Embed Size (px)
Citation preview
Integration I Day 1 CEC/Sim Workbook 1
Integration I NURS 3122 Day 1 Clinical Education Center and Simulation
Learning Activities
Clinical Education Center – 3rd Floor Simulation Center – 5th Floor
Welcome, Attendance and Questions/Answers p.2 2 Instructor 12 students 1 hour and 45 minutes
Welcome, Attendance and Questions/Answers p.82 Instructor12 students 2 hours
Activity #1 p.3 PCA pumps Including Narcan, Sedation scale, Ampules
Simulation #1 ‐Room 2 p.15Scenario #1‐New admission
Activity #2 p.5 Glucometer Including D50
Simulation #2‐Room 2 p.15Scenario #2 New admission‐30 minutes later
Activity #3 p.6 Mobility
Simulation #3‐Room 3 p.15Scenario #3‐1 hour before OR
Activity #4 Developing a Nursing Plan of Care
Simulation #4‐Room 3 p.15Scenario #4‐Transfering to pre‐op
The Clinical Education Center is packed with new clinical content and nursing application Please prepare for the simulation scenarios as you would for a clinical day. Be prepared to provide knowledgeable, effective, and safe patient care in each of the simulation
scenarios today. You will need to prepare for simulation in advance.
Please prepare before this experience:
Complete the Nursing Care Plan tool utilizing the patient data for simulation patient James Snow provided in this workbook.
You will be responsible for pages 1‐4 for simulation experience #1 and pages 5 – 10 for simulation experience #2.
No prep work is necessary for the skills you will be doing in the CEC except for the Care Plan. Just review readings as needed. These will be hands‐on learning activities, so be ready for active engagement.
Please read before this experience:
This workbook
Selected procedures
The assigned article: Bass, N. (2009). Care of the Patient with a Hip Fracture, www.nursingconsult.com. Retrieved from http://www.nursingconsult.com/nursing/clinical‐updates/full‐text?clinical_update_id=191742
Please bring to this experience:
This workbook, please review the simulation in detail. You should be familiar with the patient’s PMH, admitting diagnosis, possible interventions which include medications
Completed Care Plan including medication cards for James Snow
Stethoscope
Clinical resources i.e. pen, penlight, clipboard
Davis Drug book
Enthusiasm and the thirst to acquire nursing knowledge
Integration I Day 1 CEC/Sim Workbook 2
Clinical Education Center
Activity #1
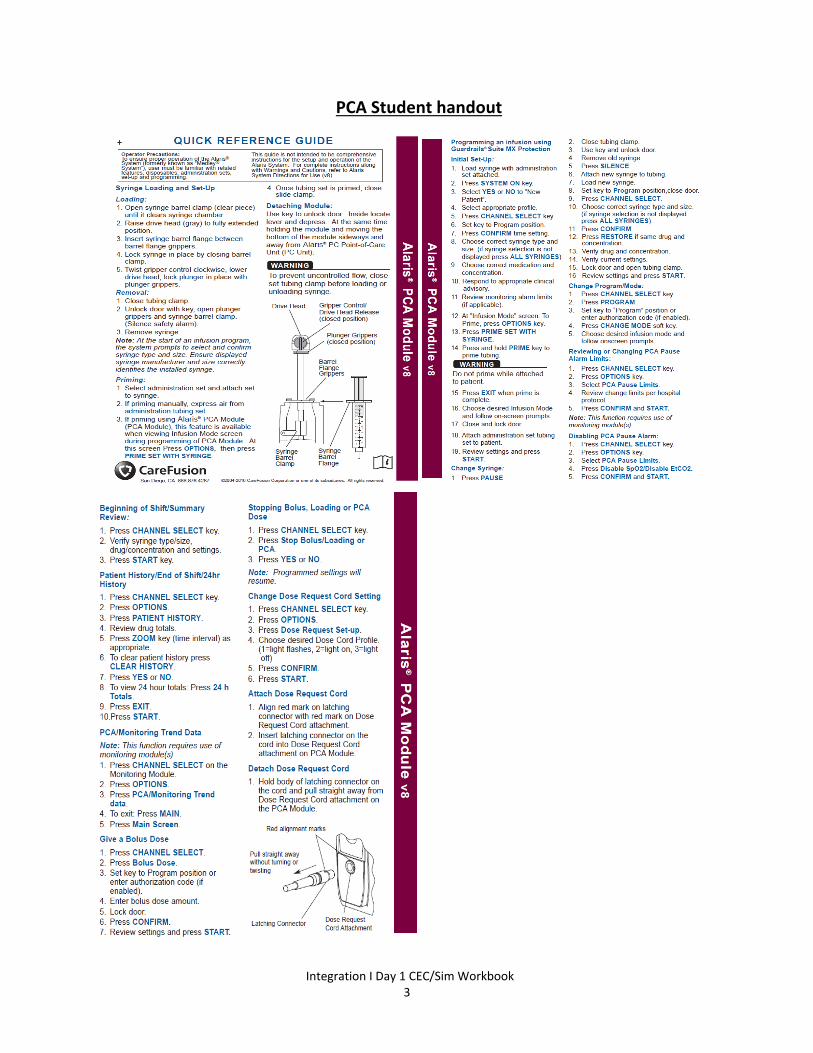
PCA pumps 30 minutes Your role as a student nurse: Review Pain Management: Patient‐Controlled Analgesia, Craven Procedure 34‐1 p. 1174 and p 1163 and p. 486 Review Lewis, Dirksen, Heitkemper, Bucher& Camera (2011) Pain, Chapter 10 p. 144 Preparing medications from Ampules Craven Procedure 19‐4 p. 450 Critical Thinking Exercise:
You are assigned to care for a patient with a PCA. Please provide patient education and verify dose settings including medication, concentration, loading dosed, bolus dose, basal rate, demand dose with lockout time. Also perform a pain assessment, obtain a patient sedation level with respiratory rate, and document total medication dose for 4 hours including dose given, dose attempts and amount infused.
The patient has a respiratory rate of 6 and is unresponsive. Prepare and give 0.1 mg Narcan IV STAT. Narcan is available in a 1mL ampule with a concentration of. 0.4mg/mL.
Activity #2
Glucometer 30 minutes Your role as a student nurse: Review Lewis, Dirksen, Heitkemper, Bucher& Camera (2011) Monitoring Blood Glucose, Chapter 49 p. 1233‐1235 Measuring Blood Glucose by Skin Puncture Craven Procedure 28‐1 p. 914 Critical Thinking Exercise:
You are assigned to obtain blood glucose on James Snow admitted to your medical/surgical unit with a surgical dx of left hip fracture. He is NPO for surgery this afternoon. How would you proceed?
Activity #3
Patient Safety: Mobility 20 minutes Your role as a student nurse: Review Using Body Mechanics to Move Patients, Craven Procedure 24‐1 p. 701 Positioning a patient in Bed, Craven Procedure 24‐2 p. 703 Assisting with Ambulation, Craven Procedure 24‐4 p. 717 Transferring a Patient to a Wheelchair, Craven Procedure 24‐7 p. 727 Critical Thinking Exercise:
Mobility Scenario I: Get patient up to WC or chair BID, Ambulate with walker a minimum of QD. May clamp NG while OOB. (p. 7 in workbook)
Mobility Scenario II: Get patient up to WC or chair BID, Ambulate with walker a minimum of QD. Can place CT to water seal while OOB. (p. 7 in workbook)
Activity #4
Developing a Nursing Plan of Care 20 minutes Your role as a student nurse: Review Lewis, Dirksen, Heitkemper, Bucher& Camera (2011) Concepts in Nursing Practice; Nursing Process in Nursing Practice pg 10 – 17. Critical Thinking Exercise:
Interactive discussion and review of Care Plan for James Snow.
Integration I Day 1 CEC/Sim Workbook 3
PCA Student handout
Integration I Day 1 CEC/Sim Workbook 4
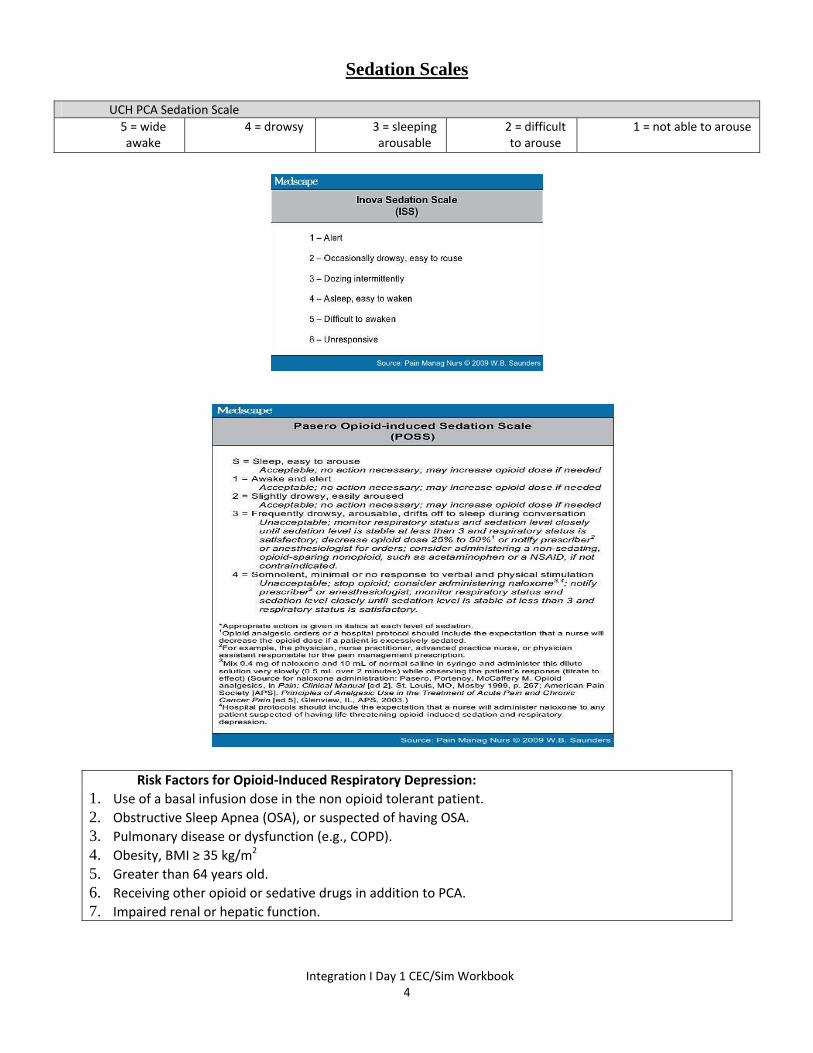
Sedation Scales
UCH PCA Sedation Scale
5 = wide awake
4 = drowsy 3 = sleeping arousable
2 = difficult to arouse
1 = not able to arouse
Risk Factors for Opioid‐Induced Respiratory Depression:
1. Use of a basal infusion dose in the non opioid tolerant patient.
2. Obstructive Sleep Apnea (OSA), or suspected of having OSA.
3. Pulmonary disease or dysfunction (e.g., COPD).
4. Obesity, BMI ≥ 35 kg/m2
5. Greater than 64 years old.
6. Receiving other opioid or sedative drugs in addition to PCA.
7. Impaired renal or hepatic function.
Integration I Day 1 CEC/Sim Workbook 5
Glucometer
Normal Values for FSBG: Before meals: 70‐130 mg/dL After meals: >180 mg/dL Critical values: <40 mg/dL or >450 mg/dL Procedure:
1. Review provider orders to determine type and frequency of glucose monitoring 2. Wash hands and don clean gloves. 3. Identify the patient by asking the patient to state his/her name. Also check the client’s identification band (confirm patient’s identity
using two patient identifiers, based on the hospital protocol). 4. Explain the procedure to the patient or parents (if patient is a child) to gain cooperation. 5. Choose the puncture site. For adults and children fingertips (and earlobe?) can be used. May massage fingertip gently and hold in a
dependent position.
For infants, the tip of the great toe or heel can be the site of puncture. 6. When glucometer is used, load the strip into the device beforehand. Remove test strip from the container and handle according to the
manufacturer’s instructions. May need to do QC with high and low controls (usually done every 24 hours). Make sure the strips have not expired and they are the correct lot number.
7. Swab alcohol pad to the chosen puncture site and allow drying thoroughly. Piecing the skin with a wet skin (alcohol) allows the chemical to pass through the outer layer of the skin thus, causing the procedure more painful and uncomfortable, and causing erroneous readings.
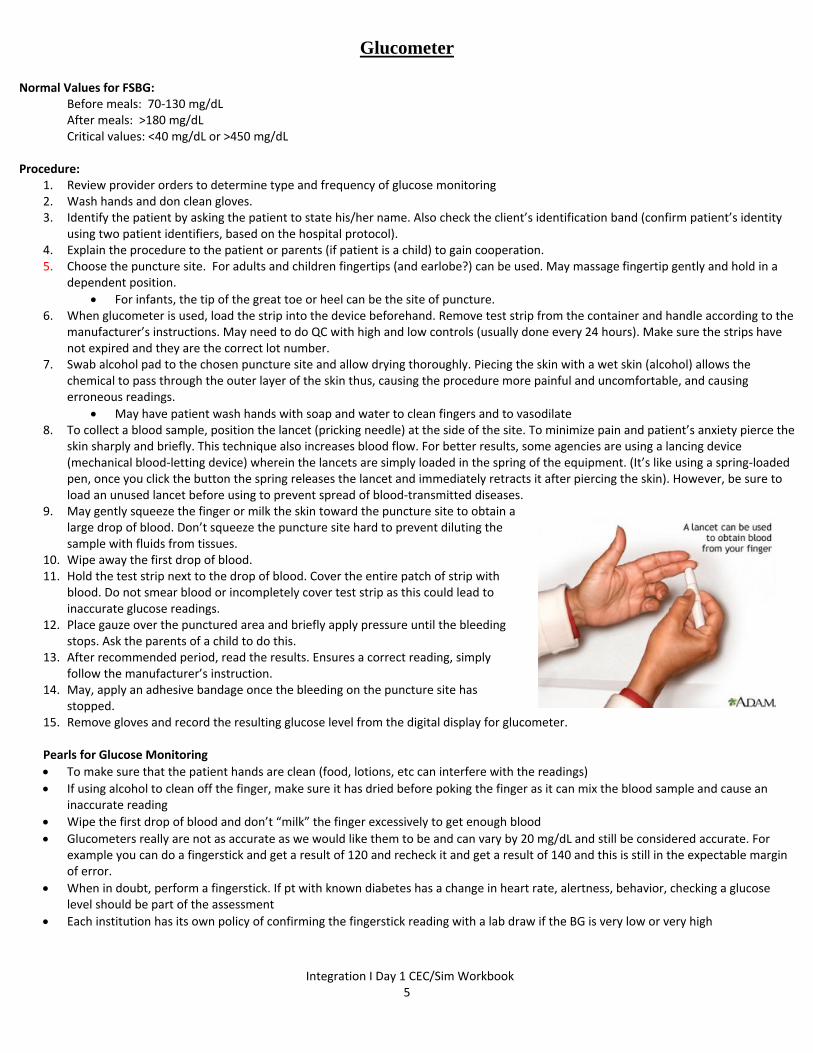
May have patient wash hands with soap and water to clean fingers and to vasodilate 8. To collect a blood sample, position the lancet (pricking needle) at the side of the site. To minimize pain and patient’s anxiety pierce the
skin sharply and briefly. This technique also increases blood flow. For better results, some agencies are using a lancing device (mechanical blood‐letting device) wherein the lancets are simply loaded in the spring of the equipment. (It’s like using a spring‐loaded pen, once you click the button the spring releases the lancet and immediately retracts it after piercing the skin). However, be sure to load an unused lancet before using to prevent spread of blood‐transmitted diseases.
9. May gently squeeze the finger or milk the skin toward the puncture site to obtain a large drop of blood. Don’t squeeze the puncture site hard to prevent diluting the sample with fluids from tissues.
10. Wipe away the first drop of blood. 11. Hold the test strip next to the drop of blood. Cover the entire patch of strip with
blood. Do not smear blood or incompletely cover test strip as this could lead to inaccurate glucose readings.
12. Place gauze over the punctured area and briefly apply pressure until the bleeding stops. Ask the parents of a child to do this.
13. After recommended period, read the results. Ensures a correct reading, simply follow the manufacturer’s instruction.
14. May, apply an adhesive bandage once the bleeding on the puncture site has stopped.
15. Remove gloves and record the resulting glucose level from the digital display for glucometer. Pearls for Glucose Monitoring
To make sure that the patient hands are clean (food, lotions, etc can interfere with the readings)
If using alcohol to clean off the finger, make sure it has dried before poking the finger as it can mix the blood sample and cause an inaccurate reading
Wipe the first drop of blood and don’t “milk” the finger excessively to get enough blood
Glucometers really are not as accurate as we would like them to be and can vary by 20 mg/dL and still be considered accurate. For example you can do a fingerstick and get a result of 120 and recheck it and get a result of 140 and this is still in the expectable margin of error.
When in doubt, perform a fingerstick. If pt with known diabetes has a change in heart rate, alertness, behavior, checking a glucose level should be part of the assessment
Each institution has its own policy of confirming the fingerstick reading with a lab draw if the BG is very low or very high
Integration I Day 1 CEC/Sim Workbook 6
+
MOBILITYIntegration I – Day I
+GATHERING STAGE
What information do I need to get this patient up safely? Do I have an order to mobilize this patient? Has PT already seen them? What were their recommendations? Does the
patient have a transfer sheet? What meds have they gotten recently? What have their vitals signs been like? Have they gotten out of bed before? What safety issues do I need to be aware of – fall risk, impulsivity, confusion,
neurologic deficits, do they need glasses or contacts, orthostatic hypotension?
What equipment do I need to get this patient up safely? What medical devices do they need when OOB – Oxygen, IV fluids/meds,
tube feeding, chest tubes etc. Do they need an orthopedic brace – cervical collar, TLSO, Jewett, splints Do I need any safety equipment – restraints, put on non-skid foot wear/shoes Do I need mobility equipment – walker, gait belt, wheel chair etc.
+CRITICAL THINKING STAGE
YOU HAVE GATHERED ALL NEEDED INFO & SUPPLIES… NOW WHAT? Is this person OK to get up RIGHT now?
What assessment’s can I do to determine this?
LOC
Orthostatic BP & Pulse
Assessment for trunk control:
While lying supine have the patient place his/her arms straight up over their head
Assessment for ability to bear weight:
While lying supine have patient grasp their left foot with their right hand, then their right foot with their left hand
Ask the patient how they were getting around prior to hospital admission
+Key Concepts in Patient Transfers
ALWAYS lock the breaks
ALWAYS make sure you have prepared the environment, your patient, and yourself properly prior to the transfer Always verbalize to your patient your expectations for them during the
transfer
Have the patient do as much as they can for themselves
Never have the patient hold on to your neck
Position what they are transferring to and what they are transferring from as close as possible to each other, at a 35-60 degree angle
Initially transfer the patient toward the stronger side to help them gain confidence
The transfer is only complete once the patient is safely positioned, draped, and has all necessary equipment within reach
+Criteria for Independent Transfers
The patient must CONSISTENTLY perform ALL parts of the transfer.
The patient does not need help with set-up.
The patient does not need to be cued to perform aspects of the transfer.
The patient is able to perform the transfer in a safe and timely manner without assistance.
*If they do not meet these criteria they need to have assistance to transfer*
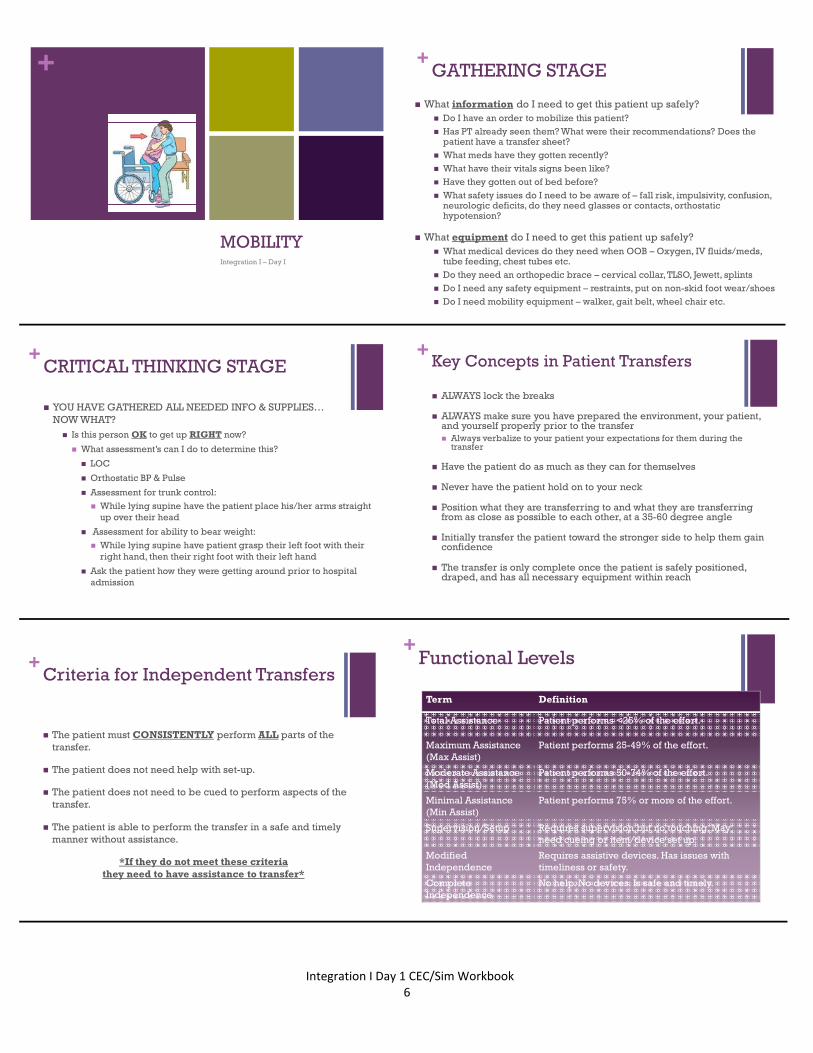
+Functional Levels
Term Definition
Total Assistance Patient performs <25% of the effort.
Maximum Assistance(Max Assist)
Patient performs 25-49% of the effort.
Moderate Assistance(Mod Assist)
Patient performs 50-74% of the effort.
Minimal Assistance(Min Assist)
Patient performs 75% or more of the effort.
Supervision/Setup Requires supervision but no touching. May need cueing or item/device set up.
Modified Independence
Requires assistive devices. Has issues with timeliness or safety.
Complete Independence
No help. No devices. Is safe and timely.
Integration I Day 1 CEC/Sim Workbook 7
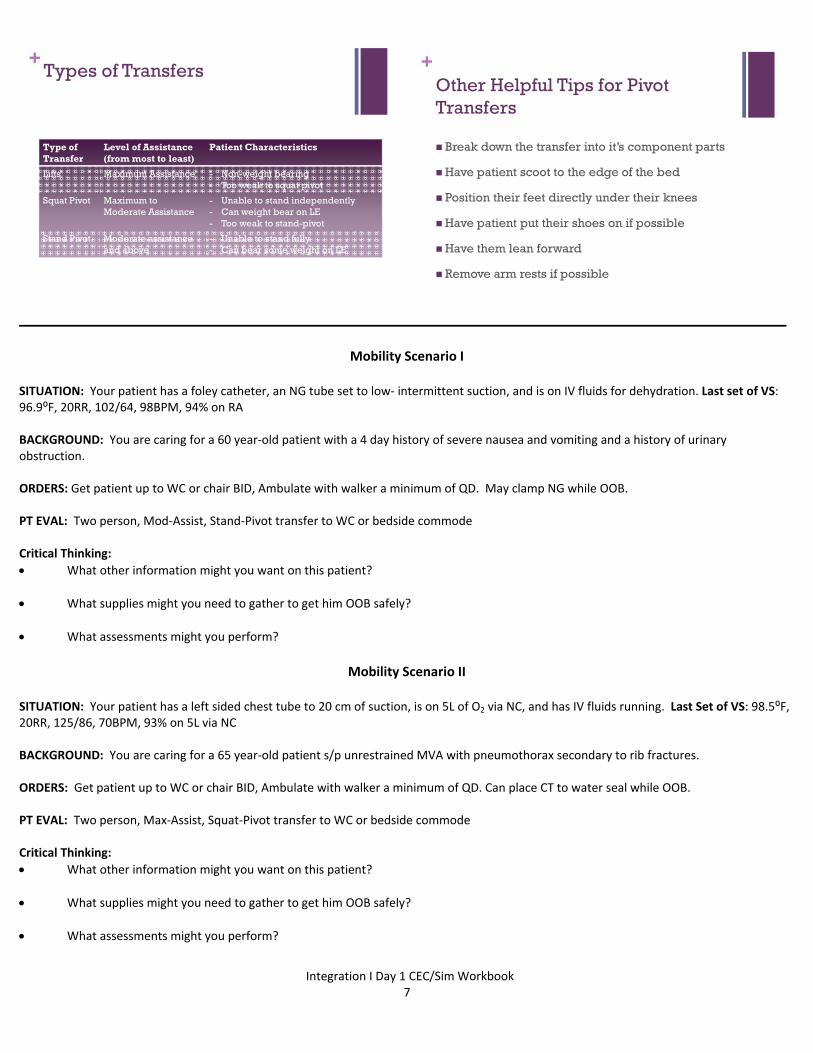
+Types of Transfers
Type of Transfer
Level of Assistance (from most to least)
Patient Characteristics
Lifts Maximum Assistance - Non-weight bearing- Too weak to squat pivot
Squat Pivot Maximum to Moderate Assistance
- Unable to stand independently- Can weight bear on LE- Too weak to stand-pivot
Stand Pivot Moderate assistance and above
- Unable to stand fully- Can bear some weight on LE
+Other Helpful Tips for Pivot Transfers
Break down the transfer into it’s component parts
Have patient scoot to the edge of the bed
Position their feet directly under their knees
Have patient put their shoes on if possible
Have them lean forward
Remove arm rests if possible
Mobility Scenario I
SITUATION: Your patient has a foley catheter, an NG tube set to low‐ intermittent suction, and is on IV fluids for dehydration. Last set of VS: 96.9⁰F, 20RR, 102/64, 98BPM, 94% on RA BACKGROUND: You are caring for a 60 year‐old patient with a 4 day history of severe nausea and vomiting and a history of urinary obstruction. ORDERS: Get patient up to WC or chair BID, Ambulate with walker a minimum of QD. May clamp NG while OOB. PT EVAL: Two person, Mod‐Assist, Stand‐Pivot transfer to WC or bedside commode Critical Thinking:
What other information might you want on this patient?
What supplies might you need to gather to get him OOB safely?
What assessments might you perform?
Mobility Scenario II
SITUATION: Your patient has a left sided chest tube to 20 cm of suction, is on 5L of O2 via NC, and has IV fluids running. Last Set of VS: 98.5⁰F, 20RR, 125/86, 70BPM, 93% on 5L via NC BACKGROUND: You are caring for a 65 year‐old patient s/p unrestrained MVA with pneumothorax secondary to rib fractures. ORDERS: Get patient up to WC or chair BID, Ambulate with walker a minimum of QD. Can place CT to water seal while OOB. PT EVAL: Two person, Max‐Assist, Squat‐Pivot transfer to WC or bedside commode Critical Thinking:
What other information might you want on this patient?
What supplies might you need to gather to get him OOB safely?
What assessments might you perform?

Integration I Day 1 CEC/Sim Workbook 8
Simulation Your role as a student nurse: Please review this workbook including each scenario, the patient’s medical orders, MAR, and admission report Review Lewis, Dirksen, Heitkemper, Bucher& Camera (2011) Chapter 63 p. 1605‐1608 Review Article: Bass, N. (2009). Care of the Patient with a Hip Fracture, www.nursingconsult.com. Retrieved from http://www.nursingconsult.com/nursing/clinical‐updates/full‐text?clinical_update_id=191742 Critical Thinking Exercise:
Be prepared to work for 15 minutes in groups of 3 to complete objectives for each scenario
Three students will actively participate in simulation and 3 students will actively observe
All 6 students will actively participate for 15 minutes with an instructor guided debrief
General Patient Medical Information for All Scenarios Today Primary Medical Diagnosis: Hip Fracture after mechanical fall
History of Present Illness:
Mr. James Snow is a 79 year old male who you are receiving on your Medical Surgical Unit from the Emergency Department. His
diagnosis is left hip fracture (Displaced Femoral Neck) and he is scheduled for surgery later today.
Situation
79 year old male admitted to orthopedic surgeon Dr. Oliver Mitchell with Dx: left hip fracture, plan for surgery later today
Back Ground
Patient is 79 year old male who fell from a ladder this morning while working in his yard. He arrived to the Emergency Department
via ambulance with obvious deformity to left hip and inability to bear weight. He was found to have a hip fracture on X‐Ray left
femoral neck displaced; CT scan of head was negative. An IV was started in the ED, labs were drawn & sent, fluid was started.
He was given 1 mg of Dilaudid for pain in the Emergency Department. He has complained of occasional shortness of breath in the
Emergency Department with a long standing history of COPD and has required Albuterol nebulizer treatment to relieve symptoms of
shortness of breath and wheezing. He also has a history of IDDM & Osteoporosis
PMH: Type 2 DM, COPD, Osteoporosis
He is very anxious about his wife. He is the primary caretaker for his wife who had a stroke last year and requires help with daily
ADLs. He has a son who lives locally and a daughter who lives in California, neither of which the Emergency Department personnel
have not been able to reach.
Assessment:
ED assessment: A & O x 4. S1 S2 no murmurs. Respiratory effort labored with wheezing at times. Now, after Albuterol neb, even and
unlabored with clear breath sounds throughout. BS active x 4 quads. Left cheek and elbow with abrasions. Left Hip with bruising and
abrasions. Left lower extremity CMS intact. Right AC with 18 gauge PIV.
Please see each scenario for specific assessment changes
Recommendations:
Please see each scenario for specific objectives
Integration I Day 1 CEC/Sim Workbook 9
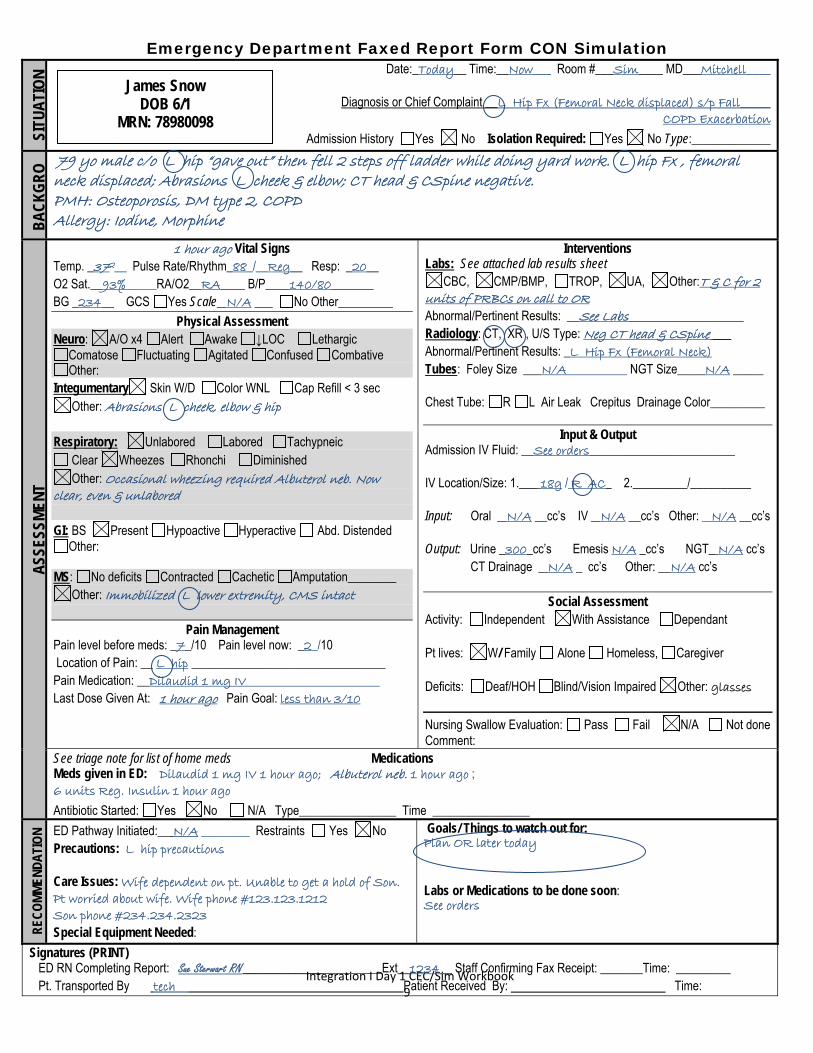
Emergency Department Faxed Report Form CON Simulation SI
TUA
TIO
N Date:_Today__ Time:__Now___ Room #___Sim____ MD___Mitchell____
Diagnosis or Chief Complaint __L Hip Fx (Femoral Neck displaced) s/p Fall_____
COPD Exacerbation Admission History Yes No Isolation Required: Yes No Type:_____________
BA
CK
GR
O 79 yo male c/o L hip “gave out” then fell 2 steps off ladder while doing yard work. L hip Fx , femoral neck displaced; Abrasions L cheek & elbow; CT head & CSpine negative. PMH: Osteoporosis, DM type 2, COPD Allergy: Iodine, Morphine
ASS
ESSM
ENT
1 hour ago Vital Signs Temp. _372__ Pulse Rate/Rhythm_88_/__Reg__ Resp: _20__ O2 Sat.__93%_____RA/O2__RA____ B/P____140/80_______ BG _234__ GCS Yes Scale_ N/A ___ No Other_________
Physical Assessment Neuro: A/O x4 Alert Awake ↓LOC Lethargic
Comatose Fluctuating Agitated Confused Combative Other:
Integumentary Skin W/D Color WNL Cap Refill < 3 sec Other: Abrasions L cheek, elbow & hip
Respiratory: Unlabored Labored Tachypneic
Clear Wheezes Rhonchi Diminished Other: Occasional wheezing required Albuterol neb. Now
clear, even & unlabored GI: BS Present Hypoactive Hyperactive Abd. Distended
Other: MS: No deficits Contracted Cachetic Amputation________
Other: Immobilized L lower extremity, CMS intact
Pain Management Pain level before meds: _7_/10 Pain level now: _2_/10 Location of Pain: __ L hip ________________________________ Pain Medication: __Dilaudid 1 mg IV______________________ Last Dose Given At: 1 hour ago Pain Goal: less than 3/10
Interventions Labs: See attached lab results sheet
CBC, CMP/BMP, TROP, UA, Other:T & C for 2 units of PRBCs on call to OR Abnormal/Pertinent Results: __See Labs___________________ Radiology: CT, XR , U/S Type: Neg CT head & CSpine ___ Abnormal/Pertinent Results: _L Hip Fx (Femoral Neck) Tubes: Foley Size ___N/A__________ NGT Size____ N/A _____ Chest Tube: R L Air Leak Crepitus Drainage Color_________
Input & Output Admission IV Fluid: __See orders________________________ IV Location/Size: 1.___ 18g / R AC_ 2._________/__________ Input: Oral _ N/A __cc’s IV _ N/A __cc’s Other: _ N/A __cc’s Output: Urine _300_cc’s Emesis N/A _cc’s NGT_ N/A cc’s CT Drainage _ N/A _ cc’s Other: __N/A cc’s
Social Assessment
Activity: Independent With Assistance Dependant Pt lives: W/ Family Alone Homeless, Caregiver Deficits: Deaf/HOH Blind/Vision Impaired Other: glasses
Nursing Swallow Evaluation: Pass Fail N/A Not done Comment:
See triage note for list of home meds Medications Meds given in ED: Dilaudid 1 mg IV 1 hour ago; Albuterol neb. 1 hour ago ; 6 units Reg. Insulin 1 hour ago
Antibiotic Started: Yes No N/A Type________________ Time ________________
REC
OM
MEN
DA
TIO
N ED Pathway Initiated:__ N/A ________ Restraints Yes No Precautions: L hip precautions Care Issues: Wife dependent on pt. Unable to get a hold of Son. Pt worried about wife. Wife phone #123.123.1212 Son phone #234.234.2323 Special Equipment Needed:
Goals/ Things to watch out for: Plan OR later today Labs or Medications to be done soon: See orders
Signatures (PRINT) ED RN Completing Report: Sue Sterwart RN_____________________Ext__1234__ Staff Confirming Fax Receipt: _______Time: _________ Pt. Transported By tech Patient Received By: Time:
James Snow DOB 6/1
MRN: 78980098
Integration I Day 1 CEC/Sim Workbook 10
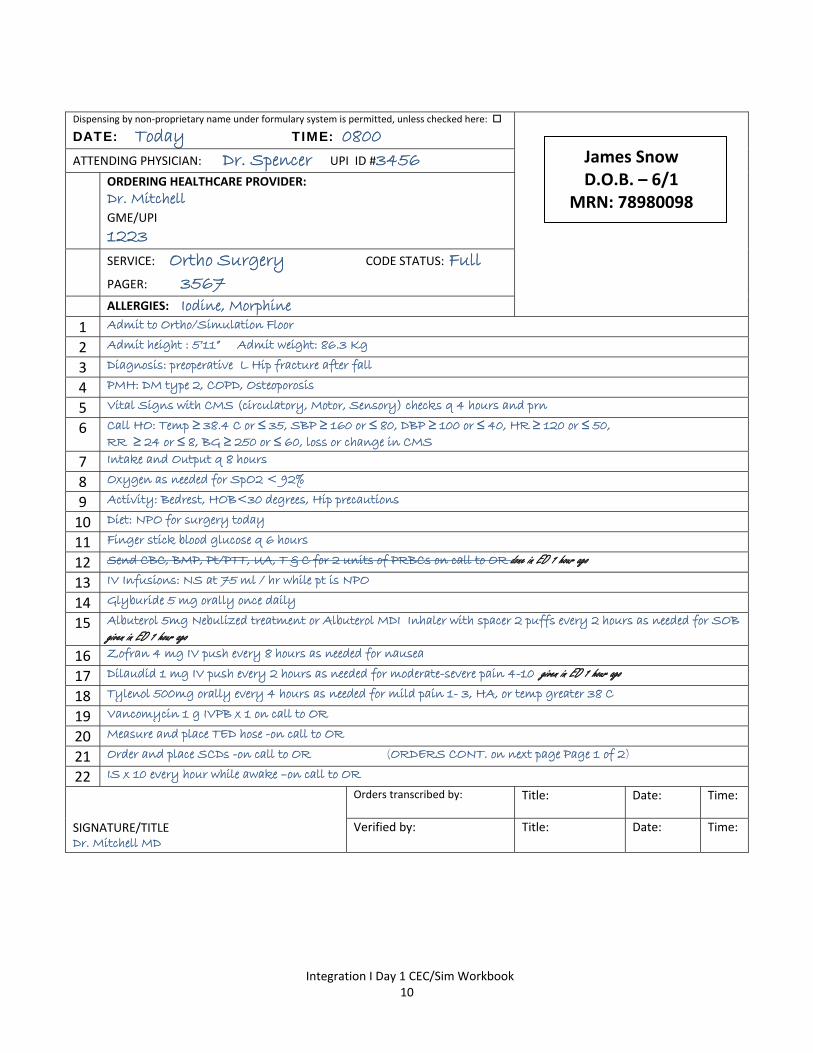
Dispensing by non‐proprietary name under formulary system is permitted, unless checked here:
DATE: Today TIME: 0800
James Snow D.O.B. – 6/1
MRN: 78980098
ATTENDING PHYSICIAN: Dr. Spencer UPI ID #3456
ORDERING HEALTHCARE PROVIDER:
Dr. Mitchell GME/UPI
1223 SERVICE: Ortho Surgery CODE STATUS: Full
PAGER: 3567 ALLERGIES: Iodine, Morphine 1 Admit to Ortho/Simulation Floor
2 Admit height : 5’11” Admit weight: 86.3 Kg
3 Diagnosis: preoperative L Hip fracture after fall
4 PMH: DM type 2, COPD, Osteoporosis
5 Vital Signs with CMS (circulatory, Motor, Sensory) checks q 4 hours and prn
6 Call HO: Temp ≥ 38.4 C or ≤ 35, SBP ≥ 160 or ≤ 80, DBP ≥ 100 or ≤ 40, HR ≥ 120 or ≤ 50, RR ≥ 24 or ≤ 8, BG ≥ 250 or ≤ 60, loss or change in CMS
7 Intake and Output q 8 hours
8 Oxygen as needed for SpO2 < 92%
9 Activity: Bedrest, HOB<30 degrees, Hip precautions
10 Diet: NPO for surgery today
11 Finger stick blood glucose q 6 hours
12 Send CBC, BMP, Pt/PTT, UA, T & C for 2 units of PRBCs on call to OR done in ED 1 hour ago
13 IV Infusions: NS at 75 ml / hr while pt is NPO
14 Glyburide 5 mg orally once daily
15 Albuterol 5mg Nebulized treatment or Albuterol MDI Inhaler with spacer 2 puffs every 2 hours as needed for SOB given in ED 1 hour ago
16 Zofran 4 mg IV push every 8 hours as needed for nausea
17 Dilaudid 1 mg IV push every 2 hours as needed for moderate-severe pain 4-10 given in ED 1 hour ago
18 Tylenol 500mg orally every 4 hours as needed for mild pain 1- 3, HA, or temp greater 38 C
19 Vancomycin 1 g IVPB x 1 on call to OR
20 Measure and place TED hose -on call to OR
21 Order and place SCDs -on call to OR (ORDERS CONT. on next page Page 1 of 2)
22 IS x 10 every hour while awake –on call to OR
SIGNATURE/TITLE Dr. Mitchell MD
Orders transcribed by:
Title: Date: Time:
Verified by:
Title:
Date: Time:
Integration I Day 1 CEC/Sim Workbook 11
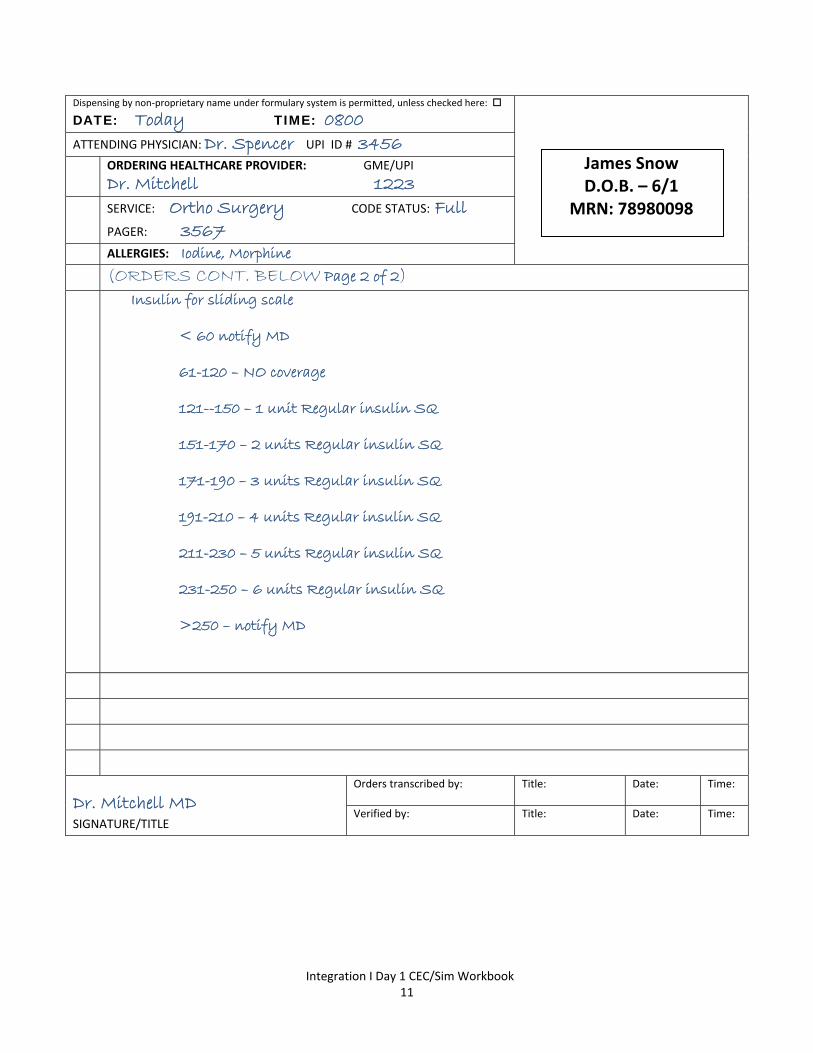
Dispensing by non‐proprietary name under formulary system is permitted, unless checked here:
DATE: Today TIME: 0800
James Snow D.O.B. – 6/1
MRN: 78980098
ATTENDING PHYSICIAN: Dr. Spencer UPI ID # 3456
ORDERING HEALTHCARE PROVIDER: GME/UPI
Dr. Mitchell 1223 SERVICE: Ortho Surgery CODE STATUS: Full
PAGER: 3567 ALLERGIES: Iodine, Morphine
(ORDERS CONT. BELOW Page 2 of 2)
Insulin for sliding scale
< 60 notify MD
61-120 – NO coverage
121--150 – 1 unit Regular insulin SQ
151-170 – 2 units Regular insulin SQ
171-190 – 3 units Regular insulin SQ
191-210 – 4 units Regular insulin SQ
211-230 – 5 units Regular insulin SQ
231-250 – 6 units Regular insulin SQ
>250 – notify MD
Dr. Mitchell MD SIGNATURE/TITLE
Orders transcribed by:
Title: Date: Time:
Verified by:
Title:
Date: Time:
Integration I Day 1 CEC/Sim Workbook 12
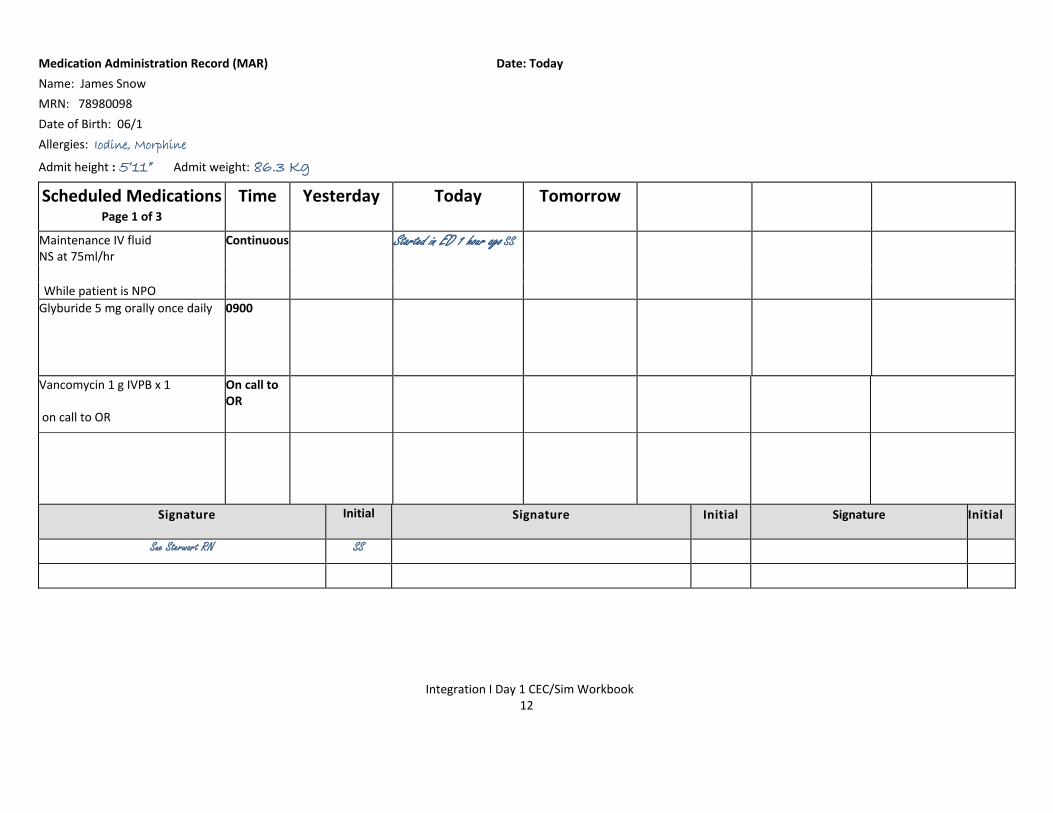
Medication Administration Record (MAR) Date: Today
Name: James Snow
MRN: 78980098
Date of Birth: 06/1
Allergies: Iodine, Morphine
Admit height : 5’11” Admit weight: 86.3 Kg
Scheduled Medications Page 1 of 3
Time Yesterday Today
Tomorrow
Maintenance IV fluid NS at 75ml/hr
Continuous Started in ED 1 hour ago SS
While patient is NPO
Glyburide 5 mg orally once daily 0900
Vancomycin 1 g IVPB x 1 on call to OR
On call to OR
Signature
Initial Signature Initial Signature Initial
Sue Sterwart RN SS
Integration I Day 1 CEC/Sim Workbook 13
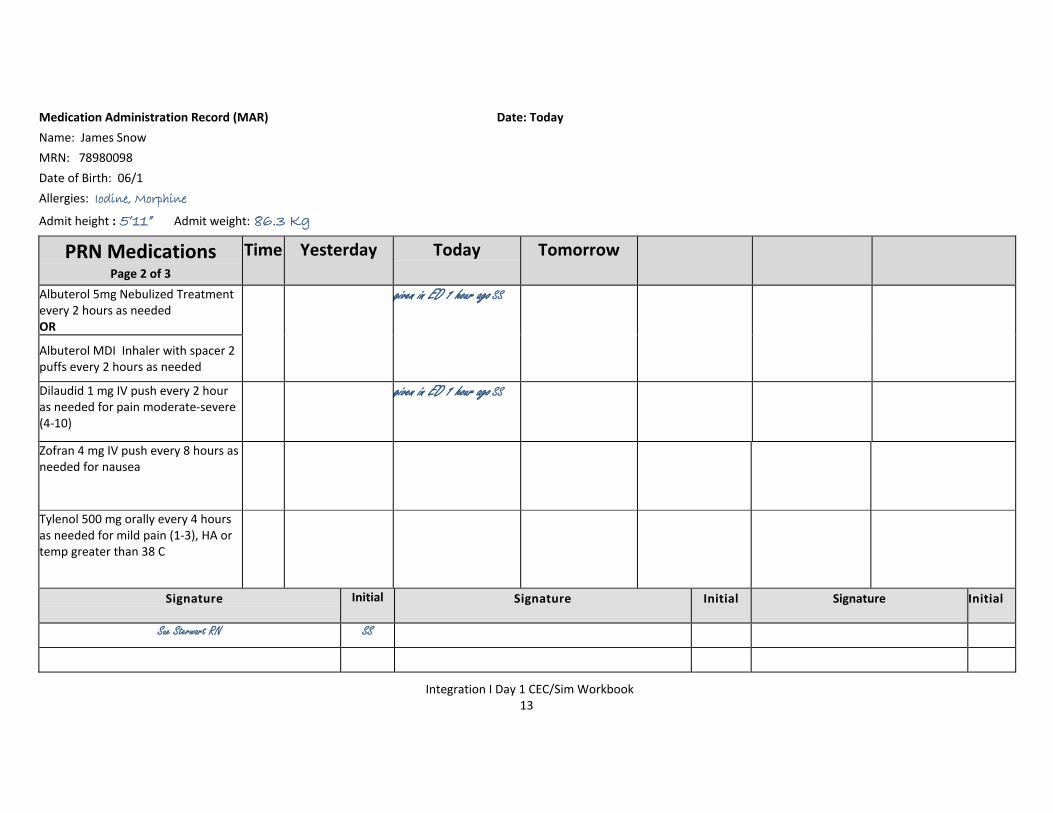
Medication Administration Record (MAR) Date: Today
Name: James Snow
MRN: 78980098
Date of Birth: 06/1
Allergies: Iodine, Morphine
Admit height : 5’11” Admit weight: 86.3 Kg
PRN Medications Page 2 of 3
Time Yesterday Today
Tomorrow
Albuterol 5mg Nebulized Treatment every 2 hours as needed OR
given in ED 1 hour ago SS
Albuterol MDI Inhaler with spacer 2 puffs every 2 hours as needed
Dilaudid 1 mg IV push every 2 hour as needed for pain moderate‐severe (4‐10)
given in ED 1 hour ago SS
Zofran 4 mg IV push every 8 hours as needed for nausea
Tylenol 500 mg orally every 4 hours as needed for mild pain (1‐3), HA or temp greater than 38 C
Signature
Initial Signature Initial Signature Initial
Sue Sterwart RN SS
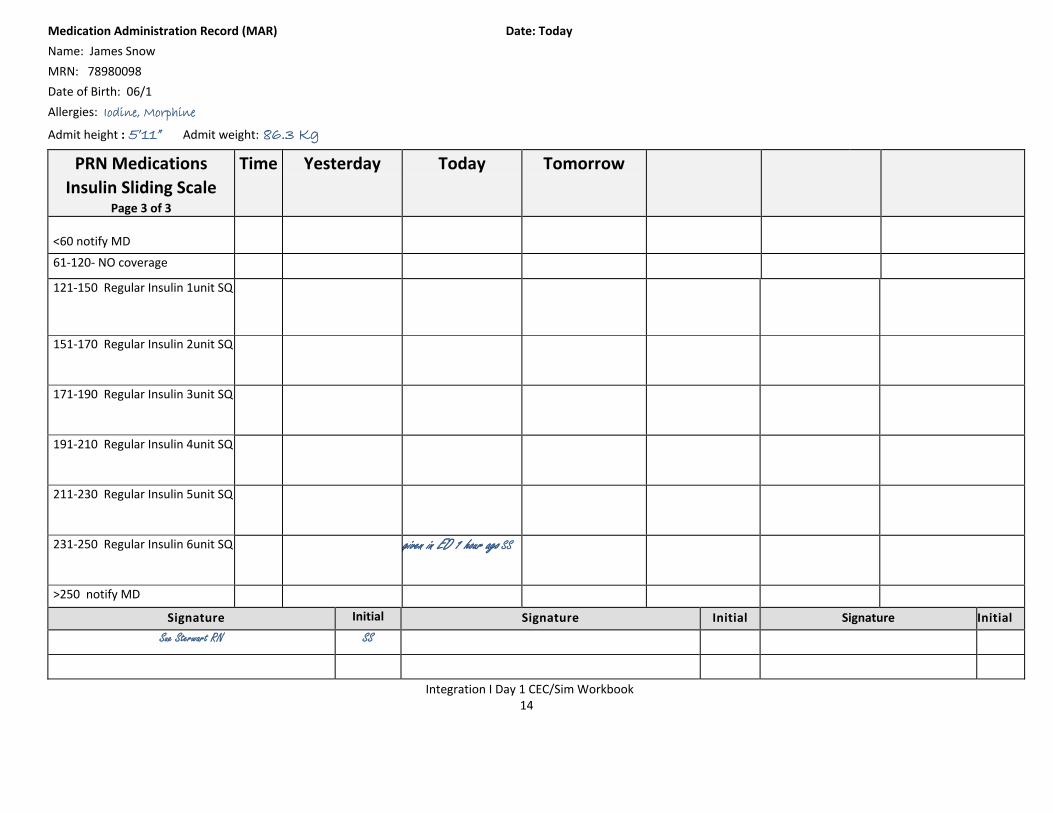
Integration I Day 1 CEC/Sim Workbook 14
Medication Administration Record (MAR) Date: Today
Name: James Snow
MRN: 78980098
Date of Birth: 06/1
Allergies: Iodine, Morphine
Admit height : 5’11” Admit weight: 86.3 Kg
PRN Medications
Insulin Sliding Scale Page 3 of 3
Time Yesterday Today Tomorrow
<60 notify MD
61‐120‐ NO coverage
121‐150 Regular Insulin 1unit SQ
151‐170 Regular Insulin 2unit SQ
171‐190 Regular Insulin 3unit SQ
191‐210 Regular Insulin 4unit SQ
211‐230 Regular Insulin 5unit SQ
231‐250 Regular Insulin 6unit SQ given in ED 1 hour ago SS
>250 notify MD
Signature Initial Signature Initial Signature Initial
Sue Sterwart RN SS
Integration I Day 1 CEC/Sim Workbook 15
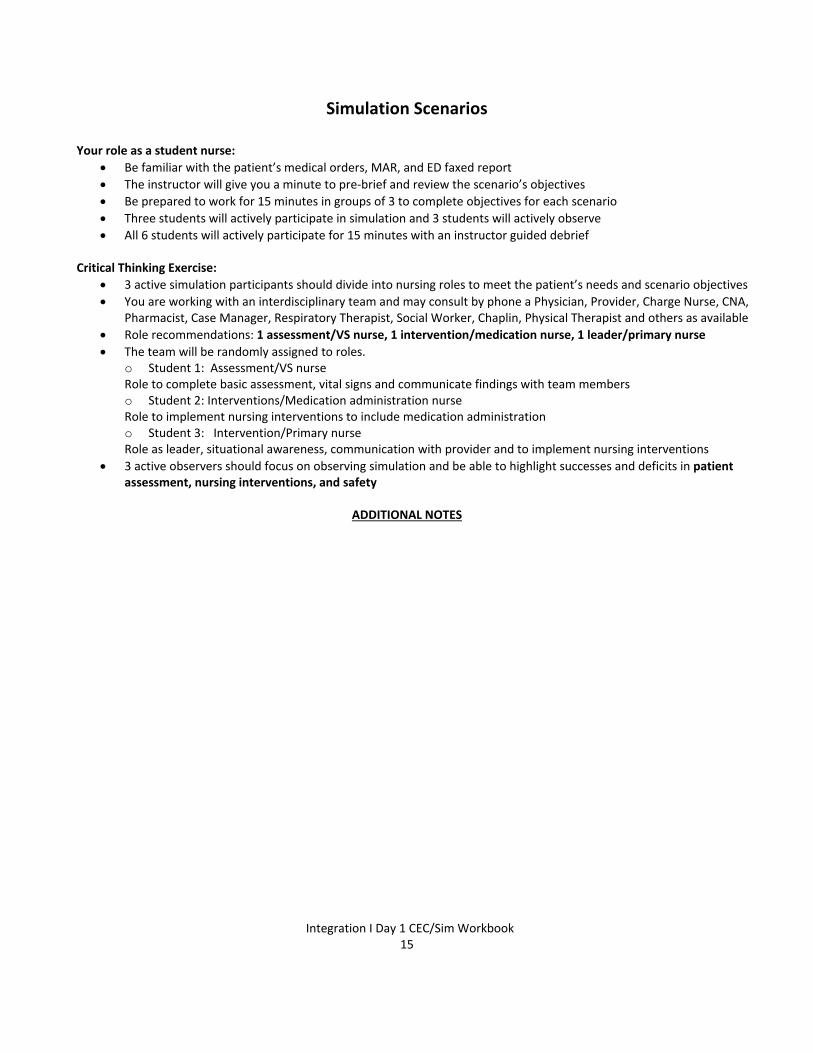
Simulation Scenarios
Your role as a student nurse:
Be familiar with the patient’s medical orders, MAR, and ED faxed report
The instructor will give you a minute to pre‐brief and review the scenario’s objectives
Be prepared to work for 15 minutes in groups of 3 to complete objectives for each scenario
Three students will actively participate in simulation and 3 students will actively observe
All 6 students will actively participate for 15 minutes with an instructor guided debrief Critical Thinking Exercise:
3 active simulation participants should divide into nursing roles to meet the patient’s needs and scenario objectives
You are working with an interdisciplinary team and may consult by phone a Physician, Provider, Charge Nurse, CNA, Pharmacist, Case Manager, Respiratory Therapist, Social Worker, Chaplin, Physical Therapist and others as available
Role recommendations: 1 assessment/VS nurse, 1 intervention/medication nurse, 1 leader/primary nurse
The team will be randomly assigned to roles. o Student 1: Assessment/VS nurse Role to complete basic assessment, vital signs and communicate findings with team members o Student 2: Interventions/Medication administration nurse Role to implement nursing interventions to include medication administration o Student 3: Intervention/Primary nurse Role as leader, situational awareness, communication with provider and to implement nursing interventions
3 active observers should focus on observing simulation and be able to highlight successes and deficits in patient assessment, nursing interventions, and safety
ADDITIONAL NOTES
Integration I Day 1 CEC/Sim Workbook 16
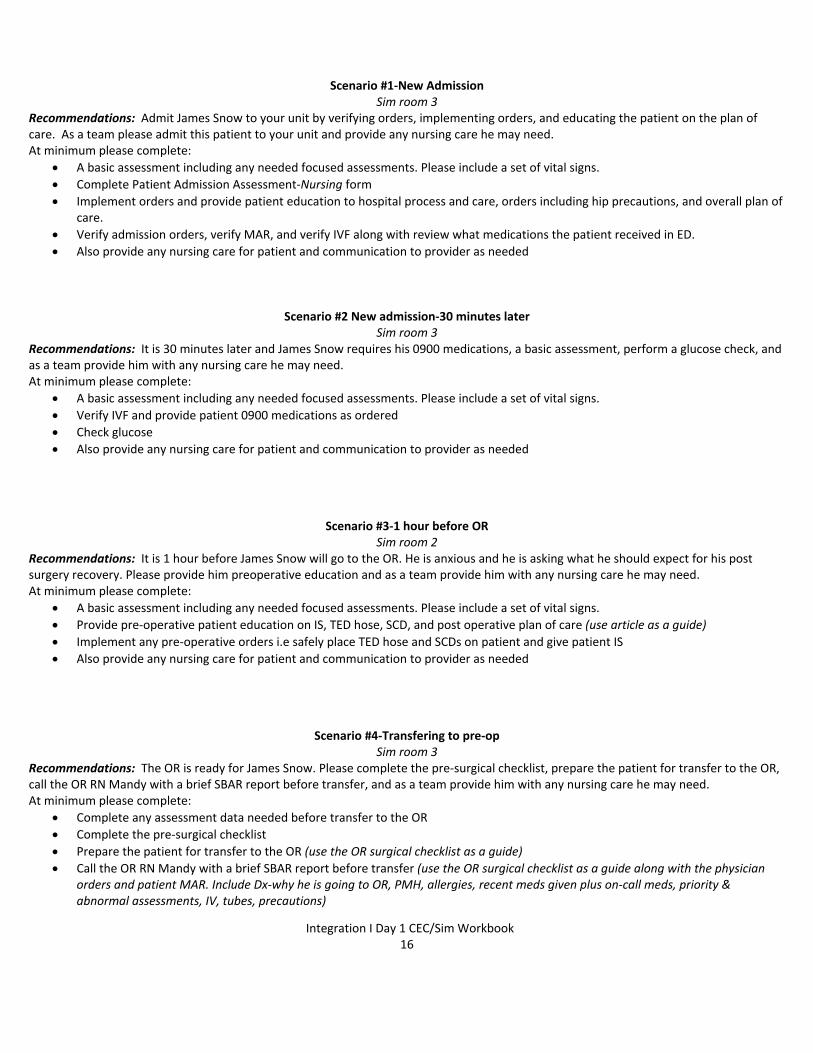
Scenario #1‐New Admission Sim room 3
Recommendations: Admit James Snow to your unit by verifying orders, implementing orders, and educating the patient on the plan of care. As a team please admit this patient to your unit and provide any nursing care he may need. At minimum please complete:
A basic assessment including any needed focused assessments. Please include a set of vital signs.
Complete Patient Admission Assessment‐Nursing form
Implement orders and provide patient education to hospital process and care, orders including hip precautions, and overall plan of care.
Verify admission orders, verify MAR, and verify IVF along with review what medications the patient received in ED.
Also provide any nursing care for patient and communication to provider as needed
Scenario #2 New admission‐30 minutes later Sim room 3
Recommendations: It is 30 minutes later and James Snow requires his 0900 medications, a basic assessment, perform a glucose check, and as a team provide him with any nursing care he may need. At minimum please complete:
A basic assessment including any needed focused assessments. Please include a set of vital signs.
Verify IVF and provide patient 0900 medications as ordered
Check glucose
Also provide any nursing care for patient and communication to provider as needed
Scenario #3‐1 hour before OR Sim room 2
Recommendations: It is 1 hour before James Snow will go to the OR. He is anxious and he is asking what he should expect for his post surgery recovery. Please provide him preoperative education and as a team provide him with any nursing care he may need. At minimum please complete:
A basic assessment including any needed focused assessments. Please include a set of vital signs.
Provide pre‐operative patient education on IS, TED hose, SCD, and post operative plan of care (use article as a guide)
Implement any pre‐operative orders i.e safely place TED hose and SCDs on patient and give patient IS
Also provide any nursing care for patient and communication to provider as needed
Scenario #4‐Transfering to pre‐op Sim room 3
Recommendations: The OR is ready for James Snow. Please complete the pre‐surgical checklist, prepare the patient for transfer to the OR, call the OR RN Mandy with a brief SBAR report before transfer, and as a team provide him with any nursing care he may need. At minimum please complete:
Complete any assessment data needed before transfer to the OR
Complete the pre‐surgical checklist
Prepare the patient for transfer to the OR (use the OR surgical checklist as a guide)
Call the OR RN Mandy with a brief SBAR report before transfer (use the OR surgical checklist as a guide along with the physician orders and patient MAR. Include Dx‐why he is going to OR, PMH, allergies, recent meds given plus on‐call meds, priority & abnormal assessments, IV, tubes, precautions)
Integration I Day 1 CEC/Sim Workbook 17
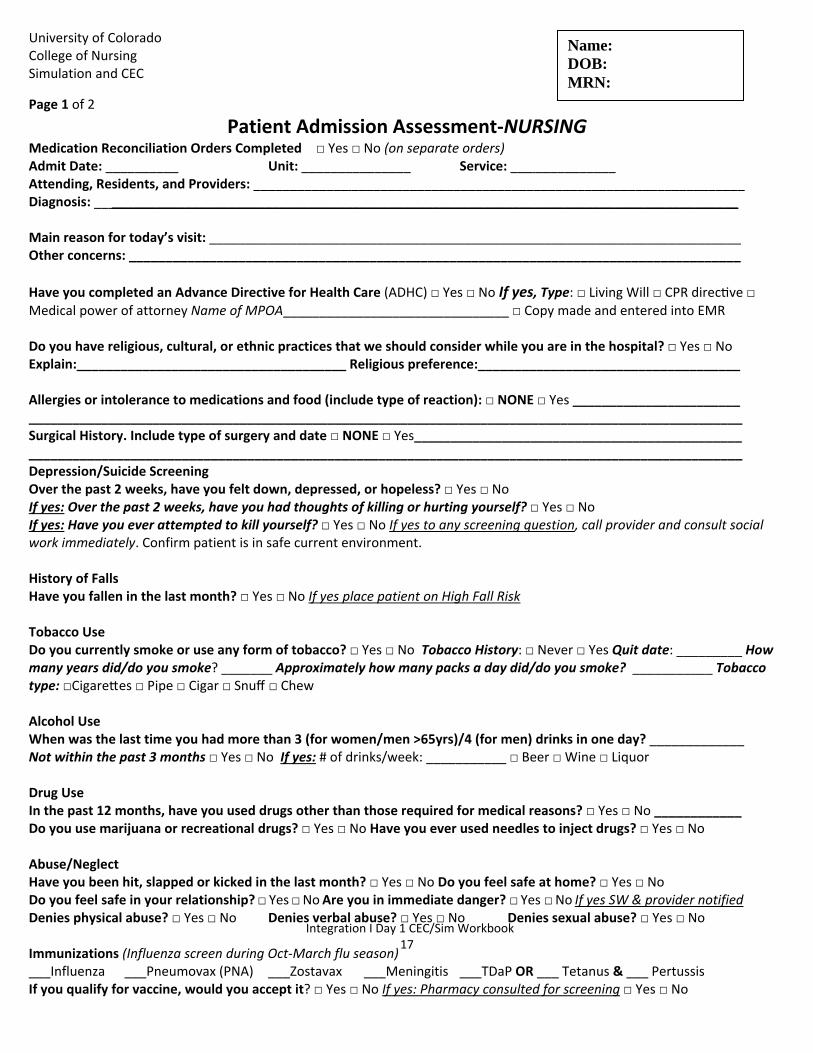
University of Colorado College of Nursing Simulation and CEC
Page 1 of 2
Patient Admission Assessment‐NURSING Medication Reconciliation Orders Completed □ Yes □ No (on separate orders) Admit Date: __________ Unit: _______________ Service: ___ ___________ Attending, Residents, and Providers: _____________ ______________________________________________________ Diagnosis: __ ______________________________________________________________________________________ Main reason for today’s visit: _________________________________________________________________________ Other concerns: ____________________________________________________________________________________
Have you completed an Advance Directive for Health Care (ADHC) □ Yes □ No If yes, Type: □ Living Will □ CPR direc ve □ Medical power of attorney Name of MPOA_______________________________ □ Copy made and entered into EMR Do you have religious, cultural, or ethnic practices that we should consider while you are in the hospital? □ Yes □ No Explain:_____________________________________ Religious preference:____________________________________ Allergies or intolerance to medications and food (include type of reaction): □ NONE □ Yes _______________________ __________________________________________________________________________________________________ Surgical History. Include type of surgery and date □ NONE □ Yes_____________________________________________ __________________________________________________________________________________________________ Depression/Suicide Screening Over the past 2 weeks, have you felt down, depressed, or hopeless? □ Yes □ No If yes: Over the past 2 weeks, have you had thoughts of killing or hurting yourself? □ Yes □ No If yes: Have you ever attempted to kill yourself? □ Yes □ No If yes to any screening question, call provider and consult social work immediately. Confirm patient is in safe current environment. History of Falls Have you fallen in the last month? □ Yes □ No If yes place patient on High Fall Risk Tobacco Use Do you currently smoke or use any form of tobacco? □ Yes □ No Tobacco History: □ Never □ Yes Quit date: _________ How many years did/do you smoke? _______ Approximately how many packs a day did/do you smoke? ___________ Tobacco type: □Cigare es □ Pipe □ Cigar □ Snuff □ Chew Alcohol Use When was the last time you had more than 3 (for women/men >65yrs)/4 (for men) drinks in one day? _____________ Not within the past 3 months □ Yes □ No If yes: # of drinks/week: ___________ □ Beer □ Wine □ Liquor Drug Use In the past 12 months, have you used drugs other than those required for medical reasons? □ Yes □ No ____________ Do you use marijuana or recreational drugs? □ Yes □ No Have you ever used needles to inject drugs? □ Yes □ No Abuse/Neglect Have you been hit, slapped or kicked in the last month? □ Yes □ No Do you feel safe at home? □ Yes □ No Do you feel safe in your relationship? □ Yes □ No Are you in immediate danger? □ Yes □ No If yes SW & provider notified Denies physical abuse? □ Yes □ No Denies verbal abuse? □ Yes □ No Denies sexual abuse? □ Yes □ No Immunizations (Influenza screen during Oct‐March flu season) ___Influenza ___Pneumovax (PNA) ___Zostavax ___Meningitis ___TDaP OR ___ Tetanus & ___ Pertussis If you qualify for vaccine, would you accept it? □ Yes □ No If yes: Pharmacy consulted for screening □ Yes □ No
Name: DOB: MRN:
Integration I Day 1 CEC/Sim Workbook 18
University of Colorado College of Nursing Simulation and CEC
Page 2 of 2
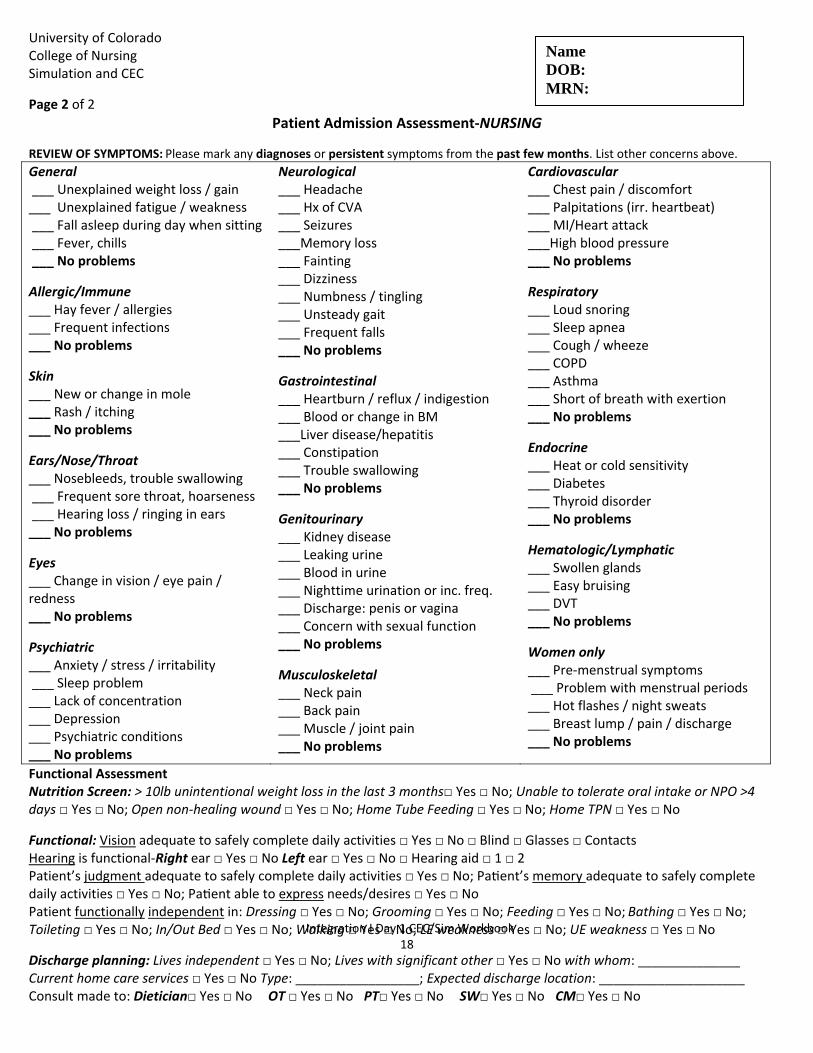
Patient Admission Assessment‐NURSING
REVIEW OF SYMPTOMS: Please mark any diagnoses or persistent symptoms from the past few months. List other concerns above.
General ___ Unexplained weight loss / gain ___ Unexplained fatigue / weakness ___ Fall asleep during day when sitting ___ Fever, chills ___ No problems
Allergic/Immune ___ Hay fever / allergies ___ Frequent infections ___ No problems
Skin ___ New or change in mole ___ Rash / itching ___ No problems
Ears/Nose/Throat ___ Nosebleeds, trouble swallowing ___ Frequent sore throat, hoarseness ___ Hearing loss / ringing in ears ___ No problems
Eyes ___ Change in vision / eye pain / redness ___ No problems
Psychiatric ___ Anxiety / stress / irritability ___ Sleep problem ___ Lack of concentration ___ Depression ___ Psychiatric conditions ___ No problems
Neurological ___ Headache ___ Hx of CVA ___ Seizures ___Memory loss ___ Fainting ___ Dizziness ___ Numbness / tingling ___ Unsteady gait ___ Frequent falls ___ No problems
Gastrointestinal ___ Heartburn / reflux / indigestion ___ Blood or change in BM ___Liver disease/hepatitis ___ Constipation ___ Trouble swallowing ___ No problems
Genitourinary ___ Kidney disease ___ Leaking urine ___ Blood in urine ___ Nighttime urination or inc. freq. ___ Discharge: penis or vagina ___ Concern with sexual function ___ No problems
Musculoskeletal ___ Neck pain ___ Back pain ___ Muscle / joint pain ___ No problems
Cardiovascular ___ Chest pain / discomfort ___ Palpitations (irr. heartbeat) ___ MI/Heart attack ___High blood pressure ___ No problems
Respiratory ___ Loud snoring ___ Sleep apnea ___ Cough / wheeze ___ COPD ___ Asthma ___ Short of breath with exertion ___ No problems
Endocrine ___ Heat or cold sensitivity ___ Diabetes ___ Thyroid disorder ___ No problems
Hematologic/Lymphatic ___ Swollen glands ___ Easy bruising ___ DVT ___ No problems
Women only ___ Pre‐menstrual symptoms ___ Problem with menstrual periods ___ Hot flashes / night sweats ___ Breast lump / pain / discharge ___ No problems
Functional Assessment Nutrition Screen: > 10lb unintentional weight loss in the last 3 months□ Yes □ No; Unable to tolerate oral intake or NPO >4 days □ Yes □ No; Open non‐healing wound □ Yes □ No; Home Tube Feeding □ Yes □ No; Home TPN □ Yes □ No
Functional: Vision adequate to safely complete daily activities □ Yes □ No □ Blind □ Glasses □ Contacts Hearing is functional‐Right ear □ Yes □ No Left ear □ Yes □ No □ Hearing aid □ 1 □ 2 Patient’s judgment adequate to safely complete daily activities □ Yes □ No; Pa ent’s memory adequate to safely complete daily activities □ Yes □ No; Pa ent able to express needs/desires □ Yes □ No Patient functionally independent in: Dressing □ Yes □ No; Grooming □ Yes □ No; Feeding □ Yes □ No; Bathing □ Yes □ No; Toileting □ Yes □ No; In/Out Bed □ Yes □ No; Walking □ Yes □ No; LE weakness □ Yes □ No; UE weakness □ Yes □ No
Discharge planning: Lives independent □ Yes □ No; Lives with significant other □ Yes □ No with whom: ______________ Current home care services □ Yes □ No Type: _________________; Expected discharge location: ____________________ Consult made to: Dietician□ Yes □ No OT □ Yes □ No PT□ Yes □ No SW□ Yes □ No CM□ Yes □ No
Name DOB: MRN:
Integration I Day 1 CEC/Sim Workbook 19
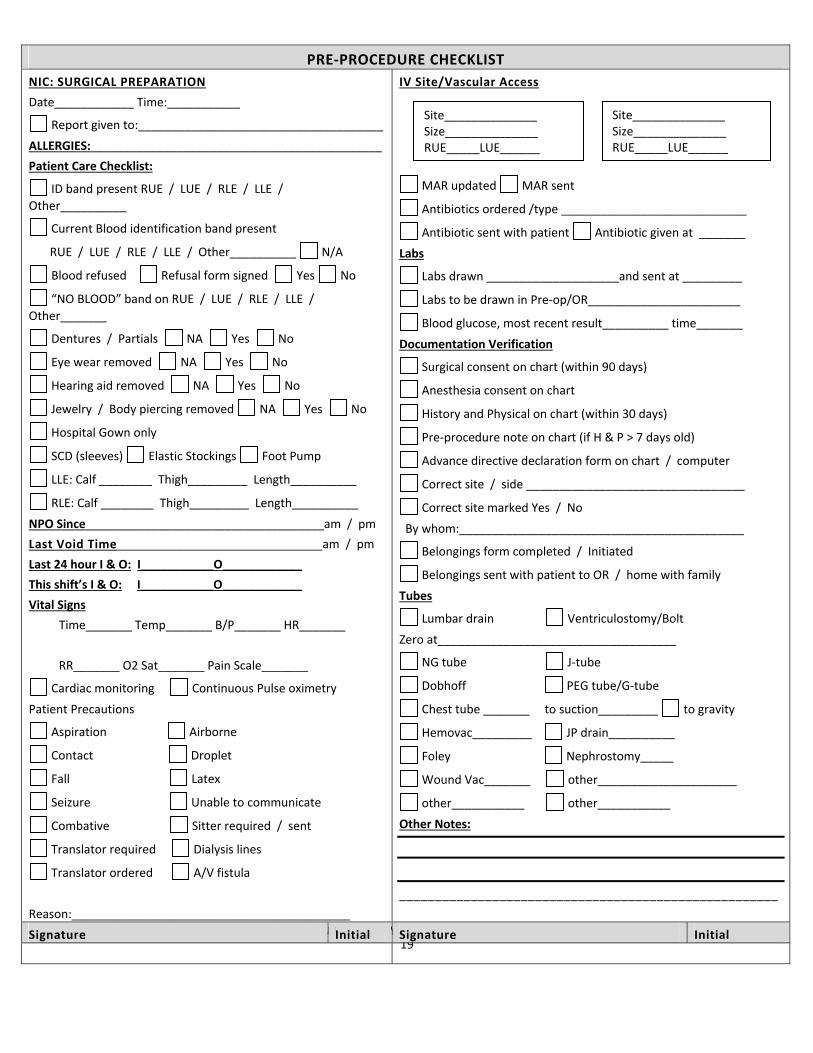
PRE‐PROCEDURE CHECKLIST
NIC: SURGICAL PREPARATION
Date____________ Time:___________
Report given to:_____________________________________
ALLERGIES:____________________________________________
Patient Care Checklist:
ID band present RUE / LUE / RLE / LLE /
Other__________
Current Blood identification band present
RUE / LUE / RLE / LLE / Other__________ N/A
Blood refused Refusal form signed Yes No
“NO BLOOD” band on RUE / LUE / RLE / LLE /
Other_______
Dentures / Partials NA Yes No
Eye wear removed NA Yes No
Hearing aid removed NA Yes No
Jewelry / Body piercing removed NA Yes No
Hospital Gown only
SCD (sleeves) Elastic Stockings Foot Pump
LLE: Calf ________ Thigh_________ Length__________
RLE: Calf ________ Thigh_________ Length__________
NPO Since____________________________________am / pm
Last Void Time_______________________________am / pm
Last 24 hour I & O: I___________O____________
This shift’s I & O: I___________O____________
Vital Signs
Time_______ Temp_______ B/P_______ HR_______
RR_______ O2 Sat_______ Pain Scale_______
Cardiac monitoring Continuous Pulse oximetry
Patient Precautions
Aspiration Airborne
Contact Droplet
Fall Latex
Seizure Unable to communicate
Combative Sitter required / sent
Translator required Dialysis lines
Translator ordered A/V fistula
Reason:__________________________________________
IV Site/Vascular Access
MAR updated MAR sent
Antibiotics ordered /type ____________________________
Antibiotic sent with patient Antibiotic given at _______
Labs
Labs drawn ____________________and sent at _________
Labs to be drawn in Pre‐op/OR_______________________
Blood glucose, most recent result__________ time_______
Documentation Verification
Surgical consent on chart (within 90 days)
Anesthesia consent on chart
History and Physical on chart (within 30 days)
Pre‐procedure note on chart (if H & P > 7 days old)
Advance directive declaration form on chart / computer
Correct site / side _________________________________
Correct site marked Yes / No
By whom:___________________________________________
Belongings form completed / Initiated
Belongings sent with patient to OR / home with family
Tubes
Lumbar drain Ventriculostomy/Bolt
Zero at____________________________________
NG tube J‐tube
Dobhoff PEG tube/G‐tube
Chest tube _______ to suction_________ to gravity
Hemovac_________ JP drain__________
Foley Nephrostomy_____
Wound Vac_______ other_____________________
other___________ other___________
Other Notes:
_____________________________________________________
Signature Initial Signature Initial
Site______________Size______________ RUE_____LUE______
Site______________Size______________ RUE_____LUE______





























