Embed Size (px)
Citation preview

I Clin Pathol 1995;48:519-524
Circulating endothelin- 1 concentrations inpatients with chronic hypoxia
C Ferri, C Bellini, C De Angelis, L De Siati, A Perrone, G Properzi, A Santucci
Institute of ClinicalMedicine,Andrea CesalpinoFoundation,"La Sapienza"University,Rome, ItalyC FerriC BelliniL De SiatiA Perrone
D.A.S.R.S. AerospaceMedical Department,Pratica di Mare,Rome, ItalyC De Angelis
Department ofInternal Medicine,University of L'Aquila,L'Aquila, ItalyG ProperziA Santucci
Correspondence to:Dr C Ferri, Instituto diI Clinica Medica,Fondazione AndreaCesalpino, Universita"La Sapienza",Viale del Policlinico,155, 00161 Rome, Italy.Accepted for publication25 August 1994
AbstractAims-To evaluate thebehaviour ofplasmaendothelin-1 in patients with chronic hy-poxia.Methods-Fifteen male patients (meanage 52-1 + 3-1 years) with mild chronic ob-structive pulmonary disease (COPD) werestudied. Twelve healthy men (mean age48 3 +554 years) served as controls. Bothpatients and controls underwent standardpulmonary function tests, echocardio-graphic evaluation, and arterial blood gasevaluation. Blood samples for endothelin-lassay were taken from a previouslyincannulated antecubital vein after 60minutes of rest in the supine position.Endothelin-1 was measured by radio-inmmunoassay after extraction fromplasma.Results-Patients with chronic hypoxiahad lower PaO2 values (66.1+6-2mmHg)than controls (83.8 + 207 mmHg) butPaCO2 values were similar (38-1+2-5 v36-7+3-1mmHg, respectively). Arterialpulmonary pressure, therefore, was higherin patients (18.1_3.7mmHg) than incontrols (10.4 + 2*7 mmHg) as were cir-culating endothelin-I concentrations(1*22±0-36 v 0 57+0-1pgiml). Further-more, plasma endothelin-l concentrationswere negatively correlated with PaO2 anddirectly correlated with pulmonary pres-sure levels. No significant correlationswere found in controls.Conclusions-These results show a clearrelation between chronic hypoxia and cir-culating endothelin-I concentrations.Therefore, chronic hypoxia may be re-garded as an important stimulus for en-dothelin-1 release and as one of the maincontributors to increased vasoconstrictionin the vascular pulmonary bed which oftenaccompanies lung disease.(JT Clin Pathol 1995;48:519-524)
Keywords: Endothelin-1, hypoxia, respiratory disease,pulmonary hypertension.
Endothelin-1 is a recently discovered peptidecomposed of 21 amino acids and released byendothelial cells.'2 Human endothelin-I is de-rived from preproendothelin-1, a 212 aminoacid peptide, via a 38 amino acid intermediateknown as big endothelin-1. The expression ofpreproendothelin-1 messenger RNA (mRNA)is stimulated by vasopressor hormones such asepinephrine, angiotensin II and arginine vaso-pressin,3 substances generated from activated/aggregating platelets such as transforming
growth factor P,B coagulation products such asthrombin,4 cytokines such as interleukin-1,5and shear stress.6 Furthermore, substancessuch as nitric oxide,7 prostacyclin,7 atrial na-triuretic peptide,8 and an unknown vascularsmooth muscle cell derived inhibitory factor9act as inhibitors of endothelin-1 productionor secretion, or both. Because of its vaso-constrictive and mitogenic properties, en-dothelin-1 affects cardiovascular, pulmonaryand renal function,' 310 and may be involved inthe development of several diseases, such asatherosclerosis,2 myocardial infarction," renaldisease,310 and systemic3 and pulmonary hy-pertension. 12With regard to the possible interactions be-
tween endothelin-1 and pulmonary functions,hypoxia stimulates the release of endothelin-1from rat resistance vessels.'3 In cultured cellsderived from human umbilical cord veins Kou-rembanas et al14 demonstrated that hypoxiainduced upregulation of endothelin-1 genetranscription results in a four- to eightfold in-crease in endothelin-1 secretion. Moreover, arecent interesting study conducted in healthymen indicated that hypobaric hypoxia inducedby trekking from 1200 m to 5000 m over eightdays caused an increase in circulating en-dothelin-1 concentrations which was inverselycorrelated with oxygen saturation.'5 Severalother factors could have influenced the be-haviour of plasma endothelin-1 in these sub-jects, including the haemodynamic andhormonal changes which usually occur fol-lowing altitude acclimatisation.'6 Moreover,oxygen tension in the blood was indirectly eval-uated as saturated haemoglobin, by per-cutaneous oxymetry, the measurement ofwhich is strongly affected by cutaneous vaso-constriction caused by total body cooling.However, the report by Giussani et al'5 clearlysuggests that hypoxia may affect plasma en-dothelin-1 concentrations. In this context, sev-eral studies reported a close correlationbetween circulating endothelin-I and arterialpulmonary pressure.3712 Therefore, we pos-tulated that a pathological condition associatedwith chronic hypoxia could be used to evaluatethe influence of blood oxygen concentrationson plasma endothelin-1 concentrations, and toverify whether or not the behaviour of thispeptide is related to both PaO2 and pulmonarypressure levels. To test this hypothesis, westudied male patients with chronic obstructivepulmonary disease (COPD), but withoutclinical, ultrasound, or biochemical evidenceof atherosclerosis, metabolic abnormalities oflipid or carbohydrate metabolism, or renalfunction abnormalities.
519
on January 26, 2020 by guest. Protected by copyright.
http://jcp.bmj.com
/J C
lin Pathol: first published as 10.1136/jcp.48.6.519 on 1 June 1995. D
ownloaded from

Ferm, Bellini, de Angelis, De Siati, Perrone, Properzi, et al
MethodsThe study was approved by the Ethics Com-mittee of the Andrea Cesalpino Foundation.All the participants gave their informed consenton entry. As several factors related to the men-strual cycle and/or menopause influence thebehaviour of several hormones which regulateendothelial function,'7 we decided to studymale patients only.Twenty five white men (mean age 53 9 + 3-8
years) with mild COPD were initially enrolledin the study. The diagnosis ofCOPD was basedon a past history of chronic bronchitis andevidence of air flow abnormalities on standardpulmonary function tests (forced expiratoryvolume in one second (FEVI) <80% predictedvalues, FEV,/vital capacity <80% normal val-ues). All were outpatients aged between 40and 60 years; had not been taking cardiacglycosides, diuretics, steroids, or theophyllinein the three months before the study; did notsmoke or drink; and had a body mass indexbetween 19 and 25 kg/m2; supine systolic anddiastolic blood pressures below 140 and90 mmHg, respectively; a serum creatinineconcentration <100 mol/l; a serum sodiumconcentration > 135 mmol/l; microalbuminuria<20 jg/minute; absence of proteinuria; normalglucose metabolism (that is, fasting glucoseconcentrations <6-0 mmol/l and a normalplasma glucose and insulin response to the oralglucose tolerance test (75 g)); serum cholesterolconcentrations between 3-7 and 5 1 mmol/l;and serum triglyceride concentrations between1P 1 and 1 6 mmol/l. Clinical and echo-Dopplerevaluation of the neck and limb vessels ex-cluded the presence of atherosclerotic lesions.Moreover, none of the patients had cardiac,hepatic or adrenal disease, or had significantperipheral oedema as assessed by clinical, ultra-sound and laboratory tests. In particular, ab-sence of cor pulmonale and left ventriculardysfunction was documented on clinical ex-amination and by electrocardiography andechocardiography. Both patients and controlsunderwent echocardiographic examinationpermitting evaluation of the main mor-phological and functional parameters, such aspulmonary pressure, left ventricular ejectionfraction and ventricular kinesis. In particular,two patients with a left ventricular ejectionfraction lower than 50% and five patients inwhom it was technically impossible to obtain areliable echo-Doppler evaluation ofpulmonaryarterial pressure were excluded from the study.The remaining cohort (18 patients, mean
age 51-7 + 4-5 years) underwent standard pul-monary function tests and analysis of arterialblood gas values. All patients had a PaCO2<40 mmHg, whereas PaO2 values ranged from55 to 75 mmHg. Twelve healthy men (meanage 48-3 + 5-4 years) served as controls. Entrycriteria were identical with those for thepatients.
After recruitment, to establish standard con-ditions, both patients and controls were placedon a normocaloric diet (about 1 g/kg protein,2 g/kg carbohydrates, 0 7 g/kg fat) for twoweeks with fixed sodium and potassium intake(120 mmol sodium and 60 mmol potassium
daily). Sodium was given as sodium chloride.Compliance with restrictions on sodium intakewas assessed by measuring 24 hour urinary so-dium and chloride excretion on the last threeconsecutive days of each week. Patients andcontrols with Na+ urinary excretion <80 or> 130 mmol/24 hours were excluded. Duringthis phase, three further patients were excludedfrom the study (all of them had a urinarysodium excretion >140mmol/24 hours). Theremaining cohort of 15 patients (mean age52 1 + 3-1 years) and 12 normal subjects con-stituted the study population. Patients wereadvised to stop using oral and/or inhaled bron-chodilators for the 12 hours before the study.Participants came to the outpatient departmentat 0800 hours and assumed the supine positionin an air conditioned room (22-24°C). Anantecubital vein was incannulated with a tefloncatheter (Viggo-Spectramed, Helsingborg,Sweden) which was kept pervious by saline(09% NaCl at a rate of 10ml/hour). After60 minutes of rest, during which blood pressureand heart rate were constantly recorded at 10minute intervals by an automatic sphygmo-manometer (Nippon Colin, Komaki, Japan),venous blood samples for determination of os-molality and plasma endothelin-1, serum elec-trolyte and creatinine concentrations weretaken from the pervious prepared antecubitalvein. This particular procedure was chosen toavoid the influence of venepuncture and bloodstasis'8 on the release of endothelin-1 fromvenous endothelial cells. Immediately after ven-ous blood sampling, arterial blood samples forevaluation of blood gas levels were drawn froma brachial artery. For correlations between cir-culating endothelin-1 and urinary Na+, K+ andcreatinine excretion, the last 24 hour collectionof each patient was used.
BIOCHEMICAL TESTSBlood samples for the plasma endothelin-1assay were collected into pre-chilled tubes(Becton Dickinson Vacutainer Systems, NewJersey, NJ, USA) containing EDTA-K3 (15%)and aprotinin (500 KIU/ml blood) andpromptly centrifuged at 1600 x g at 0-40C for15 minutes. Plasma was pipetted into poly-propylene tubes and stored at - 80°C untilassayed (mean five days, range one to 10days). Plasma endothelin- 1 was concentratedby extraction through C 18 Sep-Pak cartridges(Millipore Corporation, Marlborough, Mas-sachusetts, USA). Sep-Pak columns wereactivated with 0-1% trifluoroacetic acidbuffer, loaded with 2 ml plasma and thenwashed with 0 1% trifluoroacetic acid buffer.The retained material was eluted with 3 ml ofa buffer containing acetonitril (60%) in 0-1%trifluoroacetic acid, and dried in a vacuumby a centrifugal evaporator system (Gyrovap,Howe & Co., London UK). A commercialradioimmunoassay kit (Peninsula Laboratories,Belmont, CA, USA) was used to measure en-dothelin-1 concentrations in the reconstitutedpellet. Cross-reactivity of the system for en-dothelin-1 is 100%, but is less than 7% forboth endothelin-2 and endothelin-3 according
520
on January 26, 2020 by guest. Protected by copyright.
http://jcp.bmj.com
/J C
lin Pathol: first published as 10.1136/jcp.48.6.519 on 1 June 1995. D
ownloaded from

Oxygen and plasmaendothelin-5
to the manufacturer. Intra- and interassay co-efficients of variation in our laboratory were<10%. Recovery was 80%. Serum and urinaryelectrolytes were measured by standard laborat-ory methods using a flame photometer (Bio-technica Instruments, Rome, Italy). Plasmaosmolality was determined as freezing pointdepression by an osmometer (Fiske 2400Multi-sample Osmometer, Fiske Associates,Needham Heights, Massachusetts, USA).
BLOOD GAS EXCHANGE MEASUREMENTSArterial blood was collected in heparinised syr-inges from a brachial artery. Gas evaluationswere performed by a standard laboratory bloodgas analyser (ABL 510 Radiometer, Copen-hagen, Denmark).
BLOOD PRESSURE AND ECHOCARDIOGRAPHICEVALUATIONSSystemic arterial blood pressure and heart ratewere measured at 10 minute intervals usingan automatic sphygmomanometer (NipponColin). Mean blood pressure (MBP; mmHg)was evaluated using the formula:
MBP =DBP + (SBP-DBP)
where DBP is the diastolic and SBP the systolicblood pressure.
Echocardiographic studies were performedusing commercially available equipment with
Table 1 General characteristics (mean+ SD) of the study population
Patients ControlsVariable (n= 15) (n= 12)
Age (years) 52-1+ 3-1 48-3 _5-4Disease duration (years) 4-2+ 0-2Body mass index (kg/m2) 24-1+ 0 4 22-8 03SBP (mmHg) 127-3+ 3-1 122-9+4-5DBP (mmHg) 80-1+ 2-6 78-8+2-1MBP (mmHg) 95-8+ 3 0 935±+2-9Heart rate (beats/minute) 75-1+ 1-5 71-2+0-9Serum creatinine (pLmoIl) 81-0+10-1 80-5+9-3Creatinine clearance (ml/s) 1-6+ 0 5 1-7+0 3Blood urea (mmol/1) 10-9+ 09 11-3+1-0Serum Na+ (mmol/l) 138-4+ 3-2 139-1+3-4Serum K+ (mmol/1) 4-2+ 04 4-5+0-2Plasma fasting glucose (mmol/l) 5-1 + 0-6 4-6+0 3Plasma fasting insulin (pmol/l) 93 4+ 8-1 78-6+9-1Plasma osmolality (mmol/kg) 286-3 + 3-2 285-8+2-9Serum cholesterol (mmol/1) 4-4 + 0-2 4-2 +0-2Serum triglycerides (mmol/l) 1-5+ 0-1 1-3±0-2
SBP, systolic blood pressure; DBP, diastolic blood pressure.
Table 2 Respiratory and cardiac parameters of the study population
Patients ControlsVariable (n= 15) (n= 12)
Forced vital capacity (litre) 2-8 + 1-5 3 7 + 2-1FEV, (I/one second) 1-9 + 0-2 3-1 + 0 5***FEVI/forced vital capacity (%) 67-8 + 3-4 84-1 + 3-7tPaO2 (mmHg) 66-1 + 6-2 83-8 + 2-7tPaCO2 (mmHg) 38-1 ± 2-5 36-7 ± 3-1Arterial pH 7-37+ 0-01 7-38+ 0-001Serum bicarbonates (mmol/l) 25-1 + 2-1 24-3 + 1-8Respiratory rate (breaths/minute) 16-1 + 1-5 14-3 + 1-1Haematocrit (%) 46-1 + 1-5 45-8 ± 1-6Haemoglobin (g/l) 131-3 +10-2 145-2 +15-1Oxygen saturation (% saturated haemoglobin) 88-5 + 4-4 91-3 + 3-8Pulmonary pressure (mmHg) 18-1 + 3-7 10-4 + 2-7***Left ventricular ejection fraction (%) 65-6 ± 8-9 74-8 + 7-8**
FEV,, forced expiratory volume in one second.** p<0-01 v patients with COPD; *** p<0-001 v patients with COPD; t p<0-0005 v patientswith COPD.
left parastemal and apical approaches. Bothpatients and controls underwent a complete Mmode and B mode evaluation. Functioning ofall cardiac valves was also investigated by colourDoppler. Conventionally, blood flow directedtowards the transducer was codified in red andthat directed away from the transducer in blue;a green colour (variance) represented turbulentflow. Tricuspid regurgitation was carefullydetected: the transducer was manipulated toobtain the best visualisation of valvularinsufficiency by colour-flow Doppler mappingand a continuous wave Doppler cursor waspositioned parallel to the flow. If the angle ofintersection between the Doppler cursor andtricuspid regurgitant flow was >200, attemptsto detect tricuspid insufficiency were repeatedfrom the subcostal transducer position. In somecases the subjects were asked to take a deepbreath and to remain in inspiratory apnea: inthis way, it was usually possible to obtain anoptimal representation of tricuspid regurgitantflow and to place the Doppler cursor in positionparallel to it. The same manoeuvres were thenrepeated using the non-imaging, high-sensi-tivity Pedoff transducer. In our experience, thelatter transducer provides an opportunity todetect more defined Doppler envelopes andhigher velocities than with combined imagingand the continuous wave Doppler probe. Themaximum velocity of the signal tracing ob-served on at least two consecutive cardiac cycleswas used to calculate the pressure gradient.Optimal signals were assumed to be orientatedparallel to the direction of regurgitation andthus a flow angle correction for velocity wasnot used. The transtricuspid systolic pressuregradient (TSPG; in mmHg) was calculated onthe basis of the modified Bernoulli equation"9:
TSPG=4V2
where V represents the peak systolic velocityof the right ventricle to right atrium signal.
STATISTICAL ANALYSISAll data are presented as means + SD. Datawere recorded using a personal computer(Olivetti, Ivrea, Italy) and a database program(IBM Assistant, IBM Corporation, Armonk,New York, USA). Statistical analysis was per-formed using statistical software for biomedicalscience (Primer of Biostatistics, McGraw-Hill,New York, NY, USA). Baseline comparisonamong groups was performed using the Stu-dent's t test and analysis of variance; linearregression and correlation were used to evaluatecorrelation between two variables; p<0Q05 wasconsidered significant.
ResultsPATIENTSThe general characteristics of the patients withCOPD are given in table 1. As shown, the mainbiochemical parameters confirmed normalglucose and lipid metabolism and there wasno evidence of abnormal renal function orof electrolyte disorders. Regarding respiratoryparameters (table 2), patients with COPD were
521
on January 26, 2020 by guest. Protected by copyright.
http://jcp.bmj.com
/J C
lin Pathol: first published as 10.1136/jcp.48.6.519 on 1 June 1995. D
ownloaded from

Feni, Bellini, de Angelis, De Siati, Perrone, Properzi, et al
2-2 r
2.0 H
1.8 H
1.6
0.a
I-
EcnCu
1.4 _
1.2 k
1.0 _
0
0
0
0
0
0
00
0.8 _-
0-6 _
* .
* .
* *U
0
0-4 K
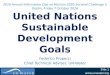
p<0-001Figure 1 Scatterplots showing plasma endothelin-1 (ET-1) concentrations in a group of hypoxaemic patients withCOPD (n= 15; El) and in a group of healthy subjects(n= 12; N). Horizontal lines indicate the mean values;Vertical lines indicate the standard deviations.
characterised by reduced forced vital capacity(2-8 +1-5 litres) and FEV, (1 -9 + 0-2 1/one sec-ond). PaO2 values were within the normal range(38-1 ± 2-5 mmHg). Arterial oxygen saturation
ECD
I-
Eam0-Cl)
2-2
2-0
1 -8
1 -6
1 -4
1-2
1-0 _
0-8 H
0-6
0-4
O CP/1
A0
0
was 88-5 + 4A4% saturated haemoglobin. Echo-cardiographic evaluation did not show any seg-mental or global alterations in cardiac kinesis.Arterial pulmonary pressure was at the higherend of the normal range (18-1 +3-7 mmHg),the normal value at our echocardiography unit,as evaluated in 384 aged matched healthysubjects, being 10-8+3-1 mmHg (range8-24 mmHg). The left ventricular ejection frac-tion was slightly reduced (65-6+8-9%), al-though it was greater than 50% in all patients.The mean circulating endothelin-1 con-centration was 1-22+ 0-36 pg/ml (fig 1). A neg-ative correlation was found between plasmaendothelin-1 concentrations and PaO2 (r=-0-614; p<002) (fig 2A). However, plasmaendothelin- 1 concentrations directly correlatedwith the degree of arterial pulmonary pressure(r=0-571; p<0-03) (fig 2B). It was also in-teresting to note that pulmonary pressure neg-atively correlated with PaO2 values (r=-0-073; p<0-003). No other correlations werefound. In particular, circulating endothelin-1concentrations did not correlate with bloodpressure, plasma glucose, or fasting insulin andlipid concentrations.
CONTROLSThe controls had normal values for glucoseand lipid metabolism, and renal function (table1). Cardiac and respiratory parameters (table2) were also normal. In particular, the controlshad normal arterial gas values (PaO2=83-8 + 2-7 mmHg; PaCO2 = 36-7 + 3-1 mmHg)and oxygen saturation (91-3+3-8% saturatedhaemoglobin). Plasma endothelin-1 con-centrations were 0-57+0-10pg/ml (fig 1) anddid not correlate with PaO2. Arterial pulmonarypressure was 10-4 +2-7mmHg and did notcorrelate with either circulating endothelin- 1concentrations or PaO2. Plasma endothelin-1concentrations also did not correlate with theother parameters evaluated, such as plasmaglucose and insulin concentrations.
COMPARISON BETWEEN GROUPSWhen intergroup comparisons were performed,some significant differences were noted. Cir-
2-2FB2-0 H
1-8 H
00
0o o
0
0
r =--614p<0.02
50 55
I-
w
ECl)Cu
0
0
60 65 70 75 85
00
r = 0-571p<0.03
1-4
1.2
1-0_
0.8-
0.6-
0.4-
5
rF
00
000
0
0
0
i 10 15 20 25
Pulmonary pressure (mmHg)
Figure 2 In patients with COPD (n= 15) plasma endothelin-1 (ET-1) concentrations were negatively correlated with(A) arterial PaO2 but were direcdy correlated with (B) arterial pulmonary pressure.
PaO2 (mmHg)
t-
522
1-6 _
on January 26, 2020 by guest. Protected by copyright.
http://jcp.bmj.com
/J C
lin Pathol: first published as 10.1136/jcp.48.6.519 on 1 June 1995. D
ownloaded from

Oxygen and plasma endothelin-1
culating endothelin-1 concentrations were sig-nificantly higher in patients with COPD thanin controls (p<0-001) (fig 1), with very littleoverlap between the two groups. Indeed, inpatients with COPD plasma endothelin-1 con-centrations ranged from 0 54 to 2 10pg/ml,whereas in controls these ranged from 0-42 to0-72 pg/ml (fig 1). As a consequence, only twopatients had plasma endothelin-1 con-centrations within the normal range, whereasthe remaining 13 had endothelin-1 con-centrations two- to fourfold higher than thosein controls.As expected, both FEV, and FEV1/vital cap-
acity were lower in the patients than controls(p<0001 and p<00005, respectively) (table 2),as was PaO2 (p<0 0005). Systolic, diastolic, andmean blood pressure values were similar in bothgroups (table 1); however, mean arterial pul-monary pressure was significantly higher inpatients than in controls (p<00001), but re-mained within the normal range in both groups.The left ventricular ejection fraction, however,was higher in controls (p<0-01) (table 2).
DiscussionEndothelins are potent vasoconstrictors andmitogens for both vascular smooth musclecells'310 and fibroblasts.20 Increased secretionof endothelin- 1 from the vascular endotheliumhas frequently been implicated in systemichypertension,3 atherosclerosis,2 myocardial in-farction,"1 renal disease,"3 0 and pulmonary hy-pertension. 1Hypoxia causes both systemic and pul-
monary arteries to constrict,2' but the mech-anism involved has not been elucidated as yet.However, based on their location, endothelialcells ofthe vascular pulmonary bed are thoughtto play a key role. In keeping with thishypothesis, changes in blood oxygen tensioninduce endothelial cells to release a numberof different vasoactive agents includingendothelin-1," platelet derived growthfactor,22 nitric oxide2' and other unknown sub-stances,24 which can modify the contractile andproliferative state of the underlying smoothmuscle cells.
All of the above data were obtained in acuteconditions, and the aim of this study was toverify how long term low PaO2 values couldaffect circulating endothelin-1 concentrations.Thus, we selected a group ofpatients with mildCOPD and to exclude confounding factorscaused by advanced disease, the patientschosen were highly selected. Disease durationwas less than five years in all cases and clinicaland biochemical tests allowed us to excludepatients with signs ofcor pulmonale, peripheraloedema, electrolyte disorders, or acid/base al-terations. All patients were hypoxemic but hadnormal PaCO2 values. Furthermore, the studywas conducted on lean normotensive subjectswith no clinical or echo-Doppler signs ofatherosclerosis, with normal blood pressure val-ues, and normal carbohydrate and lipid meta-bolism.Our results demonstrate that circulating en-
dothelin- 1 concentrations were significantly in-
creased in hypoxemic patients compared withhealthy subjects (p<0-001). Moreover, en-dothelin-1 concentrations were negatively cor-related with PaO2 and directly correlated witharterial pulmonary pressure. The latter washigher (p<0-001) in hypoxemic patients thanin the control subjects, being directly correlatedwith PaO2 in the former only.Our results concur with previous findings in
the rat,25 of increased synthesis of endothelin-1in response to hypoxia. The intracellular path-way by which hypoxia modulates endothelin-1synthesis in vascular endothelial cells is notknown, but previous findings in culturedhuman endothelial cells suggested that oxygenmay act at the nuclear level by increasingpreproendothelin-1 gene expression and con-sequently preproendothelin-1 mRNA produc-tion.'4 Action at the post-transcriptional levelis unlikely as endothelin-1 release requires denovo protein synthesis.'"0Our study extends the data reported by Giu-
ssani et all5 showing that chronic hypoxia is amajor determinant of circulating endothelin-1concentrations in patients with respiratory fail-ure, and suggesting that it may be an importantregulator of the vascular tone in the pulmonarycirculation.
In this regard, hypoxia is already regardedas a possible pathogenic factor in the de-velopment of pulmonary hypertension,26 butthe possible role of hypoxia mediated en-dothelin-1 release has never been investigated.However, Adnot et al23 have recently dem-onstrated that endothelin-1 induces greaterpulmonary vasoconstriction in rats with chronichypoxia compared with control rats. Moreover,Giaid et a!27 reported elevated endothelin-1gene expression in vascular endothelial cellsderived from the lungs of patients with bothprimary and secondary forms of pulmonaryhypertension. In keeping with these data, weshowed that pulmonary pressure values weresignificantly correlated with plasma endothelin-1concentrations, suggesting that the peptide mayact as a potent vasoconstrictor for the lungvascular bed, at least in conditions associatedwith a significant increase in its circulatingconcentrations. In agreement with this in-terpretation, De Nucci et al7 have already dem-onstrated the high avidity of the pulmonaryvasculature for circulating endothelin-1, andboth endothelial and vascular smooth musclecells receptors28 have been demonstrated in thelung. In contrast to this hypothesis, Deleuze etal29 showed that endothelin-1 induced dosedependent vasodilation in the pulmonary cir-culation of calves breathing in hypoxic con-ditions. In particular, low doses ofendothelin-1induced a mild decrease in the pulmonaryartery pressure, whereas high doses causedpulmonary vasodilation and systemic vaso-constriction. Thus, the action of endothelin-1may differ in pulmonary and systemic cir-culations, refuting the suggested pathogenicrole for endothelin-1 in the development ofpulmonary hypertension. Nevertheless, thedata from Deleuze et al29 may simply reflectthe different pressures in the two vascularbeds-the pulmonary circulation is a low pres-
523
on January 26, 2020 by guest. Protected by copyright.
http://jcp.bmj.com
/J C
lin Pathol: first published as 10.1136/jcp.48.6.519 on 1 June 1995. D
ownloaded from

Ferni, Bellini, de Angelis, De Siati, Perrone, Properzi, et al
sure, low resistance vascular bed, where cir-culating endothelin-1 is cleared rapidly.7Therefore, endothelin-1 could not constrictpulmonary vessels in vivo because of the pres-ence of highly stimulated endothelin-B re-
ceptors on the luminal endothelial surface,' 3 10and the consequent endothelin-B receptor me-diated release of prostacyclin and nitric oxide.7Endothelin-1 does not readily penetrate theexternal endothelial cell membrane29 and there-fore circulating endothelin-1 could not bind toendothelin-A receptors, which mediate vaso-
constriction and are expressed by vascularsmooth muscle cells lying beneath theendothelium."° Therefore, it could be hy-pothesised that hypoxia might alter vascularreactivity to various agents, acting either in a
paracrine or an autocrine manner and inter-acting at the vascular level. Locally, the pre-valence of constrictor agents and/or a decreasein vasodilator concentrations could lead to thedevelopment of pulmonary hypertension. Inthis context, the increase in circulating en-
dothelin-1 concentrations could reflect an in-crease in the intracellular production ofendothelin-I and its subsequent release. Ac-cording to this hypothesis, about 80% of newlygenerated endothelin-1 is secreted through thebasolateral membrane, and only 20% is re-
leased into the blood.30 Perhaps, therefore, cir-culating endothelin-1 should be regarded as a
marker for pulmonary hypertension rather thanas a cause of lung disease.
In conclusion, the present study dem-onstrates for the first time that circulating en-
dothelin-1 concentrations are increased inpatients with chronic hypoxia. In spite of theincrease in plasma endothelin-1 concentrationspatients did not have concomitant systemichypertension, renal damage, or cardiovasculardisease. Thus, it is likely that endothelin-1, inconjunction with other endothelium derivedvasoactive factors-for example, prostaglandinI2 and endothelium derived relaxing factor, actsin a autocrine/paracrine manner rather thanin an endocrine one. The direct correlationbetween plasma endothelin-1 concentrationsand pulmonary pressure values suggests thatendothelin-1 may exert its vasoconstrictiveaction in the pulmonary vascular bed. Al-ternatively, it is possible that circulating en-dothelin-1 may have not a significant effect onthe vascular tone in lung arteries, and may bea marker rather than a determinant ofpulmonary disease associated with vaso-constriction.
1 Marsen PA, Brenner BM. Nitric oxide and endothelins:novel autocrine/paracrine regulators of the circulation.Semin Nephrol 1991;11:169-85.
2 Yanagisawa M, Kurihara H, Kimura S, Tomobe Y, Ko-bayashi M, Mitsui Y, et al. A novel potent vasoconstrictorpeptide produced by vascular endothelial cells. Nature1988;332:41 1-15.
3 Luscher TF, Boulanger CM, Dohi Y, Yang Z. Endothelium-derived contracting factors. Hypertension 1992;19:117-30.
4 Schini V, Hendrickson H, Heublein D, Burnett J Jr, Van-houtte P. Thrombin enhances the release of endothelinfrom cultured porcine aortic endothelial cells. EurJ Phar-macol 1989;165:333-4.
5 Yoshizumi M, Kurihara H, Morita T, Yamashita T, Oh-hashi Y, Sugiyama T, et al. Interleukin-l increases theproduction of endothelin-I by cultured endothelial cells.Biochem Biophys Res Commun 1990;166:324-9.
6 Yoshizumi M, Kurihara H, Sugiyama T, Takaku F, Yan-agisawa M, Masaky T, et al. Hemodynamic shear stressstimulates endothelin production by cultured endothelialcells. Biochem Biophys Res Commun 1989;161:859-64.
7 De Nucci G, Thomas R, D'Orleans-Juste P, Antunes E,Walder C, Warner TD, et al. Pressor effects of endothelinare limited by its removal from the pulmonary circulationand by release of prostacyclin and endothelium derivedrelaxing factor. PnscNadAcadSci USA 1988;85:9797-800.
8 Saijonmaa 0, Ristimlki A, Fyhrquist F. Atrial natriureticpeptide, nitroglycerine, and nitroprusside reduce basaland stimulated endothelin production from cultured en-dothelial cells. Biochem Biophys Res Commun 1990;173:514-20.
9 Cade C, Ilozue V, Rubanyi GM, Parker-Botelho LG.Smooth muscle cell factor responsible for decreasing bigendothelin and endothelin produced by cultured endo-thelial cells. J Cardiovasc Pharmacol 1991;17(Suppl 7):71-5.
10 Rubanyi GM, Parker Botelho LH. Endothelins. FASEB J1991;5:2713-20.
11 Miyauchi T, Yanagisawa M, Tomizawa T, Sugishita Y,Suzuki N, Fujino M, et al. Increased plasma concentrationsof endothelin-1 and big endothelin-l in acute myocardialinfarction [letter]. Lancet 1989;ii:53-4.
12 Stewart DJ, Levy R, Cernacek P, Langleben D. Increasedplasma endothelin-1 in pulmonary hypertension-markeror mediator of disease? Ann Intern Med 1991;114:464-9.
13 Rakugi H, Tabuchi Y, Nakamaru M, Nagano M, Hi-gashimori K, Mikami H, et al. Evidence of endothelin-lrelease from resistance vessels of rats in response to hyp-oxia. Biochem Biophys Res Commun 1990;169:973-7.
14 Kourembanas S, Marsden PA, McQuillan LP, Faller DV.Hypoxia induces gene expression and secretion in culturedhuman endothelium. J7 Clin Invest 1991;88:1054-7.
15 Giussani M, Sala C, Cogo A, Ghio F, Pierini A, LegnaniD, et al. Effect of exposure to high altitude on plasmaendothelin in man and its relationship with the changesin pulmonary and systemic pressures. Sixth Europeanmeeting on Hypertension; 1993 Jun 4-7; Milan.
16 De Angelis C, Farrace S, Urbani L, Ferri C, D'Amelio R,Santucci A, et al. Effects of high altitude exposure onplasma and urinary digoxin-like substance. AmJHypertens1992;5:600-7.
17 Lenz T, Scaley JE. Tissue renin system as a possible factorin hypertension. In: Laragh JH, Brenner BM, eds. Hy-pertension, pathophysiology, diagnosis and management. NewYork: Raven Press, 1990:1319-28.
18 Wagner OF, Nowomy P, Vierhapper H, Waldhausl W.Plasma concentrations of endothelin in man: Arterio-venous differences and release during venous stasis. EurJf Clin Invest 1990;20:502-5.
19 Hatle L, Brubakk A, Tromsdal A, Angelsen B. Noninvasiveassessment of pressure drop in mitral stenosis by Dopplerultrasound. Br Heart J 1978;40: 131-40.
20 Takuwa N, Takuwa Y, Yanagisawa M, Yamashita K, MasakiT. A novel vasoactive peptide endothelin stimulates mito-genesis through inositol lipid turnover in Swiss 3T3 fibro-blasts. Jf Biol Chem 1989;264:7856-61.
21 Holden WE, McCall E. Hypoxia-induced contractions ofporcine pulmonary artery strips depend on intact endo-thelium. Exp Lung Res 1984;7:101-2.
22 Bowen-Pope DF, Hart CE, Seifert RA. Sera and conditionedmedia contain different isoforms ofplatelet-derived growthfactor (PDGF) which bind different classes of PDGFreceptors. J Biol Chem 1989;264:2502-8.
23 Adnot S, Raffestin B, Eddahibi S, Braquet P, Chabrier PE.Loss of endothelium-dependent relaxant activity in thepulmonary circulation of rats exposed to chronic hypoxia.J Clin Invest 1991;87:155-62.
24 Vender RL, Clemmons DR, Kwock L, Friedman M. Re-duced oxygen tension induces pulmonary endothelium torelease a pulmonary smooth muscle cell mitogen(s). AmRev Respir Dis 1987;135:622-7.
25 Li H, Elton TS, Chen SJ, Durand J, Chen YF, Oparil S.Chronic hypoxia stimulates pulmonary endothelin-I andendothelin receptor gene transcript levels in rats [abstract].Circulation 1993;88:I-285.
26 Davies P, Maddalo P, Reid L. Effects of chronic hypoxiaon structure and reactivity of rat lung microvessels. JApplPhysiol 1985;58:795-801.
27 Giaid A, Yanagisawa M, Langleben D, Michel RP, Levy R,Shennib H, et al. Expression of endothelin-1 in the lungsof patients with pulmonary hypertension. N EnglJ Med1993;328: 1732-9.
28 Hay DWP. Pharmacological evidence for distinct endothelinreceptors in guinea-pig bronchus and aorta. BrJPharmacol1992;106:759-61.
29 Deleuze PH, Adnot S, Shiiya N, Thoraval R, Eddahibi S,Braquet P, et al. Endothelin dilates bovine pulmonarycirculation and reverses hypoxic pulmonary vaso-constriction. Y Cariovasc Pharmacol 1992;19:354-60.
30 Wagner OF, Christ G, Wojta J, Vierhapper H, Panzer S,Nowotny PJ, et al. Polar secretion of endothelin-1 bycultured endothelial cells. YBiol Chem 1992;267:16066-8.
524
on January 26, 2020 by guest. Protected by copyright.
http://jcp.bmj.com
/J C
lin Pathol: first published as 10.1136/jcp.48.6.519 on 1 June 1995. D
ownloaded from