Embed Size (px)
Citation preview

Paul Zimmet & George AlbertiPaul Zimmet & George AlbertiCo-ChairmenCo-Chairmen
The Metabolic Syndrome: International Diabetes Federation (IDF)
consensus definition

METABOLIC SYNDROME
A cluster of risk factors for diabetes
and cardiovascular disease

The Metabolic Syndrome
A cluster of risk factors for diabetes and cardiovascular disease consisting of:
• Central (abdominal) obesity
• Diabetes, IFG and IGT
• Hypertension
• Dyslipidaemia
(“Deadly Quartet”)

International Diabetes Federation (IDF) consensus definition
In 2004, the IDF held an expert
workshop to examine how the currently
available definitions for the Metabolic
Syndrome could be improved and
developed with the aim of reaching a
consensus for the introduction of a
new and unifying definition.
THE ORIGINS
• 1920s
• 1940s/50s – Vague
• 1967 – Avogaro & Crepaldi
• 1988 - Reaven

Kylin E:
Studien ϋber das Hypertonie-Hyperglykämie
– Hyperurika miesyndrome
1923
Kylin 1923 Description

“seems to suggest a peculiar syndrome including
hyperlipemia, obesity and diabetes. The
development of ischaemic heart disease … and
hypertension is often found in these patients.”
Avogaro & Crepaldi, 1965
Crepaldi 1965 Description
The 2000 WHO Working Group attempt to describe & define the
Metabolic Syndrome was an initiative to create interest and debate – it was never meant to
be the final answer.

Metabolic Syndrome – WHO 1999
At least 1 ofAt least 1 of
• Type 2 diabetesType 2 diabetes
• IGTIGT
• Insulin resistanceInsulin resistance
• Type 2 diabetesType 2 diabetes
• IGTIGT
• Insulin resistanceInsulin resistance
• HypertensionHypertension
• ObesityObesity
• Raised TG or low HDLRaised TG or low HDL
• MicroalbuminuriaMicroalbuminuria
• HypertensionHypertension
• ObesityObesity
• Raised TG or low HDLRaised TG or low HDL
• MicroalbuminuriaMicroalbuminuria
at least 2 ofat least 2 of++ MetabolicMetabolicsyndromesyndromeMetabolicMetabolicsyndromesyndrome
• HyperuricemiaHyperuricemia
• HypercoagulabilityHypercoagulability
• HyperleptinemiaHyperleptinemia
• HyperuricemiaHyperuricemia
• HypercoagulabilityHypercoagulability
• HyperleptinemiaHyperleptinemia
Not required for definition,Not required for definition,
but may be part of the syndromebut may be part of the syndrome

Risk Factor Criterion
Abdominal ObesityMen Women
Waist Circumference>102 cm (>40 in) >88 cm (>35 in)
Triglycerides 150 mg/dL
HDL-CholesterolMenWomen
<40 mg/dL<50 mg/dL
Blood Pressure 130/85 mm Hg
Fasting Glucose 110 mg/dL
NCEP ATP III. JAMA. 2001;285:2486-2497.
The Metabolic Syndrome (ATP III) & Criteria

EGIR Definition of Metabolic Syndrome: 1999
• Insulin resistance + 2 or more of:
• Central obesity (94 cm -M; 80 cm - F)
• TG >2.9 mM OR HDL <1.0
• Hypertension (> 140/90)
• FPG > 6.1 mM

The Metabolic Syndromein Australia; Different Prevalences
for Different Criteria
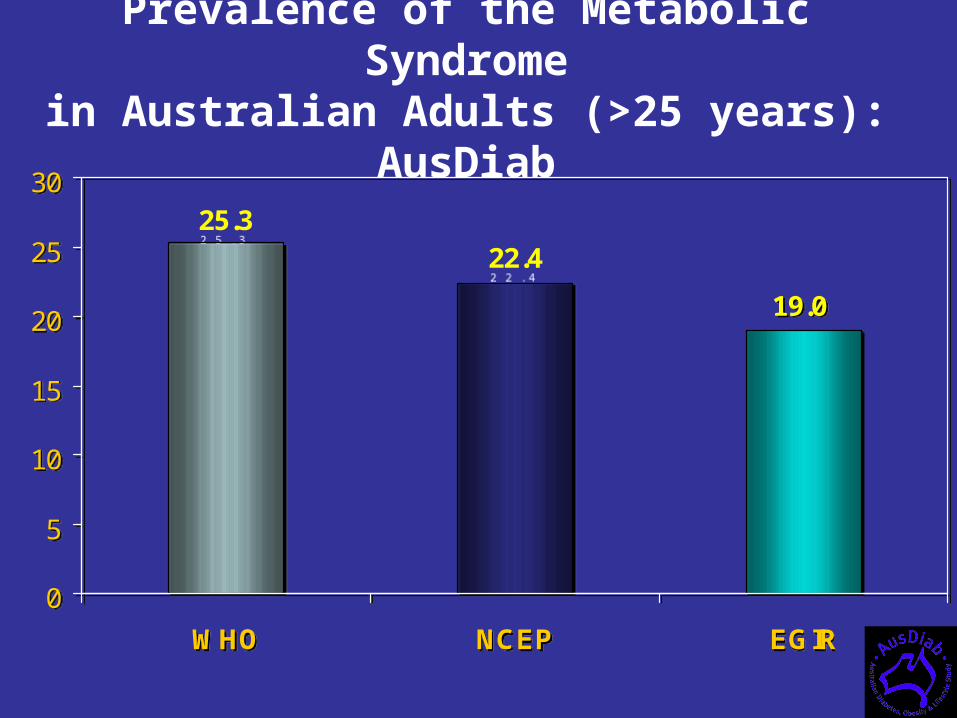
19.0
22.425.3
0
5
10
15
20
25
30
WHO NCEP EGIR
19.0
22.425.3
0
5
10
15
20
25
30
WHO NCEP EGIR
Prevalence of the Metabolic Syndromein Australian Adults (>25 years): AusDiab

Metabolic Syndrome prevalence:3 definitions in Australians - AusDiab
12.012.0
0.80.84.24.2
2.02.0
4.34.34.84.8
4.84.8
ATP III (22.4%)ATP III (22.4%)
EGIR (19.0%)EGIR
(19.0%)
WHO (25.3%)WHO
(25.3%)

RESULT
Confusion!!!

“Consensus Means That A Lot Of
People Say Collectively What No
One Believes Individually”.
“Consensus Means That A Lot Of
People Say Collectively What No
One Believes Individually”.
Abba Eban

Central obesity: a driving force for cardiovascular disease & diabetes
“Balzac” by RodinFront
Back

Developing A New Definition of the Metabolic Syndrome: IDF Objectives
Needs:
• To identify individuals at high risk of developing
cardiovascular disease (and diabetes)
• To be useful for clinicians
• To be useful for international comparisons

The new IDF definition focusses on
abdominal obesity rather than insulin
resistance
International Diabetes Federation (IDF) Consensus Definition 2005

International Diabetes Federation (IDF) Consensus Definition 2005
Central Obesity
Waist circumference – ethnicity specific*
– for Europids: Male > 94 cm
Female > 80 cm
plus any two of the following:
Raised triglycerides > 150 mg/dL (1.7 mmol/L)
or specific treatment for this lipid abnormality
Reduced HDL cholesterol < 40 mg/dL (1.03 mmol/L) in males
< 50 mg/dL (1.29 mmol/L) in females
or specific treatment for this lipid abnormality
Raised blood pressure Systolic : > 130 mmHg or
Diastolic: > 85 mmHg or
Treatment of previously diagnosed hypertension
Raised fasting plasma glucose
Fasting plasma glucose > 100 mg/dL (5.6 mmol/L) or
Previously diagnosed type 2 diabetes
If above 5.6 mmol/L or 100 mg/dL, OGTT is strongly recommended but is not necessary to define presence of the syndrome.

TG
IFG & Diabetes
AbdominalObesity
BP
HDL
Apo BLittle LDL
PAI-1
Adipo-nectin
InsulinResistance*
CRP
* HOMA, euglycemic clamp, fasting insulin etc
Microalb
Tests Recommended for Research: May Be Added To Definition Later
OGTT

Treatment of Metabolic Syndrome: 2005
AspirinDiet, Exercise, Lifestyle change
Stop smoking
CB1 Receptor Blocker
Oral hypoglycaemics
Antihypertensives
Statins & Fibrates
Insulin
ACEI &/or A2 receptor blockers

Primary management for the Metabolic Syndrome is healthy lifestyle promotion. This includes:
• moderate calorie restriction (to achieve a 5-10% loss of body weight in the first year)
• moderate increases in physical activity
• change dietary composition to reduce saturated fat and total intake, increase fibre and, if appropriate, reduce salt intake.
Recommendations for treatment

• Appropriate & aggressive therapy is essentialfor reducing patient risk of cardiovascular disease
• Lifestyle measures should be the first action
• Pharmacotherapy should have beneficial effects on– Glucose intolerance/diabetes– Obesity– Hypertension– Dyslipidaemia
• Ideally, treatment should address all of the components of the syndrome and not the individual components
Management of the Metabolic Syndrome

Summary: new IDF definition for the Metabolic Syndrome
The new IDF definition addresses both clinical and research needs:
• provides a simple entry point for primary care physicians to diagnose the Metabolic Syndrome
• providing an accessible, diagnostic tool suitable for worldwide use, taking into account ethnic differences
• establishing a comprehensive ‘platinum standard’ list of additional criteria that should be included in epidemiological studies and other research into the Metabolic Syndrome