Embed Size (px)
Citation preview

CLINICAL ARTICLEJ Neurosurg 128:1133–1138, 2018
Gliosarcoma (GS) was first described as a variant of glioblastoma (GBM) in 1895.17 Morphologically, GS has classic features of GBM, including nuclear
atypia, mitotic figures, necrosis, and endothelial prolifera-tion. In addition to these classic GBM features, GS also has sarcomatous, mesenchymal differentiation.12,19 Glio-sarcoma is rare, representing between 1% and 8% of all malignant gliomas.8,13,18,20 Given its rarity, there is a lack of epidemiological and clinical management data.4,6,31
Given the lack of data for specific management of GS, treatment paradigms generally mirror those for GBM and include trimodality therapy with surgery, radiation, and concurrent and adjuvant chemotherapy.13 However, it is unknown if this paradigm is optimal for GS because most patients in the studies demonstrating the efficacy of trimo-dality therapy had GBM.3,8,9,25,28 In fact, in the landmark GBM trial published by Stupp et al. (a study demonstrating the improvements in survival with the addition of temo-
ABBREVIATIONS CCI = Charlson Comorbidity Index; GBM = glioblastoma; GS = gliosarcoma; GTR = gross-total resection; MGMT = O6-methylguanine-DNA methyltrans-ferase; NCDB = National Cancer Database.SUBMITTED August 31, 2016. ACCEPTED December 21, 2016.INCLUDE WHEN CITING Published online June 16, 2017; DOI: 10.3171/2016.12.JNS162291.
Patterns of care and outcomes in gliosarcoma: an analysis of the National Cancer DatabaseJonathan Frandsen, MD,1 Andrew Orton, MD,1 Randy Jensen, MD, PhD,2 Howard Colman, MD, PhD,2 Adam L. Cohen, MD, MS,3 Jonathan Tward, MD, PhD,1 Dennis C. Shrieve, MD, PhD,1 and Gita Suneja, MD, MSHP1
Departments of 1Radiation Oncology, 2Neurosurgery (Clinical Neurosciences Center), and 3Oncology, Huntsman Cancer Institute, University of Utah School of Medicine, Salt Lake City, Utah
OBJECTIVE The authors compared presenting characteristics and survival for patients with gliosarcoma (GS) and glioblastoma (GBM). Additionally, they performed a survival analysis for patients who underwent GS treatments with the hypothesis that trimodality therapy (surgery followed by radiation and chemotherapy) would be superior to nontrimodality therapy (surgery alone or surgery followed by chemotherapy or radiation).METHODS Adults diagnosed with GS and GBM between the years 2004 and 2013 were queried from the National Can-cer Database. Chi-square analysis was used to compare presenting characteristics. Kaplan-Meier, Cox regression, and propensity score analyses were employed for survival analyses.RESULTS In total, data from 1102 patients with GS and 36,658 patients with GBM were analyzed. Gliosarcoma had an increased rate of gross-total resection (GTR) compared with GBM (19% vs 15%, p < 0.001). Survival was not different for patients with GBM (p = 0.068) compared with those with GS. After propensity score analysis for GS, patients receiving trimodality therapy (surgery followed by radiation and chemotherapy) had improved survival (12.9 months) compared with those not receiving trimodality therapy (5.5 months). In multivariate analysis, GTR, female sex, fewer comorbidities, trimodality therapy, and age < 65 years were associated with improved survival. There was a trend toward improved sur-vival with MGMT promoter methylation (p = 0.117).CONCLUSIONS In this large registry study, there was no difference in survival in patients with GBM compared with GS. Among GS patients, trimodality therapy significantly improved survival compared with nontrimodality therapy. Gross-total resection also improved survival, and there was a trend toward increased survival with MGMT promoter methylation in GS. The major potential confounder in this study is that patients with poor functional status may not have received aggressive radiation or chemotherapy treatments, leading to the observed outcome. This study should be considered hypothesis-generating; however, due to its rarity, conducting a clinical trial with GS patients alone may prove difficult.https://thejns.org/doi/abs/10.3171/2016.12.JNS162291KEY WORDS radiation; chemotherapy; brain tumors; neurosurgery; molecular genetics; oncology
J Neurosurg Volume 128 • April 2018 1133©AANS 2018, except where prohibited by US copyright law
Unauthenticated | Downloaded 04/05/22 10:10 AM UTC

J. Frandsen et al.
J Neurosurg Volume 128 • April 20181134
zolomide to radiation), it is unknown how many patients with GS were included in the study.28
The purpose of the present study was to evaluate the presenting characteristics and survival for GS compared with GBM in the United States. Additionally, a compara-tive effectiveness analysis was performed for GS treatment with the hypothesis that surgery followed by adjuvant ra-diation and chemotherapy would be superior to omission of one or all of these modalities, similar to GBM.
MethodsData were obtained using the National Cancer Data-
base (NCDB), a program created by the Commission on Cancer and the American Cancer Society. This database includes cases from 1500 hospitals and clinics, capturing nearly 70% of new cancer diagnoses in the United States.16 We queried the database for adults ≥ 18 years of age with a diagnosis of GS or GBM from 2004 to 2013 (reflect-ing all the years contained within the database for these diagnoses). The following exclusions were made: death on the day of diagnosis; no biopsy or surgery performed; un-known chemotherapy or radiotherapy status; neoadjuvant or intraoperative chemotherapy administered; neoadju-vant or intraoperative radiotherapy administered; and use of brachytherapy or radiosurgery.
Patient demographics and tumor characteristic for GS and GBM patients were compared using chi-square statis-tics for categorical variables and Wilcoxon rank sum tests for continuous variables. The following variables were analyzed: age at diagnosis, race, Charlson Comorbidity Index (CCI), insurance status, O6-methylguanine-DNA-methyltransferase (MGMT) gene promoter methylation status, tumor focality, extent of resection, administration of chemotherapy, administration of radiation, and receipt of trimodality therapy (surgery, radiotherapy, and che-motherapy). Extent of resection was determined by the Collaborative Stage Data Collection System (site-specific factor 7), which contains data extracted from both clini-cal and pathology reports, allowing each registrar to use multiple sources (including physician notes) to determine appropriate designation of subtotal or gross-total resec-tion (GTR). Survival outcomes for GS and GBM were then compared using Kaplan-Meier methods and the log-rank test.
The remainder of the analysis focused on GS alone. Kaplan-Meier methods were used to compare outcomes based on treatment received: surgery alone; surgery with adjuvant radiotherapy; or surgery with adjuvant ra-diation and chemotherapy. We also analyzed survival by MGMT methylation status; however, information regard-ing MGMT methylation was only available for patients di-agnosed after 2009. To identify variables associated with overall survival, univariate and multivariate Cox propor-tional hazards modeling was used. Variables were includ-ed in the multivariate analysis if they reached a p value of ≤ 0.20 on univariate analysis.
To address selection bias in the choice of trimodality therapy (surgery followed by radiotherapy and chemother-apy) versus nontrimodality therapy (surgery alone, sur-gery with chemotherapy, or surgery with radiotherapy), we
performed a propensity score analysis to correct for differ-ences in baseline demographic and tumor characteristics between the two treatment groups. Variables that were sig-nificantly associated with survival in our multivariate Cox regression analysis were included in the matching algo-rithm. Propensity scores were generated and the measured covariates between the trimodality and the nontrimodality groups were balanced.1,2 These analyses were performed using the Stata 14.0 statistical package (StataCorp). All NCDB information is de-identified; the study was submit-ted to the internal review board at the University of Utah and was exempt from review.
ResultsIn total, 36,658 individuals were identified with GBM
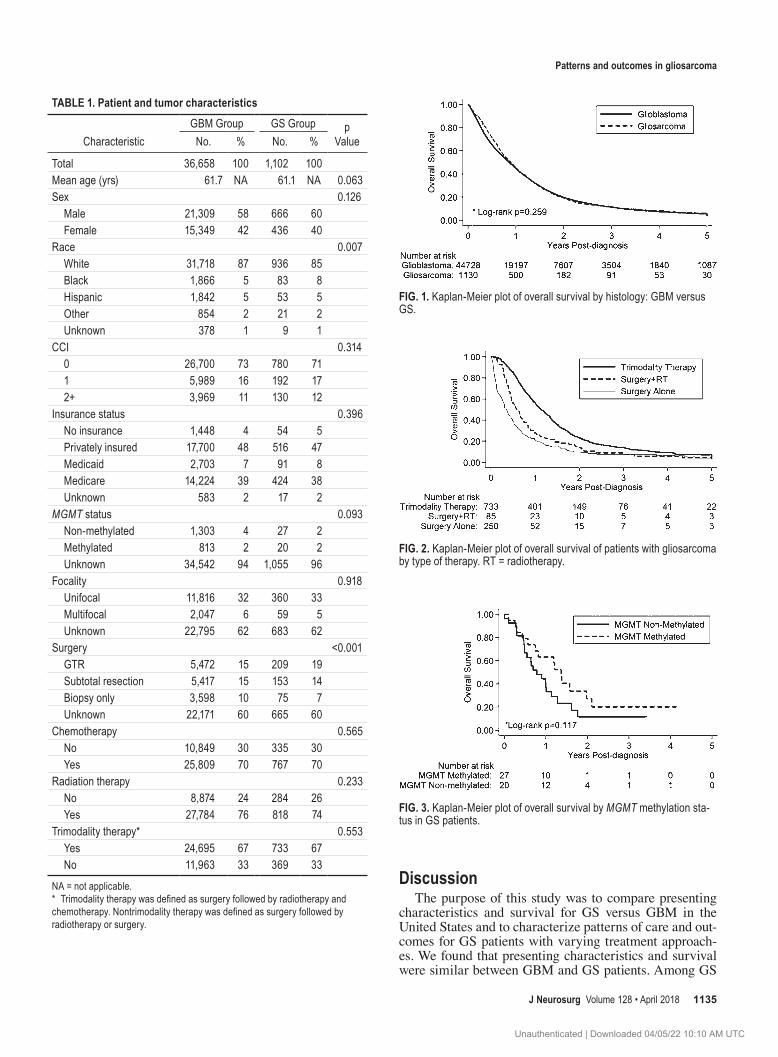
and 1102 with GS. The median follow-up time was 11.3 months and 10.4 months for GBM and GS, respectively. See Table 1 for pertinent patient and tumor characteristics. Of note, GTR was achieved more often in patients with GS than in with those with GBM. There was no differ-ence in survival for patients with GBM when comparing the two histologies by log-rank test (Fig. 1) (p = 0.068). Median survival was 11.9 and 10.7 months for individuals with GBM and GS, respectively.
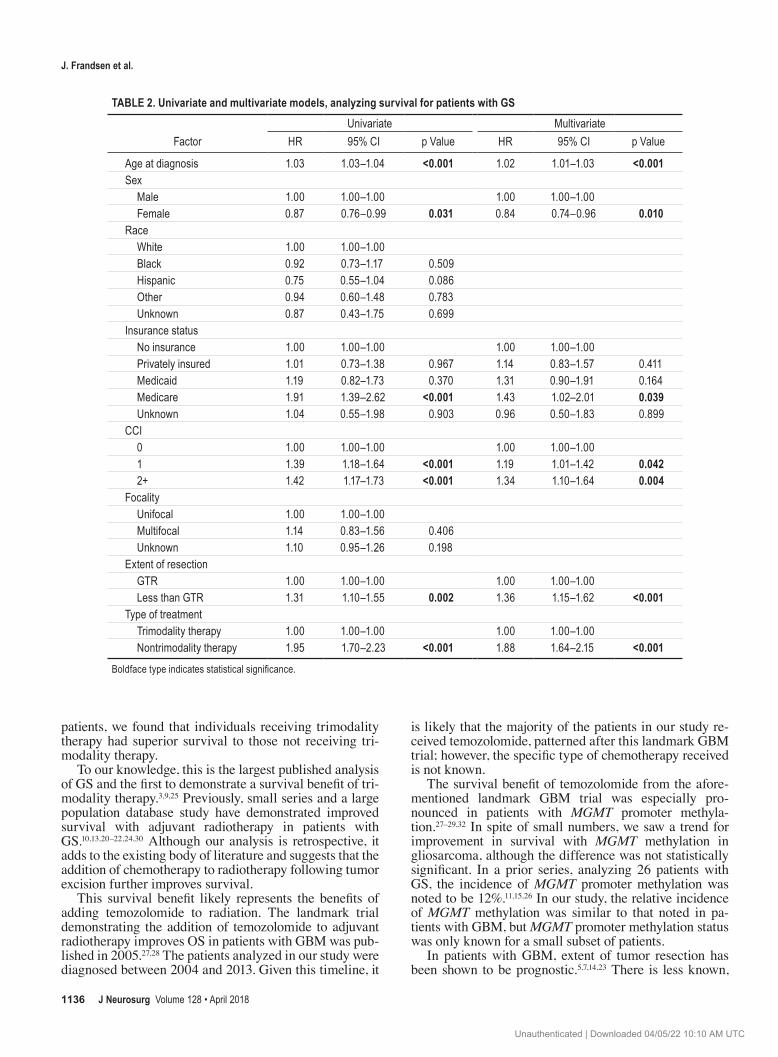
When analyzing only patients with GS by Kaplan-Mei-er methods and log-rank test, there was a survival advan-tage to receiving radiation treatment alone after surgery compared with surgery alone (Fig. 2) (p = 0.015). The me-dian survival in those receiving surgery followed by radio-therapy was 6.9 months compared with 4.3 months with surgery alone. In those who received trimodality therapy (surgery, radiotherapy, and chemotherapy), survival was improved compared with those receiving surgery alone (p < 0.001) or surgery with radiotherapy alone (Fig. 2) (p < 0.001). Median survival for an individual with GS receiv-ing trimodality therapy was 13.5 months.
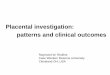
Of the 47 patients with GS that had MGMT methyla-tion status available, 27 had MGMT methylation and 20 did not. Median survival was 16.4 months for those with MGMT promoter methylation versus 9.4 months for those without MGMT promoter methylation (Fig. 3) (p = 0.117).
The results of the univariate and multivariate analyses are displayed in Table 2. Trimodality therapy and GTR were associated with improved survival in both univari-ate and multivariate models for patients with GS (Table 2). The following patient and tumor characteristics were found to be associated with worse survival for GS on both univariate and multivariate analysis: male sex, Medicare insurance, and increasing CCI (Table 2).
After propensity score analysis, patient demographic and tumor characteristics were more balanced between the trimodality and nontrimodality groups (p > 0.05 for all variables). The median survival for patients with GS remained significantly higher for those receiving trimo-dality than those not receiving trimodality therapy by log-rank test (p < 0.001) and by shared frailty univariate Cox regression (hazard ratio 2.039, 95% CI 1.716–2.422, and p < 0.001). Median survival was 12.9 months and 5.52 months for those receiving and not receiving trimodality therapy, respectively.
Unauthenticated | Downloaded 04/05/22 10:10 AM UTC
Patterns and outcomes in gliosarcoma
J Neurosurg Volume 128 • April 2018 1135
DiscussionThe purpose of this study was to compare presenting
characteristics and survival for GS versus GBM in the United States and to characterize patterns of care and out-comes for GS patients with varying treatment approach-es. We found that presenting characteristics and survival were similar between GBM and GS patients. Among GS
FIG. 1. Kaplan-Meier plot of overall survival by histology: GBM versus GS.
FIG. 2. Kaplan-Meier plot of overall survival of patients with gliosarcoma by type of therapy. RT = radiotherapy.
TABLE 1. Patient and tumor characteristics
CharacteristicGBM Group GS Group p
ValueNo. % No. %
Total 36,658 100 1,102 100Mean age (yrs) 61.7 NA 61.1 NA 0.063Sex 0.126 Male 21,309 58 666 60 Female 15,349 42 436 40Race 0.007 White 31,718 87 936 85 Black 1,866 5 83 8 Hispanic 1,842 5 53 5 Other 854 2 21 2 Unknown 378 1 9 1CCI 0.314 0 26,700 73 780 71 1 5,989 16 192 17 2+ 3,969 11 130 12Insurance status 0.396 No insurance 1,448 4 54 5 Privately insured 17,700 48 516 47 Medicaid 2,703 7 91 8 Medicare 14,224 39 424 38 Unknown 583 2 17 2MGMT status 0.093 Non-methylated 1,303 4 27 2 Methylated 813 2 20 2 Unknown 34,542 94 1,055 96Focality 0.918 Unifocal 11,816 32 360 33 Multifocal 2,047 6 59 5 Unknown 22,795 62 683 62Surgery <0.001 GTR 5,472 15 209 19 Subtotal resection 5,417 15 153 14 Biopsy only 3,598 10 75 7 Unknown 22,171 60 665 60Chemotherapy 0.565 No 10,849 30 335 30 Yes 25,809 70 767 70Radiation therapy 0.233 No 8,874 24 284 26 Yes 27,784 76 818 74Trimodality therapy* 0.553 Yes 24,695 67 733 67 No 11,963 33 369 33
NA = not applicable.* Trimodality therapy was defined as surgery followed by radiotherapy and chemotherapy. Nontrimodality therapy was defined as surgery followed by radiotherapy or surgery.
FIG. 3. Kaplan-Meier plot of overall survival by MGMT methylation sta-tus in GS patients.
Unauthenticated | Downloaded 04/05/22 10:10 AM UTC
J. Frandsen et al.
J Neurosurg Volume 128 • April 20181136
patients, we found that individuals receiving trimodality therapy had superior survival to those not receiving tri-modality therapy.
To our knowledge, this is the largest published analysis of GS and the first to demonstrate a survival benefit of tri-modality therapy.3,9,25 Previously, small series and a large population database study have demonstrated improved survival with adjuvant radiotherapy in patients with GS.10,13,20–22,24,30 Although our analysis is retrospective, it adds to the existing body of literature and suggests that the addition of chemotherapy to radiotherapy following tumor excision further improves survival.
This survival benefit likely represents the benefits of adding temozolomide to radiation. The landmark trial demonstrating the addition of temozolomide to adjuvant radiotherapy improves OS in patients with GBM was pub-lished in 2005.27,28 The patients analyzed in our study were diagnosed between 2004 and 2013. Given this timeline, it
is likely that the majority of the patients in our study re-ceived temozolomide, patterned after this landmark GBM trial; however, the specific type of chemotherapy received is not known.
The survival benefit of temozolomide from the afore-mentioned landmark GBM trial was especially pro-nounced in patients with MGMT promoter methyla-tion.27–29,32 In spite of small numbers, we saw a trend for improvement in survival with MGMT methylation in gliosarcoma, although the difference was not statistically significant. In a prior series, analyzing 26 patients with GS, the incidence of MGMT promoter methylation was noted to be 12%.11,15,26 In our study, the relative incidence of MGMT methylation was similar to that noted in pa-tients with GBM, but MGMT promoter methylation status was only known for a small subset of patients.
In patients with GBM, extent of tumor resection has been shown to be prognostic.5,7,14,23 There is less known,
TABLE 2. Univariate and multivariate models, analyzing survival for patients with GS
FactorUnivariate Multivariate
HR 95% CI p Value HR 95% CI p Value
Age at diagnosis 1.03 1.03–1.04 <0.001 1.02 1.01–1.03 <0.001Sex Male 1.00 1.00–1.00 1.00 1.00–1.00 Female 0.87 0.76–0.99 0.031 0.84 0.74–0.96 0.010Race White 1.00 1.00–1.00 Black 0.92 0.73–1.17 0.509 Hispanic 0.75 0.55–1.04 0.086 Other 0.94 0.60–1.48 0.783 Unknown 0.87 0.43–1.75 0.699Insurance status No insurance 1.00 1.00–1.00 1.00 1.00–1.00 Privately insured 1.01 0.73–1.38 0.967 1.14 0.83–1.57 0.411 Medicaid 1.19 0.82–1.73 0.370 1.31 0.90–1.91 0.164 Medicare 1.91 1.39–2.62 <0.001 1.43 1.02–2.01 0.039 Unknown 1.04 0.55–1.98 0.903 0.96 0.50–1.83 0.899CCI 0 1.00 1.00–1.00 1.00 1.00–1.00 1 1.39 1.18–1.64 <0.001 1.19 1.01–1.42 0.042 2+ 1.42 1.17–1.73 <0.001 1.34 1.10–1.64 0.004Focality Unifocal 1.00 1.00–1.00 Multifocal 1.14 0.83–1.56 0.406 Unknown 1.10 0.95–1.26 0.198Extent of resection GTR 1.00 1.00–1.00 1.00 1.00–1.00 Less than GTR 1.31 1.10–1.55 0.002 1.36 1.15–1.62 <0.001Type of treatment Trimodality therapy 1.00 1.00–1.00 1.00 1.00–1.00 Nontrimodality therapy 1.95 1.70–2.23 <0.001 1.88 1.64–2.15 <0.001
Boldface type indicates statistical significance.
Unauthenticated | Downloaded 04/05/22 10:10 AM UTC

Patterns and outcomes in gliosarcoma
J Neurosurg Volume 128 • April 2018 1137
however, regarding the utility of a GTR in patients with GS. Using the SEER database, Kozak et al. demonstrated that a biopsy alone resulted in worse survival than either subtotal resection or GTR in patients treated for GS.13 Our study also found GTR to be associated with improved sur-vival compared with subtotal resection or biopsy.
The present study provides new insight into the man-agement of and survival from GS. There are, however, several important limitations. The study is retrospective and therefore subject to selection bias. We tried to mitigate this bias with multivariate analyses and propensity score matching, but not all clinically relevant variables were available in the database. For example, patients with GS not receiving chemotherapy may have been sicker at base-line, more neurologically disabled, or have had poorer so-cial support. This information could not be gleaned from the database and was thus not included in our multivariate modeling. In addition, miscoding variables is another pos-sible bias, inherent to all large, multiinstitutional registries that depend on individual hospital registrars for coding. Registrars can make errors when entering data regarding subjective variables, such as extent of resection. In addi-tion to incorrectly entered variables, a substantial amount of data are missing from the NCDB database. For ex-ample, 60% of patients have unknown extent of resection. Missing data may lead to selection bias, where the cases with the most completely reported data are also those of patients who received the most aggressive care. This study should be considered hypothesis-generating; however, due to its rarity, conducting a clinical trial with GS patients alone may prove difficult.
ConclusionsThis is the largest study analyzing presenting characteris-tics, patterns of care, and outcomes for GS, a rare central nervous tumor. For patients with GS, presenting charac-teristics, patterns of care in the United States, and overall survival appear to be similar to GBM. Trimodality therapy significantly improved survival for patients with GS com-pared with nontrimodality therapies, even after matching cases of the available, significant covariates. Gross-total resection appeared to improve survival, and there was a trend toward improved survival in GS patients with the MGMT promoter methylation. Further research is needed to identify therapies that improve survival from GS.
References 1. Austin PC: An introduction to propensity score methods for
reducing the effects of confounding in observational studies. Multivariate Behav Res 46:399–424, 2011
2. Austin PC: Optimal caliper widths for propensity-score matching when estimating differences in means and differ-ences in proportions in observational studies. Pharm Stat 10:150–161, 2011
3. Buckner JC, Ballman KV, Michalak JC, Burton GV, Cascino TL, Schomberg PJ, et al: Phase III trial of carmustine and cisplatin compared with carmustine alone and standard radi-ation therapy or accelerated radiation therapy in patients with glioblastoma multiforme: North Central Cancer Treatment Group 93-72-52 and Southwest Oncology Group 9503 Trials. J Clin Oncol 24:3871–3879, 2006
4. Cachia D, Kamiya-Matsuoka C, Mandel JJ, Olar A, Cykow-ski MD, Armstrong TS, et al: Primary and secondary glio-sarcomas: clinical, molecular and survival characteristics. J Neurooncol 125:401–410, 2015
5. Curran WJ Jr, Scott CB, Horton J, Nelson JS, Weinstein AS, Fischbach AJ, et al: Recursive partitioning analysis of prog-nostic factors in three Radiation Therapy Oncology Group malignant glioma trials. J Natl Cancer Inst 85:704–710, 1993
6. Damodaran O, van Heerden J, Nowak AK, Bynevelt M, Mc-Donald K, Marsh J, et al: Clinical management and survival outcomes of gliosarcomas in the era of multimodality thera-py. J Clin Neurosci 21:478–481, 2014
7. Devaux BC, O’Fallon JR, Kelly PJ: Resection, biopsy, and survival in malignant glial neoplasms. A retrospective study of clinical parameters, therapy, and outcome. J Neurosurg 78:767–775, 1993
8. Galanis E, Buckner JC, Dinapoli RP, Scheithauer BW, Jen-kins RB, Wang CH, et al: Clinical outcome of gliosarcoma compared with glioblastoma multiforme: North Central Can-cer Treatment Group results. J Neurosurg 89:425–430, 1998
9. Halperin EC, Herndon J, Schold SC, Brown M, Vick N, Cairncross JG, et al: A phase III randomized prospective trial of external beam radiotherapy, mitomycin C, carmus-tine, and 6-mercaptopurine for the treatment of adults with anaplastic glioma of the brain. Int J Radiat Oncol Biol Phys 34:793–802, 1996
10. Han SJ, Yang I, Tihan T, Prados MD, Parsa AT: Primary gliosarcoma: key clinical and pathologic distinctions from glioblastoma with implications as a unique oncologic entity. J Neurooncol 96:313–320, 2010
11. Kang SH, Park KJ, Kim CY, Yu MO, Park CK, Park SH, et al: O6-methylguanine DNA methyltransferase status deter-mined by promoter methylation and immunohistochemistry in gliosarcoma and their clinical implications. J Neurooncol 101:477–486, 2011
12. Karsy M, Gelbman M, Shah P, Balumbu O, Moy F, Arslan E: Established and emerging variants of glioblastoma mul-tiforme: review of morphological and molecular features. Folia Neuropathol 50:301–321, 2012
13. Kozak KR, Mahadevan A, Moody JS: Adult gliosarcoma: epidemiology, natural history, and factors associated with outcome. Neuro Oncol 11:183–191, 2009
14. Laws ER, Parney IF, Huang W, Anderson F, Morris AM, Asher A, et al: Survival following surgery and prognostic factors for recently diagnosed malignant glioma: data from the Glioma Outcomes Project. J Neurosurg 99:467–473, 2003
15. Lee D, Kang SY, Suh YL, Jeong JY, Lee JI, Nam DH: Clini-copathologic and genomic features of gliosarcomas. J Neu-rooncol 107:643–650, 2012
16. Lerro CC, Robbins AS, Phillips JL, Stewart AK: Compari-son of cases captured in the national cancer data base with those in population-based central cancer registries. Ann Surg Oncol 20:1759–1765, 2013
17. Louis DN, Ohgaki H, Wiestler OD, Cavenee WK, Burger PC, Jouvet A, et al: The 2007 WHO classification of tumours of the central nervous system. Acta Neuropathol 114:97–109, 2007
18. Lutterbach J, Guttenberger R, Pagenstecher A: Gliosarcoma: a clinical study. Radiother Oncol 61:57–64, 2001
19. McAleer MF, Brown PD: Therapeutic management of glio-sarcoma in the temozolomide era. CNS Oncol 4:171–178, 2015
20. Meis JM, Martz KL, Nelson JS: Mixed glioblastoma multi-forme and sarcoma. A clinicopathologic study of 26 radia-tion therapy oncology group cases. Cancer 67:2342–2349, 1991
21. Morantz RA, Feigin I, Ransohoff J III: Clinical and patho-
Unauthenticated | Downloaded 04/05/22 10:10 AM UTC

J. Frandsen et al.
J Neurosurg Volume 128 • April 20181138
logical study of 24 cases of gliosarcoma. J Neurosurg 45:398–408, 1976
22. Ono N, Nakamura M, Inoue HK, Tamura M, Murata M: Congenital gliosarcoma; so-called sarcoglioma. Childs Nerv Syst 6:416–420, 1990
23. Quigley MR, Maroon JC: The relationship between survival and the extent of the resection in patients with supratentorial malignant gliomas. Neurosurgery 29:385–389, 1991
24. Salvati M, Lenzi J, Brogna C, Frati A, Piccirilli M, Giangas-pero F, et al: Childhood’s gliosarcomas: pathological and therapeutical considerations on three cases and critical re-view of the literature. Childs Nerv Syst 22:1301–1306, 2006
25. Schold SC Jr, Herndon JE, Burger PC, Halperin EC, Vick NA, Cairncross JG, et al: Randomized comparison of diazi-quone and carmustine in the treatment of adults with anaplas-tic glioma. J Clin Oncol 11:77–83, 1993
26. Singh G, Mallick S, Sharma V, Joshi N, Purkait S, Jha P, et al: A study of clinico-pathological parameters and O6-methylguanine DNA methyltransferase (MGMT) promoter methylation status in the prognostication of gliosarcoma. Neuropathology 32:534–542, 2012
27. Stupp R, Hegi ME, Mason WP, van den Bent MJ, Taphoorn MJ, Janzer RC, et al: Effects of radiotherapy with concomi-tant and adjuvant temozolomide versus radiotherapy alone on survival in glioblastoma in a randomised phase III study: 5-year analysis of the EORTC-NCIC trial. Lancet Oncol 10:459–466, 2009
28. Stupp R, Mason WP, van den Bent MJ, Weller M, Fisher B, Taphoorn MJ, et al: Radiotherapy plus concomitant and adjuvant temozolomide for glioblastoma. N Engl J Med 352:987–996, 2005
29. Stupp R, Weber DC: The role of radio- and chemotherapy in glioblastoma. Onkologie 28:315–317, 2005
30. Walker GV, Gilbert MR, Prabhu SS, Brown PD, McAleer MF: Temozolomide use in adult patients with gliosarcoma: an evolving clinical practice. J Neurooncol 112:83–89, 2013
31. Zhang G, Huang S, Zhang J, Wu Z, Lin S, Wang Y: Clinical outcome of gliosarcoma compared with glioblastoma mul-tiforme: a clinical study in Chinese patients. J Neurooncol 127:355–362, 2016
32. Zhang K, Wang XQ, Zhou B, Zhang L: The prognostic value of MGMT promoter methylation in Glioblastoma multiforme: a meta-analysis. Fam Cancer 12:449–458, 2013
Disclosures Dr. Tward received personal fees and a grant for “A Retrospective Study of Prolaris for the Prediction of Progression in Men Treated with Modern External Beam Radiation Therapy for Prostate Can-cer,” which is outside the submitted work, from Myriad Genetics; he is also a consultant for Myriad. Dr. Jensen received personal fees from Medtronic and Pharmaco-Kinesis outside the submitted work. Dr. Colman is a consutant for the following: Roche, Genen-tech, Smith, Novocure, Oxigene, Omniox, CytRx, and Insys.
Author ContributionsConception and design: Suneja, Frandsen, Orton. Acquisition of data: Suneja, Frandsen, Orton. Analysis and interpretation of data: Suneja, Frandsen, Orton, Jensen, Colman, Cohen, Shrieve. Draft-ing the article: Suneja, Frandsen, Orton. Critically revising the article: all authors. Reviewed submitted version of manuscript: all authors. Approved the final version of the manuscript on behalf of all authors: Suneja. Statistical analysis: Suneja, Frandsen, Orton. Administrative/technical/material support: Orton. Study supervi-sion: Suneja, Shrieve.
CorrespondenceGita Suneja, Department of Radiation Oncology, Huntsman Can-cer Institute, University of Utah, 1950 Circle of Hope Rm. 1570, Salt Lake City, UT 84112. email: [email protected].
Unauthenticated | Downloaded 04/05/22 10:10 AM UTC










![A Stable Secondary Gliosarcoma with Extensive ... - :: BTRT · blastoma have been reported in 0.2–1.2% of cases versus 11% for gliosarcoma [6,7]. Hematogenous metastases may result](https://img.pdfslide.us/doc/110x75/600d76555e1ed3334f2cf06e/a-stable-secondary-gliosarcoma-with-extensive-btrt-blastoma-have-been-reported.jpg)

















![Case Report Gliosarcoma with Primary Skull Base Invasiondownloads.hindawi.com/journals/crira/2016/1762195.pdfmasses comparable to GB with a temporal predominance [,]. At resection,](https://img.pdfslide.us/doc/110x75/5f47900fde36320e83385ec6/case-report-gliosarcoma-with-primary-skull-base-masses-comparable-to-gb-with-a-temporal.jpg)