Embed Size (px)
Citation preview

1
PD-related
Complications
Pr Max Dratwa
Honorary Consultant, Nephrology-Dialysis
CHU Brugmann
Brussels
Hemodialysis Vascular Access Modifies the
Association between Dialysis Modality and Survival Jeffrey Perl, Ron Wald, Philip McFarlane, Joanne M. Bargman,
Edward Vonesh,Yingbo Na, S. Vanita Jassal and Louise Moist
J Am Soc Nephrol 22: ●●●–●●●, 2011. doi: 10.1681/ASN.2010111155
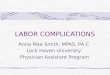
Figure 1. Survival curves for HD-CVC (short-dashed line), HD-
AVF/AVG (long-dashed line), and PD (solid line) demonstrate higher
1-year mortality in HD-CVC patients.
(A) Unadjusted. (B) Adjusted on the basis of a stratified Cox
proportional Hazards model stratified by HD-CVC, PD, and HD-
AVF/AVG and adjusted for age, race, gender, era of dialysis initiation,
end-stage renal disease comorbidity index, primary renal diagnosis,
serum albumin, eGFR, province of treatment, and late referral.
Hemodialysis Vascular Access Modifies
the Association between Dialysis Modality and Survival
Figure 2. Hemodialysis vascular access affects the association between modality
and survival in selected subgroups. *P value for interaction (int).
The models were adjusted for age, race, gender, era of dialysis initiation, ESRD
comorbidity index, primary renal diagnosis, serum albumin, estimated
GFR, province of treatment and late referral.
Perl J et al J Am Soc Nephrol 22: ●●●–●●●, 2011. doi: 10.1681/ASN.2010111155

2
Objective
• Explain the different PD-related complications and their
implications
• Broadly classified by their origin : infectious and non-infectious
Non-infectious complications of PD
• Catheter-related
• Related to elevated abdominal pressure (IPP)
• Degradation of peritoneal membrane
• Related to the presence of PD fluid
Catheter-related complications
• Pain
• Bleeding
• Perforation of bowel
• Leakage
• Malposition and/or obstruction
• Cuff extrusion
• Exit-site and tunnel infections

3
Pain during dialysate inflow or drainage
• usually improvement within few days after start of PD
• reduce speed of the outflow, incomplete dialysate outflow
• biocompatible dialysate (pH-neutral, low GDP concentration)
• intraperitoneal lidocain 2% (3-5 ml/L dialysate)
• Tidal peritoneal dialysis
• only in rare cases: catheter removal required (in this
situation exploration of the peritoneal cavity recommended)
• use curled catheters if restart of PD is planned
Catheter-related
• Difficult inflow or outflow
• Catheter migration
• Catheter obstruction (clot - omental wrapping)
• Action
• First, plain X Ray
• Laxatives
• Inject dialysate under pressure (never aspire!)
• X Ray after injection of contrast
• If no clue, laparoscopic exploration
Catheter-related
Cause Mechanism Early/Late Infusion/Drain
Constipation KT adheres to bowel both Mostly drain
Adhesions <Op Wrapping of
extremity
early both
Adhesions >Op Wrapping of
extremity
late both
Migration Diaphragm constipation both drain
Kinks both Mostly drain
Blood clots early both
Fibrin - Peritonitis Fibrin clots or
purulent fluid
late both

4
Cuff extrusion
with infection
Catheter-related
Catheter migration
Laxatives
Catheter dislocation and drainage problems

5
Uncorrect position of a peritoneal dialysis
catheter with mechanical drainage problems
Catheter
coil IUD
Treatment of catheter dislocation
• Treat meteorism, give laxatives in case of obstipation
• Instillation of 2-2.5 L dialysis fluid
• Gymnastics in order to mobilise the catheter
• If partial dialysate inflow/outflow possible:
try tidal peritoneal dialysis (high fill volume, low tidal volume)
• if conservative therapy unsuccessful:
- catheter manipulation (e.g. with semi-flexible guide wire)
- laparoscopic reposition
- catheter replacement – self locating catheter!
Catheter-related
• Catheter obstruction:
blood clot

6
Catheter-related
Catheter obstruction: fibrin clot
Vanderperren et al; Nephrol Dial Transplant 2002;17:2265-7
Catheter obstruction
• Rinsing/irrigation of the catheter with 50 ml 0.9% sodium
chloride and 5000 IE heparine
• If no improvement: instillation of 50000 IE urokinase
in 5 ml saline for at least 3 hours, 1x/day (can be
repeated twice or three times)
• Avoid streptokinase (chemical peritonitis!)
• If no improvement: catheter removal and
implantation of a new catheter (same session)
Catheter-related
Catheter obstruction: omental wrapping

7
Catheter-related
Drainage problems: Abdominal obesity
Catheter-related
« Personal shortening» of the catheter
Non-infectious complications of PD
•Catheter-related
•Related to elevated abdominal pressure
•Degradation of peritoneal membrane
•Related to the presence of PD fluid

8
Related to increased abdominal pressure
Leaks
Hydrothorax
G-oes. reflux
Appetite
Hernia
Prolapsus
Lumbar pain
Increased IPP
Normal IPP < 16 cm H2O
• Depends of:
• Volume infused + UF
• Position (sitting > standing > lying)
• Age
• Body mass index
• Certain activities : great effort,coughing, defecation (constipation!)
Related to high IPP
Respiratory:
• Alteration of respiratory function
Digestive:
• pancreatitis
• constipation
• gastro-oesophageal reflux

9
Hernia : risk factors
• IPP too high
• Multiparity
• Age?
• Previous surgery
• Previous hernia
• Polycystic kidney disease
Umbilical hernia
Inguino-scrotal hernia
Tintillier M et al; Lancet 2003;362:1893

10
Hernia : attitude
• Assess and treat before starting PD
• Make sure reduction is possible
• Surgical repair always necessary
• Stop PD
• Reintroduce PD with low volumes, supine posture (APD),
increase volume over 2 weeks
Leakage
• Pericatheter : most frequent, early, when early initiation;
easy diagnosis thanks to the presence of glucose (Dextrostix)
• Genital
• Parietal looks like ‘orange skin’ (sometimes in pt’s back!)
• Peritoneo-pleural : dyspnea, clinic and xRay
External dialysate leaks (exit site)
Mostly "early leaks" immediately after catheter implantation
"Late leaks" often associated with sudden increase of intraperitoneal
pressure and/or trauma
Symptoms:
• clear drainage from the exit site (glucose concentration exsudate > blood)
• sometimes edemateous swelling around the catheter (late leaks)
• in unclear cases: CT-peritoneography

11
Pericatheter leak
MRI picture Courtesy A. Vychytyl
Pericatheter leak
MRI picture Courtesy A. Vychytyl
Pericatheter leaks
Therapy:
• Stop PD as long as possible (at least 3-5 days)
• Start APD or CAPD with reduced fill volume
• in case of relapse: stop PD again, continuous drainage of the
peritoneal cavity (continuous connection of an outflow bag)
• Start APD or CAPD with reduced fill volume again after 1 week
• in case of relapse: surgical intervention/implantation of a new
catheter
Prophylaxis:
• exact implantation (paramedian, purse-string suture at the deep cuff)
• "break in" – period for 2 weeks before start of PD
• avoid heavy lifting/physical strain during the first 6-8 weeks

12
Leakage
• Signs : weight & expected drain volume (# UF failure )
• Associated with age and high BMI (Del Peso G et al PDI 2003; 23:249-54)
• Attitude :
• IPP (small volumes, APD)
• Catheter replacement
• Surgery
Peritoneo-pleural leak
Kanaan N et al; Nephrol Dial Transplant 1999;14:1590-2
Symptoms and signs:
•Those of pleural effusion (mostly on the right side)
Peritoneo-pleural leak
Kanaan N et al; Nephrol Dial Transplant 1999;14:1590-2
diagnostic
Thorax XRay
Pleurocentesis (comparison glucose levels pleural/blood) and drainage
Add Methylene Blue in dialysate before : NO! (painful)
Peritoneography (! Request Late Images)
- isotopic albumin*
- CT with contrast
causes
Direct communication (congenital holes)
Indirect communication via lymphatics

13
Peritoneo-pleural leak:management
Kanaan N et al; Nephrol Dial Transplant 1999;14:1590-2
temporary transfer to HD
small infusion volumes
transfer to APD
pleurodesis
• tetracycline
• blood (autologous)
• glue
• talc
Peritoneo-pleural and peritoneo-
mediastinal leak
Coche E et al Eur Radiol 2005; 15:1667-70
Other localisations of leaks
• Scars, open processus vaginalis, retroperitoneal,
pleuroperitoneal, pleuropericardial
• Diagnosis
• Physical examination
• Scintigraphy (Tc99 i.p.)
• CT-peritoneography
• Magnetic resonance imaging

14
Retroperitoneal dialysate leak
CT peritoneography
Non-infectious complications of PD
•Catheter-related
•Related to elevated abdominal pressure
•Degradation of peritoneal membrane
•Related to the presence of PD fluid
Changes in morphology of the peritoneal
membrane
The Peritoneal Biopsy Registry®
Mem
bra
ne T
hic
kness
(µ)
1000
16 15 11 24 54 37 23 8 n =
97 + months 73-96 months
49-72 months 25-48 months
0-24 months HD Uremic Donor
0
1500
500
Williams et al. J Am Soc Nephrol, 13: 470-479, 2002
Normal membrane Long-term PD membrane

15
Spearman Rank Correlation p < 0.01
(n=70)
Grade of vasculopathy
100000
80000
60000
40000
20000
0
0 1 2 3 4
Tota
l glu
cose
exposu
re (
g)
Exposure to Glucose & peritoneal histology
100000 80000 60000 40000 20000 0
5000
4000
3000
2000
1000
0
Pearson correlation p<0.01
(n=70)
Thic
kness
of
com
pact
zone (µ
)
Total Glucose exposure (g)
The Peritoneal Biopsy Registry®
Encapsulating Peritoneal Sclerosis
(EPS)
• Causes a picture of recurrent intestinal obstruction even after
stopping PD in a patient treated since several years with PD
(5 years) + severe peritoneal infections + catheter removal
EPS
Church C & Junor B N Engl J Med 2002;347:737

16
EPS
EPS
Attitude
• TPN during several months
• Adhesiolysis under coelioscopy
• Steroids
• ? Immunosuppression (role of transplantation)
• Tamoxifen (Nolvadex® : breast cancer) 200 mg bid
• ? Maybe keep the PD catheter in place and perform daily short dwell
Bad Prognosis : 50% mortality within 1 year of diagnosis
Non-infectious complications of PD
•Catheter related
•Related to elevated abdominal pressure
•Degradation of peritoneal membrane (increased permeability)
•Related to the presence of PD fluid

17
Dialysate as a diagnostic tool
Dialysate as a diagnostic tool
Causes of bloody dialysate:
- retrograde menstruation - ovulation (back thanks to PD) - peritoneal endometriosis - ectopic pregnancy - ruptured cyst (ADPKD, ovary) - cancer (ovary, colon, kidney) - peritoneal carcinomatosis - pancreatitis - splenic laceration or rupture - EPS - intra-abdominal « catastrophy »
Dialysate as a diagnostic tool
Approach to hemoperitoneum :
-cytologic analysis; Hct:0.3 %
-heparin IP 500-1000 U/2L dwell to prevent clot formation and catheter obstruction
-fast lavages using unwarmed, room t° dialysate (vasoconstriction)

18
Causes of chyloperitoneum -Non-lymphoma abdominal malignancy -Lymphoma -S/p - PD catheter insertion - cholecystectomy -AAA repair -Cirrhosis -Pancreatitis -Amyloidosis -Superior vena cava syndrome -Calcium channel blocker medication
Dialysate as a diagnostic tool
The same with UV light After fluorography
Dialysate as a diagnostic tool
Courtesy E. Goffin