Embed Size (px)
Citation preview

Patterns and Predictors of Use of Warfarin andOther Common Long-Term Medicationsin Patients with Atrial FibrillationXue Song,1 Stephen D. Sander,2 Helen Varker1 and Alpesh Amin3
1 Truven Health Analytics, Cambridge, MA, USA
2 Boehringer Ingelheim Pharmaceuticals, Inc., Ridgefield, CT, USA
3 School of Medicine, University of California, Irvine, CA, USA
Abstract Background and Objective: No study has been published that compared persistence and discontinuation of
warfarinwith other long-termmedications in patientswith atrial fibrillation (AF). The objective of this studywas
to evaluate persistence anddiscontinuationpatterns inAFpatients takingwarfarin andother common long-term
medications and identify predictors of persistence and discontinuation in this population.
Methods: Patients with warfarin prescription within 3 months after AF hospitalization discharge and
12-month data before and after the first prescription were evaluated using administrative claims data
(1 January 2005 – 31December 2007). For comparison, persistence patterns for other long-termmedications
for treatment of hypertension, hyperglycemia, heart disease, and dyslipidemia, including once- (od) and
twice- (bid) daily medications, were evaluated. Non-persistence was defined as the presence of a ‡60-day gapin medication use. Permanent discontinuation was defined as no use of the medication for ‡90 days until theend of the follow-up period. Multivariate analysis was conducted to identify predictors of warfarin non-
persistence and discontinuation.
Results: 28 384 patients with AF were identified; 16 036 (56.5%) had a warfarin prescription following AF
hospitalization. 53.5% of warfarin users were persistent for at least 1 year, similar to other long-term
medications commonly prescribed to the AF population (ranging between 45.2% and 61.3%). 42.6% of
warfarin users permanently discontinued warfarin within 1 year, also consistent with the discontinuation
rate of 32.9–52.0% of other long-term medications. Residence in the South and West regions of the US,
history of cardiac dysrhythmias, andwarfarin cost-sharing significantly decreased the likelihood of warfarin
persistence and increased the likelihood of discontinuation, while older age, history of ischemic stroke, and
warfarin use before hospitalization significantly increased warfarin persistence and decreased the likelihood
of discontinuation. Adherence of od and bid medications was similar.
Conclusion: Persistence and discontinuation with warfarin in patients with AF is consistent with other long-
term medications. Identifying factors associated with non-persistence and discontinuation with long-term
medications can help in developing targeted adherence programs.
Introduction
Nearly 2.3 million adults in the USA are currently diagnosed
with atrial fibrillation (AF), a common cardiac arrhythmia,
with more than 5.6 million projected by the year 2050.[1] The
prevalence of AF increases with age, occurring in about 9% of
adults 80 years and older.[1] AF is associated with a near 5-fold
increase in stroke incidence,[2] which can be reduced signif-
icantly with the use of antithrombotic therapy. A recent meta-
analysis demonstrated a 64% reduction in stroke incidence in
patients with AF receiving warfarin in tightly controlled ran-
domized trials; antiplatelet agents (e.g. acetylsalicylic acid
[aspirin]) were substantially less efficacious, reducing stroke by
22%.[3] Before the approval of dabigatran etexilate mesylate,
the American College of Chest Physicians strongly recommends
that AF patients with high risk or more than one moderate
ORIGINAL RESEARCH ARTICLEAm J Cardiovasc Drugs 2012; 12 (4): 245-253
1175-3277/12/0004-0245/$49.95/0
Adis ª 2012 Springer International Publishing AG. All rights reserved.

stroke risk factor be treated with warfarin, patients with one
moderate risk factor be treated with warfarin or aspirin, and
patients with no risk factors be treated with aspirin.[4,5] Com-
pared with the 2001 anticoagulant therapy guidelines that
recommended using patient’s characteristics such as age, sex,
heart disease risk, and concurrent conditions to determine
proper therapies, the 2006 guidelines emphasized considera-
tion of stroke risk in determining the need for anticoagulant
therapy. Warfarin can also be used by patients undergoing
cardioversion or catheter ablation or for the prevention of
thromboembolism.[5] Thus patients with no risk factor of stroke
may still be temporarily treated with warfarin in anticipation of
cardioversion or catheter ablation.
Patients with AF are often treated with life-long stroke risk
reduction therapy. Therefore, the importance of taking and
remaining on anticoagulation cannot be underestimated in this
patient population. Medication adherence and persistence di-
rectly impact health outcomes and healthcare utilization in
persons with chronic diseases.[6-9] However, despite its efficacy in
stroke risk reduction, warfarin persistence in patients with chronic
AF is not ideal. Gallagher et al.[10] found that the 1-year persis-
tence with warfarin in a population of UK patients aged 40 years
and older with chronic AF was only 70%. A systemic review of
96 studies found that anticoagulant therapy was underused in AF
patients with elevated risk of stroke.[11] No study has been pub-
lished that compared persistence and discontinuation of warfarin
with other long-term medications in the AF population.
This study used a large national claims dataset to examine
persistence and continuation of warfarin and other long-term
medications commonly used in non-valvular AF (NVAF) pa-
tients, and to determine predictors of persistence and con-
tinuation, especially if patient cost-sharing and dosing sched-
ules have a significant impact on persistence.
Methods
Data Source
Two Truven Health AnalyticsMarketScan�Research Data-
bases, the Commercial Claims and Encounters (Commercial)
Database and the Medicare Supplement and Coordination of
Benefit (Medicare) Database, were used in this study. The
Commercial Database contains the inpatient, outpatient, and
outpatient prescription medication experience of employees
and their dependents, covered under a variety of fee-for-service
and capitated health plans. The Medicare Database contains
the healthcare experience of individuals with Medicare sup-
plemental insurance paid for by employers. Because it covers an
older population than the Commercial Database, theMedicare
Database is a key data source for this study. Both Medicare-
covered (represented as Coordination of Benefits Amount) and
employer-paid dollars are included in this database. During
2007, there were 23 million covered lives in the Commercial
Database and 2 million retirees enrolled in the Medicare
Database. Both databases areHealth Insurance Portability and
Accountability Act (HIPAA) compliant.
Study Population
The study period covered 1 January 2005 – 31 December
2007. Patients with AF hospitalizations identified by primary
or secondary diagnosis of AF (ICD-9-CM 427.31) between
1 January 2006 and 31 December 2006 were extracted. All pa-
tients were required to have continuous enrollment with med-
ication prescription benefit for at least 12 months prior to the
hospital admission date and at least 12 months following the
date of discharge. Patients with evidence of valvular disease of
AF (i.e. hyperthyroidism, pulmonary embolism, or cardiac
surgery) during the 12-month pre-period and up to 30 days
post-discharge were excluded from the study.
Long-Term Medications
To understand whether persistence with anticoagulant ther-
apy is better or worse than other commonly taken long-term
classes of medications in a population with non-valvular AF,
six medications were selected from the antihypertensive and anti-
hyperglycemic classes. These medications were selected because,
based on the frequency distribution of all medications used in AF
patients, they were the most commonly prescribed therapeutic
classes in the AF population. Metformin extended release (once
daily [od]), metformin non-extended release (twice daily [bid]),
pioglitazone (od), sitagliptin (od), carvedilol phosphate (od), and
carvedilol (bid) had different dosing schedules (e.g. od and bid
dosing), adequate sample size (at least 300 users), and a low
likelihood of being used short-term or ‘as needed’. In addition,
lisinopril, valsartan, and simvastatin were selected to represent
treatment of heart diseases and dyslipidemia. Dosing schedules for
these medication products were extracted from package inserts.
Study Period
For the warfarin persistence analysis, patients were required
to have at least one warfarin prescription within 3 months from
their AF hospitalization discharge date. The index date was the
first warfarin prescription date following the AF hospital-
246 Song et al.
Adis ª 2012 Springer International Publishing AG. All rights reserved. Am J Cardiovasc Drugs 2012; 12 (4)

ization discharge. For the individual medication adherence
analysis, the index date was the first prescription of each in-
dividual medication. Patients were required to have 12-month
continuous enrollment with medication prescription benefit
prior to (pre-period) and 12-month continuous enrollment follow-
ing (post-period) the index date. Patients with prescriptions of
each of these nine individual medications in the 12-month pre-
period were excluded from the study to ensure that the index
date was the first prescription of such long-term medications.
For example, patients treated with metformin extended release
in the pre-period were excluded from the metformin extended
release adherence study. This is shown graphically in figure 1.
Variable Definitions
Demographic and Clinical Characteristics
Demographic characteristics (age, sex, geographic region,
health plan type, and payer) were measured on the index
date. AF complications (congestive and chronic heart failure,
cardiac dysrhythmias other than AF, ischemic stroke), and
co-morbidities (pneumonia, chronic obstructive pulmonary
disease, coronary artery disease, acute myocardial infarction,
transient ischemic attack, hypovolemia, aspiration pneumonia,
urinary tract infection, hypertension, other thyroid disease,
diabetes mellitus, cardiomyopathies, and cancer) were mea-
sured during the 12-month pre-period. CHADS2, a score that
predicts the risk of stroke in patients with non-rheumatic AF
based on evidence of congestive heart failure, hypertension, age
>75 years, diabetes, and prior stroke or transient ischemic at-
tack, was also measured during the pre-period.
The number of unique medications prescribed during the pre-
period was counted. Patient cost-sharing burden wasmeasured as
co-pay and co-insurance of the index prescription claim.
Persistence and Discontinuation Measures
Persistence and discontinuation were calculated for warfarin
and each of the selected nine long-term medications during the
12-month post-period. Non-persistence or medication inter-
ruption was defined as a single gap of at least 60 days. Dis-
continuation was defined as the lack of subsequent claims with
evidence of a specific medication for patients who remained
enrolled for at least 90 days after discontinuation of the med-
ication. Consequently, only patients who had at least 90-day
enrollment after the discontinuation of the medication were
eligible for this measure. Because claims data do not have in-
formation on prescriptions during hospitalizations, inpatient
days were considered ‘adherent’ if the patient had a prescription
of that medication prior to the admission date.
Warfarin therapy requires constant monitoring and its
dosing needs to be titrated before a consistent therapeutic in-
ternational normalized ratio (INR) is established. Therefore,
medication possession ratio (MPR) could not be measured
accurately for warfarin due to its complex dosing and man-
agement. For consistency, MPR was not reported for other
long-term medications either.
Comparisons were conducted on persistence and discontinua-
tion between warfarin and other long-term medications.
Analytic Approach
SAS (SAS Institute, Cary, NC, USA) was used to build the
analytic file and to conduct the descriptive analysis. Stata (Stata-
Corp LP, College Station, TX, USA) was used for multivariate
analysis. Statistical tests of significance for persistence and dis-
continuation were carried out for bid versus od medications. Tests
of equal proportions were used to assess the statistical significance
of categorical variables; t-tests were used for continuous variables.
⎧ ⎪ ⎪ ⎪ ⎪ ⎪ ⎪ ⎪ ⎨ ⎪ ⎪ ⎪ ⎪ ⎪ ⎪ ⎪ ⎩
⎧⎪⎪⎪⎪⎪⎪⎪⎪⎨⎪⎪⎪⎪⎪⎪⎪⎪⎩
⎧⎪⎪⎪⎪⎪⎪⎪⎪⎨⎪⎪⎪⎪⎪⎪⎪⎪⎩
⎧⎪⎪⎪⎪⎨⎪⎪⎪⎪⎩
⎧ ⎪ ⎪ ⎪ ⎪ ⎪ ⎪ ⎪ ⎪ ⎪ ⎪ ⎨ ⎪ ⎪ ⎪ ⎪ ⎪ ⎪ ⎪ ⎪ ⎪ ⎪ ⎩
Potential 12-month pre-period with no useof index medication (with exception of warfarin) Potential 12-month medication follow-up period
Index date (first prescriptionof medication of interest)
1 Jan 2005 1 Jan 2006 31 Dec 2006
AF hospitalizations
Potential 12-month post-hospitalization discharge date
Potential 12-month prior to hospitalization admission date
Fig. 1. Flow chart of the study period. AF= atrial fibrillation.
Persistence of Warfarin Treatment in AF patients 247
Adis ª 2012 Springer International Publishing AG. All rights reserved. Am J Cardiovasc Drugs 2012; 12 (4)

Multivariate analysis was conducted to examine the impact of
patient cost-sharing and dosing schedule on persistence and
discontinuation measures, holding all other factors constant.
The impact of dosing schedule was estimated for carvedilol (bid)
versus carvedilol phosphate (od) and metformin hydrochloride
non-extended release (bid) versus metformin hydrochloride ex-
tended release (od). Logistic regressionmodels were estimated to
examine whether a patient was persistent and whether a patient
discontinued therapy. Survival models were used to examine
time to non-persistence and time to discontinuation. All models
controlled for patients’ demographic (age, sex, region, payer)
characteristics, CHADS2, baseline AF complications (cardiac
dysrhythmias, heart failure, ischemic stroke), patient cost-sharing,
and number of medications in the pre-period.
Results
Patients’ Demographic and Clinical Characteristics
Of 28 384 AF patients identified, 16 036 (56.5%) patients
receiving warfarin met the study criteria, with a mean age of
73.0 years (standard deviation [SD] 11.1), 56.5% of whom were
men (table I). The largest age group was ages 75–84 years
(39.0%), followed by ages 65–74 years (24.4%). Consistent with
the age distribution, Medicare served as the primary payer for
77.4% of the population. The majority of patients lived in the
North Central (41.2%) and South (33.3%) regions of the US, a
reflection of the regional distribution inMarketScan databases,
and not necessarily reflective of the actual regional distribution
of AF patients treated with warfarin in the US. Compared with
non-persistent warfarin users, persistent users were on average
1 year older, more likely to live in the North Central region, and
less likely to live in the South and West regions.
The mean CHADS2 was 1.59 (SD 1.10, table II). About one
in three patients had congestive or chronic heart failure, and
four in ten had cardiac dysrhythmias in the pre-period. Hy-
pertension (56.7%), coronary artery disease (42.6%), diabetes
(26.2%), and chronic obstructive pulmonary disease (21.3%)
were the four most common co-morbidities. No significant
differences in most co-morbidities were found between war-
farin persistent users and non-persistent users, but persistent
users were significantly more likely to have baseline transient
ischemic attack and ischemic stroke than non-persistent users.
Non-persistent users were more likely than persistent users to
Table I. Demographic characteristics of warfarin users, overall and by persistence status
Characteristic All warfarin users Persistent warfarin users Non-persistent warfarin users p-Value
(n =16 036) [%] (n= 8586) [%] (n = 7450) [%]
Age group (y)
<45 1.2 0.7 1.8 <0.001
45–54 5.3 4.7 5.8 0.002
55–64 16.9 16.2 17.7 0.009
65–74 24.4 25.1 23.6 0.024
75–84 39.0 39.5 38.5 0.219
85+ 13.2 13.8 12.6 0.027
Mean (SD) age 73.0 (11.1) 73.5 (10.7) 72.5 (11.4) 0.435
Sex
Male 56.5 56.6 56.4 0.793
Female 43.5 43.4 43.6 0.793
Primary payer
Commercial 22.6 21.1 24.4 <0.001
Medicare 77.4 78.9 75.6 <0.001
US geographic region
Northeast 11.7 12.0 11.3 0.13
North Central 41.2 43.0 39.0 <0.001
South 33.3 31.9 35.0 <0.001
West 13.6 12.9 14.5 0.003
Unknown 0.2 0.2 0.2 0.853
248 Song et al.
Adis ª 2012 Springer International Publishing AG. All rights reserved. Am J Cardiovasc Drugs 2012; 12 (4)
have hypovolemia, although the rate was very low in both co-
horts (0.4% v. 0.1%). Warfarin users on average used 13.2 (SD
7.1) different medications in the 12-month pre-period, with
mean cost-sharing totaling $US9.06 (SD $US8.26) for index
warfarin prescription. Persistent users had slightly more med-
ications in the pre-period and lower cost-sharing for warfarin
than non-persistent users.
Warfarin Persistence and Discontinuation Measures
During the 12-month post-period, slightly more than half
(53.5%) of warfarin users were persistent on therapy, and about
four in ten (42.6%) warfarin users discontinued warfarin
treatment, i.e. there was a gap of at least 90 days without any
warfarin use by the end of the follow-up. The remaining 3.9%warfarin users were not persistent but they did not discontinue
warfarin either. On average, it took 122.2 (SD 83.4) days from
the first warfarin prescription to non-persistence and 113.6
(SD 75.1) days to warfarin discontinuation.
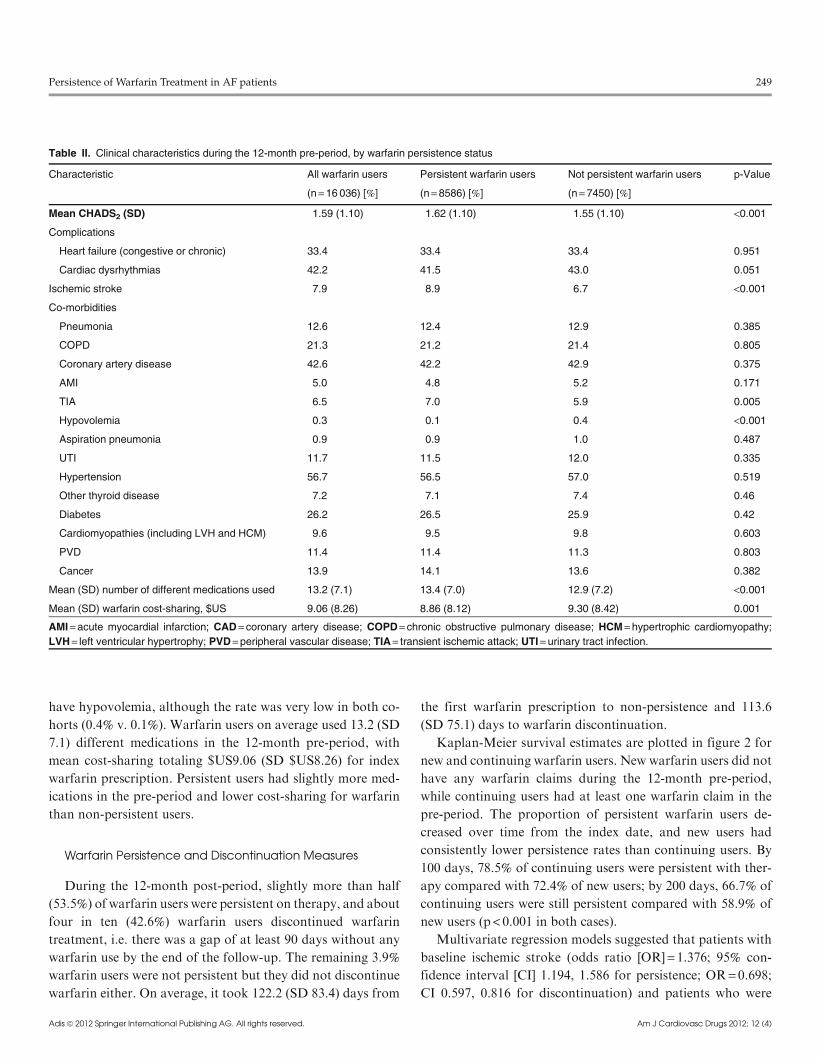
Kaplan-Meier survival estimates are plotted in figure 2 for
new and continuing warfarin users. New warfarin users did not
have any warfarin claims during the 12-month pre-period,
while continuing users had at least one warfarin claim in the
pre-period. The proportion of persistent warfarin users de-
creased over time from the index date, and new users had
consistently lower persistence rates than continuing users. By
100 days, 78.5% of continuing users were persistent with ther-
apy compared with 72.4% of new users; by 200 days, 66.7% of
continuing users were still persistent compared with 58.9% of
new users (p < 0.001 in both cases).
Multivariate regression models suggested that patients with
baseline ischemic stroke (odds ratio [OR] = 1.376; 95% con-
fidence interval [CI] 1.194, 1.586 for persistence; OR = 0.698;CI 0.597, 0.816 for discontinuation) and patients who were
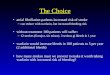
Table II. Clinical characteristics during the 12-month pre-period, by warfarin persistence status
Characteristic All warfarin users Persistent warfarin users Not persistent warfarin users p-Value
(n =16 036) [%] (n= 8586) [%] (n= 7450) [%]
Mean CHADS2 (SD) 1.59 (1.10) 1.62 (1.10) 1.55 (1.10) <0.001
Complications
Heart failure (congestive or chronic) 33.4 33.4 33.4 0.951
Cardiac dysrhythmias 42.2 41.5 43.0 0.051
Ischemic stroke 7.9 8.9 6.7 <0.001
Co-morbidities
Pneumonia 12.6 12.4 12.9 0.385
COPD 21.3 21.2 21.4 0.805
Coronary artery disease 42.6 42.2 42.9 0.375
AMI 5.0 4.8 5.2 0.171
TIA 6.5 7.0 5.9 0.005
Hypovolemia 0.3 0.1 0.4 <0.001
Aspiration pneumonia 0.9 0.9 1.0 0.487
UTI 11.7 11.5 12.0 0.335
Hypertension 56.7 56.5 57.0 0.519
Other thyroid disease 7.2 7.1 7.4 0.46
Diabetes 26.2 26.5 25.9 0.42
Cardiomyopathies (including LVH and HCM) 9.6 9.5 9.8 0.603
PVD 11.4 11.4 11.3 0.803
Cancer 13.9 14.1 13.6 0.382
Mean (SD) number of different medications used 13.2 (7.1) 13.4 (7.0) 12.9 (7.2) <0.001
Mean (SD) warfarin cost-sharing, $US 9.06 (8.26) 8.86 (8.12) 9.30 (8.42) 0.001
AMI= acute myocardial infarction; CAD= coronary artery disease; COPD= chronic obstructive pulmonary disease; HCM= hypertrophic cardiomyopathy;
LVH= left ventricular hypertrophy; PVD= peripheral vascular disease; TIA= transient ischemic attack; UTI= urinary tract infection.
Persistence of Warfarin Treatment in AF patients 249
Adis ª 2012 Springer International Publishing AG. All rights reserved. Am J Cardiovasc Drugs 2012; 12 (4)
receiving warfarin therapy at baseline (OR = 1.431; 95% CI
1.337, 1.531 for persistence; OR = 0.585; 95% CI 0.543, 0.630
for discontinuation) were more likely to be persistent and less
likely to discontinue warfarin. In addition, patients in the South
and West regions (compared with North Central), having
baseline cardiac dysrhythmias other than AF (compared with
patients who did not have cardiac dysrhythmias; OR = 0.933;95% CI 0.875, 0.994 for persistence; OR = 1.110; 95% CI 1.035,
1.189 for discontinuation), and higher warfarin cost-sharing
(OR = 0.991; 95% CI 0.987, 0.995 for persistence; OR = 1.009;95% CI 1.005, 1.013) were less likely to be persistent and more
likely to discontinue (p < 0.05 in all cases, table III). A 1-year
increase in age was associated with a lower hazard of becoming
non-persistent (hazard ratio [HR] = 0.996; 95%CI 0.992, 1.000)
and discontinuing warfarin (HR = 0.995; 95% CI 0.991, 0.999).
Persistence and Discontinuation Measures for Long-Term
Medications with Different Dosing Schedules
Discontinuation rates were not significantly different be-
tween carvedilol phosphate od versus carvedilol bid (35.0% vs
32.9%, p = 0.489), and metformin extended release od versus
metformin non-extended release bid (48.9% vs 52.0%, p = 0.375;table IV) during the 1-year follow-up period. Kaplan-Meier
curves for persistence with long-term medications and new
warfarin users are plotted in figure 3. The percentage of patients
who remained persistent decreased over time to approximately
50% at the end of the 1-year follow-up for all medications. By
100 days, 67.9% (metfomin bid) to 80.0% (carvedilol bid) of
patients were still persistent with therapy; by 200 days, 52.8%(metformin bid) to 69.3% (carvedilol phosphate od) were still
persistent. Persistence was consistently higher for carvedilol
ContinuingNew
1.00
0.75
0.50
0.25
0
0 100 200
Kap
lan-
Mei
er s
urvi
val e
stim
ates
Analysis time (days)300 400
Fig. 2. Kaplan-Meier curve on warfarin persistence: new warfarin users vs
continuing warfarin users.
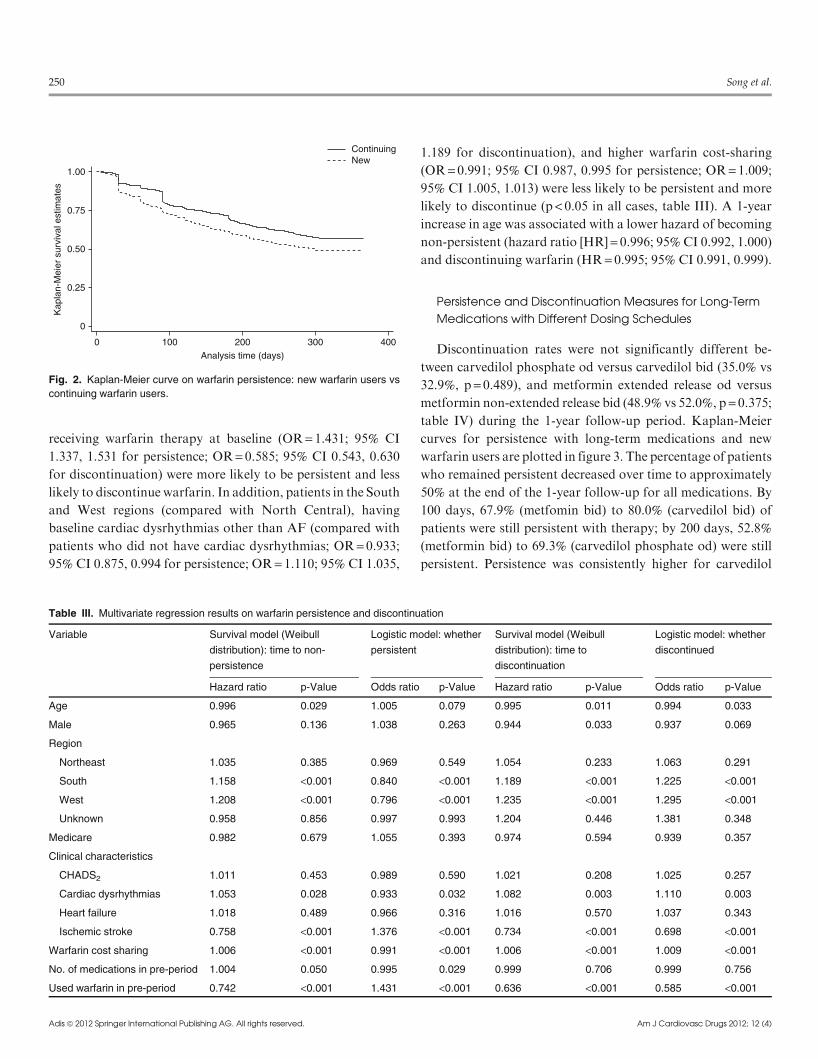
Table III. Multivariate regression results on warfarin persistence and discontinuation
Variable Survival model (Weibull
distribution): time to non-
persistence
Logistic model: whether
persistent
Survival model (Weibull
distribution): time to
discontinuation
Logistic model: whether
discontinued
Hazard ratio p-Value Odds ratio p-Value Hazard ratio p-Value Odds ratio p-Value
Age 0.996 0.029 1.005 0.079 0.995 0.011 0.994 0.033
Male 0.965 0.136 1.038 0.263 0.944 0.033 0.937 0.069
Region
Northeast 1.035 0.385 0.969 0.549 1.054 0.233 1.063 0.291
South 1.158 <0.001 0.840 <0.001 1.189 <0.001 1.225 <0.001
West 1.208 <0.001 0.796 <0.001 1.235 <0.001 1.295 <0.001
Unknown 0.958 0.856 0.997 0.993 1.204 0.446 1.381 0.348
Medicare 0.982 0.679 1.055 0.393 0.974 0.594 0.939 0.357
Clinical characteristics
CHADS2 1.011 0.453 0.989 0.590 1.021 0.208 1.025 0.257
Cardiac dysrhythmias 1.053 0.028 0.933 0.032 1.082 0.003 1.110 0.003
Heart failure 1.018 0.489 0.966 0.316 1.016 0.570 1.037 0.343
Ischemic stroke 0.758 <0.001 1.376 <0.001 0.734 <0.001 0.698 <0.001
Warfarin cost sharing 1.006 <0.001 0.991 <0.001 1.006 <0.001 1.009 <0.001
No. of medications in pre-period 1.004 0.050 0.995 0.029 0.999 0.706 0.999 0.756
Used warfarin in pre-period 0.742 <0.001 1.431 <0.001 0.636 <0.001 0.585 <0.001
250 Song et al.
Adis ª 2012 Springer International Publishing AG. All rights reserved. Am J Cardiovasc Drugs 2012; 12 (4)

and sitagliplin users than for metformin and pioglitazone users,
but there were no clearly different patterns of persistence be-
tween od and bid medications. The impact of dosing schedule
on persistence and discontinuation is presented in table V.
Multivariate regression found no significant relationship be-
tween dosing schedule and persistence or discontinuation.
Discussion
While existing studies report the adherence to guidelines for
AF management and use of oral anticoagulant in the AF pop-
ulation,[10-14] few studies have examined warfarin persistence.[10]
This studywas the first to examinewarfarin persistence aswell as
the impact of dosing schedules on persistence and discontinua-
tionmeasures of commonly prescribed long-termmedications in
the AF population using a large national managed-care claims
database. Although warfarin use requires constant INR mon-
itoring, its persistence rate was found to be similar to medi-
cations that treat hypertension, hyperglycemia, heart disease, or
dyslipidemia, which do not have a similar monitoring require-
ment. About half (53.5%) of warfarin users remained persistent
by the end of a 1-year follow-up period, consistent with other
long-term medications used by AF patients (45.2–61.3%). The
percentage of patients who continued onwarfarin therapy at the
end of 1-year follow-upwas 57.4%, lower than the 70% found by
Gallagher and colleagues[10] for patients with chronic AF and
aged 40 years or older. This difference could be the result of the
Table IV. Persistence and discontinuation of other long-term medications
Variable Carvedilol phosphate
(od) [n =326]Carvedilol (bid)
[n =1786]p-Value Metformin HCl
(ER, od) [n= 305]Metformin HCl
(non-ER, bid) [n= 917]p-Value
Mean SD Mean SD Mean SD Mean SD
Age 72.4 11.6 73.6 11.4 0.095 69.1 12.4 70.8 11.4 0.030
CHADS2 1.56 1.00 1.69 1.10 0.049 1.98 1.07 1.99 1.09 0.820
Cost sharing, $US 29.45 28.31 19.48 15.79 <0.001 10.90 14.43 7.61 6.25 <0.001
Persistence (n, %) 200 61.3% 1074 60.1% 0.684 138 45.2% 428 46.7% 0.649
Discontinuation (n, %) 114 35.0% 588 32.9% 0.489 149 48.9% 422 52.0% 0.375
Days to non-persistence 121 82 122 84 0.756 108 76 109 81 0.651
Days to discontinuation 117 78 113 78 0.604 102 70 101 73 0.983
Variable Pioglitazone HCl
(od) [n =469]Sitagliptin phosphate
(od) [n= 366]p-Value Lisinopril (n= 3030) Valsartan (n = 881) Simvastatin
(n = 2249)
Mean SD Mean SD Mean SD Mean SD Mean SD
Age 71.1 10.8 70.9 10.5 0.858 73.8 11.7 74.5 10.7 73.0 10.9
CHADS2 2.03 1.00 2.04 1.91 0.933 1.73 1.12 1.89 1.08 1.71 1.16
Cost sharing, $US 26.73 24.44 27.77 25.81 0.553 6.66 5.25 23.86 20.53 13.84 15.06
Persistence (n, %) 231 49.3% 209 57.1% 0.025 1462 48.3% 479 54.4% 1,182 52.6%
Discontinuation (n, %) 209 44.6% 130 35.5% 0.012 1386 50.5% 354 44.8% 924 45.0%
Days to non-persistence 111 80 122 84 0.009 107 82 110 81 103 78
Days to discontinuation 102 73 107 74 0.658 98 73 103 74 96 72
bid= twice daily; ER= extended release; HCl =hydrochloride; od = once daily; SD= standard deviation.
Carvedilol phosphate (od)Lisinopril (od)Metformin (od)Simvastatin (od/tid)Valsartan (od/bid)
Carvedilol (bid)Metformin (bid)Pioglitazone (od)Sitagliptin (od)Warfarin new users
Kap
lan-
Mei
er s
urvi
val e
stim
ates 1.00
0.75
0.50
0.25
0
0 100Analysis time (days)
200 300 400
Fig. 3. Kaplan-Meier curve for persistence on selected long-term medi-
cations. bid= twice daily; od= once daily; tid = three times daily.
Persistence of Warfarin Treatment in AF patients 251
Adis ª 2012 Springer International Publishing AG. All rights reserved. Am J Cardiovasc Drugs 2012; 12 (4)

different study populations included in theGallagher et al. study
and our study. All patients in our study hadAF hospitalizations
while their patients did not require AF hospitalization. Their
patients were 40 years or older and we included patients under
the age of 40 years. In addition, the vastmajority of their patients
were 65 years or older (93.7%), compared with only 76.6% of
patients in our study. Both the Gallagher et al. study and our
study found that older patients were more likely to continue on
warfarin therapy.
Although warfarin persistence decreased over time for all
warfarin users, continuing warfarin users consistently had better
persistence than new warfarin users, which was not surprising
as bleeding events tend to occur soon after initiation of warfarin
therapy. Consistent with the literature that older patients gen-
erally have better adherence than younger patients,[7,15] older
patients in our study were also estimated to be more likely to be
persistent and less likely to discontinue therapy. Compared
with patients who had no baseline ischemic stroke, patients
with baseline ischemic stroke were significantly more likely to
be persistent and less likely to discontinue therapy. Living in the
South and West regions, having baseline cardiac dysrhythmias
other than AF, and having higher warfarin cost-sharing sig-
nificantly decreased the likelihood of persistence and increased
the likelihood of discontinuation. Consistent with the exist-
ing literature regarding the impact of patient cost-sharing on
medication adherence,[7,16,17] we found higher cost-sharing
negatively related with warfarin persistence. Also consistent
with published studies, patients on od medications had similar
persistence to patients on bid medications.[18] Age, cost-sharing,
having baseline ischemic stroke or cardiac dysrhythmias were
not significant factors on persistence and discontinuation
measures in od and bid study populations, possibly because the
od versus bid cohorts had very similar characteristics as the
medications in comparison were the same medication with
different dosing schedules. This study did not find appropriate
medications taken three or four times daily with sufficient
sample size thus no comparison was conducted between three-
or four-times-daily medications and od medications.
Costs associated with AF are very high. Coyne and col-
leagues[19] estimated that the annual cost of AF was $6.65
billion in the USA and Kim et al.[20] estimated an incremental
AF-specific cost of $6 billion in the USA. Numerous studies
have shown that non-adherence is associated with higher rates
of complications and increased healthcare utilization (espe-
cially inpatient admissions and emergency room visits) and
costs.[7-9] Understanding the factors that affect persistence and
discontinuation of warfarin and other long-term medication
therapy in the AF population is important as medical plans and
policy makers can develop targeted intervention programs that
help improve persistence and adherence of long-term medi-
cations in this population.
Several limitations related to the use of administrative medi-
cal claims data should be considered when evaluating the
findings. First, because this study was based on claims data,
persistence and discontinuation was measured among patients
who had at least one prescription. Information on those patients
who received a prescription but never filled it is not available. In
addition, we could only look at refill rates, not actualmedication
consumption, which might overestimate persistence and under-
estimate discontinuation. Because our AF study population in-
cluded patients with secondary AF causes, such as urinary tract
infection and pneumonia, non-persistence of warfarin was likely
to be overestimated relative to the primary AF population. In-
cluding AF patients who had no risk factor of stroke but used
warfarin in anticipation of cardioversion or catheter ablation in
the study population could also overestimate non-persistence of
warfarin as these patients would stop using warfarin shortly.
Second, clinical information such as chart review or INR
laboratory values are not available in the claims data, therefore
we could not determine if patients discontinuedwarfarin because
of adverse events (for example, major bleeding), in preparation
for surgery, or other reasons. Further research should in-
corporate clinical data on side effects or INR values to better
understand the reasons for warfarin non-persistence and dis-
continuation. Third, some explanatory variables such as race
and household income were not available. The effects of patient
Table V. Estimated impact of dosing schedule on persistence and discontinuation measures
Hazard model Logistic model Hazard model Logistic model
Time to non-persistence Whether persistent Time to discontinuation Whether discontinued
Hazard ratio p-Value Odds ratio p-Value Hazard ratio p-Value Odds ratio p-Value
Carvedilol phosphate (od) vs carvedilol (bid) 1.065 0.531 0.921 0.524 0.930 0.496 0.910 0.491
Metformin ER (od) vs metformin (bid) 0.990 0.916 1.012 0.931 0.952 0.613 0.940 0.669
bid= twice daily; ER= extended release; od = once daily.
252 Song et al.
Adis ª 2012 Springer International Publishing AG. All rights reserved. Am J Cardiovasc Drugs 2012; 12 (4)

cost-sharing on adherence may be larger when the proportion of
income spent on healthcare is higher. Fourth, this study com-
pared persistence and discontinuation of medications with dif-
ferent dosing schedules. Medications that differ in dosing
schedulesmay differ in other ways (for example, side effects) that
could influence adherence, something not captured in this ana-
lysis. Additionally, long-term medications were included in the
study if there were at least 300 users in ourAFpopulation, which
was a random threshold. More or fewer medications would be
selected into the study if a different threshold on sample size was
used. Finally, because of the continuous enrollment criteria, very
sick AF patients who died within less than 1 year of AF hospi-
talizations were excluded from the study sample. The impact of
this exclusion on persistence and discontinuationmeasures is not
obvious. In addition, the claims data only included patients with
commercial and Medicare supplemental insurance. Thus find-
ings of this study may not be representative of the whole AF
population in the USA.
Conclusion
Persistence and continuationwith warfarin is consistent with
that of other long-term medications among patients with AF.
Higher medication cost-sharing is associated with lower per-
sistence and higher likelihood of discontinuation with warfarin.
Factors associated with non-persistence can be used to identify
patients appropriate for adherence programs.
Acknowledgments
This study was funded by Boehringer Ingelheim Pharmaceuticals, Inc.
One author (Stephen Sander) is an employee of Boehringer Ingelheim
Pharmaceuticals, Inc.
Conference presentation: A poster of the study results was presented at
the International Society of Pharmacoeconomics and Outcome Research
(ISPOR) 15thAnnual InternationalMeeting,May2010,Atlanta,GA,USA.
References1. GoAS,Hylek EM, PhillipsKA, et al. Prevalence of diagnosed atrial fibrillation
in adults: national implications for rhythm management and stroke
prevention: the AnTicoagulation and Risk Factors in Atrial Fibrillation
(ATRIA) Study. JAMA 2001; 285: 2370-5. doi:10.1001
2. Wolf PA, Abbott RD, Kannel WB. Atrial fibrillation as an independent risk
factor for stroke: The Framingham Study. Stroke 1991; 22: 983-8
3. Hart RG, Pearce LA, Aguilar MI. Meta-analysis: antithrombotic therapy to
prevent stroke in patients who have nonvalvular atrial fibrillation. Ann Intern
Med 2007; 146 (12): 857-67
4. Singer DE, Albers GW, Dalen JE, et al. Antithrombotic therapy in atrial fi-
brillation: The Seventh ACCP Conference on Antithrombotic and Throm-
bolytic Therapy. Chest 2004; 126 (3 Suppl.): 429S-6S
5. Fuster V, Ryden LE, Cannom DS, et al. ACC/AHA/ESC 2006 Guidelines for
the management of patients with atrial fibrillation: a report of the American
College of Cardiology/American Heart Association Task Force on Practice
Guidelines and the European Society of Cardiology Committee for Practice
Guidelines (Writing Committee to Revise the 2001 Guidelines for the Man-
agement of Patients With Atrial Fibrillation). Developed in collaboration
with the EuropeanHeart RhythmAssociation and theHeart RhythmSociety.
Circulation 2006; 114 (7): e257-354
6. Lin LJ, ChengMH,Lee CH, et al. Compliancewith antithrombotic prescribing
guidelines for patients with atrial fibrillation: a nationwide descriptive study
in Taiwan. Clin Ther 2008 Sep; 30 (9): 1726-36
7. Gibson TB, Song X, Alemayehu B, et al. Cost-sharing, adherence, and health
outcomes in patients with diabetes. Am J Manag Care. 2010 Aug; 16 (8):
589-600
8. Sokol MC, McGuigan KA, Verbrugge RR, et al. Impact of medication ad-
herence on hospitalization risk and healthcare cost. Med Care 2005; 43 (6):
521-30
9. Ho PM, Rumsfeld JS, Masoudi FA, et al. Effect of medication nonadherence
on hospitalization and mortality among patients with diabetes mellitus. Arch
Intern Med 2006; 166 (17): 1836-41
10. Gallagher AM, Rietbrock S, Plumb J, et al. Initiation and persistence of
warfarin or aspirin in patients with chronic atrial fibrillation in general
practice: do the appropriate patients receive stroke prophylaxis? J Thromb
Haemost 2008; 6 (9): 1500-6
11. Ogilvie IM, Newton N, Welner SA, et al. Underuse of anticoagulant in atrial
fibrillation: a systemic review. Am J Med 2010; 123 (7): 638-45
12. Bottoni N, Tritto M, Ricci R, et al. Adherence to guidelines for atrial fi-
brillation management of patients referred to cardiology departments: Studio
Italiano multicentrico sul Trattamento della Fibrillazione Atriale (SITAF).
Europace 2010; 12 (8): 1070-7
13. Tulner LR, VanCampen JP,Kuper IM, et al. Reasons for undertreatment with
oral anticoagulants in frail geriatric outpatients with atrial fibrillation:
a prospective, descriptive study. Drugs Aging 2010; 27 (1): 39-50
14. Pisters R, de Vos CB, Nieuwlaat R, et al. Use and underuse of oral anti-
coagulation for stroke prevention in atrial fibrillation: old and new para-
digms. Semin Thromb Hemost 2009; 35 (6): 554-9
15. ChernewM, Gibson TB, Yu-Isenberg K, et al. Effects of increased patient cost
sharing on socioeconomic disparities in health care. J Gen Intern Med 2008;
23 (8): 1131-6
16. GoldmanDP, Joyce GF, Zheng Y. Prescription drug cost sharing: associations
with medication and medical utilization and spending and health. JAMA
2007; 298 (1): 61-9
17. Gibson TB, Ozminkowski RJ, Goetzel RZ. The effects of prescription
drug cost sharing: a review of the evidence. Am J Manag Care 2005; 11 (11):
730-40
18. Claxton AJ, Cramer J, Pierce C. A systematic review of the associations be-
tween dose regimens and medication compliance. Clinical Therapy 2001;
23(8): 1296-310
19. Coyne KS, Paramore C, Grandy S, et al. Assessing the direct costs of treating
nonvalvular atrial fibrillation in theUnited States. Value inHealth 2006; 9 (5):
348-56
20. Kim MH, Johnston SS, Chu BC, et al. Estimation of total incremental health
care costs in patients with atrial fibrillation in the United States. Circ Car-
diovasc Qual Outcomes 2011; 4: 313-20
Correspondence: Dr Xue Song, PhD, Truven Health Analytics, 150
Cambridge Park Dr., 2nd Floor, Cambridge, MA 02140, USA.
E-mail: [email protected]
Persistence of Warfarin Treatment in AF patients 253
Adis ª 2012 Springer International Publishing AG. All rights reserved. Am J Cardiovasc Drugs 2012; 12 (4)