Embed Size (px)
Citation preview

Resilience
Leadership
July 2014
Population Health Management
Patient-CenteredCare
CONVERSATION:Accelerating workforce transformation in healthcareChanging the
Culture Change
Supported by The Healthcare Workforce Transformation Fund Training GrantCoordinated by Karen Moore, R.N., FACHE, Consultant, KMoore & Associates
Team Intelligence

MHA, through a grant from the Workforce Transformation Fund, presents this report, Changing the Conversation: Accelerating Workforce Transformation in Healthcare. We thank our more than 430 members who participated in the survey, which included interviews with leaders from hospitals around the commonwealth. The results of this survey present a call to action for executive leadership. The need to re‐design care around patients, engage in culture change, and leverage team intelligence have emerged as leading workforce goals throughout healthcare organizations. While re‐tooling the current workforce, leaders need to recognize the magnitude of the changes and the effect they will have on workers. The survey shows that resilience is a key factor in enabling the transformation to be successful. We’re learning that leaders can help transform their workforce by being a visible force for change and by supporting the retraining efforts within their organizations. This is an exciting and challenging time, and if done right, caregiving will gain effectiveness and efficiency. MHA plans to use this data to create a roadmap for our educational efforts over the next 3‐5 years. We will disseminate this report liberally in hopes that it will help provider organizations focus on training strategies to help the healthcare workforce evolve. We welcome your perusal of our survey report and look forward to hearing your thoughts on it. Sincerely,
Lynn Nicholas, FACHE President & CEO Massachusetts Hospital Association

TABLEOFCONTENTS
ExecutiveSummary……………………………………………………………………………………..p.1
I. Introduction……………………………………………………………………………………..p.2
II. Background………………………………………………………………………………………p.3
III. MethodsofInquiry……………………………………………………………………………p.4
IV. ReportofFindingsfromQualitativeInterviews………………………………….p.4
V. Survey……………………………………………………………………………………………...p.13
VI. SummaryofFindings………………………………………………………………………..p.19
VII. Weakness/BiasesandLimitations…………………………………………………….p.20
VIII. Conclusions……………………………………………………………………………………..p.20
Acknowledgements…………………………………………………………………………………….p.23
ReferenceInformationalSourcesandRecommendedArticles………………………p.24

1
ChangingtheConversation:AcceleratingWorkforceTransformationinHealthcare
EXECUTIVESUMMARY
Hospitalsandhealthsystemsneedtoaccelerateworkforcetransformationsothattheycanbesuccessfulinmakingthewide‐scalechangesneededtoredesignhealthcare.Togaingreaterunderstandingoftherealitiesofworkforceneedsandchallengesoverthenext3‐5years,theMassachusettsHospitalAssociation(MHA),fundedbyaWorkforceTransformationPlanningGrant,interviewedadiversesampleofleadersatMassachusettshealthcareorganizationsandconductedabroadsurveyofitsmembership.Acomplexpictureofemergingknowledge,science,androlesemerged,convergingonthechanginghealthcaredeliverysystem.Mostofthe459,000healthcareworkersinMassachusetts1havebeenpreparedforamodelofcarethathasbeenhospital‐centric.Yet,shiftingsitesofcare,accountabilityforcaremanagement,amorepatient‐centeredfocus,andnewskillsinteamcarearedrivingtheneedforchange.
Thechallengeofretoolingtheexistingworkforceisunprecedented.Duressamonghospitalworkersisevident.Despiteincreasedemploymentrates,healthcareworkforceproductivitynationally2continuestobethelowestthroughoutallsectors.Respondentswanthospitaleducationeffortstobemoreapplicabletochallengestheycurrentlyface,focusingmoreondealingwithchangemanagementandteamtraining.Specifically,theypointtoaneedforcreatingvaluefortheworkforcewherelearningpertainsdirectlytosupportingteam‐basedapproachestocare.Andthereisaneedforabroaderunderstandingofnewrolesandhowtheyoverlapwithexistingroles,aswellassupportofindividualcapacitytocopewitharapidlychangingenvironment.
Alleffortsatworkforcetransformationmustcomefromtheperspectiveofthepatient,respondentssay.Involvingpatientsandchroniclingpatientjourneysthroughtheirhealthcareexperiencewillbekey.Althoughtherehavebeeneffortsatimprovingthepatientexperiencethroughcustomerservicetrainingandprocessimprovementefforts,somefeeltheseeffortshavenothadtheexpectedimpact.Acceleratingtransformationwillcomenotjustfromwhatworkersdo,buttheconsciousnesswithwhichtheydoit.Itisthereforeessentialtoinvolvefrontlineworkersintheredesignofhealthcaredelivery.
Leadersandworkerswillneedtoshiftfromrigidroleandtaskorientationtowell‐definedcareerframeworksthatpromoteflexibilitytochangerolesandsettings,developnewcapabilities,andalterprofessionalfocusinresponsetothechangingenvironmentandtheneedsofpatients.Attentiontoroleintroduction,teamtrainingandinter‐professionallearning,aswellastheindividualworker’s
1 Massachusetts Healthcare Chartbook, Executive Office of Labor and Workforce Development, Commonwealth Corporation, Fall 2007, page 7. Accessed 7/25/2014
2 Kocher and Sahni, “Rethinking Health Care Labor,” New England Journal of Medicine, October 13, 2011

2
needforself‐care,reflection,andresilience,willallowcreativity,innovativelearningandcompassionateenvironmentsofcare.Finally,commitmentisneededtodedicateresourcestosupporteducationandtraining.Giventhewidescaleofworkforceredevelopmentneeded,thiscanbefacilitatedthroughcentralizedlearningcollaboratives,includingbothpublicandprivatefunding.
I. INTRODUCTION
ThepurposeofthisreportistoobtainacurrentunderstandingofhowhospitalandhealthsystemsinMassachusettsaretransformingtheirworkforcestomeettheneedsoftherapidlychanginghealthcarecommunity.
Massachusettshasledthenationintheredesignofhealthcaredeliveryoverthepast10years.Yethospitalsandhealthsystemsthecommonwealthareunderincreasingstrain.IntheU.S.,healthcareexpenditureshavegrownto17%ofGrossDomesticProduct(GDP),withprojectionstogrowto20%by2020.3However,inMassachusettstheunadjustedpercapitacostofcareissignificantlyhigherthantheU.S.average.Evenafteradjustmentforriskfactors,spendingis20%higher.
Whenlookingsolelyathospitalcare,MassachusettsexceededtheU.S.averageby41.6%,4andinlong‐termcareandhomehealthby72%.5Massachusettscostscontinuingonthistrajectorywilldoubleby2020.Furthermore,between2001and2011,theMassachusettsstatebudgethasincreasedby59%($5.1Billion)whileothersocialsupportneedssuchaspublichealth,mentalhealtheducation,andothershavebeencutby$20%($4Billion).6
Significantshiftsaretakingplacecatalyzedbyhealthcarepaymentreformtocreatenewandlargerhealthsystems,forgenewpartnershipsbetweenprovidersthroughoutthecontinuumofcare,andpilotinnovativewaystodeliverhealthcaretomeetthe“tripleaim”:improvingthepatientexperienceofcare(includingqualityandpatientsatisfaction),improvingthehealthofthepopulation,andreducingpercapitacostsofcare.
HealthcareemploymenthasoutpacedoverallemploymentintheU.S.,andyetthehealthcareworkforceislessproductivenowthanitwas20yearsago.(Productivityisdefinedastheoutputofvolumeofactivityperunitofcost.)InanarticlebyRobertKocher,M.D.andNikhilR.Sahni,publishedintheNewEnglandJournalofMedicinetitled“RethinkingHealthCareLabor,”theauthorsreportthatanyefforttoslowtherateofhealthcarespendingwillrequireachangeinlaborstructurebyreducing 3 Center for Medicare & Medicaid Services, National Health Expenditure Projections 2010-2011, Forecast Summary, Table 1, page 4.
4 The Henry J. Kaiser Family Foundation, Health Care Expenditures per Capita by Service by State of Residence, 2009, http://kff.org/other/state-indicator/health-spending-per-capita-by-service/ for notes and sources
5 Health Policy Commission, 2013 Cost Trends Report, July 2014 Supplement, p.12
6 Building a System of Care for Greater Value, presentation by Howard Grant, J.D., M.D., for the American College of Healthcare Executives, July 1, 2014

3
workers,loweringwages,orincreasingproductivity.Approachesthatencourageredesignofcaredeliverybyusingadifferentquantityandmixofworkersengaginginamuchhighervaluesetofactivitieswilldeliverthemostvalue.Theygoontocitetheneedtoleveragetechnologyandstandardizationofworktohelpeliminatewaste.Theauthorspointoutthateveryothermajorsectoroftheeconomyhasmanagedtosimultaneouslyimprovequalityandconsumersatisfactionwhilereducingcost.Thesameshouldbeachievableinthehealthcaresector.
InarecentHarvardBusinessReviewarticlebyMichaelPorterandThomasLeeM.D.titled,TheStrategyThatWillFixHealthCare:ProvidersMustLeadtheWayinMakingValuetheOverarchingGoal,theauthorsstate:“Wemustmoveawayfromasupply‐drivenhealthcaresystemorganizedaroundwhatphysiciansdo,andtowardapatient‐centeredsystemorganizedaroundwhatpatientsneed.”Dr.Leeremarkedinarecentpresentation,“Thechallengewithcaredeliveryforprovidersisthattherearetoomanypeopleinvolved,toomuchtodo,noonewithalltheinformation,andnoonewithfullaccountability.Theresultischaosanditleadstogapsinquality,safetyandefficiency.Thehealthcaresystemisunderduress.Weneedstrategiesthattranscendthepaymentmodel.Improvementofvalueisthemostrobuststrategyforallofthemajorproviderleversforsuccess.”
Theworkforceitselfisgettingincreasedattention.Howcantheworkforcetransformtoachievethetripleaim?Providersandworkersarebeingrequiredtolearnnewskills,workacrossnewboundaries,andcollaborateinunprecedentedwayswithcolleaguesaswellaswithpatientsandfamilies.However,workforcedeploymentremainsrigidandproductivitylags.
II. BACKGROUND
ThisreportwasmadepossiblebytheWorkforceTransformationFundPlanningGrantincludedinChapter224,whichwaspassedin2013withthegoalofbringingMassachusettshealthcarespendinggrowthinlinewithgrowthintheoveralleconomy.Thelawincludesmanyreferencestoimprovingthequalityofcareandbuildsontwopreviouslawsenactedin2008and2010thatexpandeddatatransparencyandreportingoncosttrendsanddriversaimedtocontrolpremiumgrowth.ThecomprehensiveChapter224introducedmandatesforprovidersandhospitalstoreviewcurrentpracticesandtoseekwaystofurtherimproveandredesigncare.
Thisgrant‐fundedproject,executedbyMHA,wasdesignedtogainunderstandingofthehospitalworkforcetrainingneedsnowandoverthenext3‐5yearsfromtheperspectivesofseniorexecutives,middlemanagers,andfrontlinestafffromMHAmemberhospitals.
OverthepastyearMHAhaslaunchedTheInstituteforCareCoordinationtoprovideeducationonskillsandexpertiseneededtoexcelatpopulationhealth/carecoordination.Thecarecoordinationroleisclearlyastartingpoint.ParticipantsintheInstitute’seducationalforumshavereportedhighvariabilityinunderstandingreformandothernewrolesbeingintroducedtopatientcaredeliveryenvironments.

4
Themovetonewmodelsofcaredeliveryiscreatingchallengesforworkersindifferentways.Somechallengesincludeunderstandingtheresourcesavailableinthecommunityforadequatecareplanning.Oneparticipantwhotookpartinthesurveystated:“Carecoordinationisworsethaneverwithfragmentedandcumbersomeelectronichealthrecords,changingfamilydynamicsbroughtonbyworkingfamiliesandsocioeconomics,andhealthcareproviderswhodon’treallyknowthepatient.”ManyoftheattendeesattheInstitute’sprogramsreportedafeelingofdisempowermentandconfusionaboutwhosejobitisto“fixthings.”Asignificantstressorreportedwasfeelingcaughtbetweensupportingpatientsandtheexpectationsforreducingcostswithoutfeelingtheyhadavoiceoraplaceformeaningfulinvolvementinchange.
Thisreportseekstounveilinformationanddatagleanedfromthisprojectthatwillhelphospitalsandhealthsystemswiththeirworkforcestrategies.ItisalsointendedtoassisttheMassachusettsHospitalAssociationoverthenext3‐5yearstoprovideneededsupport,education,andtrainingtoaccelerateworkforcechangesinthecaredeliveryenvironment.
III. METHODSOFINQUIRY
Themethodofinquirywastwofold:
1. Qualitative:Structuredinterviewswithhospitalleaderstogetinsights,perceptionsandthinkingfromthoseresponsiblefortheplanninganddeliveryofcare,andalsotoinformthedesignofthequantitativesurvey.
2. Quantitative:Thedisseminationofasurveytoobtaindataaroundknowledgeandskilldevelopmentneededinthehospitalworkplace.
TheprojectenlistedthesupportoftheGallupCompanyforsurveydesignandtoconductsomeoftheinterviews.

5
REPORTOFFINDINGSFROMQUALITATIVEINTERVIEWS
Atotalof16interviewswereconductedusingastructuredinterviewapproach.Participantswereallinvolvedwiththeplanninganddeliveryofpatientcareservicesandwereselectedtorepresentdiversemissionsandgeographiclocations.
Followingarethesetofquestionsposedtointervieweeswithsummarizeddescriptionsofthemeswhichemergedamongtheresponses.
1. Whattrendsorchangesinhealthcaredeliveryareofthegreatestinteresttoyourightnow?
Theresponsestothisquestionfellinto6themes:
DecliningreimbursementsresultingintremendouscostpressuresMHAmembersarefamiliarwiththeoverarchingissuesunderpinningtheneedforexpensereduction.However,seniorexecutivesandmanagersshouldnotoverestimatetheirworkforce’sunderstandingoftheseissues.ThereisagreatdealofvariabilityinbasicunderstandingoftheAffordableCareAct(ACA)andtheshifttonewpaymentmodelsorhowhospitalbudgetsevenwork.Oneoftheintervieweeswholedtheeducationalprogrammingofahealthcareorganizationstatedhehadfoundthiswassotruethatthehospitaldevelopedtutorialstobedoneonlinethatwereprerequisitesforsomeofthemoreadvancededucationalofferings.
Notallintervieweesledwiththeconcernofreducingexpenses.Therewasconsiderableawarenessofaneedtoprovidehealthcaretoapopulationofpeoplewhoseinsurancegivesthemgreateraccesstocarealongwiththeimplicationsforpartnershipsandcollaborationsthatneedtobecreatedinordertoachievethem.
Newmethodsofcaredelivery,providerrolesandpaymentmodelswiththedevelopmentofACOsandmedicalhomesMostintervieweesidentifiedchallengeswithworkingacrossmedicalsubspecialties,coordinatingpost‐acutecare,andcommunity/home‐basedservices.Newrolesarebeingcreatedorintroducedinnewsettings.Oneseniornursingleaderstated:“AneedforNursePractitionersisexploding.”

6
Inaddition,thereisashiftoftaskstoless‐skilledworkerswhiletheprofessionalcaredeliveryteamexpandsinitsexpertisetoincludepharmacists,nutritionist,andbehavioralhealthspecialists.Eventheseprofessionalsinnewsettingsrequiremoreflexibility,newskills,andcompetencies.
SocietalIssues:Demographicsofanagingworkforce,mixedgenerations,lackofdiversityintheworkforce,andsocioeconomicdisparityIntervieweesdiscussedthefactthattheworkforceoftendoesnotculturallyorethnicallyreflectthepatientpopulationbeingserved.Therearealsomixedgenerationsintheworkforce.With“organizationalculture”definedas“whathappenswhennooneislooking,”differentculturalperspectivesmayhinderstandardizingapproachestocare.
Thewillingnessofotherstospeakupwhensomeoneisn’tfollowingthroughisseenasimportanttobasicsafety.Thisischallenginginhospitalswithstronghierarchicalstructuresandtitlessuchas“Chief”and“Director”orwithleaderswhomaynotreflecttheculturaldiversityoftherestoftheworkforce.
Someorganizationshavereportedaddressingeconomicdisparitybyalteringbenefitsstructuresforlowerpaidworkers.
ShiftsawayfrominpatientutilizationAnactualoranticipatedtrendoflowerinpatientcensuswascited.Thesystemofcaredelivery,suchasitis,issetupsoitoftenworkseasiestonceapatientisadmittedtoahospital.Forexample,apatientreceivingcomplexcareintheemergencyroom,whoalsohasaknowndiagnosisandtreatmentplan,oftenendsupinaninpatientbed.CaseMangersinemergencyroomshavebecomecommonandhaveshiftedthefocusofemergencyroomcareplanning.Intervieweesdescribedcareplanningasgettingmorecomplex,requiringknowledgeofcommunityservicesandotheraspectsofthecontinuumofcare.
Theothersignificantimpactoflowerinpatientcensusisthattheinpatientsettinghastraditionallybeenwherecliniciansreceivedtheirtrainingandareexpectedtoworkwhenenteringtheworkforce.Manycliniciansfindtheycannotgetpositionsinhospitalsandareconcernedabouttheircareerchoice.Thereisgrowingdemandforcliniciansinmedicalhomes,outpatientsettingsandinthecommunity.Eventhesepositionsweredescribedastakinganexpertiseandfoundationoflearningfromhospitalexperience.
Abouthalftheorganizationsrepresentedbytheintervieweeshavenotyetexperienceddecreasinginpatientutilization,butareanticipatingafuturetrend.Theyhavebeenactivelylookingatpopulationswhoareusinginpatientservicesandcouldhavebeencaredforinalower‐costsetting.Someoftheseeffortsareresultinginshiftsofinpatientvolumefromtertiarycaretocommunityhospitals.

7
Informationtechnologyandbio‐technologyIntervieweesdescribedtheincreasingcapitalneededtodevelopandstaycurrentwithdemandsforpatientcare,data,andreportingneeds.Aphysicianreportedhavingtospendthreehoursdocumentingcareafterseeingapatientforanhour.ImplementationofanElectronicHealthRecord(EHR)wasoccurringinallofthehospitalsrepresented.Insomecases,thehospitalwasgoingfromapapersystemtoanEHRforthefirsttimeandothershadanEHRandweregoingtonewplatformsandvendors.AdoptingEHRsrequireslengthyplanningandimplementationperiods.Increasinginformaticsstaff,particularlycliniciansintheseroles,wasalsoatrend.
ThenewconsumerismofhealthcareandincreasedaccesstocareMorepatientshaveaccesstocareandarecoveredbyinsuranceplanswithhigherco‐paysanddeductibles(thatmayvarydependingonwheretheygoforcare).Thismayresultinpatientsseekingcareinlower‐costsettingsorforgoingcare.Thepatientwantstoknowwhatthecostimplicationsforcarewillbewhenaplanofcareorcourseoftreatmentisbeingdiscussed,representingincreasedchallengesforproviders.Atthesametimea“retail”environmentforhealthcareisemerging,givingcontinuumsmorechoicesbutdisruptingcontinuityofcareopportunities.
2.Hashealthcarereformrequiredyoutodevelopnewrolesorskillsinyourorganization/position?Howhaveyoudonethat?Hasitbeensuccessful?
Allintervieweesreportedthedevelopmentofnewrolesorskillsintheirorganizationsasaresultofchangesincaredelivery.However,mostdiscussedtheneedforamoreflexibleworkforcewith1)existingworkerstakingonnewrolesinnewmodelsofcare;2)shiftingemploymentsettings;and3)movingbetweenneededspecialtiesandchangingservicesoffered.
TakingonNewRoles:AfocusontheroleofnursingTheneedfornursepractitionersandthelackofthemwasasignificanttheme.Insomecasesteachinghospitalspartneredwithschoolsofnursingtoplaceadvancedpracticestudentsinclinicalsettings.Somecurriculumhasbeendevelopedtoaddresstheacculturationofnursepractitionersintoprimarycarepracticesettings.Despitethedecades‐longexistenceoftheroleofAdvancedPracticeRNs(APRNs)itwasfeltthatthereisstillalackofunderstandingoftheirroleandhowitisdifferentiatedfromthephysicianassistant.
Oneseniornursingleaderstatedthat,“theACAhasopenedupaccesstocare.However,oursystemsofcaredeliveryarenotready,particularlyforprimarycare.Massachusettshasnotbeenaleaderwithregardstotheroleofthenursepractitionerasitrelatestoregulationandreimbursement.Withanincreasingvolumeofpeopleseekingcare,therearedelaysinaccesstocare.Peoplearebeingseenwhentheirillnesstrajectoryhasmovedtoamoreacutelevel,resultinginsickerpatientsbeingseeninthehospital.Thisistrueforthosewithmentalillnessaswell.”

8
Manyoftheintervieweestalkedabouttheroleofnursingingeneralandreferencedthe2010InstituteofMedicinereport,TheFutureofNursing:LeadingChange,AdvancingHealth.Recognitionthatcaredeliverytakesateamandnursingcaredeliveryrequiressupportenablesnursestoworkat“thetopoftheireducation”andawayfromautilitarianfunction,andallowsthemtomovetowardsaccountabilityforcaremanagementandcoordination.
Thereisanincreasingneedcitedfornurseswithspecialtycertificationintheinpatientsetting,suchascriticalcare,emergencycare,andsurgicalnurses(includingRNfirstassistantstosurgeons).Traditionally,newgraduatenursesdidnotenterintotheserolesbutnow,almostallofthoseintervieweddescribedprogramstobringnewgraduatesdirectlyintospecialtyprogramswithextensiveorientationandmentoring.Insomecasesthishascreatedaddedstressforstaffsthatmaintainassignmentlevelswhilesupportingnewstaffacquiringcompetency.Someorganizationsweredevelopingnurseresidencyprogramsfornewgraduates.
ShiftingemploymentsettingsAspatientsmoveawayfrominpatientcarethereismoredemandforexperiencedRNsintheoutpatientsetting.CaseManagers(mostfrequentlynurses)wererecognizedashavingthesignificantrolechangeasitrelatedtodemandstoachievecontinuityofcarewhilemanaginglengthofstayandutilizationofservices.Theserolesareappearinginemergencyrooms,medicalhomes,andfollowingpatientsacrosscaresettings.Thetraininginvolvesbecomingmorefamiliarwiththeservicesavailableinacommunityinordertoputtogetheracomprehensiveplanofcare.
NewandexpandedrolesTherearenewtypesofhealthprofessionalsperformingnewfunctions.Forexample,healthcoachesandpatientnavigatorsarebeingimplementedintomedicalhomemodels.Thesehealthprofessionalscanbelicensedorunlicensedstaff,dependingontheirfocus.Ingeneral,highereducationalpreparationispreferredforpopulationmanagementofcomplexillnesses.
Intheoutpatientsettingtherehasbeenanexpansionofdutiesforpharmacists,nutritionists,socialworkersandmedicalassistants.Technologyhasmadethedelegationoffunctions–suchasvitalsignmonitoring,glucose,andotherlabchecks–easier.Onecommunityhospitaladoptedacurriculumforthemedicalassistantrolefromateachinghospitalmodel.Thisenabledthemtoadaptthesemodelsandnothaveto“reinventthewheel.”
Asworkloaddemandsincreaseforcasemanagers,someorganizationsareprovidingsupportroles(e.g.bachelor‐preparedsocialworkers)todomoreroutinedischargeplanning.Thisallowscasemanagerstospendmoretimeoncomplexcases,patientsandfamilies,andwithotherteammembers.Additionally,entry‐levelserviceroleswereidentifiedtoassistwithworkloaddemands.Oneexampleoftheserolesis“constantcompanions”whichhavebeenimplementedtohelpwiththeincreasingnumberofpatientswithbehavioralandcognitiveissues.

9
Anotherwaytominimizeemployedfull‐timeequivalents(FTEs)mightbetochangethenatureofpartnershipswithvendors.Servicessuchasfoodservices,housekeepingandclinicalengineeringarefrequentlyoutsourced.Withincreasingaccountabilityforthepatientexperience,costsofcare,andmaintainingcurrentknowledge,thesepartnershipscanlookmorelikeemployedrelationshipswherethestaffmaybeeligibleforrecognition,receivecommunications,orparticipateinstaffmeetingsandimprovementactivities.
Otherrolesdescribedwereprojectmanagersinnon‐clinicalandclinicalareasforfunctionsthatdonotfallwithintypicalclinicalservicelines,suchasdiabetesmanagement,palliativecareorspace/facilityplanningspecialists.Successwiththeseroleswasdescribedas“evolving.”Someintervieweessharedconcernsthatnotenoughattentionisplacedonintegratingrolesintoexistingpatientcaredeliveryteams.“Frequentlyotherpeopleontheteamdon’tunderstandanewroleandcomewiththeirownexpectationsofwhatthatpersonshoulddo.”Attimesnewrolesweredescribedasfragmentingcareandslowingthingsdown.Therecognitionthatthedeliveryofhealthcareiscomplexandrequiresateameffortisnotnew.”It’sjusthardtoputcoordinationintopracticewiththepaceweworkateveryday,”commentedonenurseleader.Itappearedthatmanyofthehospitalshadnotdevelopedcurriculum,competencies,orevaluationforteam‐basedcare.
3.Canyoutellmewhatyouthinkismosthelpfultobuildingaworkforce?Whatdoyoufindlacking(orbarriers)intransformingtheworkforce?
Theemploymentmarkethasbeenstrongsince2008whentheeconomiccrisishit.Infact,alloftheorganizationsrepresentedhadexperiencedlayoffs.Asaresult,mostvacantpositionshavehadmultipleapplicants,allowingorganizationstobeselectiveinhiring.Themostfrequentresponsetothequestionwastheexistingworkforceitself.Theaveragelengthofserviceinmanyorganizationsis15yearsorgreater.Despiteissuesaroundresistancetochange,loyalandexperiencedstaffwerethemostfrequentlycitedadvantagestotransitioningtheexistingworkforce.Theknowledgeofhowthingswork,thewillingnesstoorientandtrainnewemployees,andtheprideintheirworkwasoftendescribed,observedandcelebratedatroutineorganizationalevents.
Somehavereportedmeasureableimprovementwithinworkenvironmentsatisfactionthroughmoreemployeeengagement.ThoughsomeleadersfeltdesignationssuchasMagnetattractedandretainedstaff,theycouldnotpointtospecificevidencetoconfirmthesereports.AseniornursingleaderfromateachinghospitalwithMagnet‐designationnoted,“Formorethan10yearstherehasbeenaminimumhiringrequirementofaBSNforstaffnurses.We’vehadnoproblemattractingnurses.”
BarriersDespitesomeofthepositiveexperiences,therewerebarrierstotransformationneedsthatweredescribed.Thoseinclude:afearofdelegatingtransitiontasksofcaretoothers;newrolesnotbeingembracedbystaff;andlaborcontractlanguagethatmakesitchallengingtocreatenewroles(orexpandrolesofothers).Anexamplecitedofthelatterwastheimplementationof

10
residencyprogramsfornewnurses,recommendedbytheInstituteofMedicine’sFutureofNursingReport.Oneseniornursingleaderreportedthatinordertoimplementtheresidencyrolefornurses–muchlikethemodelforphysicians–alowersalaryscalewouldneedtobeimplemented.Theorganizationhadbeenunabletoimplementtheresidencyprogrambecauseunionleaderswouldnotagreetothelowerpayscale.
Otherbarrierswerewidevariationintheunderstandingofhealthcarepolicyandreform,whichformthefoundationfornewstrategiesbeingimplemented.Onedirectorstated,“There’salotoftalkaboutinter‐professionallearning,buttherereallyisnotmuchgoingon.Muchofthecollaborationneededtodelivercaredependsonexistingrelationshipsandorganizationalculture.”
Thoughintervieweesbelievedthatphysiciansandemployeeengagementstrategiesweremakingincrementalimprovementsinwaysofworkingmoreeffectivelytogether,therewasstilla“disconnect”betweenthetopoftheorganizationandthefrontlines.Onemanagerdescribedthepositiveresultsofleanprocessimprovement,butfeltthatleanwasn’talwaysembracedbyseniorleaders.
Onedirectorstatedthatalthoughcustomerservicetrainingwasavailable,itdidn’tnecessarilyresultinstaffinnatelyfeelingcompassionorunderstandingoftheperspectiveofthepatient,familyoracolleague.Inreflectingonwhycustomerserviceprogramshavehadmixedsuccessinhospitals,oneseniorleaderstated,“Thereisanawarenessoffatigueintheworkplaceforeducationtargetedat‘fixing’thestaff.Oftenwhentherearebehavioralproblemsintheworkplace,itcomesfromfearandlackofcommunicationandunderstanding.Whenfearisthebasicmodusoperandi,it’sdifficulttoexpectchange.”
Realtransformationcomesnotfromwhatworkersaretoldtodo,buttheconsciousnesswithwhichtheydoit.Thereisvariabilityinthelevelsofawareness.Thiscontributestotheabilitytoacceleratechangeintheworkenvironmentmorethanhasbeenrecognized.Intervieweestalkedabouttheresilienceoftheworkforceas“confidenceinmanagingchange.”Ifchangemanagementprogramsarenothandledcorrectly,employeesdevelopapathytoimposedprogramsfeeling“thistooshallpass.”
4.Wheredoyoulooktohirepeoplefrom?Whattypesofpeopleorexpertisewouldyouliketohaveonstaffthatyoufeeliscurrentlymissinginorderforyourorganizationtobesuccessful?
“Wemayhaveastronghiringenvironment,butthecurrenthealthcareworkforcewaseducatedandhasworkedinamodelthatdoesn’texistanymore,”statedaseniornursingexecutive.Allbutoneoftheintervieweesdescribedstrategiestolookinternallyforworkforcetransformation.Theoneexceptionnoted:“Weliketohireentry‐levelemployeesfromindustriesthathaveplacedemphasisoncustomerservicetrainingsuchasDunkinDonutsandMcDonald’s.”
Oneorganizationreporteditsinternalstrategyistohirefromwithin;thisincludeshiringandorientingstaffwithoutspecificpositionsavailable,aswellassuccessionplanningtopromotefrom

11
withintheorganization.Othereffortsincludedscreeningandinterviewingstrategiestohireforvaluesandqualitiesthatsupportteamworkandcompassion.Whatintervieweesareseekingare“teachable”staffandthewillingnesstobeflexibletochangerolesandsettings.
Theneedforbetterandmoreseamlesscareerladdersthatwillallowworkerstoretrainfordifferentsettings,servicesandpopulationswerealsoidentified.
Severaloftheintervieweesreportedchallengeswithrecruitingandretainingnursedirectorsandmanagers.Therewasconcernthattheserolesdonothavethesupportsorsalarylevelsthatwouldmakethemadesirablecareerpath.
5.Whatapproacheshavebeentakentosupporttheeducationalneedsandongoingacquisitionofnewcompetenciesintheworkforce?
Anumberofapproachesaretakentosupporttheeducationalneedsofhealthcareworkerswhoareknowledgeworkers;examplesincludeformaleducationalclasses,attendanceatoutsideconferences,andrequiringcertaincredentialsorcertificationsforthecorrespondingposition.
Timeforlearningisconsideredasignificantbarrier.Howevertheincreaseinon‐line,orinshorterintervaleducation,hasmadeitmoreattainableforstafftoparticipate.Attendingoutsideeducationthatmayteachaboutanapproachtocareadoptedatateachinghospitalisnotviewedasvaluablebythestaffinacommunityorpost‐acutesetting.Ideally,asstaffdevelopexpertise,theyvaluelearningrightonthejob.Accesstosupervisors,educatorsorclinicalspecialistsareideal,butwithbudgetcutsandwithmanagementstaffspendingmoretimeawayfromdepartments,ithasbeenachallengetomaintaintheserolesorthepresenceofmentors.
Newinformationsystemsandtheelectronicmedicalrecordhaveandwillcontinuetoconsumetrainingtimeasthesesystemsareeverchangingandregularlyupgraded.Everyinterviewee’sorganizationwasworkingwithahybridofmodelsrequiringstafftonavigatethroughdifferentsystems.Aseniorexecutivereportedthat,“Aphysiciantoldmeofacasewherehespentahalfhourwithapatientandittranslatedtothreehoursofcomputerwork.”
Simulationtrainingisbeingusedforclinicaltrainingandincreasinglyforteamtraining.
6.Howiseducation/trainingfunded?Isthefundingadequate?
Organizationsreportedvariedcommitmenttoeducationanddevelopment.Forinstance,thegoaltoattainMeaningfulUsemayresultinfundingtosupportITtraining.Mostorganizationsprovidededucationforupdatesonnewequipmentoreducationrequiredforimplementationofnewpolicies,orcredentialingandaccreditationrequirements.
Teachinghospitalsreportedmoreongoingclinicaleducationandpaidforcertifications(whichtypicallyrequiredemonstrationofongoinglearning).Outsideconferenceswerefrequently

12
mentionedfornursing,physicianleadersandseniorexecutives.Withtightbudgets,mostorganizationsaretryingtoevaluatethebesteducationvalue.Seekingphilanthropydedicatedtoeducationisemergingincommunityandteachinghospitals.
7.Wheretherearegapsinprovidingforeducationalneeds,whatwouldprovidethemostvalue?
Useoftechnology.Forexample,accesstoweb‐basedtrainingwasusedbyallorganizationsrepresented.Thisallowsorganizationsnottohavetodevelopallofthecontent.
Thereisaneedformoreinter‐professionaleducation,includinguseofsimulationtechnologyandmodelsofteamtraining.
Hospitalswanttheabilitytointegratelearningwithworkimmediately.Severalorganizationsdescribedthevalueofbringingteamstogethertohelpsolvecurrentproblemswithintheirdepartments.
MaureenBisognano,CEOoftheInstituteforHealthImprovement,spokeabout“flippingeducation”inher2013keynoteaddressattheAnnualMeetingoftheInstituteforHealthcareImprovement.Theconceptofchangingthetraditionalclassroommodelwherestudentslearnthengooutandtrytoapplywhattheyhavelearnedgets“flippedwheretheybringtheir‘homework’intotheclassroomandtheteacherismoreofa‘guide’tounlockingthesolutionsfortheproblemsencountered.”
8.Whataresomeemergingareasofpatientcaredeliverythatyouthinkrequirenewskill,rolesorresponsibilities?
PopulationHealthManagement:Althoughmodelsandevolvingcertificateprogramsareoutthere,thereisstillaneededforcliniciansaswellasexecutivesthatfosterlearninganddevelopmentofevidenced‐basedpractices.
Short‐termacutecare:Thenursepractitionerroleintheinpatientsettingincludesafocusoncaremanagementandcoordination.
Datamanagement:Asmoredatabecomesavailableregardingoutcomes,itneedstobereportedinatimelyandunderstandablemannertoallowtheteamtotakeaction.Dataspecialistsembeddedinclinicalteamswouldimprovethisarea.
Navigatorstoworkdirectlywithspecificpatientpopulationsandassistthemwithcaremanagement.
Leadershipinatransformingenvironment:Theroleofleaders–fromseniorexecutivestofrontlinesupervisors–ischangingrapidly.Thereisrecognitionbyintervieweesofthebarrierspresentedbythehierarchy.Theconceptof“teamintelligence”wasdiscussed.ThisisdefinedbySuzanneGordon,authorandjournalistwhohasstudiedhospital

13
environments,as“Theactivecapacityofindividualmembersofateamtolearn,teach,communicate,reasonandthinktogether,irrespectiveofpositioninanyhierarchy,intheserviceofrealizingsharedgoalsandasharedmission.”Intervieweesnotedtheneedforleadershiptorecognizeandsupportcapacityforteamlearningintheirorganizations.Thisultimatelyresultsinlessdependenceonhierarchyforproblemsolving.Otherexamplesfocusedoncreatingmoreconnectionbetweenleadersandfrontlineworkers,throughinitiativeslikeleanprocessimprovementandregular“rounding”indepartments.
IV. SURVEY
Thepurposeofthesurveywasto:
1. Identifypriorityknowledge,trainingandeducationneedsinthehospitalworkplacenowandoverthenextthreeyears;
2. Identifybestpracticesforaccessingeducationandhighestvaluepointforthelearner;
3. IdentifywaysMHAcancontributetosupportingmembers’workforcetransformationneeds.
Thesurveywasdistributedelectronicallyto5,187individualsfromthemembershipdatabase.ItwasavailablebetweenMay15toJune1,2014.Therewere438responsesforan8%returnrate.
SurveyresultsRespondents
Thefollowingchartshowsthebreakdownoftherolesofthe438respondents:

14
Thefollowingchartshowsthebreakdownofthetypeofhospital(teachingorcommunityhospital)orpracticegroup.
Therespondentsrankedthetopareasthattheyseeasareasofeducationneeded.Theareastheyidentifiedinrankorder:
1. CreatingEngagementBetweenPatients&Staff
2. CMS/HealthcareRegulationUpdates
3. LeadershipDevelopment
4. ChangeManagement
5. DataAnalysisandManagementSkills
6. ConflictManagement
7. EmergingTrendsinHealthcare
8. HealthcareTechnologyTrendsandPracticalApplications
9. EffectiveCommunication
10. BuildingResilienceintheWorkforce

15
Togetasenseofperceivedstaffingissueswithintheorganization,weaskedrespondentstoindicatethetopthreepositionsthattheirorganizationneedstofill.Table3showstheirtopfourrankings:
Weaskedrespondentstoindicatetheirlevelofcomfortwiththeknowledgetheyhaveinanumberofareas.Belowarethetop3areastheyindicatedthemostdiscomfort,with#1beingtheareawiththemostdiscomfort:
1. Emergingtechnologyandbiomedicaldevices
2. Behavioralhealthmanagement
3. Populationhealthmanagement
Weaskedmemberstoranktheareastheyarepersonallymostinterestedinmoreeducation:
10.75
8.75

16
Inmovingawayfromhowrespondentsperceivedtheirownknowledgeneeds,weaskedabouthowlearningneedsareviewedfortheorganizationasawhole.Thetop6outof20areasofperceivedorganizationalneedforknowledgewere:
1. Buildingaresilientworkforce2. Stressmanagement3. Changemanagement4. Leadershipinatransformingenvironment5. Datamanagementanduse6. Populationhealthmanagement
Note:Thedatashowtherespondentsseetheneedsoftheorganizationdifferentlyfromtheirownneeds–e.g.,lowneedforchangemanagementskillsforindividual,buthighneedidentifiedattheorganizationallevel.Thereisahigherrankingofimportanceofskillatmanagingthecontextforreformovernewtechnicalorclinicalskillsets.Theprioritizationisfortheorganizationtoaddressstress,buildingaresilientworkforce(definedattheabilityoftheworkforcetodealwithconflictandchange,andtodevelopleaderswithtransformationalskills.
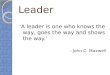
Weaskedrespondents“howpreparedorunprepared”theirorganizationiscurrentlytomeettheemerginghealthcareneedsoftheircommunity.
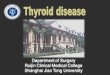
94.19%ofrespondentsfeltthattheirorganizationwas“prepared”,“wellprepared”or“verywellprepared.”Weaskedrespondentswhatarethebarriersforkeepingupwithhealthcaretrends.
0
10
20
30
40
50
Lack of Time Budget Constraints Other
Percent
Barriers
Largest Barriers for Keeping Up with
Healthcare Trend
31.72
Note:LackoftimeandBudgetRestraintsmadeupnearly75%oftherankingofbarrierstokeepingupwithhealthcaretrends.
43.22
25.06

17
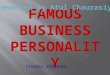
Weaskedrespondentstoreplytothisstatement:Iunderstandhowmyjobisrelatedtothemissionandpurposeofmyorganization.
Note:0%said“don’tknow/notsure”Thismayreflecttheemphasisoverthepastdecadeonthepatientexperience,customerservice,importanceofteamwork,introductionofprocessimprovementteams,rootcauseanalysis,andassuringthatemployeesareknowledgeableregardingthemissionandvisionofthehospital.
Weaskedrespondentstoreplytothisstatement:IhavetheknowledgeIneedtodomyjobright.
76.33
88.16

18
Weaskedrespondentsaboutthegenerallevelofsatisfactionwithresourcesprovidedforeducationintheirorganization:
Methodsoftrainingpreferredareindicatedbelow.Hybridtrainingwasidentifiedbyfarasthemostpreferred.
Percent
53
14.98
14.52
13.36
4.14

19
Preferencesforlengthoftraining:
Note:Lessthan7%preferredamulti‐daytrainingsession
V. SUMMARYOFFINDINGS
Apictureemergesofaworkforcethatunderstandstheeffortsandstrategicchangestheirorganizationsaremakingtorespondtohealthcarereform.Therespondentsalsoreportfeelingahighdegreeofconnectiontotheorganization’smission.However,thedegreeofconflictandstresswithintheorganizationandlearningacrossteamsappearstobeundergoingsignificantchallenges.
Respondentsprefertousetheirlimitedtimeonlearning–specificallythatwhichdirectlyappliestotheknowledgeneededfortheirroles.Thislearningshouldbedeliveredinwaysthatresultinaddingvaluetothoseissueswithwhichtheyarecurrentlystruggling.Theapproachtolearningmaydifferdependingonthetopic.Forexample,learningtoworkasateamisnotconducivetowebinarformat.Inter‐professionallearningdoneinanenvironmentthatisnotviewedasrelevanttoanindividual’sworkenvironmentmaynothaveaddedvalueeither.
Thesurveydemonstratesthatworkforcetransformationmustbedoneinsuchawayastoaddvaluetotheorganizationandtheindividual.Ashealthcarechangesfromavolumetoavalueproposition,somusttheapproachtothedevelopmentoftheworkforce.Understandingofroles,teamlearning,andindividualresiliencearethefoundationfortransformingthecurrentworkforce.Responsessuggestthatiftheenvironmentissupportedcorrectly,thestaffitselfwillengageinawaytoassuretheirlearningneedsaremetinwhatismorelikelytobeamoreproductive,efficientandrewardingmanner.

20
VI. WEAKNESS/BIASESANDLIMITATIONS
ThesurveyandassessmentwasaninitialinquiryintothedynamicspresentinMHAmemberorganizations.Theconditionofanonymitywasimportanttosupportingtheauthenticityoftheinformationobtained.Theapproachofexaminingconcurrentqualitativewithquantitativedataisidealbutmaynotdirectlycorrelate.Theassessmentofworkforcetransformationneedswasobtainedfromtheopinionsofabroadrepresentationofindividualsinhealthcare.Thisservesasastartingpointforthereinforcingandrestrainingforcesofchangeandultimatelyapathtosupportthehealthcareworkforcetransformation.Nopatientsorfamiliesparticipatedinthesurvey.
Therewassignificantemphasisanddiscussionregardingtheroleofnursinginthecontextofhealthcarereform.Thismayreflectthenumberofnursesinterviewed;however,literaturesupportedtheirperceptions.Theimportanceoftheinterdisciplinaryteamandnewrolesemergingarerecognizedandthereisanevolvingunderstandingofthenursingvaluepropositionisalsogainingfocus.Additionalstudyandreferencesincludedinthisreportpointtoopportunitiestolookwideranddeeperintootherteamrolesandskillsets.
VII. CONCLUSIONSHealthcareexpendituresaccountforasignificantpercentageofthenationalandstateeconomiesandcontinuetogrow.HealthcareorganizationsinMassachusettsandtheirworkforcesareincreasinglystrainedasmorepeopleenterthehealthcaresystemasaresultofcoverageexpansion,demandingnewapproachestocaredelivery.Itiswidelyrecognizedthatdevelopingandsupportingaproductiveworkforceisessentialtoloweringper‐capitacostsofcare.Itistimetoexpandonhowtoalignpaymentsystemsandnewmodelsofcarewithhowtotransformthehealthcareworkforceinordertodelivernewmodelsofcare.
WeappeartobefortunateinMassachusettsthatwithinourhealthcareorganizationsthereisanappreciationfortheworkforce’sknowledge,loyalty,andprideinwhattheydo.Itisthereforealsoimportanttolookcloselyatthestrengthsoftheworkforce.Thesurveyrespondentsreportstrongbeliefintheirhospitalsandfeelingconnectedtothemission.However,theunprecedentedchallengeofretoolingthecurrentworkforceforthepresentandforeseeablecircumstancespresentslargerbarrierstoremodelingeffectivecaredelivery.
Earlyadoptersarepilotingnewroleswhichareintendedtogivegreaterattentiontoteam‐baseddeliveryofcareandaccountabilityforoutcomes.Teamtrainingeffortsareintheirearlystages.Thereissignificantfocusontheroleofnursingasanextpointoffocus.Aswithallearlyinnovations,therearelessonstobelearned,improvementstobuildupon,andknowledgetodisseminate.However,thereareconsiderableculturalbarrierstochangingtheworkforce.It’simportanttonotethatlackofprogressonawidescale‐change,however,willcomeatagreatcostoflimitedproductivitythatisalreadyata20‐yearlow.Theburdenofthatcostcouldsignificantlyobstructtheabilitytomakeadvancementsintheredesignofcaredelivery.

21
Engagementoffrontlineworkersiscriticalinordertoconnectstrategicvisionwithexecution.Mosthealthcareworkershaveimportantideasforimprovinghealthcaredelivery.Itisunderstoodthatfixed,layered,fragmentedapproachestoanywork,butespeciallycomplexworkwheretherearefrequentdecisionpoints,requirespeopleandteamsworkingwithintelligence.Thenew“teamintelligence”developswithafoundationofaresilientworkforceenergizedbypossibilityinsteadoffear,understandinginsteadofconfusion,andauthoritythatcomeswithownership.Clearandongoingcommunicationbetweenleadershipandthefrontlinesiscritical.
Healthsystemchangewillrequireaworkforcewithroleandcareerflexibility.Leadersandworkersneedtoshiftfromrigidroleandtaskorientationtowelldefinedcareerframeworksthatprovideflexibilitytochangerolesandsettings,developnewcapabilitiesandalterprofessionalfocusinresponsetothechangingenvironmentandtheneedsofpatients.Laborunionswillalsoneedtobringanewvisionofpotentialtowhatwillcreatecareerlongevityandopportunityandworkwithhospitalstocreatenewandmoreflexiblestructures.
Startwiththequestion:Whatdoesthepatientneed?Manyoftheintervieweesusedexamplesofcomplexcarejourneyswithfamilymembers.Byretoolingtheworkforceandacknowledgingpatientstories,staffwillbeabletocreateidealjourneysthatincludethepatientandfamilyperspective.Knowingthepatient,integratingcareandmanagingtransitionsbetweenhome,outpatient,andacutesettingsiscriticaltodefineandtrainasateam,evaluatingresultsfromthepatientperspective.
Movingaheadandreframingsubsequentquestions:Asgreaterunderstandingisacquiredarounddiseasemanagement,carecoordination,andpatientneedsthenextstepistoposemorequestions:
‐ Doestheworkforcehavetherightskillsandcompetenciesneededtofunctioninnewmodelsofcare?
‐ Whatrolesareneededandhowcandifferentskillconfigurationsbestmeettheseneedsindifferentgeographiesandpracticesettings?
Importantconsiderationstomovingahead:
Afocusonhavingfewerteammembersaroundasmallerpopulationofpatients. Trainingindividualsfornewroleswitheducationandtrainingthatisconvenient,timely,andwithfinancialincentivesthataretakenintoconsideration.
Trainingteamstoacceptnewroles;otherteammembersneedtounderstandthecontentofnewrolesandfeeltheindividualisappropriatelytrainedtotakeonthenewrole.Theyalsoneedtounderstandhowthenewrolefitsintoworkflowandoverlapswiththeircurrentrole.
Attentiontoindividualresilienceandvitality:educatingprovidersandsupportingworkenvironmentsthatvalueself‐care,reflection,andrespectwillpromotecreativity,innovation,andcompassion.

22
Leadershipcommitmenttoresourcingworkforcetransformationincludingthedevelopmentandsupportfortransformationalleadershipskillsandstandardizingtheirownworktopartnerwithfrontlineworkers.
Applyfocustoredesigningcurriculumforstudentsinthepipelinetoincludenewsettingsforeducationandexposuretorolesandaccountabilityforcare.
Itwilltakeaconsistentcommitmentofresourcestoachievetheretoolingofthecurrentworkforceduringachallengingtimeforhealthcare.Considerationsfornewwaysoffundingorpartneringwithotherorganizationwillneedtobeconsidered.Thisfundingwillnotbejustorganizationbased,butshouldbeaimedatsupportingwidescalechange.

23
ACKNOWLEDGEMENTS
Deepappreciationmustbeextendedtothe16individualswhorepresentedfrontlinestaff,mangers,directors,seniorleadersandhospitalCEO’swhomadethemselvesavailablefortheinterviews.Theircandorandpersonalcommitmenttounderstandingandaddressingtheneedsoftheworkforcewasevident.
SeveralotherleadersprovidedperspectiveforthisreportrepresentingtwoorganizationsthatservetoleadchangeinhealthcareinMassachusettsandbeyond:SharonGale,CEO,OrganizationofNurseLeadersofMassachusettsandRhodeIslandandJoanneHealy,SeniorVicePresident,EducationandDevelopmentfortheInstituteforHealthcareImprovement.
TheGallupCompanywasengagedforassistancewiththestructuredinterviewquestionsandsurveydesign.However,itsstaffwentwellaboveandbeyondtheirscopebyaccessingsupportfromtheirconsiderablytalentedteaminordertoproducemeaningfulinformation.
Andlastly,thestaffoftheMassachusettsHospitalAssociationwhosespecificjobitistounderstandthelearningandeducationneedsofthosewhoareresponsibleforfuturecaredeliveryandwhoaremakingourhospitalsandhealthsystemsthesafest,bestexperienceforallpatientsandfamilies.RecognitiongoesespeciallytoPatNoga,RN,PhD,VicePresident,ClinicalAffairs;KirstenSingleton,CAE,ExecutiveDirector,CenterforEducation&ProfessionalDevelopment;andJillEttori,Marketing&EventsSpecialist.LynnNicholas,FACHE,CEO,championedtheapplicationforfundingforthisreportsothattheconversationaboutworkforceneedscouldbeelevatedknowingthepowerofcollectivethoughtandcollaborationthroughouttheCommonwealth.

24
REFERENCEDINFORMATIONALSOURCESANDRECOMMENDEDARTICLES
Porter,MichaelE.andLee,ThomasH.“TheStrategyThatWillFixHealthCare;providersmustleadthewayinmakingvaluetheoverarchinggoal.”HarvardBusinessReview,October2013.“Team‐Basedcompetencies;BuildingaSharedFoundationForEducationandclinicalPractice,RobertWoodJohnson,ConferenceProceedings,February16‐17,2011,WashingtonD.C.“WorkforceRolesinaRedesignedPrimaryCareModel”AmericanHospitalAssociationRoundtable,2011.“ReconfiguringtheBedsideCareTeamoftheFuture.”AmericanHospitalAssociation,Roundtable,2014.“RedesigningtheCareTeam;TheCriticalroleofFrontlineWorkersandModelsforSuccess.”EngelbergCenterforHealthCareReformatBrookings.March014Gordon,Suzanne,Mendenhall,PatrickandO’Connor,BonnieBlairBeyondthechecklist;WhatElseHealthCareCanLearnfromAviationTeamworkandSafety.IRLPress2013.Swenson,S,Pugh,M.McMullan,C.,KabcenellA.HighImpactLeadership:Improvecare,ImprovetheHealthofPopulations,andReduceCosts.”IHIWhitePaper,Cambridge,MA:InstituteforHealthcareImprovement;2013.CriticalRoles:California’sAlliedHealthWorkforceFollowUpReport,CaliforniaHospitalAssociation,March2014.InstituteofMedicineoftheNationalAcademies.TheFutureofNursing:LeadingChange,AdvancingHealth.ReportBrief.October2010Kocher,Robert,MDandSahni,NikhilR.“RethinkingHealthcareLabor,NewEnglandJournalofMedicine365:15October13,2011.