Embed Size (px)
Citation preview

Wearing-off workshop resource kit

Wearing-off
1. Long-term management of PD: Development of levodopa-associated complications
2. Introduction to wearing-off
3. Symptoms of wearing-off
4. The wearing-off study
5. The wearing-off Patient Questionnaire Card
6. Management of wearing-off
7. New perspectives
Long-term management of PD: Development of levodopa-associated complications
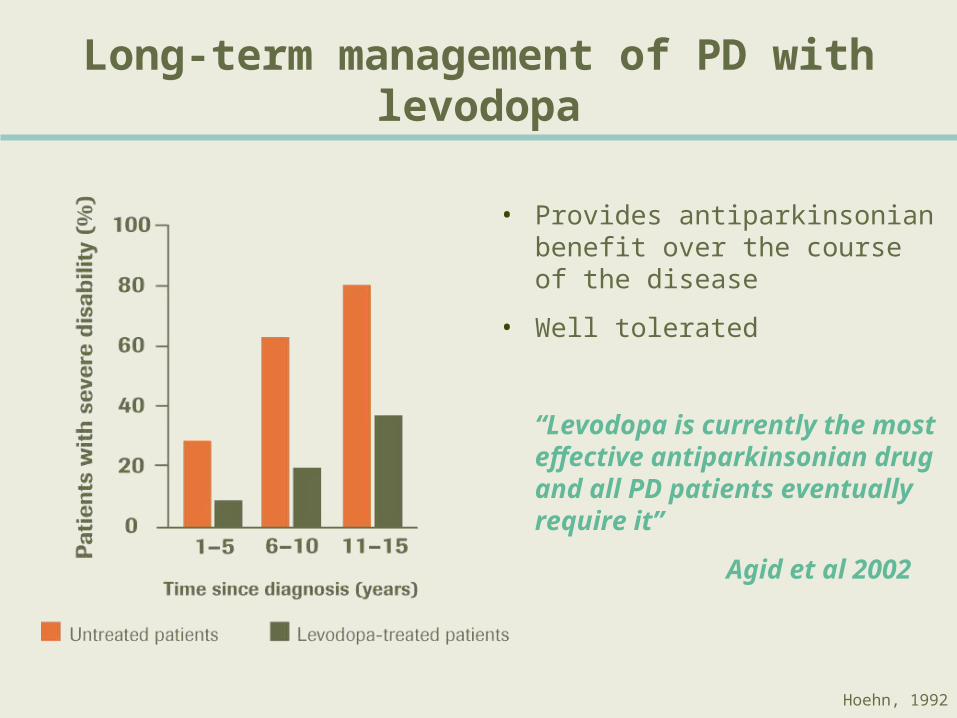
Hoehn, 1992
Long-term management of PD with levodopa
• Provides antiparkinsonian benefit over the course of the disease
• Well tolerated
“Levodopa is currently the most effective antiparkinsonian drug and all PD patients eventually require it”
Agid et al 2002

Beneficial effect of levodopa on life expectancy
Rajput, 2001

Long-term challenges:Changes in levodopa response
Obeso et al. 2000

38%
30%
5%
0
10
20
30
40
50
60
% o
f pa
tient
s
DyskinesiasWearing-off On-off effects
(n=150)
PSG, 2000
Wearing-off was the most commonly encountered motor complication
Incidence of complications in levodopa-treated patients at two years

Introduction to wearing-off

Typical pattern of wearing-off
Daily fluctuations in wearing-off

Impact of wearing-off

Physician survey Patient survey
328 Neurologists
74 Movement Disorder Specialists
54 PCPs
All physicians surveyed treated patients with PD
300 patients with PD treated with carbidopa/levodopa
Sampled through the National Parkinson’s Foundation
The PRELUDE survey
Objective: To understand perceptions of levodopa therapy among clinicians and patients

PRELUDE survey: Importance of wearing-off for patients and healthcare professionals
Managing dyskinesia #1 for
Movement Disorder
Specialists
Managing wearing-off #1 for PD patients
and PCPs
Dyskinesia
Wearing-off
What is the biggest challenge with levodopa therapy?

Within two years 12% of neurologists recognize wearing-off but 54% modify the levodopa regimen
Comtan Diagnostic survey, 2002
The large discrepancy in the numbers (54% Vs 12%) highlights the difficulty in identifying the first signs of wearing-off

Study, year Definition and Incidence
Rajput et al. 2002
A predictable decline in motor function at the end of dose in a patient with previously stable response receiving 3 or more daily levodopa doses
25% of patients had wearing-off after 4.9 years
Parkinson Study Group, 2000
A perception of loss of mobility or dexterity, usually taking place gradually over minutes and usually bearing close resemblance to the timing of antiparkinsonian medications
38% of patients had wearing-off after only 2 years
No universal definition of wearing-off
The lack of a universal definition of wearing-off may be reflected in its reported incidence in patients PSG, 2000
Rajput et al., 2002

Useful definitions of wearing-off
“Wearing-off happens when a dose that
previously used to help your symptoms
does not last as long and your next dose is
needed sooner. Symptoms of wearing-off
include changes in movement and mobility,
thoughts and feelings, sensations and
sense of well being.”
PinK working group
“Wearing-off refers to the predictable
emergence of one or more PD signs or
symptoms before the next scheduled
antiparkinsonian medication dosage.”
For the physician: For the patient:
Stacy et al, 2004
Consensus definition of wearing-off
“A generally predictable recurrence of motor or non motor symptoms that
precedes a scheduled dose and usually improves with antiparkinsonian
medication.”
In September 2004, a wearing-off working group meeting of leading international Movement Disorder Specialists arrived
at a consensus definition.

Symptoms of wearing-off

Wearing-off symptoms
Professor Fabrizio Stocchi

Challenges in identification of wearing-off
“Because patients may not be aware that the changes they are experiencing are related to their PD and are treatable, they may not spontaneously discuss their symptoms…”
“…It is, therefore, important that physicians treating PD be aware of the many different symptoms of wearing-off and specifically ask about the occurrence of such changes.”
Stacy, 2003
Motor fluctuations in wearing-off
• Return of parkinsonian symptoms
• Tremor
• Bradykinesia
• Soft voice
• Early morning stiffness
• Dystonia - often early morning
Non-motor fluctuations (NMF)
• 1976: Marsden and Parkes recognized NMF in fluctuating PD
• 1993: Riley and Lang proposed a classification that is often used today
• 1996: Hillen and Sage studied the frequency of NMF in a fluctuating population
• Using an open-ended question they identified NMF in 17% of fluctuating patients
• 2002: Witjas et al studied the frequency and disability caused by NMF in advanced PD patients
• Using a structured questionnaire they identified NMF in 100% of patients experiencing motor fluctuations
Marsden and Parkes, 1976Riley and Lang, 1993Hillen and Sage, 1996Witjas et al, 2002
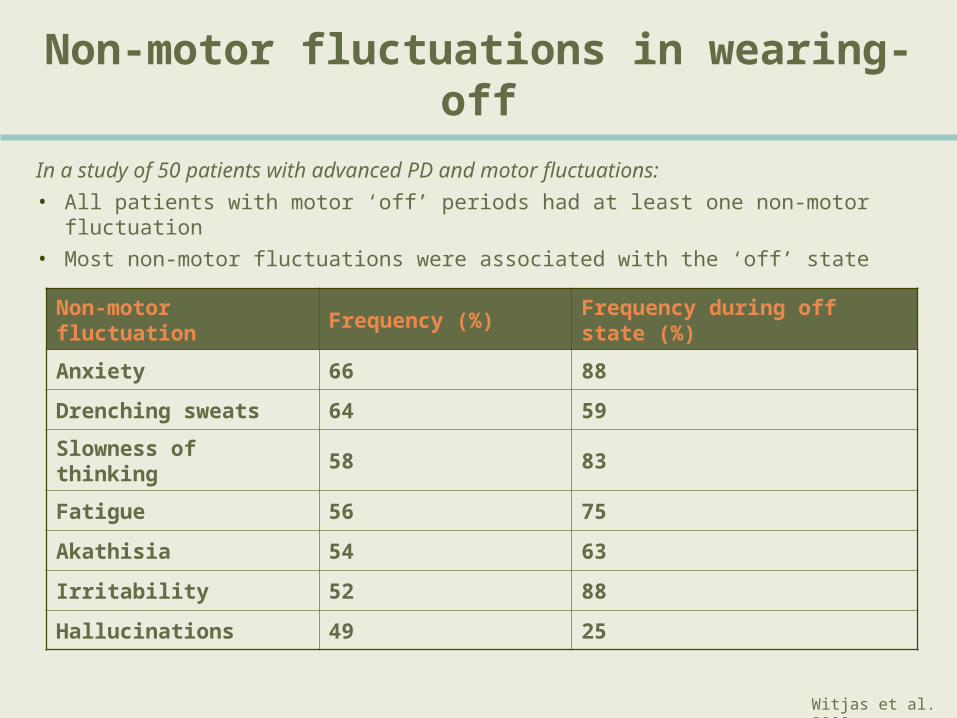
Non-motor fluctuations in wearing-off
Non-motor fluctuation Frequency (%) Frequency during off state (%)
Anxiety 66 88
Drenching sweats 64 59
Slowness of thinking 58 83
Fatigue 56 75
Akathisia 54 63
Irritability 52 88
Hallucinations 49 25
In a study of 50 patients with advanced PD and motor fluctuations:
• All patients with motor ‘off’ periods had at least one non-motor fluctuation
• Most non-motor fluctuations were associated with the ‘off’ state
Witjas et al. 2002

• 150 levodopa treated PD patients were interviewed
• 91% with fluctuations in past 30 days
• Motor symptoms were most bothersome
• The most commonly reported symptoms were:• Tremor 82%• Fatigue 75%• Difficulty moving 68%• Balance 65%• Stiffness 55%• Pain/cramp 48%• Postural changes 47%• Swallowing/speaking 45%
• Sweating 38%
US telephone survey
Novartis telephone surveyData on File

Rationale for the wearing-off study
• Given the variability in the reported frequency of both motor and non-motor fluctuations, it is clear that there are deficits in the identification of wearing-off.
• Consequently, there is a risk that wearing-off symptoms in patients who have been on levodopa therapy for <5 years may go unrecognized by clinicians during routine checks.
• As a result of this, patients with wearing-off symptoms may not be receiving maximal benefit from their therapy.
• The wearing-off study (Ali study) was therefore undertaken with the objective of developing a tool to enable neurologists and other clinicians to work with patients to rapidly and effectively identify wearing-off in their normal clinical practice.

The wearing-off study

The wearing-off study: Aim
To prospectively evaluate whether a specifically designed Patient
Questionnaire can identify the symptoms of ‘wearing-off’ in the same
number, or more, subjects than a clinical assessment conducted by a
Movement Disorder Specialist
Stacy et al., 2004
The wearing-off study: Methods
• 300 consecutive male and female patients with PD were included in the survey.
• All treating physicians were blinded to the survey.
• Clinician Assessment
– UPDRS part IV, question 36.
– Clinical Assessment Question.
• Patient evaluations were assessed using a specifically designed Patient Questionnaire including 32 (motor and non-motor) symptoms.
Stacy et al., 2004

Inclusion and exclusion criteria
Inclusion
• Able to provide informed consent.
• Male or female 30 years of age.
• Diagnosis of idiopathic PD.
• Duration of illness <5 years.
Exclusion
• Duration of PD >5 years.
• Subject unwilling to participate in Patient Questionnaire completion.
• Any other condition or clinical finding that, in the opinion of the Investigator, made the patient unsuitable for enrolment.
Stacy et al., 2004
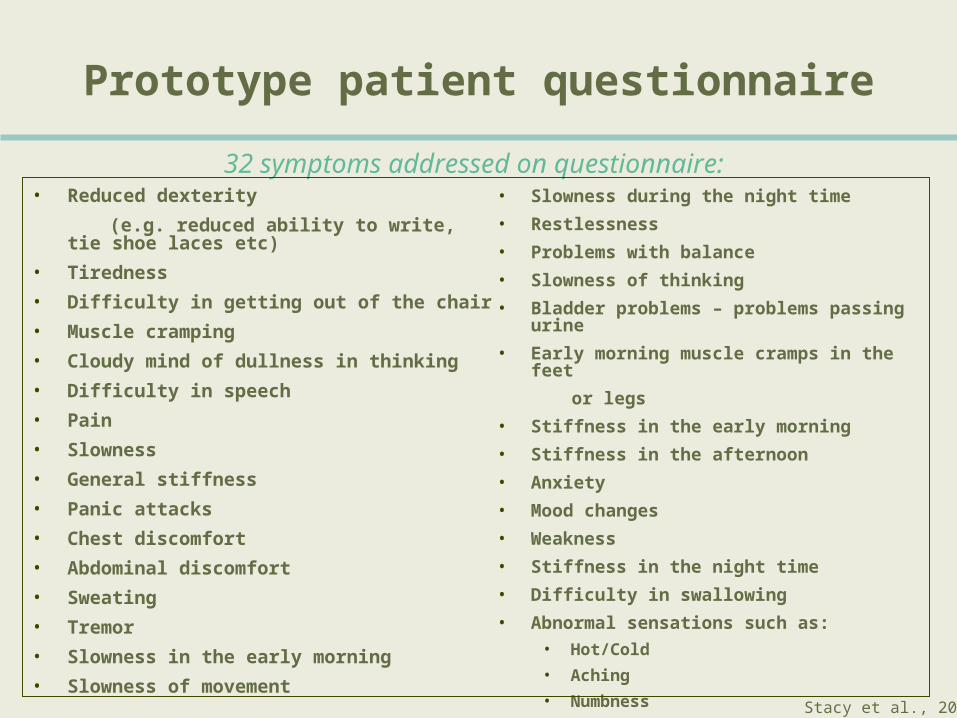
• Reduced dexterity
(e.g. reduced ability to write, tie shoe laces etc)
• Tiredness
• Difficulty in getting out of the chair
• Muscle cramping
• Cloudy mind of dullness in thinking
• Difficulty in speech
• Pain
• Slowness
• General stiffness
• Panic attacks
• Chest discomfort
• Abdominal discomfort
• Sweating
• Tremor
• Slowness in the early morning
• Slowness of movement
Prototype patient questionnaire
• Slowness during the night time
• Restlessness
• Problems with balance
• Slowness of thinking
• Bladder problems – problems passing urine
• Early morning muscle cramps in the feet
or legs
• Stiffness in the early morning
• Stiffness in the afternoon
• Anxiety
• Mood changes
• Weakness
• Stiffness in the night time
• Difficulty in swallowing
• Abnormal sensations such as:
• Hot/Cold
• Aching
• Numbness
32 symptoms addressed on questionnaire:
Stacy et al., 2004

Clinical Assessment Question
In your opinion, does this patient have one or more of the following based on this visit:
Symptom (n) (%)a) Loss of medication efficacy 37 12.8
b) Wearing off 85 29.0
c) Sleepiness 45 15.6
d) Dyskinesia 30 10.4
e) Psychiatric complications 20 6.9
f) Other dopaminergic side effects 15 5.2
g) Morning akinesia 37 12.8
Stacy et al., 2004Data on File

The wearing-off study: Protocol
Principle investigator assesses subject’s eligibility
Blinded clinician performs routine wearing-off study evaluation of the patient’s parkinsonian evaluation, including the Clinical Assessment
Question and the UPDRS
Patient completes Questionnaire. Immediately after survey completion, an independent administrative assistant reviews the completed Questionnaire
with the patient for comprehension and accuracy
The Principal Investigator reviews all survey data prior to entry into the question database
Stacy et al., 2004

Outcome measures
• Primary outcome:
• The frequency of wearing-off as determined by a Clinician Assessment compared to the Patient Questionnaire.
• Secondary outcomes:
• Identification of the types of wearing-off symptoms from Clinician Assessment and Patient Questionnaire.
• Identification of the most troublesome wearing-off symptoms per the Patient Questionnaire.
• The frequency of subjects with troublesome wearing-off symptoms per the Patient Questionnaire..
Stacy et al., 2004

Baseline demographics (n=289)
Male/Female (%) 62/38
Age (years) 72.0 9.6 [4292]
Levodopa therapy (%) 87.5
Duration of levodopa therapy (years) 1.96 1.53
Total UPDRS 36.3 17.9
Hoehn & Yahr
Stage 1 7
Stage 2 77
Stage 2.5 82
Stage 3 84
Stage 4 14
Stacy et al., 2004

Results of the wearing-off study
* p<0.05n=289 total patients
n %
Clinician assessment 85 29.4
UPDRS 36 127 43.9
Patient Questionnaire 165 57.1*
The Patient Questionnaire was superior in identifying wearing-off
Stacy et al., 2004

The Patient Questionnaire was more sensitive at identifying wearing-off than the Clinician Assessment (57.1 % vs 29.4%,
respectively)
Patient Questionnaire versus Clinician Assessment
Stacy et al., 2004

The Patient Questionnaire was more sensitive at identifying wearing-off than UPDRS
question 36 (57.1 % vs 43.9%, respectively)
Patient Questionnaire versus UPDRS 36
UPDRS Q36. Are “off” periods predictable?
Stacy et al., 2004

The wearing-off study: Summary
• With the aid of a questionnaire patients identified symptoms of wearing off more frequently than movement disorder specialists.• Wearing-off was not always noted by clinician, even
though the UPDRS question 36 suggested this symptom was present.
• Questions regarding re-emergence of non-motor symptoms may contribute to the identification of wearing-off.
Stacy et al., 2004
The wearing-off study
Professor Mark Stacy

The wearing-off Patient Questionnaire Card

Development of the Patient Questionnaire Card
It was determined by the working group that:
• A Patient Questionnaire Card of 32 symptoms would not be suitable for general use and that the symptom list should be shortened.
• This procedure should also include reduction of any redundancies in the list of 32 symptoms included in the prototype.
For the purposes of developing the questionnaire into the final
Patient Questionnaire Card, the primary analyses were:
• Ranked identification of the types of wearing-off symptoms included in the prototype Patient Questionnaire.
• Identification of the most troublesome wearing-off symptoms by subject survey.

Development of the Patient Questionnaire Card
2. The relationship between questionnaire-identified wearing-off and individual symptoms explored using discriminate analysis and a stepwise approach to find which were the best predictors.
3. Multiple linear regression analysis undertaken to evaluate which symptoms contributed most to the perception of troublesomeness.
4. Factor analysis used to identify the underlying dimensions within question one of the Patient Questionnaire Card (presence of symptoms).
1. Prototype Patient Questionnaire Card data merged on a patient by patient basis with data from the wearing-off study database.

16 of the 32 questions identified 100% of patients with wearing-off using the prototype patient questionnaire
TremorSlowness in early morning
Anxiety
Slowness during night Mood changes Weakness
Problems with balanceSlowness of movementReduced dexterity
Numbness Stiffness in the afternoon
Stiffness in the morning
Cloudy mind / dullness thinkingAbdominal discomfortSlowness, muscle crampingDifficulty getting out of the chair
1st 3 explain 75.2%
+ next 3 explain 78.7%
+ next 3 explain 93.3%
+ next 3 explain 97.5%
+ next 4 explain 100%

Patient Questionnaire Card Q2: Most troublesome symptoms
n=165
Symptom Total % patientsTremor
Problems with balance
Reduced dexterity
26.7
26.1
25.5
Difficulty in speech
General stiffness
Tiredness
16.4
16.4
15.2
Slowness
Slowness of movement
Slowness of thinking
15.2
12.7
12.1
Difficulty getting out of chair
Weakness
Pain
10.3
8.5
8.5
Muscle cramping
Cloudy Mind
All others
8.5
7.9
<5

19 symptoms included in the consolidated Patient Questionnaire Card
• 16 symptoms were required to capture all subjects with wearing-off. These included 2 definitions of stiffness and 3 of slowness:
• Simplified into general stiffness and slowness of movement.
• Analysis of troublesome symptoms, identified: • Difficulty in speech.• Pain.
• Regression analysis of other symptoms correlated with being troublesome or wishing to change treatment identified: • Sweating.• Experience hot and cold.• Experience panic attacks.• Aching.
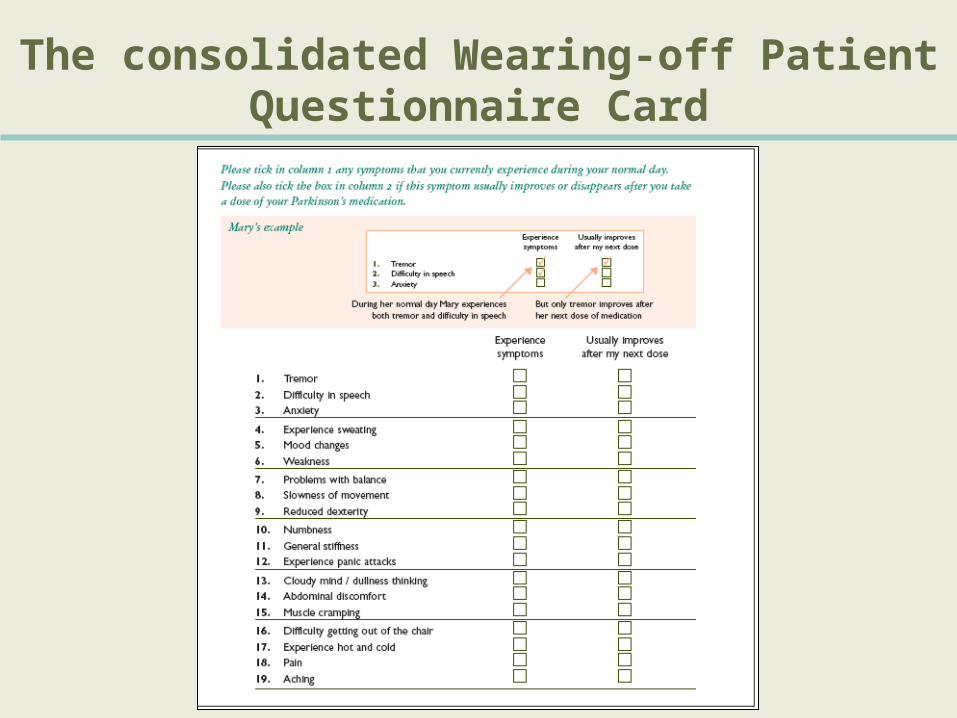
The consolidated Wearing-off Patient Questionnaire Card

Adapted Patient Questionnaire Cards
Patient Questionnaire Card
Professor Kapil Sethi
Management of wearing-off

Identification of wearing-off
Professor Mark Stacy

Development of complications related to dopaminergic therapy
Reduction in the capacity of the striatum to store dopamine
Fluctuations in plasma levodopa levels due to the drug’s short half-life
Progressive degeneration of dopamine neurons
Wearing-off
Ad
van
cin
g P
D
Dyskinesia

Pulsatile dopaminergic receptor activation
1. Pulsatile stimulation contributes to the development of complications related to dopaminergic therapy.
Pulsatile stimulation of brain dopamine receptors results from:
• Loss of striatal dopamine terminals.
• The use of dopaminergic agents with short half-lives.
2. Levodopa has a relatively short half-life (60–90 min).
The therapeutic hypothesis:
Strategies that provide levodopa to the brain in a less pulsatile and ‘more continuous’ manner may reduce the
risk of motor complications

Limitations of traditional strategies to treat wearing-off
Increase dosing frequency
Increase dose Decrease interdose interval Controlled-release preparations
Peak-dose dyskinesias
Limited utility and complicated dosing
schedule beyond 4 to 5 doses/day
Delayed ‘On’ or occasional lack of ‘On’ response with advancing disease
Variable/Short-term Control
Higher peakconcentrations
May work in earlier stages Unpredictable drug absorption
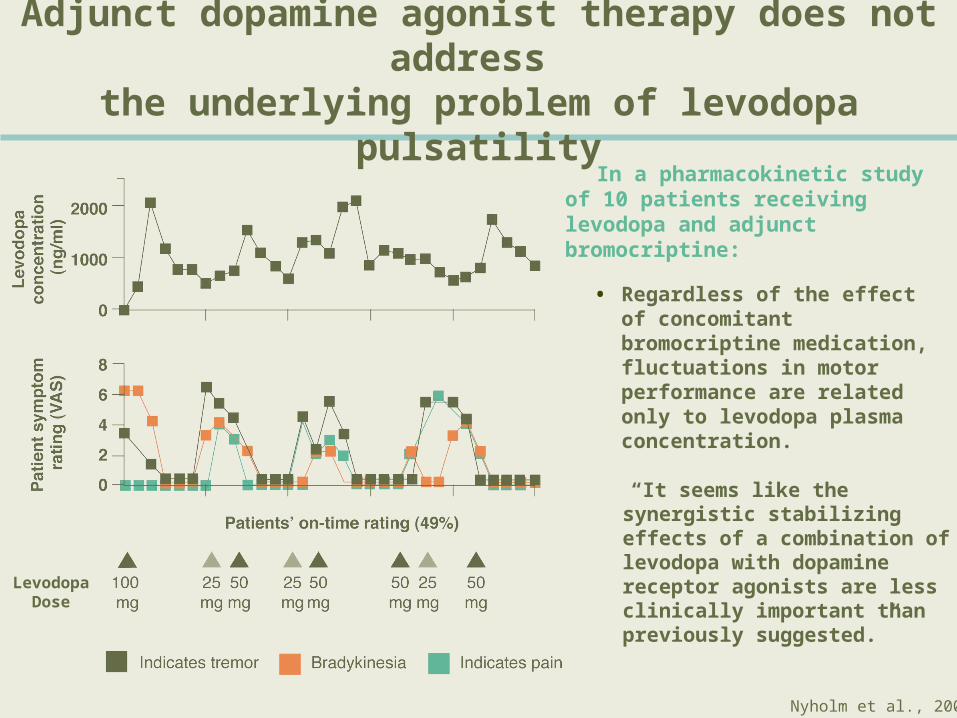
Adjunct dopamine agonist therapy does not address
the underlying problem of levodopa pulsatility In a pharmacokinetic study of 10
patients receiving levodopa and adjunct bromocriptine:
LevodopaDose
• Regardless of the effect of concomitant bromocriptine medication, fluctuations in motor performance are related only to levodopa plasma concentration.
“It seems like the synergistic stabilizing effects of a combination of levodopa with dopamine receptor agonists are less clinically important than previously suggested.”
Nyholm et al., 2002

Optimizing levodopa pharmacokinetics
Dual inhibition leads to increased access of levodopa to the brain
Gordin et al. 2003

Optimizing levodopa therapy: Combining levodopa with entacapone
Stocchi et al. 2003

Optimizing levodopa therapy
Professor Fabrizio Stocchi

New perspectives

Professor Mark Stacy
The wearing-off card – Facilitating a team approach to the treatment of wearing-off

Increasing awareness and improving diagnosis of wearing-off

The management of wearing-off: Role of COMT inhibition
Professor Kapil Sethi





























