellis ldquoBloomrsquos syndrome Why not pre-mature aging A comparison of the BLM andWRN helicasesrdquoAgeing Research Reviews vol 33 pp 36ndash51 2017
[71] C Keller K R Keller S B Shew and S E Plon ldquoGrowthdeficiency and malnutrition in Bloom syndromerdquo Journal ofPediatrics vol 134 no 4 pp 472ndash479 1999
[72] A Diaz M G Vogiatzi M M Sanz and J German ldquoEval-uation of short stature carbohydrate metabolism and otherendocrinopathies in Bloomrsquos syndromerdquo Hormone Researchvol 66 no 3 pp 111ndash117 2006
[73] C Ling J Huang Z Yan et al ldquoBloom syndrome complexpromotes FANCM recruitment to stalled replication forksand facilitates both repair and traverse of DNA interstrandcrosslinksrdquo Cell Discovery vol 2 article 16047 2016
[74] J S Renes R H Willemsen A Wagner M J J Finken and AC SHokken-Koelega ldquoBloom syndrome in short children bornsmall for gestational age A challenging diagnosisrdquoThe Journalof Clinical EndocrinologyampMetabolism vol 98 no 10 pp 3932ndash3938 2013
[75] M Maciejczyk B Mikoluc B Pietrucha et al ldquoOxidativestress mitochondrial abnormalities and antioxidant defense inAtaxia-telangiectasia Bloom syndrome andNijmegen breakagesyndromerdquo Redox Biology vol 11 pp 375ndash383 2017
[76] R M Brosh M Bellani Y Liu and M M Seidman ldquoFanconiAnemia A DNA repair disorder characterized by accelerateddecline of the hematopoietic stem cell compartment and otherfeatures of agingrdquo Ageing Research Reviews vol 33 pp 67ndash752017
[77] S Yan M Sorrell and Z Berman ldquoFunctional interplay be-tween ATMATR-mediated DNA damage response and DNArepair pathways in oxidative stressrdquo Cellular and Molecular LifeSciences vol 71 no 20 pp 3951ndash3967 2014
[78] L M M Nardozza A C R Caetano A C P Zamarian etal ldquoFetal growth restriction current knowledgerdquo Archives ofGynecology and Obstetrics vol 295 no 5 pp 1061ndash1077 2017
[79] M Tomas Vila J P Verdu M R Piera and C O AlonsoldquoNijmegen breakage syndrome phenotype a disorder to con-sider in the diagnosis ofmicrocephalyrdquoAnales De Pediatria vol74 pp 58ndash60 2011
Submit your manuscripts athttpswwwhindawicom
Stem CellsInternational
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
MEDIATORSINFLAMMATION
of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Behavioural Neurology
EndocrinologyInternational Journal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Disease Markers
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
BioMed Research International
OncologyJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Oxidative Medicine and Cellular Longevity
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
PPAR Research
The Scientific World JournalHindawi Publishing Corporation httpwwwhindawicom Volume 2014
Immunology ResearchHindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Journal of
ObesityJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Computational and Mathematical Methods in Medicine
OphthalmologyJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Diabetes ResearchJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Research and TreatmentAIDS
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Gastroenterology Research and Practice
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Parkinsonrsquos Disease
Evidence-Based Complementary and Alternative Medicine
Volume 2014Hindawi Publishing Corporationhttpwwwhindawicom

12 BioMed Research International
shot Furthermore there are other Mendelian syndromeswith mutations in DNA repair genes that characteristicallyshow adult noncommunicable diseases but do not haveIUGR such is the case for Werner syndrome a progeroiddisease caused by biallelic mutations in another RecQ heli-case (RecQ4) that clinically presents with postnatal shortstature and a prevalence of type 2 diabetes mellitus of 70[50 70 74]
Natural history of FA NBS and BS documented throughthe existing patient registries has allowed the identificationof noncommunicable diseases to be a part of the clinicalspectrum of these syndromes (Table 2) Meanwhile from theinformation available through SS case reports no adult onsetdisease has been found to be part of this phenotype To thebest of our knowledge the direct investigation of nonevidentendocrinologic alterations like glucose homeostasis or dys-lipidemia has not been directlymade in SS patients For a raredisease like SS such a study can only be done if a fairly largegroup of patients like the one found in registries is availableIf such a study was to be performed hidden features in SSpatients could be unraveled
Oxidative stress sensibility is a cellular feature sharedby all the SIC syndromes with IUGR that could contributeto the explanation of the premature development of non-communicable adult diseases in these patients Reports haveshown that BS and NBS cells have endogenous reactiveoxygen species (ROS) overproduction and an impairedmitochondrial homeostasis [75] it is also well known thatFA cells show increased levels of oxidative damage [3876] and there is evidence that oxidative stress can activateATR-mediated checkpoint signaling [77] Since this kind ofdamage has soundly been related to age-associated diseasesthat result from tissue degeneration exacerbated oxidativedamage found in these syndromes could result in cellu-lar aging that manifests as overall premature aging withparticular symptoms like glucose homeostasis alterations[76 77]
Fetal growth restriction is a multifactorial conditionwhere wide arrays of factors converge Fetal aspects inparticular those affecting the genetic constitution of thefetus have been recognized to play an important role Ithas been demonstrated that chromosomal abnormalities andmonogenic syndromes caused by mutations in genes thatparticipate in growth or metabolic pathways directly affectfetal growth [78] Even though they are rare entities CISappear as another group of monogenic pathologies thatbroaden the list of genetic fetal factors of fetal growthrestriction
Consent
The necessary consent for the publication of the photographswas obtained
Conflicts of Interest
The authors declare that there are no conflicts of interestregarding the publication of this paper
Authorsrsquo Contributions
The three authors contributed equally andwrote the first draftof the paper The final version was approved by everyone
Acknowledgments
This paper is supported by SEP-CONACYT Project 243102Benilde Garcıa-de Teresa received the 574025 scholarshipfrom CONACYT The paper is also supported by PAPIIT-UNAM Project IA202615 and Fondos Federales INP Project41-2014
References
[1] K W J Derks J H J Hoeijmakers and J Pothof ldquoThe DNAdamage response The omics era and its impactrdquo DNA Repairvol 19 pp 214ndash220 2014
[2] S P Jackson and J Bartek ldquoThe DNA-damage response inhuman biology and diseaserdquoNature vol 461 no 7267 pp 1071ndash1078 2009
[3] J H J Hoeijmakers ldquoDNA damage aging and cancerrdquo TheNew England Journal of Medicine vol 361 no 15 pp 1475ndash14852009
[4] G Spivak ldquoNucleotide excision repair in humansrdquoDNARepairvol 36 pp 13ndash18 2015
[5] J Vijg XDong BMilholland andL Zhang ldquoGenome instabil-ity a conserved mechanism of ageingrdquo Essays in Biochemistryvol 61 no 3 pp 305ndash315 2017
[6] J I Garaycoechea and K J Patel ldquoWhy does the bone marrowfail in Fanconi anemiardquo Blood vol 123 no 1 pp 26ndash34 2014
[7] R Ceccaldi B Rondinelli andAD DrsquoAndrea ldquoRepair PathwayChoices andConsequences at theDouble-Strand BreakrdquoTrendsin Cell Biology vol 26 no 1 pp 52ndash64 2016
[8] R Biehs M Steinlage O Barton et al ldquoDNA Double-StrandBreak Resection Occurs during Non-homologous End Joiningin G1 but Is Distinct from Resection during HomologousRecombinationrdquo Molecular Cell vol 65 no 4 pp 671ndash684e52017
[9] A Ciccia and S J Elledge ldquoTheDNAdamage response makingit safe to play with knivesrdquoMolecular Cell vol 40 no 2 pp 179ndash204 2010
[10] L H Pearl A C Schierz S E Ward B Al-Lazikani and F MG Pearl ldquoTherapeutic opportunities within the DNA damageresponserdquo Nature Reviews Cancer vol 15 no 3 pp 166ndash1802015
[11] S-F Yang C-W Chang R-J Wei Y-L Shiue S-N Wang andY-T Yeh ldquoInvolvement of DNA damage response pathways inhepatocellular carcinomardquo BioMed Research International vol2014 Article ID 153867 2014
[12] M He W Zhou C Li and M Guo ldquoMicroRNAs DNAdamage response and cancer treatmentrdquo International Journalof Molecular Sciences vol 17 no 12 article no 2087 2016
[13] K A Cimprich and D Cortez ldquoATR an essential regulator ofgenome integrityrdquo Nature Reviews Molecular Cell Biology vol9 no 8 pp 616ndash627 2008
[14] B M Sirbu and D Cortez ldquoDNA damage response three levelsof DNA repair regulationrdquo Cold Spring Harbor Perspectives inBiology vol 5 article a012724 no 8 2013
BioMed Research International 13
[15] C Beck I Robert B Reina-San-Martin V Schreiber andF Dantzer ldquoPoly(ADP-ribose) polymerases in double-strandbreak repair focus on PARP1 PARP2 and PARP3rdquo Experimen-tal Cell Research vol 329 no 1 pp 18ndash25 2014
[16] D W Meek ldquoTumour suppression by p53 a role for the DNAdamage responserdquo Nature Reviews Cancer vol 9 no 10 pp714ndash723 2009
[17] A Rodrıguez L Torres U Juarez et al ldquoFanconi anemiacells with unrepaired DNA damage activate components of thecheckpoint recovery processrdquo Theoretical Biology and MedicalModelling vol 12 no 1 article 11 2015
[18] H Wang X Zhang L Teng and R J Legerski ldquoDNA damagecheckpoint recovery and cancer developmentrdquo ExperimentalCell Research vol 334 no 2 pp 350ndash358 2015
[19] P A Jeggo L H Pearl and A M Carr ldquoDNA repair genomestability and cancer A historical perspectiverdquo Nature ReviewsCancer vol 16 no 1 pp 35ndash42 2016
[20] F S Alkuraya ldquoPrimordial dwarfism An updaterdquo CurrentOpinion in Endocrinology Diabetes and Obesity vol 22 no 1pp 55ndash64 2015
[21] P Fortini C Ferretti and E Dogliotti ldquoThe response to DNAdamage during differentiation pathways and consequencesrdquoMutation ResearchmdashFundamental and Molecular Mechanismsof Mutagenesis vol 743-744 pp 160ndash168 2013
[22] B R Adams S E Golding R R Rao and K Valerie ldquoDynamicdependence on ATR and ATM for double-Strand break repairin human embryonic stem cells and neural descendantsrdquo PLoSONE vol 5 article e10001 no 4 2010
[23] A Klingseisen and A P Jackson ldquoMechanisms and pathways ofgrowth failure in primordial dwarfismrdquo Genes amp Developmentvol 25 no 19 pp 2011ndash2024 2011
[24] H Mokrani-Benhelli L Gaillard P Biasutto et al ldquoPrimaryMicrocephaly Impaired DNA Replication and Genomic Insta-bility Caused by Compound Heterozygous ATR MutationsrdquoHuman Mutation vol 34 no 2 pp 374ndash384 2013
[25] M OrsquoDriscoll A R Gennery J Seidel P Concannon and PA Jeggo ldquoAn overview of three new disorders associated withgenetic instability LIG4 syndrome RS-SCID and ATR-Seckelsyndromerdquo DNA Repair vol 3 no 8-9 pp 1227ndash1235 2004
[26] P Khetarpal S Das I Panigrahi and A Munshi ldquoPrimordialdwarfism overview of clinical and genetic aspectsrdquo MolecularGenetics and Genomics vol 291 no 1 pp 1ndash15 2016
[27] TOgi SWalker T Stiff et al ldquoIdentification of the First ATRIP-Deficient Patient and Novel Mutations in ATRDefine a ClinicalSpectrum for ATR-ATRIP Seckel Syndromerdquo PLoS Geneticsvol 8 no 11 Article ID e1002945 2012
[28] A Verloes S Drunat and P Gressens Primary autosomalrecessive microcephalies and Seckel syndrome spectrum disor-ders 2013
[29] A D Brown B W Sager A Gorthi S S Tonapi E J Brownand A J R Bishop ldquoATR suppresses endogenous DNA damageand allows completion of homologous recombination repairrdquoPLoS ONE vol 9 article e91222 no 3 2014
[30] E J Brown and D Baltimore ldquoEssential and dispensable rolesof ATR in cell cycle arrest and genome maintenancerdquo Genes ampDevelopment vol 17 no 5 pp 615ndash628 2003
[31] B Fitzgerald M OrsquoDriscoll K Chong S Keating and PShannon ldquoNeuropathology of fetal stage Seckel syndromeA case report providing a morphological correlate for theemerging molecular mechanismsrdquo Brain amp Development vol34 no 3 pp 238ndash243 2012
[32] L I Mullee and C G Morrison ldquoCentrosomes in the DNAdamage responsemdashthe hub outside the centrerdquo ChromosomeResearch vol 24 no 1 pp 35ndash51 2016
[33] K M Takikawa A Kikuchi A Yokoyama et al ldquoPerinatalfindings of Seckel syndrome A case report of a fetus showingprimordial dwarfism and severe microcephalyrdquo Fetal Diagnosisand Therapy vol 24 no 4 pp 405ndash408 2009
[34] Y Ruzankina C Pinzon-Guzman A Asare et al ldquoDeletion ofthe Developmentally Essential Gene ATR in Adult Mice Leadsto Age-Related Phenotypes and Stem Cell Lossrdquo Cell Stem Cellvol 1 no 1 pp 113ndash126 2007
[35] N E Mamrak A Shimamura and N G Howlett ldquoRecentdiscoveries in the molecular pathogenesis of the inherited bonemarrow failure syndrome Fanconi anemiardquo Blood Reviews vol31 no 3 pp 93ndash99 2017
[36] B P Alter ldquoDiagnosis Genetics and Management of InheritedBone Marrow Failure Syndromesrdquo International Journal ofHematology vol 2007 no 1 pp 29ndash39 2007
[37] L B Pontel I V Rosado G Burgos-Barragan et al ldquoEndoge-nous Formaldehyde Is a Hematopoietic Stem Cell Genotoxinand Metabolic Carcinogenrdquo Molecular Cell vol 60 no 1 pp177ndash188 2015
[38] G Pagano P Degan M DrsquoIschia et al ldquoOxidative stress asa multiple effector in Fanconi anaemia clinical phenotyperdquoEuropean Journal of Haematology vol 75 no 2 pp 93ndash1002005
[39] P FGiampietro P CVerlander J GDavis andADAuerbachldquoDiagnosis of Fanconi anemia in patients without congenitalmalformations An International Fanconi Anemia Registrystudyrdquo American Journal of Medical Genetics vol 68 no 1 pp58ndash61 1997
[40] P F Giampietro B Adler-Brecher P C Verlander S GPavlakis J G Davis and A D Auerbach ldquoThe need for moreaccurate and timely diagnosis in Fanconi anemia A report fromthe International Fanconi Anemia Registryrdquo Pediatrics vol 91no 6 pp 1116ndash1120 1993
[41] M P Wajnrajch J M Gertner Z Huma et al ldquoEvaluationof growth and hormonal status in patients referred to theinternational fanconi anemia registryrdquo Pediatrics vol 107 no4 I pp 744ndash754 2001
[42] N Giri D L Batista B P Alter and C A Stratakis ldquoEndocrineabnormalities in patients with fanconi anemiardquo The Journal ofClinical Endocrinology amp Metabolism vol 92 no 7 pp 2624ndash2631 2007
[43] S R Rose K C Myers M M Rutter et al ldquoEndocrine phe-notype of children and adults with Fanconi anemiardquo PediatricBlood amp Cancer vol 59 no 4 pp 690ndash696 2012
[44] A D Auerbach B Adler and R S K Chaganti ldquoPrenatal andpostnatal diagnosis and carrier detection of Fanconi anemia bya cytogeneticmethodrdquoPediatrics vol 67 no 1 pp 128ndash135 1981
[45] A D Auerbach M Sagi and B Adler ldquoFanconi anemiaPrenatal diagnosis in 30 fetuses at riskrdquo Pediatrics vol 76 no5 pp 794ndash800 1985
[46] L Faivre M F Portnoı G Pals et al ldquoShould chromosomebreakage studies be performed in patients with VACTERLassociationrdquo American Journal of Medical Genetics vol 137 no1 pp 55ndash58 2005
[47] B P Alter P S Rosenberg and L C Brody ldquoClinicaland molecular features associated with biallelic mutations inFANCD1BRCA2rdquo Journal ofMedical Genetics vol 44 no 1 pp1ndash9 2007
14 BioMed Research International
[48] K Myers S M Davies R E Harris et al ldquoThe clinicalphenotype of children with Fanconi anemia caused by biallelicFANCD1BRCA2mutationsrdquo Pediatric Blood amp Cancer vol 58no 3 pp 462ndash465 2012
[49] B G Yoon H N Kim U J Han et al ldquoLong-term follow-up of Fanconi anemia Clinical manifestation and treatmentoutcomerdquo Korean Journal of Pediatrics vol 57 no 3 pp 125ndash134 2014
[50] J G Hall ldquoReview and hypothesis Syndromes with severeintrauterine growth restriction and very short stature - Are theyrelated to the epigeneticmechanism(s) of fetal survival involvedin the developmental origins of adult health and diseaserdquoAmerican Journal of Medical Genetics Part A vol 152 no 2 pp512ndash527 2010
[51] A Petryk R K Shankar N Giri et al ldquoEndocrine disordersin Fanconi anemia Recommendations for screening and treat-mentrdquoThe Journal of Clinical Endocrinology ampMetabolism vol100 no 3 pp 803ndash811 2015
[52] S R RoseMM Rutter RMueller et al ldquoBonemineral densityis normal in children with Fanconi anemiardquo Pediatric Blood ampCancer vol 57 no 6 pp 1034ndash1038 2011
[53] A Petryk L E Polgreen J L Barnum et al ldquoBone mineraldensity in childrenwith fanconi anemia after hematopoietic celltransplantationrdquo Biology of Blood and Marrow Transplantationvol 21 no 5 pp 894ndash899 2015
[54] R Purkait A Mukherji S Datta and R Bhadra ldquoRenal arterystenosis An unusual etiology of hypertensive encephalopathyin a childwith fanconi anemiardquo Saudi Journal of KidneyDiseasesand Transplantation vol 26 no 4 pp 778ndash782 2015
[55] K H Chrzanowska H Gregorek B Dembowska-BaginskaM A Kalina and M Digweed ldquoNijmegen breakage syndrome(NBS)rdquoOrphanet Journal of Rare Diseases vol 7 article 13 2012
[56] L C Riches A M Lynch and N J Gooderham ldquoEarly eventsin the mammalian response to DNA double-strand breaksrdquoMutagenesis vol 23 no 5 pp 331ndash339 2008
[57] K Chrzanowska M Kalina H Rysiewski et al ldquoGrowthpattern in patients withNijmegen breakage syndrome evidencefroma longitudinal studyrdquoHormoneResearch in Paediatrics vol74 article S38 2010
[58] Group TINBSS ldquoNijmegen breakage syndromerdquo Archives ofDisease in Childhood vol 82 pp 400ndash406 2000
[59] M Digweed and K Sperling ldquoNijmegen breakage syndromeClinical manifestation of defective response to DNA double-strand breaksrdquo DNA Repair vol 3 no 8-9 pp 1207ndash1217 2004
[60] E Seemanova ldquoAn increased risk for malignant neoplasmsin heterozygotes for a syndrome of microcephaly normalintelligence growth retardation remarkable facies immun-odeficiency and chromosomal instabilityrdquo Mutation ResearchReviews in Genetic Toxicology vol 238 no 3 pp 321ndash324 1990
[61] K H Chrzanowska M Szarras-Czapnik M Gajdulewicz et alldquoHigh prevalence of primary ovarian insufficiency in girls andyoung women with Nijmegen breakage syndrome Evidencefrom a longitudinal studyrdquoThe Journal of Clinical Endocrinologyamp Metabolism vol 95 no 7 pp 3133ndash3140 2010
[62] C M R Weemaes T W J Hustinx J M J C Scheres P J JV Munster J A J M Bakkeren and R D F M Taalman ldquoAnew chromosomal instability disorder The nijmegen breakagesyndromerdquo Acta Paediatrica Scandinavica vol 70 no 4 pp557ndash564 1981
[63] A J Green J R W Yates A M R Taylor et al ldquoSevere micro-cephaly with normal intellectual development The Nijmegen
breakage syndromerdquo Archives of Disease in Childhood vol 73no 5 pp 431ndash434 1995
[64] D Gupta and A Nagarkar ldquoSpeech impairment in Nijmegenbreakage syndrome A rare anomalyrdquo International Journal ofPediatric Otorhinolaryngology vol 73 no 6 pp 873ndash875 2009
[65] P Muschke H Gola R Varon et al ldquoRetrospective diagnosisand subsequent prenatal diagnosis of Nijmegen breakage syn-dromerdquo Prenatal Diagnosis vol 24 no 2 pp 111ndash113 2004
[66] S Pasic M Cupic T Jovanovic S Djukic M Kavaric andI Lazarevic ldquoNijmegen breakage syndrome and chronic pol-yarthritisrdquo Italian Journal of Pediatrics vol 39 no 1 article no59 2013
[67] J P Patel J M Puck R Srinivasan et al ldquoNijmegen BreakageSyndrome Detected by Newborn Screening for T Cell ReceptorExcision Circles (TRECs)rdquo Journal of Clinical Immunology vol35 no 2 pp 227ndash233 2015
[68] I Demuth and M Digweed ldquoThe clinical manifestation of adefective response to DNA double-strand breaks as exemplifiedby Nijmegen breakage syndromerdquoOncogene vol 26 no 56 pp7792ndash7798 2007
[69] H Arora A H Chacon S Choudhary et al ldquoBloom syn-dromerdquo International Journal of Dermatology vol 53 no 7 pp798ndash802 2014
[70] C de Renty and N A Ellis ldquoBloomrsquos syndrome Why not pre-mature aging A comparison of the BLM andWRN helicasesrdquoAgeing Research Reviews vol 33 pp 36ndash51 2017
[71] C Keller K R Keller S B Shew and S E Plon ldquoGrowthdeficiency and malnutrition in Bloom syndromerdquo Journal ofPediatrics vol 134 no 4 pp 472ndash479 1999
[72] A Diaz M G Vogiatzi M M Sanz and J German ldquoEval-uation of short stature carbohydrate metabolism and otherendocrinopathies in Bloomrsquos syndromerdquo Hormone Researchvol 66 no 3 pp 111ndash117 2006
[73] C Ling J Huang Z Yan et al ldquoBloom syndrome complexpromotes FANCM recruitment to stalled replication forksand facilitates both repair and traverse of DNA interstrandcrosslinksrdquo Cell Discovery vol 2 article 16047 2016
[74] J S Renes R H Willemsen A Wagner M J J Finken and AC SHokken-Koelega ldquoBloom syndrome in short children bornsmall for gestational age A challenging diagnosisrdquoThe Journalof Clinical EndocrinologyampMetabolism vol 98 no 10 pp 3932ndash3938 2013
[75] M Maciejczyk B Mikoluc B Pietrucha et al ldquoOxidativestress mitochondrial abnormalities and antioxidant defense inAtaxia-telangiectasia Bloom syndrome andNijmegen breakagesyndromerdquo Redox Biology vol 11 pp 375ndash383 2017
[76] R M Brosh M Bellani Y Liu and M M Seidman ldquoFanconiAnemia A DNA repair disorder characterized by accelerateddecline of the hematopoietic stem cell compartment and otherfeatures of agingrdquo Ageing Research Reviews vol 33 pp 67ndash752017
[77] S Yan M Sorrell and Z Berman ldquoFunctional interplay be-tween ATMATR-mediated DNA damage response and DNArepair pathways in oxidative stressrdquo Cellular and Molecular LifeSciences vol 71 no 20 pp 3951ndash3967 2014
[78] L M M Nardozza A C R Caetano A C P Zamarian etal ldquoFetal growth restriction current knowledgerdquo Archives ofGynecology and Obstetrics vol 295 no 5 pp 1061ndash1077 2017
[79] M Tomas Vila J P Verdu M R Piera and C O AlonsoldquoNijmegen breakage syndrome phenotype a disorder to con-sider in the diagnosis ofmicrocephalyrdquoAnales De Pediatria vol74 pp 58ndash60 2011
Submit your manuscripts athttpswwwhindawicom
Stem CellsInternational
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
MEDIATORSINFLAMMATION
of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Behavioural Neurology
EndocrinologyInternational Journal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Disease Markers
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
BioMed Research International
OncologyJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Oxidative Medicine and Cellular Longevity
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
PPAR Research
The Scientific World JournalHindawi Publishing Corporation httpwwwhindawicom Volume 2014
Immunology ResearchHindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Journal of
ObesityJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Computational and Mathematical Methods in Medicine
OphthalmologyJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Diabetes ResearchJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Research and TreatmentAIDS
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Gastroenterology Research and Practice
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Parkinsonrsquos Disease
Evidence-Based Complementary and Alternative Medicine
Volume 2014Hindawi Publishing Corporationhttpwwwhindawicom

BioMed Research International 13
[15] C Beck I Robert B Reina-San-Martin V Schreiber andF Dantzer ldquoPoly(ADP-ribose) polymerases in double-strandbreak repair focus on PARP1 PARP2 and PARP3rdquo Experimen-tal Cell Research vol 329 no 1 pp 18ndash25 2014
[16] D W Meek ldquoTumour suppression by p53 a role for the DNAdamage responserdquo Nature Reviews Cancer vol 9 no 10 pp714ndash723 2009
[17] A Rodrıguez L Torres U Juarez et al ldquoFanconi anemiacells with unrepaired DNA damage activate components of thecheckpoint recovery processrdquo Theoretical Biology and MedicalModelling vol 12 no 1 article 11 2015
[18] H Wang X Zhang L Teng and R J Legerski ldquoDNA damagecheckpoint recovery and cancer developmentrdquo ExperimentalCell Research vol 334 no 2 pp 350ndash358 2015
[19] P A Jeggo L H Pearl and A M Carr ldquoDNA repair genomestability and cancer A historical perspectiverdquo Nature ReviewsCancer vol 16 no 1 pp 35ndash42 2016
[20] F S Alkuraya ldquoPrimordial dwarfism An updaterdquo CurrentOpinion in Endocrinology Diabetes and Obesity vol 22 no 1pp 55ndash64 2015
[21] P Fortini C Ferretti and E Dogliotti ldquoThe response to DNAdamage during differentiation pathways and consequencesrdquoMutation ResearchmdashFundamental and Molecular Mechanismsof Mutagenesis vol 743-744 pp 160ndash168 2013
[22] B R Adams S E Golding R R Rao and K Valerie ldquoDynamicdependence on ATR and ATM for double-Strand break repairin human embryonic stem cells and neural descendantsrdquo PLoSONE vol 5 article e10001 no 4 2010
[23] A Klingseisen and A P Jackson ldquoMechanisms and pathways ofgrowth failure in primordial dwarfismrdquo Genes amp Developmentvol 25 no 19 pp 2011ndash2024 2011
[24] H Mokrani-Benhelli L Gaillard P Biasutto et al ldquoPrimaryMicrocephaly Impaired DNA Replication and Genomic Insta-bility Caused by Compound Heterozygous ATR MutationsrdquoHuman Mutation vol 34 no 2 pp 374ndash384 2013
[25] M OrsquoDriscoll A R Gennery J Seidel P Concannon and PA Jeggo ldquoAn overview of three new disorders associated withgenetic instability LIG4 syndrome RS-SCID and ATR-Seckelsyndromerdquo DNA Repair vol 3 no 8-9 pp 1227ndash1235 2004
[26] P Khetarpal S Das I Panigrahi and A Munshi ldquoPrimordialdwarfism overview of clinical and genetic aspectsrdquo MolecularGenetics and Genomics vol 291 no 1 pp 1ndash15 2016
[27] TOgi SWalker T Stiff et al ldquoIdentification of the First ATRIP-Deficient Patient and Novel Mutations in ATRDefine a ClinicalSpectrum for ATR-ATRIP Seckel Syndromerdquo PLoS Geneticsvol 8 no 11 Article ID e1002945 2012
[28] A Verloes S Drunat and P Gressens Primary autosomalrecessive microcephalies and Seckel syndrome spectrum disor-ders 2013
[29] A D Brown B W Sager A Gorthi S S Tonapi E J Brownand A J R Bishop ldquoATR suppresses endogenous DNA damageand allows completion of homologous recombination repairrdquoPLoS ONE vol 9 article e91222 no 3 2014
[30] E J Brown and D Baltimore ldquoEssential and dispensable rolesof ATR in cell cycle arrest and genome maintenancerdquo Genes ampDevelopment vol 17 no 5 pp 615ndash628 2003
[31] B Fitzgerald M OrsquoDriscoll K Chong S Keating and PShannon ldquoNeuropathology of fetal stage Seckel syndromeA case report providing a morphological correlate for theemerging molecular mechanismsrdquo Brain amp Development vol34 no 3 pp 238ndash243 2012
[32] L I Mullee and C G Morrison ldquoCentrosomes in the DNAdamage responsemdashthe hub outside the centrerdquo ChromosomeResearch vol 24 no 1 pp 35ndash51 2016
[33] K M Takikawa A Kikuchi A Yokoyama et al ldquoPerinatalfindings of Seckel syndrome A case report of a fetus showingprimordial dwarfism and severe microcephalyrdquo Fetal Diagnosisand Therapy vol 24 no 4 pp 405ndash408 2009
[34] Y Ruzankina C Pinzon-Guzman A Asare et al ldquoDeletion ofthe Developmentally Essential Gene ATR in Adult Mice Leadsto Age-Related Phenotypes and Stem Cell Lossrdquo Cell Stem Cellvol 1 no 1 pp 113ndash126 2007
[35] N E Mamrak A Shimamura and N G Howlett ldquoRecentdiscoveries in the molecular pathogenesis of the inherited bonemarrow failure syndrome Fanconi anemiardquo Blood Reviews vol31 no 3 pp 93ndash99 2017
[36] B P Alter ldquoDiagnosis Genetics and Management of InheritedBone Marrow Failure Syndromesrdquo International Journal ofHematology vol 2007 no 1 pp 29ndash39 2007
[37] L B Pontel I V Rosado G Burgos-Barragan et al ldquoEndoge-nous Formaldehyde Is a Hematopoietic Stem Cell Genotoxinand Metabolic Carcinogenrdquo Molecular Cell vol 60 no 1 pp177ndash188 2015
[38] G Pagano P Degan M DrsquoIschia et al ldquoOxidative stress asa multiple effector in Fanconi anaemia clinical phenotyperdquoEuropean Journal of Haematology vol 75 no 2 pp 93ndash1002005
[39] P FGiampietro P CVerlander J GDavis andADAuerbachldquoDiagnosis of Fanconi anemia in patients without congenitalmalformations An International Fanconi Anemia Registrystudyrdquo American Journal of Medical Genetics vol 68 no 1 pp58ndash61 1997
[40] P F Giampietro B Adler-Brecher P C Verlander S GPavlakis J G Davis and A D Auerbach ldquoThe need for moreaccurate and timely diagnosis in Fanconi anemia A report fromthe International Fanconi Anemia Registryrdquo Pediatrics vol 91no 6 pp 1116ndash1120 1993
[41] M P Wajnrajch J M Gertner Z Huma et al ldquoEvaluationof growth and hormonal status in patients referred to theinternational fanconi anemia registryrdquo Pediatrics vol 107 no4 I pp 744ndash754 2001
[42] N Giri D L Batista B P Alter and C A Stratakis ldquoEndocrineabnormalities in patients with fanconi anemiardquo The Journal ofClinical Endocrinology amp Metabolism vol 92 no 7 pp 2624ndash2631 2007
[43] S R Rose K C Myers M M Rutter et al ldquoEndocrine phe-notype of children and adults with Fanconi anemiardquo PediatricBlood amp Cancer vol 59 no 4 pp 690ndash696 2012
[44] A D Auerbach B Adler and R S K Chaganti ldquoPrenatal andpostnatal diagnosis and carrier detection of Fanconi anemia bya cytogeneticmethodrdquoPediatrics vol 67 no 1 pp 128ndash135 1981
[45] A D Auerbach M Sagi and B Adler ldquoFanconi anemiaPrenatal diagnosis in 30 fetuses at riskrdquo Pediatrics vol 76 no5 pp 794ndash800 1985
[46] L Faivre M F Portnoı G Pals et al ldquoShould chromosomebreakage studies be performed in patients with VACTERLassociationrdquo American Journal of Medical Genetics vol 137 no1 pp 55ndash58 2005
[47] B P Alter P S Rosenberg and L C Brody ldquoClinicaland molecular features associated with biallelic mutations inFANCD1BRCA2rdquo Journal ofMedical Genetics vol 44 no 1 pp1ndash9 2007
14 BioMed Research International
[48] K Myers S M Davies R E Harris et al ldquoThe clinicalphenotype of children with Fanconi anemia caused by biallelicFANCD1BRCA2mutationsrdquo Pediatric Blood amp Cancer vol 58no 3 pp 462ndash465 2012
[49] B G Yoon H N Kim U J Han et al ldquoLong-term follow-up of Fanconi anemia Clinical manifestation and treatmentoutcomerdquo Korean Journal of Pediatrics vol 57 no 3 pp 125ndash134 2014
[50] J G Hall ldquoReview and hypothesis Syndromes with severeintrauterine growth restriction and very short stature - Are theyrelated to the epigeneticmechanism(s) of fetal survival involvedin the developmental origins of adult health and diseaserdquoAmerican Journal of Medical Genetics Part A vol 152 no 2 pp512ndash527 2010
[51] A Petryk R K Shankar N Giri et al ldquoEndocrine disordersin Fanconi anemia Recommendations for screening and treat-mentrdquoThe Journal of Clinical Endocrinology ampMetabolism vol100 no 3 pp 803ndash811 2015
[52] S R RoseMM Rutter RMueller et al ldquoBonemineral densityis normal in children with Fanconi anemiardquo Pediatric Blood ampCancer vol 57 no 6 pp 1034ndash1038 2011
[53] A Petryk L E Polgreen J L Barnum et al ldquoBone mineraldensity in childrenwith fanconi anemia after hematopoietic celltransplantationrdquo Biology of Blood and Marrow Transplantationvol 21 no 5 pp 894ndash899 2015
[54] R Purkait A Mukherji S Datta and R Bhadra ldquoRenal arterystenosis An unusual etiology of hypertensive encephalopathyin a childwith fanconi anemiardquo Saudi Journal of KidneyDiseasesand Transplantation vol 26 no 4 pp 778ndash782 2015
[55] K H Chrzanowska H Gregorek B Dembowska-BaginskaM A Kalina and M Digweed ldquoNijmegen breakage syndrome(NBS)rdquoOrphanet Journal of Rare Diseases vol 7 article 13 2012
[56] L C Riches A M Lynch and N J Gooderham ldquoEarly eventsin the mammalian response to DNA double-strand breaksrdquoMutagenesis vol 23 no 5 pp 331ndash339 2008
[57] K Chrzanowska M Kalina H Rysiewski et al ldquoGrowthpattern in patients withNijmegen breakage syndrome evidencefroma longitudinal studyrdquoHormoneResearch in Paediatrics vol74 article S38 2010
[58] Group TINBSS ldquoNijmegen breakage syndromerdquo Archives ofDisease in Childhood vol 82 pp 400ndash406 2000
[59] M Digweed and K Sperling ldquoNijmegen breakage syndromeClinical manifestation of defective response to DNA double-strand breaksrdquo DNA Repair vol 3 no 8-9 pp 1207ndash1217 2004
[60] E Seemanova ldquoAn increased risk for malignant neoplasmsin heterozygotes for a syndrome of microcephaly normalintelligence growth retardation remarkable facies immun-odeficiency and chromosomal instabilityrdquo Mutation ResearchReviews in Genetic Toxicology vol 238 no 3 pp 321ndash324 1990
[61] K H Chrzanowska M Szarras-Czapnik M Gajdulewicz et alldquoHigh prevalence of primary ovarian insufficiency in girls andyoung women with Nijmegen breakage syndrome Evidencefrom a longitudinal studyrdquoThe Journal of Clinical Endocrinologyamp Metabolism vol 95 no 7 pp 3133ndash3140 2010
[62] C M R Weemaes T W J Hustinx J M J C Scheres P J JV Munster J A J M Bakkeren and R D F M Taalman ldquoAnew chromosomal instability disorder The nijmegen breakagesyndromerdquo Acta Paediatrica Scandinavica vol 70 no 4 pp557ndash564 1981
[63] A J Green J R W Yates A M R Taylor et al ldquoSevere micro-cephaly with normal intellectual development The Nijmegen
breakage syndromerdquo Archives of Disease in Childhood vol 73no 5 pp 431ndash434 1995
[64] D Gupta and A Nagarkar ldquoSpeech impairment in Nijmegenbreakage syndrome A rare anomalyrdquo International Journal ofPediatric Otorhinolaryngology vol 73 no 6 pp 873ndash875 2009
[65] P Muschke H Gola R Varon et al ldquoRetrospective diagnosisand subsequent prenatal diagnosis of Nijmegen breakage syn-dromerdquo Prenatal Diagnosis vol 24 no 2 pp 111ndash113 2004
[66] S Pasic M Cupic T Jovanovic S Djukic M Kavaric andI Lazarevic ldquoNijmegen breakage syndrome and chronic pol-yarthritisrdquo Italian Journal of Pediatrics vol 39 no 1 article no59 2013
[67] J P Patel J M Puck R Srinivasan et al ldquoNijmegen BreakageSyndrome Detected by Newborn Screening for T Cell ReceptorExcision Circles (TRECs)rdquo Journal of Clinical Immunology vol35 no 2 pp 227ndash233 2015
[68] I Demuth and M Digweed ldquoThe clinical manifestation of adefective response to DNA double-strand breaks as exemplifiedby Nijmegen breakage syndromerdquoOncogene vol 26 no 56 pp7792ndash7798 2007
[69] H Arora A H Chacon S Choudhary et al ldquoBloom syn-dromerdquo International Journal of Dermatology vol 53 no 7 pp798ndash802 2014
[70] C de Renty and N A Ellis ldquoBloomrsquos syndrome Why not pre-mature aging A comparison of the BLM andWRN helicasesrdquoAgeing Research Reviews vol 33 pp 36ndash51 2017
[71] C Keller K R Keller S B Shew and S E Plon ldquoGrowthdeficiency and malnutrition in Bloom syndromerdquo Journal ofPediatrics vol 134 no 4 pp 472ndash479 1999
[72] A Diaz M G Vogiatzi M M Sanz and J German ldquoEval-uation of short stature carbohydrate metabolism and otherendocrinopathies in Bloomrsquos syndromerdquo Hormone Researchvol 66 no 3 pp 111ndash117 2006
[73] C Ling J Huang Z Yan et al ldquoBloom syndrome complexpromotes FANCM recruitment to stalled replication forksand facilitates both repair and traverse of DNA interstrandcrosslinksrdquo Cell Discovery vol 2 article 16047 2016
[74] J S Renes R H Willemsen A Wagner M J J Finken and AC SHokken-Koelega ldquoBloom syndrome in short children bornsmall for gestational age A challenging diagnosisrdquoThe Journalof Clinical EndocrinologyampMetabolism vol 98 no 10 pp 3932ndash3938 2013
[75] M Maciejczyk B Mikoluc B Pietrucha et al ldquoOxidativestress mitochondrial abnormalities and antioxidant defense inAtaxia-telangiectasia Bloom syndrome andNijmegen breakagesyndromerdquo Redox Biology vol 11 pp 375ndash383 2017
[76] R M Brosh M Bellani Y Liu and M M Seidman ldquoFanconiAnemia A DNA repair disorder characterized by accelerateddecline of the hematopoietic stem cell compartment and otherfeatures of agingrdquo Ageing Research Reviews vol 33 pp 67ndash752017
[77] S Yan M Sorrell and Z Berman ldquoFunctional interplay be-tween ATMATR-mediated DNA damage response and DNArepair pathways in oxidative stressrdquo Cellular and Molecular LifeSciences vol 71 no 20 pp 3951ndash3967 2014
[78] L M M Nardozza A C R Caetano A C P Zamarian etal ldquoFetal growth restriction current knowledgerdquo Archives ofGynecology and Obstetrics vol 295 no 5 pp 1061ndash1077 2017
[79] M Tomas Vila J P Verdu M R Piera and C O AlonsoldquoNijmegen breakage syndrome phenotype a disorder to con-sider in the diagnosis ofmicrocephalyrdquoAnales De Pediatria vol74 pp 58ndash60 2011
Submit your manuscripts athttpswwwhindawicom
Stem CellsInternational
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
MEDIATORSINFLAMMATION
of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Behavioural Neurology
EndocrinologyInternational Journal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Disease Markers
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
BioMed Research International
OncologyJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Oxidative Medicine and Cellular Longevity
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
PPAR Research
The Scientific World JournalHindawi Publishing Corporation httpwwwhindawicom Volume 2014
Immunology ResearchHindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Journal of
ObesityJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Computational and Mathematical Methods in Medicine
OphthalmologyJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Diabetes ResearchJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Research and TreatmentAIDS
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Gastroenterology Research and Practice
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Parkinsonrsquos Disease
Evidence-Based Complementary and Alternative Medicine
Volume 2014Hindawi Publishing Corporationhttpwwwhindawicom

14 BioMed Research International
[48] K Myers S M Davies R E Harris et al ldquoThe clinicalphenotype of children with Fanconi anemia caused by biallelicFANCD1BRCA2mutationsrdquo Pediatric Blood amp Cancer vol 58no 3 pp 462ndash465 2012
[49] B G Yoon H N Kim U J Han et al ldquoLong-term follow-up of Fanconi anemia Clinical manifestation and treatmentoutcomerdquo Korean Journal of Pediatrics vol 57 no 3 pp 125ndash134 2014
[50] J G Hall ldquoReview and hypothesis Syndromes with severeintrauterine growth restriction and very short stature - Are theyrelated to the epigeneticmechanism(s) of fetal survival involvedin the developmental origins of adult health and diseaserdquoAmerican Journal of Medical Genetics Part A vol 152 no 2 pp512ndash527 2010
[51] A Petryk R K Shankar N Giri et al ldquoEndocrine disordersin Fanconi anemia Recommendations for screening and treat-mentrdquoThe Journal of Clinical Endocrinology ampMetabolism vol100 no 3 pp 803ndash811 2015
[52] S R RoseMM Rutter RMueller et al ldquoBonemineral densityis normal in children with Fanconi anemiardquo Pediatric Blood ampCancer vol 57 no 6 pp 1034ndash1038 2011
[53] A Petryk L E Polgreen J L Barnum et al ldquoBone mineraldensity in childrenwith fanconi anemia after hematopoietic celltransplantationrdquo Biology of Blood and Marrow Transplantationvol 21 no 5 pp 894ndash899 2015
[54] R Purkait A Mukherji S Datta and R Bhadra ldquoRenal arterystenosis An unusual etiology of hypertensive encephalopathyin a childwith fanconi anemiardquo Saudi Journal of KidneyDiseasesand Transplantation vol 26 no 4 pp 778ndash782 2015
[55] K H Chrzanowska H Gregorek B Dembowska-BaginskaM A Kalina and M Digweed ldquoNijmegen breakage syndrome(NBS)rdquoOrphanet Journal of Rare Diseases vol 7 article 13 2012
[56] L C Riches A M Lynch and N J Gooderham ldquoEarly eventsin the mammalian response to DNA double-strand breaksrdquoMutagenesis vol 23 no 5 pp 331ndash339 2008
[57] K Chrzanowska M Kalina H Rysiewski et al ldquoGrowthpattern in patients withNijmegen breakage syndrome evidencefroma longitudinal studyrdquoHormoneResearch in Paediatrics vol74 article S38 2010
[58] Group TINBSS ldquoNijmegen breakage syndromerdquo Archives ofDisease in Childhood vol 82 pp 400ndash406 2000
[59] M Digweed and K Sperling ldquoNijmegen breakage syndromeClinical manifestation of defective response to DNA double-strand breaksrdquo DNA Repair vol 3 no 8-9 pp 1207ndash1217 2004
[60] E Seemanova ldquoAn increased risk for malignant neoplasmsin heterozygotes for a syndrome of microcephaly normalintelligence growth retardation remarkable facies immun-odeficiency and chromosomal instabilityrdquo Mutation ResearchReviews in Genetic Toxicology vol 238 no 3 pp 321ndash324 1990
[61] K H Chrzanowska M Szarras-Czapnik M Gajdulewicz et alldquoHigh prevalence of primary ovarian insufficiency in girls andyoung women with Nijmegen breakage syndrome Evidencefrom a longitudinal studyrdquoThe Journal of Clinical Endocrinologyamp Metabolism vol 95 no 7 pp 3133ndash3140 2010
[62] C M R Weemaes T W J Hustinx J M J C Scheres P J JV Munster J A J M Bakkeren and R D F M Taalman ldquoAnew chromosomal instability disorder The nijmegen breakagesyndromerdquo Acta Paediatrica Scandinavica vol 70 no 4 pp557ndash564 1981
[63] A J Green J R W Yates A M R Taylor et al ldquoSevere micro-cephaly with normal intellectual development The Nijmegen
breakage syndromerdquo Archives of Disease in Childhood vol 73no 5 pp 431ndash434 1995
[64] D Gupta and A Nagarkar ldquoSpeech impairment in Nijmegenbreakage syndrome A rare anomalyrdquo International Journal ofPediatric Otorhinolaryngology vol 73 no 6 pp 873ndash875 2009
[65] P Muschke H Gola R Varon et al ldquoRetrospective diagnosisand subsequent prenatal diagnosis of Nijmegen breakage syn-dromerdquo Prenatal Diagnosis vol 24 no 2 pp 111ndash113 2004
[66] S Pasic M Cupic T Jovanovic S Djukic M Kavaric andI Lazarevic ldquoNijmegen breakage syndrome and chronic pol-yarthritisrdquo Italian Journal of Pediatrics vol 39 no 1 article no59 2013
[67] J P Patel J M Puck R Srinivasan et al ldquoNijmegen BreakageSyndrome Detected by Newborn Screening for T Cell ReceptorExcision Circles (TRECs)rdquo Journal of Clinical Immunology vol35 no 2 pp 227ndash233 2015
[68] I Demuth and M Digweed ldquoThe clinical manifestation of adefective response to DNA double-strand breaks as exemplifiedby Nijmegen breakage syndromerdquoOncogene vol 26 no 56 pp7792ndash7798 2007
[69] H Arora A H Chacon S Choudhary et al ldquoBloom syn-dromerdquo International Journal of Dermatology vol 53 no 7 pp798ndash802 2014
[70] C de Renty and N A Ellis ldquoBloomrsquos syndrome Why not pre-mature aging A comparison of the BLM andWRN helicasesrdquoAgeing Research Reviews vol 33 pp 36ndash51 2017
[71] C Keller K R Keller S B Shew and S E Plon ldquoGrowthdeficiency and malnutrition in Bloom syndromerdquo Journal ofPediatrics vol 134 no 4 pp 472ndash479 1999
[72] A Diaz M G Vogiatzi M M Sanz and J German ldquoEval-uation of short stature carbohydrate metabolism and otherendocrinopathies in Bloomrsquos syndromerdquo Hormone Researchvol 66 no 3 pp 111ndash117 2006
[73] C Ling J Huang Z Yan et al ldquoBloom syndrome complexpromotes FANCM recruitment to stalled replication forksand facilitates both repair and traverse of DNA interstrandcrosslinksrdquo Cell Discovery vol 2 article 16047 2016
[74] J S Renes R H Willemsen A Wagner M J J Finken and AC SHokken-Koelega ldquoBloom syndrome in short children bornsmall for gestational age A challenging diagnosisrdquoThe Journalof Clinical EndocrinologyampMetabolism vol 98 no 10 pp 3932ndash3938 2013
[75] M Maciejczyk B Mikoluc B Pietrucha et al ldquoOxidativestress mitochondrial abnormalities and antioxidant defense inAtaxia-telangiectasia Bloom syndrome andNijmegen breakagesyndromerdquo Redox Biology vol 11 pp 375ndash383 2017
[76] R M Brosh M Bellani Y Liu and M M Seidman ldquoFanconiAnemia A DNA repair disorder characterized by accelerateddecline of the hematopoietic stem cell compartment and otherfeatures of agingrdquo Ageing Research Reviews vol 33 pp 67ndash752017
[77] S Yan M Sorrell and Z Berman ldquoFunctional interplay be-tween ATMATR-mediated DNA damage response and DNArepair pathways in oxidative stressrdquo Cellular and Molecular LifeSciences vol 71 no 20 pp 3951ndash3967 2014
[78] L M M Nardozza A C R Caetano A C P Zamarian etal ldquoFetal growth restriction current knowledgerdquo Archives ofGynecology and Obstetrics vol 295 no 5 pp 1061ndash1077 2017
[79] M Tomas Vila J P Verdu M R Piera and C O AlonsoldquoNijmegen breakage syndrome phenotype a disorder to con-sider in the diagnosis ofmicrocephalyrdquoAnales De Pediatria vol74 pp 58ndash60 2011
Submit your manuscripts athttpswwwhindawicom
Stem CellsInternational
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
MEDIATORSINFLAMMATION
of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Behavioural Neurology
EndocrinologyInternational Journal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Disease Markers
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
BioMed Research International
OncologyJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Oxidative Medicine and Cellular Longevity
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
PPAR Research
The Scientific World JournalHindawi Publishing Corporation httpwwwhindawicom Volume 2014
Immunology ResearchHindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Journal of
ObesityJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Computational and Mathematical Methods in Medicine
OphthalmologyJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Diabetes ResearchJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Research and TreatmentAIDS
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Gastroenterology Research and Practice
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Parkinsonrsquos Disease
Evidence-Based Complementary and Alternative Medicine
Volume 2014Hindawi Publishing Corporationhttpwwwhindawicom

Submit your manuscripts athttpswwwhindawicom
Stem CellsInternational
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
MEDIATORSINFLAMMATION
of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Behavioural Neurology
EndocrinologyInternational Journal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Disease Markers
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
BioMed Research International
OncologyJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Oxidative Medicine and Cellular Longevity
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
PPAR Research
The Scientific World JournalHindawi Publishing Corporation httpwwwhindawicom Volume 2014
Immunology ResearchHindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Journal of
ObesityJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Computational and Mathematical Methods in Medicine
OphthalmologyJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Diabetes ResearchJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Research and TreatmentAIDS
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Gastroenterology Research and Practice
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Parkinsonrsquos Disease
Evidence-Based Complementary and Alternative Medicine
Volume 2014Hindawi Publishing Corporationhttpwwwhindawicom