Embed Size (px)
Citation preview

Allergy and Immunology for the ABIM Exam
Patricia Stewart, MDAssistant Professor of Medicine and Pediatrics
University of Mississippi Medical [email protected]

I do not have a financial interest/arrangement of affiliation that could be perceived as a real or apparent conflict of interest in the context of the subject of this presentation.
Thank you to Dr. Lindsey McMullan for original slide set, now modified.
Disclosures

Allergy/Immunology 2% ◦ Anaphylaxis◦ Asthma (also listed in Pulmonary)◦ Rhinitis/Sinusitis/Conjunctivitis◦ Food allergy◦ Urticaria and angioedema (also listed in Derm)◦ Skin disorders◦ Drug allergy◦ Primary immunodeficiency◦ Allergic complications of transfusions◦ Autoimmune systemic disorders
ABIM Blueprint*
*As of January 2015

Allergy◦ Rhinitis◦ Asthma◦ Urticaria◦ Angioedema◦ Anaphylaxis◦ Drug Allergy◦ Atopic Derm/Contact Derm◦ Eosinophilic Esophagitis
Immunology◦ Basic overview◦ Complement
deficiencies◦ CVID◦ Selective IgA
deficiency◦ Vaccines:
Indications for withholding live vaccines
Outline

Type I◦ IgE mediated◦ Immediate (anaphylaxis, etc)◦ Symptoms from mast cell degranulation
Type II◦ Antibody (IgG, IgM, some IgA) mediated◦ Cytotoxic◦ Ex: PCN induced autoimmune hemolytic anemia
Type III◦ Immune Complex mediated◦ IgG, IgM, activated complement, neutrophils◦ Ex: Serum Sickness
Type IV◦ Delayed hypersensitivity, T cell mediated◦ Ex: TB skin test, contact dermatitis
Gell-Coombs Hypersensitivity

A 32 y/o F has a history of seasonal allergic rhinitis in the spring which has typically been well controlled however she has noticed persistent, clear, rhinorrhea and nasal congestion for the past 3 months. She has no pets, no mold exposure, and symptoms do not improve with travel. She has no facial or dental pain. Current daily medications include cetirizine, pseudoephedrine, oxymetazoline nasal spray. She is otherwise healthy. Physical exam is remarkable only for slightly edematous, erythematous nasal turbinates with clear nasal drainage.
Which is the most appropriate diagnosis?A: Vasomotor rhinitisB: Chronic rhinosinusitisC: Wegener’s (Granulomatosis with polyangiitis) D: Rhinitis medicamentosa
Question #1

Inflammation of nasal mucosa causing: rhinorrhea, nasal itching, sneezing, congestion, post nasal drainage
Allergic rhinitis◦ Seasonal or perennial (or both)◦ Can confirm with skin test or in-vitro specific IgE
antibody assay ◦ Rx:
environmental control First line med: Intranasal steroids Second line meds: PO antihistamines, Leukotriene
receptor antagonists Allergy immunotherapy (shots or dissolvable tablets)
Rhinitis

URI related rhinitis◦ Do not select antibiotics
Non-allergic Rhinitis ◦ Other names:
Vasomotor: reaction to neurogenic/vagal stimuli NARES (non allergic rhinitis with eosinophilia
syndrome)◦ Negative allergy testing◦ Rx: Again, Intranasal steroids

Rhinitis medicamentosa◦ Refractory congestion due to chronic use of
topical nasal decongestants ◦ Rx: withdraw the nasal decongestant
Other etiologies:◦ Mechanical obstruction (septal deviation, polyps)◦ Sinusitis◦ Wegener’s
Key words: systemic illness, ulcerations◦ Cystic fibrosis
Key words: young, malnourished, polyps, chronic sinusitis, infertility, chronic/recurrent bronchitis
◦ Medications: propranolol, alpha-methyldopa◦ CSF leak
Key words: Unilateral Dx: check beta-2 transferrin

Rhinitis with Nasal Polyps◦ Tip off- anosmia◦ Immunodeficiency◦ Cystic fibrosis◦ Aspirin Exacerbated Respiratory Disease (Aspirin
Sensitive Asthma)◦ Allergic Fungal Sinusitis
Key Words: hyper-attenuation on CT scan
Pregnancy Rhinitis◦ Congestion and rhinitis limited to pregnancy

Testing◦ Spirometry◦ Methacholine Challenge
Classify based on risk and severity◦ Most severe characteristic
Start treatment at appropriate levels◦ preferred vs alternative therapies
Asthma

A 35 y/o Female comes in for evaluation of wheezing, shortness of breath, and chest tightness. She has taken no medication for these symptoms which occur approximately 3 times weekly for the past month without nocturnal awakenings. She has a history of childhood asthma, but until now has had no asthma or allergy symptoms. Spirometry performed in your office shows an FEV1 of 90% predicted and FEV1/FVC ratio of 85. Physical exam is unremarkable.
Which of the following is the next best option?A: order bronchial challenge testingB: start inhaled budesonide twice dailyC: set her up for allergy testingD: Start inhaled corticosteroid/long acting albuterol
combination therapy
Question #2

Suggestive symptoms in conjunction with testing
Spirometry/PFTs◦ Decreased FEV1/FVC ratio◦ Response to beta-agonist
FEV1 improvement of 12% AND 200 mL
◦ Normal Spirometry does not rule out asthma
Asthma Diagnosis
1. National Asthma Education and Prevention Program Expert Panel Report 3 (NAEPP EPR3); http://www.nhlbi.nih.gov/files/docs/guidelines/asthgdln.pdf
2. Interpretative strategies for lung function tests. Pellegrino R, Viegi G, Brusasco V, et. Al. Eur Respir J. 2005 Nov;26(5):948-68.

Normal
Non-reversible
Reversible

◦ Does NOT diagnose asthma
◦ DOES indicate airway hyper-responsiveness (AHR) Perform when symptomatic
◦ NPV is good- if negative- rules OUT asthma
◦ Positive is 20% decrease in FEV1
Methacholine Challenge

A 45 y/o M with a long standing history of asthma and allergies to dust mites comes in for evaluation. Despite therapy with ICS/LABA combination with appropriate technique, appropriate environmental control, and a recently completed course of immunotherapy, he continues to require his short acting albuterol 3 times a week. He is not a smoker. He has required 4 courses of oral steroids in the past year. Today physical is notable only for occasional expiratory wheeze, and FEV1 of 70% with normal inspiratory loop. Review of previous lab work is notable for IgE of 200 IU/mL, absolute eosinophil count of 230, positive specific IgE to dust mites, and a normal chest x-ray.
The next most appropriate treatment is?A: omalizumabB: repeat allergy immunotherapyC: long acting inhaled anticholinergic D: Have him evaluated for vocal cord dysfunction
Question #3

Classify Asthma Appropriately
From National Asthma Education and Prevention Program. Expert Panel Report 3: guidelines for the diagnosis and management of asthma. Bethesda, Md.:NIH/National Heart, Lung, and Blood Institute; 2007. http://www.nhlbi.nih.gov/health-pro/guidelines/current/asthma-guidelines/full-report

Step up/down
Assess Asthma Control
From National Asthma Education and Prevention Program. Expert Panel Report 3: guidelines for the diagnosis and management of asthma. Bethesda, Md.:NIH/National Heart, Lung, and Blood Institute; 2007. http://www.nhlbi.nih.gov/health-pro/guidelines/current/asthma-guidelines/full-report

Start Appropriate Asthma Therapy
From National Asthma Education and Prevention Program. Expert Panel Report 3: guidelines for the diagnosis and management of asthma. Bethesda, Md.:NIH/National Heart, Lung, and Blood Institute; 2007. http://www.nhlbi.nih.gov/health-pro/guidelines/current/asthma-guidelines/full-report

Rescue Medications◦ Short acting beta-agonists (SABA)
Controller Medications◦ Inhaled Corticosteroids (ICS)◦ Long acting Beta Agonists (LABA)
Black Box (BB) Warning- in asthma, do not give alone◦ Leukotriene Receptor antagonists (LTRA)◦ ICS/LABA combinations
Asthma Medications

◦ Omalizumab- anti-IgE Black Box warning (anaphylaxis) Dosing- based on IgE and weight
◦ Others: Oral Steroids Theophylline (know drug interactions ex: levels
increase with fluoroquinolones, macrolides, st john’s wort, amiodarone, diltiazem, cimetidine and levels decrease with rifampin, phenytoin, phenobarb, cannabis, carbamazepime)

A 50 y/o M with a long history of asthma treated in a different state comes to establish care with you. He requires his albuterol multiple times daily despite being on an ICS/LABA combo and leukotriene modifier with excellent compliance. He only gets slight relief. He has never smoked and has no other medical problems. He states that the last 2 months of living in his new house with no carpets, pets, or mold exposure and a Hepa Filter are the best his asthma has ever been. Review of previous records indicates an IgE of 150 IU/mL, normal chest x-ray, and allergic sensitization to cats and dogs. Physical exam is remarkable only for occasional expiratory wheeze. Spirometry is significant for FEV1 of 70%, FEV1/FVC of 72%. FEV1 improves 20% after nebulized albuterol and he notices tremendous benefit.
Which is the most appropriate treatment?A: Double the dose of his inhaled steroidsB: start OmalizumabC: Assess inhaler techniqueD: Add daily prednisone
Question #4

A 25 y/o F has had worsening of her asthma after being well controlled on a medium dose inhaled steroid. She now uses short acting albuterol for wheezing 3-4 times a week but has not noticed increased rhinitis, post nasal drip, heartburn, or fever. She demonstrates appropriate inhaler technique. Physical exam is notable only for soft end-expiratory wheezes in all lung fields.
Which is the most appropriate treatment?A: Add short acting anticholinergicB: Give penicillin antibioticsC: Add long acting albuterolD: Double dose of inhaled steroids
Question #5

Consider◦ GERD◦ Sinusitis◦ Compliance/technique◦ Alternative diagnosis
Out of control asthmatic

Exercise induced asthma- symptoms with exercise only◦ During or after exercise
Peaks 5-10 minutes after stopping activity, resolve < 30 min
◦ Screen with exercise testing: 15% reduction FEV1
◦ Rx: Pretreat with SABA 10-15 min before exercise Cough Variant Asthma
◦ Cough is predominant or only symptom◦ Distinguish from other causes of chronic cough (rhinitis,
GERD, etc) Occupational Asthma
◦ Symptoms at work◦ Significant improvement on weekends, vacations
Asthma Variants

A 44 y/o F is seen for worsening of asthma. She was previously controlled on ICS/LABA combo, with short acting albuterol. She is now having daily wheezing, dyspnea, and a productive cough. Other than a history of seasonal allergies which are controlled, she is healthy. Inhaler technique is good. PE is remarkable only for expiratory wheezing in all lung fields. Lab evaluation is notable for 13% eosinophils, IgE of 1200 ng/mL, and CXR with patchy upper lobe infiltrate and increased bronchial markings. CT chest reveals mucous plugging and central bronchiectasis.
Which is the next most appropriate diagnostic step?A: Bronchoscopy with BAL and biopsyB: aspergillus IgE testingC: Sweat chlorideD: Sputum gram stain and culture
Question #6

A 47 y/o M with h/o asthma and allergies comes for f/u due to increase in nonproductive cough. He has also noticed a paresthesia in his left leg and decreased grip in his right hand. Physical is notable for BP of 150/100, scattered expiratory rhonchi on lung exam, and decreased strength in R hand and L foot. Your CBC is remarkable for 32% eosinophilia
What is the next best test to establish the diagnosis?A: ANCA testingB: CXRC: full PFTsD: MRI brain
Question #7

A 24 y/o F is seen in the urgent care clinic for sudden onset of asthma exacerbation. She has a history of sudden exacerbations requiring unscheduled visits, but between exacerbations, pulmonary function testing and physical are unremarkable. She takes inhaled fluticasone and short acting albuterol. Physical is remarkable for audible wheezing on both inspiration and expiration. Wheezing is heard only in central lung fields. She is mildly tachycardic, but physical exam is otherwise unremarkable. She does not respond to nebulized albuterol and ipratropium x 3 or IV corticosteroids and continues to wheeze. O2 sat is 98% on room air.
Part 1: What is the next most appropriate step? A: CXRB: IV magnesiumC: IM corticosteroidsD: laryngoscopy
Question #8 part 1

A 24 y/o F is seen in the urgent care clinic for sudden onset of asthma exacerbation. She has a history of sudden exacerbations requiring unscheduled visits, but between exacerbations, pulmonary function testing and physical are unremarkable. She takes inhaled fluticasone and short acting albuterol. Physical is remarkable for audible wheezing on both inspiration and expiration. Wheezing is heard only in central lung fields. She is mildly tachycardic, but physical exam is otherwise unremarkable. She does not respond to nebulized albuterol and ipratropium x 3 or IV corticosteroids and continues to wheeze. O2 sat is 98% on room air.
Part 2: What is the most appropriate addition to her routine therapy?A: Addition of long acting albuterolB: daily corticosteroidsC: Speech therapyD: omalizumab
Question #8 part 2

Everything that wheezes is not asthma◦ Heart failure, COPD, upper airway obstruction, others
ABPA/ABPM (allergic bronchopulmonary aspergillosis (mycosis))◦ Dx:
Asthma or Cystic Fibrosis Elevated IgE
Asthmatic: > 1000 ng/mL or 417 IU/L Positive IgE test to A. fumigatus, other molds Positive Aspergillus IgG Immediate skin test reactivity to A. fumigatus, other molds Eosinophilia Radiographic pulmonary findings
Opacities on CXR Bronchiectasis on HRCT
◦ Rx: oral steroids, follow IgE
Asthma DDx
For further reading if needed: Greenberger PA et. al. Allergic Bronchopulmonary Aspergillosis. J Allergy Clin Immunol Pract. 2014: 2(6):703-708.

Churg Strauss◦ Now called Eosinophilic granulomatosis with
polyangiitis◦ Sinusitis, asthma, eosinophilia, vasculitis◦ Transient pulmonary infiltrates◦ Small vessel vasculitis◦ Neuropathies (mononeuritis multiplex)◦ MPO/P-ANCA◦ Rx: oral steroids +/- cyclophosphamide

VCD (vocal cord dysfunction)◦ Female 2:1◦ Athletes◦ Bronchodilator non-responsive◦ Mimics asthma, recurrent wheezing (may also
have stridor)◦ Difficulty getting breath IN (Asthma- expiration)◦ Can occur with or without asthma◦ Flattening of inspiratory curve on spirometry◦ If symptomatic: laryngoscopy◦ Rx: Speech therapy, behavior modification,
patient education

A 35 y/o Female comes in for evaluation of wheezing, shortness of breath, and chest tightness. She has taken no medication for these symptoms which occur approximately 3 times weekly for the past month without nocturnal awakenings. She is 18 weeks pregnant. She has a history of childhood asthma, but until now has had no asthma or allergy symptoms. Spirometry performed in your office shows an FEV1 of 90% predicted and FEV1/FVC ratio of 85. Physical exam is unremarkable.
Which of the following is the next best option?A: order bronchial challenge testingB: start inhaled budesonide twice dailyC: set her up for allergy testingD: Start inhaled corticosteroid/long acting albuterol
combination therapy
Question #9

Step up therapy indications similar for non-pregnant◦ Safer to be exposed to medications with limited data (ex:
LABA, SABA) than have ongoing symptoms and exacerbations
Class B: ◦ PO: cetirizine, loratadine, montelukast◦ intranasal: budesonide◦ Inhaled: budesonide◦ Injectable: Omalizumab (anti-IgE) but be aware of BB
warning for anaphylaxis Do NOT pick skin prick testing, start allergy
immunotherapy, or perform bronchial challenge in the pregnant patient
Asthma in Pregnancy

A 32 y/o F is in the urgent care clinic with widespread pruritic wheals, each lasting 2-4 hours. This is the 3rd day she has had this rash. She does not have any other symptoms and does not have swelling. Diphenhydramine has minimally helped the itching, but is making her very sleepy. She takes no other medications and is otherwise healthy. Physical exam is remarkable only for scattered edematous, indurated wheals to her face, trunk, upper and lower extremities b/l. She also has marked dermatographism.
What is the next best step in management?A: skin biopsyB: admission to the hospitalC: start her on cetirizine and ranitidineD: treat with high potency topical steroid
Question #10

A 52 y/o F is being evaluated for a 1 month history of daily wheals which are pruritic, but also have a burning quality. Each lesion persists around 48 hours. After resolution, some lesions are leaving a bruise. They occur on all extremities and her trunk, but are the worst on her lower extremities. The only other associated signs are some pain in her hands and her feet that she has attributed to the extremely cold weather, and a recent slight discoloration in her urine.
What is the next best step in management?A: Skin biopsyB: admission to the hospitalC: check thyroid antibodiesD: treat with high potency topical steroid
Question #11

Classification:◦ Acute urticaria (< 6 weeks)◦ Chronic urticaria (> 6 weeks)◦ Physical urticaria (pressure, cold, vibratory,
cholinergic, etc)◦ Urticarial Vasculitis◦ Contact urticaria ◦ Urticaria and angioedema as components of
anaphylaxis
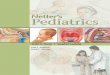
Urticaria

Attribution: By James Heilman, MD http://creativecommons.org/licenses/by-sa/3.0) via Wikimedia Commonshttp://commons.wikimedia.org/wiki/File:Hives2010.JPGImage not altered

Urticaria Diagnosis Points◦ Hallmark: rapid appearance of pruritic wheals
which disappear within 24 hours Lesions lasting >24 hours or palpable purpura raise
concerns for urticarial vasculitis or other underlying disease- Perform Biopsy Can also check CBC , ESR/CRP, complement levels, Hep
B/C, cryoglobulins, SPEP
◦ DO NOT work up for or diagnose HAE if the patient has urticaria. HAE patients do not have hives

Treatment ◦ Acute urticaria: remove inciting source (food,
drug, etc)◦ Chronic urticaria:
Rx: H1 +/- H2 blocker Do NOT pick oral or systemic steroids- only indicated
in VERY symptomatic patients with urticaria in short term
NEW: Omalizumab was approved by the FDA for chronic idiopathic urticaria resistant to antihistamines in 2014. Dosing is either 150 mg SC qmonth or 300 mg SC qmonth. NOT dependent on IgE levels or weight (different from dosing for asthma)

Classification Characteristics
Cholinergic urticaria
Occurs in response to an increase in core body temperature; lesions present as small papules with a prominent surrounding erythematous flare
Dermatographism
Rapidly induced by pressure
Delayed pressure-induced urticaria
Patients often experience systemic symptomsSwelling and burning of palms and soles may occur
Exercise-induced urticaria
On a continuum with exercise-induced anaphylaxis; many patients only develop symptoms if primed by an ingested allergen prior to exercise
Solar urticaria Mast cell activation in certain wavelengths of light
Acquired Cold urticaria
Mediated by IgE or cryoglobulinCould be related to underlying infectionRisk of shock with immersion in cold waterTest with 5 minute ice cube challenge
Familial Cold urticaria
Not actually have degranulation of mast cellsAssociated fevers, chills, myalgiasAutoinflammatory syndrome
Physical Urticarias

A 25 y/o F is being seen in the ED for mild laryngeal angioedema, lip and tongue swelling, and severe abdominal cramping. She tells you that as a child, she didn’t like to ride bikes due to genital swelling afterward, and over the past several months she has had unexplained, recurrent severe abdominal cramping despite extensive, unrevealing lab work up and various medications which have not helped. This is the first time she has had any type of upper airway symptoms. She is an only child; her maternal uncle and her cousin have similar symptoms. Physical exam is remarkable for obvious angioedema of both lips, a mildly enlarged tongue. Abdomen is not distended and only mildly TTP. Vitals are normal, she speaks easily in complete sentences, and O2 sat is 100% on room air. ENT is on the way to evaluate the degree of laryngeal edema.
Part #1: Which of the following will best establish the diagnosis
A: ex-lapB: extensive allergy testing to foodsC: SPEP and UPEPD: C4 and C1 esterase inhibitor function
Question #12 Part 1

A 25 y/o F is being seen in the ED for mild laryngeal angioedema, lip and tongue swelling, and severe abdominal cramping. She tells you that as a child, she didn’t like to ride bikes due to genital swelling afterward, and over the past several months she has had unexplained, recurrent severe abdominal cramping despite extensive, unrevealing lab work up and various medications which have not helped. This is the first time she has had any type of upper airway symptoms. She is an only child; her maternal uncle and her cousin have similar symptoms. Physical exam is remarkable for obvious angioedema of both lips, a mildly enlarged tongue. Abdomen is not distended and only mildly TTP. Vitals are normal, she speaks easily in complete sentences, and O2 sat is 100% on room air. ENT is on the way to evaluate the degree of laryngeal edema.
Part #2: Which of the following would be the most appropriate treatment to give this patient in the emergency room?
A: Epinephrine 1:1000, 0.3 mg IMB: Epinephrine 1:10,0000 IV dripC: high dose glucocorticoidsD: C1 esterase inhibitor
Question #12 Part 2

Sudden, temporary edema of localized area (ie lips, face, genitals, hands, feet)
Abdominal pain may indicate bowel wall edema If there is urticarial, it is NOT HAE ACE Inhibitors- typically face/lip/tongue- can be
> 6 months after drug initiation◦ Rx: stop ACE-I
Treatment for non-HAE angioedema◦ If airway compromise or hypotension:
Epinephrine, epinephrine, epinephrine- 1st line Could then add antihistamines, corticosteroids
◦ No airway compromise or hemodynamic instability: Antihistamines, corticosteroids
Angioedema

Angioedema WITHOUT urticarial May have abdominal pain that is recurrent and
unexplained Type 1,2- autosomal dominant No hives, no itch Triggers can include:
◦ Trauma, dental visit, surgery, menses, puberty Treat acute attacks with:
◦ C1-esterase inhibitor concentrate◦ ecallantide (plasma kallikrein inhibitor)◦ icatibant (Bradykinin B2 receptor antagonist)◦ !!Epinephrine is NOT effective!!
Hereditary Angioedema

Type 1 Type 2 Acquired HAE with normal C1 INH
C1 esterase level
Low Normal Low Normal
C1 esterase function
Low Low Low Normal
C1q Normal Normal Low Normal
C4 Low Low Low Normal
Other info
Inherited Inherited Associated with lympho-proliferative disorders
No family history
• Autosomal dominant• Females more likely • Tends to present after
puberty• Attacks may be fewer and
less frequent with more facial and less abdominal/multiorgan involvement
• Triggers also include increased estrogen states

Question #13 A 28 y/o M is seen in the ED for shortness of breath after a
bee sting to his arm 15 minutes ago. He also feels nauseated, and his lips are starting to feel puffy. Physical is notable for BP of 100/60, PR 100, RR 22, T 98.6. He is agitated, lip is noticeably swollen, and wheezing is heard in all lung fields. There is no evidence of laryngeal swelling and no rash.
Which of the following is the most appropriate therapy?A: IV diphenhydramine and IV methylprednisoloneB: IV epinephrine, IV methylprednisolone, IM diphenhydramineC: IM epinephrine, inhaled albuterolD: inhaled albuterol, IV fluids, IV diphenhydramine and reassurance

Life-threatening reaction◦ IgE Dependent
Common Causes: Food (peanut/nut, shellfish etc.) Medications (PCN, NSAID) Insect Stings (hymenoptera or fire ant bites) Latex
◦ Non-IgE Dependent Common Cause:
Radiocontrast media
Anaphylaxis

Timing:◦ 30 min- 2 hours after injected substance◦ Can progress and get worse or be biphasic
Rx: EPINEPHRINE 0.3 mg of 1:1000 given IM in vastus lateralis ◦ Add ins: albuterol for bronchospasm, IV fluids for
hypotension, steroids for late phase response, antihistamines for cutaneous symptom relief
◦ Standard life support (oxygen, airway assessment, arrhythmia intervention, etc.)
◦ If on beta-blocker and refractory to epinephrine- give glucagon
◦ Clinical Pearl: Lay them Down. (sitting up associated with fatal anaphylaxis)

Other Points:◦ Elevated tryptase (within first several hours) can
confirm◦ Patients should be discharged with autoinjectable
epinephrine◦ Anaphylaxis from insect sting needs evaluation
for possible venom immunotherapy◦ No obvious trigger- consider mastocytosis (check
tryptase at baseline) or idiopathic anaphylaxis

Cutaneous mastocytosis◦ Urticaria pigmentosa: macule which forms wheal
with gentle stroking (Darier’s sign)◦ Indolent, benign course
Systemic mastocytosis◦ Increased mast cells in tissues
Multi-organ complaints (flushing, GI complaints, etc.◦ Consider if severe anaphylaxis from insect sting◦ Dx: baseline tryptase elevated is indicative
Mastocytosis

A 55 y/o F is being evaluated for an itchy rash that she has had for 3 days. She also feels like her face is puffy. Her only medication is an anticonvulsant that she takes for epilepsy. This medication was changed 3 weeks ago. Physical is notable for T: 101.3, PR: 103, BP: 135/80, RR: 14, face is slightly edematous, she has mild generalized erythema with papules coalescing into plaques on her trunk and extremities diffusely. There are no lesions on her mucosal surfaces. Tender lymph nodes are palpated in the cervical, axillary, and inguinal regions. Laboratory is remarkable for 13% eosinophilia on CBC, and ALT of 328 u/L, and AST of 362 u/L.
Which of the following is the most likely diagnosis?A: Toxic epidermal necrolysisB: IgE mediated drug reactionC: Drug reaction with eosinophilia and systemic symptoms D: acute viral infection
Question #14

A 43 y/o F is evaluated after sustaining a dog bite to her calf 2 days ago. The wound is tender, red, and warm. She is up to date on her tetanus vaccination, and the dog is determined to not have rabies. She has an anaphylactic response to penicillins. Physical exam is notable for Temperature of 102.6, necrotic appearing wound with significant warmth, erythema, and tenderness to touch to the left calf. There is no inguinal lymphadenopathy.
Which of the following is the most appropriate treatment? A: ampicillin-clavulanateB: azithromycinC: clindamycinD: ciprofloxacin plus clindamycin
Question #15

Drug Allergy

Drug Mediated Skin Eruption
Description/Other info
Common Culprits
Maculopapular and morbilliform (small discrete papules)
Most common type.
Distribution: symmetric, truncal rarely on palms or soles
Associated: fever and pruritus
Onset: 8-10 days after initiation
AntibioticsdiureticsMany others
Urticarial Second most common type- with or without angioedema
Onset: a few days after initiation
Antibiotics, contrastMost could cause

Drug Mediated Skin Eruption
Description/Other info
Common Culprits
Erythema multiforme, SJS, TEN
Spectrum: target lesions (EM)
involvement of mucous membranes with systemic symptoms (SJS)
life-threatening loss of epidermis (TEN)
SJS: 10% body involvement TEN: at least 30% body involvement
Nikolsky’s sign may be present, may send biopsy
EM: herpes and mycoplasma pneumoniae as causes, less often a medication
SJS/TEN: Anticonvulsants, sulfonamides, beta-lactams, NSAIDs, sertraline, pantoprazole, tramadol, allopurinol
HLA can be important for some (Abacavir, carbamazepime)

Drug Mediated Skin Eruption
Description/Other info
Common Culprits
Fixed Drug Eruption Discrete, often round or oval lesions that recur in exactly the same spot when re-challenged with the drug
Antibiotics, antifungals, NSAIDs, acetaminophen, anticonvulsants, barbituates
Red Man Syndrome Body flushing, hypotension, muscle pain
- From histamine release, not IgE mediated allergy
Vancomycin, ciprofloxacin
AGEP (acute generalized exanthematous pustulosis)
Widespread erythema with small pustules sometimes with fever, leukocytosis, occasionally eosinophila
Antibiotics, antimalarials, terbinafine, diltiazem

Drug Mediated Skin Eruption
Description/Other info
Common Culprits
DRESS (Drug reaction with eosinophilia and systemic symptoms)
and
Drug Induced Hypersensitivity Syndrome (DISH)
Overlapping symptoms, may be a continuum or same thing
Facial edema, erythema, fever, lymphadenopathy, in DRESS- eosinophilia, can have hepatitis and nephritis. Can notice purpura, blistering, skin pain, skin necrosis, chills, lethargy
Onset: within 12 weeks of initiationMay persist for weeks
Anticonvulsants

Drug Mediated Skin Eruption
Description/Other info
Common Culprits
Photosensitive skin reaction
Phototoxic: severe sunburn after drug exposure (tetracycline)
Photoallergic: rash after days or months of use (sulfonamides)
Onset: any time
Diuretics, tetracycline, amiodarone, fluoroquinolones, sulfonamides, psoralens, phenothiazines

Medication Common Reactions Skin Testing Available?
Rx (other than avoid)
Radiocontrast
Non-IgE mast cell degranulation
No Low osmolar agent and pre-treat
Vancomycin Red Man No Slow infusion and pre-treat
ASA, NSAIDs Several types both IgE mediated and non-IgE mediated
No Avoidance
Penicillins IgE mediated or delayed reactions (immune complex, morbilliform, etc)
Yes for IgE only: skin test, do not pick RAST/ELISA
IgE mediated only: Desensitize if must have (ie pregnant with syphilis)
Other types- only avoidance

Question #16 A 53 y/o F has a pruritic rash on both hands. She works
as a hair stylist and notices the rash improves when she goes on vacations. Topical corticosteroids are helpful, but the rash returns quickly when she stops them. Physical exam is remarkable for erythematous, scaling patches to her fingers, wrists, and the dorsum of both hands.
Which of the following is the next most appropriate step in diagnosis?
A: Skin prick testing to dust mitesB: Patch testingC: KOH preparationD: skin biopsy

Flexural surfaces Intermittent flares Etiology multifactorial
◦ Includes genetics, environment (ex: allergens), immune system (ex: filaggrin mutations)
Differential Diagnosis◦ Allergic contact dermatitis, Irritant dermatitis,
Cutaneous T cell lymphoma Treatment:
◦ Moisturization ◦ Topical Steroids PRN during flares◦ Topical calcineurin ◦ Treat infection if needed
Atopic Dermatitis

Can be difficult to distinguish irritant vs allergic
Allergic (ACD)- Type IV sensitivity reaction (delayed)◦ Look for erythema, edema, vesicles, bullae◦ Dx ACD: Patch Test◦ Rx: avoidance of triggers, topical steroids
Contact Dermatitis

Allergen Common Route of Patient Exposure
Nickel sulfate Jewelry
Neomycin Topical antibiotics
Balsam of Peru (marker for fragrance allergy)
Cologne or perfume
Fragrance mix Most personal care products; products labeled “unscented” may contain masking fragrances
Thimerosal (frequently positive, but rarely relevant)
Eye-care products (eye drops, contact lens solutions); preservative in some vaccines
Sodium gold thiosulfate Jewelry; dental work
Quaternium-15 (formaldehyde-releasing preservative)
Personal care products
Formaldehyde Personal care products
Bacitracin Topical antibiotic; may cross-react with neomycin
Cobalt chloride Blue paint; vitamin B12 (cyanocobalamin); may cross-react with other metals, including nickel

A 45 y/o man is evaluated for a 5-year history of solid-food dysphagia. Solid foods such as meats and breads tend to stick at the mid-esophagus. His symptoms have been progressively increasing. He has occasional heartburn but no weight loss or trouble swallowing liquids. He has been seen in the ER for food impaction. He takes no medications. Physical examination is normal. Endoscopy reveals rings and furrows in the esophagus, and mid-esophageal biopsies show 16 eosinophils/hpf.
Which of the following is the most appropriate next step in his management?
A: Initiate swallowed aerosolized corticosteroidsB: Food allergy testingC: Esophageal DilationD: Initiate PPI
Question #17

General presentation in adults is food impaction and solid-food dysphagia
Dx: EGD with biopsy, >15 eosinophils per HPF and exclude GERD (PPI trial, other)◦ Other findings on EGD: rings, longitudinal furrows,
sometimes strictures (not pathognomonic) Rx: swallowed aerosolized corticosteroids
Eosinophilic Esophagitis

Immunology

Innate Immune System Responds quickly, but not specifically
Adaptive Immune System Respond specifically but more slowly
Humoral Cell-mediated
HLA determines self vs non-self◦ Class I HLA: HLA-A, B, C◦ Class II HLA: HLA- DP, DQ, DR
Components

3 pathways◦ Classical Pathways:
C1, C2, C4, C3-C9 Screen with CH50 (checks all components C1-C9)
◦ Alternative Pathway: Factor B, Factor D, Properdin, C3-C9
◦ Lectin Pathway: Mannose-binding lectin, MASP1, MASP2, C3-C9
C5-9 combine to form membrane attack complex (MAC)- they are the common terminal pathway
Complement System

IgG: main Ig in serum, major Ig in immune response Part of a memory response Passes through placenta, activates complement 4 subtypes: IgG1, IgG2, IgG3, IgG4
IgA: Works primarily in mucosal tissues Secreted in breast milk 2 subtypes: IgA1, IgA2
IgM: First Ig type produced in an infection Activates complement
IgE: Lowest concentration in serum Involved in allergic disease
Immunoglobulins (Ig)

A 19 y/o college sophomore is following up with you after hospitalization 2 weeks ago for meningococcal meningitis. HIV antibody was negative. He had an episode of meningococcal meningitis last year after starting school when an outbreak went through his dorm. He received the meningococcal vaccination when he was 15 y/o. He is otherwise healthy, and takes no medications. He is currently living in a dorm. Physical exam today is unremarkable.
Which of the following is most likely to establish a diagnosis?A: CH50 (total hemolytic complement level)B: IgG and meningococcal titersC: CD4 countD: IgG, IgM, IgA
Question #18

HAE◦ AD, C1-inhibitor
C1, C2, C4 deficiencies◦ Recurrent sinopulmonary infections◦ Encapsulated bacteria◦ Some have increased incidence in rheumatoid
disease (SLE) C3 deficiency
◦ Severe pyogenic infections
Complement deficiencies

Terminal complement deficiency (C5-9)◦ Recurrent Neisseria infections (menigococcal or
gonococcal) Look for recurrent meningitis or septicemia
◦ Dx: Start by checking CH50 (total complement)◦ Rx: Varies based on deficiency. Consideration for
vaccinating frequently (ex: meningococcal vaccine q3 years for terminal complement deficiency) and prophylactic antibiotics

A 21 y/o college student is following up with you after hospitalization for pneumonia 6 weeks ago. She had one other episode of pneumonia 2 years ago. She has asthma, and received both the pneumococcal vaccine and tetanus vaccine just before she started college her freshman year. She tells you that she gets 3-4 sinus infections every year, had an episode of giardiasis as a freshman, and her older brother has lymphoma. Physical exam is unremarkable. Review of her hospital chart indicates that HIV antibody is negative.
Which of the following is the next best step in establishing the diagnosis?
A: CD4 countB: IgA, IgG, IgM levelsC: delayed hypersensitivity testing to tetanusD: CH50 (total hemolytic complement)
Question #19

An 18 y/o F comes to see you for evaluation. She was in an MVC and required blood transfusion in the emergency room to which she anaphylaxed. She has a history of well controlled asthma, peanut anaphylaxis, and allergic rhinitis to tree pollen. She gets otitis media about once a year despite tympanostomy tubes, and is treated for sinusitis 2-3 times yearly. She is otherwise healthy. Physical exam is unremarkable on today’s visit.
Which of the following is the most likely diagnosis?
A: CVIDB: contamination of tubing with peanut productC: selective IgA deficiencyD: terminal complement deficiency
Question #20

Most common PID presenting in adult life◦ Hypogammaglobulinemia AND inability to make
antibodies◦ Recurrent bacterial infections ◦ GI manifestations include giardia, chronic diarrhea,
malabsorption◦ Some with autoimmune problems◦ Some with granulomatous manifestations (noncaseating)◦ Increased risk for lymphomas
Dx: Check IgG, IgA, IgM and titers to pneumococcal and tetanus vaccinations
Rx: immunoglobulin replacement therapy (IVIg or SCIg)
Common Variable Immunodeficiency (CVID)

Most common immunodeficiency Low IgA only Most are asymptomatic If symptomatic- usually respiratory
infections (upper/lower), otitis May have autoantibodies to IgA- can
anaphylax to transfusion (wash blood first) WATCH OUT: Do NOT give immunoglobulin
replacement therapy
Selective IgA Deficiency

http://www.cdc.gov/vaccines/ Contraindicated for ALL vaccines: prior
serious allergic reaction to the vaccine or any component of the vaccine
Live vaccines◦ Withhold in pregnancy ◦ Generally withhold in immunodeficiency
(particularly cell-mediated) Some exceptions HIV with CD4 > 200 may be able to receive these
vaccines
Vaccinations

Vaccine Important Points
Indications Do Not Give to
Varicella Live- 2 doses
Childhood vaccine13 y/o and older- 2 doses 28 days apart if never had vaccine or chickenpox
Pregnant women (should not get pregnant x 1 month)- Caution in immunocompromised
Herpes Zoster
Live >= 60 y/o regardless of zoster history
Do not give in immunocompromised
HPV Not live- 3 doses
Bivalent- females onlyQuadrivalent- males or femalesApproved 9-26Start at 11,12Catch up 13- 26 F13-21 M (permitted to 26)
Not recommended in pregnancy
Ok to give if already HPV+

Vaccine Important Points
Indications Do Not Give to
MMR Live Childhood vaccineGive dose to young adult if cannot document immunity/immunization
Immunocompromisedpregnancy
Meningococcal
Not live
1 > 16 y/o
Booster if < 16
Adolescents, Students in dorms, military: 1 doseAsplenia, HIV, Complement deficiency- 2 dosesBooster q5 years for asplenia, complement deficiency
Pregnancy- only give if really needed
Hep B Not live
3 doses
ChildhoodAdults-at risk of either exposure or morbidity, travel, if they desire
Hep A Not live
2 doses
ChildhoodAdults: MSM, IVD users, travel endemic area, chronic liver disease (not Hep B/C if liver ok)

Answers to Questions1: D2: A3: A4: C5: C6: B7: A8: part 1- D, part 2-C9: B10: C
11: A12: part 1-D, part 2-D13: C14: C15: D16: B17: D18: A19: B20: C

Information on the slides are compilations of the following references: Text Books:
◦ Adkinson NF, Bochner BS, Burks AW, et al. Middleton’s Allergy Principles and Practice. 8th Ed. Philadelphia, PA: Saunders; 2014.
◦ Adkinson NF, Bochner BS, Busse WW, Holgate ST, Lemanske RF, Simons FE. Middleton’s Allergy Principles and Practice. 7th Ed. St Louis MO: Mosby; 2009.
◦ Abbas AK, Lichtman AH, Pillai S. Cellular and Molecular Immunology. 7th Ed. Philadelphia, PA: Saunders; 2012.
◦ Bellanti JA. Immunology IV: Clinical Applications in Health and Disease. Bethesda, MD: I Care Press; 2012.
Board Review Materials:◦ MKSAP 16◦ Med Study Internal Medicine Review Core Curriculum 13th Edition (2009/2010)
Board Review materials were used to assist with case presentations and to ensure appropriate topics and key words were covered. Text Book references were used to ensure the science and specifics are the most up to date and accurate information.
Individual Journal Articles Referenced on applicable slides if appropriate
Reference Information